3: Documentation
1. List the five purposes for patient records.
2. Describe the electronic health record (EHR) and the personal health record (PHR).
3. Determine when the use of Situation, Background, Assessment, and Recommendation is beneficial.
4. State important legal aspects of chart ownership, access, confidentiality, and patient care documentation.
5. Describe differences between traditional and problem-oriented medical records.
6. Describe the basic guidelines for and the mechanics of charting.
7. Describe the differences in documenting care with activities of daily living and physical assessment forms, narrative, SOAPE, and focus formats.
8. Discuss documentation and clinical (critical) pathways.
9. Discuss home health care documentation.
10. Discuss long-term health care documentation.
11. Discuss issues related to computerization in documentation.
Key Terms
auditors
(p.
41
)
chart (health care record)
(p.
40
)
charting
(p.
40
)
charting by exception
(p.
48
)
computers on wheels
(p.
42
)
database
(DĀ-tă-bās, p.
42
)
diagnosis-related groups
(p.
41
)
documenting
(p.
40
)
electronic health record
(p.
40
)
electronic medical record
(p.
40
)
informatics
(p.
43
)
ISBAR
(p.
43
)
Kardex (or Rand)
(p.
48
)
narrative charting
(p.
45
)
nomenclature
(NŌ-mĕn-klā-chŭr, p.
43
)
nursing care plan
(p.
48
)
nursing notes
(p.
42
)
patient portal
(p.
43
)
peer review
(p.
41
)
personal health record
(p.
43
)
point-of-care
(p.
42
)
problem list
(p.
46
)
problem-oriented medical record
(p.
46
)
quality assurance, assessment, and improvement
(p.
41
)
recording
(p.
40
)
SOAPE
(SŌP, p.
46
)
SOAPIER
(SŌP-ē-ŭr, p.
46
)
traditional (block) chart
(p.
45
)
The chart (health care record) has never been more important in the health care system than it is today; it is a legal record that is used to meet the many demands of the health, accreditation, medical insurance, and legal systems.
The process of adding information to the chart is called charting, recording, or documenting. Documenting involves recording the interventions carried out to meet the patient’s needs. In the charting of interventions, documenting the type of intervention, the time care was rendered, and the signature and title of the person providing care is essential. Anything written or printed that is a record or proof of activities will play a role in this process. Although many details are necessary to remember when documenting in the chart, the process is not difficult but is often time consuming. Good documentation reflects the nursing process. Documentation is an integral part of the implementation phase of the nursing process (see Chapter 5) and is necessary for the evaluation of patient care and for reimbursement for the cost of care provided. In the past, all documenting in the patient’s health records involved written documentation. Today a majority of facilities use some form of electronic health record (EHR), also sometimes referred to as electronic medical record (EMR). EHRs are used in various settings, including hospitals, long-term care settings, health care provider’s offices, clinics, and home care agencies.
The licensed practical/vocational nurse (LPN/LVN) must understand how to use medical records
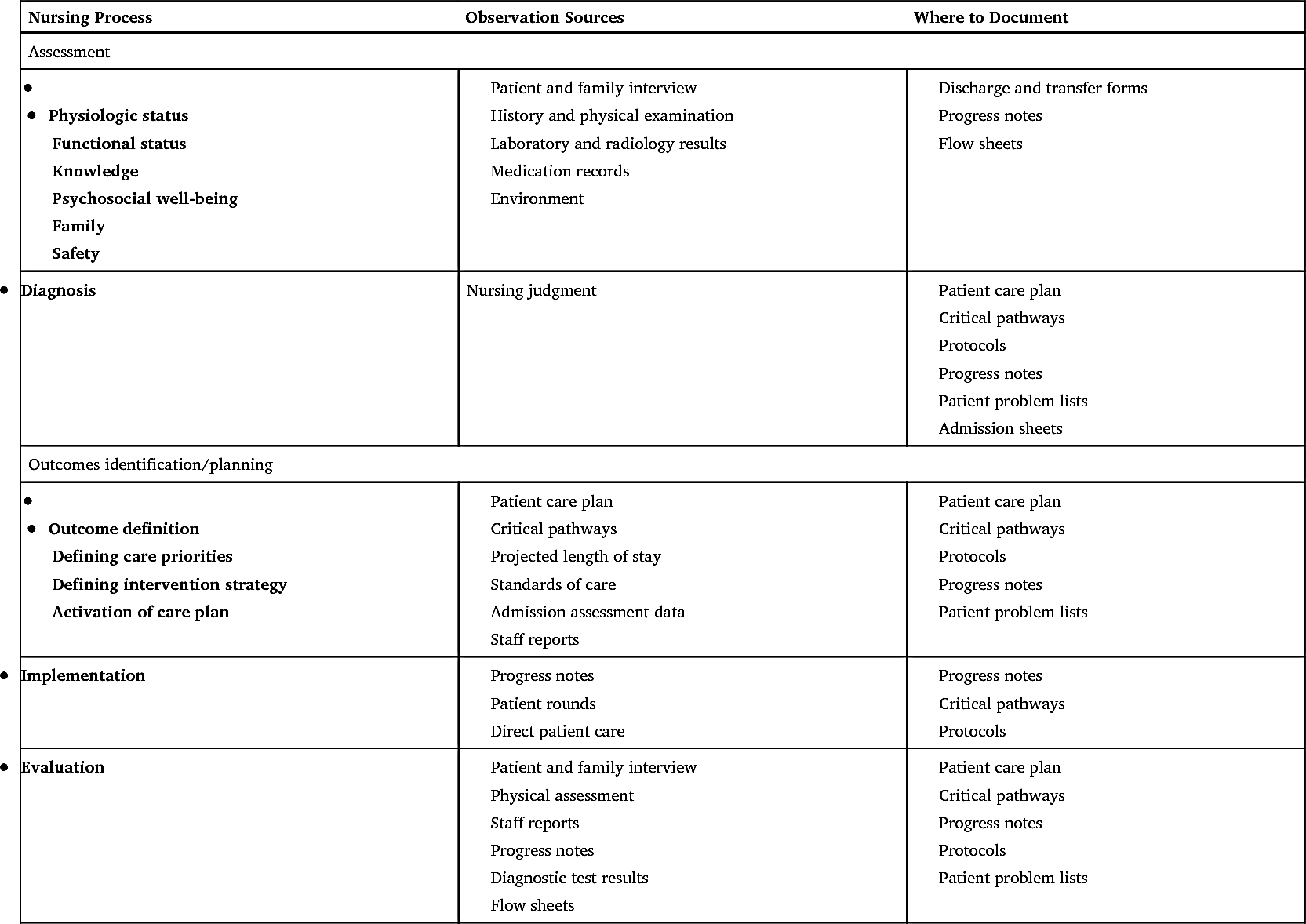
effectively and efficiently. This chapter addresses the purposes for health records, the common types of records, the basic guidelines and rules for documentation, and legal concerns. Knowledge of these guidelines and the ability to chart completely, accurately, and legibly (when using written records) are requirements for licensure and employment as a nurse. See Table 3.1 and Chapter 5 for information on the nursing process and documentation.
Purposes of Patient Records
The five basic purposes for accurate and complete patient records are (1) documented communication; (2) permanent record for accountability; (3) legal record of care; (4) teaching; and (5) research and data collection.
The patient’s chart provides a concise, accurate, and permanent record of past and current medical and nursing problems, plans for care, care given, and the patient’s responses to various treatments. The record facilitates accurate communication and continuity of care among all members of the health care team. Recorded information is not as easily lost or altered as the spoken word. Proper charting covers all areas of patient needs and concerns: physical, emotional, psychological, social, and spiritual.
This permanent record sometimes is used by various government and other agencies to evaluate the institution’s patient care, to justify cost reimbursement for care provided, and to establish or review accreditation. Current regulations require chart audits (review of specific chart components for completion and appropriateness) by officially appointed auditors (people appointed to examine patient charts and health records to assess quality of care). Auditors check to see whether all ordered care was charted as given and whether responses to specific care plan items and treatments are noted. Institutions have medical and peer review systems (an appraisal by professional coworkers of equal status). Peer review appraises the manner in which an individual nurse conducts practice, education, or research. Institutions also have specific procedures to provide for quality assurance, assessment, and improvement, which is an audit in health care that evaluates services provided and the results achieved compared with accepted standards. Accurate and legible records are the only means institutions have to prove that they are providing care to meet patient needs and established standards.
Cost reimbursement rates by the government plans (Medicare, Medicaid) are based on the prospective payment system of diagnosis-related groups (DRGs; a
system that classifies patients by age, diagnosis, surgical procedure, and other information with 25 major diagnostic categories and hundreds of different sub-categories to predict the use of hospital resources, including length of stay, resulting in a fixed payment amount) (CMS, 2019). Many private insurance companies now use similar illness categories when setting hospital payment rates. Institutions are reimbursed by insurance companies or government programs only for documented patient care. The payers carefully review various items in patient medical records, including the nursing notes (the form on the patient’s chart on which nurses record their observations, the care given, and the patient’s responses), when deciding whether the necessary and ordered care is being given or was given.
The patient chart or health record is a legal document; when necessary and appropriate, it is used in court proceedings. Although the physician or institution owns the original record, lawyers and courts are able to gain access to it. Therefore it is important to chart in a very detailed manner to protect those involved in patient care.
Patient health records also are used for teaching. Students in the health care professions learn more quickly and easily if examples of good charting are shared. Individuals also learn from their mistakes and the mistakes of others. It is important for students to remember that the patient’s information is to be held confidential.
Patient records that involve research and data collection have many uses in the health field. For example, the government periodically publishes data on certain diseases and the effectiveness of new treatments. In addition, the pressure to contain or limit health care costs has made data regarding the usual length of hospitalization and the cost of treatment for specific illnesses or surgeries important for governmental and other health insurance providers.
Electronic Health Record
In many health care settings, the EHR facilitates delivery of patient care and supports the data analysis necessary for coordinating patient care. EHRs contain information that is identical to that found in traditional records but eliminate repetitive entries and allow more freedom of access to the database (Fig. 3.1). In general, EHRs increase efficiency, consistency, and accuracy and decrease costs. Legibility is a further benefit of these systems.
The scope of the use of EHR for documentation in health care agencies varies depending on the agency. In addition to documentation of nursing care and interventions, most health care agencies have incorporated information systems for management of admissions, billing, and the communication of orders for diet, pharmacy, and diagnostic tests. A benefit of the EHR is the ability for all health care providers to view a patient’s records, encouraging increased continuity of care. In addition, agency-wide computer information systems are more efficient because information entered in the system can be transferred automatically to other areas. In regard to nursing documentation, systems often include options for generating individualized care plans, automated Kardex forms, acuity levels, and medication administration records (MARs). Although the terms EMR and EHR often are used interchangeably, a key difference between the EHR and the EMR is that the EHR allows the exchange of patient data not only within a facility but also from one facility to another. The EMR typically is set up to exchange patient data within a facility (Office of the National Coordinator for Health Information Technology, 2011).

EHR systems vary in the way they are accessed, depending on the facility. Some systems permit computer input only at the nurses’ station; some facilities have bedside systems, also referred to as point-of-care (POC) systems; and others use handheld systems that look similar to a cell phone. POC systems are sometimes housed on wheeled carts referred to as computers on wheels, or COWs. Nurses should be sure that patients and their family members are aware that the handheld systems are an EHR device in order to prevent the patient or family member from perceiving the staff to be on their personal cell phones during their shift. Charting at the bedside saves time and allows current information to be immediately available to all who need it. Some systems automatically retrieve and record information from electronic devices (e.g., vital signs) and simultaneously enter the data in all relevant locations in the record, which cuts down on duplication of effort. In addition, some systems prompt for certain data to be entered, which results in more accurate and complete record keeping.
Electronic charting procedures vary by agency. Data often are recorded in flow-sheet format for easy storage and retrieval. Some agencies incorporate the use of free-text narratives in addition to standardized phrases to allow specific and individualized documentation. The standard phrases indicate information such as
patient health problems, interventions, and outcomes classification systems. Assessment data, for instance, are entered by selecting from a list of preformulated choices, which means that the accuracy and pertinence of the data entered depend on the nurse’s familiarity with the language the system uses to name the patient problems, the lists of data for assessment, and anything else that is entered by picking from a list.
Naming conventions, or nomenclature (a classified system of technical or scientific names and terminology), must be considered when choosing computer-based documentation. The field of medical or nursing informatics (the study of information processing) is evolving constantly, which requires that software programs be updated on a regular basis to stay current with changes in terminology. In addition, considerable time must be invested in training personnel in charting procedures and the terminology the system uses and in conducting ongoing refresher training. Newly hired personnel need to learn a new system even if they already have had considerable experience in the field.
In addition to the EHR, the personal health record (PHR) is an extension of the EHR that allows patients to input their information into an electronic database. One benefit of a PHR system is for those patients who see health care providers who are not part of the same organization and EHR system. In this case the patient inputs information from these providers into one system so all health information is stored in one place. Points of contention for the PHR are how the information is going to be stored, and the PHR must be updated by the patient themselves manually and in a timely manner to be kept current (Mayo Clinic Staff, 2020).
Patient portals (an Online system through a healthcare facility that provides a patient with access to their own health information, correspondence with providers, logging of appointments, etc.) are another method of tracking health information. Most health care systems have patient portals in which patients have electronic access to their health information. Patient portals contain information such as lab, radiology, and other test results as well as the patient’s current medication lists. In addition, most patient portals allow patients to send messages to their health care provider. The patient portal differs from a PHR in that the patient cannot add their own health information to a patient portal. It should be noted that lab and diagnostic results will not be visible to the patient until their provider has viewed and released the information for the patient to see. This usually occurs in approximately 24 to 72 hours after results are available.
ISBAR
ISBAR (identification, situation, background, assessment, and recommendation) is a method of communication among health care workers and a part of documentation of communication that has occurred among health care staff. ISBAR is considered a safety measure in preventing errors from poor communication during interactions between health care personnel, the communication between nurses that occurs from one shift to the next, or when a nurse phones a health care provider with information about a patient. SBAR is recognized by The Joint Commission as one method of meeting National Patient Safety Goals (TJC, 2017; TJC, 2020). When ISBAR occurs between a nurse and a health care provider over the telephone and an order is received from the health care provider, a facility often mandates using an additional “R” in the communication exchange. The additional “R” (ISBARR) represents “read back.” This occurs when the nurse reads back the order to the health care provider to ensure what the nurse heard was accurate. See Box 3.1 for an example of the use of ISBARR.
Basic Guidelines For Documentation
The quality and accuracy of the nursing notes are extremely important. They have a decisive impact on the success or failure of communication. Sometimes the nursing notes clearly and concisely convey the intended message; sometimes, in contrast, they cause confusion and errors in communication and patient care. Correct choice of words and spelling; grammar and punctuation; and good penmanship and other writing skills (with non–computer-based systems) are critical. The LPN/LVN must ensure the information recorded in the chart is clear, concise, complete, and accurate.
The registered nurse (RN) has primary responsibility for each patient’s initial admission nursing history, physical assessment, and development of the care plan based on the patient health care problem identified. Contributions by all team members during this initial process as well as during later updating sessions are important.
The forms used to provide documentation of patient care vary based on each health care institution’s policy. Each facility uses a combination of graphics, care flow sheets, and narrative or SOAPE notes (see description
in later material) to document observations, care, and responses. The LPN/LVN should be sure that nursing notes correlate with the medical orders, Kardex information, and nursing care plan.
Charting Rules
See Box 3.2 for generally accepted documentation rules that provide consistency in documentation between health care providers and facilities. These rules also meet the standards expected by the individuals and the agencies that use the charts. Some of the rules apply to handwritten documentation. With a computerized documentation system, as is used with an EHR or EMR, the LPN/LVN should follow the guidelines for that particular system.
Legal Basis of Documentation
Accurate documentation is one of the best defenses in the event of legal claims associated with nursing care (see Chapter 2). To limit nursing liability, the nursing documentation must indicate clearly that individualized, goal-directed nursing care was provided to a patient based on the nursing assessment. The record has to describe exactly what happened to a patient. This is best achieved when the chart is updated immediately after providing care. Although nursing care may have been excellent, if the care was not documented, a court of law will consider that care was not provided. It is the nurse’s responsibility to indicate all assessments, interventions, patient responses, instructions, and referrals in the medical record.
Inappropriate documentation may lead to nursing malpractice. Some examples of inappropriate documentation include not charting the correct time that events occurred or that an event occurred at all, failing to record verbal orders, charting nursing care in advance, and documenting incorrect data. Table 3.2 lists some legal guidelines for documentation to be kept in mind. Again, some of the rules apply to handwritten documentation. With a computerized documentation system, follow the guidelines for that particular system.
Common Medical Abbreviations and Terminology
Use standard medical abbreviations and terminology for effective documentation. Avoid using abbreviations or terms that are not standard or in question. Use of the complete word is always better if unsure of the proper abbreviation. Many abbreviations that once were accepted are now found on “abbreviations to avoid” lists because of the probability of error if these terms are used. Most facilities have a published list of generally accepted medical abbreviations and the terms approved for use in charting. The use of abbreviations when charting can be confusing if a facility’s approved abbreviations are not followed. For example, is “BS” breath sounds, bowel sounds, or blood sugar? In addition, abbreviations used for communication outside of the health care facility, such as cell and smartphone texting abbreviations, must never be used in patient records. (See Appendix A for a list of commonly used abbreviations and The Joint Commission’s list of abbreviations to avoid.)
Methods of Recording
The documentation system selected by a health care facility optimally reflects the philosophy of the facility and the way nursing care is implemented.
Professionally executed charting is legal proof of care given and communicates the patient’s status and progress. The nursing process shapes the approach to providing care, and in turn, effective documentation of the care the nurse provides reflects the nursing process.
Traditional Chart
The traditional (block) chart is divided into sections or blocks. Emphasis is placed on specific sections (or sheets for noncomputerized charts) of information. Typical sections are the following: admission information, physician’s orders, progress notes, history and physical examination data, nurse’s admission information, care plan and nursing notes, graphics, and laboratory and x-ray examination reports. The order, the content, and the number of the sections vary among institutions. Nurses use flow sheets, graphics, and narrative charting (recording of patient care in descriptive form) (Fig. 3.2) to chart observations, care, and responses. Narrative charting is used for computerized and noncomputerized nurse’s notes. Narrative charting includes the data (subjective, objective, or both) about the basic patient need or problem, whether anyone has been contacted or consulted, care and
treatments provided (implementation), and the patient’s response to treatment (evaluation). Information obtained from the nurse’s assessment of the patient is clustered (see Chapter 5) and organized in a head-to-toe manner. This type of charting is documented in an abbreviated story form instead of in the outline style of the problem-oriented medical record format described in the following section.
Problem-Oriented Medical Record
The problem-oriented medical record (POMR) is organized according to the scientific problem-solving system or method. The principal sections are database, problem list, care plan, and progress notes. The accumulated data, or database, from the history, the physical examination, and the diagnostic tests are used to identify and prioritize the health problems on the master medical and other problem lists.

Nurse's notes on patient's conditions such as blood pressure, oxygen level, abdomen, edema. Nurse's notes: 0 8 0 0 Alert and oriented times 3, p t. is conversing with the nurse. Blood pressure 132 over 84. P 88 and regular, R 20 and unlabored, T 98.7. Reports 2 over 10 pain is tolerable to right anterior chest wall incision, states "P C A is controlling my pain well". The handgrip and arm strength are strong to the right, weak on the left. Push pull strength to lower extremities, strong to the right, and weak to the left. P E R R L. Oral mucosa pink, moist, and intact. Apical pulse auscultated for 1 minute at 88 bits per minute, strong and regular rhythm, lungs clear anterior and posterior in all fields. Oxygen saturated 95 percent with oxygen at 2 liter via N by C. Using incentive spirometer every hour with 10 breaths reaching a maximum of 1300 milliliter. Abdomen soft and non-distended with bowel sounds times 4 quads. No edema to extremities, skin turgor immediate return, capillary refill less than 3 seconds. Dressing to chest wall incision dry and intact, due to be changed today. Jackson-Pratt has 75 milliliter of serosanguinous fluid. Intravenous D 5 1 over 2 N S infusing into right forearm with no signs of infiltration, P C A.
This problem list (Fig. 3.3) of active, inactive, potential, and resolved problems serves as the index for chart documentation. Together, representatives of all the disciplines involved with the patient’s care develop a care plan with identified patient problems (Fig. 3.4). All health care providers—physicians, nurses, social workers, and therapists—chart on the same progress notes with forms such as narrative notes, flow sheets, and discharge summaries to document patient progress. This is done to facilitate and enhance communication between care providers.
SOAPIER (SOAPE documentation) (Box 3.3) is an acronym for seven different aspects of charting. For notes on specific patient problems, only the necessary parts needed for completeness are used.
- S Subjective information is what the patient states or feels; only the patient can provide this information.
- O Objective information is what the nurse can measure or factually describe.
- A Assessment refers to an analysis or potential diagnosis of the cause of the patient’s problem or need.
- P Plan is the general statement of the plan of care to be given or action to be taken.
- I Intervention or implementation is the specific care given or action taken.
- E Evaluation is an appraisal of the response and effectiveness of the plan.
- R Revision includes the changes that may be made to the original plan of care.
SOAPE is the briefer adaptation of the charting format for the POMR. In this more compact form, the care given or action taken (intervention [I]) is included in the notations under planning. The needed plan revisions (R) are noted in the evaluation section after the evaluation of the response to treatment is recorded. Fig. 3.5 shows the SOAPE charting forms in the progress notes that commonly are used in the patient’s medical record.
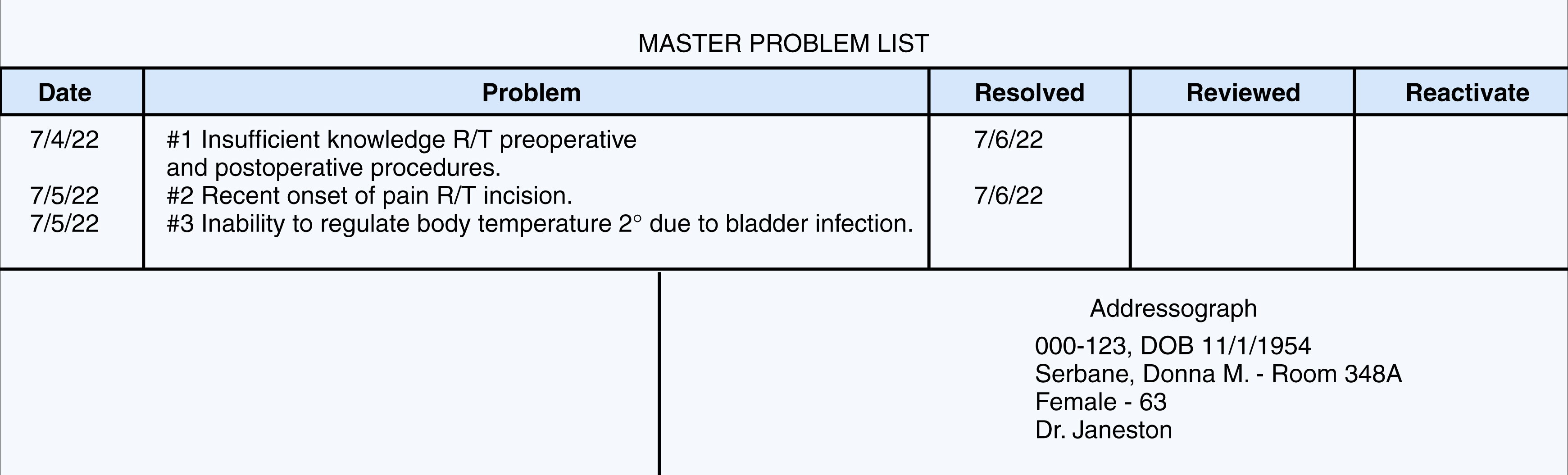
A table of a master problem list with four rows and five columns. Row 1, table heading master problem list. Row 2, column headers, column 1: Date, column 2: Problem, column 3, Resolved, column 4, Reviewed, and column 5, Reactivate. Row 3, column 1, 7 April 2022, column 2, number 1 insufficient knowledge R/T preoperative and postoperative procedures and column 3, 7 June 2022, column 1, 7 May 2022, column 2 number 2 recent onset of pain R/T incision, column 3, 7 June 2022. Column 1, 7 May 2022, column 2, number 3 inability to regulate body temperature 2 degrees due to bladder infection. Row 4, column 2, Addressograph 0 0 0 – 1 2 3, 11 January 1954, Serbane, Donna M – Room 348 A, Female – 63, nursing assistant Janeston.
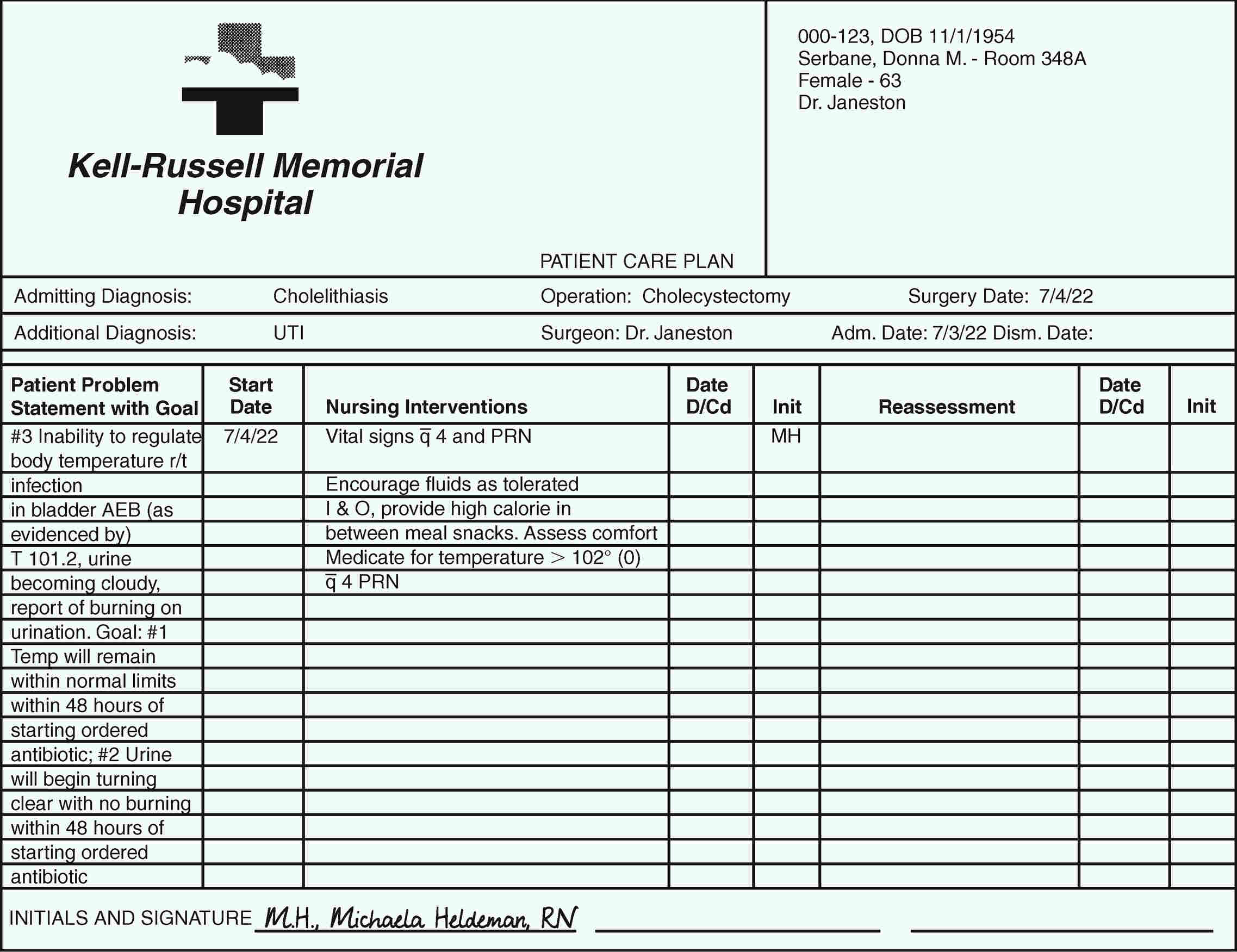
A patient care plan from Kell-Russell Memorial Hospital with hospital name and logo on the left and hospital address on the right. Row two includes admitting diagnosis, operation, and surgery date. Row three contains additional diagnosis, surgeon name, admission date, and dism date. Row four has column headings patient problem statement with a goal, start date, nursing interventions, date D by C d, Init, assessment, date D by C d, and Init. Eighteen rows include the components under the patient problem statement with a goal. Six rows have components under nursing interventions.
Focus Charting Format
In the focus charting format (Box 3.4), which was developed by nurses, a modified list of patient problems statements is used as an index for nursing documentation. Note the similarity of this list to the problem list used for the POMR. Focus charting can be used with traditional and POMR charting.
Focus charting uses the nursing process and the more positive concept of the patient’s needs rather than medical diagnoses and problems. The focus is sometimes a current patient concern or behavior and sometimes a significant change in patient status or behavior or a significant event in the patient’s therapy. A focus is not a medical diagnosis.
DARE is the acronym for four different aspects of charting using the focus format (see Box 3.4). Data (D) are subjective and objective and are equivalent to the assessment step of the nursing process. Action (A) is a combination of planning and implementation. Response (R) of the patient is the same as evaluation of effectiveness. Some facilities include education or patient teaching (E). The nurse does not need to use all the DARE steps each time notes are documented on a particular focus (Fig. 3.6).
Charting by Exception
Some facilities require the narrative notes for each shift to include a minimum of three entries and a flow sheet on which the nurse charts care given. Behind this policy is the legally derived charting concept that if the care was not documented, it is considered that care was not provided. All care must be charted, but this is a time-consuming, detailed, and defensive method.

A table of S O A P E charting progress notes with 13 rows includes two rows of column headers. The first row of column headers includes last name, first name, attending physician, room number, hospital number, and date of birth. The second row of column headers is the date, and a physician should sign notes. Row 3, column 1, 7 – 5 – 22. Row 3, column 2, 0 9 3 0 problem number 1 inability to regulate body temperature. Row 4, column 2, (patient problem: elevated body temperature). Row 5, column 2, S feels hot and flushed. Has burning on urination and heavy feeling over bladder area. C / o some discomfort in it. Flank. Row 6, column 2, O temperature 101 2 (0) elevated from 99 8 at 0 7 3 0 A M. Skin warm, flushed, dry. Urinating in 100 to 200 m L a m prime t s. Urine dark, Row 7, column 2, amber and cloudy. Foley Cath. D c prime d 7/4 at 2200. Lungs clear. Row 8, column 2, A possible bladder infection secondary to Foley catheter. Row 9, column 2, P Notify nursing assistant Janeston of temperature elevation, dysuria, and back discomfort. Assess for other signs of infection. To x-ray Row 10, column 2, for chest evaluation. Begin oral antibiotics after catheterization and urine specimen to the laboratory for C and S per nursing assistant Janeston Row 11, column 2, orders. Encourage increased oral fluids. Row 12, column 2, E urine to the laboratory, x-ray of chest ordered, chest and breath sounds clear. Nonproductive cough. Drank 500 m L of water this Row 13, column 2, shift. 2230 urine less concentrated.
To alleviate this problem, many facilities now have a policy called charting by exception (CBE). The nurse charts complete physical assessments, observations, vital signs, intravenous (IV) site and rate, and other pertinent data at the beginning of each shift. During the shift, the only notes the nurse makes are for additional treatments done or planned treatments withheld, changes in patient condition, and new concerns. Notations are made reflecting progress or revisions for all active patient problems on the nursing care plan.
With the CBE method of documentation, the nurse uses more detailed flow sheets, which enhances the focus on existing concerns. One format that may be used is the problem, intervention, and evaluation (PIE) format. It is a problem-solving approach, so PIE is similar to the SOAPE format; the main difference is that SOAPE charting originated from the medical model, whereas PIE charting arose from the nursing process. The SOAPE method of documentation also is oriented to the problems, interventions, and evaluations involved in nursing care. It was designed to provide an ongoing plan of nursing care with daily documentation. The care and assessment flow sheets consist of standardized assessment criteria and interventions. With this method, the nurse assesses all areas and compares the results with normal standards. The PIE format may be written in several ways, so the nurse should use the format dictated by the agency’s policy. At each shift, the nurse evaluates each patient problem at least once, and if the problem remains unresolved, the nurse ensures it is addressed continually until resolution is reached. After the patient problem is resolved, it no longer is covered by the daily documentation.
Sometimes the nurse uses a variation of the PIE format that includes assessment (A) data before the PIE (APIE). These assessment data include subjective (S) and objective (O) data. This assists the nurse to follow the steps of the nursing process (Fig. 3.7).
Record-Keeping Forms and Examples
Different facilities use a variety of forms to make medical record documentation easy and quick, yet comprehensive. Many forms help eliminate the need to duplicate data repeatedly in the nursing notes. The forms present several types of information in a format more accessible than compilation of all progress notes. Most of the forms are self-explanatory regarding the type of information required from the nurse (Fig. 3.8). It is unnecessary to chart a narrative note each time a medication is given (see Chapter 17) or a bath (see Chapter 9) or measurement of vital signs (see Chapter 12).
The nursing Kardex (or Rand) system is used by some facilities to consolidate patient orders and care needs in a centralized, concise way. The cumulative care file or Rand is kept at the nursing station for quick reference or is part of the EHR or EMR. Forms vary among institutions based on information required for care (Fig. 3.9).
The nursing care plan (which outlines the proposed nursing care based on the nursing assessment and the identified patient problems to provide continuity of care) is developed to meet the nursing care needs of a patient. Many facilities use standardized care plans for certain conditions or surgeries; however, individualization of the plan of care based on each patient’s own needs or circumstances is also important. This kind of plan, developed by nurses for nurses, is based on
nursing assessment and identified patient problems. Standardized nursing care plans include the pertinent patient problems, goals, and plans for care and specific actions for care implementation and evaluation.
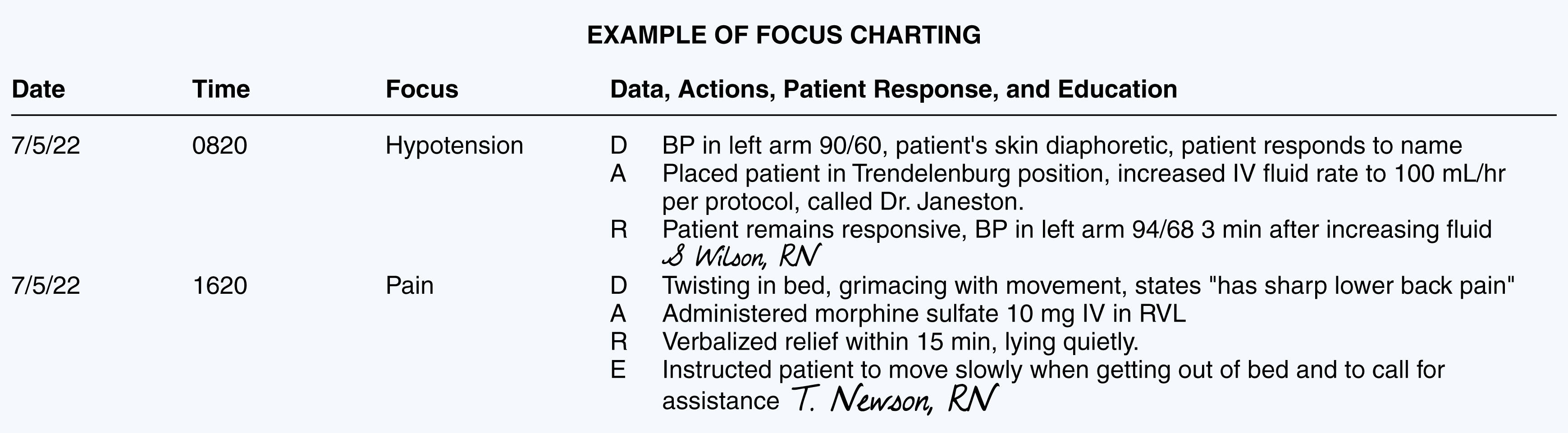
A table of focus charting nurse's notes with 3 rows and four columns. Row 1, columns headers are column 1, date, column 2, time, column 3, focus, and column 4 data, actions, patient response, and education. Row 2, column 1, 7 May 20222, column 2, 0 8 2 0, column 3, hypotension, column 4, D, B P in left arm 90 by 60, patient's skin diaphoretic, the patient responds to name, A Placed patient in Trendelenburg position, increased intravenous fluid rate to 100 milliliter per hour per protocol, called nursing assistant Janeston, and R Patient remains responsive, B P in left arm 94 by 68 3 minutes after increasing fluid, S Wilson, R N. Row 3, column 1, 7 May 2022, column 2, 1 6 2 0, column 3, pain, and column 4, D Twisting in bed, grimacing with movement, states "has sharp lower back pain' A Administered morphine sulfate 10 mg intravenous in R V L R Verbalized relief within 15 minutes, lying quietly. E Instructed the patient to move slowly when getting out of bed and to call for assistance. T Newson, R N.
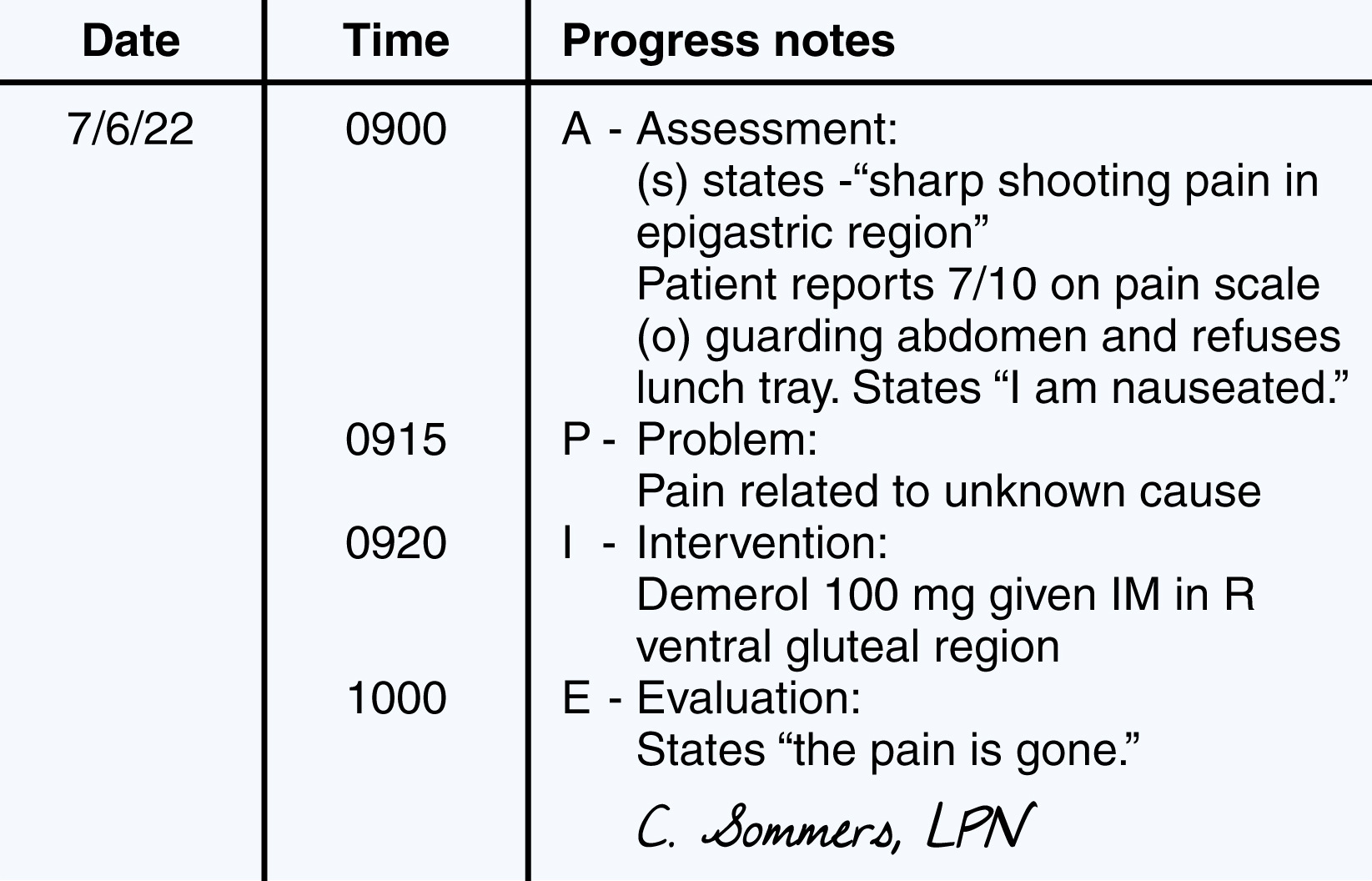
A table of assessment, problem, intervention, and evaluation with three columns and four rows. Row 1, column headers, column 1, date, column 2, time, column 3, progress notes. Row 2, column 1, 7 June 2022, column 2 0 9 0 0, column 3 A Assessment (s) states “sharp shooting pain in epigastric region ”, patient reports 7 over 10 on pain scale (0) guarding abdomen and refuses lunch tray. States, “I am nauseated.”. Row 3, column 2 0 9 1 5, P “ problem: pain related to an unknown cause. Row 4, column 2, 0 9 2 0,I ” intervention, Demerol 100 milligrams given I M in R ventral gluteal region. Row 5, column 2, 1000, column 3 E-evaluation: states “the pain is gone”. C. sommers, L P N.
Incident Reports
An incident report (form used to document any event not consistent with the routine operation of a health care unit or the routine care of a patient, Fig. 3.10) is sometimes necessary in response to an unplanned occurrence within a health care facility. For example, if a nurse neglects to give a medication or treatment or gives an incorrect dose of a drug, an incident report must be filed. Either of these events has the potential to cause injury. Incident reports also are filled out for any unusual event in a hospital (e.g., injuries to a patient, visitor, hospital personnel). Many staff members are reluctant to fill out these forms, but this information helps the facility risk manager and unit managers to track occurrences of incidents. One of the benefits of tracking particular incidents is to prevent future problems through education and other corrective measures.
When filling out an incident report, give only objective, observed information. Do not admit liability or give unnecessary details. Include in the incident report care given to the patient in response to the incident and the name of the health care provider notified. When charting the incident in the patient’s nursing notes, do not mention the incident report, because doing so makes it easier for an attorney to request that document for a court case (Table 3.3).
Twenty-Four–Hour Patient Care Records and Acuity Charting Forms
The nursing records may be consolidated into a system that accommodates a 24-hour period. A 24-hour record-keeping system helps eliminate unnecessary record-keeping forms. It is easier to obtain accurate assessment information and documentation of activities of daily living with 24-hour notations. In addition, 24-hour patient care records often use flow sheets and checklists to enhance efficiency further.
Twenty-four–hour patient care records provide the foundation for an acuity charting system. Acuity charting uses a score that rates each patient by severity of illness. With documentation and analysis of nursing interventions, an overall level of acuity for each patient is determined. For example, perhaps an acuity system rates patients from 1 to 5 (1 is high, 5 is low). A patient returning from surgery with multisystem problems is an acuity level 1. On the same continuum, another patient awaiting discharge after a successful recovery from surgery is an acuity level 5. One benefit is the ability to determine efficient staffing patterns according to the acuity levels of the patients on a particular nursing unit. The patient-to-staff ratios depend on a composite gathering of data in regard to the 24-hour interventions necessary for implementing care.
Discharge Summary Forms
Much emphasis is placed on preparing a patient for a timely discharge from a health care institution. Ideally, discharge planning begins at admission, and in some cases, even before admission, as is necessary with same-day surgery admissions and childbirth. Nurses continue discharge planning as the patient’s condition changes. Patients and family should be involved in the discharge planning process.
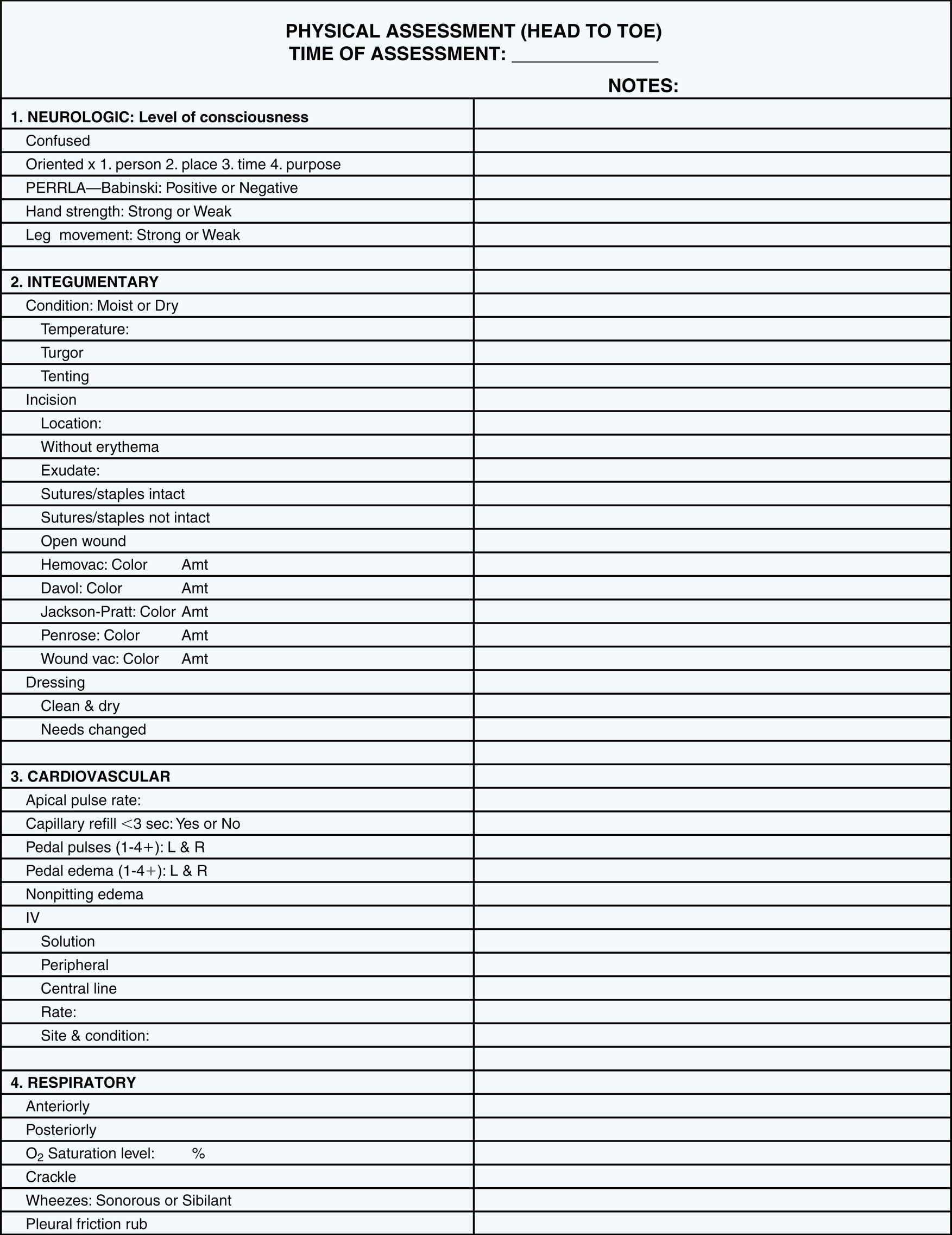
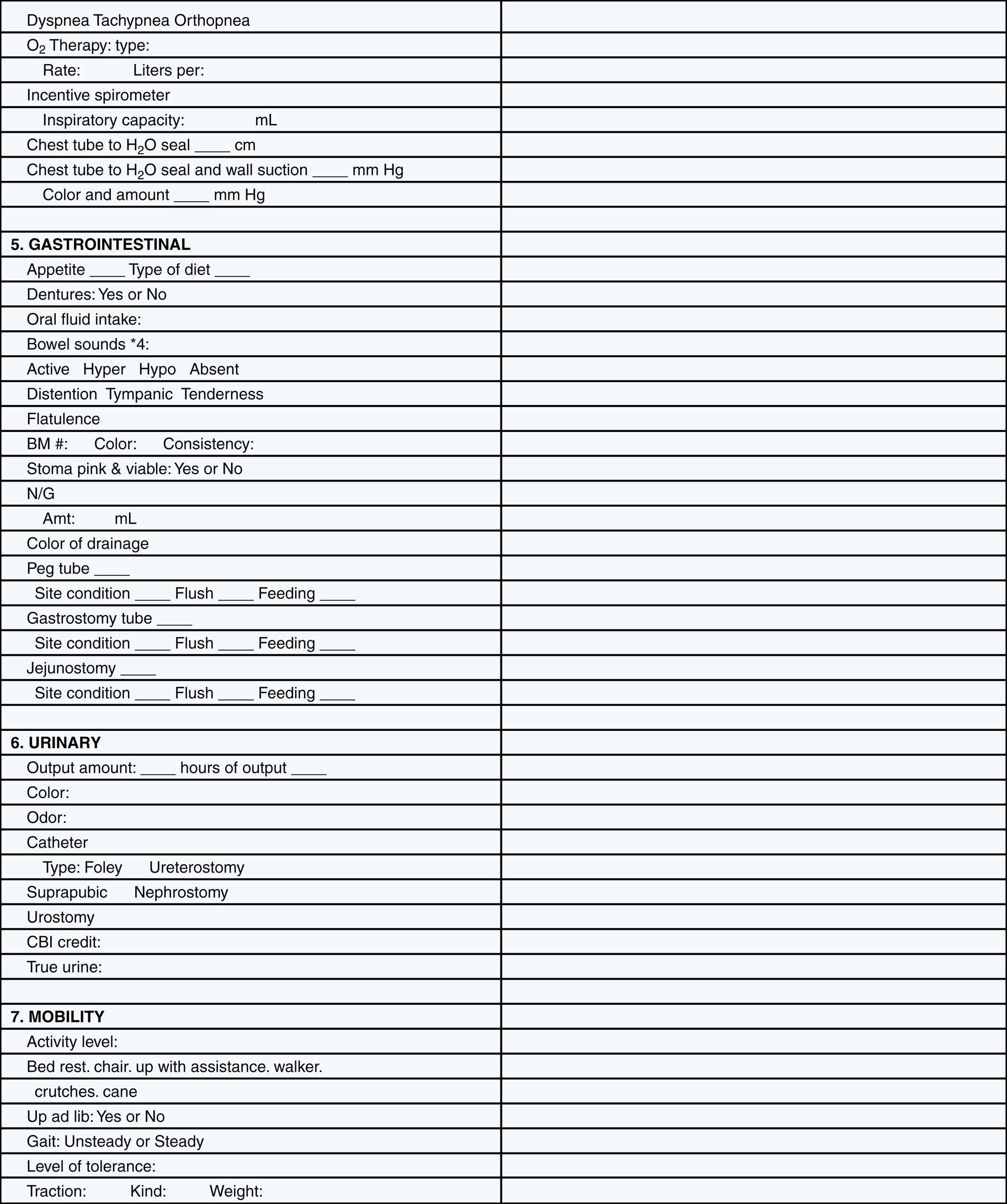
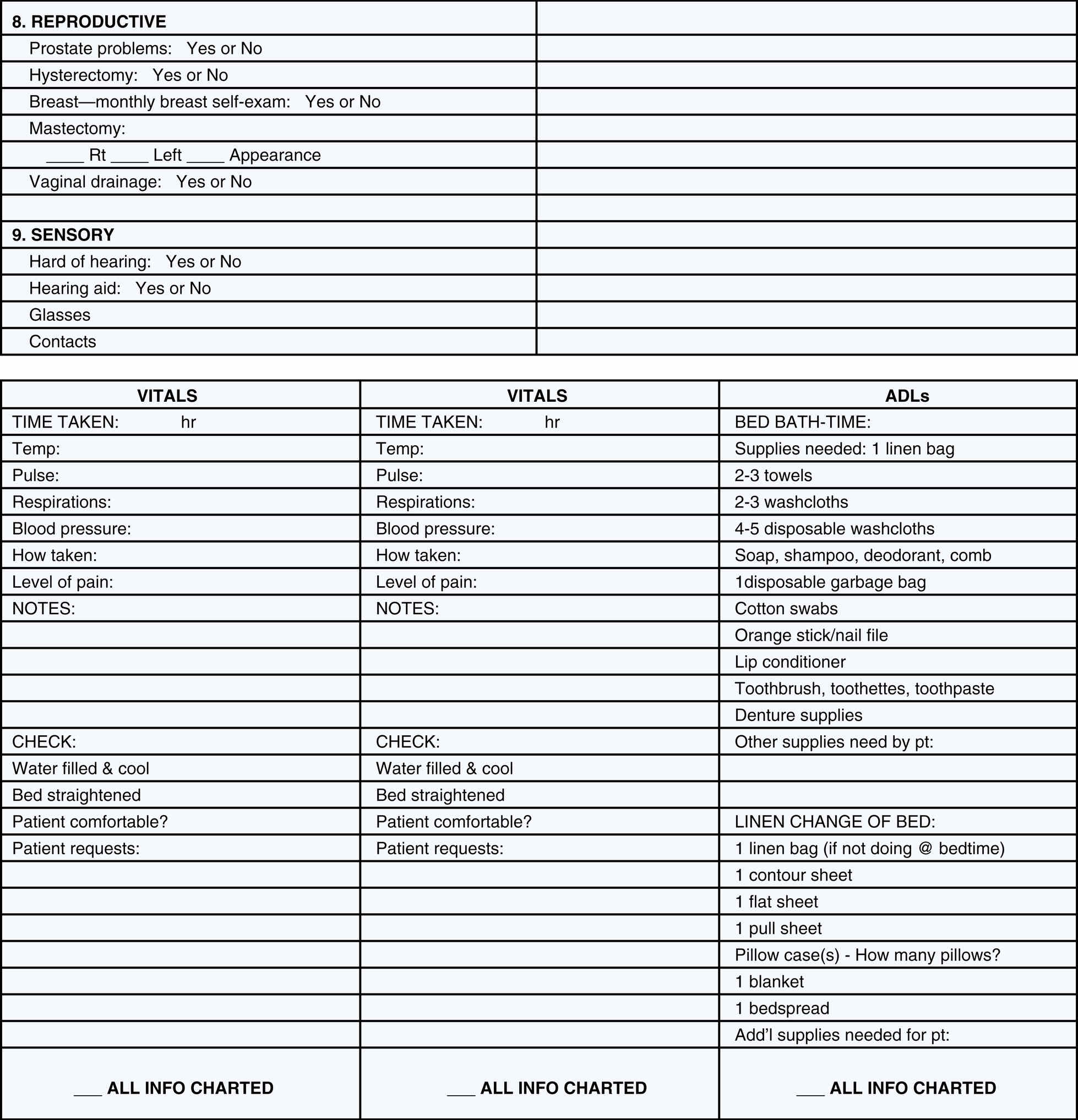
A nursing care record with a header, physical assessment (head to toe). Time of assessment, notes, patient details related to row headers 1. Neurologic, level of consciousness, 2. Integumentary, 3. Cardiovascular, and 4. Respiratory. Continuation of the nursing care record with patent details related to 5. Gastrointestinal, 6. Urinary and 7, mobility. Continuation of the nursing care record with patient details related to 8. reproductive, 9. Sensory and a table with vitals including time taken and check, A D L s including bed bath time and linen change of bed.
A discharge summary form provides important information that pertains to the patient’s continued health care after discharge. A discharge summary always should be provided to the patient or the family (or both) so that there is written documentation of instructions given to the patient and so that the patient can refer to those instructions after being discharged. Discharge summary forms (see Fig. 11.5) make the summary concise and instructive. Often the form includes a copy that is given to the patient, a family member, or a home health care nurse and a copy that is kept with the patient records. Home health care agencies or extended nursing care facilities also benefit from receiving information on these summary forms and use it to provide better continuity of care.
Documentation and Clinical (Critical) Pathways
Documentation tools that integrate the standards of care of multiple disciplines have been developed to meet the needs of managed care. Managed care is a
systematic approach to care that provides a framework for the coordination of medical and nursing interventions.
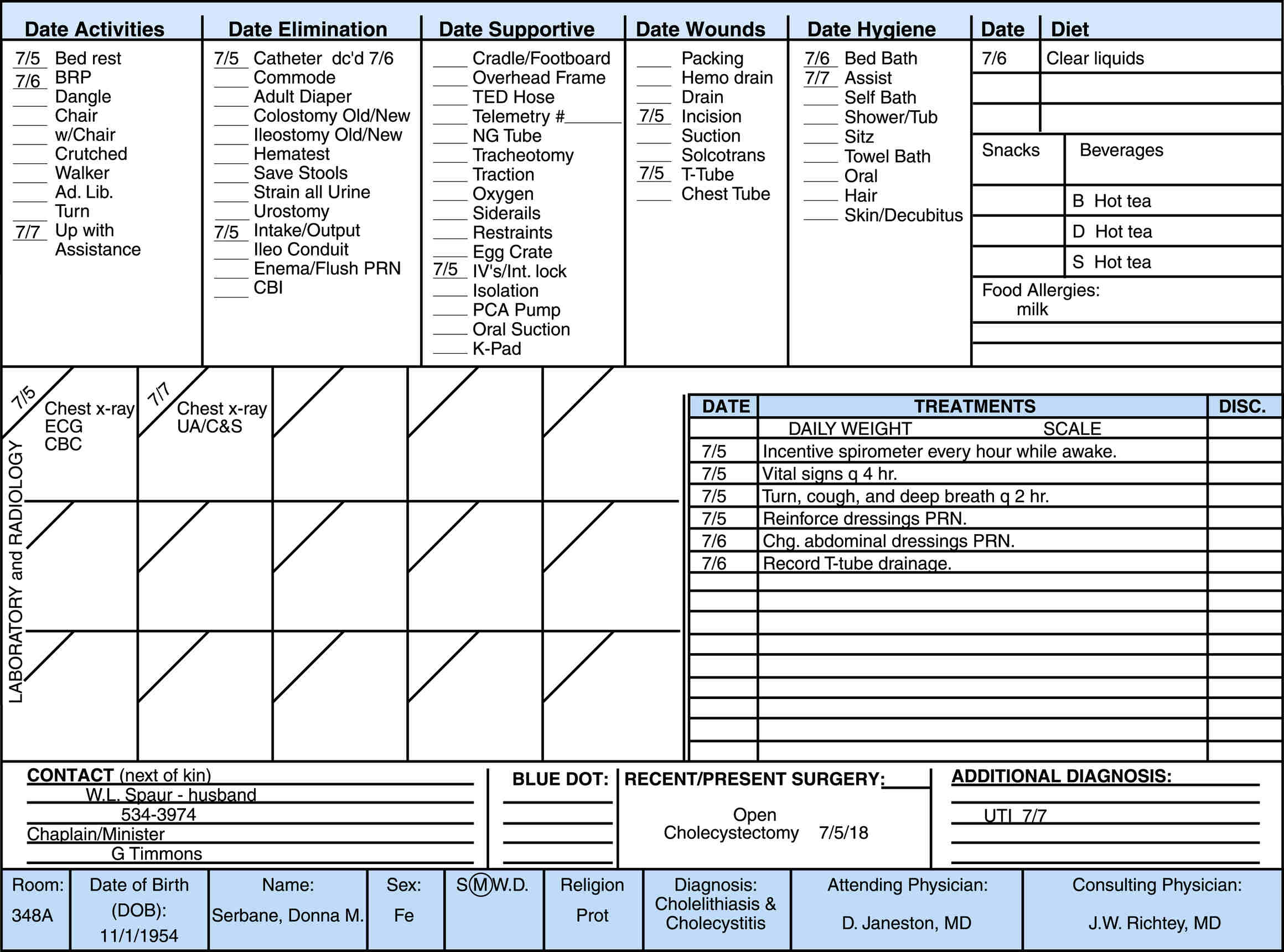
A nursing Kardex or Rand card with column headers date activities, date elimination, date supportive, date wounds, date hygiene, date, diet, laboratory, and radiology, chest X-ray, E C G, C B C, Chest X-ray U A by C, and S. A table with date, treatments, and D i s c and daily weight scale. Contact address, blue dot, recent/present surgery, additional diagnosis.
These documentation tools are called clinical (critical) pathways. Clinical (critical) pathways allow staff from all disciplines to develop standardized, integrated care plans for a projected length of stay for patients of a specific case type. The case types that have clinical (critical) pathways are usually those that occur in high volume and are predictable. A clinical (critical) pathway for a total hip repair may recommend on a day-to-day basis the level of activity, pain control therapy, advancement in diet, and educational topics necessary for a patient’s recovery.
The exact contents and format of these clinical (critical) pathways vary among institutions. The contents include a care plan, interventions specific for each day of hospitalization, and a documentation tool. The clinical (critical) pathway replaces other nursing forms such as the nursing care plan.
The LPN/LVN and other team members use the pathways to monitor a patient’s progress and as a documentation tool. CBE is frequently the method used with pathways. Staff members document only when anticipated interventions are not provided as projected.
Many agencies use military time, a 24-hour system that uses digit numbers to indicate morning, afternoon, and evening times regardless of which method of documentation is used (Fig. 3.11).
Home Health Care Documentation
The home health care industry continues to grow in our society for a number of reasons. Limitations in coverage within the acute care setting are a major cause for the growth, as is the desire patients have to be cared for in their home rather than in a health care facility.
Documentation in the home health care system has different implications than in other areas of nursing. The primary difference is the nature of the home setting, which dictates that a narrower scope of people (e.g., patient, family, direct health care provider) witness the majority of care. Home health care requires that the entire health care team work closely together. The documentation of care must be accurate and complete so that all members of the team are able to ascertain what care is rendered in the home. In addition,
the documentation provides the quality control and the justification for reimbursement from Medicare, Medicaid, or private insurance companies. Nurses have to document all their services for payment (e.g., direct skilled care, patient instructions, skilled observations, evaluation visits). The nurse is the pivotal person in the documentation of the delivery of home health care.

An incident report of Kell-Russell memorial hospital, with hospital name, instructions, patient name, age, sex, address, type of patient, inpatient, outpatient or emergency, visitor, employee, date and time of variance, the exact location of variance, description of variance, nature of the injury of the patient, equipment or supplies involved, I D and present location, the reason for variance, notification details to physician, time of notification, signatures of the patient, physician, and witness. The incident report is confidential, not part of the medical record.

A concentric circle shows a military time clock in 12 hours format and 24 hours format in the outer circle. In the inner circle, there is an analog clock showing the time of 10 O clock and 10 minutes.
Home health care documentation has several components that the nurse must consider. Medicare, Medicaid, and private insurance typically have similar requirements in regard to documentation. The patient’s eligibility for home care must be assessed thoroughly and documented. The nurse must document in detail any procedures, treatments, or medications administered and response to these interventions. Another important aspect of health care documentation is noting any patient education and demonstration of learning. Home health documentation also must reflect coordination of services by all members of the health care team and evidence of compliance with regulations (CMS, n.d.). Home health care is discussed in more detail in Chapter 37.
Long-Term Health Care Documentation
An ever-increasing number of older adults need care in long-term health care facilities. Because many individuals live in this setting for the rest of their lives, they are referred to as residents rather than as patients. The acuity of residents’ conditions, and the number of their disabilities, continues to escalate commensurate with their age. Nursing personnel often face challenges much different from those in the acute care setting. These differences establish a significantly different basis for nursing documentation.
Outside agencies are instrumental in determining the standards and policies for documentation in long-term health care. For example, the Omnibus Budget Reconciliation Act (OBRA) of 1987 instituted significant Medicare and Medicaid requirements for long-term care provision and documentation. Among the requirements of OBRA are minimum data sets (MDS) and regulated standards for resident assessments, individualized care plans, and qualifications for health care providers (RNs and LPN/LVNs). In addition, the department of health in each state governs the frequency of the required nursing entries in the records of residents in long-term care facilities. Long-term care documentation supports a multidisciplinary approach in the assessment (referred to as the MDS) and the planning process (referred to as resident assessment protocols) of the residents. Often long-term care agencies also have skilled care units where patients or residents stay when, in response to mandates for shorter hospital stays, they need increased levels of care and are not able to return directly to their usual residence after a hospital admission. Multidisciplinary communication among such health care providers as nurses, unlicensed assistive personnel (UAP), social workers, physical therapists, and dietitians is essential in the regulated documentation process. The fiscal management of long-term care hinges on the justification of nursing care as demonstrated in sound documentation of the services rendered. Additional documentation information in long-term care is discussed in Chapter 38.
Special Issues in Documentation
Record Ownership and Access
The original health care record or chart is the property of the institution or the health care provider. On admission to the health care facility, the patient usually is asked to sign a form granting permission for appropriate people, such as insurance carriers, to have access to the record as necessary. Patients may not have immediate access to their full records, depending on the agency policy. Lawyers, with the patient’s written permission, are given access to the patient’s medical records. Courts have the legal right to obtain records for review and use in the case of a lawsuit.
Patients have gained access rights to their records in most states, but only if they follow the established policy of each facility. A written request for chart access may be required, and institutions can specify a period that allows the physician and the facility to review the record and give a response. Sometimes the institution requires that a staff member or physician be present while the individual looks through the chart to answer questions and to protect the integrity of the record. Patients also may ask for a copy of their medical records. The use of patient portals has helped immensely
in giving access to much of a patient’s record. While it doesn’t allow viewing of the primary provider’s anecdotal notes or nurse’s notes, as previously mentioned the patient portal does allow for viewing of items such as lab and diagnostic test results.
Confidentiality
Health care personnel are required to respect the confidentiality of the patient’s record. The Patient Care Partnership (patients, when admitted to a facility, receive this information regarding their rights and responsibilities) and the law guarantee that medical information is kept private, unless the information is needed in providing care or the patient gives permission for others to see it (American Hospital Association, n.d.). The Health Insurance Portability and Accountability Act (HIPAA), an act of Congress passed in 1996, affords certain protections to persons covered by health care plans, including continuity of coverage when changing jobs, standards for electronic health care transactions, and primary safeguards for the privacy of individually identifiable patient information (see Chapter 2).
Ethical codes of practice also emphasize the LPN/LVN’s obligation to preserve patient privacy by holding patient information in highest confidentiality. Health care personnel may not read a record, or allow others to do so, without a clinical reason, and personnel must hold the information regarding the patient in confidence. Furthermore, trust is necessary for good nurse-patient relationships, and breaking confidences is a way to lose patient trust. Breaking laws concerning patient confidentiality often leads to job termination, lawsuits, or both (see Chapter 2).
Student nurses are reminded that no information is to leave the clinical site and that any documents that have patient identifying information must be closely guarded at all times within the facility. Any printouts or notes with patient identifiers that have been used by the student must be shredded before leaving the clinical agency. In addition, the student must be vigilant in keeping documents in a safe place when in the clinical agency; documents with patient identifiers never should be left anywhere unattended, such as on bedside tables in the patient’s room, at the nurses’ station, or on conference room tables. Any information that the student does need for course assignment purposes regarding assigned patients should have no identification information on the documents. Identification information is not limited to the patient’s name, age, or identification number. Any unique information about the patient, such as medical diagnosis or past medical history, is considered a patient identifier.
Electronic Documentation Safeguards
Charting with an electronic system is an efficient method of documentation, but the security of the system must be considered when considering legal and ethical issues. Confidentiality, access to information, and inappropriate alterations in patient records are areas of concern. Networks typically are protected by a firewall from illegitimate outside access. Some computer systems permit online access from remote sites, but this further complicates the task of keeping the system secure. To protect the patient’s rights and keep the patient’s record confidential, anyone who enters data into or consults a computerized record has to log on to the system with a secure password. The institution may require the user to change passwords at certain time frames, such as every 90 days, to maintain security. Because the password is assigned only to individual health care personnel, any data entered are credited automatically to whoever signed in; thus personnel must never share the password with anyone. Be sure to log off the system before leaving the terminal to ensure that information about a patient does not remain on the monitor display for others to view.
It is also necessary to protect computer-generated printouts and prevent the indiscriminate duplication or distribution of information about patients. Most facilities that use computer charting incorporate a system for logging and tracking computer printouts (Box 3.5) and have protocols for shredding the copies that are made.
Use Of Fax Machines
Fax machines send written documents over telephone lines to transmit data quickly between health care facilities, such as health care provider’s offices, hospitals, long-term care facilities, and laboratories. HIPAA rules allow for a patient’s medical records and information to be faxed. Information can be transmitted from health care providers to health care facilities and vice versa. For example, laboratory results can be sent via fax, email, or phone to a health care provider, or a health care provider may fax medical information to another professional for consultation. Various safeguards must be in place to maintain patient confidentiality and privacy. Some facilities require that the sender verify the fax number with the recipient. Similarly, a facility may preprogram frequently faxed numbers into the system to prevent incorrect dialing of the intended number. Although fax machines are still used, they are being used less by facilities that have an EHR system in place.