Other Renal Artery Diseases
Renal Arterial Aneurysms
A renal arterial aneurysm is a localized dilatation of the main renal artery or its branches or both caused by weakening of the elastic tissue and media of the arterial wall. The estimated incidence of such lesions in the general population ranges from 0.09% to 0.3%. Renal arterial aneurysms may be clinically significant because of a causative relation to hypertension, associated local symptoms, or the risk of catastrophic rupture in certain situations (Novick, 1982). According to the classification of Poutasse (1975), there are four basic types of renal artery aneurysms: saccular, fusiform, dissecting, and intrarenal (Fig. 39–17).

Figure 39–17 Selective renal arteriograms demonstrate the four types of renal artery aneurysms. A, Saccular aneurysm located at the bifurcation of the main renal artery. B, Fusiform aneurysm distal to a stenotic lesion of the main renal artery. C, Dissecting aneurysm involving a renal artery branch. D, Intrarenal aneurysm.
Saccular aneurysms are the most common type and constitute about 75% of renal artery aneurysms. They generally occur at the bifurcation of the renal artery, perhaps owing to an inherent weakness in the wall of the artery at this point. Because of this location, branch arterial involvement is common. The incidence of bilateral or multiple aneurysms or both is approximately 25%. These aneurysms may become involved with secondary atherosclerotic degeneration or intramural calcification or both. Incompletely calcified aneurysms may become soft, thin, and ulcerated between zones of calcification, thus predisposing to rupture. In addition to rupturing spontaneously, saccular aneurysms may erode into the renal vein or into the renal pelvis. Mural thrombus formation may also occur within saccular aneurysms, occasionally leading to peripheral renal embolization.
Fusiform aneurysms occur as a uniform dilatation of an entire segment of the renal artery to as much as three to four times its normal diameter. These aneurysms range in length from 1 to 3 cm and are generally not calcified. They are typically found in young hypertensive patients with stenosing fibrous renal arterial disease. The fusiform aneurysm is actually a poststenotic dilatation and can involve either the main renal artery or its branches. The major complication of this lesion is thrombosis of the involved arterial segment from progressive proximal stenosing vascular disease.
A dissecting aneurysm results from a tear in the internal elastic membrane of the renal artery, and as blood flows through the opening, the intima is separated from the remainder of the arterial wall. In some patients, the dissection may reenter the lumen distally to preserve renal function. In other cases, arterial thrombosis with renal infarction or rupture with hemorrhage may occur. Dissecting aneurysms are most often complications of renal arterial involvement with atherosclerosis, intimal fibroplasia, or perimedial fibroplasia. Less commonly, such an aneurysm may occur as an extension of a dissecting aortic aneurysm.
Intrarenal arterial aneurysms are of mixed origin and may be congenital, post-traumatic, iatrogenic, neoplastic, or associated with polyarteritis nodosa. They are usually saccular or fusiform and may or may not be calcified. Intrarenal aneurysms constitute approximately 17% of all renal arterial aneurysms, and they do have the propensity for rupture. Intrarenal aneurysms that occur after blunt trauma or closed renal biopsy occasionally resolve spontaneously with expectant management.
In general, the diagnosis of renal arterial aneurysm should be considered when ringlike calcification in or near the renal hilum is found on a plain abdominal radiograph. These calcifications occur in about 50% of cases. The majority of renal arterial aneurysms are small and asymptomatic. The most common clinical manifestations are hypertension, subcostal or flank pain, hematuria, an abdominal bruit, and, rarely, a palpable pulsating mass. RVH is reported to occur in 15% to 75% of patients and may be due to turbulent flow within an aneurysm, associated arterial stenosis, dissection, arteriovenous fistula formation, thromboembolism, or compression of adjacent arterial branches by a large aneurysm. Complications of renal arterial aneurysms include peripheral dissection, arterial thrombosis with renal infarction, emboli arising from mural thrombus within an aneurysm, obstructive uropathy, erosion into a vein with formation of an arteriovenous fistula, and spontaneous rupture with hemorrhage. Factors that appear to predispose to aneurysmal rupture include absent or incomplete calcification, aneurysmal size greater than 2 cm in diameter, coexisting hypertension, and pregnancy.
A small (2-cm) well-calcified renal arterial aneurysm in an asymptomatic normotensive patient does not require operative intervention. These aneurysms can be followed with serial plain abdominal radiographs to detect any change in size. Surgical removal is indicated for renal arterial aneurysms, regardless of size, in (1) aneurysm causing renal ischemia and hypertension, (2) dissecting aneurysm, (3) aneurysm associated with local symptoms such as flank pain or hematuria, (4) aneurysm occurring in a woman of child-bearing age who is likely to conceive, (5) aneurysm occurring with functionally significant renal arterial stenosis, (6) aneurysm with radiographic evidence of expansion on serial radiographs, or (7) aneurysm containing a thrombus detectable on angiography with evidence of distal embolization.
When none of these criteria are present, small (2-cm) asymptomatic noncalcified or incompletely calcified aneurysms can be managed nonoperatively. Such patients should be followed periodically with serial CT or MRI studies to document the size of the aneurysm. It is not possible to rigidly define indications for operative intervention in asymptomatic patients with aneurysms greater than 2 cm in diameter and with none of the previous criteria. The available data would seem to support surgical excision, if these aneurysms are not calcified throughout or are intrarenal because of the increased tendency to rupture in these settings.
In the largest series of renal artery surgery reported in the recent literature (Henke et al, 2001), a total of 121 patients underwent surgical repair. Eight unplanned nephrectomies were necessary resulting in the need for permanent dialysis in one patient, no perioperative mortality was encountered, and all but two reconstructions remained patent at follow-up.
In a retrospective review of surgical repair of renal artery aneurysms in 94 patients, Pfeiffer and colleagues (2003) encountered one postoperative mortality (in an emergency repair secondary to aneurysm rupture), overall morbidity of 17%, and a primary success rate of 97%.
English and colleagues (2004) reported their results of surgical repair of 72 renal artery aneurysms of varying etiology over a 16-year period. Only one aneurysm was deemed not reconstructable, and nephrectomy was performed. One operative mortality was encountered, and 12% of patients had significant perioperative morbidity, with 96% of repairs maintaining patency at 48 months.
A significant body of literature (almost all case reports) has accumulated over the last few years reporting successful endovascular management of renal artery aneurysms as well as dissection of the renal artery. In the case of renal artery aneurysms, two methods of endovascular treatment are reported. The first involves embolization of the aneurysm (usually with coils) to occlude it without disrupting the renal blood flow (Halloul et al, 2000; Karkos et al, 2000; Mounayer et al, 2000; Tshomba et al, 2002; Lupattelli et al, 2003). The second method involves placing an arterial stent in the renal artery or the branch where the aneurysm originates, thereby maintaining flow through the stent and effectively excluding the aneurysm (Tan et al, 2001; Bruce and Kuan, 2002; Pershad and Heuser, 2004). Stenting the renal artery across an aneurysm has also been described as a successful and rapid method of dealing with ruptured renal artery aneurysm (Schneidereit et al, 2003). Dissection of the renal artery also can be managed endovascularly by placing a renal artery stent through the area of dissection to keep the lumen patent and keep the dissected intima immobilized against the outer layers of the artery (Bilge et al, 2003).
Renal Arteriovenous Fistula
Renal arteriovenous fistulas are relatively uncommon lesions that are generally discovered during the course of angiographic evaluation for suspected renal or renovascular disease. There are three categories of renal arteriovenous fistulas: congenital, idiopathic, and acquired (Tynes et al, 1970; Novick, 1982).
Congenital fistulas have a cirsoid or angiomatous configuration with multiple communications between arteries and veins. They are usually supplied by a renal arterial branch of normal caliber. The angiographic appearance is one of multiple, small, interconnecting arterial and venous channels with impaired distal renal parenchymal vascularity and early filling of the renal vein. They constitute 22% to 25% of all renal arteriovenous fistulas, occur equally in both sexes, and generally do not become manifest until adult life.
Idiopathic fistulas are single, are not cirsoid, and have no apparent cause. They constitute only 3% to 5% of all renal arteriovenous fistulas. These lesions are called idiopathic because their angiographic appearance is similar to that of acquired arteriovenous fistulas, but their origin is unclear.
Acquired fistulas are the most common type, accounting for 70% to 75% of all renal arteriovenous fistulas. On angiography, they appear as solitary communications between an artery and a vein. By far the most common cause is iatrogenic trauma resulting from needle biopsy of the kidney (Fig. 39–18). Other causes include renal carcinoma, blunt or penetrating renal trauma, inflammation, and renal surgery such as nephrectomy, partial nephrectomy, or nephrolithotomy.
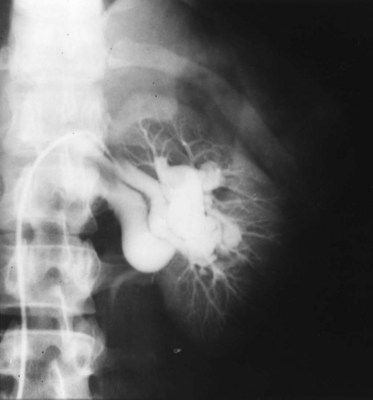
Figure 39–18 Left renal arteriogram shows renal arteriovenous fistula with early filling of the renal vein. This patient had previously undergone needle biopsy of the left kidney.
The clinical manifestations of a renal arteriovenous fistula depend on the size of the fistula. Approximately 75% of patients have an abdominal bruit, which is usually loud, high pitched, and continuous with systolic accentuation. Congestive heart failure, cardiomegaly, and diastolic hypertension are observed in 50% of patients. Hematuria is present in about one third of cases, tachycardia is occasionally found, and a palpable flank mass from spontaneous rupture is rarely encountered.
The management of a patient with a renal arteriovenous fistula depends on the cause of the fistula and the associated clinical manifestations. For patients with renal carcinoma, immediate nephrectomy is obviously indicated. Approximately 70% of fistulas occurring after needle biopsy of the kidney close spontaneously within 18 months. A smaller number of fistulas diagnosed immediately after renal trauma have also resolved spontaneously. Therefore in the absence of significant related symptoms, expectant management is appropriate initially in these cases.
Treatment of renal arteriovenous fistulas is indicated for patients who have hypertension, heart failure, severe hematuria, serial angiographic evidence of an expanding lesion, rupture, or progressive renal failure. When specific therapy of these lesions is indicated, renal-sparing procedures should be employed whenever possible.
Transcatheter angiographic occlusion is a nonsurgical therapeutic alternative that has been employed primarily in treating patients with postbiopsy fistulas, in which the arteriovenous connecting vessels are usually small. More recently, transcatheter occlusion of congenital or idiopathic fistulas with a stainless steel coil has also been performed.
Various operations have been employed in the surgical treatment of renal arteriovenous fistulas. Most congenital or cirsoid fistulas have been managed with total or partial nephrectomy, because of the difficulty of completely excising the many small communicating vessels. In patients with idiopathic or acquired fistulas, a single communication between the artery and the vein is characteristically present, and surgical obliteration of the fistula with preservation of the involved kidney is more often possible.
Renal Artery Thrombosis or Embolism
Thromboembolic disorders of the renal artery can present as fulminant clinical syndromes that threaten life or may be entirely asymptomatic and detected only at postmortem examination (Hoxie and Coggins, 1940; Schoenbaum et al, 1971). The various causes of acute renal artery thrombosis or embolism are listed in Table 39–14. The term paradoxical embolism refers to a clot originating in the venous circulation that gains entrance to the systemic arterial circulation through an intracardiac septal defect.
Table 39–14 Causes of Renal Arterial Thrombosis and Embolism
| Renal Artery Thrombosis |
| Renal Artery Embolism |
Renal arterial thrombosis commonly involves the proximal or middle third of the main renal artery, whereas renal arterial embolization generally involves peripheral arterial branches. Acute arterial occlusion is more common on the left side because of the more acute angle between the left renal artery and the aorta. Post-traumatic renal arterial occlusion is also more common on the left side, presumably because of the acute angulation of the shorter left renal artery at its aortic junction, which predisposes to intimal disruption with deceleration of the mobile kidney.
The clinical symptomatology in these disorders is extremely varied. Bilateral acute renal arterial occlusion presents with rapidly progressing oliguric renal failure, whereas chronic occlusion of a single renal artery may be unnoticed because of the development of collateral circulation. The most common symptoms, when present, are dull, aching abdominal or flank pain often associated with nausea, vomiting, and fever. Other findings include hypertension, albuminuria, microscopic hematuria, leukocytosis, and elevation of serum lactate dehydrogenase levels.
Patients with unilateral renal arterial embolic occlusion generally have serious underlying extrarenal disease and are best managed nonoperatively with systemic anticoagulation or by percutaneous transcatheter thromboembolectomy (Millan et al, 1978; Hamilton, 1996). Patients with unilateral traumatic renal arterial thrombosis also often have severe associated injuries, and the results of vascular reconstruction are generally unsatisfactory unless this is undertaken within several hours of the time of injury. Surgical treatment in these cases is generally ill advised when a normal contralateral kidney is present. Percutaneous intra-arterial infusion of a fibrinolytic agent, such as streptokinase, now offers a nonoperative approach to the management of acute renal arterial thrombosis (Hamilton, 1996).
Renovascular reconstruction is generally indicated when renal artery thrombosis or embolism occurs bilaterally or in a solitary kidney. Alternatively, if angiographic and isotopic studies in such cases demonstrate an extensive collateral vascular supply maintaining renal viability, an initial therapeutic trial with one of the previously mentioned nonoperative approaches may be worthwhile.
Neurofibromatosis
Neurofibromatosis affecting the renal arteries is a congenital hereditary disorder characterized by café-au-lait cutaneous pigmentation, cutaneous neurofibromas, tumors of the CNS, skeletal disorders, and occasional gigantism (Grad and Rance, 1972; Tilford and Kelsch, 1973). Hypertension in patients with neurofibromatosis is most often due to renal artery stenosis; less commonly, this may be the result of an associated pheochromocytoma or aortic coarctation. Vascular abnormality occurs in the kidneys, heart, and gastrointestinal tract and consists of fibrosis and thickening of the intima, proliferation of neural tissue within the arterial wall, perivascular nodular proliferations, and occasional aneurysmal dilatation. In the kidney, arterial stenosis usually occurs at the origin or in the proximal third of the main renal artery, and the angiographic appearance may be indistinguishable from that of intimal fibroplasia. Considering the young age of these patients, renal revascularization is generally the treatment of choice for associated RVH.
Middle Aortic Syndrome
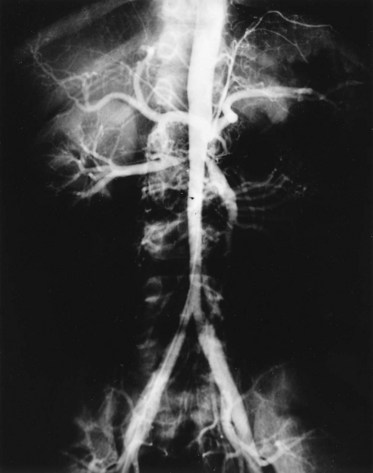
The middle aortic syndrome is a rare disorder, occurring in children or young adults, characterized by nonspecific stenosing arteritis affecting the aorta and its major branches, including the renal arteries (Fig. 39–19). This is thought to be a form of Takayasu disease, and an autoimmune pathogenesis is suspected (Kaufman, 1973). This disease can extensively involve the subdiaphragmatic aorta or, in some cases, may spare the aorta and involve primarily the renal or splanchnic vessels. The natural history is not well understood because most cases are diagnosed when the disease has already resulted in significant renal arterial stenosis in young good-risk patients, thus necessitating early revascularization. Because the inflammatory process generally does not extend to involve the iliac arteries, renal autotransplantation is the surgical treatment of choice.
Extrinsic Obstruction
Extrinsic obstruction of the renal artery has been observed but is extremely rare (Silver and Clements, 1976). Neural tissue, musculocutaneous fibers, and diaphragmatic crura have been suggested as etiologic factors contributing to this process. Other possible causes of extrinsic perivascular fibrosis include inflammation, trauma, tumor, or prior radiation.
The Page Kidney
In 1934, Page (1939) produced a renin-dependent model of hypertension by wrapping a dog kidney in cellophane. Hypertension could be reversed by removing the cellophane wrap or the kidney. The clinical equivalent of this hypertensive model is the kidney compressed by a subcapsular or perirenal process causing renal ischemia, inducing unilateral hypersecretion of renin and contralateral suppression. Causes of the perinephric process include blunt trauma, closed renal biopsy, anticoagulation, or hemorrhage from a tumor.
The diagnosis of the Page kidney depends on the presence of either a surrounding hematoma or an encasing fibrous pseudocapsule. Imaging with ultrasonography, CT, or MRI localizes the hematoma or fibrous capsule.
The treatment of the Page kidney aims to preserve renal function and cure hypertension. Medical antihypertensive therapy plus observation, percutaneous evacuation of the perirenal hematoma, open drainage of the hematoma, and nephrectomy have all been used (Suffrin, 1975).
Some cases of the acute Page kidney with new-onset hypertension have spontaneously resolved. A hematoma may reabsorb, relieving the parenchymal compression without forming an adhesive fibrotic pseudocapsule. Treatment with medical antihypertensive therapy can control the blood pressure until the hematoma resolves. If the hematoma does not resolve, it may be drained percutaneously or surgically.
Renal Parenchymal Disease
Renin-mediated hypertension may be secondary to a variety of renal parenchymal diseases. The incidence of hypertension in patients with chronic pyelonephritis is approximately 5% to 10%. The mechanism of renin-mediated hypertension in such kidneys with segmental scars is ischemia of the relatively normal renal cortex in proximity to areas of interstitial fibrosis, within which are small vessels with intimal thickening. Other renal disorders that may cause hypertension include hydronephrosis, congenital hypoplasia or dysplasia, segmental hypoplasia (Ask-Upmark kidney), vesicoureteral reflux, renal cell carcinoma, benign cyst, Wilms tumor, radiation nephritis, or juxtaglomerular cell tumor.
Key Points: Management of Patients with Renal Artery Disease
Case DB, Laragh JH. Reactive hyperreninemia in renovascular hypertension after angiotensin blockage with saralasin or converting enzyme inhibitor. Ann Intern Med. 1979;91:153-160.
Chrysochou C, Buckley DL, Kalra PA. Magnetic resonance imaging: advances in the investigation of atheromatous renovascular disease. J Nephrol. 2008;21:468-477.
Dubel GJ, Murphy TP. The role of percutaneous revascularization for renal artery stenosis. Vasc Med. 2008;13:141-156.
Dworkin LD, Jamerson KA. Is renal artery stenting the correct treatment of renal artery stenosis? Case against angioplasty and stenting of atherosclerotic renal artery stenosis. Circulation. 2007;115:271-276. discussion 276
Fergany A, Kolettis P, Novick AC. The contemporary role of extra-anatomical surgical renal revascularization in patients with atherosclerotic renal artery disease. J Urol. 1995;153:1798-1802.
Hansen KJ, Edwards MS, Craven TE, et al. Prevalence of renovascular disease in the elderly: a population-based study. J Vasc Surg. 2002;36:443-451.
Kaylor W, Novick AC, Ziegelbaum M, et al. Reversal of end-stage renal failure with surgical revascularization in patients with atherosclerotic renal artery occlusion. J Urol. 1989;141:486-488.
Lawrie GM, Morris GC, Claeser DH, DeBakey ME. Renovascular reconstruction: factors affecting long-term prognosis in 919 patients followed up in 31 years. Am J Cardiol. 1989;63:1085-1092.
Novick AC, Scoble J, Hamilton G, editors. Renal vascular disease. London: WB Saunders, 1996.
Novick AC, Straffon RA, Stewart BH, et al. Diminished operative morbidity and mortality following revascularization for atherosclerotic renovascular disease. JAMA. 1981;246:749-753.
Novick AC, Ziegelbaum M, Vidt DG, et al. Trends in surgical revascularization for renal artery disease: ten years’ experience. JAMA. 1987;257:498-501.
Olin JW, Melia M, Young JR, et al. Prevalence of atherosclerotic renal artery stenosis in patients with atherosclerosis elsewhere. Am J Med. 1990;188:46-51.
Pimenta E, Oparil S. Renin inhibitors: novel agents for renoprotection or a better angiotensin receptor blocker for blood pressure lowering? Cardiol Clin. 2008;26:527-535.
Schreiber MJ, Pohl MA, Novick AC. The natural history of atherosclerotic and fibrous renal artery disease. Urol Clin North Am. 1984;11:383.
Steinbach F, Novick AC, Campbell S, Dykstra D. Long-term survival after surgical revascularization for atherosclerotic renal artery disease. J Urol. 1997;158:38-41.
Taylor ATJr, Fletcher JW, Nally JVJr, et al. Procedure guideline for diagnosis of renovascular hypertension. Society of Nuclear Medicine. J Nucl Med. 1998;39:1297-1302.
Tullus K, Brennan E, Hamilton G, et al. Renovascular hypertension in children. Lancet. 2008;371:1453-1463.
Zähringer M, Pattynama PM, Talen A, Sapoval M. Drug-eluting stents in renal artery stenosis. Eur Radiol. 2008;18:678-682.
Zeller T, Bonvini RF, Sixt S. Color-coded duplex ultrasound for diagnosis of renal artery stenosis and as follow-up examination after revascularization. Catheter Cardiovasc Interv. 2008;71:995-999.
Aguilera G. Factors controlling steroid biosynthesis in the zona glomerulosa of the adrenal. J Steroid Biochem Mol Biol. 1993;45:147-151.
Ailawadi G, Stanley JC, Williams DM, et al. Gadolinium as a nonnephrotoxic contrast agent for catheter-based arteriographic evaluation of renal arteries in patients with azotemia. J Vasc Surg. 2003;37(2):346-352.
Aqel RA, Zoghbi GJ, Baldwin SA, et al. Prevalence of renal artery stenosis in high-risk veterans referred to cardiac catheterization. J Hypertens. 2003;21:1157-1162.
Arendshorst WJ, Finn WF. Renal hemodynamics in the rat before and during inhibition of angiotensin II. Am J Physiol. 1977;233:F290-F297.
Atlas SA, Laragh JH, Sealey JE, Hesson TE. An inactive, prorenin-like substance in human kidney and plasma. Clin Sci. 1980;59(Suppl. 6):29S-33S.
Baboolal K, Evans C, Moore RH. Incidence of end-stage renal disease in medically treated patients with severe bilateral atherosclerotic renovascular disease. Am J Kidney Dis. 1998;31:971-977.
Baert AL, Wilms G, Amery A, et al. Percutaneous transluminal renal angioplasty: initial results and long-term follow-up in 202 patients. Cardiovasc Intervent Radiol. 1990;13:22-28.
Bedoya L, Ziegelbaum M, Vidt DG, et al. The effect of baseline renal function on the outcome following renal revascularization. Cleve Clin J Med. 1989;59:415-421.
Beek FJ, Kaatee R, Beutler JJ, et al. Complications during renal artery stent placement for atherosclerotic ostial stenosis. Cardiovasc Intervent Radiol. 1997;20:184-190.
Belenfant X, Meyrier A, Jacquot C. Supportive treatment improves survival in multivisceral cholesterol crystal embolism. Am J Kidney Dis. 1999;33:840-850.
Bilge AK, Nisanci Y, Yilmaz E, et al. Renovascular hypertension secondary to spontaneous renal artery dissection and treatment with stenting. Int J Clin Pract. 2003;57(5):435-436.
Blake WD, Wegria R, Ward HP, Frank CW. Effect of renal arterial constriction on excretion of sodium and water. Am J Physiol. 1950;163:422.
Blantz RC, Konnen KS, Tucker BJ. Angiotensin II effects upon the glomerular microcirculation and ultrafiltration coefficient of the rat. J Clin Invest. 1976;57:419-434.
Blum U, Krumme B, Flugel P, et al. Treatment of ostial renal-artery stenoses with vascular endoprostheses after unsuccessful balloon angioplasty. N Engl J Med. 1997;336:459-465.
Boisclair C, Therasse E, Oliva VL, et al. Treatment of renal angioplasty failure by percutaneous renal artery stenting with Palmaz stents: midterm technical and clinical results. AJR Am J Roentgenol. 1997;168:245-251.
Bonelli FS, McKusick MA, Textor SC, et al. Renal artery angioplasty: technical results and clinical outcome in 320 patients. Mayo Clin Proc. 1995;70:1041-1052.
Boyd AS, Zic JA, Abraham JL. Gadolinium deposition in nephrogenic fibrosing dermopathy. J Am Acad Dermatol. 2007;56(1):27-30.
Braun-Menendez E, Fasciolo JC, Leloir LR, Munoz JM. The substance causing renal hypertension. J Physiol. 1940;98:283.
Bredenberg CE, Sampson LN, Ray FS, et al. Changing patterns in surgery for chronic renal artery occlusive diseases. J Vasc Surg. 1992;15:1018-1024.
Brentjens JR, Matsuo S, Andres GA, et al. Gametes contain angiotensin converting enzyme (kininase II). Experientia. 1986;42:399-402.
Bright R. Reports of medical cases, selected with a view of illustrating symptoms and cure of disease by reference to morbid anatomy. London: Longman Group; 1827.
Broome DR, Girguis MS, Baron PW, et al. Gadodiamide-associated nephrogenic systemic fibrosis: why radiologists should be concerned. AJR Am J Roentgenol. 2007;188:586-592.
Browne RF, Riordan EO, Roberts JA, et al. Renal artery aneurysms: diagnosis and surveillance with 3D contrast-enhanced magnetic resonance angiography. Eur Radiol. 2004;14(10):1807-1812.
Bruce M, Kuan YM. Endoluminal stent-graft repair of a renal artery aneurysm. J Endovasc Ther. 2002;9(3):359-362.
Brunner HR, Laragh JH, Baer L, et al. Essential hypertension: renin and aldosterone, heart attack and stroke. N Engl J Med. 1972;286:441-449.
Bumpus FM, Schwarz H, Page IH. Synthesis and pharmacology of the octapeptide angiotensin. Science. 1957;125:886.
Buonocore E, Meaney TF, Borkowski GP, et al. Digital subtraction angiography of the abdominal aorta and renal arteries. Comparison with conventional aortography. Radiology. 1981;139:281-286.
Burket MW, Cooper CJ, Kennedy DJ, et al. Renal artery angioplasty and stent placement: predictors of a favorable outcome. Am Heart J. 2000;139:64-71.
Butler AM. Chronic pyelonephritis and arterial hypertension. J Clin Invest. 1937;16:889.
Canzanello VJ, Millan VG, Spiegel JE, et al. Percutaneous transluminal renal angioplasty in management of atherosclerotic renovascular hypertension: results in 100 patients. Hypertension. 1989;13:163-172.
Caridi JG, Stavropoulos SW, Hawkins IFJr. Carbon dioxide digital subtraction angiography for renal artery stent placement. J Vasc Interv Radiol. 1999;10:635-640.
Carrell RW, Pemberton PA, Boswell DR. The serpins: evolution and adaptation in a family of protease inhibitors. Cold Spring Harb Symp Quant Biol. 1987;52:527-535.
Case DB, Laragh JH. Reactive hyperreninemia in renovascular hypertension after angiotensin blockage with saralasin or converting enzyme inhibitor. Ann Intern Med. 1979;91:153-160.
Chaikof EL, Smith RB, Salam AA, et al. Ischemic nephropathy and concomitant aortic disease. A ten-year experience. J Vasc Surg. 1994;19:135-148.
Chappell M, Ferrario C. Angiotensin-(1-7) in hypertension. Curr Opin Nephrol Hypertens. 1999;8:231-235.
Chavan A, Hausmann D, Brunkhorst R. Intravascular ultrasound to establish the indication for renal angioplasty. Nephrol Dial Transplant. 1998;13:1583-1584.
Chen R, Novick AC, Pohl M. Reversible renin mediated massive proteinuria successfully treated by nephrectomy. J Urol. 1995;153:133-134.
Cherr GS, Hansen KJ, Craven TE, et al. Surgical management of atherosclerotic renovascular disease. J Vasc Surg. 2002;35(2):236-245.
Chevalier RL, Tegtmeyer CJ, Gomez RA. Percutaneous transluminal angioplasty for renovascular hypertension in children. Pediatr Nephrol. 1987;1:89-98.
Chiche L, Kieffer E, Sabatier J, et al. Renal autotransplantation for vascular disease: late outcome according to etiology. J Vasc Surg. 2003;37(2):353-361.
Chobanian AV, Bakris GL, Black HR, et al. Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure. National Heart, Lung, and Blood Institute; National High Blood Pressure Education Program Coordinating Committee. Seventh report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure. Hypertension. 2003;42:1206-1252.
Choudhri AH, Cleland JGF, Rowlands PC, et al. Unsuspected renal artery stenosis in peripheral vascular disease. BMJ. 1990;301:1197-1198.
Chrysochou C, Buckley DL, Kalra PA. Magnetic resonance imaging: advances in the investigation of atheromatous renovascular disease. J Nephrol. 2008;21:468-477.
Corradi B, Malberti F, Farini M, et al. Chronic renal failure due to atheromatous renovascular disease in the elderly. Contrib Nephrol. 1993;105:167-171.
Courtel JV, Soto B, Niaudet P, et al. Percutaneous transluminal angioplasty of renal artery stenosis in children. Pediatr Radiol. 1998;28:59-63.
Danilov SM, Faerman AI, Printseva OYU, et al. Immunohistochemical study of angiotensin-converting enzyme in human tissues using monoclonal antibodies. Histochemistry. 1987;87:487-490.
De Cobelli F, Venturini M, Vanzulli A, et al. Renal arterial stenosis: prospective comparison of color Doppler US and breath-hold, three-dimensional, dynamic, gadolinium-enhanced MR angiography. Radiology. 2000;214:373-380.
Dean RH, Callis JT, Smith BM, Meacham PW. Failed percutaneous transluminal renal angioplasty: experience with lesions requiring operative interventions. J Vasc Surg. 1987;6:301-307.
Dean RH, Tribble RW, Hansen KJ, et al. Evolution of renal insufficiency in ischemic nephropathy. Ann Surg. 1991;213:446-456.
de Fraissinette B, Garcier JM, Dieu V, et al. Percutaneous transluminal angioplasty of dysplastic stenoses of the renal artery: results on 70 adults. Cardiovasc Intervent Radiol. 2003;26(1):46-51.
Deitch JS, Hansen KJ, Regan JD, et al. Infected renal artery pseudoaneurysm and mycotic aortic aneurysm after percutaneous transluminal renal artery angioplasty and stent placement in a patient with a solitary kidney. J Vasc Surg. 1998;28:340-344.
Deyu Z, Lisheng L, Ruping D, et al. Percutaneous transluminal renal angioplasty in aortoarteritis. Int J Cardiol. 1998;66(Suppl. 1):S205-S211.
Dondi M. Captopril renal scintigraphy with 99mTc-mercaptoacetyltriglycine (99mTc-MAG3) for detecting renal artery stenosis. Am J Hypertens. 1991;4:737S-740S.
Dong ZJ, Li SH, Lu XC. Percutaneous transluminal angioplasty for renovascular hypertension in arteritis: experience in China. Radiology. 1987;162:477-479.
Dorros G, Jaff M, Mathiak L, et al. Four-year follow-up of Palmaz-Schatz sent revascularization as treatment for atherosclerotic renal artery stenosis. Circulation. 1998;98:642-647.
Dotter CT, Judkins MP. Transluminal treatment of arteriosclerotic obstruction. Description of a new technic and a preliminary report of its application. Circulation. 1964;30:654.
D’Souza SJ, Tsai WS, Silver MM, et al. Diagnosis and management of stenotic aorto-arteriopathy in childhood. J Pediatr. 1998;132:1016-1022.
Dzau VJ, Ellison KE, Brody T, et al. A comparative study of the distributions of renin and angiotensinogen messenger ribonucleic acids in rat and mouse tissues. Endocrinology. 1987;120:2334-2338.
Egido J. Vasoactive hormones and renal sclerosis. Kidney Int. 1996;49:587-597.
Ehlers MR, Riordan JF. Angiotensin-converting enzyme: new concepts concerning its biological role. Biochemistry. 1989;28:5311-5318.
Eldrup-Jorgensen J, Harvey HR, Sampson LN, et al. Should percutaneous transluminal renal artery angioplasty be applied to ostial renal artery atherosclerosis? J Vasc Surg. 1995;21:909-914. discussion 914–15
Eng E, Veniant M, Floege J, et al. Renal proliferative and phenotypic changes in rats with two-kidney, one-clip Goldblatt hypertension. Am J Hypertens. 1994;7:177-185.
English WP, Pearce JD, Craven TE, et al. Surgical management of renal artery aneurysms. J Vasc Surg. 2004;40(1):53-60.
Erbsloh-Moller B, Dumas A, Roth D, et al. Furosemide-131I-hippuran renography after angiotensin-converting enzyme inhibition for the diagnosis of renovascular hypertension. Am J Med. 1991;90:23-29.
Erturk E, Novick AC, Vidt DG, Cunningham R. Secondary renal revascularization for recurrent renal artery stenosis. Cleve Clin J Med. 1989;56:427-431.
Eyler WR, Clark MD, Garman JE, et al. Angiography of the renal areas including a comparative study of renal arterial stenosis in patients with and without hypertension. Radiology. 1962;78:879.
Fatica RA, Port FK, Young EW. Incidence trends and mortality in end-stage renal disease attributed to renovascular disease in the United States. Am J Kidney Dis. 2001;37(6):1184-1190.
Fergany A, Kolettis P, Novick AC. The contemporary role of extra-anatomical surgical renal revascularization in patients with atherosclerotic renal artery disease. J Urol. 1995;153:1798-1802.
Fiala LA, Jackson MR, Gillespie DL, et al. Primary stenting of atherosclerotic renal artery ostial stenosis. Ann Vasc Surg. 1998;12:128-133.
Fine MJ, Kapoor W, Falanga V. Cholesterol crystal embolization: a review of 221 cases in the English literature. Angiology. 1987;38:769-784.
Fitridge RA, Petrucco M, Dunlop CM, et al. Arteriography in chronic renal failure: a case for carbon dioxide. Cardiovasc Surg. 1999;7:323-326.
Fitzsimons JT. Angiotensin stimulation of the central nervous system. Rev Physiol Biochem Pharmacol. 1980;87:117-167.
Fleischmann D. MDCT of renal and mesenteric vessels. Eur Radiol. 2003;13(Suppl. 5):M94-101.
Franco-Saenz R, Suzuki S, Tan SY, Mulrow PJ. Prostaglandin stimulation of renin release: independence of beta-adrenergic receptor activity and possible mechanism of action. Endocrinology. 1980;106:1400-1404.
Frederickson ED, Wilcox CS, Bucci M, et al. A prospective evaluation of a simplified captopril test for the detection of renovascular hypertension. Arch Intern Med. 1990;150:569-572.
Friedland J, Setton C, Silverstein E. Induction of angiotensin converting enzyme in human monocytes in culture. Biochem Biophys Res Commun. 1978;83:843-849.
Gauthier B, Trachtman H, Frank R, Pillari G. Inadequacy of captopril challenge test for diagnosing renovascular hypertension in children and adolescents. Pediatr Nephrol. 1991;5:42-44.
Geisterfer AA, Peach MJ, Owens GK. Angiotensin II induces hypertrophy, not hyperplasia, of cultured rat aortic smooth muscle cells. Circ Res. 1988;62:749-756.
Ghantous VE, Eisen TD, Sherman AH, Finkelstein FO. Evaluating patients with renal failure for renal artery stenosis with gadolinium-enhanced magnetic resonance angiography. Am J Kidney Dis. 1999;33:36-42.
Gifford RWJr, McCormack LJ, Poutasse EF. The atrophic kidney: its role in hypertension. Mayo Clin Proc. 1965;40:834-852.
Gilfeather M, Yoon HC, Siegelman ES, et al. Renal artery stenosis: evaluation with conventional angiography versus gadolinium-enhanced MR angiography. Radiology. 1999;210:367-372.
Goldblatt H, Lynch J, Hanzal RF, Summerville WW. Studies on experimental hypertension. I. The production of persistent elevation of systolic blood pressure by means of renal ischemia. J Exp Med. 1934;59:347.
Goldfarb DA, Diz DI, Tubbs RR, et al. Angiotensin II receptor subtypes in the human renal cortex and renal cell carcinoma. J Urol. 1994;151:208-213.
Goodfriend TL, Elliott ME, Catt KJ. Drug therapy: angiotensin receptors and their antagonists. N Engl J Med. 1996;334:1649-1654.
Goormaghtigh N, Grimson KS. Vascular changes in renal ischemia, cell mitosis in the media of arteries. Proc Soc Exp Biol Med. 1939;42:227.
Gordon GI, Vogelzang RL, Curry RH, et al. Endovascular infection after renal artery stent placement. J Vasc Interv Radiol. 1996;7:669-672.
Gosse P, Dupas JY, Reynaud P, et al. Captopril test in the detection of renovascular hypertension in a population with low prevalence of the disease. A prospective study. Am J Hypertens. 1989;2:191-193.
Grad E, Rance CP. Bilateral renal artery stenosis in association with neurofibromatosis (Recklinghausen’s disease): report of two cases. J Pediatr. 1972;80:804-808.
Greminger P, Steiner A, Schneider E, et al. Cure and improvement of renovascular hypertension after percutaneous transluminal angioplasty of renal artery stenosis. Nephron. 1989;51:362-366.
Grist TM. Magnetic resonance angiography of renal artery stenosis. Am J Kidney Dis. 1994;24:700-712.
Gruntzig A, Kuhlmann U, Vetter W, et al. Treatment of renovascular hypertension with percutaneous transluminal dilatation of a renal-artery stenosis. Lancet. 1978;1:801-802.
Gunning ME, Ingelfinger JR, King AJ, Brenner BM. Vasoactive peptides and the kidney. In: Brenner BM, editor. The kidney. 5th ed. Philadelphia: WB Saunders; 1996:627-712.
Hagspiel KD, Stone JR, Leung DA. Renal angioplasty and stent placement with distal protection: preliminary experience with the FilterWire EX. J Vasc Interv Radiol. 2005;16:125-131.
Hall JE, Guyton AC, Jackson TE, et al. Control of glomerular filtration rate by renin-angiotensin system. Am J Physiol. 1977;233:F366-F372.
Hallett JW, Fowl R, O’Brien PC, et al. Renovascular operations in patients with chronic renal insufficiency: do the benefits justify the risks? J Vasc Surg. 1987;5:622-627.
Halloul Z, Buerger T, Grote R, Meyer F. Selective embolization of a renal artery aneurysm. Vasa. 2000;29(4):285-287.
Halpern EJ, Nazarian LN, Wechsler RJ, et al. US, CT, and MR evaluation of accessory renal arteries and proximal renal arterial branches. Acad Radiol. 1999;6:299-304.
Hamilton G. Fibrinolytic therapy in renovascular disease. In: Novick A, Scoble J, Hamilton G, editors. Renal vascular disease. Philadelphia: WB Saunders; 1996:417-430.
Hansen KJ, Edwards MS, Craven TE, et al. Prevalence of renovascular disease in the elderly: a population-based study. J Vasc Surg. 2002;36(3):443-451.
Hansen KJ, Starr SM, Sands E, et al. Contemporary surgical management of renovascular disease. J Vasc Surg. 1992;16:319-331.
Hany TF, Leung DA, Pfammatter T, Debatin JF. Contrast-enhanced magnetic resonance angiography of the renal arteries. Original investigation. Invest Radiol. 1998;33:653-659.
Harden PN, MacLeod MJ, Rodger RS, et al. Effect of renal-artery stenting on progression of renovascular renal failure. Lancet. 1997;349:1133-1136.
Harding MB, Smith LR, Himmestein SI, et al. Renal artery stenosis: prevalence and associated risk factors in patients undergoing routine cardiac catheterization. J Am Soc Nephrol. 1992;2:1608-1616.
Harris PJ, Young JA. Dose-dependent stimulation and inhibition of proximal tubular sodium reabsorption by angiotensin II in the rat kidney. Pflugers Arch. 1977;367:295-297.
Hawkins IFJr, Wilcox CS, Kerns SR, Sabatelli FW. CO2 digital angiography: a safer contrast agent for renal vascular imaging? Am J Kidney Dis. 1994;24:685-694.
Hayes JM, Risius B, Novick AC, et al. Experience with percutaneous transluminal angioplasty for renal artery stenosis at the Cleveland Clinic. J Urol. 1988;139:488-492.
Henke PK, Cardneau JD, Welling TH3rd, et al. Renal artery aneurysms: a 35-year clinical experience with 252 aneurysms in 168 patients. Ann Surg. 2001;234(4):454-462. discussion 462–3
Hennequin LM, Joffre FG, Rousseau HP, et al. Renal artery stent placement: long-term results with the Wallstent endoprosthesis. Radiology. 1994;191:713-719.
Henry M, Amor M, Henry I, et al. Stent placement in the renal artery: three-year experience with the Palmaz stent. J Vasc Interv Radiol. 1996;7:343-350.
Henry M, Klonaris C, Henry I, et al. Protected renal stenting with the PercuSurge GuardWire device: a pilot study. J Endovasc Ther. 2001;8:227-237.
Hofbeck M, Singer H, Rupprecht T, et al. Successful percutaneous transluminal angioplasty for treatment of renovascular hypertension in a 15-month-old child. Eur J Pediatr. 1998;157:512-514.
Hoffman O, Carreres T, Sapoval MR, et al. Ostial renal artery stenosis angioplasty: immediate and mid-term angiographic and clinical results. J Vasc Interv Radiol. 1998;9:65-73.
Hoj Nielsen A, Knudsen F. Angiotensinogen is an acute-phase protein in man. Scand J Clin Lab Invest. 1987;47:175-178.
Holden A, Hill A, Jaff MR, Pilmore H. Renal artery stent revascularization with embolic protection in patients with ischemic nephropathy. Kidney Int. 2006;70:948-955.
Holley KE, Hunt JC, Brown Al, et al. Renal artery stenosis: a clinical-pathologic study in normotensive patients. Am J Med. 1964;37:14.
Horiuchi M, Akishita M, Dzau VJ. Recent progress in angiotensin II type 2 receptor research in the cardiovascular system. Hypertension. 1999;33:613-621.
Howard JE, Conner TB. Use of differential renal function studies in the diagnosis of renovascular hypertension. Am J Surg. 1964;107:58.
Hoxie HJ, Coggins CB. Renal infarction: statistical study in 205 cases. Arch Intern Med. 1940;65:587-594.
Hricik DE, Browning PJ, Kopelman R, et al. Captopril-induced functional renal insufficiency in patients with bilateral renal artery stenosis or renal artery stenosing in a solitary kidney. N Engl J Med. 1983;308:373-376.
Hura CE, Kunau RTJr. Angiotensin II-stimulated prostaglandin production by canine renal afferent arterioles. Am J Physiol. 1988;254:F734-F738.
Iannone LA, Underwood PL, Nath A, et al. Effect of primary balloon expandable renal artery stents on long-term patency, renal function, and blood pressure in hypertensive and renal insufficient patients with renal artery stenosis. Cathet Cardiovasc Diagn. 1996;37:243-250.
Imamura H, Isobe M, Takenaka H, et al. Successful stenting of bilateral renal artery stenosis due to fibromuscular dysplasia assessed by use of pressure guidewire technique: a case report. Angiology. 1998;49:69-74.
Jensen G, Zachrisson BF, Delin K, et al. Treatment of renovascular hypertension: one year results of renal angioplasty. Kidney Int. 1995;48:1936-1945.
Joffre F, Rousseau H, Bernadet P, et al. Midterm results of renal artery stenting. Cardiovasc Intervent Radiol. 1992;15:313-318.
Kageyama R, Ohkubo H, Nakanishi S. Primary structure of human preangiotensinogen deduced from the cloned cDNA sequence. Biochemistry. 1984;23:3603-3609.
Kang PM, Landau AJ, Eberhardt RT, Frishman WH. Angiotensin II receptor antagonists: a new approach to blockade on the renin-angiotensin system. Am Heart J. 1994;127:1388-1401.
Kaplan-Pavlovcic S, Nadja C. Captopril renography and duplex Doppler sonography in the diagnosis of renovascular hypertension. Nephrol Dial Transplant. 1998;13:313-317.
Karagiannis A, Douma S, Voyiatzis K, et al. Percutaneous transluminal renal angioplasty in patients with renovascular hypertension: long-term results. Hypertens Res. 1995;18:27-31.
Karkos CD, D’Souza SP, Thomson GJ, et al. Renal artery aneurysm: endovascular treatment by coil embolisation with preservation of renal blood flow. Eur J Vasc Endovasc Surg. 2000;19(2):214-216.
Kaufman JJ. The middle aortic syndrome: report of a case treated by renal autotransplantation. J Urol. 1973;109:711-715.
Kaylor W, Novick AC, Ziegelbaum M, et al. Reversal of end-stage renal failure with surgical revascularization in patients with atherosclerotic renal artery occlusion. J Urol. 1989;141:486-488.
Keeton TK, Campbell WB. The pharmacologic alteration of renin release. Pharmacol Rev. 1980;32:81-227.
Kennedy DJ, Colyer WR, Brewster PS, et al. Renal insufficiency as a predictor of adverse events and mortality after renal artery stent placement. Am J Kidney Dis. 2003;42(5):926-935.
Kim TS, Chung JW, Park JH, et al. Renal artery evaluation: comparison of spiral CT angiography to intra-arterial DSA. J Vasc Interv Radiol. 1998;9:553-559.
Klinge J, Mali WP, Puijlaert CB, et al. Percutaneous transluminal renal angioplasty: initial and long-term results. Radiology. 1989;171:501-506.
Klow NE, Paulsen D, Vatne K, et al. Percutaneous transluminal renal artery angioplasty using the coaxial technique. Ten years of experience from 591 procedures in 419 patients. Acta Radiol. 1998;39:594-603.
Krishnamurthi V, Novick AC, Myles JL. Atheroembolic renal disease: effect on morbidity and survival after revascularization for atherosclerotic renal artery stenosis. J Urol. 1999;161:1093-1096.
Kriss VM, Cottrill CM, Gurley JC. Carbon dioxide (CO2) angiography in children. Pediatr Radiol. 1997;27:807-810.
Kuhn FP, Kutkuhn B, Torsello G, Modder U. Renal artery stenosis: preliminary results of treatment with the Strecker stent. Radiology. 1991;180:367-372.
Kumar A, Shapiro AP. Proteinuria and nephrotic syndrome induced by renin in patients with renal artery stenosis. Arch Intern Med. 1980;140:1631-1634.
Laragh JH, Blumenfeld JD. Essential hypertension. In: Brenner BM, editor. The kidney. 5th ed. Philadelphia: WB Saunders; 1996:2071.
Lawrie GM, Morris CGJR, DeBakey ME. Long-term results of treatment of the totally occluded renal artery in 40 patients with renovascular hypertension. Surgery. 1980;88:753-759.
Lawrie GM, Morris GC, Claeser DH, DeBakey ME. Renovascular reconstruction: factors affecting long-term prognosis in 919 patients followed up in 31 years. Am J Cardiol. 1989;63:1085-1092.
Leadbetter WF, Burkland CF. Hypertension in unilateral renal disease. J Urol. 1938;39:611.
Lee ML, Chaou WT, Wang JK, et al. Percutaneous transluminal angioplasty of renal artery stenosis in a 9-month-old hypertensive girl with congestive heart failure. Acta Paediatr. 1999;88:1165-1167.
Leertouwer TC, Gussenhoven EJ, Bosch JL, et al. Stent placement for renal arterial stenosis: where do we stand? A meta-analysis. Radiology. 2000;216:78-85.
Leung DA, Hoffmann U, Pfammatter T, et al. Magnetic resonance angiography versus duplex sonography for diagnosing renovascular disease. Hypertension. 1999;33:726-731.
Lew EA. High blood pressure, other risk factors and longevity. In: Laragh JH, editor. The insurance viewpoint in hypertension manual. New York: Yorke Medical; 1973:105-119.
Lewin A, Blaufox MD, Castle H, et al. Apparent prevalence of curable hypertension in the Hypertension Detection and Follow-up Program. Arch Intern Med. 1985;145:424-427.
Liang CD, Ko SF, Fang CY. Percutaneous transluminal angioplasty of renal artery stenosis in a child with hypertensive heart disease. Cathet Cardiovasc Intervent. 1999;48:374-377.
Libertino JA, Bosco PJ, Ying CY, et al. Renal revascularization to preserve and restore renal function. J Urol. 1992;147:1485-1487.
Libertino JA, Flam TA, Zinman LN, et al. Changing concepts in surgical management of renovascular hypertension. Arch Intern Med. 1988;148:357-359.
Lieberman J, Sastre A. Angiotensin-converting enzyme activity in postmortem human tissues. Lab Invest. 1983;48:711-717.
Lorenz JN, Kotchen TA, Ott CE. Effect of Na and Cl infusion on loop function and plasma renin activity in rats. Am J Physiol. 1990;258:F1328-F1335.
Losinno F, Zuccala A, Busato F, Zucchelli P. Renal artery angioplasty for renovascular hypertension and preservation of renal function: long-term angiographic and clinical follow-up. AJR Am J Roentgenol. 1994;162:853-857.
Lovaria A, Nicolini A, Meregaglia D, et al. Interventional radiology in the treatment of renal artery stenosis. Ann Urol (Paris). 1999;33:146-155.
Lund G, Sinaiko A, Castaneda-Zuniga W, et al. Percutaneous transluminal angioplasty for treatment of renal artery stenosis in children. Eur J Radiol. 1984;4:254-257.
Lupattelli T, Abubacker Z, Morgan R, Belli AM. Embolization of a renal artery aneurysm using ethylene vinyl alcohol copolymer (Onyx). J Endovasc Ther. 2003;10(2):366-370.
MacLeod M, Taylor AD, Baxter G, et al. Renal artery stenosis managed by Palmaz stent insertion: technical and clinical outcome. J Hypertens. 1995;13:1791-1795.
Mai M, Geiger H, Hilgers KF, et al. Early interstitial changes in hypertension-induced renal injury. Hypertension. 1993;22:754-765.
Mailloux LU, Bellucci AG, Mosey RT, et al. Predictors of survival in patients undergoing dialysis. Am J Med. 1988;84:855-862.
Major P, Genest J, Cartier P, Kuchel O. Hereditary fibromuscular dysplasia with renovascular hypertension [letter]. Ann Intern Med. 1977;86:583.
Martin LG, Casarella WJ, Alspaugh JP, Chuang VP. Renal artery angioplasty: increased technical success and decreased complications in the second 100 patients. Radiology. 1986;159:631-634.
Martin LG, Casarella WJ, Gaylord GM. Azotemia caused by renal artery stenosis: treatment by percutaneous angioplasty. AJR Am J Roentgenol. 1988;150:839-844.
Martin LG, Price RB, Casarella WJ, et al. Percutaneous angioplasty in clinical management of renovascular hypertension: initial and long-term results. Radiology. 1985;155:629-633.
Martinez AG, Novick AC, Hayes JM. Surgical treatment of renal artery stenosis after failed percutaneous transluminal angioplasty. J Urol. 1990;144:1094-1096.
Maxwell MH, Bleifer KH, Franklin SS, Varady PD. Cooperative study of renovascular hypertension. Demographic analysis of the study. JAMA. 1972;220:1195-1204.
McCann RL, Bollinger RR, Newman GE. Surgical renal artery reconstruction after percutaneous transluminal angioplasty. J Vasc Surg. 1988;8:394-398.
Mercier C, Piquet P, Alimi Y, et al. Occlusive disease of the renal arteries and chronic renal failure: the limits of reconstructive surgery. Ann Vasc Surg. 1990;4:166-170.
Millan VG, McCauley J, Kopelman RI, Madias NE. Percutaneous transluminal renal angioplasty in nonatherosclerotic renovascular hypertension. Long-term results. Hypertension. 1985;7:668-674.
Millan VG, Sher MH, Deterling RAJr, et al. Transcatheter thromboembolectomy of acute renal artery occlusion. Arch Surg. 1978;113:1086-1092.
Miralles M, Cairols M, Cotillas J, et al. Value of Doppler parameters in the diagnosis of renal artery stenosis. J Vasc Surg. 1996;23:428-435.
Miralles M, Santiso A, Gimenez A, et al. Renal duplex scanning: correlation with angiography and isotopic renography. Eur J Vasc Surg. 1993;7:188-194.
Missouris CG, Allen CM, Balen FG, et al. Non-invasive screening for renal artery stenosis with ultrasound contrast enhancement. J Hypertens. 1996;14:519-524.
Missouris CG, Buchenham T, Cappuccio FP, MacGregor GA. Renal artery stenosis: a common and important problem in patients with peripheral vascular disease. Am J Med. 1994;96:10-14.
Mizoguchi H, Dzau VJ, Siwek LG, Barger AC. Effect of intrarenal administration of dopamine on renin release in conscious dogs. Am J Physiol. 1983;244:H39-H45.
Mohomed FA. The etiology of Bright’s disease and the prealbuminuric stage. Med Chir Trans. 1874;57:197.
Mollo M, Pelet V, Mouawad J, et al. Evaluation of color duplex ultrasound scanning in diagnosis of renal artery stenosis, compared to angiography: a prospective study on 53 patients. Eur J Vasc Endovasc Surg. 1997;14:305-309.
Morris GC, Heider CF, Moyer JH. The protective effect of subfiltration arterial pressure on the kidney. Surg Forum. 1956;6:623-627.
Mounayer C, Aymard A, Saint-Maurice JP, et al. Balloon-assisted coil embolization for large-necked renal artery aneurysms. Cardiovasc Intervent Radiol. 2000;23(3):228-230.
Muller FB, Sealey JE, Case DB, et al. The captopril test for identifying renovascular disease in hypertensive patients. Am J Med. 1986;80:633-644.
Murphy KJ, Rubin JM. Power Doppler: it’s a good thing. Semin Ultrasound CT MR. 1997;18:13-21.
Nally JV. Captopril renography. In: Novick AC, Scoble J, Hamilton G, editors. Renal vascular disease. London: WB Saunders; 1996:195-203.
Nally JVJr, Chen C, Fine E, et al. Diagnostic criteria of renovascular hypertension with captopril renography. A consensus statement. Am J Hypertens. 1991;4:749S-752S.
Nazzal MM, Hoballah JJ, Miller EV, et al. Renal hilar Doppler analysis is of value in the management of patients with renovascular disease. Am J Surg. 1997;174:164-168.
Neri E, Bonanomi G, Vignali C, et al. Spiral CT virtual endoscopy of abdominal arteries: clinical applications. Abdom Imaging. 2000;25:59-61.
Nicholson JP, Teichman SL, Alderman MH, et al. Cigarette smoking and renovascular hypertension. Lancet. 1983;2:765-766.
Novick AC. Renal arterial aneurysms and arteriovenous fistulas. In: Novick AC, Straffon RA, editors. Vascular problems in urologic surgery. Philadelphia: WB Saunders; 1982:189-204.
Novick AC. Atherosclerotic ischemic nephropathy. Epidemiology and clinical considerations. Urol Clin North Am. 1994;21:195-200.
Novick AC. Percutaneous transluminal angioplasty and surgery of the renal artery. Eur J Vasc Surg. 1994;8:1-9.
Novick AC, Scoble J, Hamilton G, editors. Renal vascular disease. London: WB Saunders, 1996.
Novick AC, Straffon RA, Stewart BH, et al. Diminished operative morbidity and mortality following revascularization for atherosclerotic renovascular disease. JAMA. 1981;246:749-753.
Novick AC, Textor SC, Bodie B, et al. Revascularization to preserve renal function in patients with atherosclerotic renovascular disease. Urol Clin North Am. 1984;11:477-490.
Novick AC, Zaki S, Goldfarb D, Hodge EE. Epidemiologic and clinical comparison of renal artery stenosis in black patients and white patients. J Vasc Surg. 1994;20:1-5.
Novick AC, Ziegelbaum M, Vidt DG, et al. Trends in surgical revascularization for renal artery disease: ten years’ experience. JAMA. 1987;257:498-501.
Nussberger J, Wuerzner G, Jensen C, Brunner HR. Angiotensin II suppression in humans by the orally active renin inhibitor Aliskiren (SPP100): comparison with enalapril. Hypertension. 2002;39:E1-E8.
Olin JW, Melia M, Young JR, et al. Prevalence of atherosclerotic renal artery stenosis in patients with atherosclerosis elsewhere. Am J Med. 1990;188:46-51.
Olin JW, Piedmonte MR, Young JR, et al. The utility of duplex ultrasound scanning of the renal arteries for diagnosing significant renal artery stenosis. Ann Intern Med. 1995;122:833-838.
Omary RA, Frayne R, Unal O, et al. Intraarterial gadolinium-enhanced 2D and 3D MR angiography: a preliminary study. J Vasc Interv Radiol. 1999;10:1315-1321.
Othersen JB, Maize JC, Woolson RF, Budisavljevic MN. Nephrogenic systemic fibrosis after exposure to gadolinium in patients with renal failure. Nephrol Dial Transplant. 2007 Nov;22(11):3179-3185.
Page IH. The production of persistent arterial hypertension by cellophane perinephritis. JAMA. 1939;113:2046-2048.
Page IH, Helmer OM. A crystalline pressor substance (angiotensin) resulting from the reaction between renin and renin activator. J Exp Med. 1940;71:29.
Pandey KN, Misono KS, Inagami T. Evidence for intracellular formation of angiotensins: coexistence of renin and angiotensin-converting enzyme in Leydig cells of rat testis. Biochem Biophys Res Commun. 1984;122:1337-1343.
Pannier-Moreau I, Grimbert P, Fiquet-Kempf B, et al. Possible familial origin of multifocal renal artery fibromuscular dysplasia. J Hypertens. 1997;15:1797-1801.
Pannu HK, Fishman EK. Multidetector computed tomographic evaluation of the renal artery. Abdom Imaging. 2002;27(6):611-619.
Papachristopoulos G, Bis KG, Shetty AN, et al. Breath-hold 3D MR angiography of the renal vasculature using a contrast-enhanced multiecho gradient-echo technique. Invest Radiol. 1999;34:731-738.
Paulsen D, Klow NE, Rogstad B, et al. Preservation of renal function by percutaneous transluminal angioplasty in ischaemic renal disease. Nephrol Dial Transplant. 1999;14:1454-1461.
Peach MJ, Bumpus FM, Khairallah PA. Release of adrenal catecholamines by angiotensin I. J Pharmacol Exp Ther. 1971;176:366-376.
Perkovic V, Thomson KR, Becker GJ. Factors affecting outcome after percutaneous renal artery stent insertion. J Nephrol. 2002;15(6):649-654.
Perkovic V, Thomson KR, Mitchell PJ, et al. Treatment of renovascular disease with percutaneous stent insertion: long-term outcomes. Australas Radiol. 2001;45(4):438-443.
Pershad A, Heuser R. Renal artery aneurysm: successful exclusion with a stent graft. Catheter Cardiovasc Interv. 2004;61(3):314-316.
Pfeiffer T, Reiher L, Grabitz K, et al. Reconstruction for renal artery aneurysm: operative techniques and long-term results. J Vasc Surg. 2003;37(2):293-300.
Picciotto G, Sargiotto A, Petrarulo M, et al. Reliability of captopril renography in patients under chronic therapy with angiotensin II (AT1) receptor antagonists. J Nucl Med. 2003;44(10):1574-1581.
Pickering SG, Pickering TG. Part I: Hypertension: definitions, natural histories and consequences. Part II: modern definitions and clinical expressions of hypertension. In: Laragh JH, Brenner BM, editors. Hypertension: pathophysiology, diagnosis, and management. 2nd ed. New York: Raven; 1995:3-21.
Pickering TG, Blumenfeld JD, Laragh JH. Renovascular hypertension and ischemic nephropathy. In: Brenner BM, editor. The kidney. 5th ed. Philadelphia: WB Saunders; 1996:2106-2125.
Pickering TG, Sos TA, Vaughan EDJr, et al. Predictive value and changes of renin secretion in hypertensive patients with unilateral renovascular disease undergoing successful renal angioplasty. Am J Med. 1984;76:398-404.
Pitts RF, Duggan JJ. Studies on diuretics. II. The relationship between glomerular filtration rate, proximal tubular absorption of sodium, and diuretic efficacy of mercurials. J Clin Invest. 1950;29:372.
Plouin PF, Darne B, Chatellier G, et al. Restenosis after a first percutaneous transluminal renal angioplasty. Hypertension. 1993;21:89-96.
Poutasse EF, Dustan HP. Arteriosclerosis and renal hypertension: indications for aortography in hypertensive patients and results of surgical treatment of obstructive lesions of renal artery. JAMA. 1957;165:1521.
Poutasse EF. Renal artery aneurysms. J Urol. 1975;113:443-449.
Prokop M. CT angiography of the abdominal arteries. Abdom Imaging. 1998;23:462-468.
Raynaud AC, Beyssen BM, Turmel-Rodrigues LE, et al. Renal artery stent placement: immediate and midterm technical and clinical results. J Vasc Interv Radiol. 1994;5:849-858.
Rees CR, Snead D. Results of United States multicenter trial of stents in renal arteries [abstract]. Cardiovasc Intervent Radiol. 1994;17(Suppl. 2):S1-S145.
Rees CR. Stents for atherosclerotic renovascular disease. J Vasc Interv Radiol. 1999;10:689-705.
Riehl J, Schmitt H, Bongartz D, et al. Renal artery stenosis: evaluation with color duplex ultrasonography. Nephrol Dial Transplant. 1997;12:1608-1614.
Rihal CS, Textor SC, Breen JF, et al. Incidental renal artery stenosis among a prospective cohort of hypertensive patients undergoing coronary angiography. Mayo Clin Proc. 2002;77(4):309-316.
Rodriguez-Lopez JA, Werner A, Ray LI, et al. Renal artery stenosis treated with stent deployment: indications, technique, and outcome for 108 patients. J Vasc Surg. 1999;29:617-624.
Rundback JH, Gray RJ, Rozenblit G, et al. Renal artery stent placement for the management of ischemic nephropathy. J Vasc Interv Radiol. 1998;9:413-420.
Rundback JH, Shah PM, Wong J, et al. Livedo reticularis, rhabdomyolysis, massive intestinal infarction, and death after carbon dioxide arteriography. J Vasc Surg. 1997;26:337-340.
Salmon P, Brown MA. Renal artery stenosis and peripheral vascular disease: implications for ACE inhibitor therapy. Lancet. 1990;336:321.
Savader SJ, Lund GB, Venbrux AC. Doppler flow wire evaluation of renal artery blood flow before and after PTA: initial results. J Vasc Interv Radiol. 1998;9:451-460.
Sawicki PT, Kaiser S, Heinenmann L, et al. Prevalence of renal artery stenosis in diabetes mellitus: an autopsy study. J Intern Med. 1991;229:489-492.
Schambelan M, Glickman M, Stockigt JR, Biglieri EG. Selective renal-vein renin sampling in hypertensive patients with segmental renal lesions. N Engl J Med. 1974;290:1153-1157.
Schefft P, Novick AC, Stewart BH, et al. Renal revascularization in patients with total occlusion of the renal artery. J Urol. 1980;124:184-186.
Schneidereit NP, Lee S, Morris DC, Chen JC. Endovascular repair of a ruptured renal artery aneurysm. J Endovasc Ther. 2003;10(1):71-74.
Schoenbaum SG, Goldman MA, Siegelman SS. Renal arterial embolization. Angiology. 1971;22:332-343.
Schreiber MJJr, Novick AC, Pohl MA. The natural history of atherosclerotic and fibrous renal artery disease. World J Urol. 1989;7:59.
Schreiber MJ, Pohl MA, Novick AC. The natural history of atherosclerotic and fibrous renal artery disease. Urol Clin North Am. 1984;11:383-392.
Schreier DZ, Weaver FA, Frankhouse J, et al. A prospective study of carbon dioxide-digital subtraction vs standard contrast arteriography in the evaluation of the renal arteries. Arch Surg. 1996;131:503-507. discussion 507–508
Scoble JE, Maher ER, Hamilton G, et al. Atherosclerotic renovascular disease causing impairment: a case for treatment. Clin Nephrol. 1989;31:119-122.
Sealey JE, Buhler FR, Laragh JH, Vaughan EDJr. Renovascular hypertension: renin measurements to indicate hypersecretion and contralateral suppression, estimate renal plasma flow, and score for surgical curability. Am J Med. 1973;55:402-414.
Sealey JE, Moon C, Laragh JH, Atlas SA. Plasma prorenin in normal, hypertensive, and anephric subjects and its effect on renin measurements. Circ Res. 1977;40(Suppl. 1):I41-I45.
Seikaly MG, Arant BSJr, Seney FDJr. Endogenous angiotensin concentrations in specific intrarenal fluid compartments of the rat. J Clin Invest. 1990;86:1352-1357.
Setaro JF, Saddler MC, Chen CC, et al. Simplified captopril renography in diagnosis and treatment of renal artery stenosis. Hypertension. 1991;18:289-298.
Sfakianakis GN, Sfakianakis ED. Nuclear medicine in pediatric urology and nephrology. J Nucl Med. 1988;29:1287-1300.
Shannon HM, Gillespie IN, Moss JG. Salvage of the solitary kidney by insertion of a renal artery stent. AJR Am J Roentgenol. 1998;171:217-222.
Sharma S, Gupta H, Saxena A, et al. Results of renal angioplasty in nonspecific aortoarteritis (Takayasu disease). J Vasc Interv Radiol. 1998;9:429-435.
Sharma S, Thatai D, Saxena A, et al. Renovascular hypertension resulting from nonspecific aortoarteritis in children: midterm results of percutaneous transluminal renal angioplasty and predictors of restenosis. AJR Am J Roentgenol. 1996;166:157-162.
Siemons L, van den Heuvel P, Parizel G, et al. Peritoneal dialysis in acute renal failure due to cholesterol embolization: two cases of recovery of renal function and extended survival. Clin Nephrol. 1987;28:205-208.
Silver D, Clements JB. Renovascular hypertension from renal artery compression by congenital bands. Ann Surg. 1976;183:161-166.
Simon G, Coleman CC. Captopril-stimulated renal vein renin measurements in the diagnosis of atherosclerotic renovascular hypertension. Am J Hypertens. 1994;7:1-6.
Simon N, Franklin SS, Bleifer KH, Maxwell MH. Clinical characteristics of renovascular hypertension. JAMA. 1972;220:1209-1218.
Simunic S, Winter-Fuduric I, Radanovic B, et al. Percutaneous transluminal renal angioplasty (PTRA) as a method of therapy for renovascular hypertension in children. Eur J Radiol. 1990;10:143-146.
Sivamurthy N, Surowiec SM, Culakova E, et al. Divergent outcomes after percutaneous therapy for symptomatic renal artery stenosis. J Vasc Surg. 2004;39(3):565-574.
Skeggs LT, Marsh WH, Kahn JR, Shumway NP. The existence of two forms of hypertension. J Exp Med. 1954;99:275.
Smallridge RC, Rogers J, Verma PS. Serum angiotensin-converting enzyme. Alterations in hyperthyroidism, hypothyroidism, and subacute thyroiditis. JAMA. 1983;250:2489-2493.
Smith CW, Winfield AC, Price RR, et al. Evaluation of digital venous angiography for the diagnosis of renovascular hypertension. Radiology. 1982;144:51-54.
Smith HW. Hypertension and urologic disease. Am J Med. 1948;4:724.
Smith P, Rush TW, Evans AT. The technique of translumbar arteriography. JAMA. 1952;148:255.
Sos TA, Pickering TG, Sniderman K, et al. Percutaneous transluminal renal angioplasty in renovascular hypertension due to atheroma or fibromuscular dysplasia. N Engl J Med. 1983;309:274-279.
Spinosa DJ, Matsumoto AH, Angle JF, et al. Renal insufficiency: usefulness of gadodiamide-enhanced renal angiography to supplement CO2-enhanced renal angiography for diagnosis and percutaneous treatment. Radiology. 1999;210:663-672.
Stanley JC, Whitehouse WM, Zelenock GB, et al. Reoperation from complications of renal artery reconstructive surgery undertaken for treatment of renovascular hypertension. J Vasc Surg. 1985;2:133-142.
Steinbach F, Novick AC, Campbell S, Dykstra D. Long-term survival after surgical revascularization for atherosclerotic renal artery disease. J Urol. 1997;158:38-41.
Stewart BH, Dustan HP, Kiser WS, et al. Correlation of angiography and natural history in evaluation of patients with renovascular hypertension. J Urol. 1970;104:231-238.
Stoll M, Meffert S, Stroth U, Unger T. Growth or antigrowth: angiotensin and the endothelium. J Hypertens. 1995;13:1529-1534.
Strandness DEJr. Duplex imaging for the detection of renal artery stenosis. Am J Kidney Dis. 1994;24:674-678.
Strittmatter SM, Snyder SH. Angiotensin converting enzyme immunohistochemistry in rat brain and pituitary gland: correlation of isozyme type with cellular localization. Neuroscience. 1987;21:407-420.
Studdy PR, Lapworth R, Bird R. Angiotensin-converting enzyme and its clinical significance—a review. J Clin Pathol. 1983;36:938-947.
Suffrin G. The Page kidney: a correctable form of arterial hypertension. J Urol. 1975;113:450-454.
Svetkey LP, Himmelstein SI, Dunnick NR, et al. Prospective analysis of strategies for diagnosing renovascular hypertension. Hypertension. 1989;14:247-257.
Swartbol P, Thorvinger BOT, Parsson H, et al. Renal artery stenosis in patients with peripheral vascular disease and its correlation to hypertension: a retrospective study. Int Angiol. 1992;11:195-199.
Sweet CS, Kadowitz PJ, Brody MJ. Arterial hypertension elicited by prolonged intra-vertebral infusion of angiotensin II in conscious dog. Am J Physiol. 1971;221:1640-1644.
Tan WA, Chough S, Saito J, Wholey MH, Eles G. Covered stent for renal artery aneurysm. Catheter Cardiovasc Interv. 2001;52(1):106-109.
Taylor ATJr, Fletcher JW, Nally JVJr, et al. Procedure guideline for diagnosis of renovascular hypertension. Society of Nuclear Medicine. J Nucl Med. 1998;39:1297-1302.
Tegtmeyer CJ, Dyer R, Teates CD, et al. Percutaneous transluminal dilatation of the renal arteries: techniques and results. Radiology. 1980;135:589-599.
Tegtmeyer CJ, Kellum CD, Ayers C. Percutaneous transluminal angioplasty of the renal artery. Results and long-term follow-up. Radiology. 1984;153:77-84.
Tegtmeyer CJ, Selby JB, Hartwell GD, et al. Results and complications of angioplasty in fibromuscular disease. Circulation. 1991;83(Suppl. 2):I155-I161.
Tewksbury DA, Dart RA. High molecular weight angiotensinogen levels in hypertensive pregnant women. Hypertension. 1982;4:729-734.
Textor SC. Pathophysiology of renal failure in renovascular disease. Am J Kidney Dis. 1994;24:642-651.
Textor SC. Pathophysiology of renal failure in ischemic renal disease. In: Novick AC, Scoble J, Hamilton G, editors. Renal vascular disease. London: WB Saunders; 1996:289-302.
Textor SC, Novick AC, Steinmuller D, Streem S. Renal function limiting antihypertensive therapy as an indication for renal revascularization. Arch Intern Med. 1983;143:2208-2211.
Thornton J, O’Callaghan J, Walshe J, et al. Comparison of digital subtraction angiography with gadolinium-enhanced magnetic resonance angiography in the diagnosis of renal artery stenosis. Eur Radiol. 1999;9:930-934.
Tigerstedt R, Bergemann TG. Niere und Kreislauf. Scand Arch Physiol. 1898;8:233.
Tilford D, Kelsch RC. Renal artery stenosis in childhood neurofibromatosis. Am J Dis Child. 1973;126:665-668.
Timmermans PB, Benfield P, Chiu AT, et al. Angiotensin II receptors and functional correlates. Am J Hypertens. 1992;5:221S-235S.
Tobian L, Tomboulian A, Janecek J. The effect of high perfusion pressure on the granulation of juxtaglomerular cells in an isolated kidney. J Clin Invest. 1959;38:605.
Tollefson DE, Ernst CB. Natural history of atherosclerotic renal artery stenosis associated with aortic disease. J Vasc Surg. 1991;14:327-331.
Traube L. Uhber den Zusammenhang von Herz- und Nieren-Krankheiten. In: Gesammelte Beitraege zur Pathologic und Physiologic, vol II, part I. Clinical Investigations. Berlin: A Hirschwalt; 1856.
Tshomba Y, Deleo G, Ferrari S, et al. Renal artery aneurysm: improved renal function after coil embolization. J Endovasc Ther. 2002;9(1):54-58.
Tsoukas AI, Hertzer NR, Mascha EJ, et al. Simultaneous aortic replacement and renal artery revascularization: the influence of preoperative renal function on early risk and late outcome. J Vasc Surg. 2001;34(6):1041-1049.
Tuttle KR, Chouinard RF, Webber JT, et al. Treatment of atherosclerotic ostial renal artery stenosis with the intravascular stent. Am J Kidney Dis. 1998;32:611-622.
Tyagi S, Kaul UA, Satsangi DK, Arora R. Percutaneous transluminal angioplasty for renovascular hypertension in children: initial and long-term results. Pediatrics. 1997;99:44-49.
Tynes WV, Devine CJJr, Devine PC, et al. Surgical treatment of renal arteriovenous fistulas: report of five cases. J Urol. 1970;103:692-698.
Ugur O, Serdengecti M, Karacalioglu O, et al. Comparison of Tc-99m EC and Tc-99m DTPA captopril scintigraphy to diagnose renal artery stenosis. Clin Nucl Med. 1999;24:553-560.
Unger T, Badoer E, Ganten D, et al. Brain angiotensin: pathways and pharmacology. Circulation. 1988;77:I40-I54.
Uzu T, Takeji M, Yamada N, et al. Prevalence and outcome of renal artery stenosis in atherosclerotic patients with renal dysfunction. Hypertens Res. 2002;25(4):537-542.
Valentine RJ, Myers SI, Miller GL, et al. Detection of unsuspected renal artery stenosis in patients with abdominal aortic aneurysms: refined indications for preoperative aortography. Ann Vasc Surg. 1993;7:220-224.
van Ampting JM, Penne EL, Beek FJ, et al. Prevalence of atherosclerotic renal artery stenosis in patients starting dialysis. Nephrol Dial Transplant. 2003;18(6):1147-1151.
Van Bockel JH, Van Schilfgaarde R, Felthuis W, et al. Surgical treatment of renovascular hypertension caused by arteriosclerosis: influence of preoperative factors on blood pressure control early and late after reconstructive surgery. Surgery. 1987;101:698-705.
Van de Ven PJ, Beutler JJ, Kaatee R, et al. Transluminal vascular stent for ostial atherosclerotic renal artery stenosis. Lancet. 1995;346:672-674.
Van de Ven PJ, Kaatee R, Beutler JJ, et al. Arterial stenting and balloon angioplasty in ostial atherosclerotic renovascular disease: a randomized trial. Lancet. 1999;353:282-286.
Van der Hulst VP, van Baalen J, Kool LS, et al. Renal artery stenosis: endovascular flow wire study for validation of Doppler US. Radiology. 1996;200:165-168.
Van Hoe L, De Jaegere T, Bosmans H, et al. Breath-hold contrast-enhanced three-dimensional MR angiography of the abdomen: time-resolved imaging versus single-phase imaging. Radiology. 2000;214:149-156.
van Jaarsveld BC, Krijnen P, Pieterman H, et al. The effect of balloon angioplasty on hypertension in atherosclerotic renal-artery stenosis. Dutch Renal Artery Stenosis Intervention Cooperative Study Group. N Engl J Med. 2000;342:1007-1014.
Vaughan EDJr, Buhler FR, Laragh JH, et al. Renovascular hypertension: renin measurements to indicate hypersecretion and contralateral suppression, estimate renal plasma flow, and score for surgical curability. Am J Med. 1973;55:402-414.
Vetrovec GW, Landwehr DM, Edwards VL. Incidence of renal artery stenosis in hypertensive patients undergoing coronary angiography. J Interv Cardiol. 1989;2:69-76.
Vidt DG, Eisle G, Gephardt GN, et al. Atheroembolic renal disease: association with renal arterial stenosis. Cleve Clin J Med. 1989;56:407-413.
Von Knorring J, Edgren J, Lepantalo M. Long-term results of percutaneous transluminal angioplasty in renovascular hypertension. Acta Radiol. 1996;37:36-40.
Wasser WG, Krakoff LR, Haimov M, et al. Restoration of renal function after bilateral renal artery occlusion. Arch Intern Med. 1981;141:1647-1651.
Weibull H, Bergqvist D, Bergentz SE, et al. Percutaneous transluminal renal angioplasty versus surgical reconstruction of atherosclerotic renal artery stenosis: a prospective randomized study. J Vasc Surg. 1993;18:841-850. discussion 850–852
White CJ, Ramee SR, Collins TJ, et al. Renal artery stent placement: utility in lesions difficult to treat with balloon angioplasty. J Am Coll Cardiol. 1997;30:1445-1450.
Whorton AR, Lazar JD, Smigel MD, Oates JA. Prostaglandin-mediated renin release from renal cortical slices. Adv Prostaglandin Thromboxane Res. 1980;7:1123-1129.
Willmann JK, Wildermuth S, Pfammatter T, et al. Aortoiliac and renal arteries: prospective intraindividual comparison of contrast-enhanced three-dimensional MR angiography and multi-detector row CT angiography. Radiology. 2003;226(3):798-811.
Wilms G, Marchal G, Penne P, et al. The angiographic incidence of renal artery stenosis in the atherosclerotic population. Eur J Radiol. 1990;10:195-197.
Wilms GE, Baert AL, Staessen JA, Amery AK. Renal artery stenosis: evaluation with intravenous digital subtraction angiography. Radiology. 1986;160:713-715.
Wilms GE, Peene PT, Baert AL, et al. Renal artery stent placement with use of the Wallstent endoprosthesis. Radiology. 1991;179:457-462.
Wittenberg G, Kenn W, Tschammler A, et al. Spiral CT angiography of renal arteries: comparison with angiography. Eur Radiol. 1999;9:546-551.
Wollenweber J, Sheps SG, Davis DG. Clinical course of atherosclerotic renovascular disease. Am J Cardiol. 1968;21:60-71.
Wyszyńūska T, Cichocka E, Wieteska-Klimczak A, et al. A single pediatric center experience with 1025 children with hypertension. Acta Paediatr. 1992;81:244-246.
Yotsumoto H, Sato S, Shibuya M. Localization of angiotensin converting enzyme (dipeptidyl carboxypeptidase) in swine sperm by immunofluorescence. Life Sci. 1984;35:1257-1261.
Zähringer M, Sapoval M, Pattynama PM, et al. Sirolimus-eluting versus bare-metal low-profile stent for renal artery treatment (GREAT Trial): angiographic follow-up after 6 months and clinical outcome up to 2 years. J Endovasc Ther. 2007;14:460-468.
Zeller T, Frank U, Muller C, et al. Predictors of improved renal function after percutaneous stent-supported angioplasty of severe atherosclerotic ostial renal artery stenosis. Circulation. 2003;108(18):2244-2249.
Zeller T, Frank U, Muller C, et al. Stent-supported angioplasty of severe atherosclerotic renal artery stenosis preserves renal function and improves blood pressure control: long-term results from a prospective registry of 456 lesions. J Endovasc Ther. 2004;11(2):95-106.
Zierler RE, Bergelin RO, Isaacson JA, Strandness DEJr. Natural history of atherosclerotic renal artery stenosis: a prospective study with duplex ultrasonography. J Vasc Surg. 1994;19:250-257.
Zimbler MS, Pickering TG, Sos TA, Laragh JH. Proteinuria in renovascular hypertension and the effects of renal angioplasty. Am J Cardiol. 1987;59:406-408.
Zinman L, Libertino JA. Revascularization of the chronic totally occluded renal artery with restoration of renal function. J Urol. 1977;118:517-521.
Zuccala A, Losinno F, Gaggi R, Zucchelli P. Late improvement of renal function in patients treated by percutaneous transluminal renal angioplasty. Contrib Nephrol. 1996;119:74-77.
Zuccala A, Losinno F, Zucchelli A, Zucchelli PC. Renovascular disease in diabetes mellitus: treatment by percutaneous transluminal renal angioplasty. Nephrol Dial Transplant. 1998;13(Suppl. 8):26-29.
Zucchelli P, Chiarini C, Zuccala A, et al. Renal ischemia is the real problem in renovascular hypertension. In: Glorioso N, editor. Renovascular hypertension. New York: Raven; 1987:273-278.