Ureteroenteric Anastomotic Stricture
Incidence and Etiology
Several factors determine the incidence of stricture formation at the anastomosis of the ureter and intestine at the time of urinary diversion. The longest follow-up data available are for urinary conduits, in which the stricture rate is between 4% and 8% and more common on the left (Schmidt et al, 1973; Skinner et al, 1980). Factors potentially influencing outcome in this population include the technique used for ureteral dissection, the segment of bowel used for the diversion, and the type of anastomosis performed. Because ureteral ischemia is central to the etiology of ureteroenteric strictures, careful attention to dissection is necessary to prevent complications. The ureteral blood supply runs parallel to the ureter in the adventitia. Although ureteral mobilization is necessary to approximate the ureter and bowel and prevent tension on the anastomosis, stripping the ureter of its surrounding adventitia can lead to distal ureteral ischemia and stricture formation. When performing an ileal conduit, the left ureter is brought underneath the sigmoid mesentery just overlying the aorta. The additional length and dissection needed on the left and the possibility of angulation around the inferior mesenteric artery may lead to a higher incidence of stricture formation on the left (Mansson et al, 1989).
Much controversy exists over the choice of bowel segment employed for conduit diversion. One theoretic advantage to the use of colon is the feasibility of performing a nonrefluxing anastomosis. However, the reported incidence of renal deterioration with a nonrefluxing versus a refluxing ureterocolonic anastomosis has been mixed, and there does not appear to be a clear advantage with respect to renal function and colonization to a nonrefluxing anastomosis. The issues influencing stricture formation in continent urinary diversions become even more complex owing to the variety of bowel segments, reservoir configurations, and types of anastomoses available for reconstruction. The reported rate of ureteroenteric anastomotic stricture after continent diversion is 3% to 25%, with the majority presenting within the first 2 years (Lugagne et al, 1997; Weijerman et al, 1998; Kouba et al, 2007). Despite the paucity of randomized studies, there is a growing body of evidence in the literature that the risk of obstruction with a nonrefluxing anastomosis is significantly higher than that of a refluxing anastomosis. Pantuck and colleagues (2000) compared 60 nonrefluxing ureteroenteric anastomoses with 56 direct, refluxing anastomoses and found the long-term stricture rate to be 13% and 1.7%, respectively. With a mean follow-up of 41 months, there was no significant difference in the two groups with respect to hydronephrosis, pyelonephritis, nephrolithiasis, or renal insufficiency. Similarly, Roth and colleagues (1996) found a greater than fivefold increase in ureteral strictures in the group undergoing a nonrefluxing anastomosis. Their data also indicated that the risk of obstruction was unrelated to surgical expertise.
Studer and colleagues (1995) have reported a randomized study evaluating a nonrefluxing versus a refluxing anastomosis into an isoperistaltic afferent ileal limb. Thirteen percent of nonrefluxing anastomoses resulted in stricture formation, as compared with 3% of refluxing anastomoses. Although there is no clear evidence that reflux into an adult kidney is detrimental, it is clear that obstruction is quite harmful to renal function. These studies and others support the use of a refluxing anastomosis in low-pressure continent reservoirs.
Kouba and colleagues compared the Wallace and Bricker technique of ureteroileal anastomosis for continent and incontinent diversions and found low rates of stricture (0% to 3%) using both techniques in 186 patients with 34-month follow-up. Notably, using the Wallace technique (joined ureters) no strictures were identified compared with 3.7% in patients undergoing Bricker techniques (separate ureters). Of note, the group undergoing the Bricker anastomosis had a higher BMI than the Wallace group (Kouba et al, 2007).
Evaluation
A minimally invasive means of screening the upper tracts in patients who have undergone any type of urinary diversion is a renal ultrasound. In addition, patients with renal colic, recurrent urinary tract infection, or loss of renal function will require evaluation. In patients with hydronephrosis on ultrasound, an intravenous pyelogram and contrast study of the conduit or reservoir will provide information on the length and location of the stricture. If a stone or recurrent tumor is suggested, a CT scan or MRI may be helpful. Diuretic renography is indicated in patients with chronic hydronephrosis to assess differential renal function and confirm the presence of functional obstruction. If hydronephrosis is present but renal function is insufficient for intravenous urogram or renography, placement of a nephrostomy tube and performance of an antegrade nephrostogram is both diagnostic and therapeutic. This approach is also useful before endoscopic intervention and clarifies stricture length, which aids in surgical planning.
Indications for Intervention
Not all patients with urinary diversion and hydronephrosis require intervention. Most patients with a long-term urinary conduit will have an element of chronic hydronephrosis that is not secondary to obstruction. In this population, a decrease in renal function or loss of reflux on a routine loop-o-gram should prompt diuretic renography to quantitatively assess for functional obstruction. Indications for intervention in patients with diversions and hydronephrosis include pain, infection, and renal insufficiency associated with functional obstruction. Although recurrence of transitional cell carcinoma at the level of the anastomosis is uncommon, the radiographic picture of an irregular mass at the level of the stricture and the rapid progression of obstruction and loss of renal function should prompt further evaluation and intervention (Tsuji et al, 1996).
A particularly challenging subset of patients is those undergoing urinary diversion as part of a pelvic exenteration for gynecologic malignancy. Penalver and colleagues (1998) reported on 66 patients, 95% of who had undergone previous pelvic irradiation. Early and late complications at the ureteroenteric anastomosis were 22% and 10%, respectively. Eighty-five percent of their postoperative complications were managed successfully by conservative measures such as percutaneous nephrostomy.
Endourologic Management
Endourologic management of ureteroenteric strictures has evolved in a manner analogous to that for ureteral stricture disease. Although the initial procedures involved simple balloon dilatation and stent placement, unsatisfactory results led to incisional techniques using electrocautery and more recently the laser was applied using both fluoroscopic and direct endoscopic control. The current state-of-the-art incisional technique for endoureterotomy includes small-caliber flexible ureteroscopic instrumentation along with holmium laser incision (Siegel et al, 1982; Muench et al, 1987; Cornud et al, 1992; Delvecchio et al, 2000; Laven et al, 2001, 2003).
Endourologic management of ureteroenteric or ureterocolic strictures, unlike the management of ureteral strictures, still favors antegrade management. As such, endourologic procedures typically begin with antegrade percutaneous access. Simple percutaneous drainage is continued to allow relief of any associated infection or obstruction-related renal dysfunction. Once the patient is clinically stable, fluoroscopic control is used to pass a guidewire in an antegrade fashion across the anastomotic stricture, over which a balloon catheter can be positioned and inflated until the waist disappears. Stents are a routine part of endourologic management, and these are generally inserted in this same antegrade fashion. However, because of difficulty with mucus plugging of stents in this setting, many centers routinely use an internal/external stent, which can be easily flushed or changed over a wire. In addition, retrograde looposcopic access can be combined with percutaneous access and antegrade passage of a wire. With through-and-through control, the anastomosis can be visualized fluoroscopically or, preferably, with direct ureteroscopic, looposcopic, or trans-stomascopic visualization. Any number of procedures can then be used for the dilatation itself including balloon dilatation alone, electroincision with an electrode or hot wire cutting balloon, or holmium laser incision. In all cases, a stent is placed, usually for 4 to 8 weeks.
Balloon dilatation of ureteroenteric strictures was one of the first endourologic forms of management used, and fortunately long-term results are available. Notably, short-term reports using high-pressure balloon dilation have demonstrated success rates as high as 61% (Ravery et al, 1998). Alternatively, Shapiro and colleagues (1998) reported balloon dilatation for 37 benign ureteroenteric strictures in 29 patients. Only 6 (16%) were considered to have a successful result at least 1 year after interventional treatment, and repeat dilatations were often required to maintain ureteral patency. Similarly, Kwak and colleagues (1995) achieved an overall success rate of less than 30% at 9 months for patients undergoing antegrade balloon dilatation of ureteroenteric strictures. More recently, DiMarco and colleagues (2001) reported a 5% 3-year success rate in 52 balloon dilations of ureteroenteric anastomotic strictures.
Metallic stents have also been used for ureteroenteric anastomotic strictures, with acceptable short-term results. Overall, of 30 patients in the published literature, the reported patency rate is greater than 80% with 6- to 22-month follow-up (Kurzer and Leveillee, 2005). There is a higher incidence of encrustation and stone formation when using metallic stents for ureteroenteric anastomotic strictures, as well as the risk of tissue ingrowth and recurrent obstruction (Kurzer and Leveillee, 2005). This may explain the limited published data using this approach. This author analyzed published success rates with endoureterotomy and balloon dilation and identified success rates in the literature of 18% and 63%, respectfully.
Cautery wire balloon incision has also been reported in patients treated for ureteroenteric strictures (Lin et al, 1999). For benign strictures, a stent-free long-term patency was achieved in only 30% of patients. Meretyk and colleagues reviewed the long-term results of endourologic management of ureteroenteric anastomotic strictures at Washington University. In that study, 15 patients with 19 ureteroenteric strictures were followed for an average of 2.5 years. An antegrade approach was used most frequently and was usually combined with electroincision. A 57% long-term stent-free patency rate was achieved, even with follow-up longer than 2 years (Meretyk et al, 1991). Whereas long-term patency of most endoscopic procedures seems to be in the range of 50%, such approaches are still used preferentially as the initial intervention, reserving open operative management for those patients failing endourologic intervention (Kramolowsky et al, 1987, 1988).
Cornud and associates (1996) reported their long-term results with percutaneous electroincision of ureterointestinal anastomotic strictures and specifically compared the results of fluoroscopic and endoscopic guidance. Twenty-seven patients were followed for longer than 1 year after stent removal, and an overall patency rate of 71% was reported. These investigators found better results when direct endoscopic control was combined with fluoroscopic guidance, compared with fluoroscopic guidance alone. In that report, right common iliac artery damage was reported during electroincision in one patient who had the procedure performed under fluoroscopic guidance alone. As a result, direct visual approaches have been favored for the management of ureteroenteric or ureterocolic anastomotic strictures, and the holmium laser has proven to be an excellent incisional tool. Endoureterotomy is typically performed antegrade, and success rates ranging from 50% to 80% have been reported (Singal et al, 1997; Laven et al, 2001; Watterson et al, 2002). These reports suggest the left side is more resistant to management because as the majority of the failures occurred on the left side in one series (Laven et al, 2003). When considering endoscopic incision of a left ureteroenteric stricture, the risk of hemorrhage is a consideration because the sigmoid mesentery can be in close proximity. This, taken with the lower success rates of all endoscopic approaches on the left side, supports serious consideration to open repair when treating left ureteroenteric strictures. In spite of this, Lovaco and colleagues reported good success treating 25 ureteroenteric strictures with endoureterotomy by an intraluminal invagination technique, with 80% success at more than 50 months’ follow-up. Of note, this approach increases the distance between the incision site and surrounding vessels and viscera and does not favor left or right strictures (Lovaco et al, 2005).
Open Intervention
Open surgical management of ureterointestinal strictures is technically challenging and associated with a longer recovery than endoscopic options but is often necessary due to the low success rates of less invasive alternatives, in particular balloon dilatation (DiMarco et al, 2001). When undertaking open repair, it is optimal to sterilize the urine and prepare the bowel preoperatively. If a cutaneous stoma is present, it is prepared into the field and the conduit or reservoir drained with a Foley catheter during the procedure. Placement of a nephrostomy tube and ureteral stent is helpful. Through a midline incision, the conduit or reservoir is identified and preserved, the colon is reflected medially, and the proximal, dilated ureter is identified and traced down to the area of the previous anastomosis. Care is taken to preserve the adventitia and associated blood supply. If enough ureteral length is available, the ureter can be transected proximal to the stricture, spatulated, and anastomosed to a convenient area of the bowel. If the dissection is particularly difficult, there may be significant trauma to the conduit or reservoir, requiring major revision. In addition, insufficient ureteral length may require an additional segment of bowel to interpose between the ureter and the reservoir. The anastomosis is carried out over a 7-Fr stent, and a drain is left in situ. The stent remains for 4 to 6 weeks. Satisfactory long-term success rates have been reported with open repair, as high as 80% (Laven et al, 2003). As expected, strictures longer than 1 cm were more likely to recur and the left side had lower success rates (DiMarco et al, 2001; Laven et al, 2003). Major complications were encountered in 11% of cases in one series (DiMarco et al, 2001).
Key Points: Ureteroenteric Strictures
Retroperitoneal Fibrosis
Presentation and Etiology
Retroperitoneal fibrosis (RPF) is typically characterized by the presence of an inflammatory, fibrotic process in the retroperitoneum causing compression of the retroperitoneal structures including the ureters. RPF most commonly affects patients who are 40 to 60 years of age. However, more than 30 cases of RPF have been reported in patients younger than 18 years of age (Van Bommel, 2002). RPF cases have a male predominance, with a male-to-female ratio of 2 to 3 : 1. The true incidence is unknown but has been estimated to be 1 : 200,000 to 1 : 500,000 per year.
The retroperitoneal fibrotic mass generally centers around the distal aorta at L4-L5 and wraps around the ureters, leading to hydronephrosis via extrinsic compression on the ureters or interference with ureteral peristalsis (Lepor and Walsh, 1979; Koep and Zuidema, 1987). In most patients, the presenting symptom is pain in the lower back and/or flank. The pain, which is typically dull, noncolicky, and unchanged with posture, may radiate to the lower abdomen or groin. Furthermore, the pain is often relieved by aspirin rather than narcotics. Other symptoms include weight loss, anorexia, nausea, generalized malaise, fever, hypertension, and oliguria/anuria. The mass may compress the inferior vena cava, resulting in deep venous thrombosis and lower extremity edema (Rhee et al, 1994). The mass may extend proximally to the renal hilum and encase the renal vein, resulting in renal vein hypertension and subsequent gross hematuria (Powell et al, 2000). Aortic obstruction and involvement of the mediastinum, the biliary system, the mesentery, and the kidney itself are rare (Tripodi et al, 1998; Azuma et al, 1999; Dejaco et al, 1999; Klisnick et al, 1999). Distal extension to the bifurcation of the iliac vessels may occur, and extension to spermatic cord with scrotal involvement has been reported (Palmer and Rosenthal, 1999; Schulte-Baukloh et al, 1999). Duration of symptoms before diagnosis is usually 4 to 6 months, and approximately half of the patients present with fibrosis that has caused significant ureteral obstruction and symptoms secondary to uremia.
In approximately 70% of the cases, the disease is idiopathic. However, there is increasing evidence that idiopathic RPF may be an immune-mediated periaortitis. Ceroid, a complex polymer of oxidized lipids and protein found in atherosclerotic plaques, has been suggested as the antigen initiating the inflammatory response (Parums et al, 1991). Indeed, a higher incidence of aortic aneurysms has been identified in patients with RPF (Breems et al, 2000). RPF usually presents as an isolated disease entity, but it may present as part of multifocal fibrosclerosis, a rare syndrome characterized by fibrosis involving multiple organ systems. In such a scenario, the clinical presentation may include RPF, sclerosing mediastinitis, sclerosing cholangitis, orbital pseudotumor, and Riedel thyroiditis (Dehner and Coffin, 1998; Özgen and Cila, 2000). The pathogenesis of these disorders is unknown but appears to be autoimmune in nature.
Among the 30% of RPF patients that have an identifiable etiology, drugs such as methysergide (Sansert) and other ergot alkyloids are most commonly associated with RPF. β Blockers and phenacetin have also been implicated. The exact pathophysiology of drug-induced RPF remains unknown. Other causes of RPF include malignancies such as lymphoma, the most common malignancy in RPF cases, and multiple myeloma, carcinoid, pancreatic cancer, prostate cancer, and sarcoma (Webb and Dawson-Edwards, 1967; Usher et al, 1977). Radiotherapy for retroperitoneal malignancy is also known to produce a residual fibrotic mass leading to secondary ureteral obstruction. Abdominal aortic aneurysm may cause significant retroperitoneal inflammatory reaction, leading to fibrosis and ureteral obstruction. In addition, infectious etiologies such as tuberculosis, actinomyces, gonorrhea, or schistosomiasis have been suggested in the pathogenesis of RPF.
Association of retroperitoneal fibrosis with membranous glomerulonephritis has also been documented in the literature (Mercadal et al, 2000; Shirota et al, 2002). The exact etiology remains unclear, although the association has been speculated to be secondary to an unknown antigen triggering systemic immune response that leads to retroperitoneal fibrosis. Association of retroperitoneal fibrosis with ankylosing spondylitis and Wegner granulomatosis has also been reported, further suggesting an underlying immune etiology in some patients (Izzedine et al, 2002; LeBlanc et al, 2002).
Pathologically, the typical gross appearance of RPF is that of a smooth, flat, tan-colored, dense mass enveloping the surrounding retroperitoneal structures. It is also known to invade the ureter or psoas muscle. Histologically, the appearance of RPF is that of a nonspecific inflammatory process that varies with the stage of the disease. Early in the disease, affected tissue consists mainly of collagen bundles with capillary proliferation and inflammatory cells including lymphocytes, plasma cells, and fibroblasts. In the later stage, the mass becomes relatively acellular and avascular, consisting of sheets of hypocellular collagen. RPF secondary to malignancy is often histologically indistinguishable from idiopathic RPF, and it can be identified only on the basis of the demonstration of small islands of tumor cells within the fibrotic mass.
Evaluation
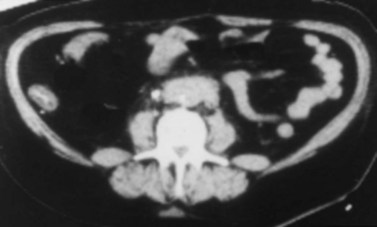
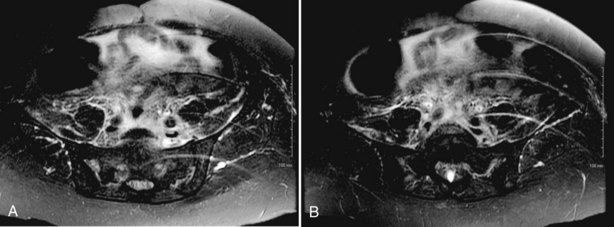
In most RPF patients, the clinical symptoms are generally nonspecific, and physical examination is usually unrevealing. Laboratory evaluation may reveal an elevated erythrocyte sedimentation rate, moderate leukocytosis, anemia, and variable renal insufficiency with associated electrolyte abnormalities. If the overall renal function is normal, an excretory urogram (EVU) or more commonly computed tomography (CT) with contrast may be performed. Typical EVU findings include hydronephrosis with medial deviation of the proximal ureter and midureter and a smoothly tapered ureter at the level of obstruction. Urinary obstruction is usually bilateral, but unilateral cases have been described. Uncommonly, there are patients with symptoms of urinary obstruction but little hydronephrosis on imaging. CT scan typically reveals hydronephrosis associated with a well-delineated retroperitoneal soft tissue mass enveloping the great vessels and the ureters (Fig. 41–36). If the patient has significant renal impairment, a retrograde pyelogram may be performed. In the radiographic evaluation of RPF, magnetic resonance imaging (MRI) can also be helpful because the mass itself has characteristic T1- and T2-weighted images. Retroperitoneal fibrosis is characterized as a diffusely low signal intensity on T1-weighted imaging, although the T2 signal may vary considerably, with high signal intensity consistent with active disease (Fig. 41–37A and B). With treatment, T2 signal often diminishes and thus provides a measure of therapeutic efficacy. Moreover, gadolinium enhancement may also prove valuable in assessing the response to treatment because associated decreases in gadolinium contrast enhancement should also be expected following appropriate therapy (Cronin et al, 2008). If a kidney is suspected to be nonfunctioning, differential renography should be considered to determine renal function because it may affect surgical planning. Representative biopsies of the mass should be obtained percutaneously or at the time of open or laparoscopic ureterolysis to rule out malignancy and allow one to proceed with treatment for RPF.
Management
Initial Management
The initial management of RPF depends on the patient’s clinical status. Patients with hydronephrosis and uremia should be emergently decompressed by either percutaneous nephrostomy or indwelling ureteral stents. The advantages to placing ureteral stents include the opportunity to perform retrograde pyelograms to evaluate the anatomy and the convenience of internal drainage. Interestingly, ureteral stent placement is usually not difficult to perform in the setting of ureteral obstruction due to RPF. In a critically ill patient with electrolyte abnormalities and little or no urine output, nephrostomy tube placement can be performed at the bedside with local anesthesia. Following renal decompression, the patient needs to be monitored closely for postobstructive diuresis, renal function status, and appropriate replacement of fluids and electrolytes.
Following the initial management described earlier, an attempt to search for the etiology of RPF should be made. Methysergide or any other potentially inciting drug, if identified, should be discontinued. Although most patients with malignant RPF have a prior history of malignancy, a thorough evaluation for occult malignancy with careful application of imaging studies is necessary. Biopsy to rule out malignancy, performed percutaneously or at the time of ureterolysis to provide long-term relief of obstruction, needs to be considered. However, some believe that in patients with classic radiographic features on MRI or CT, no lymphadenopathy, and no history of prior malignancy, a biopsy is not essential before medical therapy.
Medical Management
Once the diagnosis of idiopathic RPF is made, the most common primary medical management has been steroid therapy. Although there has been no large clinical series because the disease entity is uncommon, there are approximately 170 cases of idiopathic RPF treated with steroids that resulted in about an 80% clinical response in the medical literature including having a decrease in size of the mass and improvement in ureteral obstruction or inferior vena cava compression (Kearney et al, 1976; Baker et al, 1987; Adam et al, 1998; Higgins et al, 1998; Van Bommel, 2002; Fry et al, 2008). The characteristic clinical response to steroid therapy includes resolution of pain and constitutional symptoms within days after treatment, a rapid fall of erythrocyte sedimentation rate, and diuresis. Dose and duration of steroid therapy varied considerably in the literature, but most therapies were of 6 months or greater in duration. Chronic steroid therapy up to 2 years has been shown to provide significant improvement in clinical symptoms and regression of retroperitoneal mass in 1 recent report involving 12 patients (Kardar et al, 2002). Although steroids do not reverse the established fibrosis, further inflammatory reaction and fibrosis with their associated symptomatology and sequaelae may be minimized. Therefore it appears that patients who have the evidence of active inflammation—manifested by increased erythrocyte sedimentation rate, leukocytosis, or active inflammation on a biopsy—are more likely to respond to steroid therapy.
In addition to steroids, other agents have been described to provide benefit in idiopathic RPF in isolated case reports including azathioprine, cyclophosphamide, cyclosporine, colchicine, and mycophenolate mofetil (Wagenknecht et al, 1981; McDougal et al, 1991; Grotz et al, 1998; Marzano et al, 2001; Vega et al, 2009). Medroxyprogesterone acetate, progesterone, and particularly tamoxifen, a nonsteroidal antiestrogen, have been found to be beneficial in idiopathic RPF in several case reports (Clark et al, 1991; Benson et al, 1993; Al-Musawi et al, 1998; Dedeoglu et al, 2000; Puce et al 2000). The exact mechanisms of action of these medications are unclear, but they are believed to inhibit fibroblastic proliferation leading to clinical response. Use of alternative or additional agents may decrease or eliminate steroid usage.
Surgical Management: Open Ureterolysis
Ureterolysis may be performed open surgically or laparoscopically, although open surgery has been considered the standard (Lindell and Lehtonen, 1988; Elashry et al, 1996). It is performed with concomitant biopsy of the mass in patients with an unclear diagnosis as the definitive initial treatment or in those who fail medical therapy. When an open surgery is performed, a midline, transperitoneal abdominal incision is made to allow access to both ureters. Placement of ureteral catheters or stents before the abdominal incision is advisable to assist identification and dissection of the ureters. Although hydronephrosis may be unilateral on preoperative assessment, the process is generally bilateral requiring bilateral ureterolysis. Following medial mobilization of the ascending and descending colon, deep biopsies of the mass should be obtained for frozen and permanent section to rule out malignancy. Dissection should begin at the distal, nondilated ureteral segment to avoid injury to the thin, dilated proximal segment. A right-angle clamp can be placed between the ureter and the retroperitoneal mass along the course of the ureter, and the fibrotic tissue is then incised above the clamp. This is repeated throughout the length of the entrapped ureter, using both blunt and sharp dissection techniques to free the affected ureter from its fibrous bed. The ureteral wall may become quite thin at times following the dissection. An inadvertent ureterotomy should be closed with absorbable suture. Ureteral excision with ureteroureterostomy is usually unnecessary.
Following bilateral ureterolysis, the ureters should be repositioned and protected from further fibrous entrapment. Several surgical options are available. One option is to retract the ureters laterally and secure the overlying peritoneum medially to the psoas muscle to maintain the ureters in this location. Another option is to close the peritoneum behind the ureters so that the ureters may be displaced anteriorly into the peritoneal cavity (Tresidder et al, 1972). It is important not to obstruct the ureter in the closure of the peritoneum at the ureteral hiatus. In a report on a group of patients with idiopathic RPF undergoing intraperitoneal placement of the ureters or lateral retroperitoneal placement of the ureters, no difference in the radiologic or clinical outcome was found (Barbalias and Liatsikos, 1999). In the setting of extensive RPF, a more definitive approach is to surround the ureters with omentum and reposition them within the peritoneal cavity (Carini et al, 1982). To perform the omental wrap, the omentum is first mobilized from its attachment to the transverse colon, followed by its division along its midline with ligation of the small omental vessels up to the gastric attachment. The short gastric vessels are then divided and ligated at the level of the stomach wall, after which the two halves of the omentum can be retracted laterally on the basis of the right and left gastroepiploic arteries. The entire length of the ureter can be surrounded by omental tissue, which is tacked in place with absorbable sutures (Fig. 41–38A and B). The omentum provides protection of the ureter against recurrent extrinsic compression and vascularity to a potentially ischemic ureter. Steroid therapy may be used postoperatively in an attempt to prevent recurrent upper tract and venous compression. If no ureterotomy occurs during ureterolysis, the previously placed stents may be removed shortly after surgery.

Figure 41–38 A, Preoperative intravenous pyelogram (IVP) of a patient with idiopathic retroperitoneal fibrosis, showing bilateral hydronephrosis with medial deviation of the ureters. B, Postoperative IVP of the same patient following surgical ureterolysis with intraperitoneal omental wrapping.
If ureterolysis is impossible to perform due to extensive periureteral fibrosis, renal autotransplantation may be performed if the ipsilateral renal unit demonstrates satisfactory function (Penalver et al, 2001). If no significant renal function can be recovered after an adequate time period of decompression in the presence of the satisfactory contralateral renal function, nephrectomy may be considered.
Surgical Management: Laparoscopic Ureterolysis
The first laparoscopic ureterolysis was reported by Kavoussi and Clayman in 1992. Subsequent success with such technique was confirmed by others (Puppo et al, 1994). A more recent report described an experience with laparoscopic ureterolysis in 13 patients including bilateral procedure in 7 and unilateral procedure in 6 (Fugita et al, 2001). Preoperative stent placement was performed in all cases before laparoscopy. For each ureter, the laparoscopic procedure was performed using a transperitoneal four-port approach. Following incision of the posterior peritoneum and mobilization of the colon, the affected ureter was dissected free from the retroperitoneal fibrotic tissue. Multiple frozen-section biopsies of the periureteral tissue were obtained to rule out malignancy. The edge of the posterior peritoneum was reapproximated to the sidewall underneath the ureter to intraperitonealize the ureter. Laparoscopic ureterolysis was completed successfully in 85% (11) of the cases, with 2 (15%) open conversions due to iliac vein injury (in one patient) and marked fibrosis (in one patient). Mean operative time was 381 minutes for bilateral procedures and 192 minutes for unilateral procedures. Mean use of parenteral analgesics was 59 mg of morphine sulfate equivalent. Mean hospital stay was 4 days. Postoperative complications occurred in 30% (four) of the patients including epididymitis, umbilical port erythema, prolonged ileus, and urinary retention. Pathology showed fibrous tissue with lymphocytes, plasma cells, macrophages, and fibroblast proliferation in all cases. At a mean follow-up of 30 months, upper tract imaging such as intravenous urography or renal scan showed lack of obstruction in 92% (12) of the patients. A multi-institutional survey that included 17 academic centers identified that centers with a fellowship-trained laparoscopist performed laparoscopic ureterolysis, and in 59% of centers urologists performed the medical management. Notably in this survey the reported laparoscopic success rates were 83% (Duchene et al, 2007).
Key Points: Retroperitoneal Fibrosis
Anderson JC, Hynes W. Retrocaval ureter: a case diagnosed preoperatively and treated successfully by a plastic operation. Br J Urol. 1949;21:209.
Boxer RJ, Fritzsche P, Skinner DG, et al. Replacement of the ureter by small intestine: clinical application and results of the ileal ureter in 89 patients. J Urol. 1979;121:728.
Canes D, Berger A, Gettman MT, et al. Minimally invasive approaches to ureteropelvic junction obstruction. Urol Clin North Am. 2008;35:25.
Carini M, Selli C, Rizzo M, et al. Surgical treatment of retroperitoneal fibrosis with omentoplasty. Surgery. 1982;91:137.
Foley FEB. New plastic operation for stricture at the ureteropelvic junction. J Urol. 1937;38:643.
Inagaki T, Rha KH, Ong AM, et al. Laparoscopic pyeloplasty: current status. BJU Int. 2005;95(Suppl. 2):102.
Jarrett TW, Chan DY, Charambura TC, et al. Laparoscopic pyeloplasty: the first 100 cases. J Urol. 2002;167:1253.
Link RE, Bhayani SB, Kavoussi LR. A prospective comparison of robotic and laparoscopic pyeloplasty. Ann Surg. 2006;243:486.
Mufarrij PW, Woods M, Shah OD, et al. Robotic dismembered pyeloplasty: a 6-year, multi-institutional experience. J Urol. 2008;180:1391.
Ockerblad NF. Reimplantation of the ureter into the bladder by a flap method. J Urol. 1947;57:845.
Richstone L, Seideman CA, Reggio E, et al. Pathologic findings in patients with ureteropelvic junction obstruction and crossing vessels. Urology. 2009;73:716.
Turner-Warwick RT, Worth PHL. The psoas bladder-hitch procedure for the replacement of the lower third of the ureter. Br J Urol. 1969;41:701.
Adam U, Mack D, Forstner R, et al. Conservative treatment of acute Ormond’s disease. Tech Urol. 1998;5:54.
Ahn M, Loughlin KR. Psoas hitch ureteral reimplantation in adults—analysis of modified technique and timing of repair. Urology. 2001;58:184.
Al-Musawi P, Mitchenere P, Al-Akraa M. Idiopathic retroperitoneal fibrosis treated with tamoxifen only. Br J Urol. 1998;82:442.
Albani JM, Yost AJ, et al. Ureteropelvic junction obstruction: determining durability of endourological intervention. J Urol. 2004;171:579.
Allen TD. Congenital ureteral stricture. J Urol. 1970;104:196.
Anderson JC, Hynes W. Retrocaval ureter: a case diagnosed preoperatively and treated successfully by a plastic operation. Br J Urol. 1949;21:209.
Aslan P, Preminger GM. Retrograde balloon cautery incision of ureteropelvic junction obstruction. Urol Clin North Am. 1998;25:295.
Atug F, Woods M, Burgess SV, et al. Robotic assisted laparoscopic pyeloplasty in children. J Urol. 2005;174:1440.
Atug F, Castle EP, Burgess SV, et al. Concomitant management of renal calculi and pelvi-ureteric junction obstruction with robotic laparoscopic surgery. BJU Int. 2005;96:1365.
Austen M, Kalble T. Secondary malignancies in different forms of urinary diversion using isolated gut. J Urol. 2004;172:831.
Azuma T, Kato Y, Suetomi T, et al. Idiopathic retroperitoneal fibrosis presenting as duodenal obstruction. J Urol. 1999;162:1680.
Baba S, Oya M, Miyahara M, et al. Laparoscopic surgical correction of circumcaval ureter. Urology. 1994;44:122.
Bachmann A, Ruszat R, Forster T, et al. Retroperitoneoscopic pyeloplasty for ureteropelvic junction obstruction (UPJO): solving the technical difficulties. Eur Urol. 2006;49:264.
Badlani G, Eshghi M, Smith AD. Percutaneous surgery for ureteropelvic junction obstruction (endopyelotomy): technique and early results. J Urol. 1986;135:26.
Badlani G, Karlin G, Smith AD. Complications of endopyelotomy: analysis in series of 64 patients. J Urol. 1988;140:473.
Bagley DH, Huffman J, Lyon E, et al. Endoscopic ureteropyelostomy: opening the obliterated ureteropelvic junction with nephroscopy and flexible ureteropyeloscopy. J Urol. 1985;133:462.
Baker LR, Mallinson WJ, Gregory MC, et al. Idiopathic retroperitoneal fibrosis. A retrospective analysis of 60 cases. Br J Urol. 1987;60:497.
Banner MP, Pollack HW. Dilatation of ureteral stenosis: techniques and experience in 44 patients. AJR Am J Roentgenol. 1984;143:789.
Banner MP, Pollack HM, Ring EJ, et al. Catheter dilatation of benign ureteral strictures. Radiology. 1983;147:427.
Barbalias GA, Liatsikos EN. Idiopathic retroperitoneal fibrosis revisited. Int Urol Nephrol. 1999;31:423.
Bauer JJ, Bishoff JT, Moore RG, et al. Laparoscopic versus open pyeloplasty: assessment of objective and subjective outcome. J Urol. 1999;162:692.
Beaghler MA, Taylor FC, et al. A combined antegrade and retrograde technique for reestablishing ureteral continuity. Tech Urol. 1997;3:44.
Bejjani B, Belman AB. Ureteropelvic junction obstruction in newborns and infants. J Urol. 1982;128:770.
Bellman GC. Complications of endopyelotomy. J Endourol. 1996;10:177.
Benson JR, Baum M. Tamoxifen for retroperitoneal fibrosis. Lancet. 1993;341:836.
Benson MC, Ring KS, Olsson CA. Ureteral reconstruction and bypass: Experience with ileal interposition, the Boari flap—psoas hitch and renal autotransplantation. J Urol. 1990;143:20.
Berger RM, Lebowitz JM, Carroll PA. Ureteral polyps presenting as ureteropelvic junction obstruction in children. J Urol. 1982;128:805.
Bernstein GT, Mandell J, Lebowits RL, et al. Ureteropelvic junction obstruction in the neonate. J Urol. 1988;140:1216.
Berzeg S, Baumgart E, Beyersdorff D, et al. Late complication of Boari bladder flap. Eur Radiol. 2003;13:1604.
Biyani CS, Cornford PA, Powell CS. Retrograde endoureteropyelotomy with the holmium:YAG laser. Initial experience. Eur Urol. 1997;32:471.
Blueblond-Langner R, Rha KH, Pinto PA, et al. Laparoscopic-assisted renal autotransplantation. Urology. 2004;63:853.
Bodie B, Novick AC, Rose M, et al. Long-term results with renal autotransplantation for ureteral replacement. J Urol. 1986;136:1187.
Bonfig R, Gerharz EW, Riedmiller H. Ileal ureteric replacement in complex reconstruction of the urinary tract. BJU Int. 2004;93:575.
Borin JF, Melamud O, Clayman RV. Initial experience with full length metal stent to relieve malignant ureteral obstruction. J Endourol. 2006;20:300.
Bovie P, Ong AM, Rha K, et al. Laparoscopic management of ureteropelvic junction obstruction in patients with upper urinary tract anomalies. J Urol. 2004;171:77.
Boxer RJ, Fritzsche P, Skinner DG, et al. Replacement of the ureter by small intestine: clinical application and results of the ileal ureter in 89 patients. J Urol. 1979;121:728.
Boylu U, Oommen M, Lee BR, et al. Ureteropelvic junction obstruction secondary to crossing vessels—to transpose or not? The robotic experience. J Urol. 2009;181:1751.
Brannen GE, Bush WH, Lewis GP. Endopyelotomy for primary repair of ureteropelvic junction obstruction. J Urol. 1988;139:29.
Brannan W. Useful applications of transureteroureterostomy in adults and children. J Urol. 1975;113:460.
Breems DA, Haye H, van der Meulen J. The role of advanced atherosclerosis in idiopathic retroperitoneal fibrosis. Neth J Med. 2000;56:38.
Brooks JD, Kavoussi LR, Preminger GM, et al. Comparison of open and endourologic approaches to the obstructed ureteropelvic junction. Urology. 1995;46:791.
Butani RP, Eschghi M. Cold knife retrograde endopyelotomy: a long term follow-up. J Endourol. 2008;22:657.
Calvert RC, Morsy MM, Zelhof B, et al. Comparison of laparoscopic and open pyeloplasty in 100 patients with pelvi-ureteric junction obstruction. Surg Endosc. 2008;22:411.
Canes D, Berger A, Gettman MT, et al. Minimally invasive approaches to ureteropelvic junction obstruction. Urol Clin North Am. 2008;35:25.
Cardella JF, Hunter DW, Castaneda-Zuniga WR, et al. Electrolysis for recanalization of urinary collecting system obstructions: a percutaneous approach. Radiology. 1985;155:87.
Carini M, Selli C, Rizzo M, et al. Surgical treatment of retroperitoneal fibrosis with omentoplasty. Surgery. 1982;91:137.
Carlton CEJr, Guthrie AG, Scott RJr. Surgical correction of ureteral injury. J Trauma. 1969;9:457.
Casale P, Mucksavage P, Resnick M, et al. Robotic ureterocalicostomy in the pediatric population. J Urol. 2008;180:2643.
Cassis AN, Brannen GE, Bush WH, et al. Endopyelotomy: review of results and complications. J Urol. 1991;146:1492.
Castle EP, Nunez R, Desai PJ, et al. Ureteroarterial fistula following laser endopyelotomy. J Urol. 2009;181:1343.
Chandhoke PS, Clayman RV, Stone AM, et al. Endopyelotomy and endoureterotomy with the Acucise ureteral cutting balloon device: preliminary experience. J Endourol. 1993;7:45.
Chang R, Marshall FF, Mitchell S. Percutaneous management of benign ureteral strictures and fistulas. J Urol. 1987;137:1126.
Chiou YY, Shieh CC, et al. Intrinsic expression of Th2 cytokines in urothelium of congenital ureteropelvic junction obstruction. Kidney Int. 2005;67:638.
Chuang CK, Chu SH, Liao SK. Renal autotransplantation for ureter stricture and renovascular disorders. Chang Keng I Hsueh Tsa Chih. 1999;22:621.
Chung SY, Stein RJ, et al. 15-year experience with the management of extrinsic ureteral obstruction with indwelling ureteral stents. J Urol. 2004;172:592.
Clark CP, Vanderpool D, Preskitt JT. The response of retroperitoneal fibrosis to tamoxifen. Surgery. 1991;109:502.
Clark WR, Malek RS. Ureteropelvic junction obstruction: observations on the classic type I adults. J Urol. 1987;138:276.
Clayman RV, Basler JW, Kavoussi L, et al. Ureteronephroscopic endopyelotomy. J Urol. 1990;144:246.
Cohen TD, Gross MB, Preminger GM. Long-term follow-up of Acucise incision of ureteropelvic junction obstruction and ureteral strictures. Urology. 1996;47:317.
Conlin MJ, Bagley DH. Ureteroscopic endopyelotomy at a single setting. J Urol. 1998;159:727.
Conlin MJ, Gomella LG, Bagley DH. Endoscopic ureteroureterostomy for obliterated ureteral segments. J Urol. 1996;156:1394.
Conlin MJ. Results of selective management of ureteropelvic junction obstruction. J Endourol. 2002;16:233.
Considine J. Retrocaval ureter. Br J Urol. 1966;38:412.
Cornud F, Lefebvre JF, Chretien Y, et al. Percutaneous transrenal electro-incisions of ureterointestinal anastomotic strictures: long-term results and comparison of fluoroscopic and endoscopic guidance. J Urol. 1996;155:1575.
Cornud F, Mendelsberg M, Chretien Y, et al. Fluoroscopically guided percutaneous transrenal electro-incision of ureterointestinal anastomotic strictures. J Urol. 1992;147:578.
Couvelaire R, Auvert J, Moulonguet A. Implantations et anastomoses ureterocalicielles: Techniques et indications. J Urol Nephrol. 1964;70:437.
Cronin CG, Lohan DG, Blake MA, et al. Retroperitoneal fibrosis: a review of clinical features and imaging findings. AJR. 2008;191:423.
Culp OS, DeWeerd JH. A pelvic flap operation for certain types of ureteropelvic obstruction: preliminary report. Mayo Clin Proc. 1951;26:483.
Dalrymple NC, Verga M, Anderson KR, et al. The value of unenhanced helical computerized tomography in the management of acute flank pain. J Urol. 1998;159:735.
Danuser H, Ackermann DK, Bohlen D, et al. Endopyelotomy for primary ureteropelvic junction obstruction: risk factors determine the success rate. J Urol. 1998;159:56.
Danuser H, Hochreiter WW, et al. Influence of stent size on the success of antegrade endopyelotomy for primary ureteropelvic junction obstruction: results of 2 consecutive series. J Urol. 2001;166:902.
Das S, Amar AD. Ureteropelvic junction obstruction with associated renal anomalies. J Urol. 1984;131:872.
Davis DM. Intubated ureterostomy: a new operation for ureteral and ureteropelvic strictures. Surg Gynecol Obstet. 1943;76:513.
Dedeoglu F, Rose CD, Athreya BH. Successful treatment of retroperitoneal fibrosis with tamoxifen in a child. J Rheum. 2000;28:1693.
Dehner LP, Coffin CM. Idiopathic fibrosclerotic disorders and other inflammatory pseudotumors. Semin Diagn Pathol. 1998;15:161.
De Jonge MK, van der Beek C, Weil EHJ, Coolsaet BLRA. Antegrade ureteroscopy: a new tool in management of severe ureteral strictures. Urology. 1986;27:49.
Dejaco C, Ferenci P, Schober E, et al. Stenosis of the common bile duct due to Ormond’s disease: case report and review of literature. J Hepatol. 1999;31:156.
Delvecchio FC, Kuo RL, Iselin CE, et al. Combined antegrade and retrograde endoscopic approach for the management of urinary diversion—associated pathology. J Endourol. 2000;14:251.
DiMarco DS, Gettman MT, McGee SM, et al. Long-term success of antegrade endopyelotomy compared with pyeloplasty at a single institution. J Endourol. 2006;20:707.
DiMarco DS, LeRoy AJ, et al. Long-term results of treatment for ureteroenteric strictures. Urology. 2001;58:909.
DiSandro MJ, Kogan BA. Neonatal management: role for early intervention. Urol Clin North Am. 1998;25:187.
Docimo SG, Dewolf WC. High failure rate of indwelling ureteral stents in patients with extrinsic obstruction: experience at 2 institutions. J Urol. 1989;142:277.
Doo CK, Hong B, Park T, et al. Long-term outcome of endopyelotomy for the treatment of ureteropelvic junction obstruction: how long should patients be followed up? J Endourol. 2007;21:158.
Duchene DA, Winfield HN, Cadeddu JA, et al. Multi-institutional survey of laparoscopic ureterolysis for retroperitoneal fibrosis. Urology. 2007;69:1017.
Eden CG, Cahill D, Allen JD. Laparoscopic dismembered pyeloplasty: 50 consecutive cases. BJU Int. 2001;88:526.
Ehrlich RM, Gershman A, Fuchs G. Laparoscopic vesicoureteroplasty in children: initial case reports. Urology. 1993;43:255.
Ehrlich RM, Melman A, Skinner DG. The use of vesicopsoas hitch in urologic surgery. J Urol. 1978;119:322.
El Abd SA, El Shaer AF, El Mahrouky AS, et al. Long-term results of endourologic and percutaneous management of ureteral strictures in bilharzial patients. J Endourol. 1996;10:35.
El Nahas AR, Shoma AM, Eraky I, et al. Prospective randomized comparison of ureteroscopic endopyelotomy using holmium: YAG laser and balloon catheter. J Urol. 2006;175:614.
Elashry OM, Nakada SY, Wolf SKJr, et al. Ureterolysis for extrinsic ureteral obstruction: a comparison of laparoscopic and open surgical techniques. J Urol. 1996;156:1403.
Ellis JH, Campo RP, Mars MV, et al. Genitourinary radiology: positional variation in the Whitaker test. Radiology. 1995;197:253.
Fabrizio MD, Kavoussi LR, Jackman S, et al. Laparoscopic nephrectomy for autotransplantation. Urology. 2000;55:145iii.
Fielding JR, Steele G, Fox LA, et al. Spiral computerized tomography in the evaluation of acute flank pain: a replacement for excretory urography. J Urol. 1997;157:2071.
Finnerty DP, Trulock TS, Berman W, et al. Transluminal balloon dilations of ureteral strictures. J Urol. 1984;131:1056.
Foley FEB. New plastic operation for stricture at the ureteropelvic junction. J Urol. 1937;38:643.
Foote JW, Blennerhassett JB, Wigglesworth FW, et al. Observations on the ureteropelvic junction. J Urol. 1970;104:252.
Fry AC, Singh S, Gunda SS, et al. Successful use of steroids and ureteric stents in 24 patients with idiopathic retroperitoneal fibrosis: a retrospective study. Nephron Clin Pract. 2008;108:c213.
Fugita OE, Dinlenc C, Kavousi L. The laparoscopic Boari flap. J Urol. 2001;166:51.
Gdor Y, Gabr AH, Faerber GJ, et al. Success of laser endoureterotomy of ureteral strictures associated with ureteral stones is related to stone impaction. J Endourol. 2008;22:2507.
Gdor Y, Gabr AH, Faerber GJ, et al. Ho:YAG laser endoureterotomy for the treatment of transplant ureteral strictures. Transplantation. 2008;85:1318.
Gerber GS, Kim JC. Ureteroscopic endopyelotomy in the treatment of patients with ureteropelvic junction obstruction. Urology. 2000;55:198.
Gerber GS, Lyon ES. Endopyelotomy: patient selection, results, and complications. Urology. 1994;43:1.
Gettman MT, Lotan Y, et al. Cost-effective treatment for ureteropelvic junction obstruction: a decision tree analysis. J Urol. 2003;169:228.
Giddens JL, Grotas AB, Grasso M. Stone granuloma causes ureteropelvic junction obstruction after percutaneous nephrolithotomy and antegrade endopyelotomy. J Urol. 2000;164:118.
Gill IS, Cherullo EE, Steinberg AP, et al. Laparoscopic ureterocalicostomy: initial experience. J Urol. 2004;171:1227.
Gill IS, Desai MM, Kaouk JH, et al. Percutaneous endopyeloplasty: description of new technique. J Urol. 2002;168:2097.
Gill IS, Savage SJ, Senagore AJ, et al. Laparoscopic ileal ureter. J Urol. 2000;163:1199.
Gill IS, Uzzo R, Hobart MG, et al. Laparoscopic retroperitoneal live donor right nephrectomy for purposes of allotransplantation and autotransplantation. J Urol. 2000;164:1500.
Goldfischer ER, Gerber GS. Endoscopic management of ureteral strictures. J Urol. 1997;157:770.
Gosling JA, Dixon JS. Functional obstruction of the ureter and renal pelvis: a histological and electron microscopic study. Br J Urol. 1978;50:145.
Grotz W, Zedtwitz I, Andre M, Schollmeyer P. Treatment of retroperitoneal fibrosis by mycophenolate mofetil and corticosteroids. Lancet. 1998;352:1195.
Guiter J, Cuenant E, Mourad G, et al. [Re-establishment of urinary continuity by uretero-ureterostomy in renal transplantation. Apropos of 135 cases] (in French). J Urol (Paris). 1985;91:27.
Gundeti MS, Reynolds WS, Duffy PG, et al. Further experience with the vascular hitch (laparoscopic transposition of lower pole crossing vessels): an alternate treatment for pediatric ureterovascular ureteropelvic junction obstruction. J Urol. 2008;180:1832.
Gupta M, Tuncay OL, Smith AD. Open surgical exploration after failed endopyelotomy: a 12-year perspective. J Urol. 1997;157:1613.
Gupta NP, Hemal AK, Singh I, et al. Retroperitoneoscopic ureterolysis and reconstruction of retrocaval ureter. J Endourol. 2001;15:291.
Hanna MK. Some observations on congenital ureteropelvic junction obstruction. Urology. 1978;12:151.
Hanna MK. Antenatal hydronephrosis and ureteropelvic junction obstruction: the case for early intervention. Urology. 2000;55:612.
Hanna MK, Jeffs RD, Sturgess JM, et al. Ureteral structure and ultrastructure: Part II. Congenital ureteropelvic junction obstruction and primary obstructive megaureter. J Urol. 1976;116:725.
Harada N, Tanimura M, Fukuyama K, et al. Surgical management of a long ureteral defect: advancement of the ureter by descent of the kidney. J Urol. 1964;92:192.
Hardy JD. High ureteral injuries: management by autotransplantation of the kidney. JAMA. 1963;184:111.
Harmon WJ, Sershon PD, Blute ML, et al. Ureteroscopy: current practice and long-term complications. J Urol. 1997;157:28.
Harzmann R, Kopper B, Carl P. [Cancer induction by urinary drainage or diversion through intestinal segments?] (German.). Urologe A. 1986;25:198.
Hemal AK, Rao R, Sharma S, et al. Pure robotic retrocaval ureter repair. Int Braz J Urol. 2008;34:734.
Hendren WH, Hensle TW. Transureteroureterostomy: experience with 75 cases. J Urol. 1980;123:826.
Herts BR, Coll DM, Lieber ML, et al. Triphasic helical CT of the kidneys: contribution of vascular phase scanning in patients before urologic surgery. AJR Am J Roentgenol. 1999;173:1273.
Hibi H, Ohori T, Taki T, et al. Long-term results of endoureterotomy using a holmium laser. Int J Urol. 2007;14:872.
Higgins CC. Transuretero-ureteral anastomosis: report of clinical case. Trans Am Assoc Genitourin Surg. 1934;27:279.
Higgins PM, Bennett-Jones DN, Naish PF, Aber GM. Non-operative management of retroperitoneal fibrosis. Br J Surg. 1998;75:573.
Hinman F, Oppenheimer R. Functional characteristics of the ileal segment as a valve. J Urol. 1958;80:448.
Hodges CV, Barry JM, Fuchs EF, et al. Transureteroureterostomy: 25-year experience with 100 patients. J Urol. 1980;123:834.
Hsu THS, Presti JC. Anterior extraperitoneal approach to laparoscopic pyeloplasty in horseshoe kidney: a novel technique. Urology. 2003;62:1114.
Hsu THS, Chang S, Hsu S. Laparoscopic calicovesicostomy: a novel surgical procedure. Urology. 2006;68:413.
Hwang TK, Yoon JY, Ahn JH, et al. Percutaneous endoscopic management of upper ureteral stricture: size of stent. J Urol. 1996;155:882.
Inagaki T, Rha KH, Ong AM. Laparoscopic pyeloplasty: current status. BJU Int. 2005;95:102.
Inglis JA, Tolley DA. Ureteroscopic pyelolysis for pelviureteric junction obstruction. Br J Urol. 1986;58:250.
Izzedine H, Servais A, Launay-Vacher V, et al. Retroperitoneal fibrosis due to Wegener’s granulomatosis: a misdiagnosis as tuberculosis. Am J Med. 2002;113:164.
Jabbour ME, Goldfischer ER, Klima WJ, et al. Endopyelotomy after failed pyeloplasty: the long-term results. J Urol. 1998;160:690.
Jacobs JA, Berger BW, Goldman SM, et al. Ureteropelvic obstruction in adults with previously normal pyelograms: a report of five cases. J Urol. 1979;121:242.
Janetschek G, Peschel R, Altarac S. Laparoscopic and retroperitoneoscopic repair of ureteropelvic junction obstruction. Urology. 1996;47:311.
Janetschek G, Peschel R, Frauscher F. Laparoscopic pyeloplasty. Urol Clinc North Am. 2000;7:695.
Jarrett TW, Chan DY, Charambura TC, et al. Laparoscopic pyeloplasty: the first 100 cases. J Urol. 2002;167:1253.
Johnson DB, Solomon SB, Su L-M, et al. Defining the complications of cryoablation and radiofrequency ablation of small renal tumors: a multi-institutional review. J Urol. 2004;172:874.
Johnston JH, Evans JP, Glassberg KI, et al. Pelvic hydronephrosis in children: a review of 219 personal cases. J Urol. 1977;117:97.
Kaouk JH, Hafron J, Parekattil S, et al. Is retroperitoneal approach feasible for robotic dismembered pyeloplasty: initial experience and long-term results. J Endourol. 2008;22:2153.
Kardar AH, Kattan S, Lindstedt E, et al. Steroid therapy for idiopathic retroperitoneal fibrosis: dose and duration. J Urol. 2002;168:550.
Karlin GS, Badlani GH, Smith AD. Endopyelotomy versus open pyeloplasty: comparison in 88 patients. J Urol. 1988;140:476.
Kavoussi LR, Clayman RV, Brunt LM, et al. Laparoscopic ureterolysis. J Urol. 1992;147:426.
Kavoussi LR, Peters CA. Laparoscopic pyeloplasty. J Urol. 1993;150:1891.
Kay R. Procedures for ureteropelvic junction obstruction. In: Novick AC, Streem SB, Pontes JE, editors. Stewart’s operative urology. 2nd ed. Baltimore: Williams & Wilkins; 1989:220-233.
Kearney GP, Mahoney EM, Sciammas FD, et al. Venacavography, corticosteroids and surgery in the management of idiopathic retroperitoneal fibrosis. J Urol. 1976;115:32.
Keeley FXJr, Bagley DH, et al. Laparoscopic division of crossing vessels at the ureteropelvic junction. J Endourol. 1996;10:163.
Kelalis PP. Ureteropelvic junction. In: Kelalis PP, King LR, editors. Clinical pediatric urology. Philadelphia: WB Saunders; 1976:239-257.
Kennelly MJ, Konnak JW, Herwig KR. Vesicopyeloplasty in renal transplant: a 20 year follow-up. J Urol. 1993;150:1118.
King LR, Coughlin PWF, Bloch EC, et al. The case for immediate pyeloplasty in the neonate with ureteropelvic junction obstruction. J Urol. 1984;132:725.
King LR, Coughlin PWF, Ford KK, et al. Initial experiences with percutaneous and transurethral ablation of postoperative ureteral strictures in children. J Urol. 1984;131:1167.
Kletscher BA, Segura JW, LeRoy AJ, et al. Percutaneous antegrade endoscopic pyelotomy: review of 50 consecutive cases. J Urol. 1995;153:701.
Klingler HC, Remzi M, Janetschek G, et al. Comparison of open and laparoscopic pyeloplasty techniques in treatment of uretero-pelvic junction obstruction. Eur Urol. 2003;44:340.
Klisnick A, Fourcade J, Rulvard M, et al. Combined idiopathic retroperitoneal and mediastinal fibrosis with pericardial involvement. Clin Nephrol. 1999;52:51.
Knerr I, Dittrich K, et al. Alteration of neuronal and endothelial nitric oxide synthase and neuropeptide Y in congenital ureteropelvic junction obstruction. Urol Res. 2001;29:134.
Knowles DR, Staiman VR, et al. Long-term results of the treatment of complete distal ureteral stenosis using a cutting balloon catheter device. J Urol. 2001;166(6):2087.
Knudsen BE, Cook AJ, et al. Percutaneous antegrade endopyelotomy: long-term results from one institution. Urology. 2004;63:230.
Koch MO, McDougal WS. The pathophysiology of hyperchloremic metabolic acidosis after urinary diversion through intestinal segments. Surgery. 1985;98:561.
Koep L, Zuidema GD. The clinical significance of retroperitoneal fibrosis. Surgery. 1987;81:250.
Koff SA. Neonatal management of unilateral hydronephrosis: role for delayed intervention. Urol Clin North Am. 1998;25:181.
Koff SA. Postnatal management of antenatal hydronephrosis using an observational approach. Urology. 2000;55:609.
Koff SA, Campbell KD. The nonoperative management of unilateral neonatal hydronephrosis: natural history of poorly functioning kidneys. J Urol. 1994;152:593.
Koff SA, Hayden LJ, Cirulli C, et al. Pathophysiology of ureteropelvic junction obstruction: experimental and clinical observations. J Urol. 1986;136:336.
Korth K, Kuenkel M, Erschig M. Percutaneous pyeloplasty. Urology. 1988;31:503.
Kouba E, Wallen EM, Pruthi RS. Management of ureteral obstruction due to advanced malignancy: optimizing therapeutic and palliative outcomes. J Urol. 2007;180:444.
Kramolowsky EV, Clayman RV, Weyman PJ. Endourological management of ureteroileal anastomotic strictures: is it effective? J Urol. 1987;137:390.
Kramolowsky EV, Clayman RV, Weyman PJ. Management of ureterointestinal anastomotic strictures: comparison of open surgical and endourological repair. J Urol. 1988;139:1195.
Kumon H, Tsugawa M, Hashimoto H, et al. Impact of 3-dimensional helical computerized tomography on selection of operative methods for ureteropelvic junction obstruction. J Urol. 1997;158:1696.
Kurzer E, Leveillee RJ. Endoscopic management of ureterointestinal strictures after radical cystectomy. J Endourol. 2005;19:677.
1892 Kuster: Ein fall von resection des ureter. Arch Klin Chir. 1892;44:850.
Kwak S, Leef JA, Rosenblum JD. Percutaneous balloon catheter dilatation of benign ureteral strictures: effect of multiple dilatation procedures on long-term patency. AJR Am J Roentgenol. 1995;165:97.
Lacquet JP, Cacroix H, Nevelsteen A, Suy R. Inflammatory abdominal aortic aneurysms. A retrospective study of 110 cases. Acta Chir Belg. 1997;97:286.
Lam JS, Bingham JB, et al. Endoscopic treatment of fibroepithelial polyps of the renal pelvis and ureter. Urology. 2003;62:810.
Lam JS, Cooper KL, et al. Impact of hydronephrosis and renal function on treatment outcome: antegrade versus retrograde endopyelotomy. Urology. 2003;61:1107.
Lane BR, Desai MM, Hegarty NJ, et al. Long-term efficacy of holmium laser endoureterotomy for benign ureteral strictures. Urology. 2006;67:894.
Lau KO, Hia TN, Cheng C, Tay SK. Outcome of obstructive uropathy after pelvic irradiation in patients with carcinoma of the uterine cervix. Ann Acad Med Singapore. 1998;27:631.
Laungani R, Patil N, Krane LS. Robotic-assisted ureterovaginal fistula repair: report of efficacy and feasibility. J Laparoendosc Adv Surg Tech A. 2008;18:731.
Laven BA, O’Connor RC, et al. Long-term results of endoureterotomy and open surgical revision for the management of ureteroenteric strictures after urinary diversion. J Urol. 2003;170:1226.
Laven BA, O’Connor RC, et al. Long-term results of antegrade endoureterotomy using the holmium laser in patients with ureterointestinal strictures. Urology. 2001;58(6):924.
Lawler LP, Jarret TW, et al. Adult ureteropelvic junction obstruction: insights with three-dimensional multi-detector row CT. Radiographics. 2005;25:121.
LeBlanc CM, Inman RD, Dent P, et al. Retroperitoneal fibrosis: an extraarticular manifestation of ankylosing spondylitis. Arthritis Rheum. 2002;47:210.
Lebowitz RL, Johan BG. The coexistence of ureteropelvic junction obstruction and reflux. AJR Am J Roentgenol. 1982;140:231.
Lechevallier E, Eghazarian C, Ortega JC, et al. Retrograde Acucise endopyelotomy: long-term results. J Endourol. 1999;13:575.
Lee RS, Retik AB, Borer JG, et al. Pediatric robot assisted laparoscopic dismembered pyeloplasty: comparison with a cohort of open surgery. J Urol. 2006;175:683.
Lepor H, Walsh PC. Idiopathic retroperitoneal fibrosis. J Urol. 1979;122:1.
Levitt SB, Nabizadeh I, Javaid M, et al. Primary calicoureterostomy for pelvioureteral junction obstruction: indications and results. J Urol. 1981;126:382.
Liatsikos E, Kalidonis P, Kyriazis I, et al. Ureteral obstruction: is the full metallic double-pigtail stent the way to go? Eur Urol. 2010;57:480.
Lin DW, Bush WH, Mayo ME. Endourological treatment of ureteroenteric strictures: efficacy of Acucise endoureterotomy. J Urol. 1999;162:696.
Lindell OI, Lehtonen TA. Surgical treatment of ureteric obstruction in idiopathic retroperitoneal fibrosis. Scand J Urol Nephrol Suppl. 1988;110:299.
Link RE, Bhayani SB, Kavoussi LR. A prospective comparison of robotic and laparoscopic pyeloplasty. Ann Surg. 2006;243:486.
Lovaco F, Serrano A, Fernández I, et al. Endoureterotomy by intraluminal invagination for non-malignant ureterointestinal anastomotic strictures: description of a new surgical technique and long-term follow up. J Urol. 2005;174:1851.
Lugagne PM, Herve JM, Lebret T, et al. Ureteroileal implantation in orthotopic neobladder with Le Duc-Camey mucosal-through technique: risk of stenosis and long-term follow-up. J Urol. 1997;158:765.
Macksood MJ, Roth DR, Chang CH, et al. Benign fibroepithelial polyps as a cause of intermittent ureteropelvic junction obstruction in a child: a case report and review of the literature. J Urol. 1985;134:951.
Madi R, Roberts WW, Wolf JSJr. Late failures after laparoscopic pyeloplasty. Urology. 2008;71:677.
Maizels M, Stephens FD. Valves of the ureter as a cause of primary obstruction of the ureter: anatomic, embryologic and clinical aspects. J Urol. 1980;123:742.
Malden ES, Picus D, Clayman RV. Arteriovenous fistula complicating endopyelotomy. J Urol. 1992;148:1520.
Malek RS. Intermittent hydronephrosis: the occult ureteropelvic obstruction. J Urol. 1983;130:863.
Mandhani A, Kapoor R, et al. Is a 2-week duration sufficient for stenting in endopyelotomy? J Urol. 2003;169:886.
Mansson W, Ahlgren G, White T. Glomerular filtration rate up to 10 years after urinary diversion of different types. A comparative study of ileal and colonic conduit, refluxing and antirefluxing ureteral anastomosis and continent caecal reservoir. Scand J Urol Nephrol. 1989;23:195.
Martinez J, Kaplan N, Boyarsky S. Laboratory and clinical studies of ureteral replacement by ileum. J Urol. 1965;93:185.
Marzano A, Trapani A, Leone N, et al. Treatment of idiiopathic retroperitoneal fibrosis using cyclosporin. Ann Rheum Dis. 2001;60:427.
Masood J, Panah A, Zaman F, et al. Laparoscopic cranial placation in pelviureteral junction obstruction by aberrant lower pole artery. J Endourol. 2009;23:7.
Mata JA, Culkin DJ, Venable DD. Techniques for bypassing and stenting ureteral obstructions. J Urol. 1994;152:917.
Mathews R, Marshall FF. Versatility of the adult psoas hitch ureteral reimplantation. J Urol. 1997;158:2078.
Matiaga BR, Shah OD, Hart LJ, Assimos DG. Ileal ureter substitution: a contemporary series. Urology. 2003;62:998.
Matin SF, Yost A, et al. Ureteroscopic laser endopyelotomy: a single-center experience. J Endourol. 2003;17:401.
Matsuda T, Yasumoto R, Tsujino T. Laparoscopic treatment of a retrocaval ureter. Eur Urol. 1996;29:115.
McClinton S, Steyn JH, et al. Retrograde balloon dilatation for pelviureteric junction obstruction. Br J Urol. 1993;71:152.
McDougal WS, MacDonell RCJr. Treatment of idiopathic retroperitoneal fibrosis by immunosuppression. J Urol. 1991;145:112.
McQuitty DA, Boone TB, Preminger GM. Lower pole calicostomy for the management of iatrogenic ureteropelvic junction obstruction. J Urol. 1995;153:142.
Meng MV, Freise CE, Stoller ML. Expanded experience with laparoscopic nephrectomy and autotransplantation for severe ureteral injury. J Urol. 2003;169:1363.
Meng MV, Stoller ML. Hellstrom technique revisited: laparoscopic management of ureteroplevic junction obstruction. Urology. 2003;62:404.
Mercadal L, Martinez F, Barrou B, et al. Retroperitoneal fibrosis and membranous nephropathy. Clin Nephrol. 2000;53:71.
Meretyk S, Albala DM, Clayman RV, et al. Endoureterotomy for treatment of ureteral strictures. J Urol. 1992;147:1502.
Meretyk S, Clayman RV, Kavoussi LR, et al. Endourological treatment of ureteroenteric anastomotic strictures: long-term follow-up. J Urol. 1991;145:723.
Metzelder ML, Schier F, Petersen C, et al. Laparoscopic transabdominal pyeloplasty in children is feasible irrespective of age. J Urol. 2006;175:688.
Middleton RG. Routine use of the psoas hitch in ureteral reimplantation. J Urol. 1980;123:352.
Mitty HA, Train JS, Dan SJ. Antegrade ureteral stenting in the management of fistulas, strictures, and calculi. Radiology. 1983;149:433.
Moon YT, Kerbl K, et al. Evaluation of optimal stent size after endourologic incision of ureteral strictures. J Endourol. 1995;9:15.
Motiwala HG, Shah SA, Patel SM. Ureteric substitution with Boari bladder flap. Br J Urol. 1990;66:369.
Motola JA, Badlani GH, Smith AD. Results of 212 consecutive endopyelotomies: an 8-year follow-up. J Urol. 1993;149:453.
Motola JA, Fried R, Badlani GH, Smith AD. Failed endopyelotomy: implications for future surgery on the ureteropelvic junction. J Urol. 1993;150:821.
Muench PJ, Cates HR, Raney AM, et al. Endoscopic management of the obliterated ureteroileal anastomosis. J Urol. 1987;137:277.
Muffarrij PW, Shah OD, Berger AD, et al. Robotic reconstruction of the upper urinary tract. J Urol. 2007;278:2002.
Mure PY, Mollard P, Mouriquand P. Transureteroureterostomy in childhood and adolescence: long-term results in 69 cases. J Urol. 2000;163:946.
Nadler RB, Rao GS, Pearle MS, et al. Acucise endopyelotomy: assessment of long-term durability. J Urol. 1996;156:1094.
Nakada SY. Surgical techniques in urology: Acucise endopyelotomy. Urology. 2000;55:277.
Nakada SY, Soble JJ, Gardner SM, et al. Comparison of Acucise endopyelotomy and endoballoon rupture for management of secondary proximal ureteral stricture in the porcine model. J Endourol. 1996;10:311.
Nakada SY, Wolf JSJr, Brink JA. Retrospective analysis of the effect of crossing vessels on successful retrograde endopyelotomy outcomes using spiral computerized tomography angiography. J Urol. 1998;159:62.
Naude JH. Buccal mucosal grafts in the treatment of ureteric lesions. Br J Urol. 1999;83:751.
Nesbit RM. Diagnosis of intermittent hydronephrosis: importance of pyelography during episodes of pain. J Urol. 1956;75:767.
Netto NRJr, Ferreira U, Lemos GC, et al. Endourological management of ureteral strictures. J Urol. 1990;144:631.
Nezhat CH, Malik S, Nezhat F, et al. Laparoscopic ureteroneocystostomy and vesicopsoas hitch for infiltrative endometriosis. JSLS. 2004;8:3.
Nezhat C, Nezhat F, Green B. Laparoscopic treatment of obstructed ureter due to endometriosis by resection and ureteroureterostomy: a case report. J Urol. 1992;148:865.
Nezhat CH, Nezhat F, Seidman D, et al. Laparoscopic ureteroureterostomy: a prospective follow-up of 9 patients. Primary Care Update Ob Gyns. 1998;5:200.
Niemczyk P, Krisch EB, et al. Use of diuretic renogram in evaluation of patients before and after endopyelotomy. Urology. 1999;53:271.
Novick AC, Stewart BH. Experience with extracorporeal renal operations and autotransplantation in the management of complicated urologic disorders. Surg Gynecol Obstet. 1981;153:10.
Ockerblad NF. Reimplantation of the ureter into the bladder by a flap method. J Urol. 1947;57:845.
Oh BR, Kwon DD, Park KS, et al. Late presentation of ureteral injury after laparoscopic surgery. Obstet Gynecol. 2000;95:337.
Ono Y, Ohshima S, Kinukawa T, et al. Endopyeloureterotomy via a transpelvic extraureteral approach. J Urol. 1992;147:352.
O’Reilly PH. Diuresis renography eight years later: an update. J Urol. 1986;136:993.
O’Reilly PH. Functional outcome of pyeloplasty for ureteropelvic junction obstruction: prospective study in 30 consecutive cases. J Urol. 1989;142:273.
Özgen A, Cila A. Riedel’s thyroiditis in multifocal fibrosclerosis: CT and MR imaging findings. AJNR Am J Neuroradiol. 2000;21:320.
Palese MA, Munver R, Phillips CK, et al. Robot-assisted laparoscopic dismembered pyeloplasty. JSLS. 2005;9:252.
Palmer LS, Rosenthal SA. Testicular encasement by retroperitoneal fibrosis: a rare testicular mass. Urology. 1999;53:619.
Pantuck AJ, Han KR, Perrotti M, et al. Ureteroenteric anastomosis in continent urinary diversion: long-term results and complications of direct versus nonrefluxing techniques. J Urol. 2000;163:450.
Parums DV, Choudhury RP, Shields SA, Davies AH. Characterisation of inflammatory cells associated with “idiopathic retroperitoneal fibrosis.”. Br J Urol. 1991;67:564.
Passerini-Glazel G, Meneghini A, Aragona F, et al. Technical options in complex ureteral lesions: “ureter-sparing” surgery. Eur Urol. 1994;25:273.
Passerotti CC, Diamond DA, Borer JG, et al. Robot-assisted laparoscopic ureteroureterostomy: description of technique. J Endourol. 2008;22:581.
Patil NN, Mottrie A, Sundaram B, et al. Robotic-assisted laparoscopic ureteral reimplantation with psoas hitch: a multi-insitutional, multinational evaluation. Urology. 2008;72:47.
Pearle MS, Moon YT, et al. Comparison of retrograde endo-pyelotomy and endo-balloon rupture of the ureteropelvic junction in a porcine model. J Urol. 1994;152:2232.
Penalver GC, Sanchez TA, Gonzalez DR, et al. Follow-up of a case of retroperitoneal fibroses treated sequentially via right side autotransplant and left ureterolysis with wrapper of posterior preperitoneal fat. Int Urol Nephrol. 2001;32:629.
Penalver MA, Angioli R, Mirhashemi R, Malik R. Management of early and late complications of ileocolonic continent reservoir (Miami pouch). Gynecol Oncol. 1998;69:185.
Persky L, Krause JR, Boltuch RL. Initial complications and late results in dismembered pyeloplasty. J Urol. 1977;118:162.
Pesce C, Costa L, Campobasso P, et al. Successful use of transureteroureterostomy in children: a clnical study. Eur J Pediatr Surg. 2001;11:395.
Peschel R, Neururer R, Bartsch G, Gettman MT. Robotic pyeloplasty: technique and results. Urol Clin North Am. 2004;31:737.
Piaggio LA, Gonzalez R. Laproscopic transureteroureterostomy: a novel approach. J Urol. 2007;177:2311.
Pienkny AJ, Herts B, Streem SB. Contemporary diagnosis of retrocaval ureter. J Endourol. 1999;13:721.
Polascik JT, Chen NR. Laparoscopic ureteroureterostomy for retrocaval ureter. J Urol. 1998;160:121.
Ponsky LE, Streem SB. Retrograde endopyelotomy: a comparative study of hot-wire balloon and ureteroscopic laser. J Endourol. 2006;20:823.
Popescu C. The surgical management of postoperative ureteral fistulas. Surg Gynecol Obstet. 1964;119:1079.
Powell CR, Schwartz BF, Stoney RJ, Stoller ML. Gross hematuria secondary to renal vein hypertension from unilateral retroperitoneal fibrosis. Urology. 2000;55:436.
Pozniak MA, Nakada SY. Three-dimensional computed tomographic angiography of a horseshoe kidney with ureteropelvic junction obstruction. Urology. 1997;49:267.
Prout GRJr, Koontz WWJr. Partial vesical immobilization: an important adjunct to ureteroneocystostomy. J Urol. 1970;103:147.
Puce R, Porcaro AB, Curti P, et al. Treatment of retroperitoneal fibrosis with tamoxifen: case report and review of literature. Arch Esp Urol. 2000;53:184.
Puppo P, Carmignani G, Galluci M, et al. Bilateral laparoscopic ureterolysis. Eur Urol. 1994;25:82.
Quillin SP, Brink JA, Heiken JP, et al. Helical (spiral) CT angiography for identification of crossing vessels at the ureteroscopic junction. AJR Am J Roentgenol. 1996;166:1125.
Ramakumar S, Lancini V, Chan DY, et al. Laparoscopic pyeloplasty with concomitant pyelolithotomy. J Urol. 2002;167:1378.
Ramalingam M, Selvarajan K. Laparoscopic transperitoneal repair of retrocaval ureter: report of two cases. J Endourol. 2003;17:85.
Ramanathan R, Kumar A, Kapoor R, Bhandari M. Relief of urinary tract obstruction in tuberculosis to improve renal function. Analysis of predictive factors. Br J Urol. 1998;81:199.
Ramsay JWA, Miller RA, Kellett MJ, et al. Percutaneous pyelolysis: indications, complications and results. Br J Urol. 1984;56:586.
Rassweiler JJ, Teber D, Frede T. Complications of laparoscopic pyeloplasty. World J Urol. 2008;26:539.
Rassweiler JJ, Subotic S, Feist-Schwenk M, et al. Minimally invasive treatment of ureteropelvic junction obstruction: long-term experience with an algorithm for laser endopyelotomy and laparoscopic retroperitoneal pyeloplasty. J Urol. 2007;177:1000.
Ravery V, de la TA, et al. Balloon catheter dilatation in the treatment of ureteral and ureteroenteric stricture. J Endourol. 1998;12:335.
Reddy PK, Evans RM. Laparoscopic ureteroneocystostomy. J Urol. 1994;152:2057.
Rhee RY, Gloviczki P, Luthra HS, et al. Iliocaval complications of retroperitoneal fibrosis. Am J Surg. 1994;168:179.
Richter F, Irwin RJ, Watson RA, Lang EK. Endourologic management of benign ureteral strictures with and without compromised vascular supply. Urology. 2000;55:652.
Richstone L, Seideman CA, Reggio E, et al. Pathologic findings in patients with ureteropelvic junction obstruction and crossing vessels. Urology. 2009;73:716.
Riehle RAJr, Vaughan EDJr. Renin participation in hypertension associated with unilateral hydronephrosis. J Urol. 1981;126:243.
Roarke MC, Sandler CM. Provocative imaging: diuretic renography. Urol Clin North Am. 1998;25:227.
Roberts WW, Cadeddu JA, Micali S, et al. Ureteral stricture formation after removal of impacted calculi. J Urol. 1998;159:723.
Rodo Salas J, Martin Hortiguela E, Salarich de Arbell J. [Psoas fixation of the bladder. An efficient aid in cases of repeat surgery of the uretero-vesical junction] (in Spanish). Arch Esp Urol. 1991;44:125.
Romero FR, Wagner AA, Trapp C, et al. Transmesenteric laparoscopic pyeloplasty. J Urol. 2006;176:2526.
Rosevear HM, Kim SP, Wenzler DL. Retrograde ureteral stents for extrinsic ureteral obstruction: nine years’ experience at University of Michigan. Urology. 2007;70:846.
Ross JH, Streem SB, Novick AC, et al. Ureterocalicostomy for reconstruction of complicated pelviureteric junction obstruction. Br J Urol. 1990;65:322.
Roth DR, Gonzales ETJr. Management of ureteropelvic junction obstruction in infants. J Urol. 1983;129:108.
Roth S, Weining C, Hertle L. Simplified uretero-intestinal implantation in continent cutaneous urinary diversion using ileovalvular segment as afferent loop and appendix as continent outlet. J Urol. 1996;155:1200.
Salomon L, Hoznek A, Balian C, et al. Retroperitoneal laparoscopy of a retrocaval ureter. BJU Int. 1999;84:181.
Sampaio FJB, Favorito LA. Ureteropelvic junction stenosis: vascular anatomical background for endopyelotomy. J Urol. 1993;150:1787.
Sampaio FJ. Vascular anatomy at the ureteropelvic junction. Urol Clin North Am. 1998;25:251.
Scardino PL, Prince CL. Vertical flap ureteropelvioplasty: preliminary report. South Med J. 1953;46:325.
Schaeffer AJ, Grayhack JT. Surgical management of ureteropelvic junction obstruction. In: Walsh PC, Gittes RF, Perlmutter AD, Stamey TA, editors. Campbell’s urology. 5th ed. Philadelphia: WB Saunders; 1986:2505-2533.
Schimpf MO, Wagner JR. Robot-assisted laparoscopic distal ureteral surgery. JSLS. 2009;13:44.
Schneider AW, Conrad S, Busch R, et al. The cold-knife technique for endourological management of stenosis in the upper urinary tract. J Urol. 1991;146:961.
Schmidt JD, Hawtrey CE, et al. Complications, results and problems of ileal conduit diversions. J Urol. 1973;109:210.
Schuessler WW, Grune MT, Tecuanhuey LV, et al. Laparoscopic dismembered pyeloplasty. J Urol. 1993;150:1795.
Schulte-Baukloh H, Knispel HH, Dallenbach F, Miller K. Scrotal involvement with idiopathic retroperitoneal fibrosis. J Urol. 1999;162:1692.
Schumacher M, Studer UE, Danuser H. Antegrade endopyelotomy for the treatment of ureteropelvic junction obstruction in transplanted kidneys. J Endourol. 2006;20:305.
Schwentner C, Pelzer A, Neururer R. Robotic Anderson-Hynes pyeloplasty: 5-year experience of one center. BJU Int. 2007;100:880.
Scott FB, Greenberg M. Submucosal bladder flap ureteroplasty: clinical experience. South Med J. 1972;65:1308.
Shalhav AL, Giusti G, Elbahnasy AM, et al. Adult endopyelotomy: impact of etiology and antegrade versus retrograde approach on outcome. J Urol. 1998;160:685.
Shapiro EY, Cho JS, Srinivasan A, et al. Long-term follow-up for salvage laparoscopic pyeloplasty after failed open pyeloplasty. Urology. 2009;73:115.
Shirota S, Tsuchiya K, Takada M, et al. Retroperitoneal fibrosis associated with membranous nephropathy effectively treated with steroids. Int Med. 2002;41:20.
Shoemaker, cited by Moore EV, Weber R, Woodward ER, et al. Isolated ileal loops for ureteral repair. Surg Gynecol Obstet. 1956;102:87.
Shokeir AA, Nijman RJM. Antenatal hydronephrosis: changing concepts in diagnosis and subsequent management. BJU Int. 2000;85:987.
Siegel JH, Padula G, Yatto RP, et al. Combined endoscopic and percutaneous approach for the treatment of ureterocolic strictures. Radiology. 1982;145:841.
Simforoosh N, Basiri A, Tabibi A, et al. A comparison between laparoscopic and open pyeloplasty in patients with ureteropelvic junction obstruction. Urol J. 2004;1:165.
Simforoosh N, Tabibi A, Nouralizadeh A, et al. Laparoscopic management of ureteropelvic junction obstruction by division of anterior crossing vein and cephalad relocation of anterior crossing artery. J Endourol. 2005;19:827.
Singal RK, Denstedt JD, et al. Holmium-yag laser endoureterotomy for treatment of ureteral stricture. Urology. 1997;50:875.
Skinner DG, Crawford ED, et al. Complications of radical cystectomy for carcinoma of the bladder. J Urol. 1980;123:640.
Smith KM, Shrivastava D, Ravish IR, et al. Robot-assisted laparoscopic ureteroureterostomy for proximal ureteral obstruction in children. J Pediatr Urol. 2009;5:475.
Sofras F, Livadas K, et al. Retrograde Acucise endopyelotomy: is it worth its cost? J Endourol. 2004;18:466.
Solari V, Piotrowska AP, et al. Altered expression of interstitial cells of Cajal in congenital ureteropelvic junction obstruction. J Urol. 2003;170:2420.
Soulie M, Salomon L, Patard JJ, et al. Extraperitoneal laparoscopic pyeloplasty: a multicenter study of 55 procedures. J Urol. 2001;166:48.
Stauss J, Connolly LP, et al. Dynamic renal scintigraphy in children with vesicoureteral reflux and suspected coexisting ureteropelvic junction obstruction. J Urol. 2003;170:1966.
Stefanovic KB, Bukurov NS, Marinkovic JM. Non-antireflux versus antireflux ureteroneocystostomy in adults. Br J Urol. 1991;67:263.
Stein RJ, Gill IS, Desai MM. Comparison of surgical approaches to ureteropelvic junction obstruction: endopyeloplasty versus endopyelotomy versus laparoscopic pyeloplasty. Curr Urol Rep. 2007;8:14.
Stein RJ, Turna B, Nguyen MM, et al. Laparoscopic pyeloplasty with concomitant pyelolithotomy: technique and outcomes. J Endourol. 2008;22:1251.
Stephens FD. Ureterovascular hydronephrosis and the “aberrant” renal vessels. J Urol. 1982;128:984.
Streem SB. Percutaneous endopyelotomy. Urol Clin North Am. 2000;27:685.
Streem SB, Geisinger MA. Prevention and management of hemorrhage associated with cautery wire balloon incision of ureteropelvic junction obstruction. J Urol. 1995;153:1904.
Studer UE, Danuser H, Merz VW, et al. Experience in 100 patients with an ileal low pressure bladder substitute combined with an afferent tubular isoperistaltic segment. J Urol. 1995;154:49.
Sugarbaker PH, Gutman M, Verghese M. Transureteroureterostomy: an adjunct to the management of advanced primary and recurrent pelvic malignancy. Int J Colorectal Dis. 2003;18:40.
Sundaram CP, Grubb RL, Rehman J, et al. Laparoscopic pyeloplasty for secondary ureteroplevic junction obstruction. J Urol. 2003;169:2037.
Sung GT, Gill IS, Hsu THS. Robotic-assisted laparoscopic pyeloplasty: a pilot study. Urology. 1999;53:1099.
Tawfiek ER, Liu J, Bagley DH. Ureteroscopic treatment of ureteropelvic junction obstruction. J Urol. 1998;160:1643.
Thomas JC, DeMarco RT, Donohoe JM, et al. Management of the failed pyeloplasty: a contemporary review. J Urol. 2005;174:2363.
Thomas R, Monga M, Klein E. Ureteroscopic retrograde endopyelotomy for management of ureteropelvic junction obstruction. J Endourol. 1996;10:141.
Thompson IM, Baker J, Robards VL, et al. Clinical experience with renal capsule flap pyeloplasty. J Urol. 1969;101:487.
Thompson IM, Ross GJr. Long-term results of bladder flap repair of ureteral injuries. J Urol. 1974;111:483.
Tresidder GC, Blandy JP, Singh M. Omental sleeve to prevent retroperitoneal fibrosis around the ureter. Urol Int. 1972;27:144.
Tripodi SA, Mattei FM, Giovannelli V, et al. Idiopathic retroperitoneal fibrosis simulating renal malignancy. J Urol. 1998;160:2145.
Tsuji Y, Nakamura H, Ariyoshi A. Upper urinary tract involvement after cystectomy and ileal conduit diversion for primary bladder carcinoma. Eur Urol. 1996;29:216.
Turk IA, Davis JW, Winkelmann B, et al. Laparoscopic dismembered pyeloplasty—the method of choice in the presence of an enlarged renal pelvis and crossing vessels. Eur Urol. 2002;42:268.
Usher SM, Brendler H, Ciavarra V. Retroperitoneal fibrosis secondary to metastatic neoplasm. Urology. 1977;9:191.
Vaarala MH, Marttila T, Paananen I, et al. Retrospective analysis of long-term outcomes of 64 patients treated by endopyelotomy in two low volume hospitals: good and durable results. J Endourol. 2008;22:1659.
Van Bommel EFH. Retroperitoneal fibrosis. Neth J Med. 2002;60:231.
Van Cangh PJ, Jorion JL, Wese FX, Opsomer RJ. Endoureteropyelotomy: percutaneous treatment of ureteropelvic junction obstruction. J Urol. 1989;141:1317.
Van Cangh PJ, Wilmart JF, Opsomer RJ, et al. Long-term results and late recurrence after endoureteropyelotomy: a critical analysis of prognostic factors. J Urol. 1994;151:934.
Varkarakis IM, Bhayani SB, Allaf ME, et al. Management of secondary ureteropelvic junction obstruction after failed primary laparoscopic pyeloplasty. J Urol. 2004;172:180.
Vega J, Goecke H, Tapia H, et al. Treatment of idiopathic retroperitoneal fibrosis with colchicine and steroids: a case series. Am J Kidney Dis. 2009;53:628.
Vieweg J, The C, Freed K, et al. Unenhanced helical computerized tomography for the evaluation of patients with acute flank pain. J Urol. 1998;160:679.
Voegeli DR, Crummy AB, McDermott JC, et al. Percutaneous dilation of ureteral strictures in renal transplant patients. Radiology. 1988;169:185.
Wagenknecht LV, Hardy JC. Value of various treatments for retroperitoneal fibrosis. Eur Urol. 1981;7:193.
Wagner JR, D’Agostino R, Babayan RK. Renal arterioureteral hemorrhage: complication of Acucise endopyelotomy. Urology. 1996;48:139.
Wagner JR, Schimpf MO, Cohen JL. Robot-assisted laparoscopic ileal ureter. JSLS. 2008;12:306.
Waldner M, Hertle L, Roth S. Ileal ureteral substitution in reconstructive urological surgery: is an antireflux procedure necessary? J Urol. 1999;162:323.
Waters WB, Whitmore WF, Lage AL, et al. Segmental replacement of the ureter using tapered and non-tapered ileum. Invest Urol. 1981;18:258.
Watterson JD, Sofer M, et al. Holmium: YAG laser endoureterotomy for ureterointestinal strictures. J Urol. 2002;167:1692.
Webb AJ, Dawson-Edwards P. Malignant retroperitoneal fibrosis. Br J Surg. 1967;54:505.
Webber RJ, Pandian SS, et al. Retrograde balloon dilatation for pelviureteric junction obstruction: long-term follow-up. J Endourol. 1997;11:239.
Weijerman PC, Schurmans JR, Hop WC, et al. Morbidity and quality of life in patients with orthotopic and heterotopic continent urinary diversion. Urology. 1998;51:51.
Weiss JN, Badlani GH, Smith AD. Complications of endopyelotomy. Urol Clin North Am. 1988;15:449.
Wenzler DL, Kim SP, Rosevear HM, et al. Success of ureteral stents for intrinsic ureteral obstruction. J Endourol. 2008;22:295.
Williams SK, Levillee RJ. Expanding the horizons: robot-assisted reconstructive surgery of the distal ureter. J Endourol. 2009;23:457.
Wolf JSJr, Elashry OM, Clayman RV. Long-term results of endoureterotomy for benign ureteral and ureteroenteric strictures. J Urol. 1997;158:759.
Wollin M, Duffy PG, Diamond DA, et al. Priorities in urinary diversion following pyeloplasty. J Urol. 1989;142:576.
Wolpert JJ, Woodard JR, Parrott TS. Pyeloplasty in the young infant. J Urol. 1989;142:573.
Wotkowicz C, Libertino JA. Renal autotransplantation. BJU International. 2004;93:253.
Yamada S, Ono Y, Ohshima A, et al. Transurethral ureteroscopic ureterotomy assisted by a prior balloon dilation for relieving ureteral strictures. J Urol. 1995;153:1418.
Yang Y, Zhou X, et al. The expression of epidermal growth factor and transforming growth factor-beta1 in the stenotic tissue of congenital pelvi-ureteric junction obstruction in children. J Pediatr Surg. 2003;38:1656.
Yanke BV, Lallas CD, Pagnani C, et al. The minimally invasive treatment of ureteropelvic junction obstruction: a review of our experience during the last decade. J Urol. 2008;180:1397.
Yohannes P, Smith AD. Dual stent placement for the treatment of a persistent urine leak after partial nephrectomy—comment. Urology. 2001;57:356.
Zeltser IS, Liu JB, et al. The incidence of crossing vessels in patients with normal ureteropelvic junction examined with endoluminal ultrasound. J Urol. 2004;172:2304.
Zincke H, Kelasis PP, Culp OS. Ureteropelvic obstruction in children. Surg Gynecol Obstet. 1974;139:873.