The Child with an Emotional or Behavioral Condition
1 Define each key term listed.
2 Differentiate among the following terms: psychiatrist, psychoanalyst, clinical psychologist, and counselor.
3 Discuss the impact of early childhood experience on a person’s adult life.
4 Discuss the effect of childhood autism on growth and development.
5 Discuss behavioral therapy and how it is applied to obsessive compulsive disorders and depression in children.
6 List the symptoms of potential suicide in children and adolescents.
7 Discuss immediate and long-range plans for the suicidal patient.
8 List four behaviors that may indicate substance abuse.
9 Name two programs for members of families of alcoholics.
10 Discuss the problems facing children of alcoholics.
11 List four symptoms of attention deficit hyperactivity disorder.
12 Describe techniques of helping children with attention deficit hyperactivity disorder to adjust to the school setting.
13 Compare and contrast the characteristics of bulimia nervosa and anorexia nervosa.
 , p. 748)
, p. 748) , p. 748)
, p. 748) http://evolve.elsevier.com/Leifer
http://evolve.elsevier.com/Leifer
The Nurse’s Role
The nurse is often the person who has the greatest amount of contact with the family. Assessing child-parent relations is an important and ongoing aspect of care. To work effectively with the disturbed child, nurses first must understand the types of behavior considered within normal range. The Diagnostic and Statistical Manual of Mental Disorders (4th ed., text revision) (DSM-IV-TR) (American Psychiatric Association [APA], 2000) is a resource that defines mental disorders and is used by health professionals to aid in diagnoses of specific mental health conditions. Nurses are valuable members of the multidisciplinary health care team in that they work closely with hospitalized acutely ill children, long-term chronically ill children, and children in school. Nurses should keep a careful record of behavior and note relationships with members of the family. Such notations are meaningful to the physician and other staff members, who are as concerned with prevention of problems as they are with treating them.
Every day, everywhere, children are trying to cope with stress. Many succeed and grow stronger; some do not. Early childhood intervention programs are helpful in preventing major problems that affect growth and development. Parenting classes teach what to expect at various ages and stages. They also stress the importance of age-appropriate discipline and guidance. Parent groups provide education, socialization, and support. Other agencies provide a variety of services. Some services include the National Alliance for the Mentally Ill (NAMI), Family Service Association of America, Toughlove, and Youth Suicide National Center. Nurses must be aware of such resources to guide parents appropriately.
When parents request guidance, the nurse encourages them to seek help from their family physician or pediatrician or from a community mental health center. In the hospital, a psychiatric clinical nurse specialist (CNS) is an excellent resource. If the child is in school, the services of the school psychologist or guidance counselor may prove valuable. Some religious centers employ counselors who are available free of charge to parishioners. Families who lack adequate financial resources can be directed to the appropriate agencies. Some agencies not only provide emergency funds but also can establish a budgeting system for those receiving minimum wages. This is particularly helpful when the parents are young adolescents.
No matter how dysfunctional the parent-child relationship, most children consciously and unconsciously identify with parental values. Discrediting of the parents’ values by the health care provider threatens the child’s security and creates anxiety. The nurse reassures parents and helps them regain or maintain confidence in their parenting role. In addition, because children do not seek treatment on their own, the nurse should assist parents in becoming invested in the treatment modality. Finally, as a professional, the nurse supports organizations concerned with mental health, votes on issues that are pertinent to the welfare of children in the community, and offers services when needed.
 Nursing Tip
Nursing TipTypes and Settings of Treatment
The basic staff of the modern child guidance clinic is composed of a psychiatrist, a psychologist, a social worker, a pediatrician, and the nurse. Usually the child guidance clinic provides diagnostic and treatment services. It may be part of a hospital, school, court, or public health or welfare service, or it may be an independent agency.
The psychiatrist is a medical doctor who specializes in mental disorders. The psychoanalyst is usually a psychiatrist but may be a psychologist; all psychoanalysts have advanced training in psychoanalytic theory and practice. The clinical psychologist has an advanced degree in clinical psychology from a recognized university. Many of these specialists work in the school system with children, teachers, and families to prevent or resolve problems. A counselor is a professional with a master’s degree from an accredited institution. Many counselors specialize in a specific area, such as substance abuse or counseling of children. In most states, counselors must be licensed.
Children who do not respond well to individual outpatient therapy may require the type of care provided in residential treatment centers. Their home situations may be so disruptive that they might benefit from a change of environment. This alternative also provides a cooling-down period for the family. Family therapy is begun and includes all family members. The length of stay for the child varies from 1 to 3 weeks. Partial hospitalization programs in which the child attends therapy during the day and returns home at night are popular.
Intervention may involve individual, family, or group therapy; behavior modification; or milieu therapy. It may also involve a combination of these therapies. Behavior modification focuses on modifying specific behaviors by means of stimulus and response conditioning. Milieu therapy refers to the physical and social environment provided for the child. Art therapy, music therapy, and play therapy are particularly helpful in dealing with younger children who have difficulty expressing themselves. Recreation therapy is also valuable. Bibliotherapy, the reading of stories about children in a situation similar to the child’s situation, is also therapeutic. Creating an emotionally safe environment is basic to all forms of therapy.
Origins of Emotional and Behavioral Conditions
Early childhood experiences are critical to personality formation. Situations that disrupt family patterns can have a lasting impact on the child. Children who come from these dysfunctional families may experience any of the following: failure to develop a sense of trust (in their caregivers and environment), excessive fears, misdirected anger manifested as behavioral problems, depression, low self-esteem, lack of confidence, and feelings of lack of control over themselves and their environment. These and other manifestations may make children feel negative about themselves and the world. They experience guilt and may blame themselves when confronted with disappointment and failure.
Growing up can be painful even under the best circumstances. It is difficult for the child in the early school years to live up to so many rapidly developing standards. Guilt and anxiety develop. Finger sucking, nail biting, excessive fears, stuttering, and conduct problems are reflections of nervous tension.
The current trend toward prevention by identifying risk factors and advocating early intervention is a major goal of children’s mental health services. The term psychosomatic has come to refer to the dysfunctions of the body that seem to have an emotional or a mental basis. Each person has a different potential for coping with life. Truancy, lying, stealing, failure in school, and a crisis such as death or divorce of parents are but a few of the difficulties that may necessitate intervention. Box 33-1 summarizes some of the disorders that can affect behavior and appear during infancy, childhood, and adolescence. Some behavioral disorders are caused by genetic factors; for example, autism is thought to have autosomal recessive inheritance.
Organic Behavioral Disorders
Autism is a developmental disorder manifested by motor-sensory, cognitive, and behavioral dysfunctions. It involves impaired social interaction, communication, and interests. Autism refers to one of five disorders defined in the DSM-IV-TR (APA, 2000) as a development disorder, autistic disorder, Asperger’s disorder, and others such as Rett syndrome and disintegrative disorder (APA, 2000). It is often referred to autism spectrum disorder (ASD) (Cole, 2009). It may be caused by a defect in neurogenesis in the early weeks of fetal life, occurs in 6.69 per 1,000 children, and is more common in males.
Lack of pointing or gesturing at an early age, failure to make eye contact and look at others, poor attention behavior, poor orientation to one’s name, and repetitive behaviors are significant signs of dysfunction by 1 year of age. Research has shown that cognitive delays do not always occur. Peer-related social behavior normally develops early in the preschool period, with symbolic play normally emerging by 2 years of age. Autistic children do not show interest in other children and have difficulty engaging in pretend play. Solitary play is the preference of the autistic child.
Early identification and intervention may help the autistic child. The nurse who is alert to dysfunctions in the social behavior of young children can facilitate early referral, which may result in more meaningful social advances for the autistic child. A checklist for autism in toddlers (CHAT) can be done at 18 months of age. Many sources of information and assessment questionnaires are available online (see Online Resources at the end of the chapter). Treatment of autism involves providing well-structured home and school environments, behavior modification, and in some cases the use of specific drugs to deal with specific behavioral problems. The goal of therapy is to maximize ability to live independently.
Drug therapy of autism is not curative. Haloperidol calms the child without sedating, but it offers no help with learning abilities. Stimulants such as amphetamines decrease hyperactivity, but they impair cognition and may increase self-injurious behavior. A multidisciplinary approach to care is essential. The nurse’s role is to identify abnormal behavior as early as possible, refer for follow-up care, and monitor the side effects of prescribed medications.
The nurse’s approach to the patient should be slow paced, with few distractions. The child should be allowed to become familiar with the office, room, or equipment. Permission should be asked of the child before touching him or her, and sudden movements or loud noise should be avoided. Safety and family support are priorities. The development of meaningful language by 5 years of age is a favorable prognosis, although most autistic children require long-term care.
Obsessive-Compulsive Disorders in Children
With obsessive-compulsive disorder (OCD), a recurrent, persistent, repetitive thought invades the conscious mind (obsession), or a ritual movement or activity (not related to adapting to the environment) assumes inordinate importance (compulsion). The rituals or movements may involve touching an object, saying a certain word, or washing the hands repetitively. OCD in children differs from OCD in adults in that the symptoms are not usually part of an obsessive personality. The behavior may start as early as 4 years of age but may not be noticed as interfering with daily functioning until 10 years of age or older. Children usually are aware of their compulsive behavior and may voluntarily control themselves while in school with peers. Untreated, the problem grows to interfere with total functioning. OCD is related to depression and other psychiatric disorders such as Tourette’s syndrome; suicidal behavior is a high risk for adolescents with OCD.
OCD does not involve an impairment of cognitive function or interpersonal relationships. OCD has a genetic origin. Some research studies show involvement of the basal ganglia of the frontal lobe and a problem with the neurohormonal system. Children often become withdrawn and isolated from their peers and family. Poor school performance is related to compulsive repetitive behavior rather than a deficit in intelligence. Family conflicts arise to compound the problem. Clomipramine is one medication used to control behavior. Fluoxetine and fluvoxamine alter serotonin uptake and are effective for OCD problems.
Behavior therapy combined with medication provides the best results. The treatment involves exposure to the stressor or obsession and prevention of the compulsory response. For behavior therapy to be successful, however, the child must be motivated and capable of following directions. Parent and sibling involvement and support are essential. The nurse’s role is to assess normal growth and development and understand that ritualistic behavior that is normal at 3 years of age is normally replaced by hobbies of collecting and special interests by 8 years of age. Prolonged ritualistic behavior should be referred for follow-up care. Assessing the response to and side effects of medications used to treat OCD is an important nursing role.
Environmental or Biochemical Behavioral Disorders
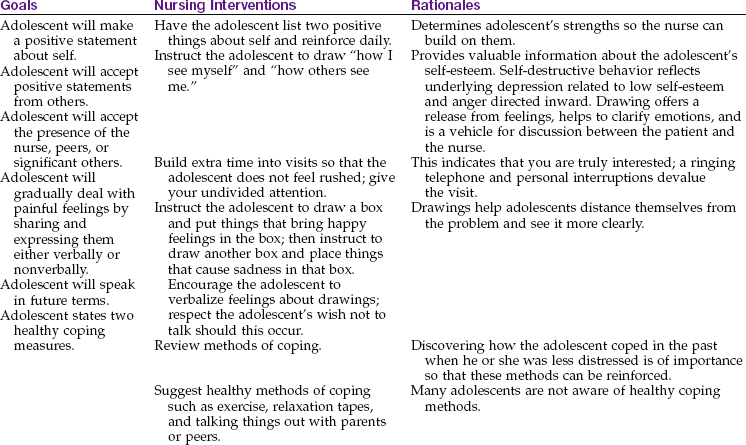
Depression in a child is not as easy to identify as depression in an adult. Many children have difficulty expressing their feelings and often “act out” their concerns. Depression is an emotion common to childhood. Sadness caused by receiving poor grades, moving to a new community, or losing a pet may trigger a depressive mood that results in either a dependent type or a disruptive type of behavior. These manifestations are resolved in a short time and are considered perfectly normal.
A major depressive or mood disorder is usually characterized by a prolonged behavioral change from baseline that interferes with schooling, family life, and/or age-specific activities. Symptoms can include loss of appetite, sleep problems, lethargy, social withdrawal, and sudden drop in grades. In young children, head banging, truancy, lying, and stealing can occur. If left untreated, depressive behavior can lead to substance abuse and/or suicide. Inheritance factors, organic factors, and environmental factors all contribute to major depressive disorders in children. Treatment of depressive disorders is often on an outpatient basis and may include prescribed drugs.
Nursing responsibilities include recognizing the signs of depression and initiating appropriate and prompt referral (Nursing Care Plan 33-1). Educating parents and school personnel concerning the identification of children at risk is an important nursing function in the community and in the hospital setting.
 Nursing Care Plan
Nursing Care Plan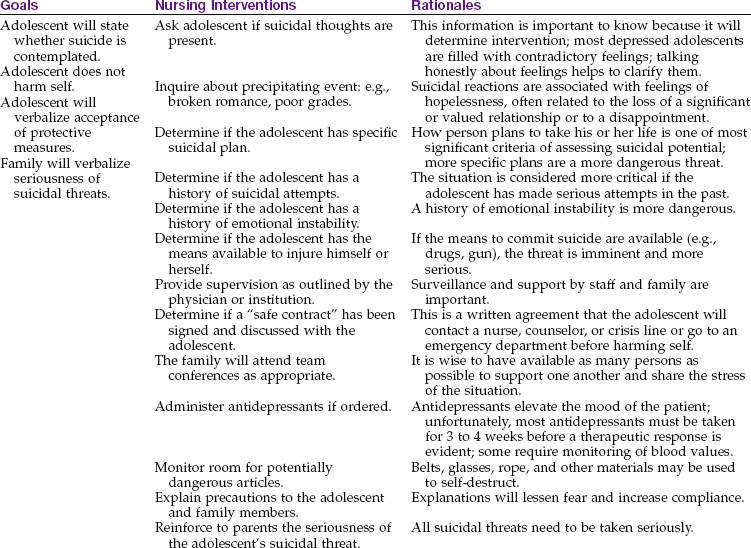
Suicide
Suicide is the third leading cause of death in adolescents after accidents and homicide. Completed suicides are more common in boys than in girls, but girls make more attempts using less lethal means. Many adolescent suicides are not intended to end in death but instead are a cry for help that may end tragically. The risk of a successful suicide increases when there is a plan of action, a means to carry out the plan, and an absence of obvious resources to turn to for help. The breakdown of family ties, pressure to succeed, or foiled relationships may trigger a low self-esteem or frustration that results in the turning of feelings of hostility or hopelessness inward.
Suicidal behaviors can be identified as suicidal ideation, which involves thoughts about suicide; suicidal gestures, which are an attempt at a suicidal action that does not result in injury; and a suicidal attempt, an action that is seriously intended to cause death (although it may be unsuccessful). Some adolescents may exhibit rage behavior or an emotional outburst that results in an impulsive act that can result in accidental death. Some adolescents display a chronic type of high-risk behavior that can lead to serious injury or death. The nurse’s role lies in education, prevention, and identification of those children at risk and prompt referral for follow-up care.
 Safety Alert!
Safety Alert!Some manifestations of suicidal behavior include a flat affect or “fixed” facial expression; a deterioration in school performance; isolation from friends and family; changes in physical appearance; giving away of cherished possessions; and talk of death. The nurse is a vital link in working with school personnel to develop peer support groups and educate families concerning the available community resources. Mental health associations, hotlines, drop-in centers, safe houses, and free clinics are community resources that can be used.
Substance Abuse
Substance abuse is the illegal use of drugs, alcohol, or tobacco for the purpose of producing an altered state of consciousness. Substances may be ingested, injected, or inhaled to produce the desired effect. Four levels of substance abuse have been established: experimentation, controlled use, abuse, and dependence. Although there is often a fine line between controlled use and abuse, frequency may be a major signal. This is especially true when accompanied by inappropriateness, such as “getting stoned” at the weekend party versus on the way to school.
There are two types of dependence: psychological and physical. Psychological dependence includes a craving for and a compulsive need to use a substance. Physical dependence occurs with drugs such as heroin and alcohol. People become “hooked on the drug” and experience physical withdrawal symptoms in addition to psychological dependence. Tolerance develops when a user’s body becomes accustomed to certain drugs. The person must then increase the dose each time to maintain its effect. Table 33-1 summarizes the characteristics of some of the more commonly abused drugs and the adolescent’s reactions to them. Table 33-2 lists street names for some of these drugs.
Table 33-1
Characteristics of Abused Drugs and Their Acute Reactions in Adolescents*
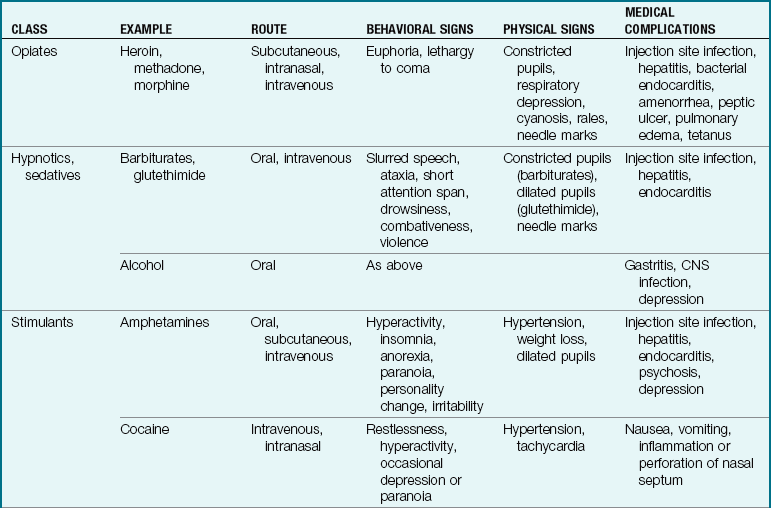
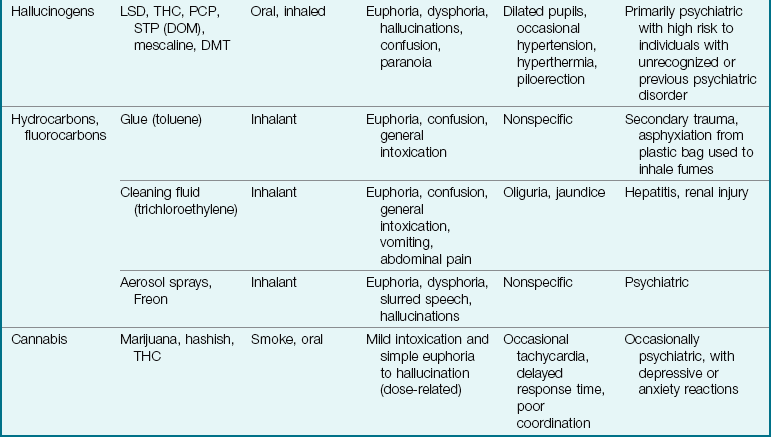
CNS, Central nervous system; DMT, dimethyltryptamine; LSD, lysergic acid diethylamide; PCP, phencyclidine hydrochloride; STP (DOM), 2,5-dimethoxy-4-methylamphetamine; THC, tetrahydrocannabinol.
*Data modified from Kliegman, R., Marcdante, K., Jenson, H., & Behrman, R. (2005). Nelson essentials of pediatrics (5th ed.). Philadelphia: Saunders.
Table 33-2
Street Names for Commonly Abused Drugs*
| STREET NAME | DRUG |
| Debs | Amphetamines |
| Apache | Fentanyl |
| Angel dust | Dimethyltryptamine (DMT) or phencyclidine hydrochloride (PCP) sprinkled over parsley or tobacco |
| Barbs | Barbiturates |
| Bin laden | Heroin (after September 11, 2001) |
| Black | Lysergic acid diethylamide (LSD) |
| Bullets | Secobarbital (Seconal) |
| Charlie | Cocaine |
| Coke | Cocaine |
| Crack | A form of cocaine |
| Crap | Heroin |
| Downers | Barbiturates or tranquilizers |
| E | Ecstasy (Methylenedioxymethamphetamine) |
| Gamma Oh | Gamma hydroxybutyrate (GHB) |
| Goof ball | Cocaine mixed with heroin; depressants |
| Horse | Heroin |
| Hospital heroin | Dilaudid |
| Joint | Marijuana cigarette |
| Kicker | Oxycontin |
| Mickey | Combination of alcohol and a hypnotic drug |
| Pot | Marijuana |
| Pikachu | Pills containing PCP and ecstasy |
| Roofies | Rohypnol |
| Smack | Heroin |
| Speed | Methamphetamine |
| Special K | Ketamine |
| Yellow jackets | Pentobarbital |
*These names often change and vary within subcultures.
Data from Office of National Drug Control Policy. “Street Terms” available at www.whitehousedrugpolicy.gov/streetterms/. Accessed December 28, 2009.
Alcohol
Experimentation with alcohol has traditionally been accepted as a normal part of growing up. Most states have legal drinking age laws that are well-defined and enforced. However, studies have shown that eighth-grade children have experimented with beverages containing alcohol. Nurses must educate the public that alcoholism is a disease with established criteria that are both treatable and preventable. The devastating physical consequences of alcohol abuse as well as the increased risk of accidents and injury should be discussed with children as early as at elementary-school age. School nurses and parent-teacher associations can work together to prevent alcohol abuse and identify alcohol abusers who can be referred for follow-up care. Al-Anon, Alateen, and Alcoholics Anonymous (AA) are programs listed in most local telephone directories in the United States, and they welcome the young adolescent seeking help with an alcohol problem. Alcoholism is often a family disease. Adults often serve alcohol freely at social events in the home and therefore offer mixed messages about alcohol use to their children.
Cocaine
The easy availability of cocaine and the affordability of “crack” cocaine are the causes of increased experimentation by children. The drug can be snorted, smoked, or used intravenously. The drug can cause life-threatening systemic responses as well as aggressive, antisocial behavior. Acute overdose can result in death. Treatment usually necessitates inpatient residential care.
Gateway Substances
Gateway substances are common household products and alcohol that can be abused to achieve an altered state of consciousness, or “high” (Figure 33-1). A feeling of euphoria can be followed by central nervous system depression, seizures, and cardiac arrest. “Huffing” substances include cleaning fluid, glue, lighter fluid, paints, shoe polish, various aerosols, and gasolines that are inhaled in various ways. They are called gateway substances because their use often leads to the abuse of stronger drugs (such as cocaine) and drug addiction.

Marijuana
Marijuana is a hemp plant (Cannabis sativa). Hashish, the portion of the plant that is most potent, is smoked or ingested and rapidly absorbed by the body and metabolized by the liver. Asthmatic children can have serious reactions because of the bronchoconstriction that occurs when smoking this substance. A loss of inhibitions, euphoria, and a loss of coordination and of goal-direction are associated with the use of this substance. Users should be referred for professional counseling.
Opiates
Heroin is the most common opiate abused by adolescents. Because opiate users often drop out of school, statistics concerning use by children in school are lacking. The main consequence of heroin abuse is related to the sharing of unsterile needles, which places the adolescent at risk for human immunodeficiency virus (HIV) infection. Hepatitis and other infections are also common among heroin users. Long-term treatment programs are the therapy of choice for adolescents.
Prevention and Nursing Goals
The prevention of substance abuse begins by helping expectant parents to develop good parenting skills. It is imperative that children learn to feel good about themselves very early in life. They need a safe environment and adults whom they can trust and who serve as good role models. As orderly development proceeds, the growing child learns to interact with others and develops a sense of identity. A positive self-image and feelings of self-worth help adolescents fine-tune their adaptive coping skills. In time they rely on their own problem-solving abilities and ideally do not need chemicals to manage the complexities of life. Nurses in their various settings can contribute to this process. They can also educate their patients about the seriousness of substance abuse.
Although it is generally true that problem drinkers cannot be helped unless they want to be helped, more intervention is now being done. Most adolescents involved in substance abuse do not choose to enter treatment but are coerced by family members or the juvenile justice system. Although the issue is controversial, clinical experience in substance abuse treatment settings has shown that many adolescents become interested in treatment and make behavioral changes after they have been required to enter a treatment program.
Children of Alcoholics
Pathophysiology: Until recently, little attention has been given to children of alcoholics. This trend is changing, and support groups such as Adult Children of Alcoholics are more numerous. This discussion is directed to young children of alcoholics, although unresolved issues are similar in adults. Pediatric nurses are in an excellent position to recognize and intervene in cases in which physical or emotional neglect exists because of parental alcoholism. These problems stem from the parents’ preoccupation with the disease. It is not unusual for both parents to be users.
Children of alcoholics are often confused by the unpredictability of family life. They do not understand why their needs are not being met. In some families there is a role reversal, with the child being forced to act maturely and make decisions ordinarily assumed by a parent. Often these children believe they are responsible for the disruptive environment. They are at high risk for emotional or physical abuse, including sexual abuse. Children of alcoholics are also strong candidates for becoming alcoholics as adults. Role models are distorted or lacking. A parent may try to cover up for the alcohol-abusing partner by lying to employers and relatives but may punish the child for the same behavior. The child may become isolated from peers while trying to avoid embarrassment at home.
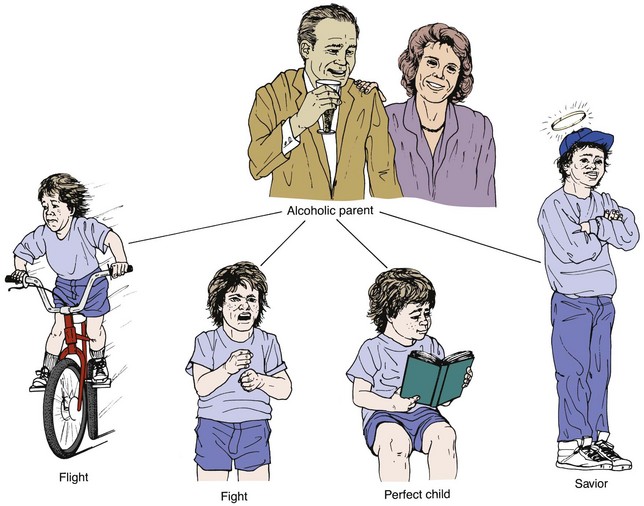
Four predominant coping patterns of children of alcoholics are flight, fight, the perfect child, and the super coper or family savior (Figure 33-2). The child who flees may do so literally or emotionally. The goal is to get away; as the child grows older, more and more time is spent away from home. Feelings are buried and left unexpressed. The child fighter is aggressive and displays acting-out behavior. The perfect child tries to gain love by never causing any trouble; he or she is obedient and is generally a good student. The savior or super coper feels overly responsible, often has a job to help out, and tries to do everything perfectly.
Manifestations, Nursing Care, and Treatment: Early recognition of and intervention for children of alcoholics are paramount. The astute nurse with a heightened awareness of alcoholism can expand admission observations and nursing history. Some clues that may or may not be related to this problem include a refusal to talk about family life, poor school grades or overachievement, an unusual need to please, fatigue, passive or acting-out behavior, or maturity beyond the child’s years. Treatment is multifold. One immediate priority is to teach the child how to get help in an emergency and to put him or her in touch with someone from the extended family, the school, or another suitable agency. Cultural diversities must be incorporated into treatment plans.
Attention Deficit Hyperactivity Disorder
Pathophysiology: Attention deficit hyperactivity disorder (ADHD) refers to a developmentally inappropriate degree of gross motor activity, impulsivity, and inattention in the school or home setting that begins before age 7 years, lasts more than 6 months, and is not related to the existence of any other central nervous system illness. It is more common in boys than in girls. It occurs more often in some families, which suggests a genetic connection. The DSM-IV-TR (APA, 2000) has defined the condition precisely and has established specific criteria for diagnosis.
Learning disability is an educational term; however, learning disabilities often occur in children with ADHD. Although these children may have average or above-average intellectual ability, they experience difficulties in areas such as the following:
• Receptive language: listening and understanding
• Expressive language: an inability to express ideas
• Information processing: differentiating words that look or sound alike
• Memory: remembering personal information or spelling
• Motor coordination: copying forms, printing, writing
• Orientation: confusing left and right
• Behavioral problem: difficulty in concentrating, impatience
A quick office tool used to identify children who have learning disabilities has been developed called the Einstein Evaluation of School-Related Skills. It tests reading, math, auditory memory, language, visual function, and motor function. It can be given as a screening tool in the clinic to children in kindergarten through fifth grade. Early intervention can help the child reach his or her full potential.
Dyslexia (reading difficulties) and dysgraphia (writing difficulties) may be apparent. These children may transpose letters; for example, they may read “pot” for “top.” They may also have difficulty in expressing themselves.
Manifestations: The symptoms of ADHD as defined by the DSM-IV-TR (APA, 2000), usually occur before 7 years of age and are summarized as follows:
• Inattention (at least three of the following): is easily distracted, needs a calm atmosphere in which to work, fails to complete work, does not appear to listen, has difficulty concentrating unless instruction is one-to-one, needs information repeated
• Impulsivity (at least three of the following): is disruptive with other children, talks out in class, is extremely excitable, cannot wait turn, is overly talkative, requires a lot of supervision
• Hyperactivity (at least two of the following): climbs on furniture, fidgets, is always “on the go,” cannot stay seated, does things in a loud and noisy way
The history involves a description of the child’s behavior and responses, an observation of parenting style, and an understanding of the existing family stresses. The coping strategies of the child should be observed, and input from schoolteachers is sought. Psychologists may interpret behavior rating scales administered to the child.
The management of ADHD is multidisciplinary. Family education to manage their knowledge deficit about the condition, counseling to help the family and child cope with the problems encountered, and medication to help control some symptoms are the core of therapy. Medications such as methylphenidate (Ritalin) and dextroamphetamine (Dexedrine) may be prescribed but may interfere with alertness and cognitive ability. Emphasizing the strengths of the child rather than the problems is essential to any plan of care. Various support groups can aid parents in their coping skills. The school nurse can help teachers develop strategies for managing children with ADHD in the classroom (see Health Promotion box). Increasing positive interactions, providing tutoring, giving computer assistance, and using behavioral management strategies under the supervision of a professional psychologist are helpful approaches to care. ADHD is a chronic condition that can persist through adulthood. Some children who are “labeled” in school develop low self-esteem and antisocial behavior.
 Health Promotion
Health Promotion
Strategies for Managing the Child with ADHD in the Classroom
• Seat the child in the front of the classroom to minimize distraction.
• Whenever necessary remind the child to focus his or her attention.
Modified from Berkowitz, C. (2000). Pediatrics, a primary care approach. Philadelphia: Saunders.
Anorexia Nervosa
Pathophysiology: Anorexia nervosa (anorexia, “want of appetite,” and nervosa, “nervous”) is a form of self-starvation seen mostly in adolescent girls. Only 10% of patients with eating disorders are male. The criteria for this disorder are well outlined in the DSM-IV-TR (APA, 2000). It is characterized by the following:
• Failure to maintain the minimum normal weight for age and height (less than 85% of expected weight)
• An intense fear of gaining weight
The etiology of anorexia nervosa may be genetic. The adolescents characteristically have average to superior intelligence and are overachievers who expect to be perfect in all areas. For young people with the disorder, their own emerging sexuality is very threatening. They experience anxiety and guilt over an imagined or a real fear of intimacy. They have low self-esteem, are obedient, and are nonassertive and shy.
Families of these young people are often dysfunctional. They may exhibit such abnormal behaviors as overprotectiveness, rigidity, lack of privacy, and inability to resolve conflicts. Affluent families may be at high risk when the concept of being thinner rules and the focus is on diet and exercise.
Manifestations: The primary symptom of anorexia nervosa is severe weight loss. Adolescents who wish to be fashion models or actresses or who participate in sports, dance, or gymnastics activities may be at risk for developing an eating disorder. On physical examination, some of the following conditions may be evident: dry skin, amenorrhea, lanugo hair over the back and extremities, cold intolerance, low blood pressure, abdominal pain, and constipation.
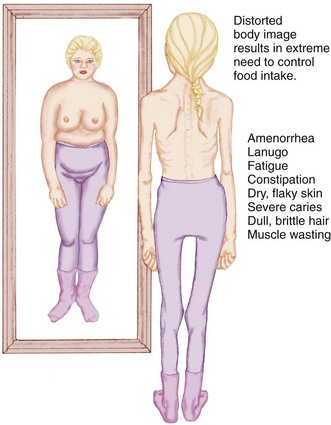
Adolescents with anorexia experience feelings of helplessness, lack of control, low self-esteem, and depression. Socialization with peers diminishes. Mealtime becomes a family battleground. The body image becomes increasingly disturbed (Figure 33-3), and there is a lack of self-identity. The young person remains egocentric and unable to complete normal adolescent tasks. Although eating less, the anorexic individual is preoccupied with food and its preparation. Hunger is denied. The patient complains of bloating and abdominal pain after ingesting small amounts of food.
Treatment and Nursing Care: The treatment of anorexia nervosa is complex and involves several modalities. Some hospitals have eating disorder units. A brief period of hospitalization may be necessary to correct electrolyte imbalance, establish a minimum restoration of nutrients, and stabilize the patient’s weight. It also provides a time-out from a dysfunctional home environment.
Therapies include individual and family psychotherapy, behavior therapy, and pharmacological therapy. Antidepressant medications may be helpful. The nurse plays an important role in ensuring that the atmosphere is relaxed and nonpunitive. Follow-up after discharge from the unit is essential. Individual and family therapy is continued.
Nurses working with adolescents in any capacity must be alert to the symptoms of this condition; a lack of recognition is one of the biggest obstacles to treatment. In the early stages, dissatisfaction with body image, amenorrhea, and social isolation are suspect. Young people must be educated about the seriousness of the disorder. Educational materials, referral sources, and counseling are available from the National Association of Anorexia Nervosa and Associated Disorders. Encouragement and support from self-help groups is also valuable.
Prognosis: Most patients gain weight in the hospital regardless of the type of therapy. However, this may not predict future success. Complications include gastritis, cardiac dysrhythmias, inflammation of the intestine, and kidney problems. Fatalities do occur, particularly in untreated persons. Approximately 50% of patients are cured, approximately 30% improve but continue to have dysfunctional eating problems and a distorted body image (although they function well in school and at work), and approximately 15% remain chronically ill through adulthood.
Bulimia
Bulimia, or compulsive eating, is recognized by the DSM-IV-TR (APA, 2000) as a separate eating disorder. It has been estimated that as many as 5% of college women and 1% of college men have this condition. It is characterized by recurrent episodes of uncontrolled binge eating followed by self-induced vomiting and the misuse of laxatives and/or diuretics.
Family dysfunctions are usually present in children with bulimia; unlike with anorexia, however, the mother-daughter relationship is usually distant or strained. Depression and alcoholism may be a family problem. The binge-purge cycle is thought to be a coping mechanism for dealing with guilt, depression, and low self-esteem. Impulsive behaviors are characteristic of adolescents with bulimia.
Persistent vomiting can cause erosion of tooth enamel and eventual tooth loss. The use of laxatives and self-induced vomiting can cause electrolyte imbalance. Muscle weakness will result if emetics are routinely used to induce vomiting. The HEADSSS (Home, Employment or Education, Activities, Drugs, Sexual activity, Suicidal ideas, Safety) format of interviewing adolescents is helpful in obtaining a detailed assessment.
The nursing role in dealing with adolescents with eating disorders is to educate, prevent, identify, and refer. It is very difficult to identify an adolescent with a weight obsession in a society in which weight and thinness define beauty. This concept is reinforced in movies and magazines. A supportive and respectful but firm manner should be maintained by the nurse. Establishing trust with the adolescent is the first step in education, referral, and treatment. Adolescents with eating disorders must maintain a sense of control in their therapy for success to be achieved. Compromise and contracts must replace authoritative restrictions on diet and activity. A referral to support groups and child and family counseling groups is helpful. A multidisciplinary approach with nurse, pediatrician, nutritionist, psychiatrist, and social worker helps to achieve a positive outcome.
Minimizing the Impact of Behavioral Disorders in Children
The primary care physician gathers data concerning behavioral problems based on the Developmental Troubleshooters Eclectic Checklist for Kids and Teenagers (D-TECKT), a comprehensive guide offering approaches to care developed by the American Academy of Pediatrics (Tellerman et al., 2005). The guide includes a database of parental concerns and an assessment of developmental issues (such as development of trust, handling separation, toddler autonomy, magical thinking of preschoolers, peer issues with school-age children, independence issues in adolescence, and sexual identity). Data concerning environmental issues, discipline techniques, family dynamics, and communication issues are also collected. Once the source of the problem is identified, a combination of mental health interventions can be implemented or the child can be referred as needed.
Effect of the Illness on Growth and Development
Children respond to traumatic events in their life and to stressors within the family, in the school, and within the peer or social group. The duration and intensity of the stressful event and the child’s coping skills determine the impact on the growth and development process. Knowledge of normal growth and development throughout childhood combined with good observation and listening skills can enable the nurse to play a major role in minimizing the negative impact of behavioral problems on growth and development. Because outpatient services play a significant role in health care today, nurses must be aware of agencies and support groups available to children with behavioral disorders and their parents. Prompt, early referral and treatment can improve the prognosis of emotional and behavioral disorders, enabling the children to reach their potential in growth and development.
Children’s behavioral problems necessitate a total family approach to care. Education of the community (school personnel), family (parents and siblings), and child is an essential nursing responsibility. Patient advocacy with a focus on prevention and long-term management are goals of care. A knowledgeable, caring, understanding, and supportive nature is valuable for any nurse caring for children with behavioral disorders.
Effect of the Illness on Siblings
Most siblings of children with emotional disorders either suffer emotional scars or develop protective coping mechanisms to deal with their experiences. Siblings of children with long-term illness are at risk for developing poor self-esteem and problems with their own peer relationships. Some siblings, however, are resilient and develop strength and positive coping mechanisms. Sibling rivalry, a competition between siblings for the attention or love of parents, is a normal part of growth and development, but guilt on the part of the other sibling enters the picture when one sibling becomes ill. Sibling rivalry teaches interactive social skills that will be used with friends and at work later in life. A child who is left at home with a baby-sitter while the parents tend to an ill sibling in the hospital may feel abandoned and often is burdened with extra household responsibilities that may add to the stress. Some children may react negatively to the stress of making dinner for the rest of the family, whereas other children react positively and develop positive self-esteem, knowing they are trusted with such a task.
The nurse can provide support for the family system, identify available resources, and collaborate with the health care team to meet total family needs.
Get Ready for the NCLEX® Examination!
Key Points
• Early childhood experiences are critical to personality formation.
• The child’s environment must be safe, and the child must be able to trust caretakers.
• Nurses play an important role in the mental and emotional assessment of children because they often have the most contact with the hospitalized child and family.
• Talk of suicide must always be taken seriously.
• The risk of suicide increases when there is a definite plan of action, the means are available, and the person has few resources for help and support.
• Substance abuse is the number one problem of American adolescents.
• Al-Anon and Alateen are two excellent resources for family members of alcoholics.
• The Diagnostic and Statistical Manual of Mental Disorders (4th ed., text revision) (DSM-IV-TR) (APA, 2000) lists specific criteria for diagnosing various mental conditions seen in children and adults.
• Attention deficit hyperactivity disorder is characterized by a developmentally inappropriate degree of gross motor activity, impulsivity, distractibility, and inattention in school or at home.
• Behavioral problems can be caused by the stresses accompanying the transition from childhood to adulthood or by genetic or biochemical factors.
• Autistic children do not show interest in other children, do not make eye contact, and do not engage in “pretend” play.
• Sudden movements and loud noises should be avoided when caring for children with autism.
• Obsessive-compulsive disorders in children do not involve impaired cognitive functioning.
• Ritualistic behavior may interfere with daily activities.
• A major depressive disorder is characterized by a prolonged behavioral change from baseline that interferes with school or age-specific activities.
• Substances abused by children and adolescents may be inhaled, injected, or ingested. The practice of sharing unsterile needles may lead to HIV infection.
• Emphasizing the strengths of the child rather than the weaknesses is essential when caring for a child with a behavioral disorder.
• Anorexia nervosa can lead to starvation and death.
• Bulimia is an eating disorder that involves bingeing and purging and can result in deterioration of teeth and electrolyte imbalance.
• Education, prevention, identification, and referral are essential nursing functions in the care of the child with a behavioral disorder.
Additional Learning Resources
 Go to your Study Guide for additional learning activities to help you master this chapter content.
Go to your Study Guide for additional learning activities to help you master this chapter content.
Go to your Evolve website (http://evolve.elsevier.com/Leifer) for the following FREE learning resources:
• Answer Guidelines for Critical Thinking Questions
• Answers and Rationales for Review Questions for the NCLEX® Examination
• Glossary with English and Spanish pronunciations
• Interactive Review Questions for the NCLEX® Examination
• Patient Teaching Plans in English and Spanish
 Online Resources
Online Resources• Agency for Healthcare Research and Quality: http://ahrq.gov/clinic
• Autism Research Center: www.autismresearchcenter.com
• Autism Society: www.autism-society.org
• International Dyslexia Association: www.interdys.org
• National Association of Anorexia Nervosa and Associated Disorders: www.anad.org
• National Center for Learning Disabilities: www.ncld.org
• Office of National Drug Control Policy: www.whitehousedrugpolicy.gov/pdf/street_terms.pdf
• Signs of Autism: www.firstsigns.org; www.cdc.gov/ncbddd/autism/index.htm; www.autismspeaks.org
Review Questions for the NCLEX® Examination
1. The adolescent with anorexia nervosa has a body self-image characteristically expressed by:
1. wearing tight clothing to emphasize thinness.
2. increasing elation as weight is lost.
2. A priority goal in the approach to a child with anorexia nervosa is to:
3. A child with suspected bulimia should be assessed for:
4. An important approach to the care for a 7-year-old child diagnosed with attention deficit hyperactivity disorder (ADHD) is to encourage:
5. When assessing an 8-year-old child with obsessive-compulsive disorder (OCD), the nurse would expect to find: