Pharyngeal Pouches, Membranes, and Clefts
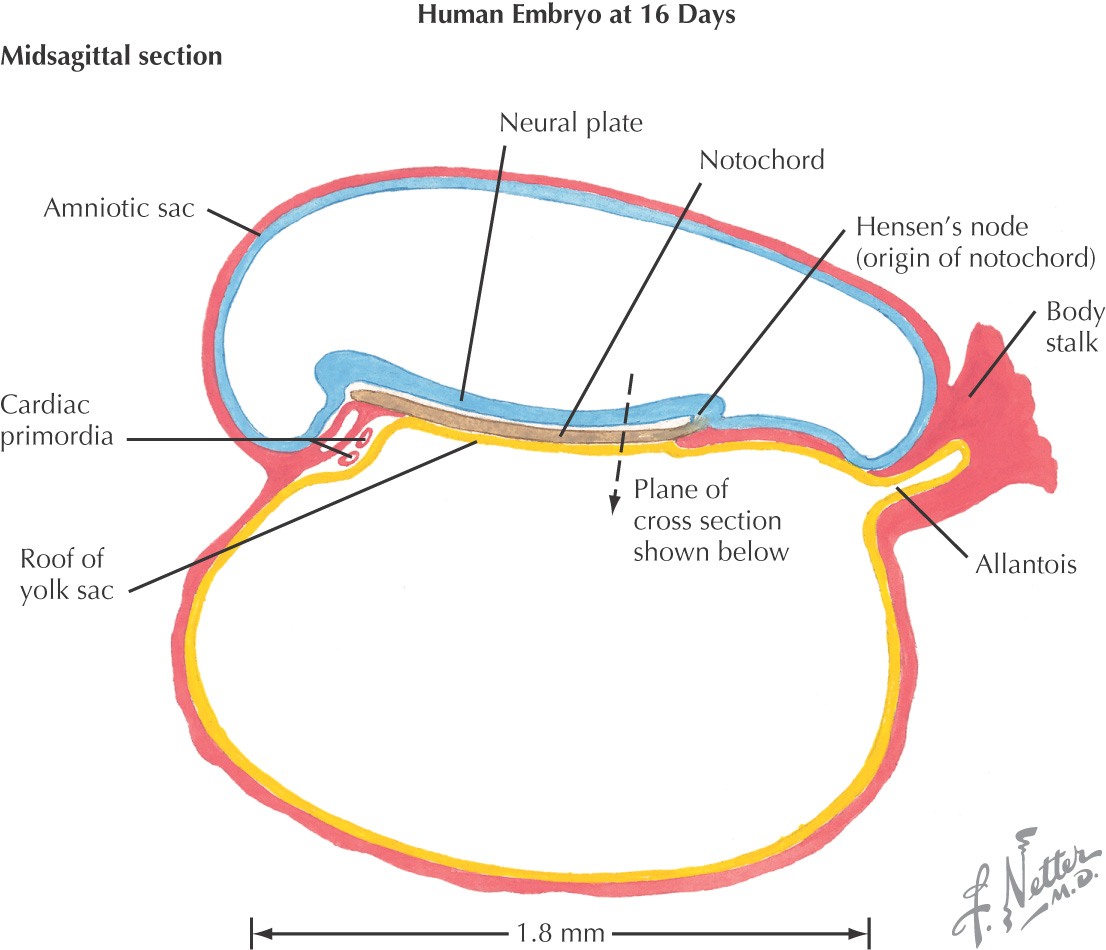
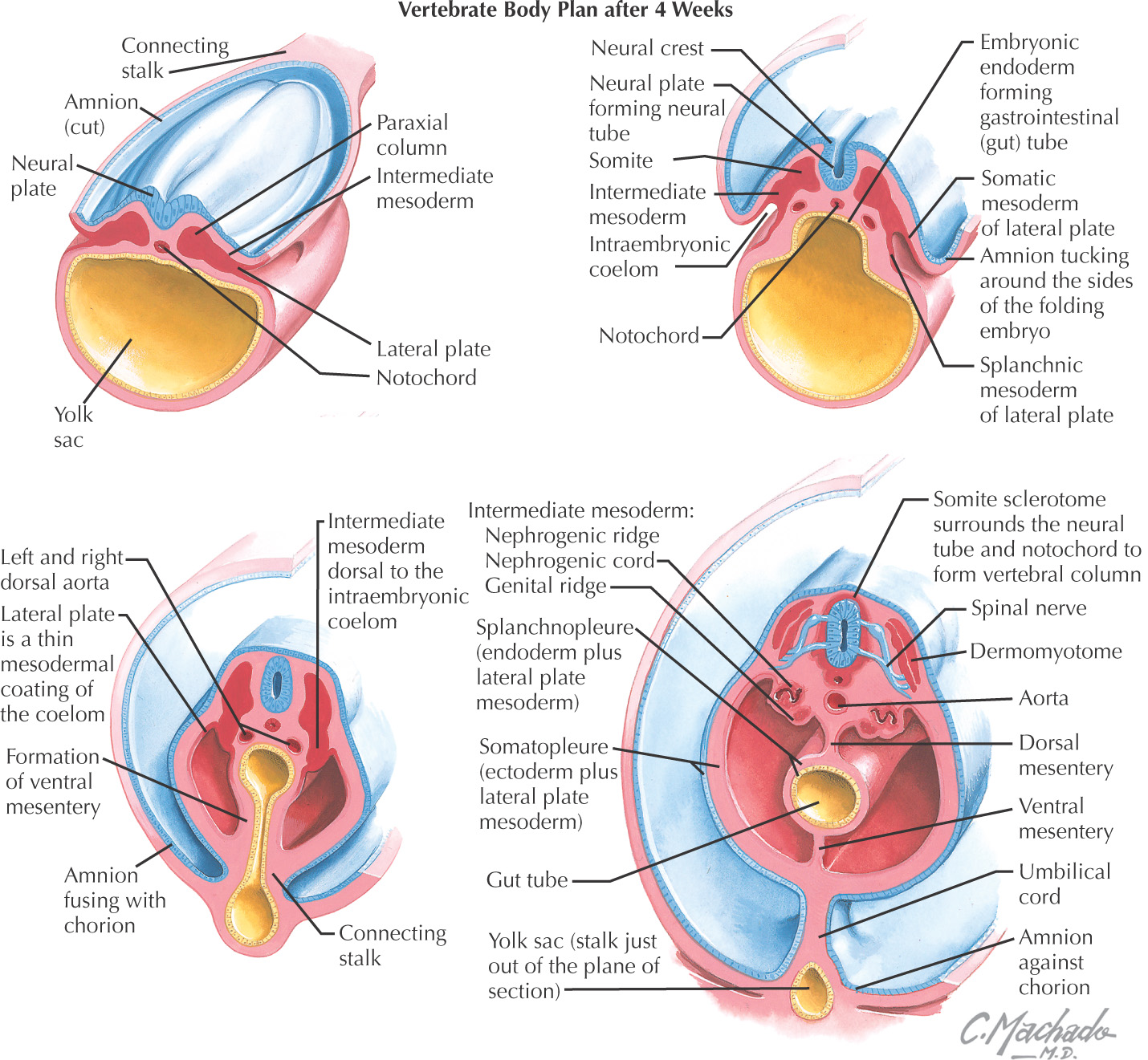
3 major germ layers form the initial developing embryo:
Mesoderm differentiates into:
Ectoderm gives rise to 2 layers:
The head and neck are formed by:
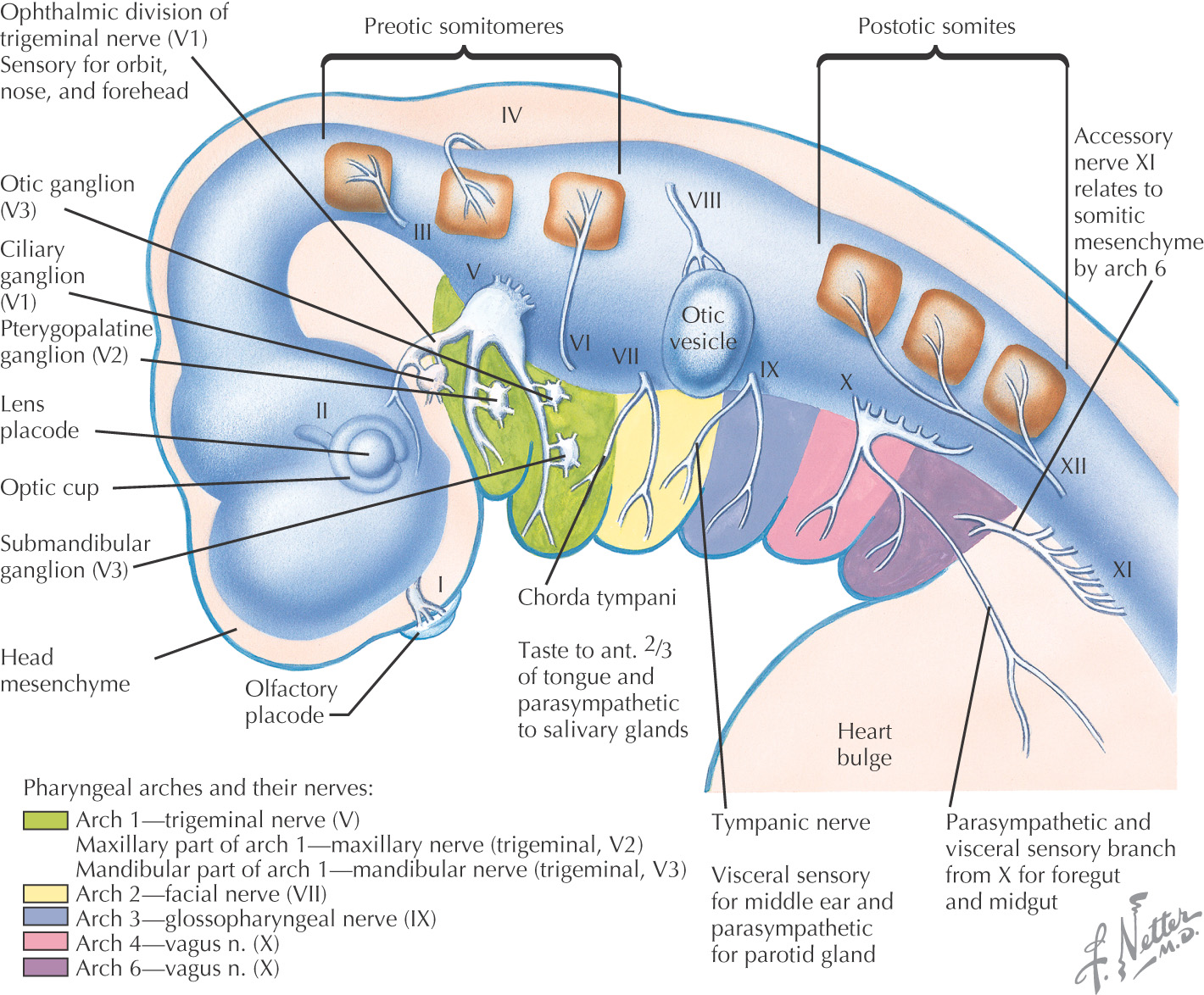
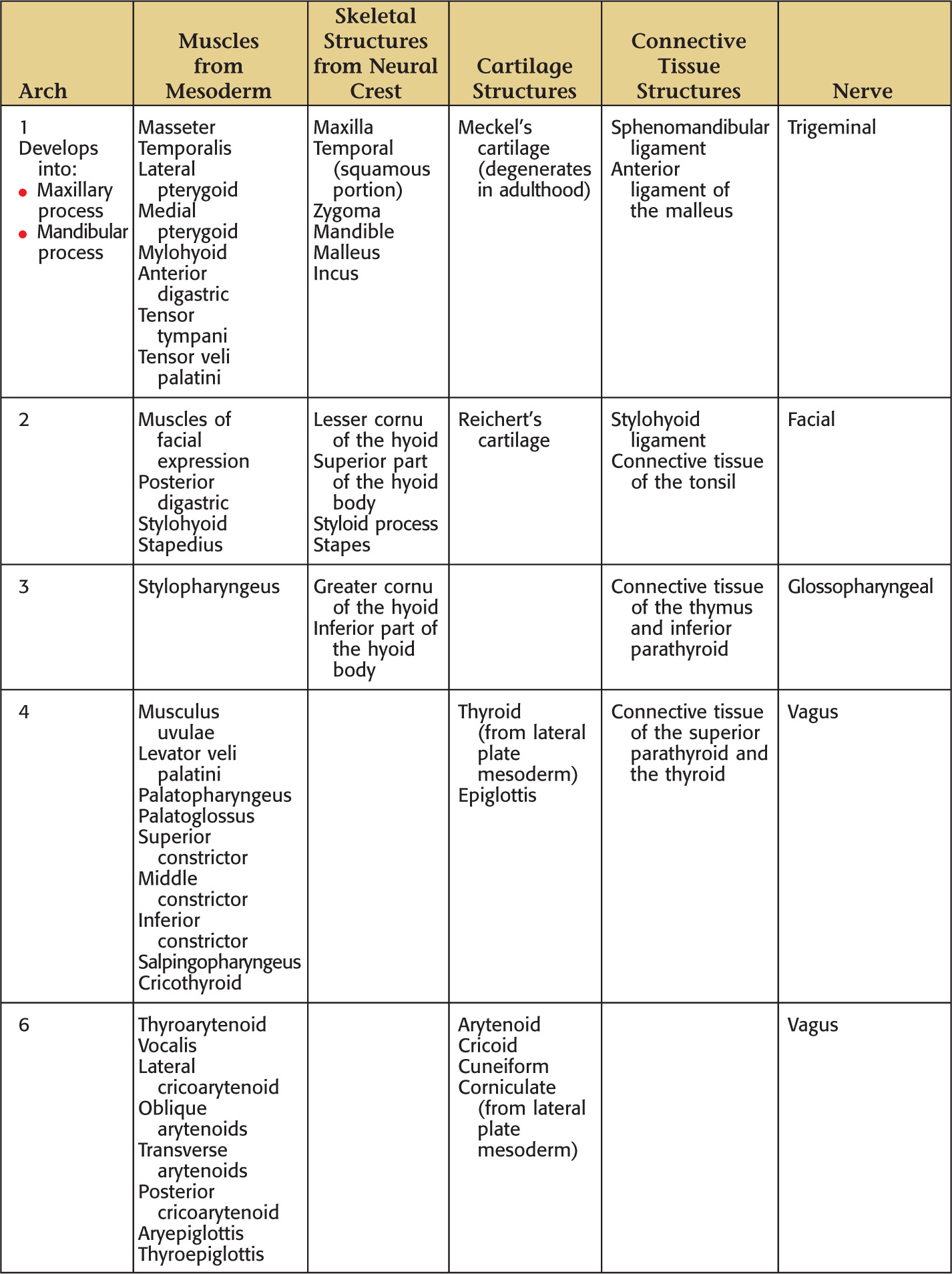
Most of the head and neck is formed from the pharyngeal arches

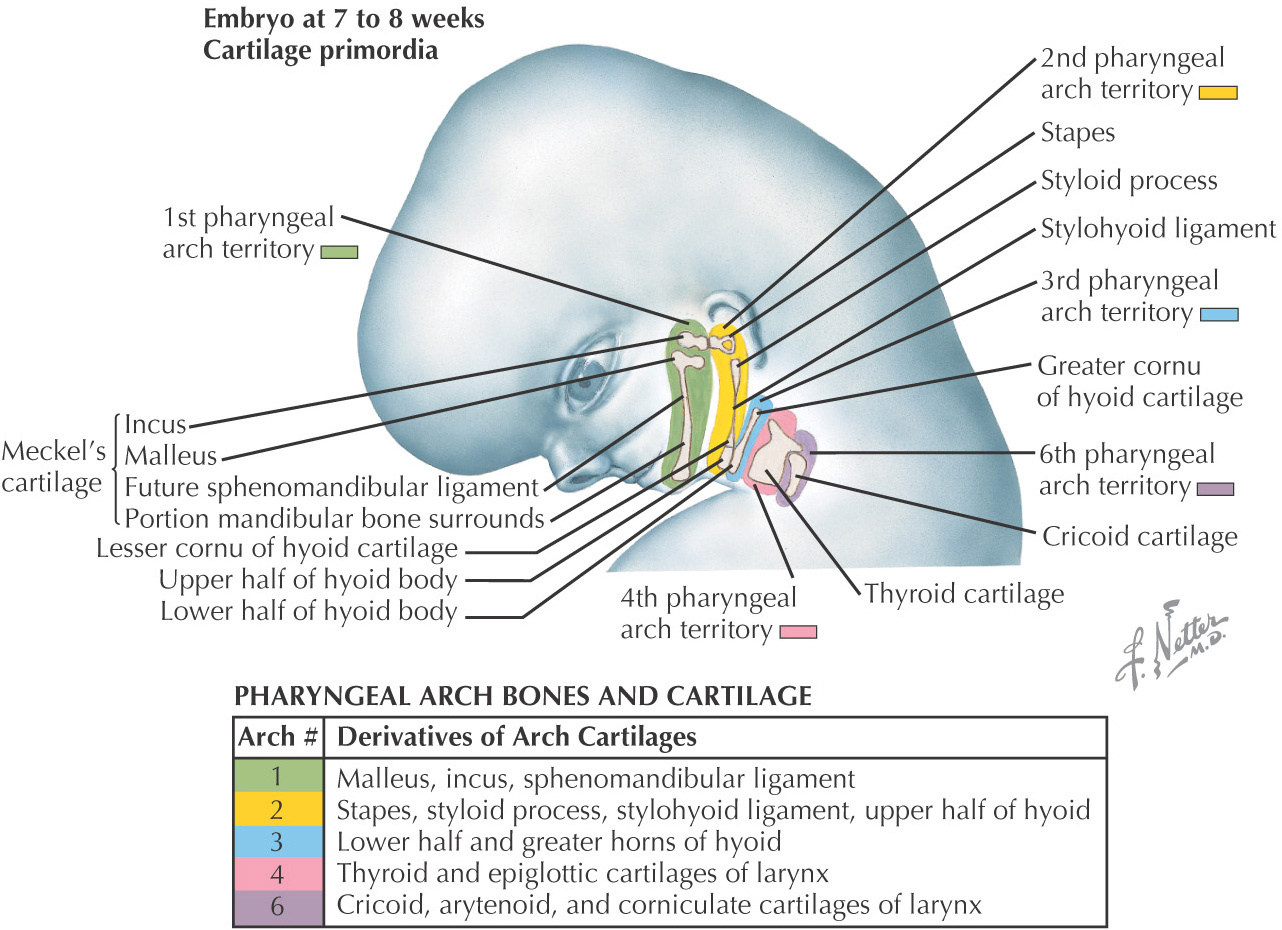
Start forming in the 4th week of development
Develop as blocks separated by pharyngeal clefts
Initially, 6 arches develop, but the 5th regresses
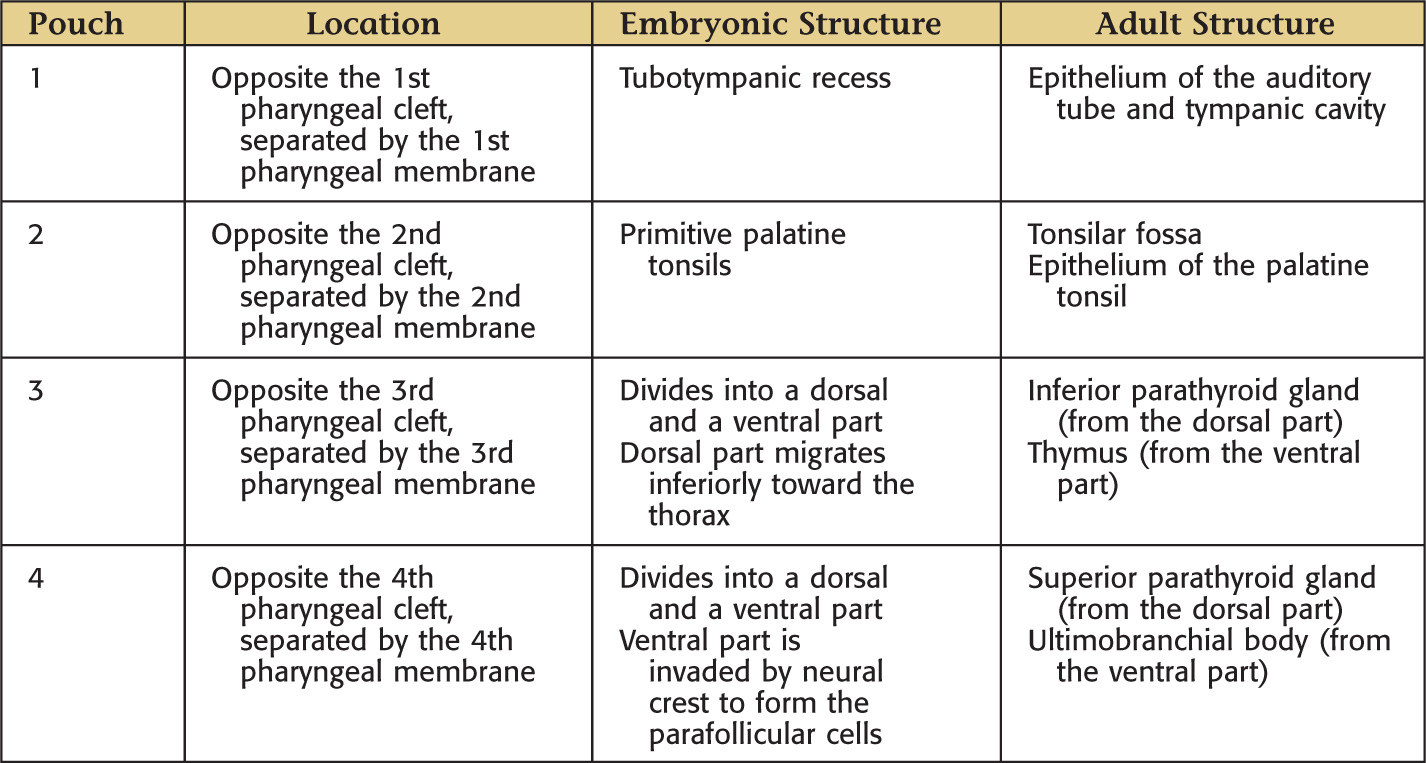
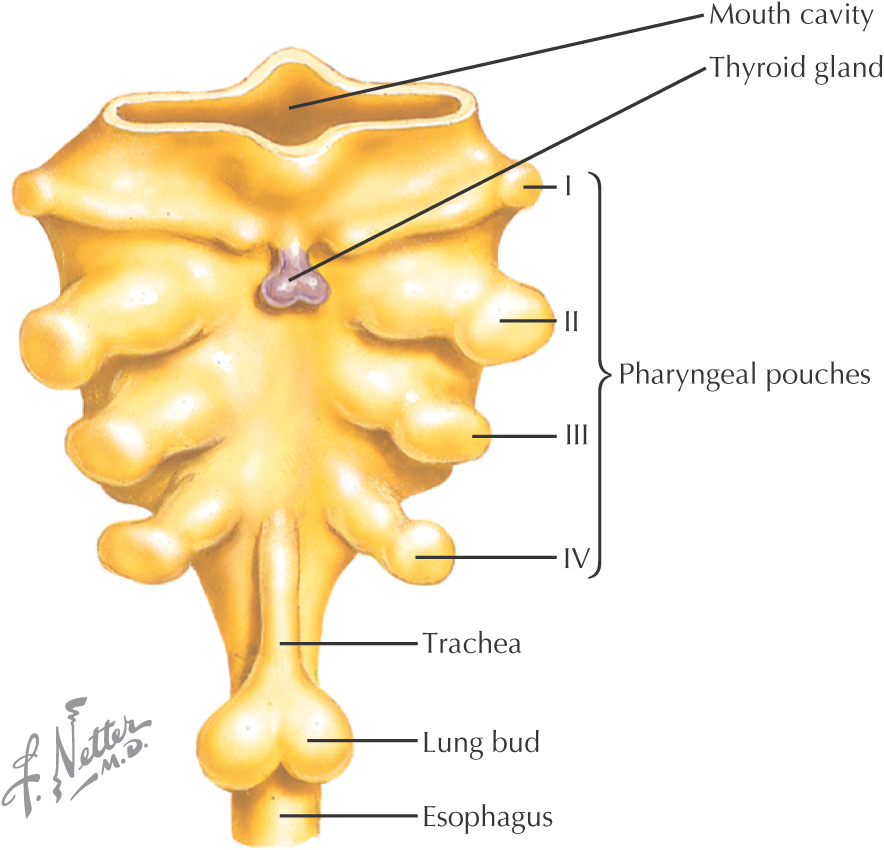
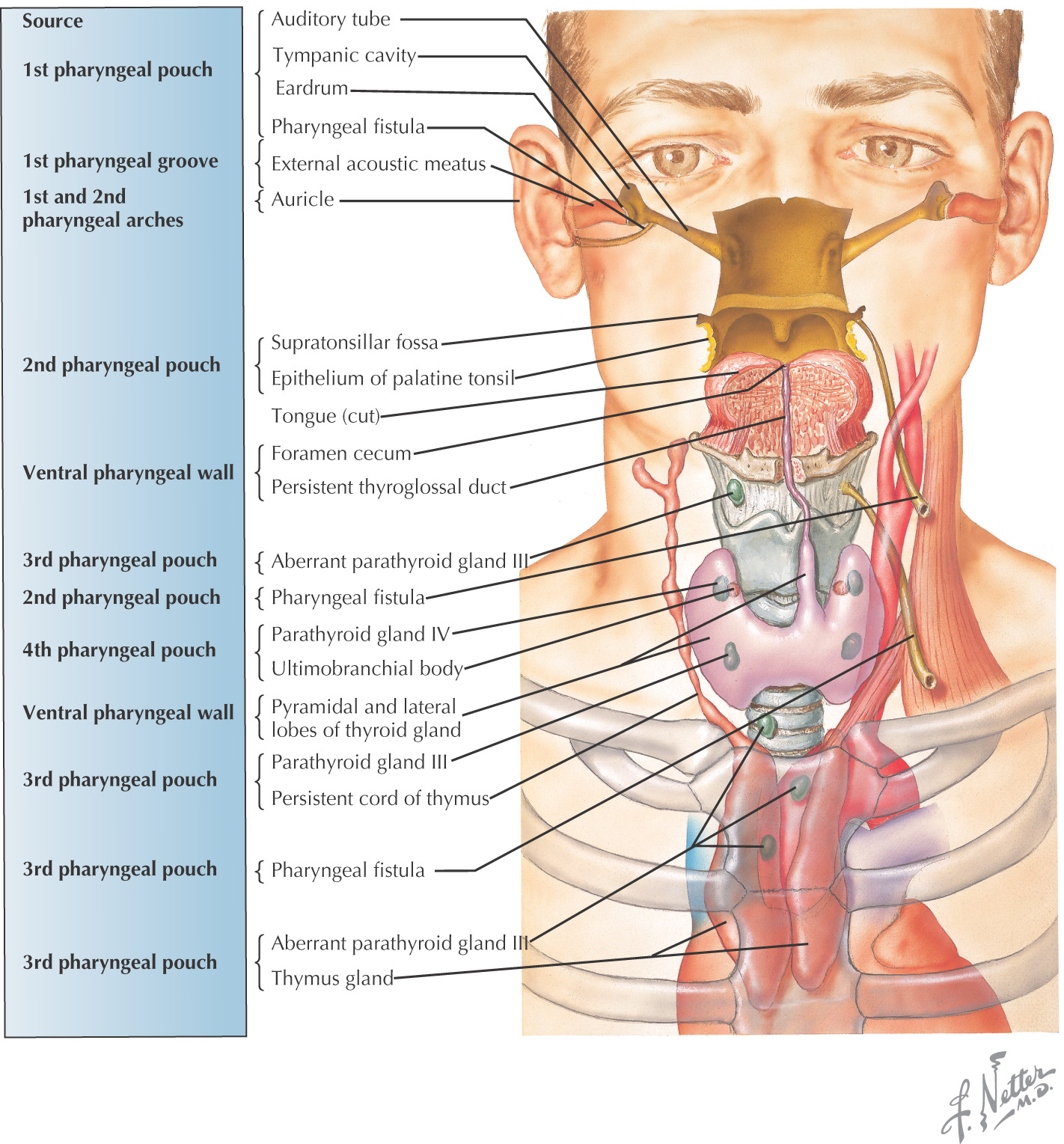
Arising from the endoderm are compartments called pharyngeal pouches that extend toward the pharyngeal clefts
Help form 4 of the 5 swellings of the face:
• 2 mandibular processes (pharyngeal arch)
• 2 maxillary processes (pharyngeal arch)
Composed of:
• Central part–lateral plate mesoderm, paraxial mesoderm, neural crest
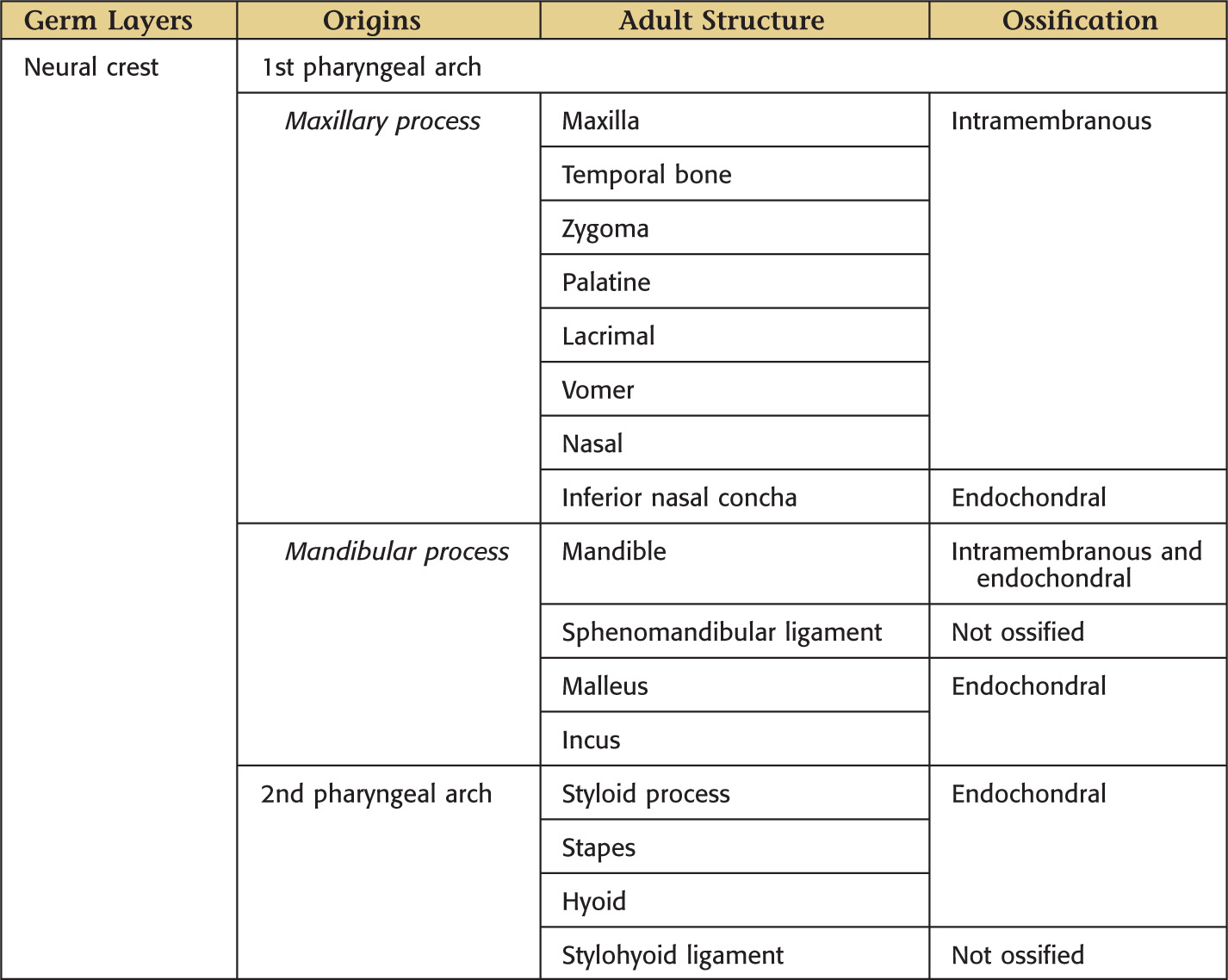
Skeletal components develop from the neural crest tissue
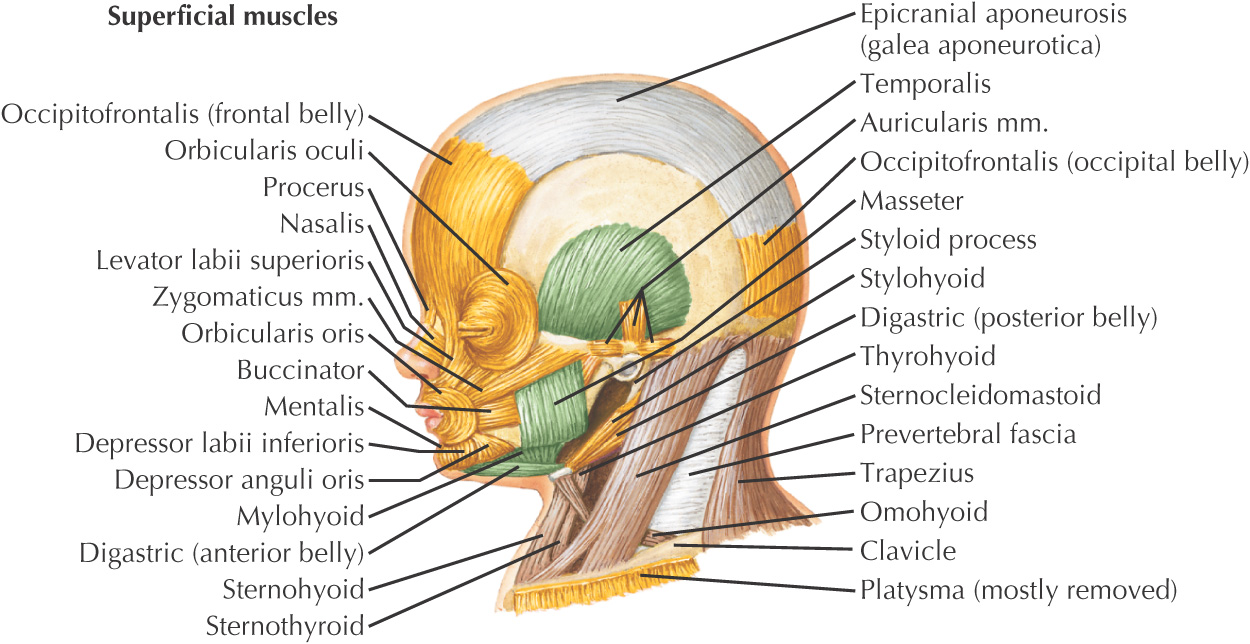
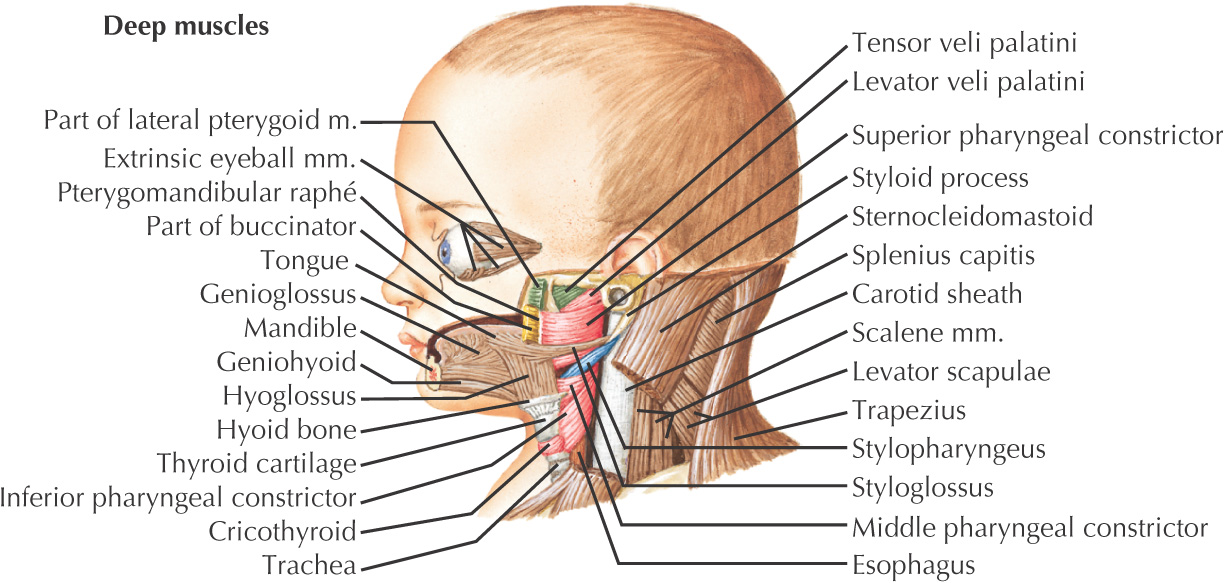
Muscular structures develop collectively from the mesoderm
Each arch is innervated by a cranial nerve that migrates with the muscles
Pharyngeal pouches—4 develop from endoderm
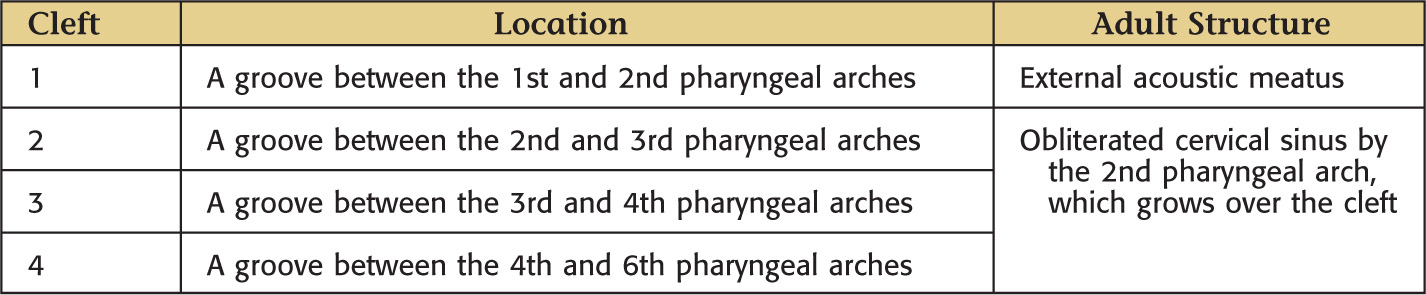
Pharyngeal clefts—each is a groove formed from ectoderm
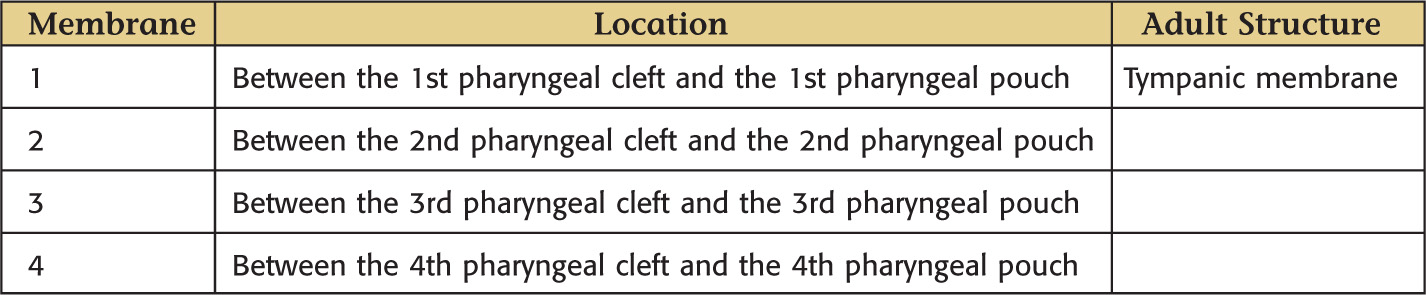
Pharyngeal membranes—each is composed of tissue located between a pharyngeal pouch and a pharyngeal cleft; composed of external ectoderm, mesoderm and neural crest in the core, and an internal endoderm lining
Skull is formed from:
• Lateral plate mesoderm (neck region)
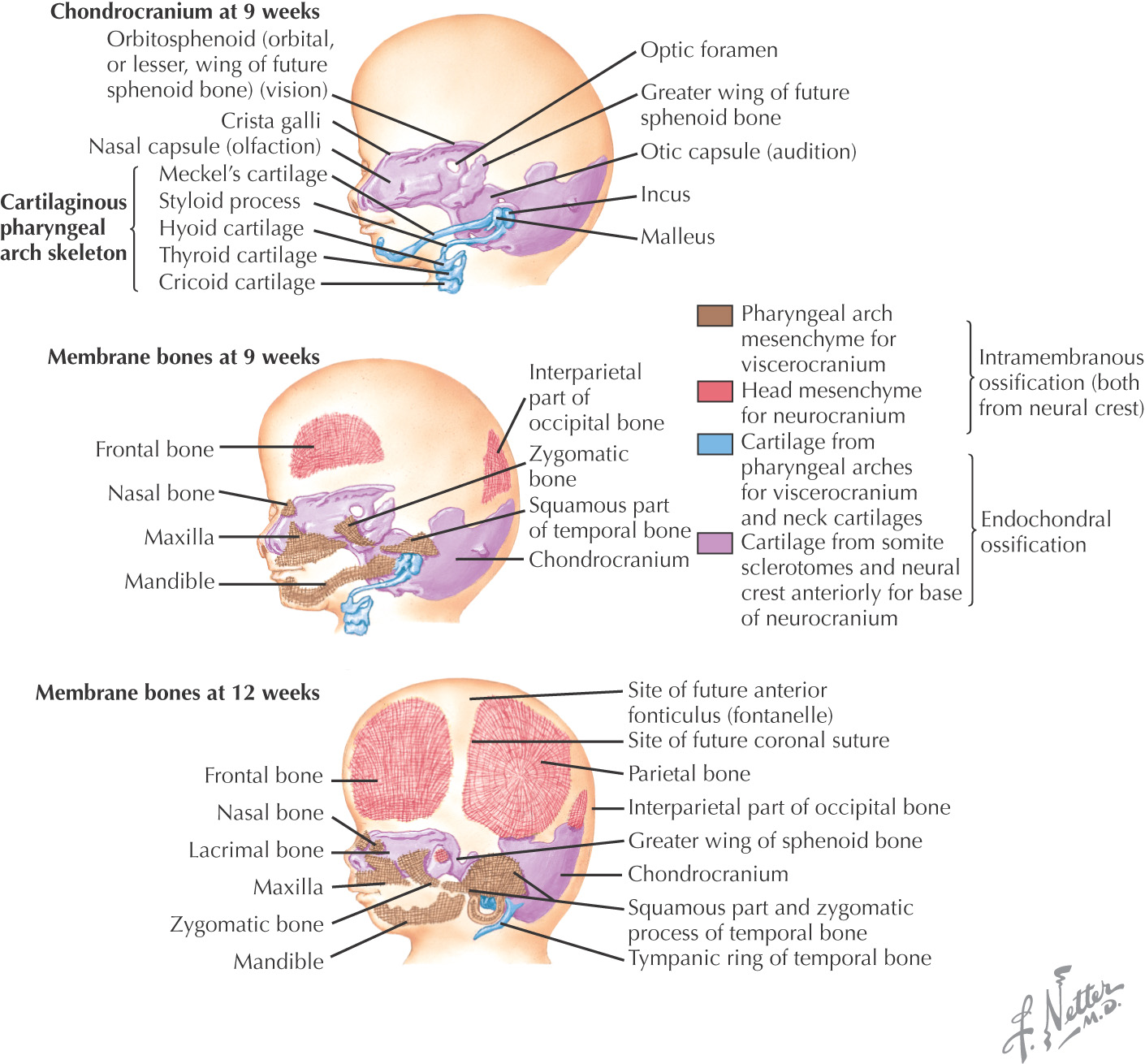
Bony skull is formed by either of 2 mechanisms:
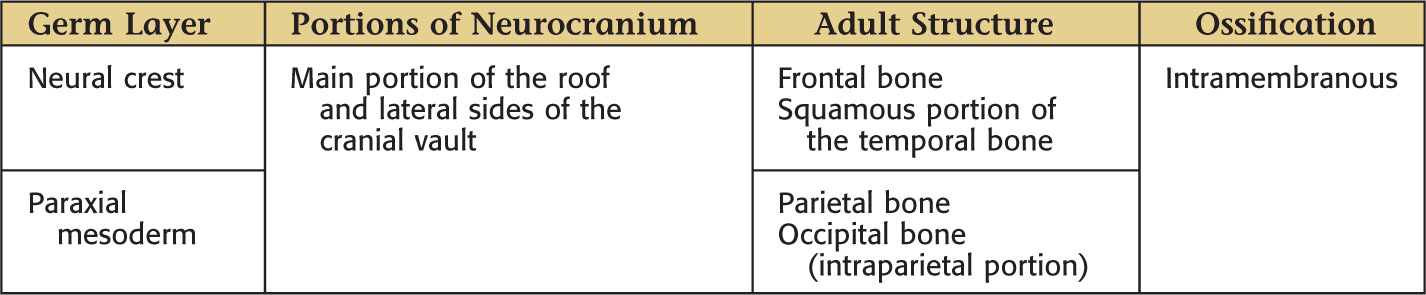
• Intramembranous ossification
Skull development is divided into 2 parts:
• Viscerocranium—forms the bones of the face
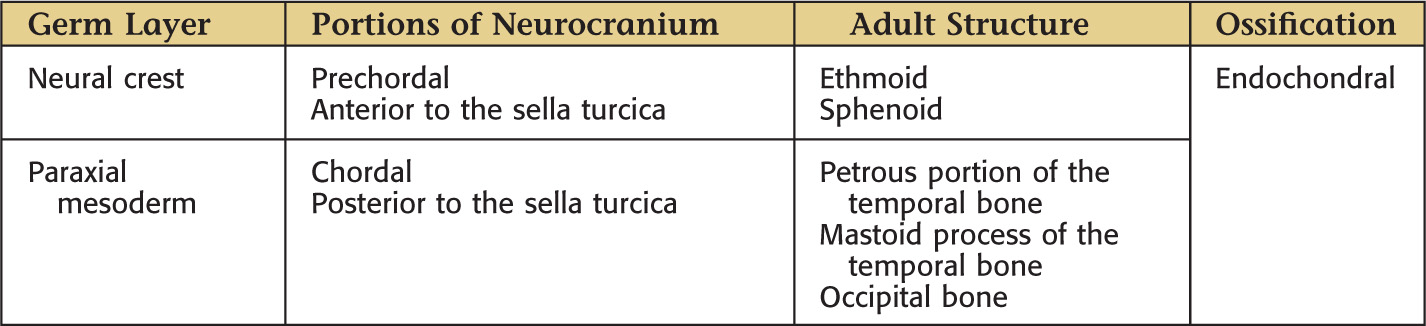
• Neurocranium—forms the bones of the cranial base and cranial vault and can be divided into membranous neurocranium and cartilaginous neurocranium
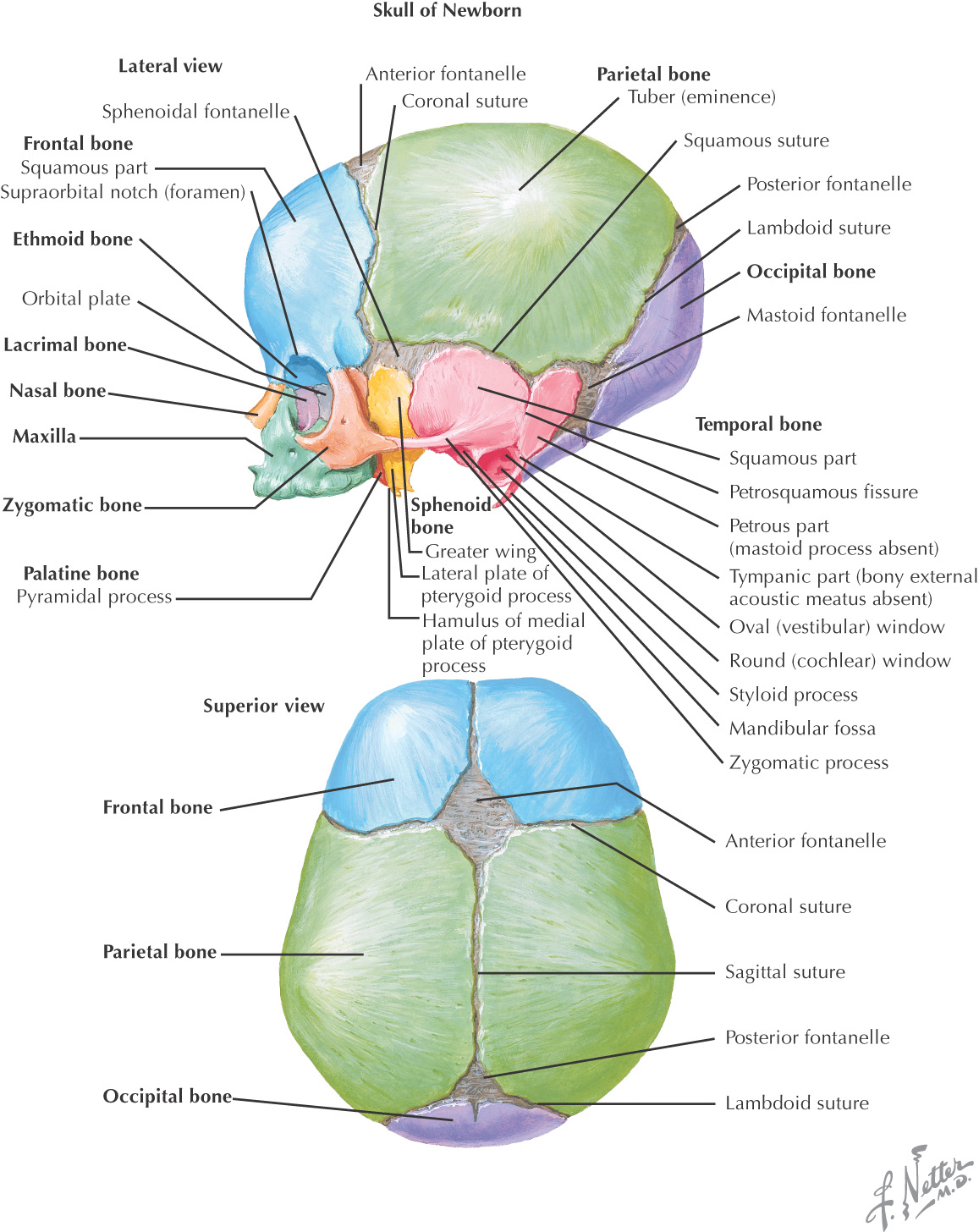
Fontanelle |
Time of Closure |
Anterior fontanelle (bregma) |
4–26 months |
Posterior fontanelle (lambda) |
1–2 months |
Sphenoidal fontanelle (pterion) |
2–3 months |
Mastoid fontanelle (asterion) |
12–18 months |
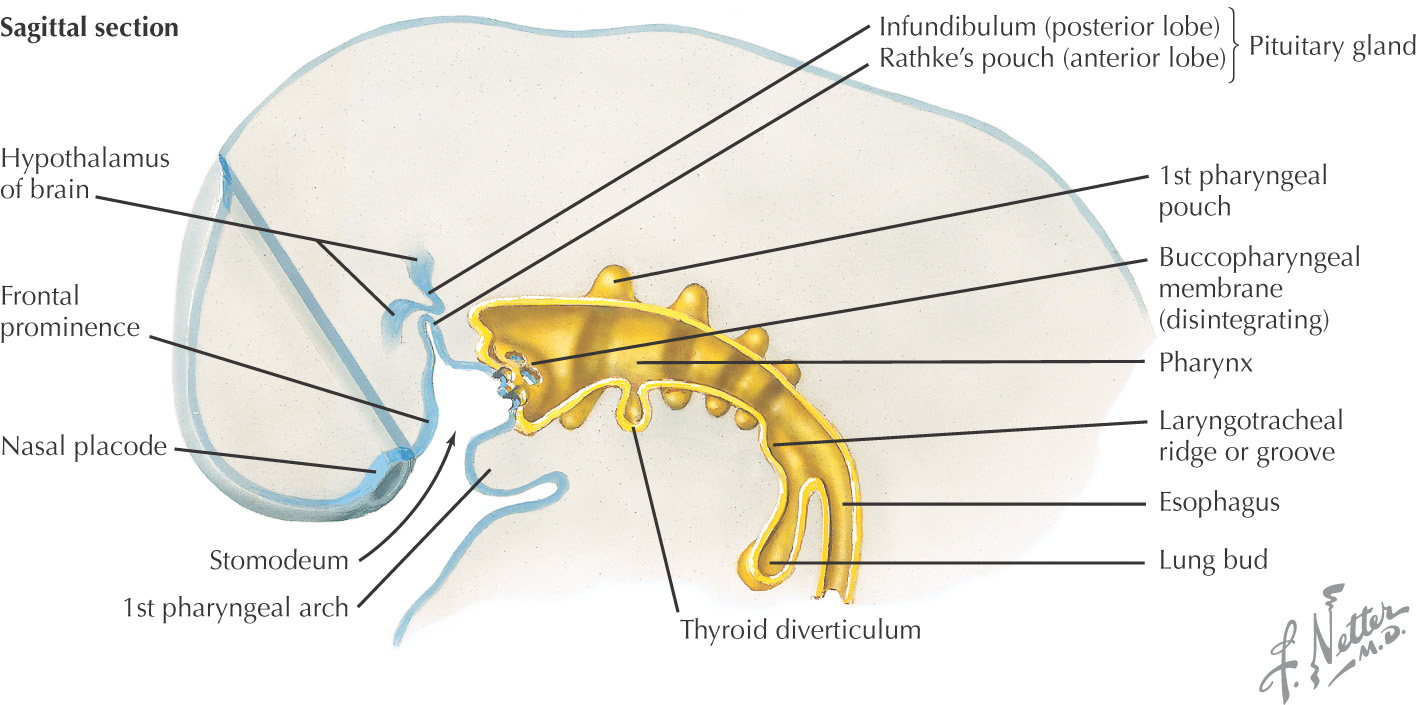
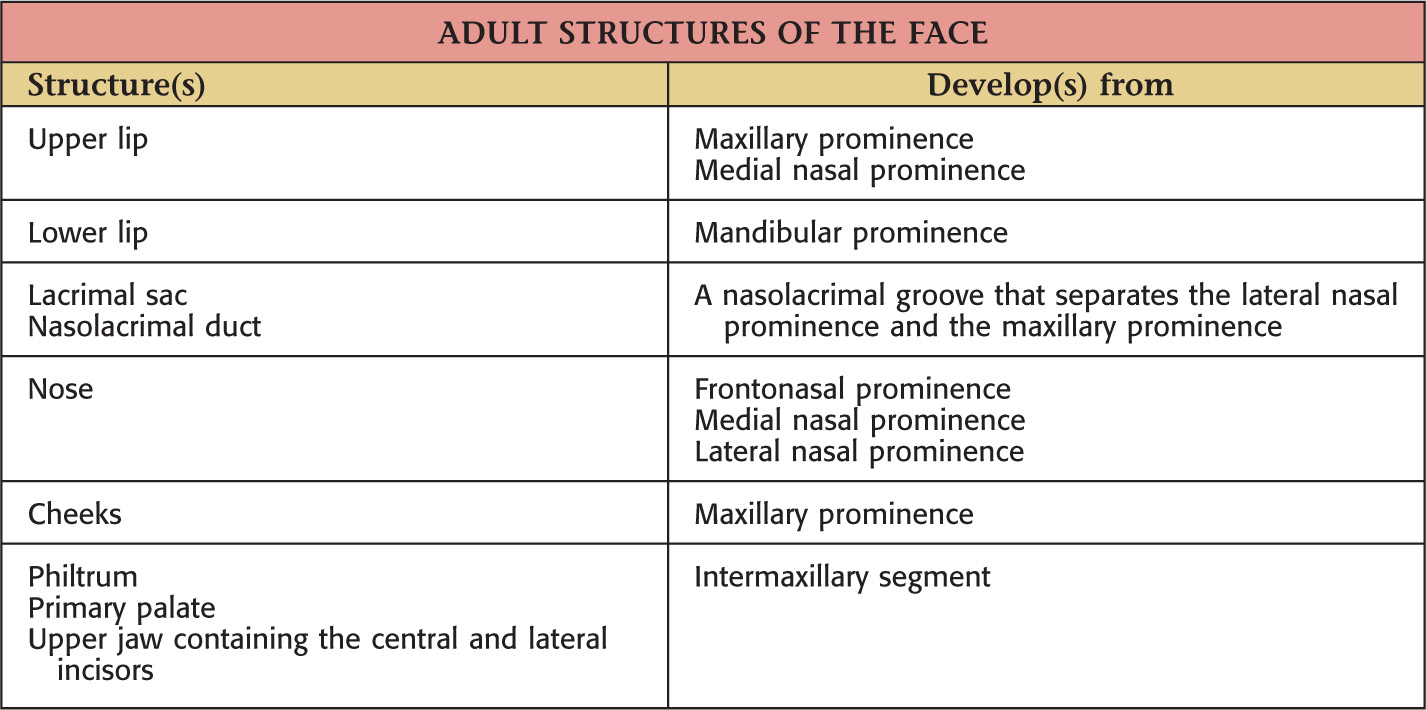
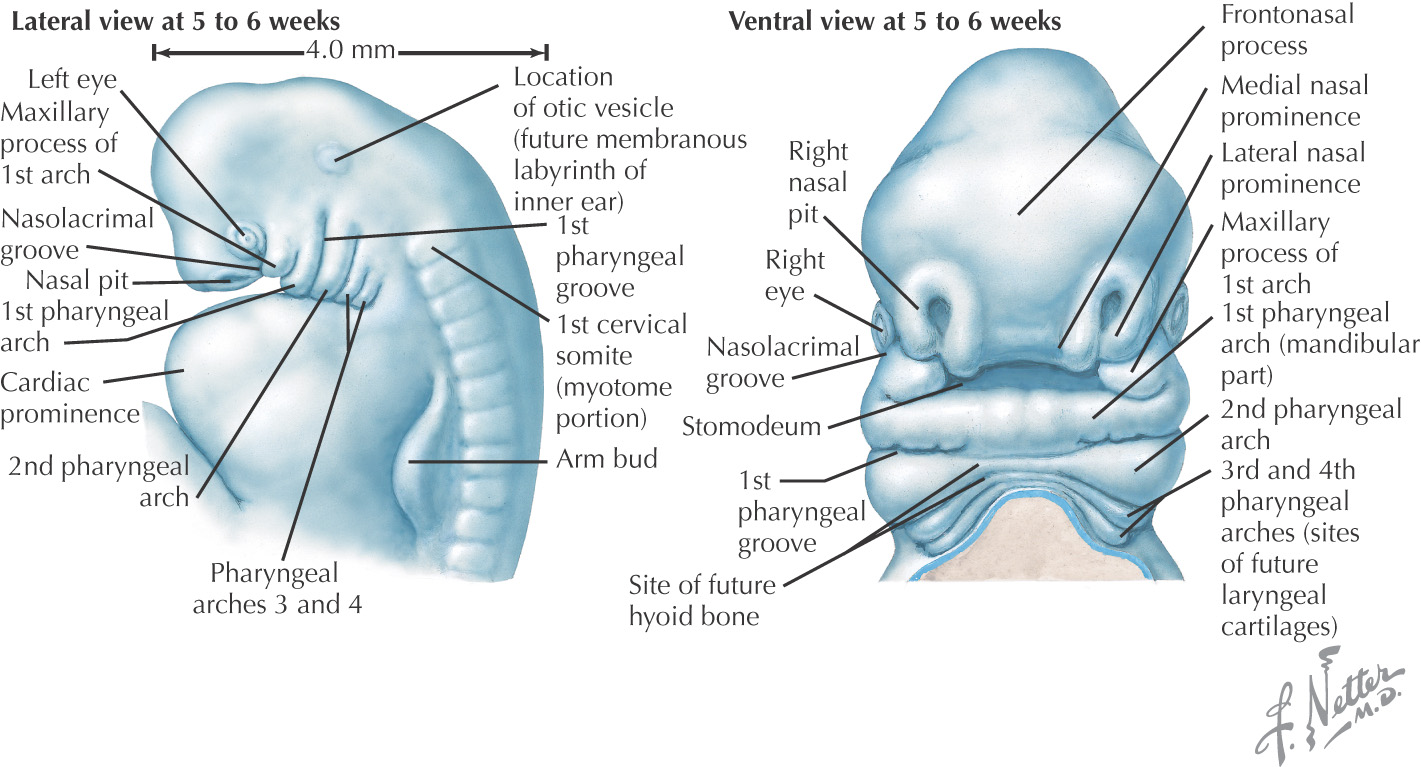
The face is formed mainly from neural crest, which makes 3 swellings that surround the stomodeum:
• Maxillary prominence (from the 1st pharyngeal arch)
• Mandibular prominence (from the 1st pharyngeal arch)
Lateral to the frontonasal prominence, 2 additional areas of ectoderm form the 2 nasal placodes that invaginate in the center to form nasal pits, creating ridges of tissue on either side of the pits:
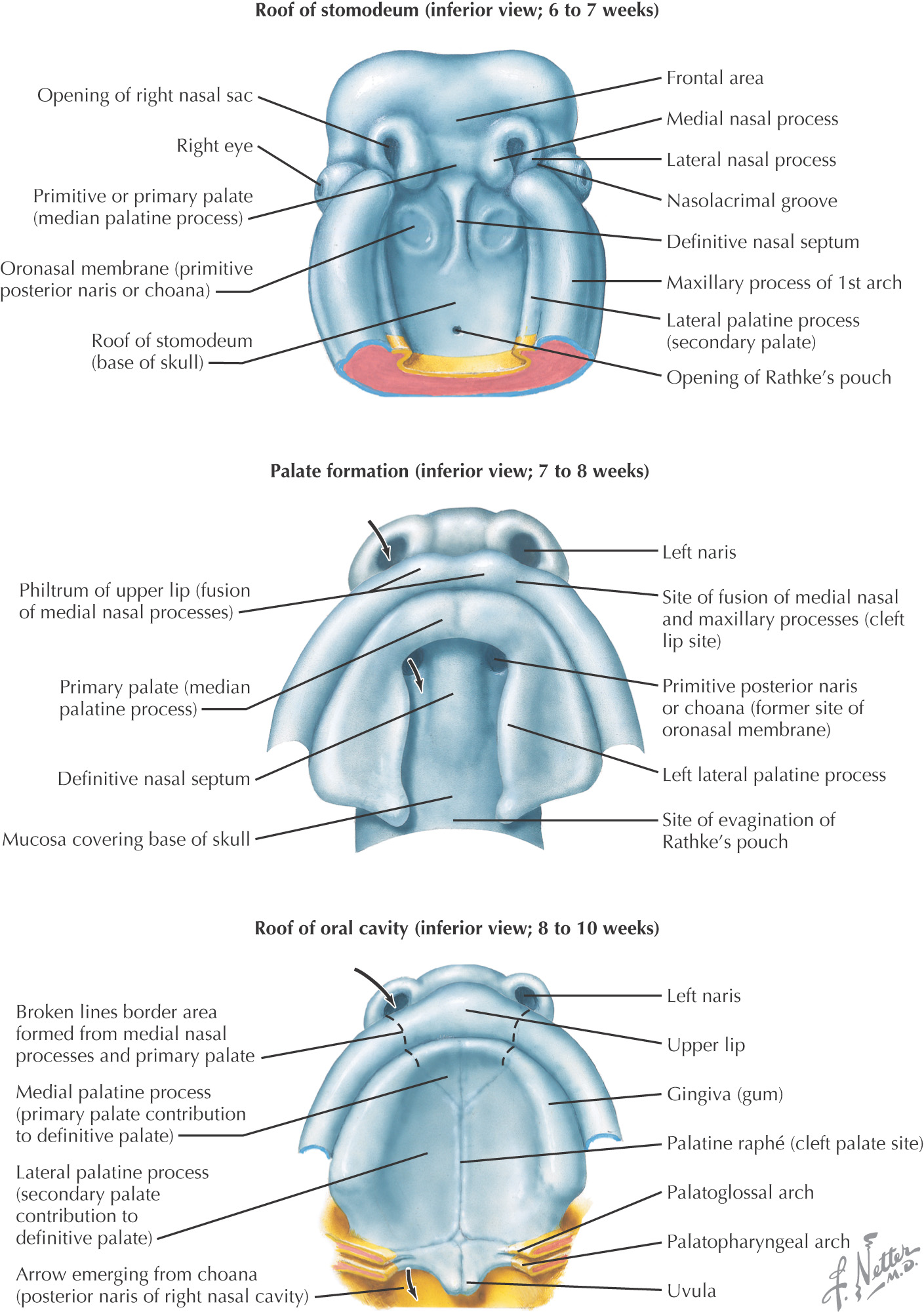
Fusion of the medial nasal prominences at the midline results in formation of the intermaxillary segment
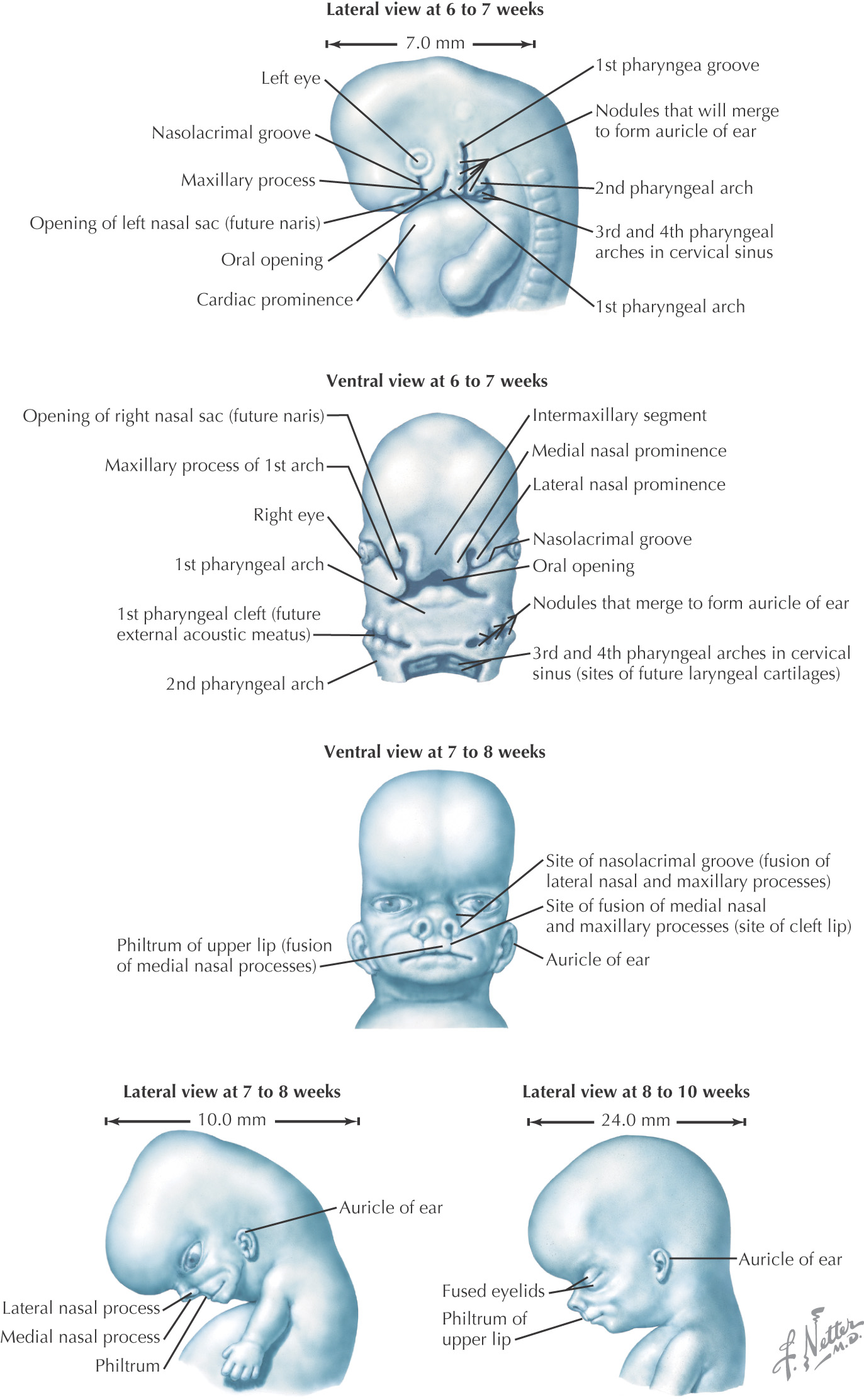
Formed by the:
• Primary palate (intermaxillary segment)
• Secondary palate (protrusions from the maxillary prominences)
Intermaxillary segment: the initial portion of the palate in development; contains the central and lateral incisors
Swellings of the maxillary prominence form shelves that project medially and are separated by the tongue
When the tongue no longer occupies the space between the palatal shelves, these processes fuse together to form the secondary palate
The primary and secondary palatal tissues all meet at the incisive foramen
Primary and secondary palates and the nasal septum fuse to form the definitive palate
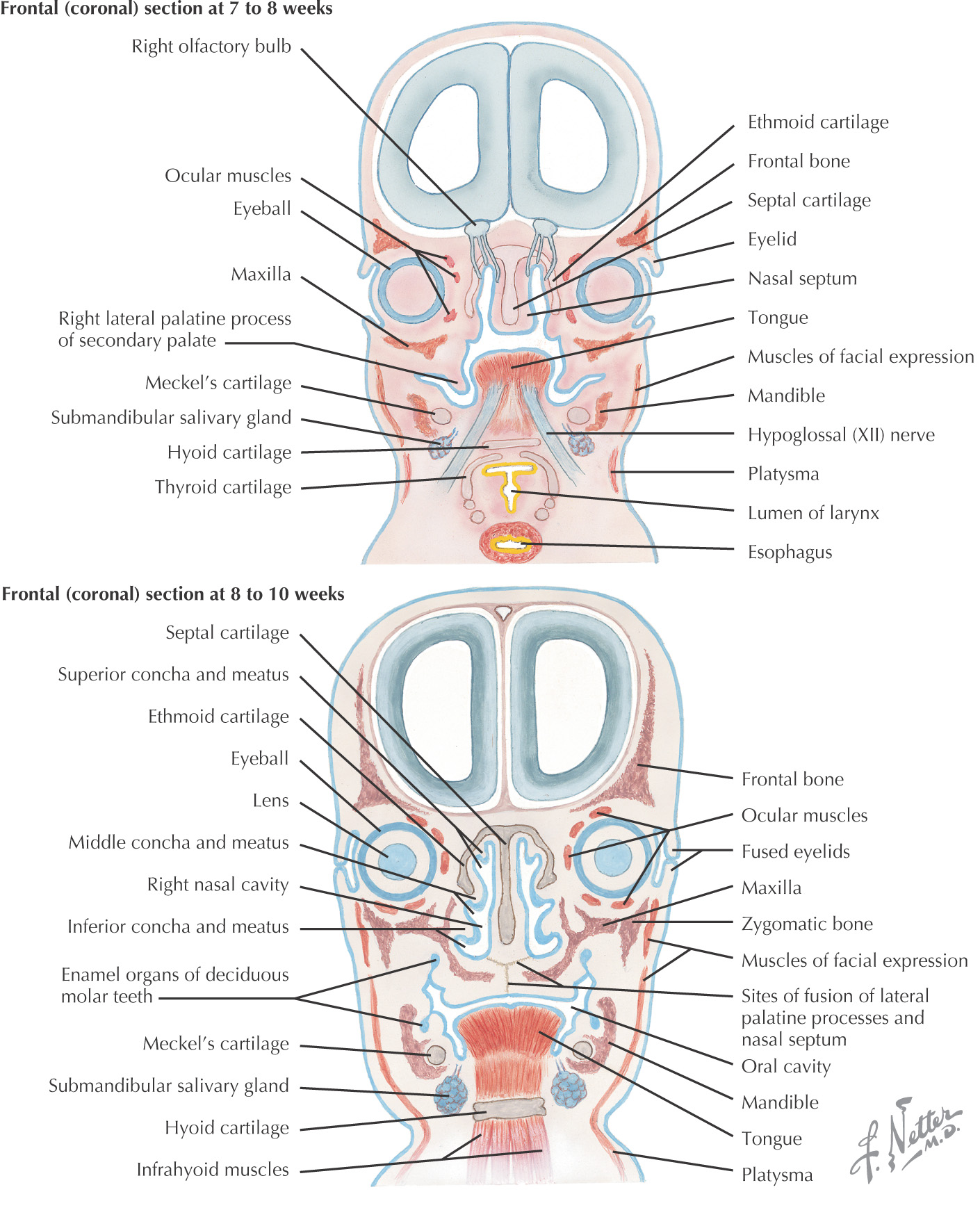
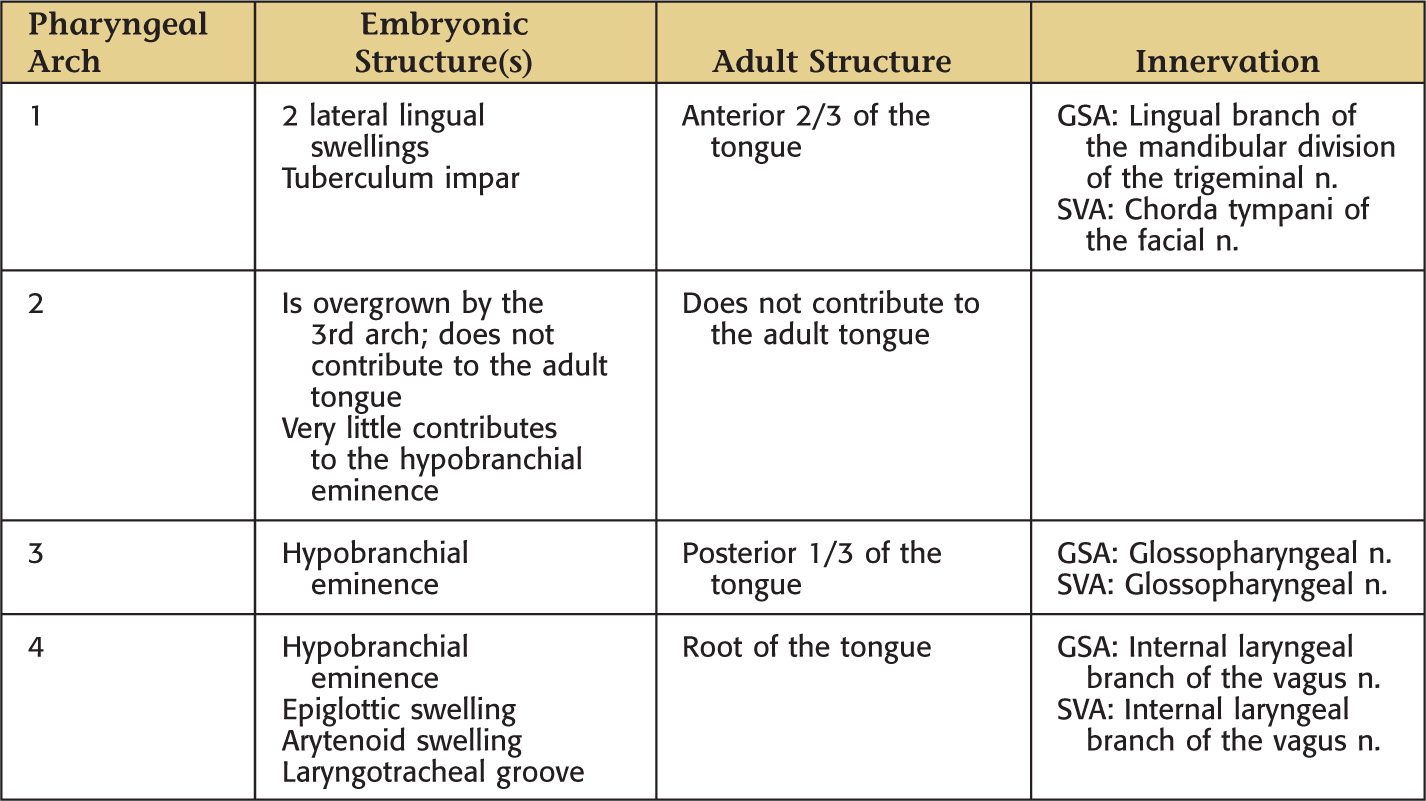
Mesoderm from the occipital somites migrates anteriorly with the hypoglossal nerve to give rise to the extrinsic and intrinsic muscles of the tongue
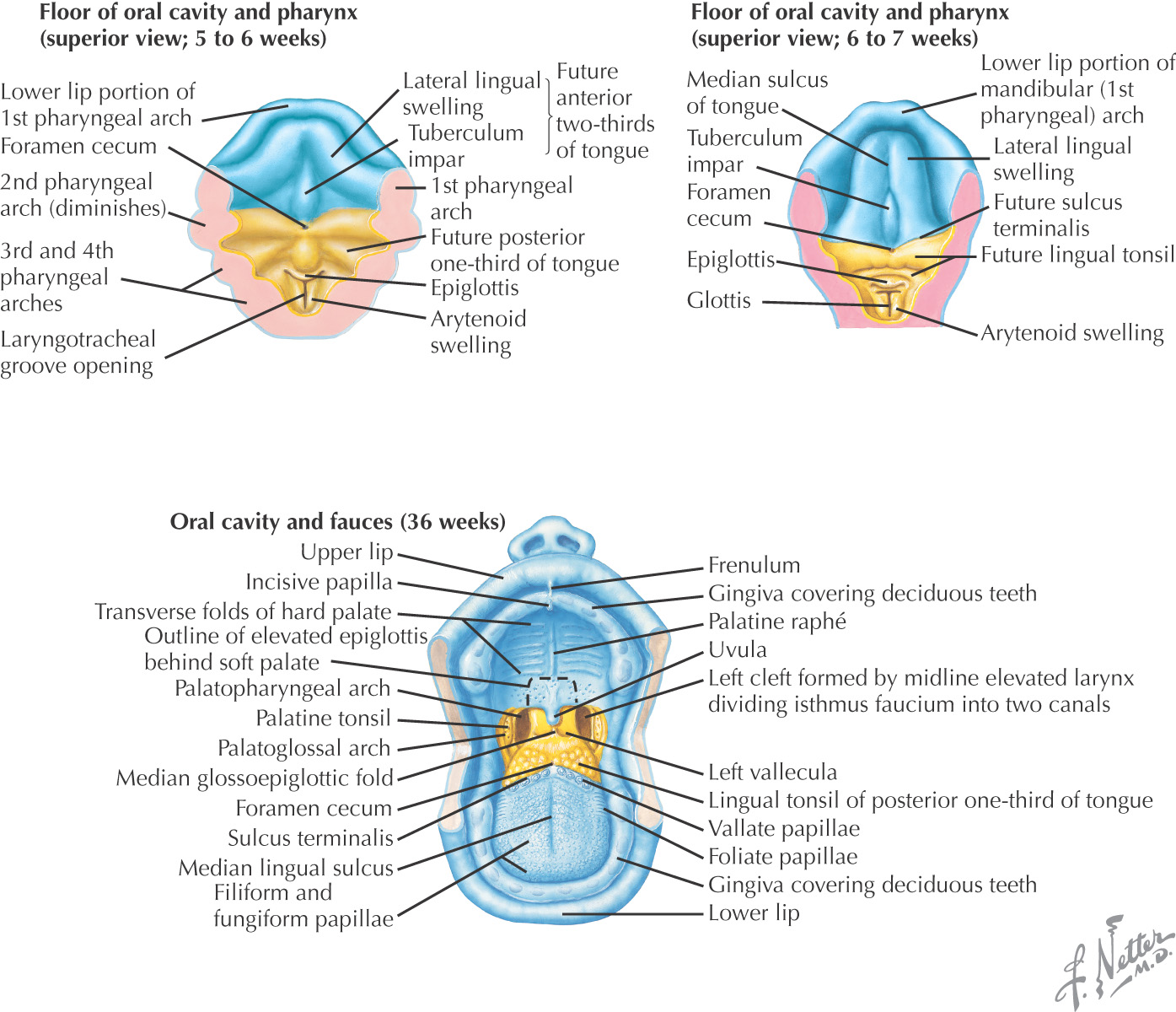
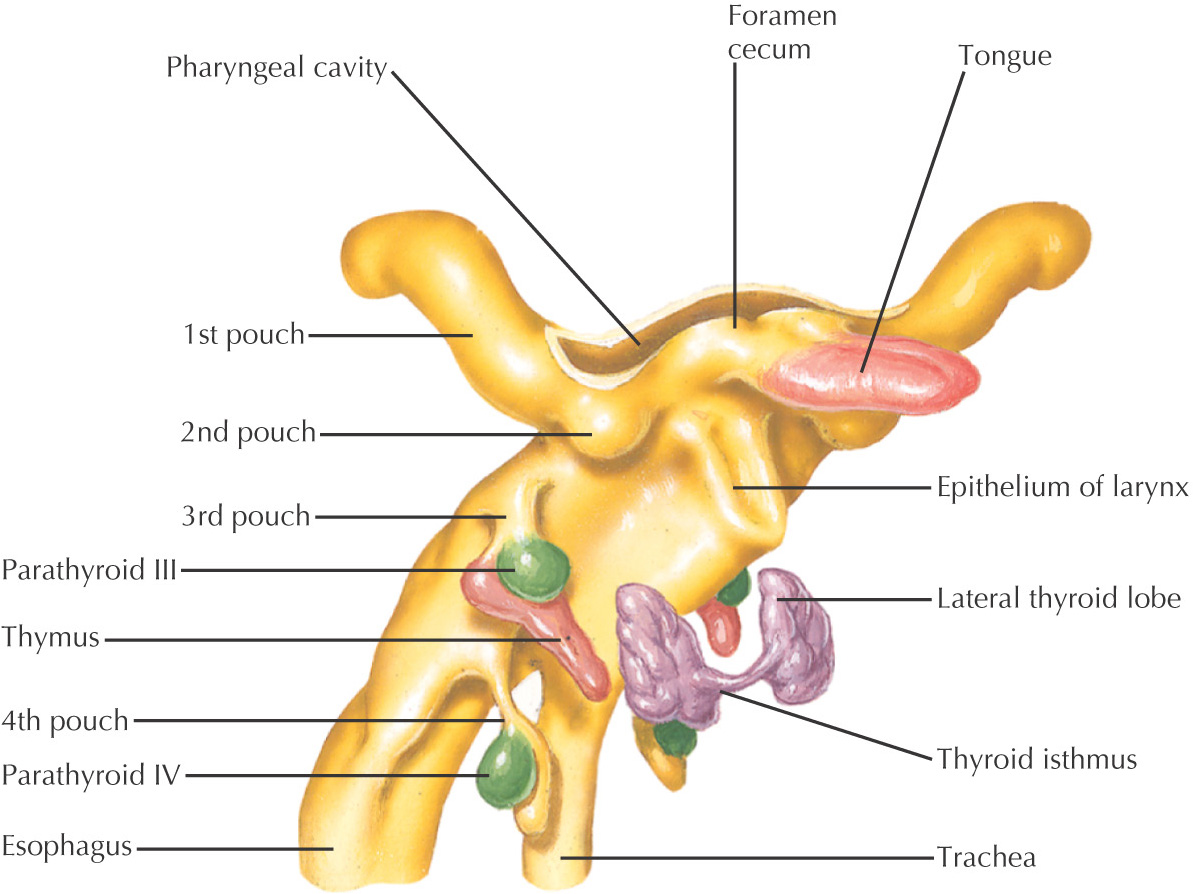
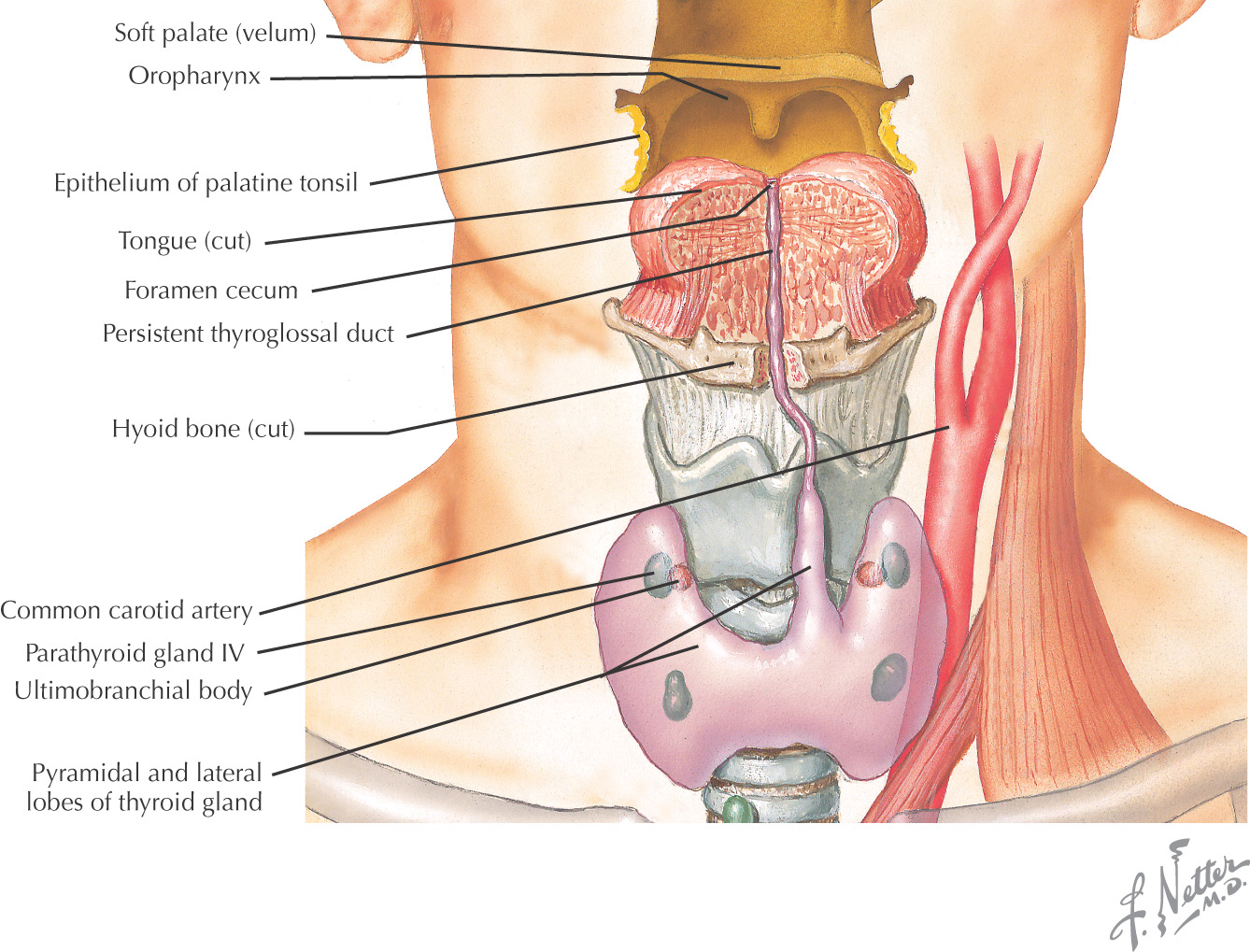
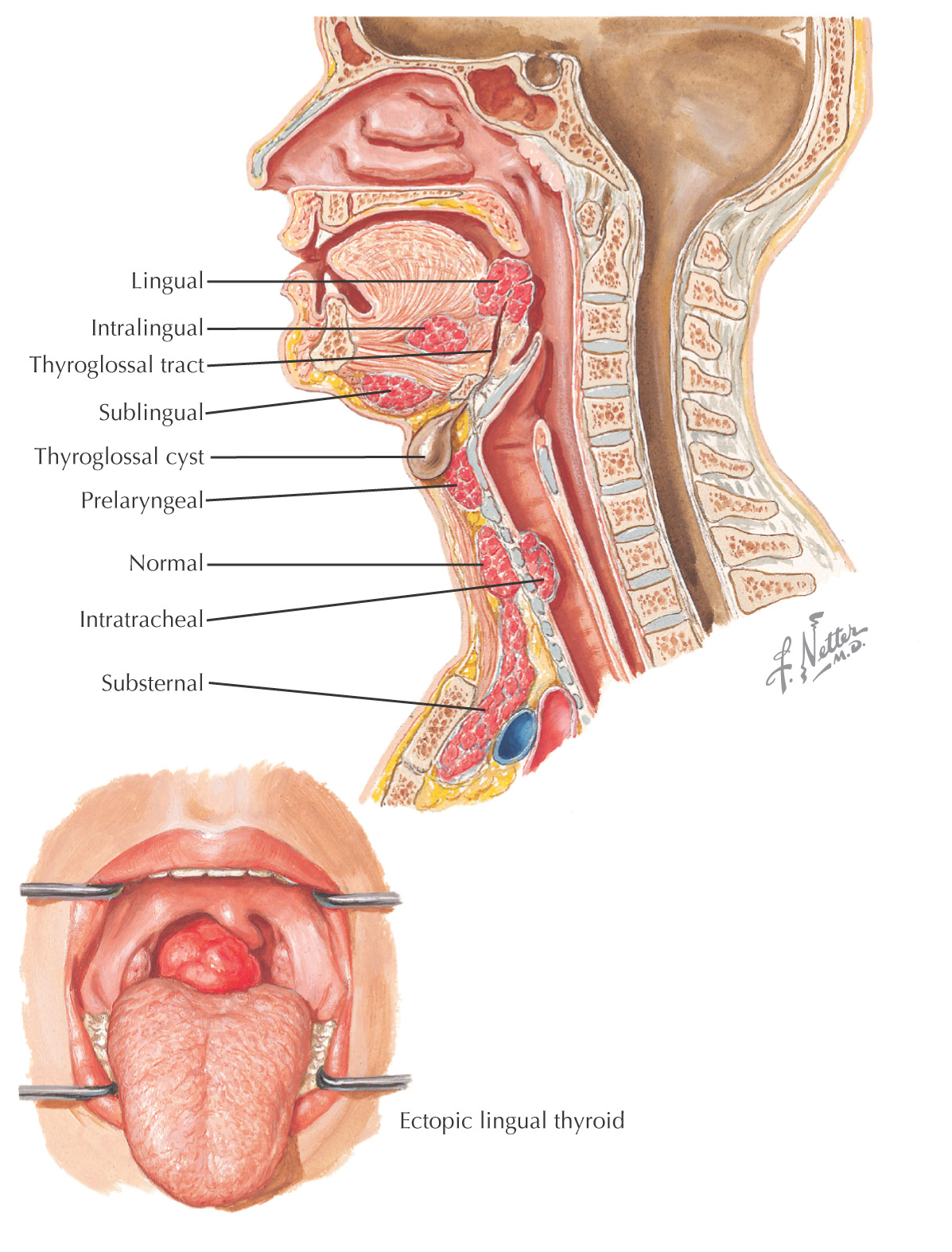
Begins as an invagination at the foramen cecum
Descends inferiorly to its final position alongside the larynx
May be connected to the foramen cecum by the thyroglossal duct
Divided into 2 lateral lobes connected by an isthmus, from which a pyramidal lobe sometimes develops
Follicular cells are derived from the endoderm; parafollicular cells are derived from the ultimobranchial body
Thyroid tissue in an aberrant location
Often the only thyroid tissue in the affected person
Susceptible to thyroid diseases like normal thyroid tissue
May occur anywhere along the migratory pathway of the thyroid gland beginning at the foramen cecum
Usually located at the base of the tongue (lingual thyroid)
Common locations include:
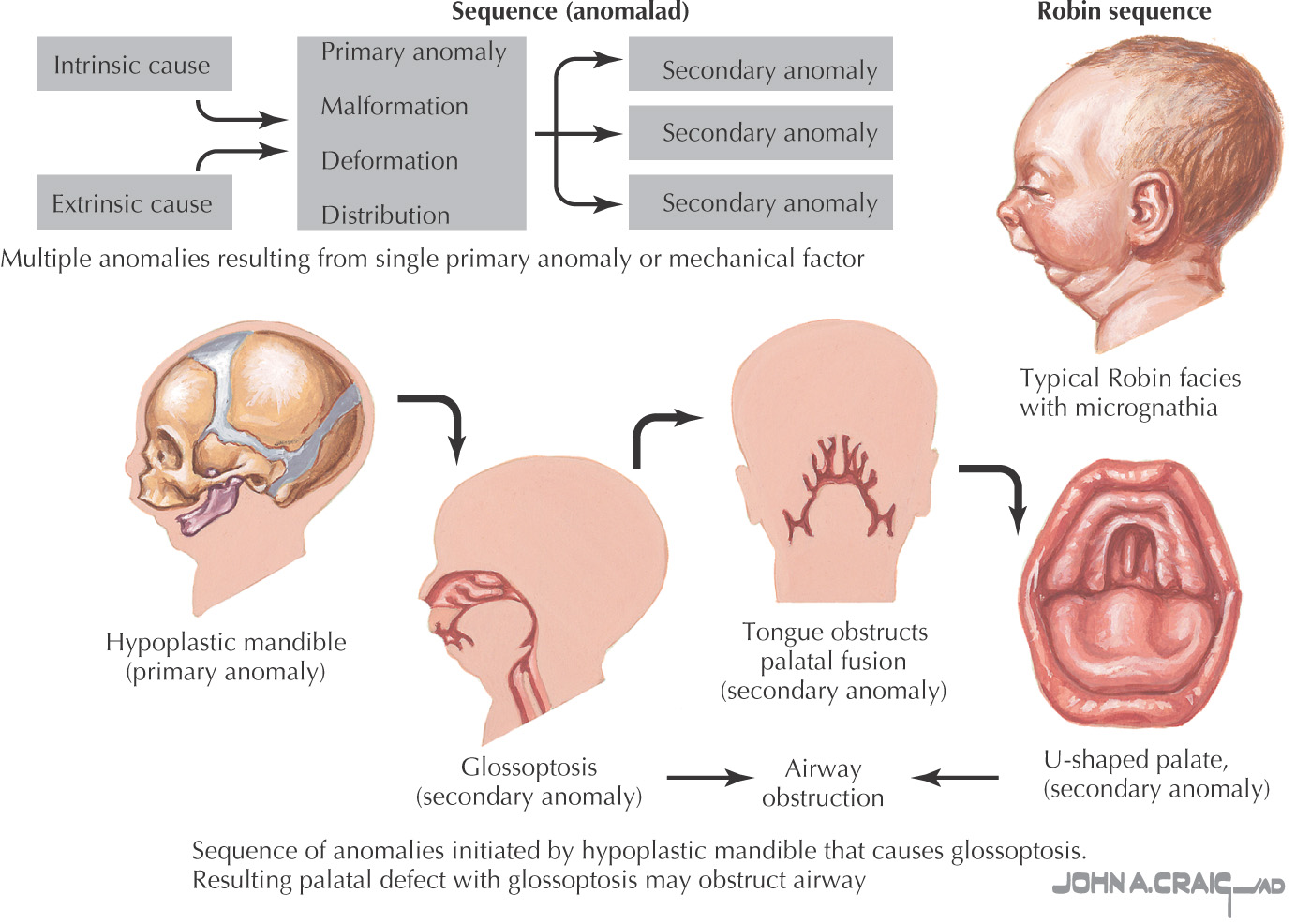
First reported as a condition characterized by micrognathia, cleft palate, and glossoptosis
Now includes any condition with a series of anomalies caused by events initiated by a single malformation
In this micrognathia, the inferior dental arch is posterior to the superior arch
The cleft palate may affect the hard and the soft palate
Glossoptosis (posterior displacement of the tongue) may cause airway obstruction or apnea
The mandible usually grows fairly quickly during childhood
Multiple surgeries typically needed to correct the cleft palate and to aid speech development in children
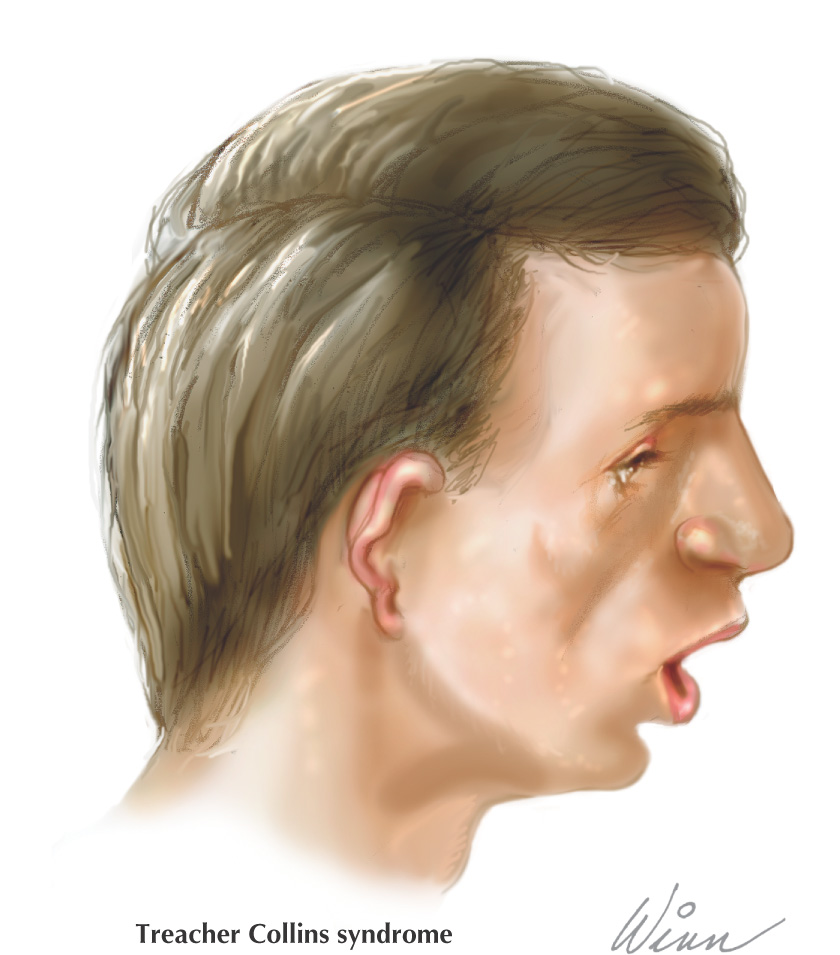
A hereditary condition affecting the head and neck
Thought to be caused by a defect in the gene or chromosome 5
Children of an affected parent have a 50% risk of having the syndrome
Clinical manifestations include:
• Notching of the lower eyelids
• Hypoplastic zygomatic bones (zygomas)
• Underdeveloped or malformed ears or “sideburns,” or both, are prominent
Common associated problems include:
• Eating/breathing difficulties
A rare condition caused by a deletion on chromosome 22, characterized by a wide array of clinical manifestations
Possible explanation: proper development is dependent on migration of neural crest cells to the area of the pharyngeal pouches
Although researchers described the syndrome as abnormal development of the 3rd and 4th pharyngeal pouches, defects involving the 1st to the 6th pouches have been observed
Possible associated problems include:
• Congenital heart defects (such as tetralogy of Fallot, right infundibular stenosis, truncus arteriosus, aberrant left subclavian artery, and ventricular septal defect)
• Facial defects (such as cleft palate, microstomia, downslanting eyes, low-set ears, or hypertelorism)
• Increased vulnerability to infections (due to impaired immune system from the loss of T cells associated with absence or hypoplasia of the thymus)

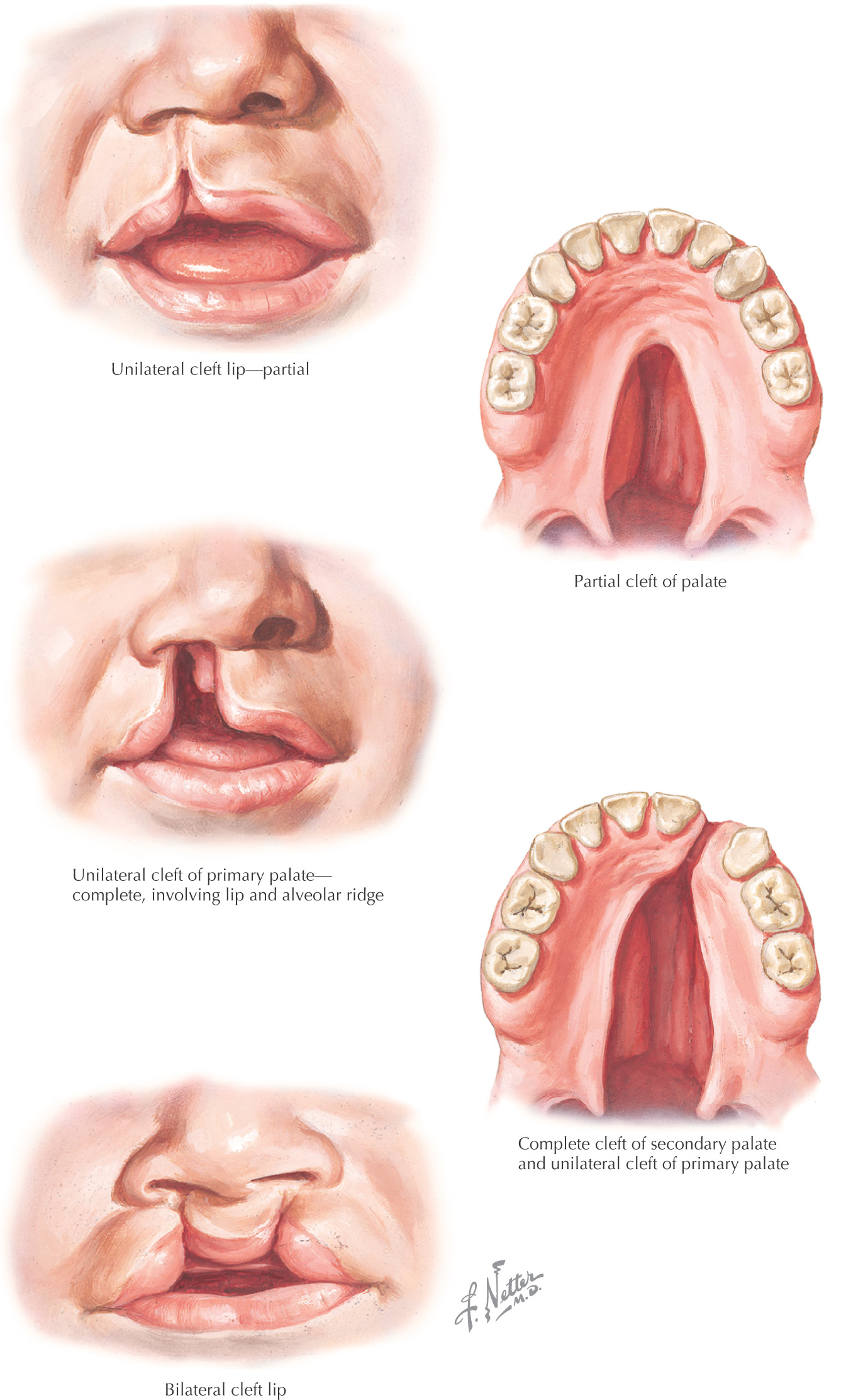
Cleft lip: a gap in the upper lip
Cleft palate: a gap in the palate
Classification of the developmental defect is with reference to the incisive foramen:
Both cleft lip and cleft palate often cause difficulty with feeding and eventually speech
Surgery is the most common form of treatment for both
Occurs anterior to the incisive foramen and results from a failure of the mesenchyme in the lateral palatine process to fuse with the intermaxillary segment (primary palate)
Common types of primary cleft:
• Unilateral cleft lip and primary palate
• Bilateral cleft lip and primary palate
Occurs posterior to the incisive foramen; results from failure of the lateral palatine process to fuse together
Common types of secondary cleft:
• Unilateral cleft in hard and soft palate
• Bilateral cleft of hard and soft palate
Extends through the lip, the primary palate, and the lateral palatine process; results from a failure of the lateral palatine process to fuse together with each other, as well as with the nasal septum and primary palate
Common types of complete cleft:
• Unilateral cleft lip and cleft palate
• Bilateral cleft lip and cleft palate