Overview and Topographic Anatomy
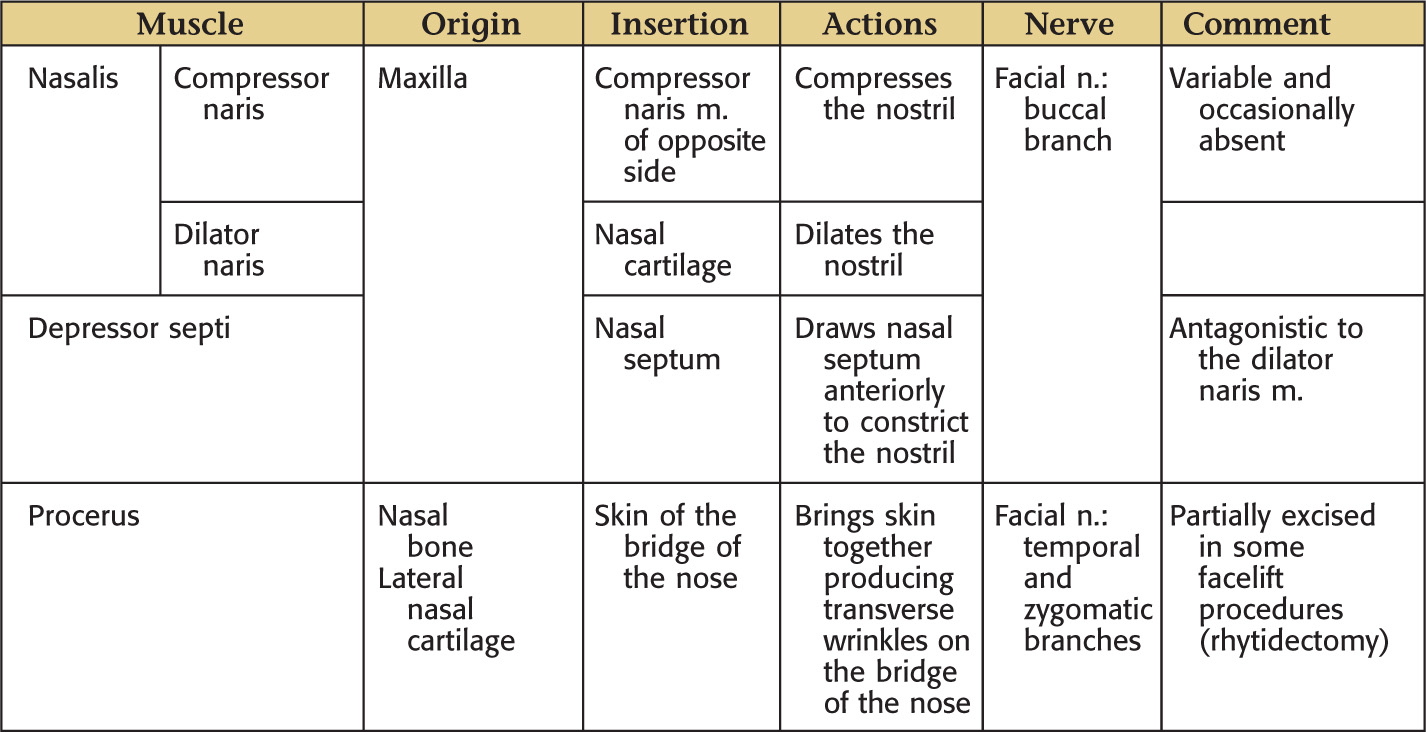
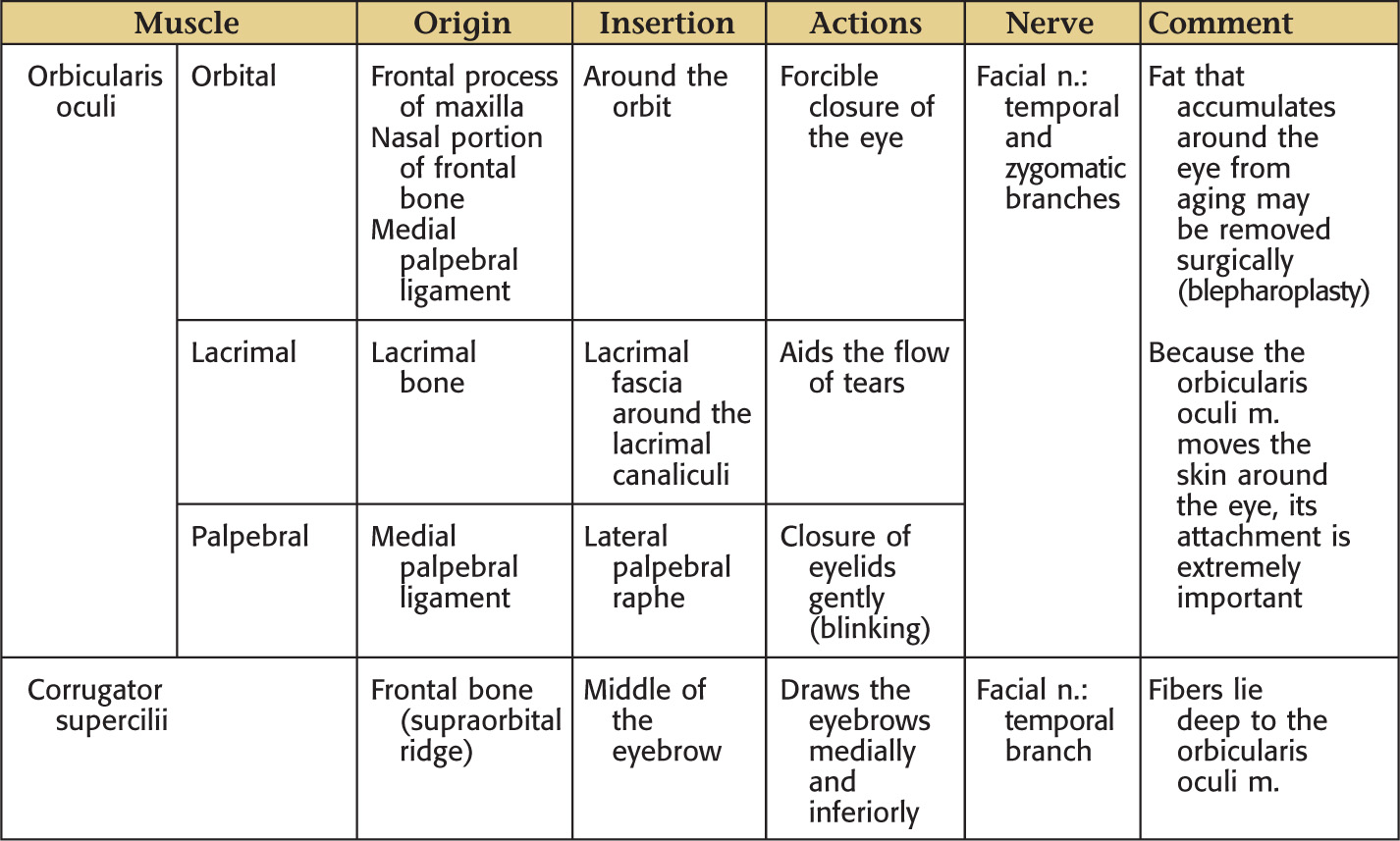
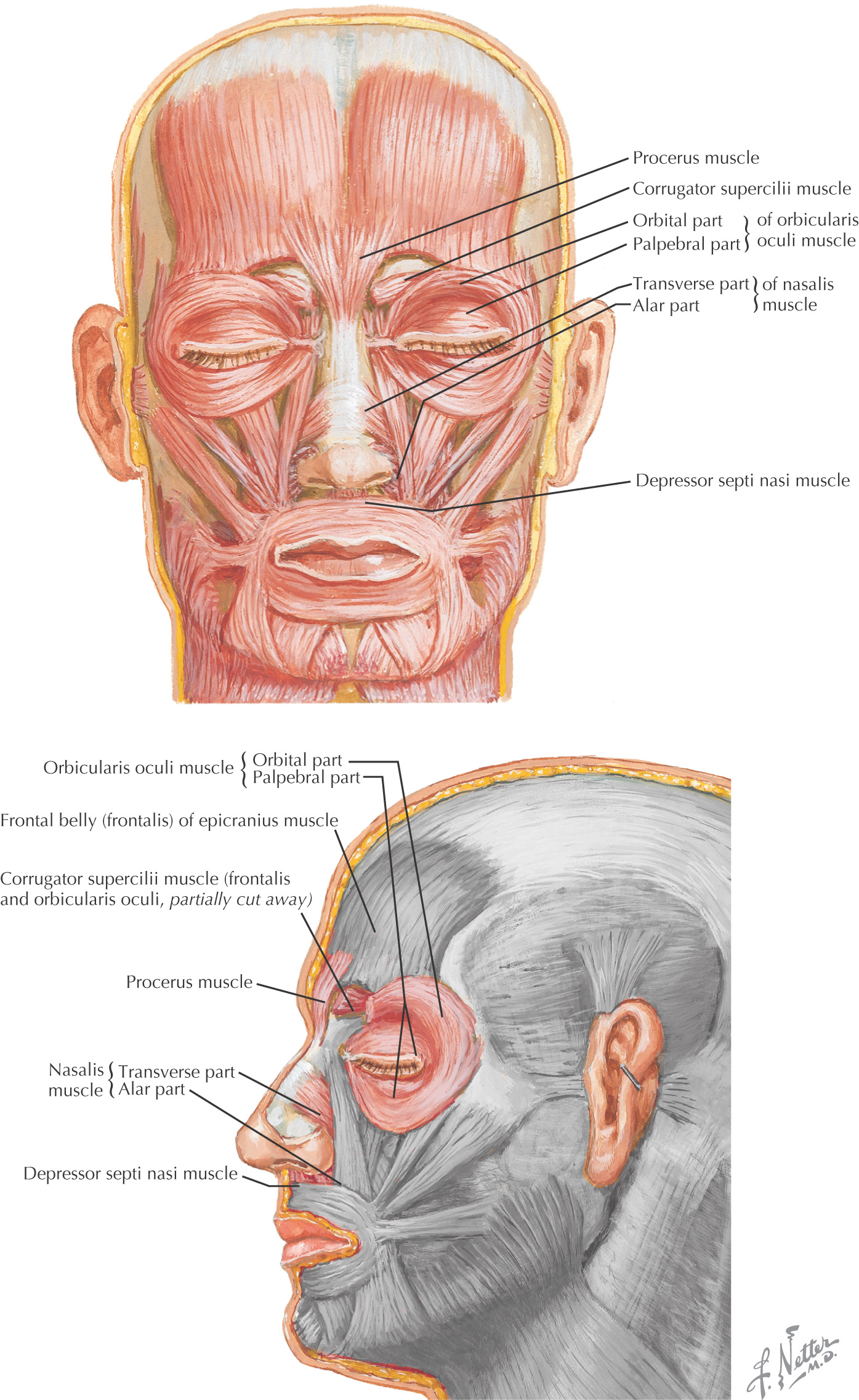
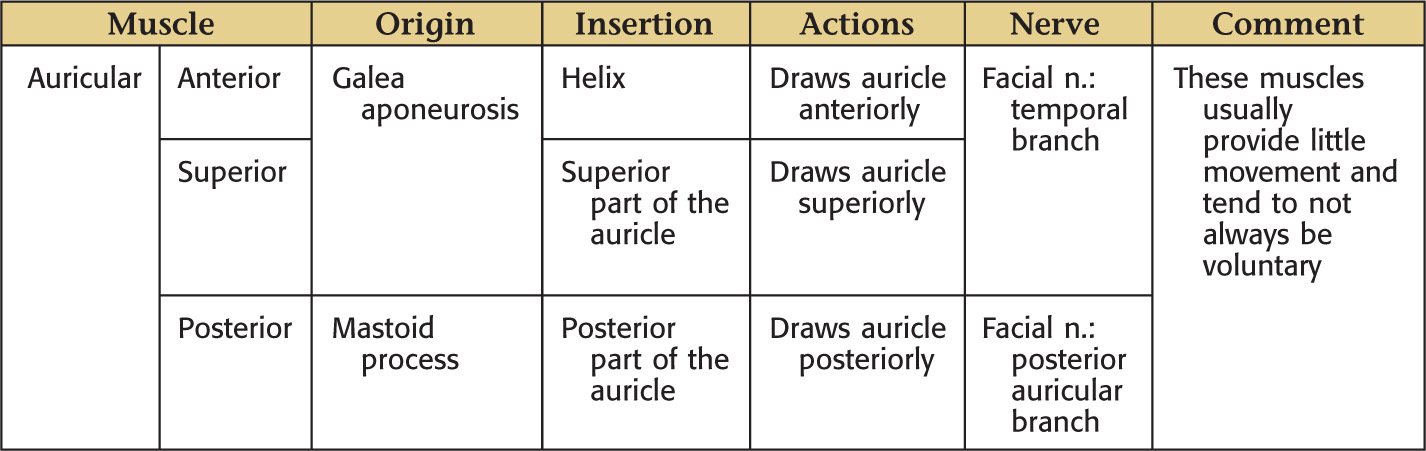
Overview of Muscles of Facial Expression
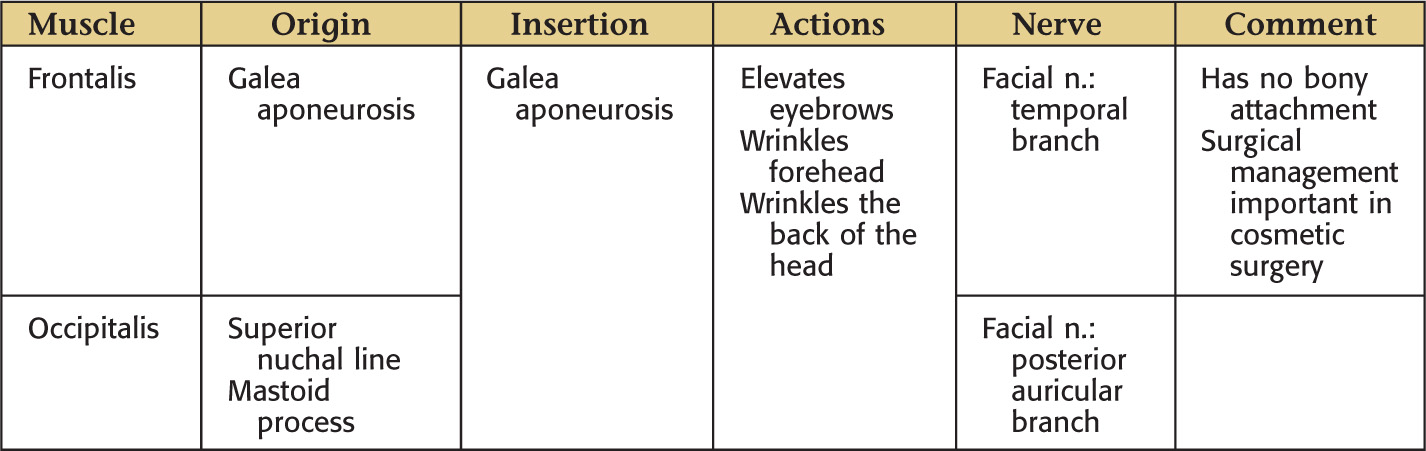
The area bordered by the forehead, superior part of the cranium, and occipital area immediately superior to the superior nuchal line
The lateral portion of the scalp blends with the temporal area because it extends inferiorly to the zygomatic arch
Anatomy of the scalp is important because of frequent trauma in this region
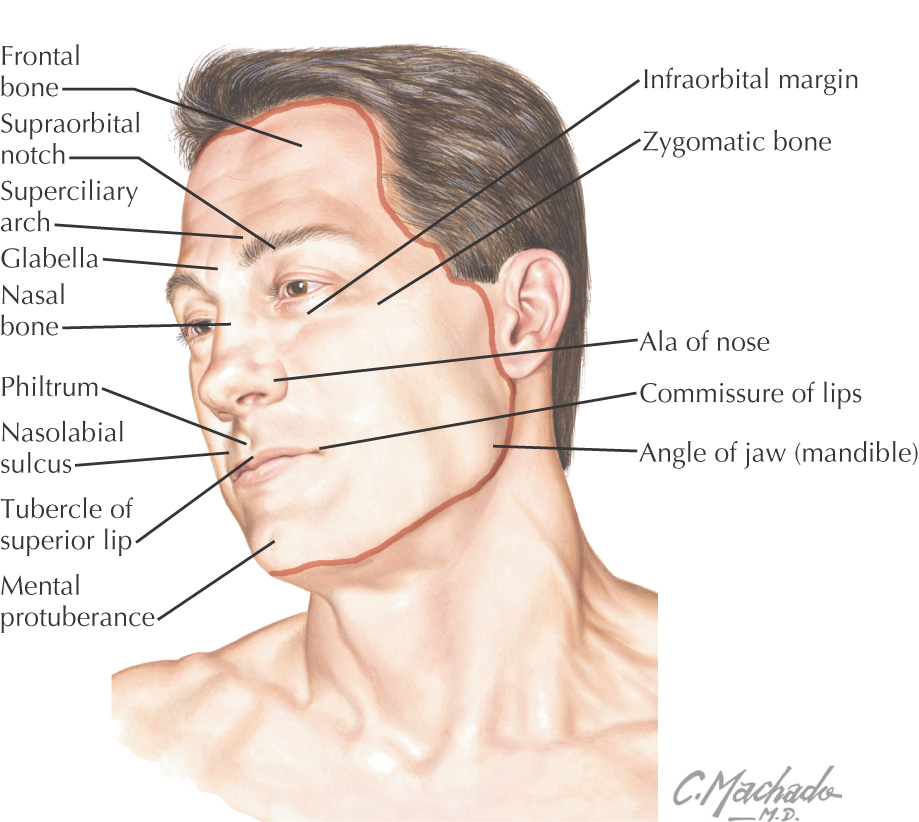
The area bordered within the hairline, anterior border of the auricles, and the chin
Major contents: eyes, nose, mouth, muscles of facial expression, muscles of mastication, parotid gland, trigeminal nerve, and facial nerve
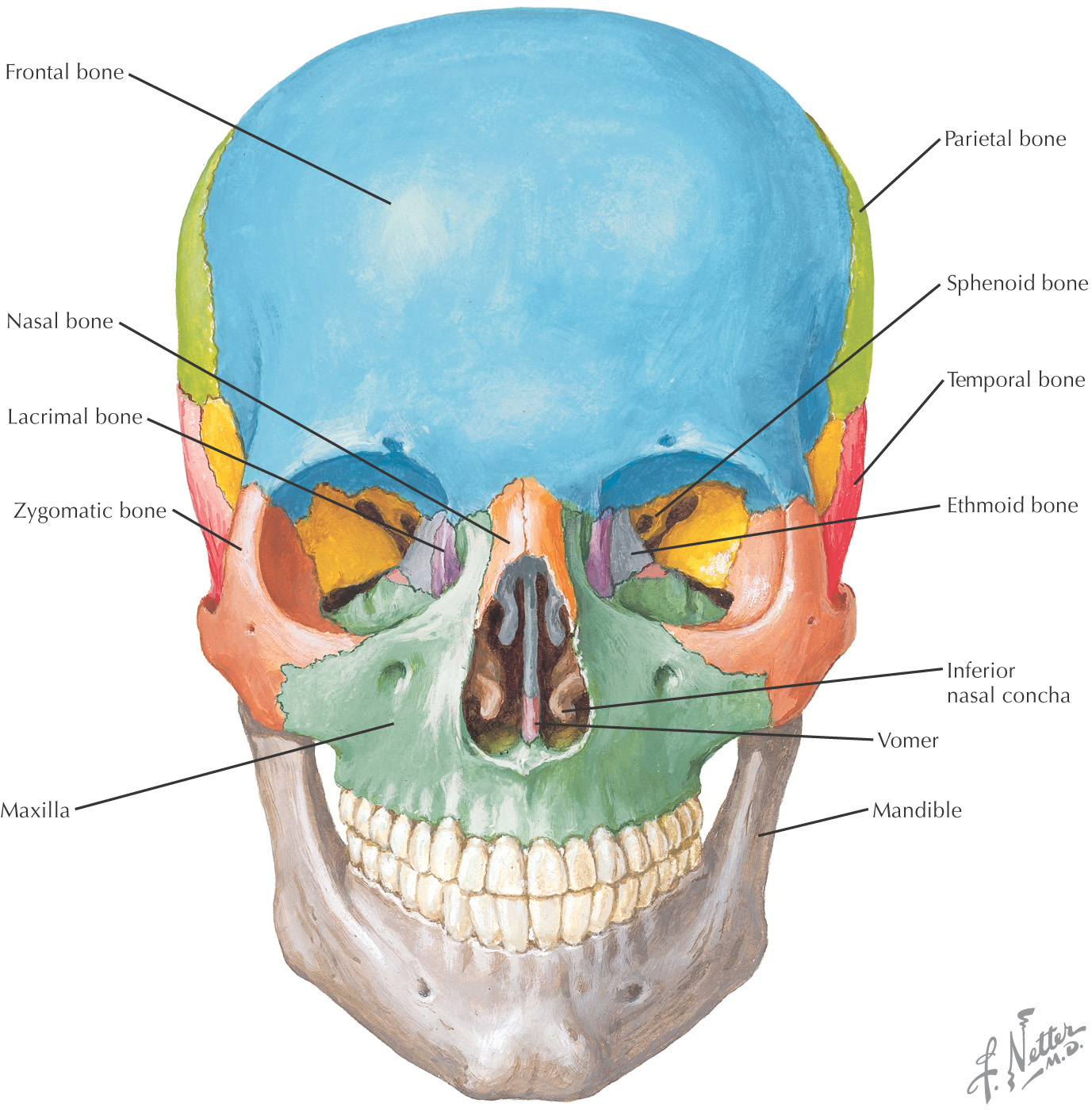
Bones of the facial skeleton:
Besides the nasal bone, the most commonly fractured bone of the facial skeleton is the zygomatic bone
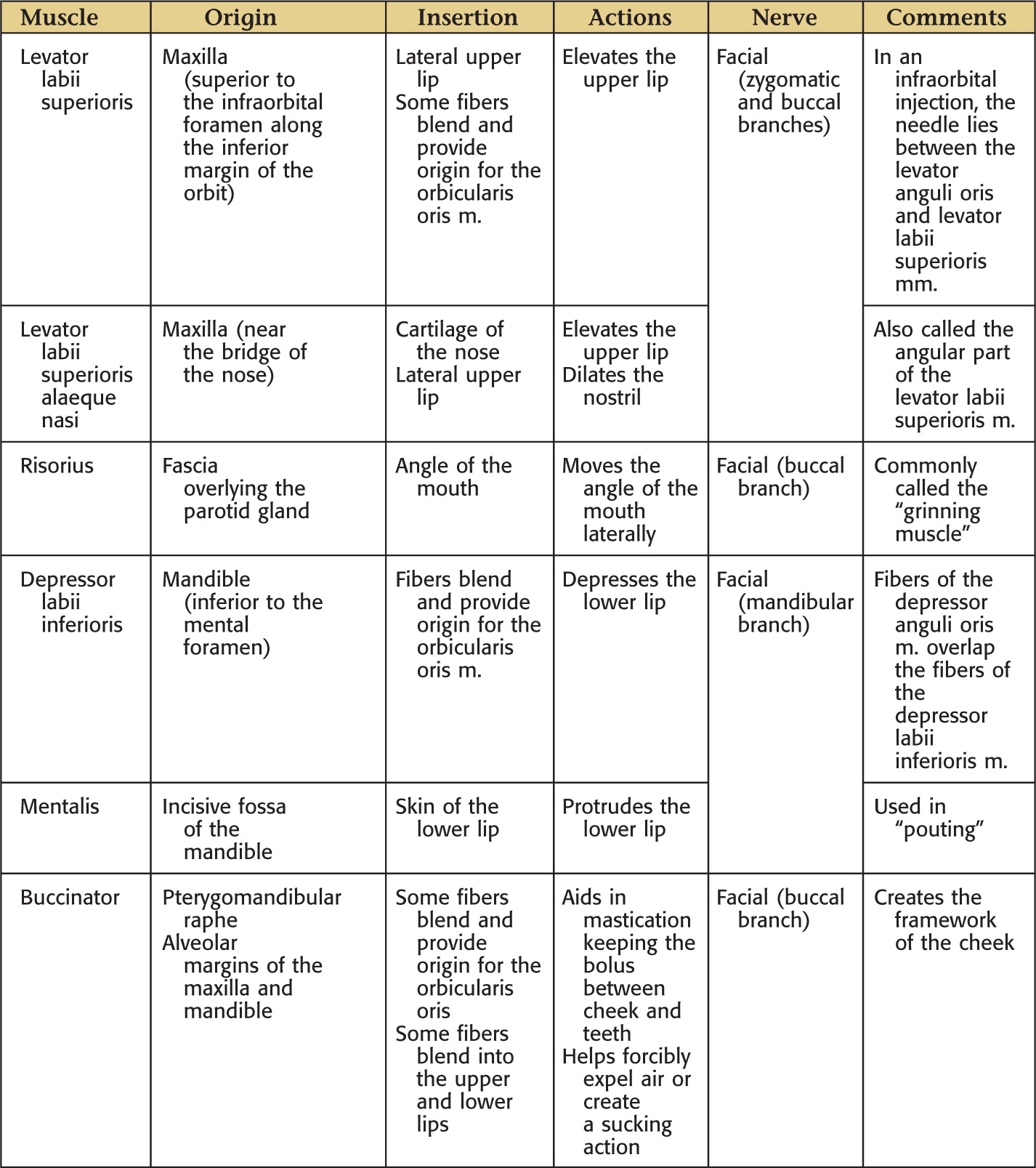
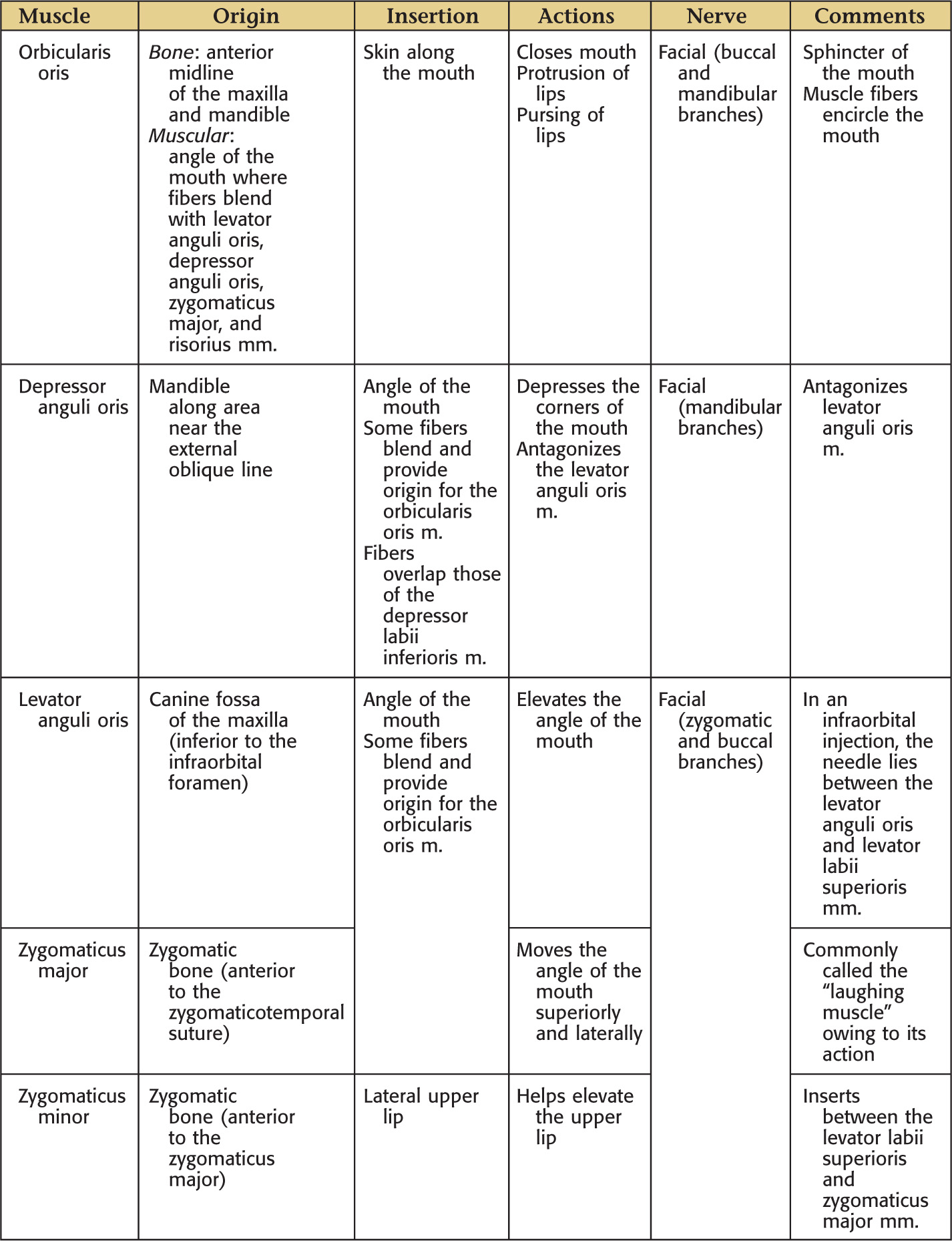
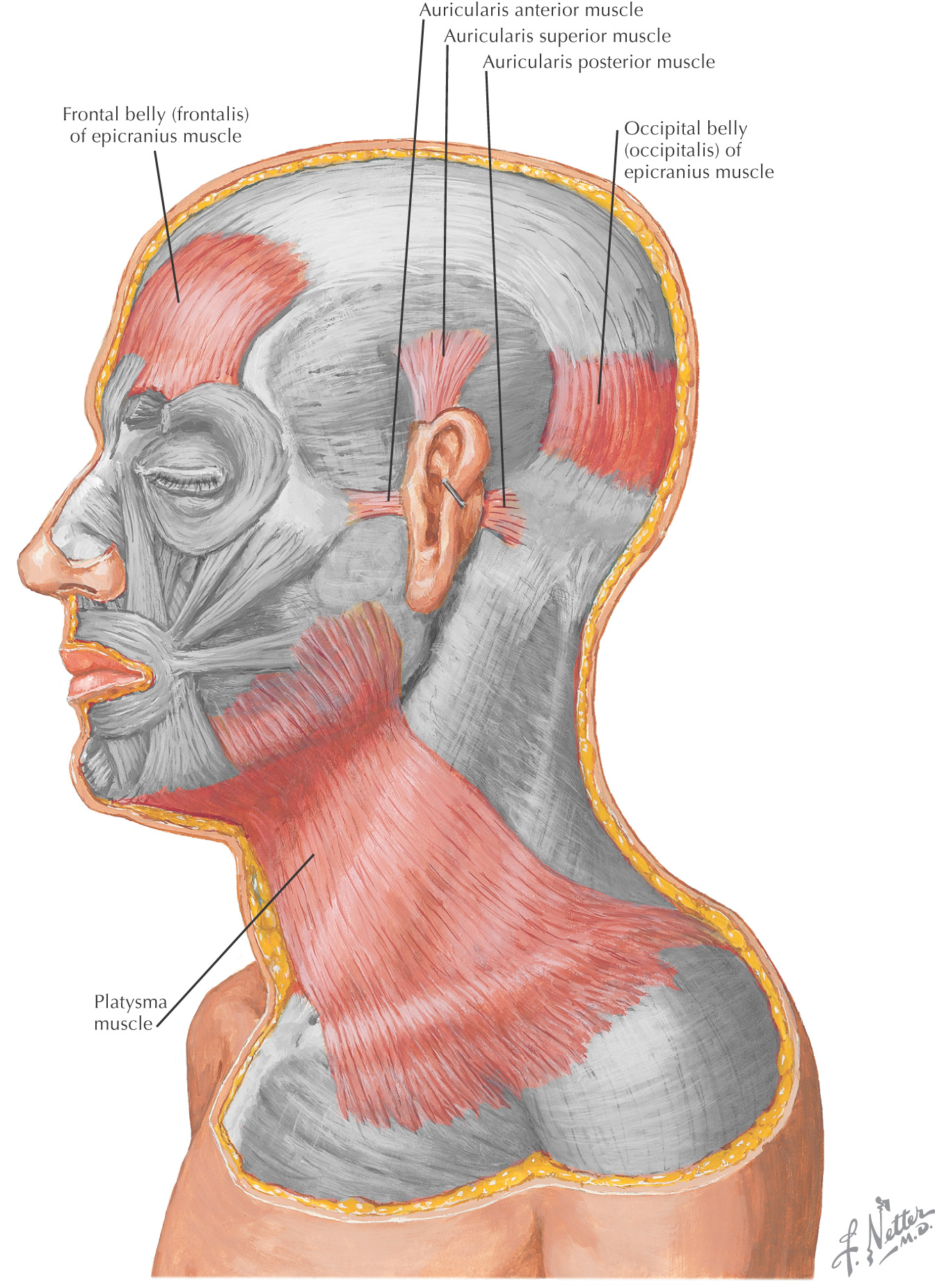
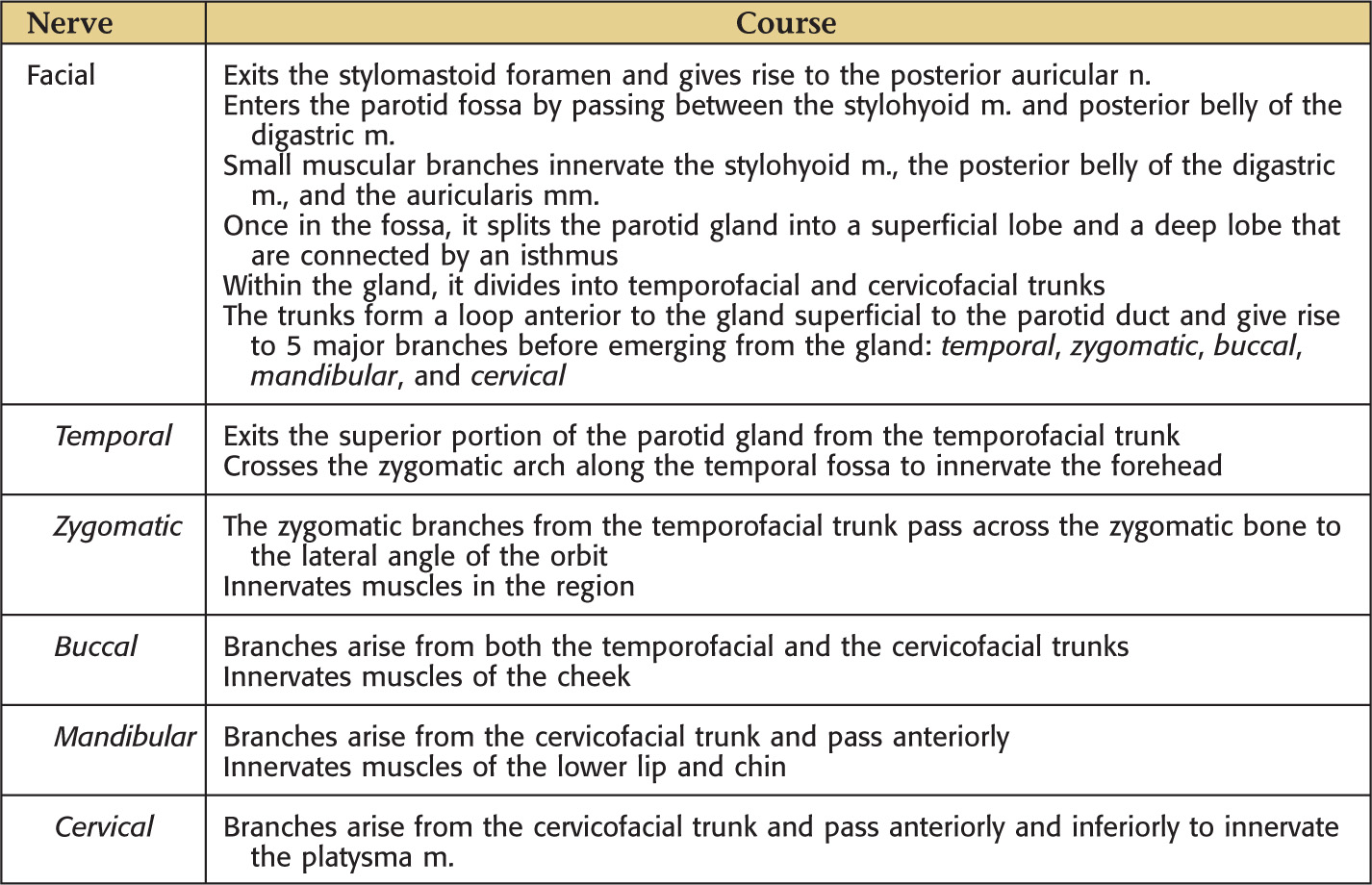
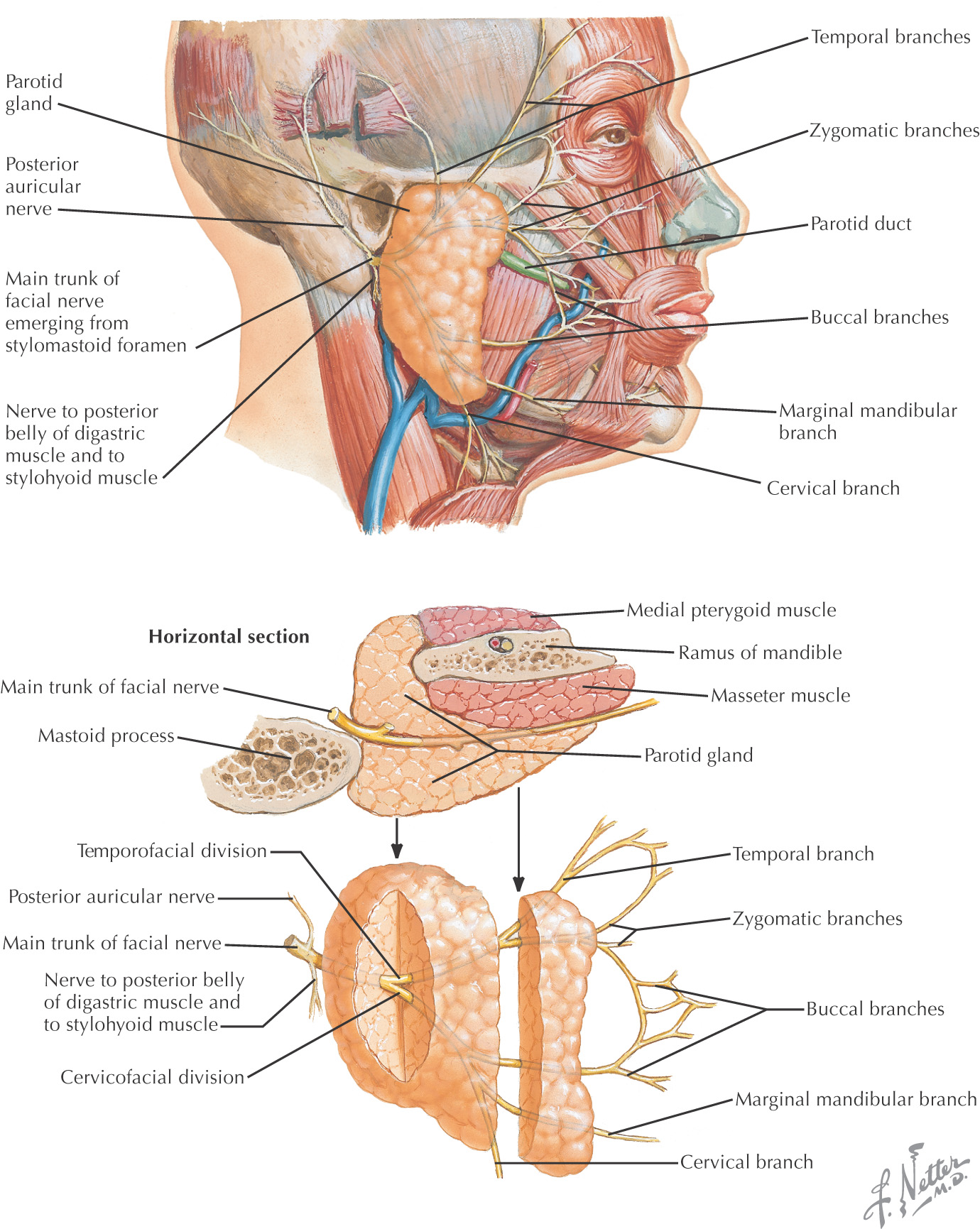
Innervated by the facial nerve
Derivatives of the 2nd pharyngeal arch
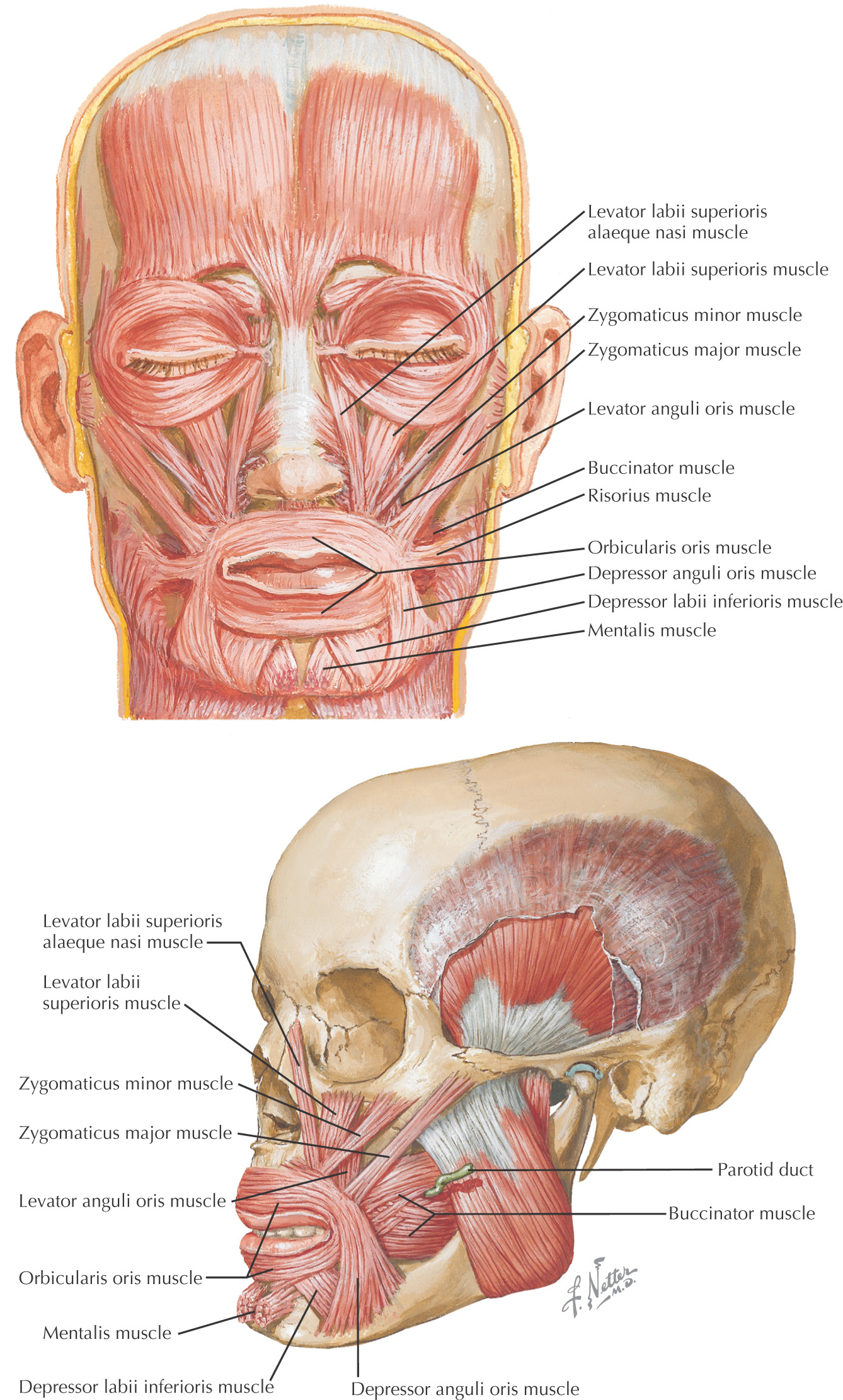
Originate from either bone or fascia and insert on the skin
The Superficial Muscular Aponeurotic System (SMAS) is a term used to describe the relationship of the muscles of facial expression located within the superficial fascia
The SMAS is maneuvered in a rhytidectomy (facelift)
There is no deep fascia along the face
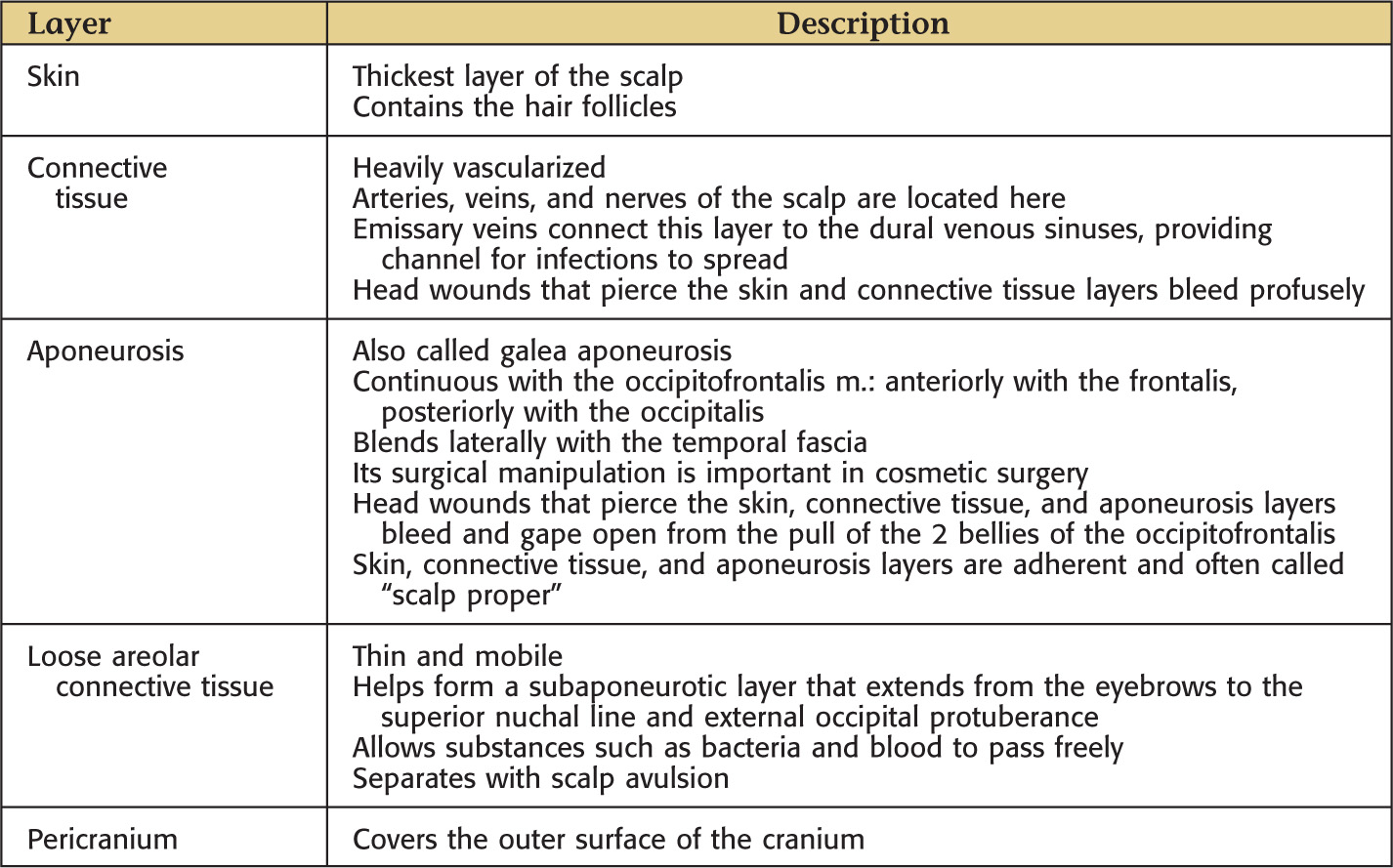
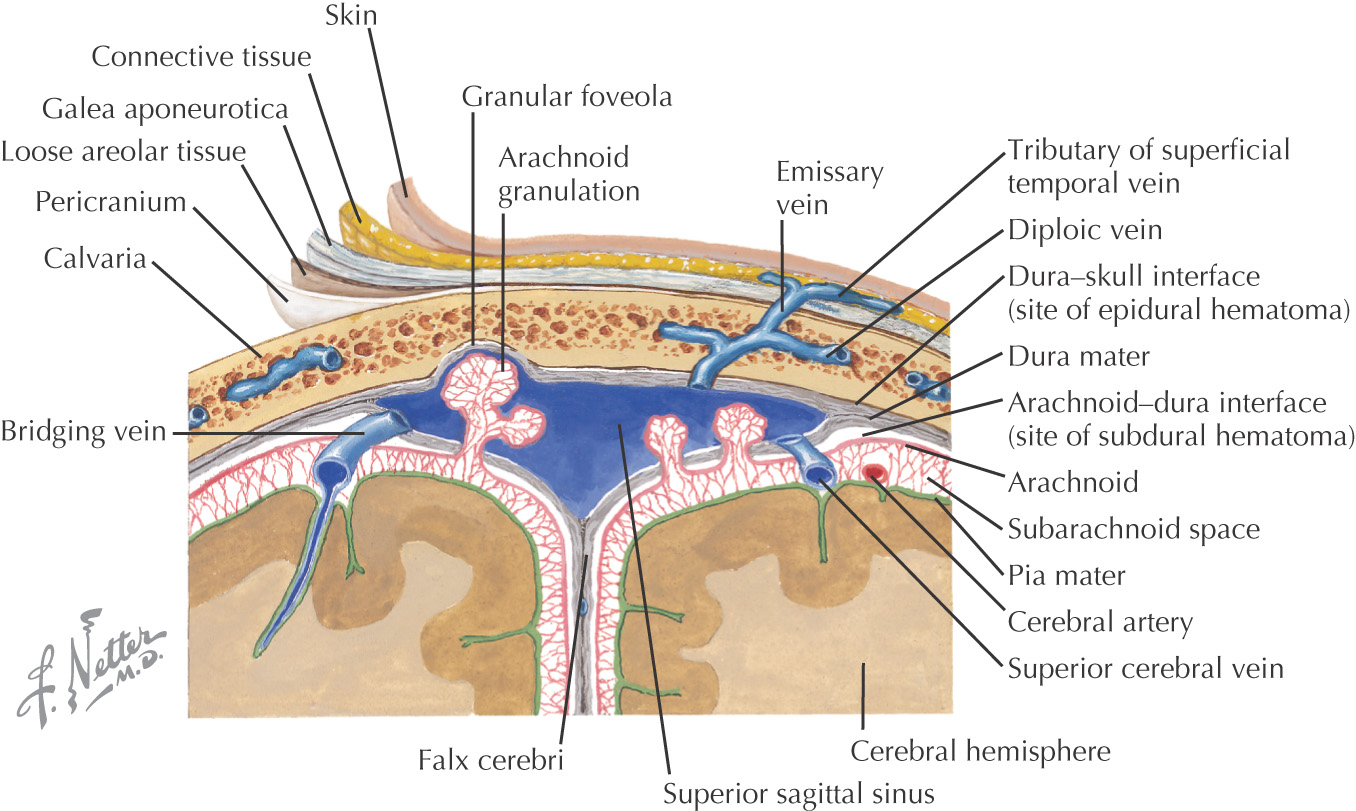
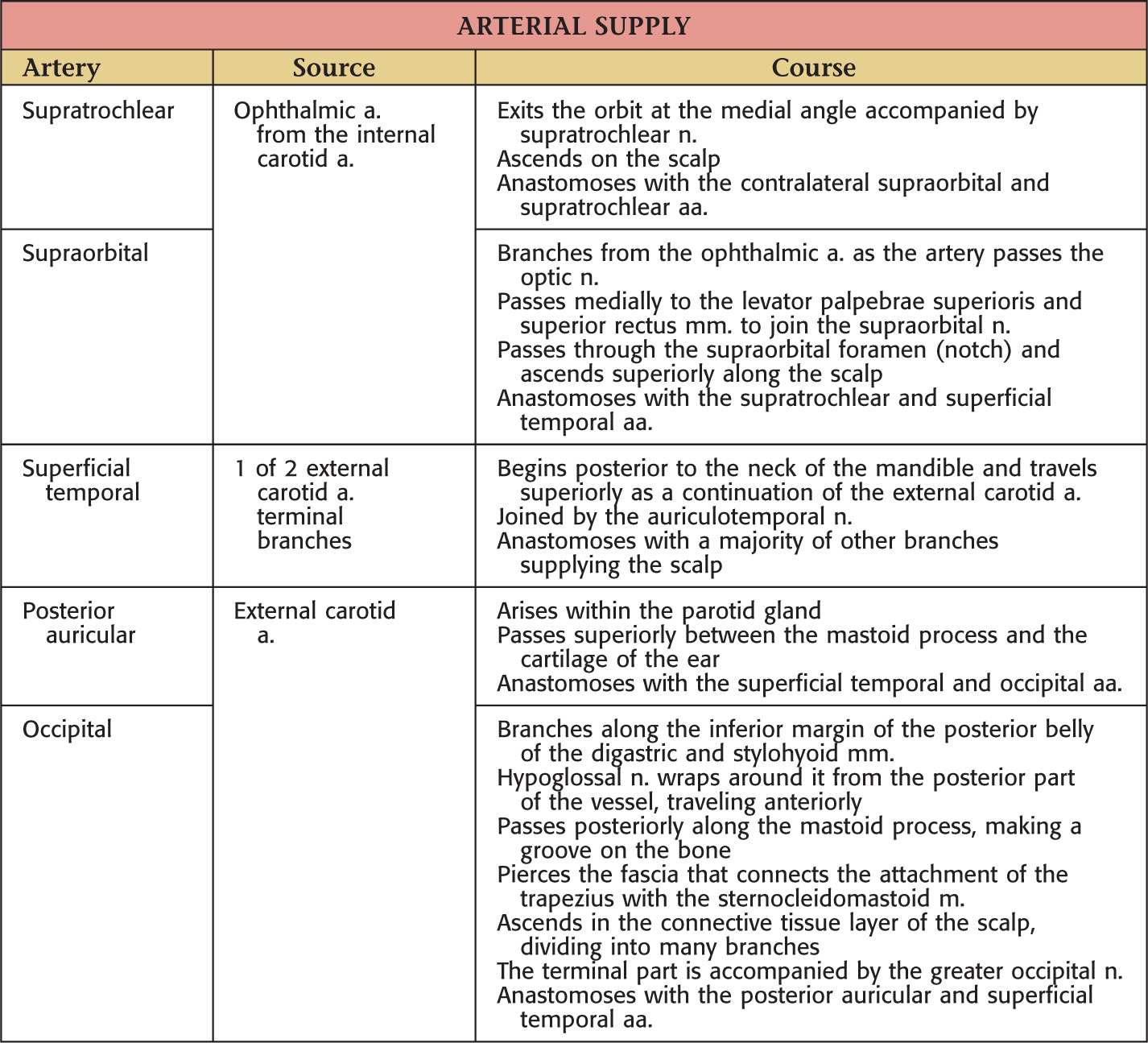
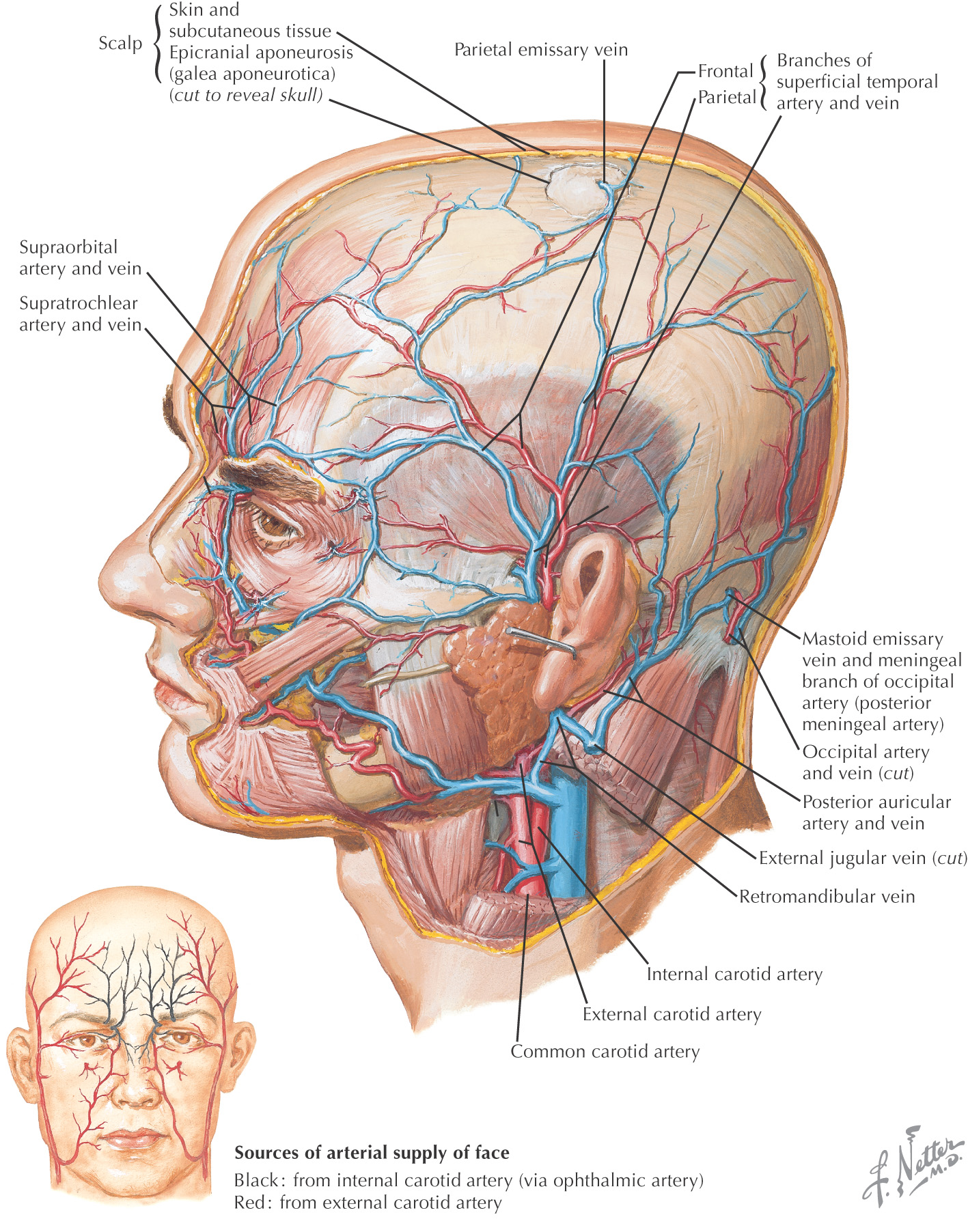
Highly vascularized; the vessels anastomose freely on the scalp
Arteries are derived from the external and the internal carotid arteries
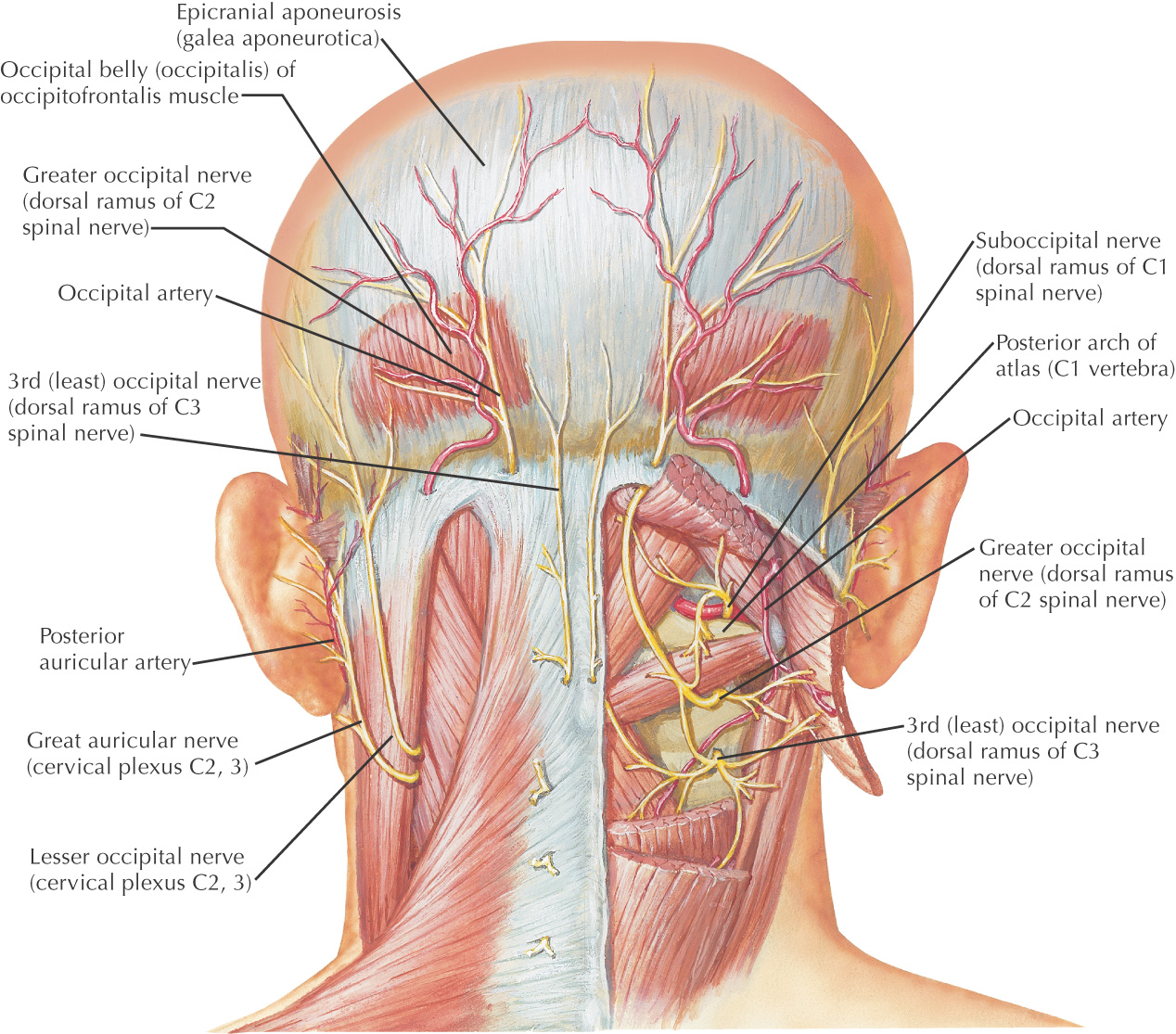
The neurovascular supply arises from the anterior, lateral, and posterior scalp regions
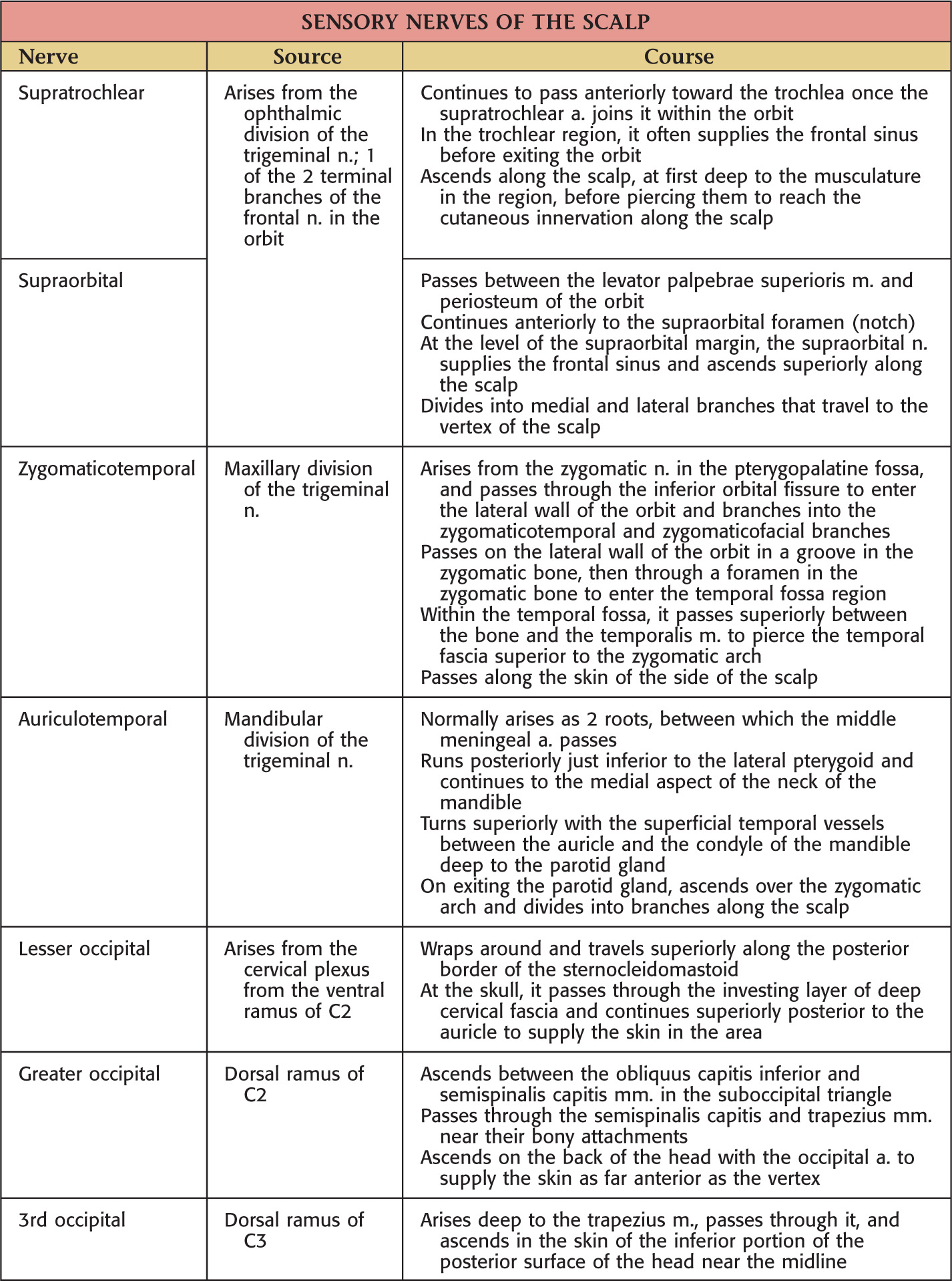
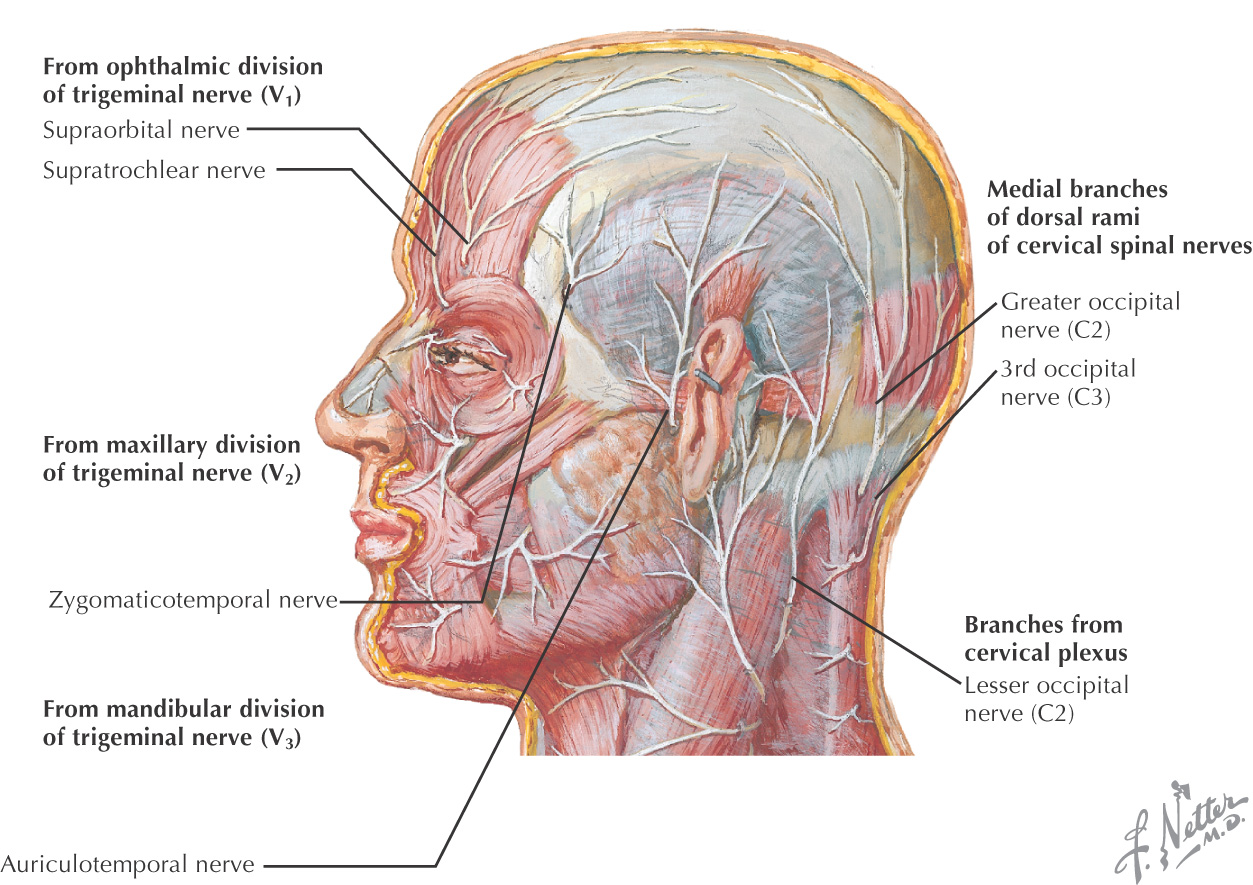
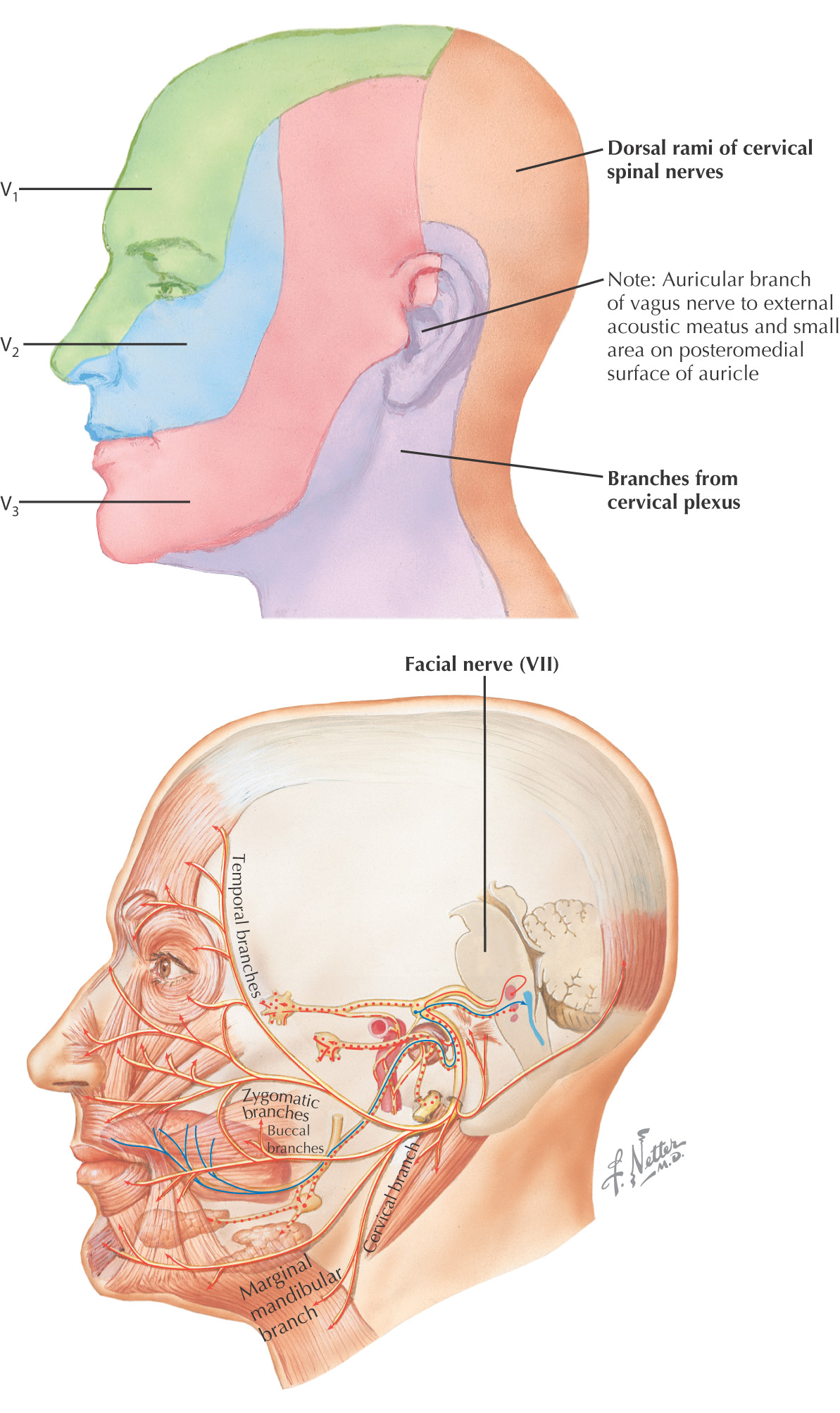
Sensory supply is derived from all 3 divisions of the trigeminal nerve, branches of the cervical plexus, and upper cervical dorsal rami
These nerves travel in the scalp’s connective tissue layer
Innervated by the facial nerve
Derivatives of the 2nd pharyngeal arch
Insert into the skin to provide movement
Most muscles of facial expression are localized around the facial orifices
There is no deep fascia along the face

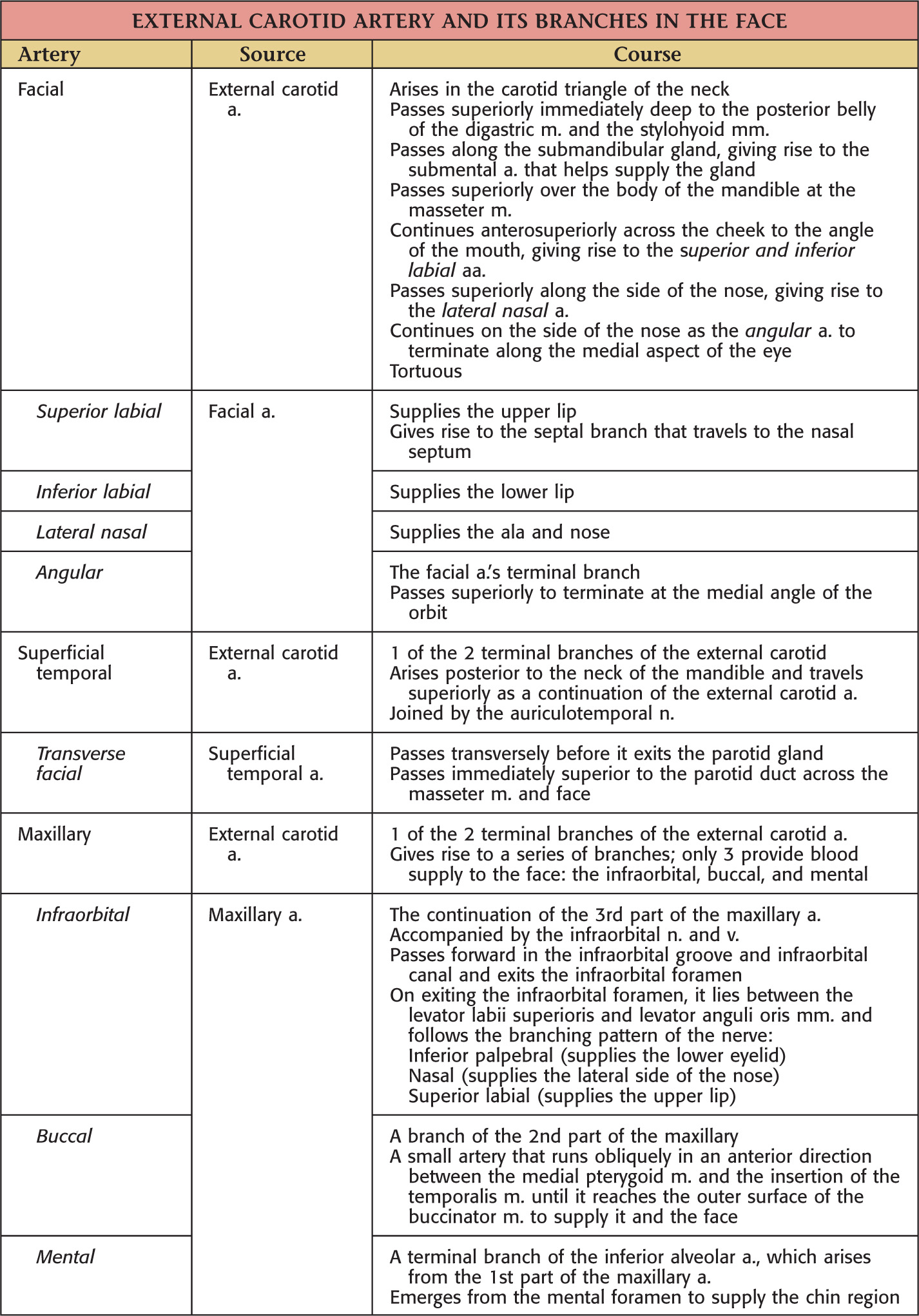
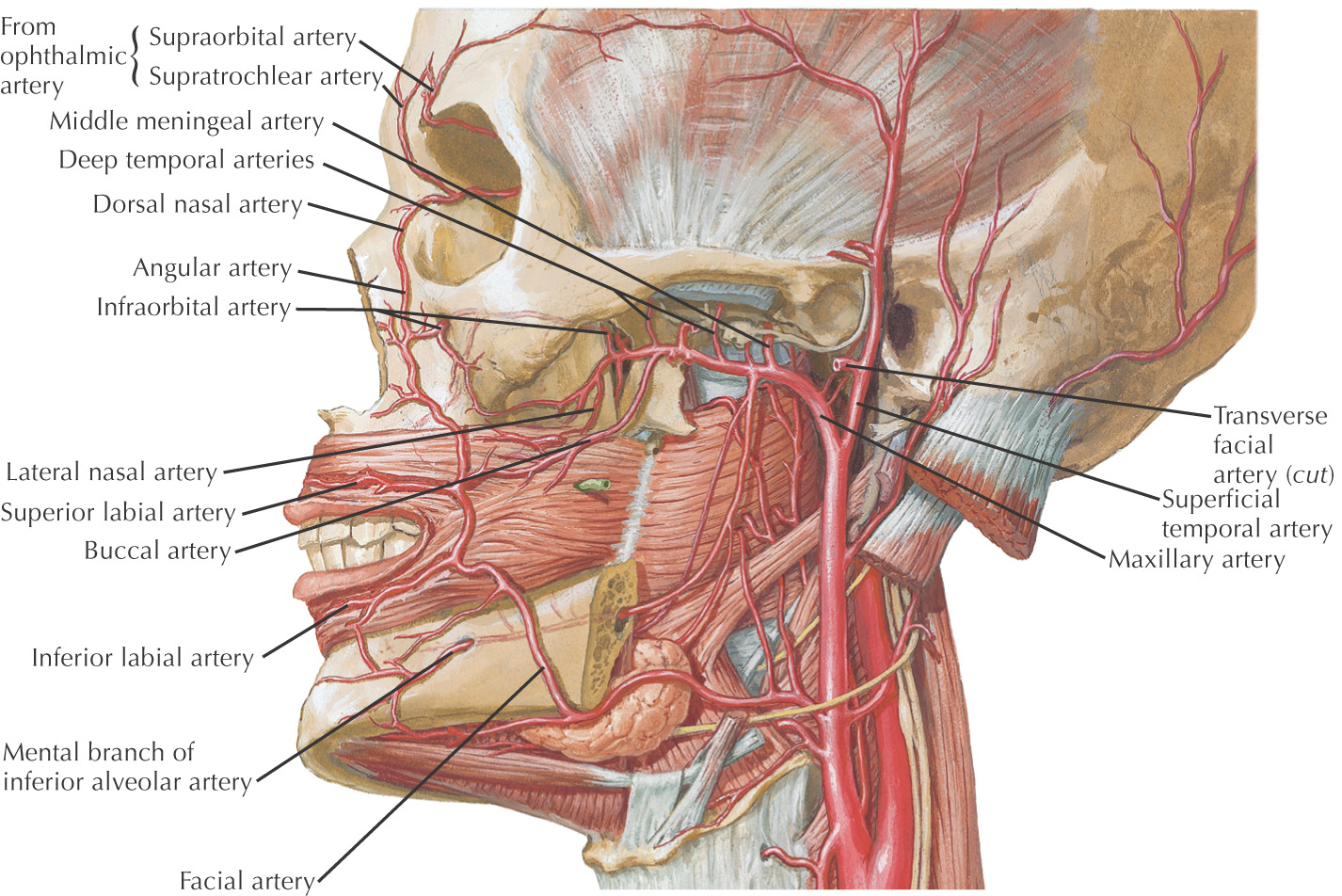
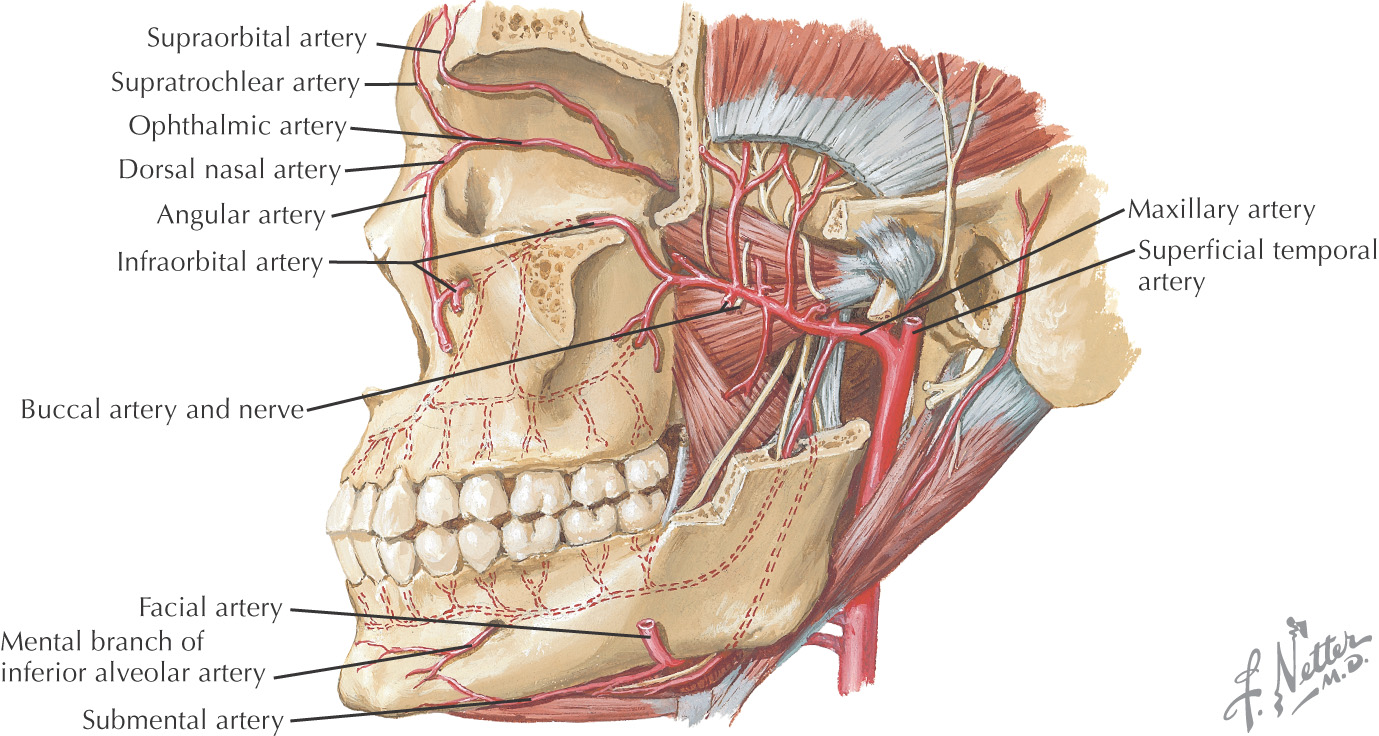
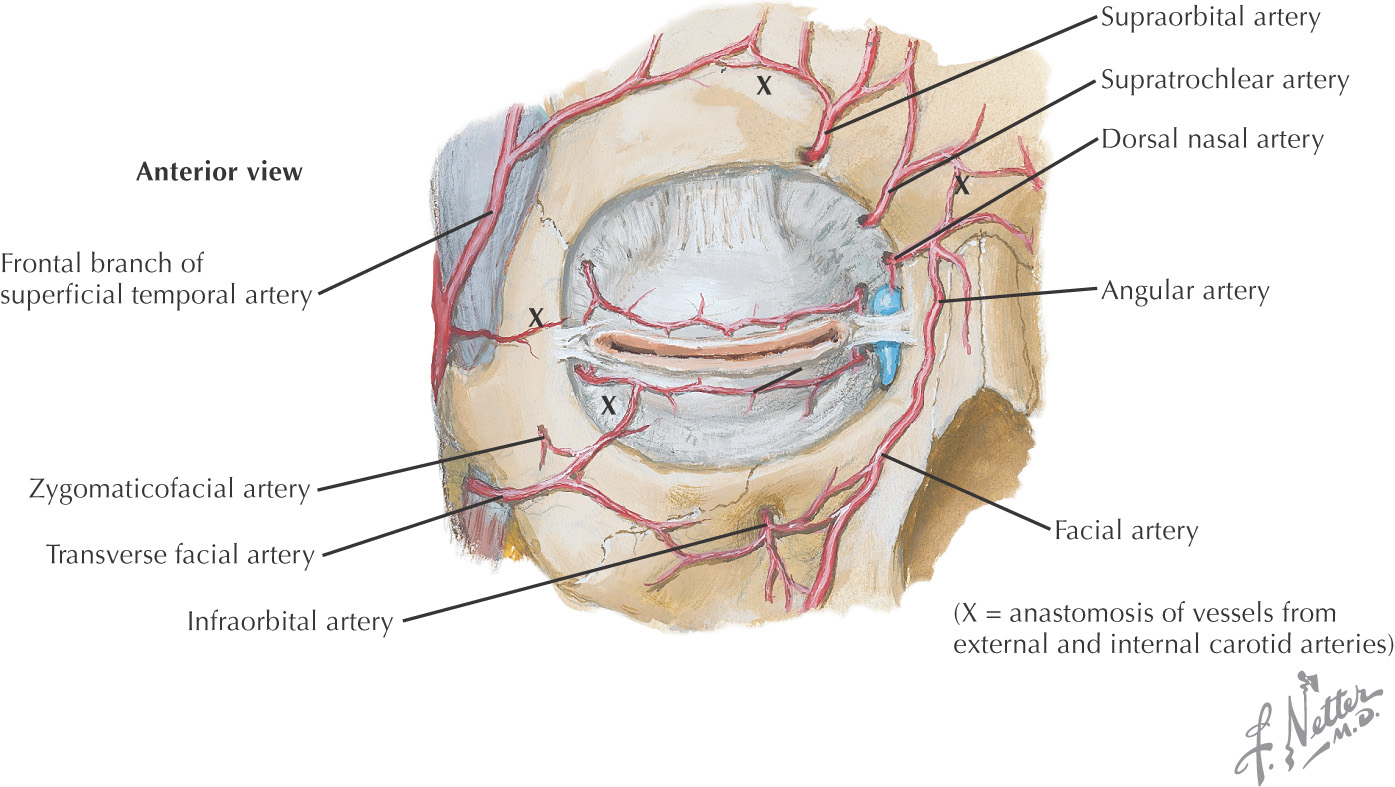
Most of the arterial supply to the face arises from the superficial temporal artery and facial branches of the external carotid artery
The maxillary branch of the external carotid supplies most areas that the superficial temporal and facial branches do not supply
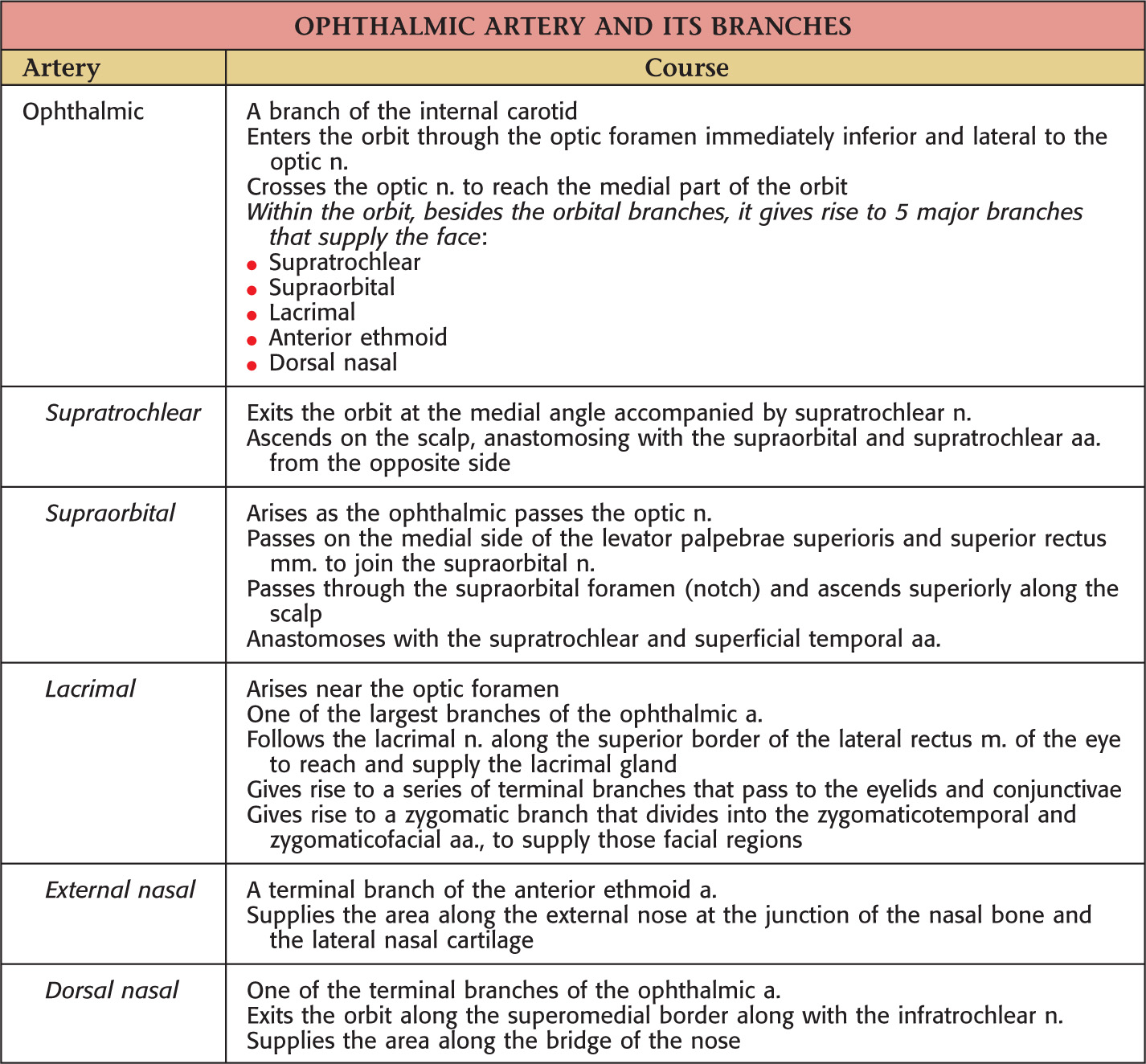
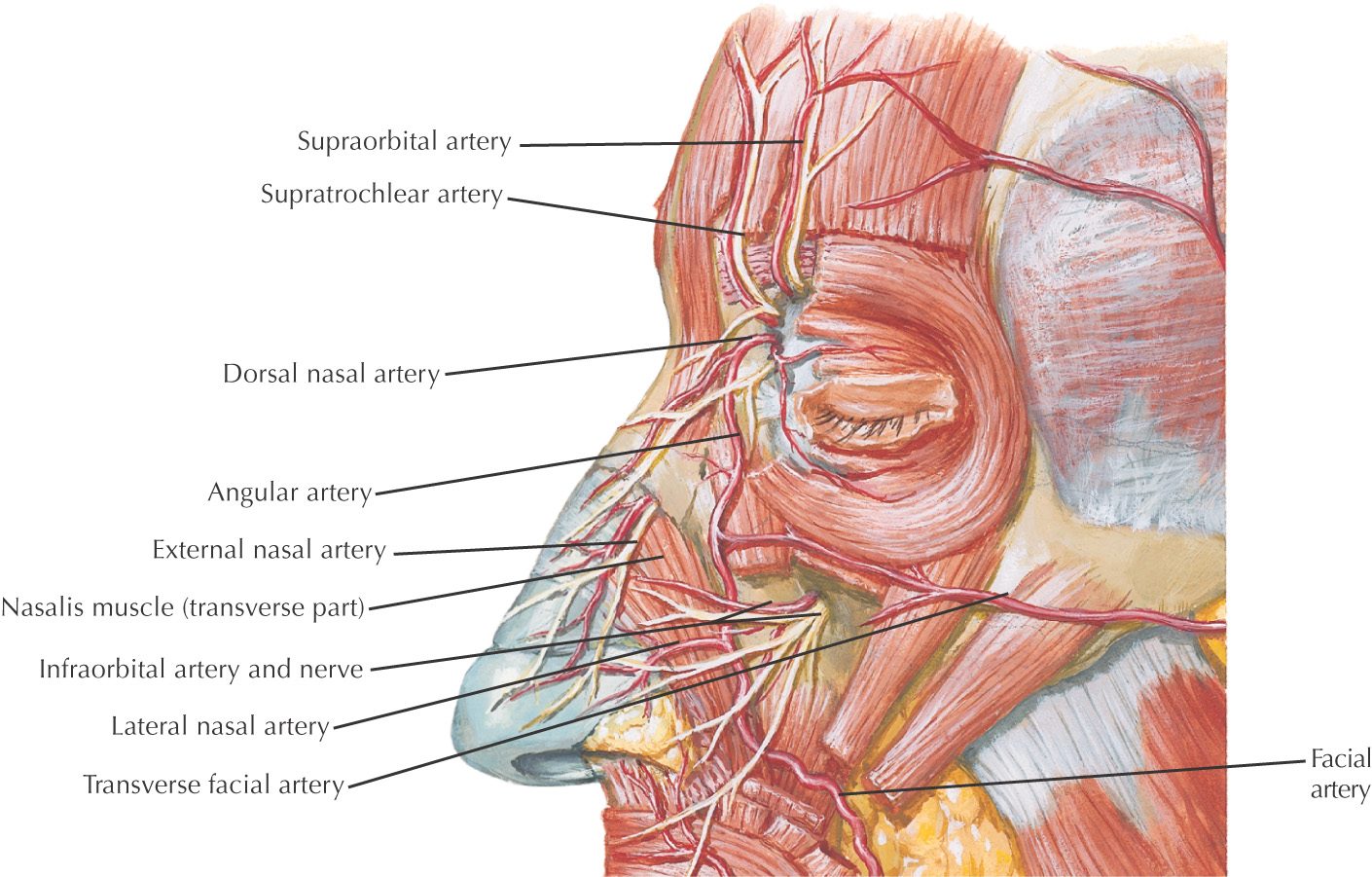
The internal carotid artery supplies the anterior portion of the forehead and dorsal surface of the nose via ophthalmic artery branches
The arteries of the face anastomose freely
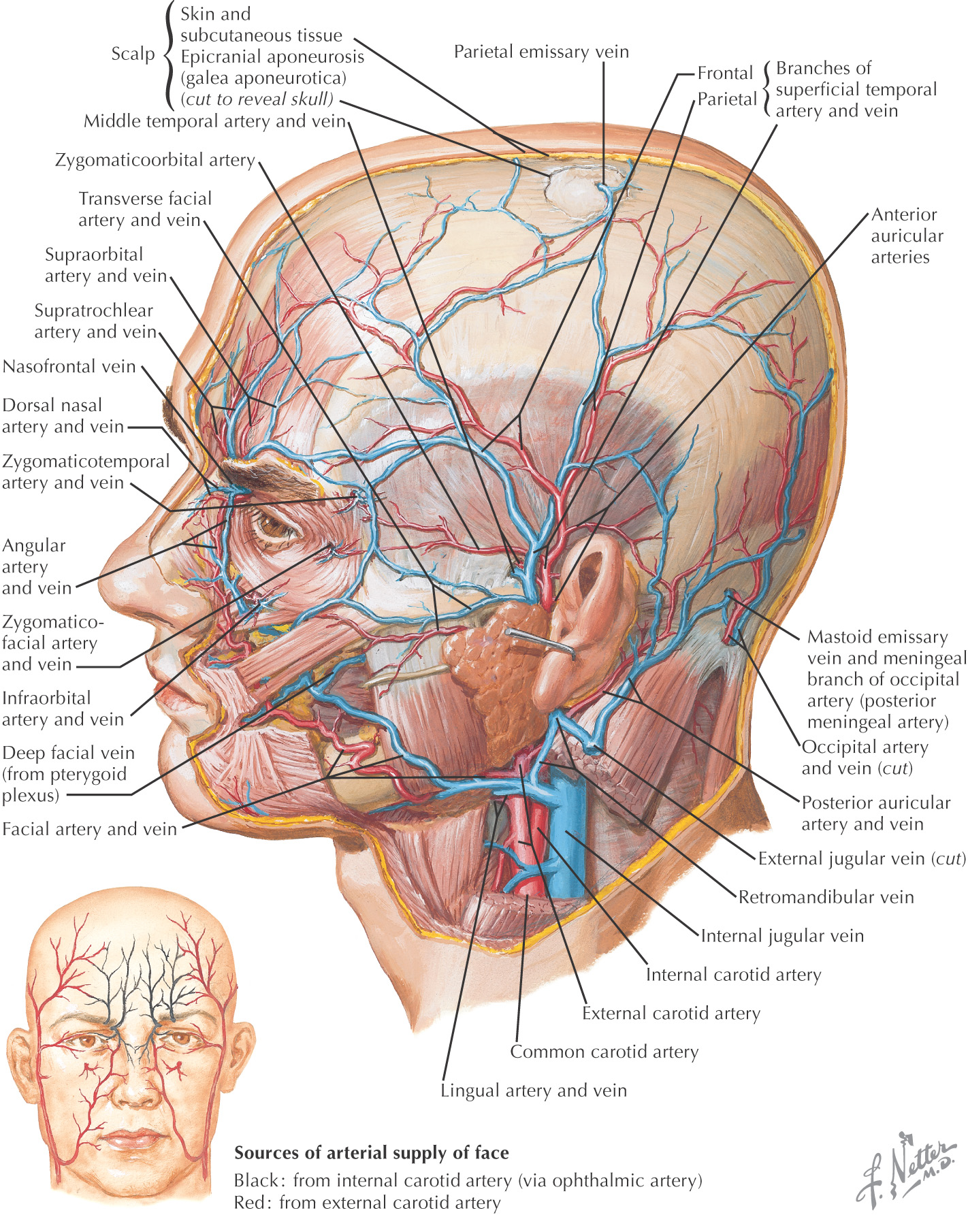
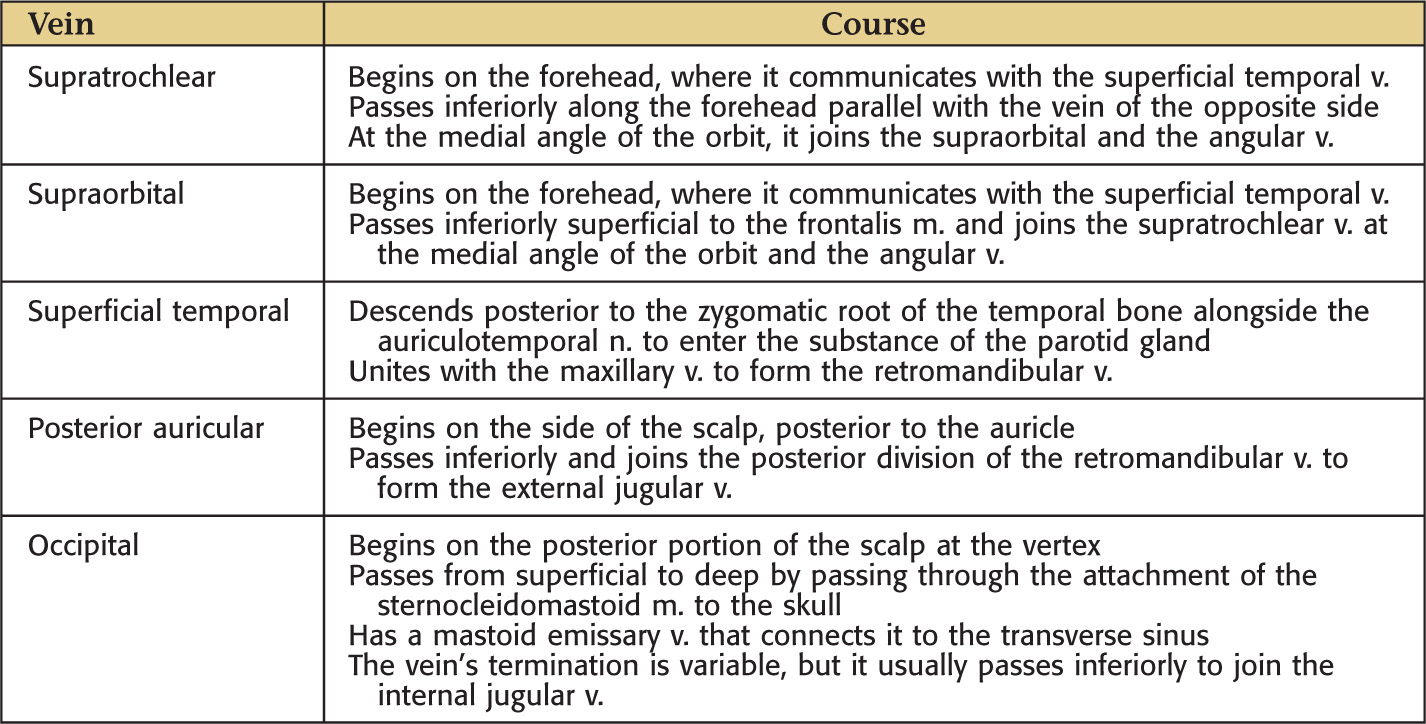
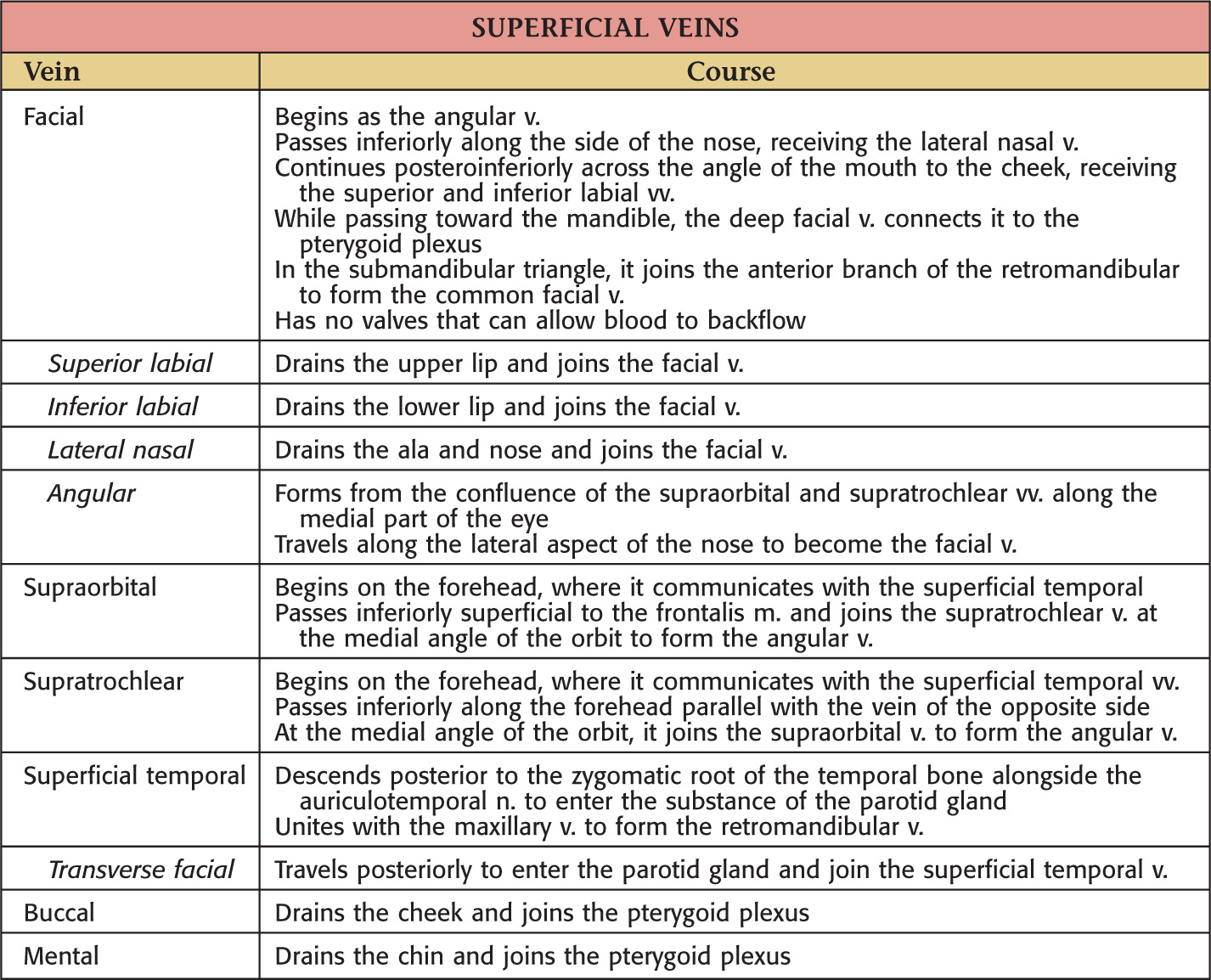
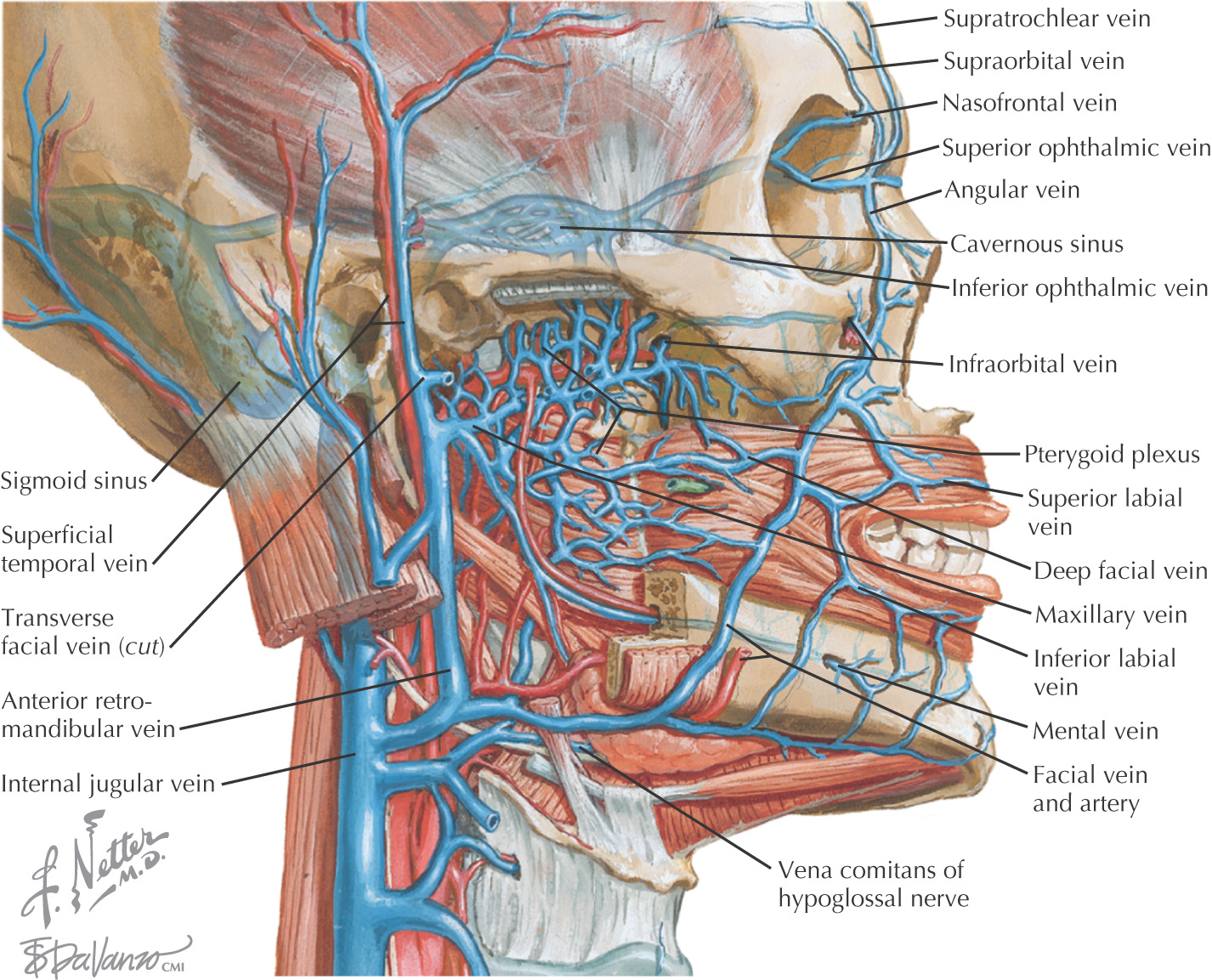
Facial veins have similar distribution pattern to that for the arteries
Highly variable
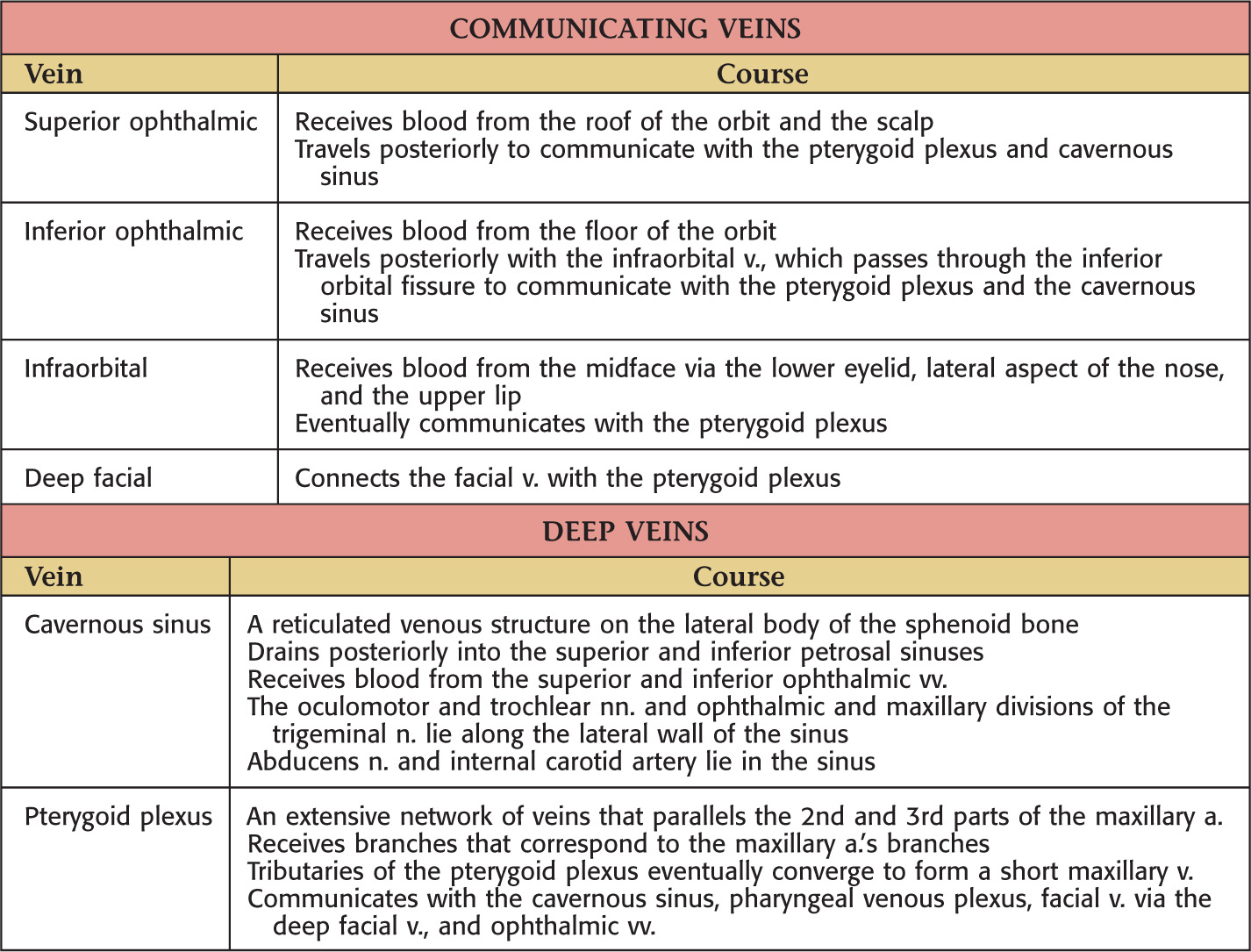
Connect to the deeper vessels such as the pterygoid plexus and cavernous sinus
Many motor and sensory nerves supply the face
All motor nerves are from the facial nerve and supply the muscles of facial expression
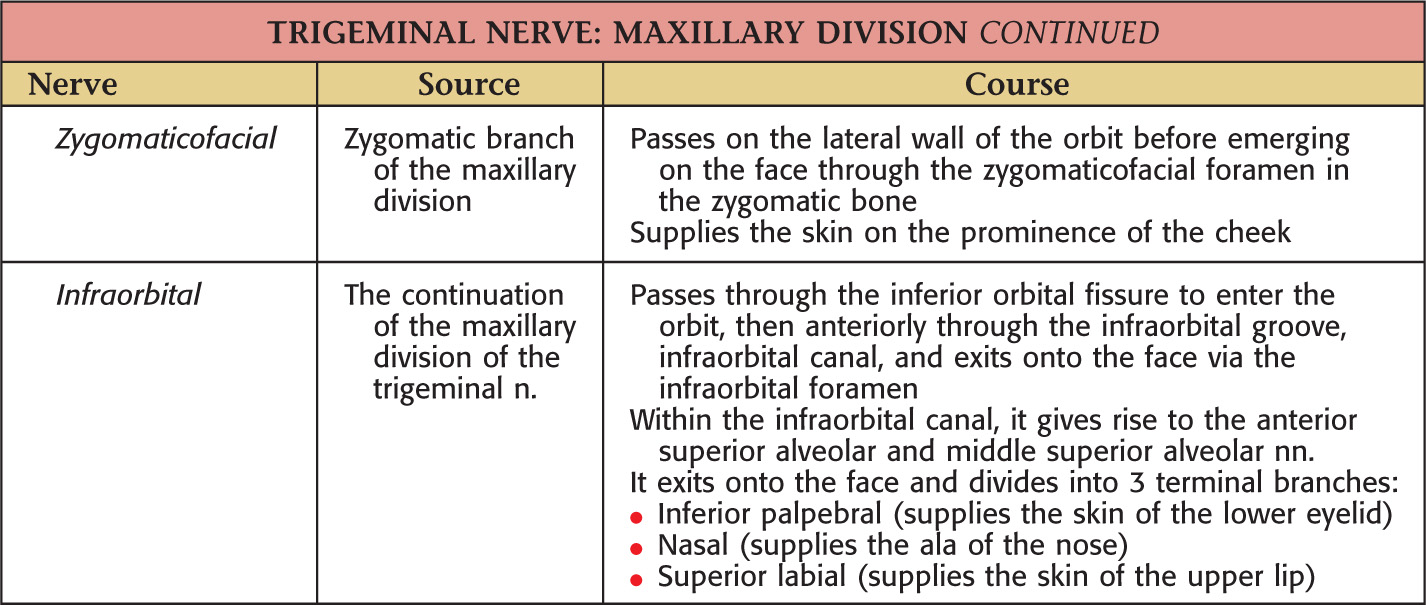
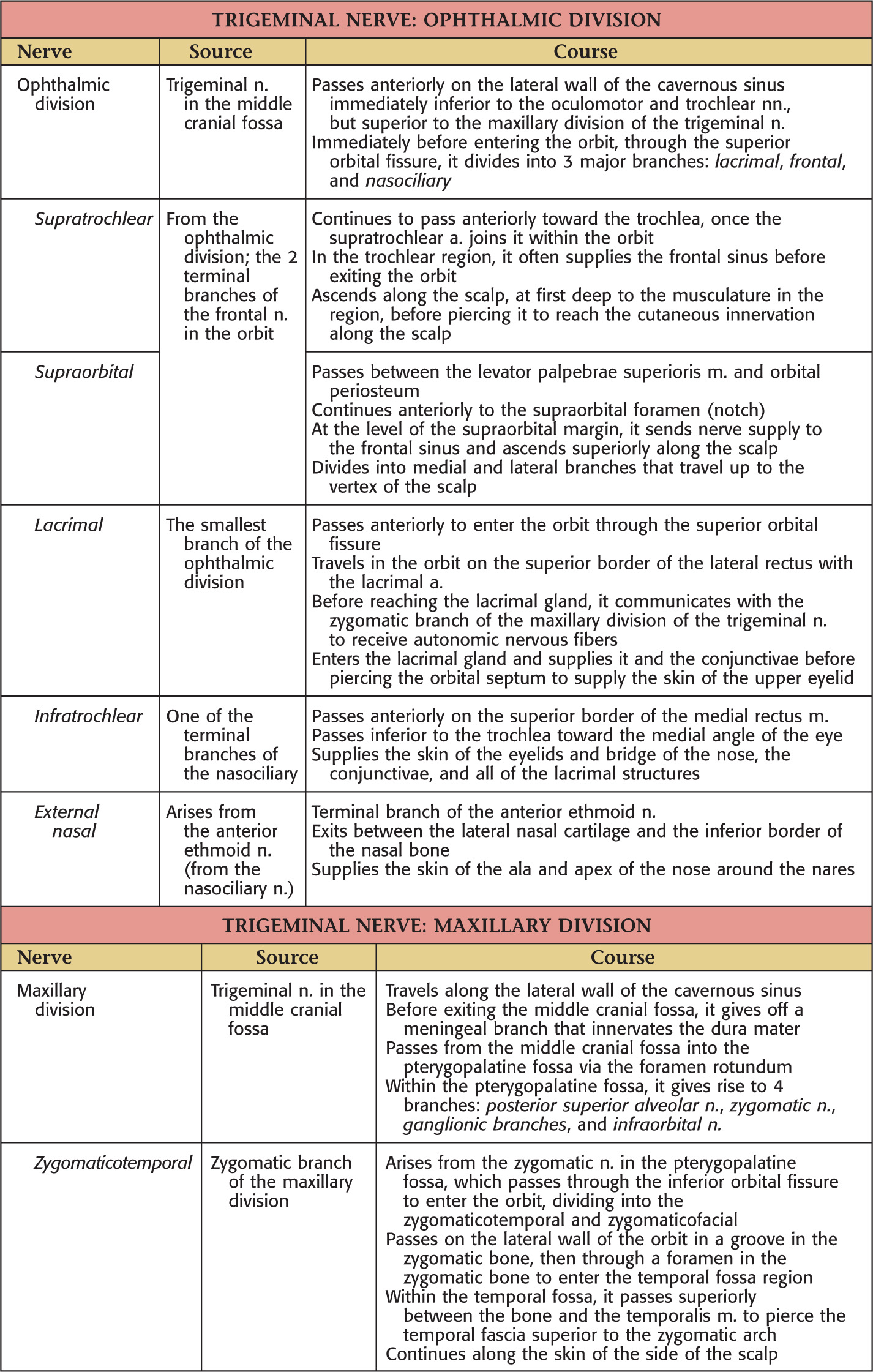
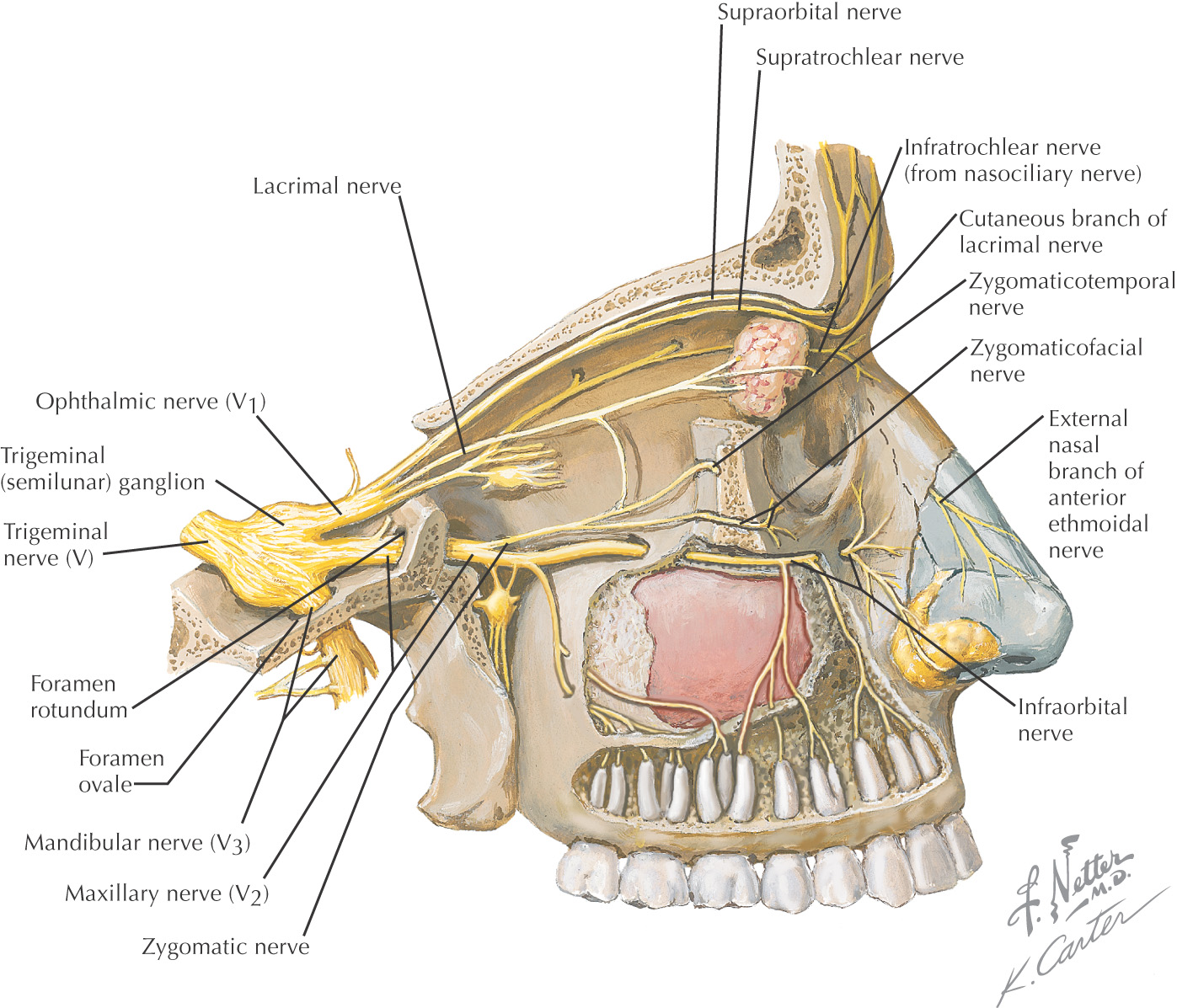
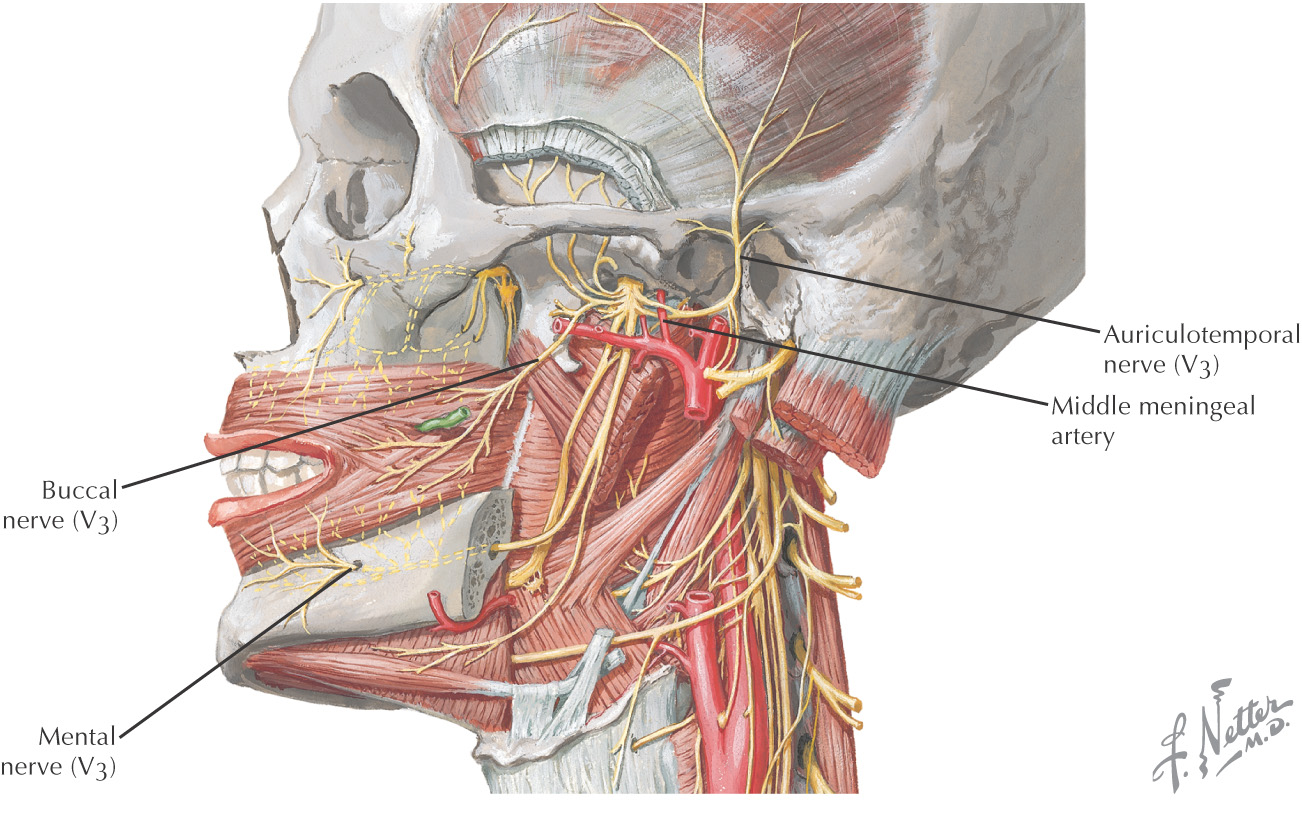
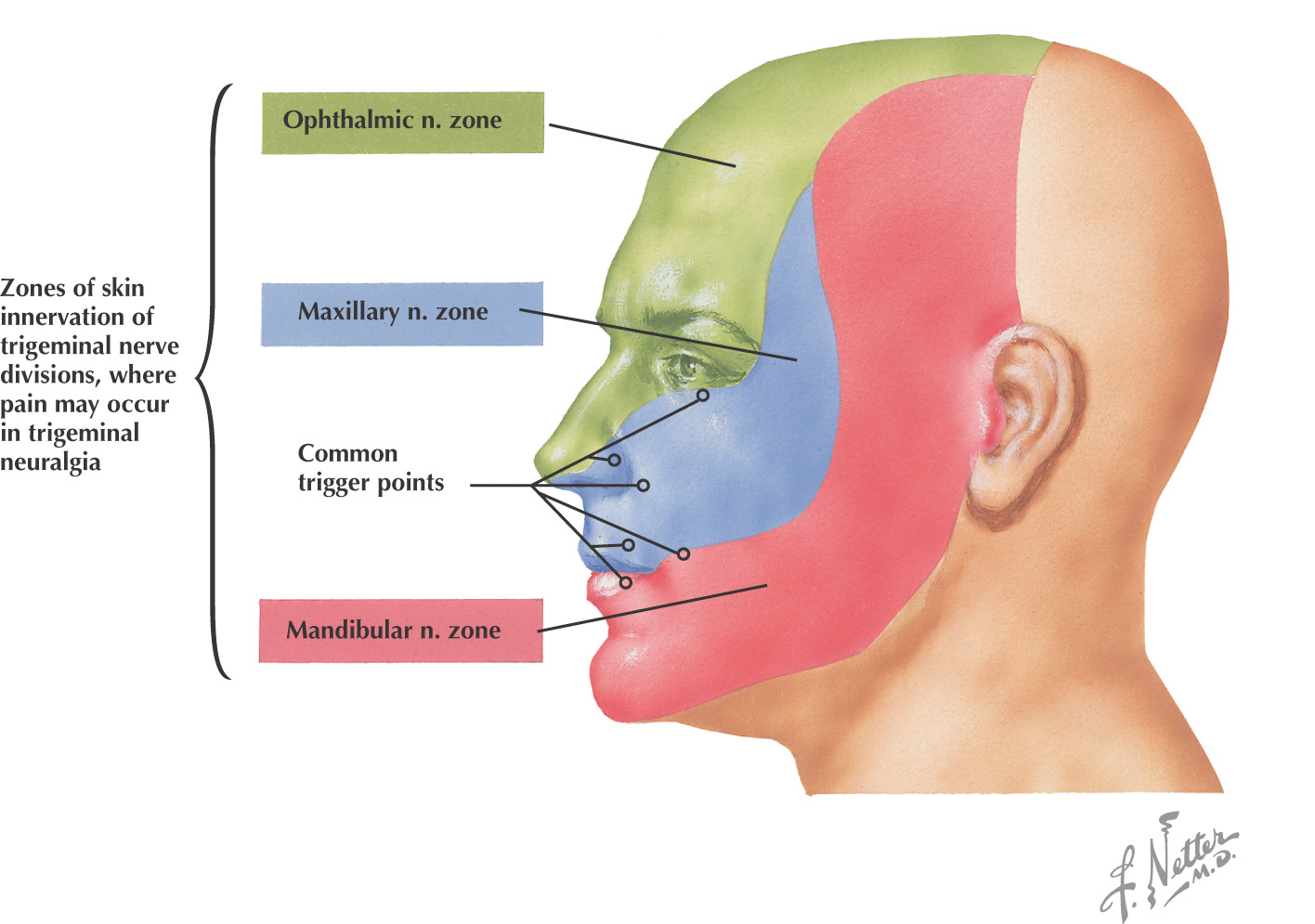
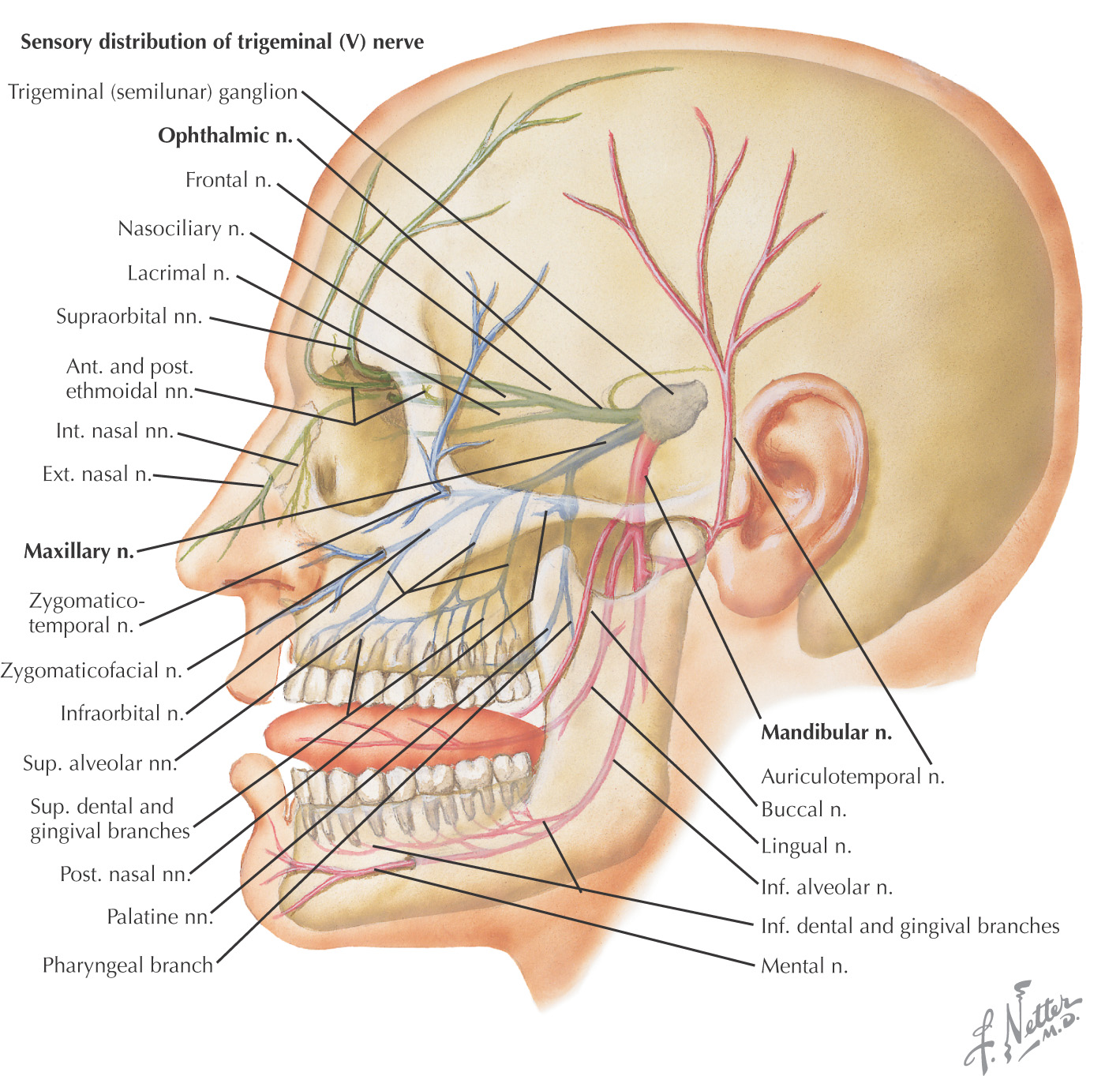
Sensory nerves of the face are derived mainly from the 3 divisions of the trigeminal nerve (V1, V2, V3)
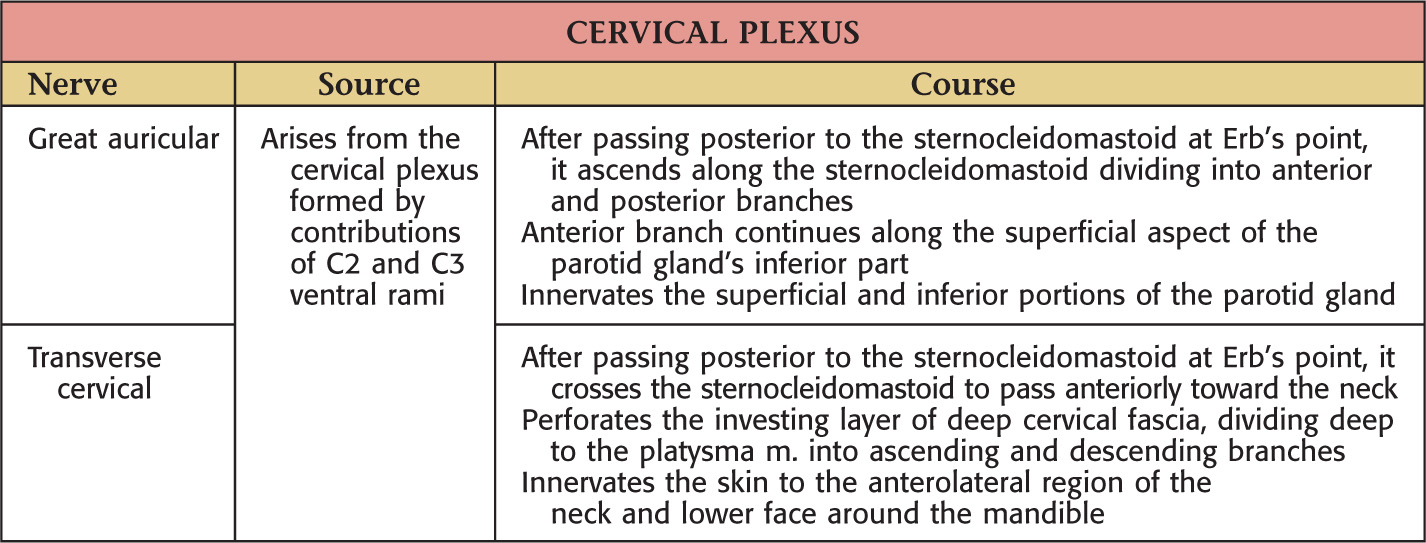
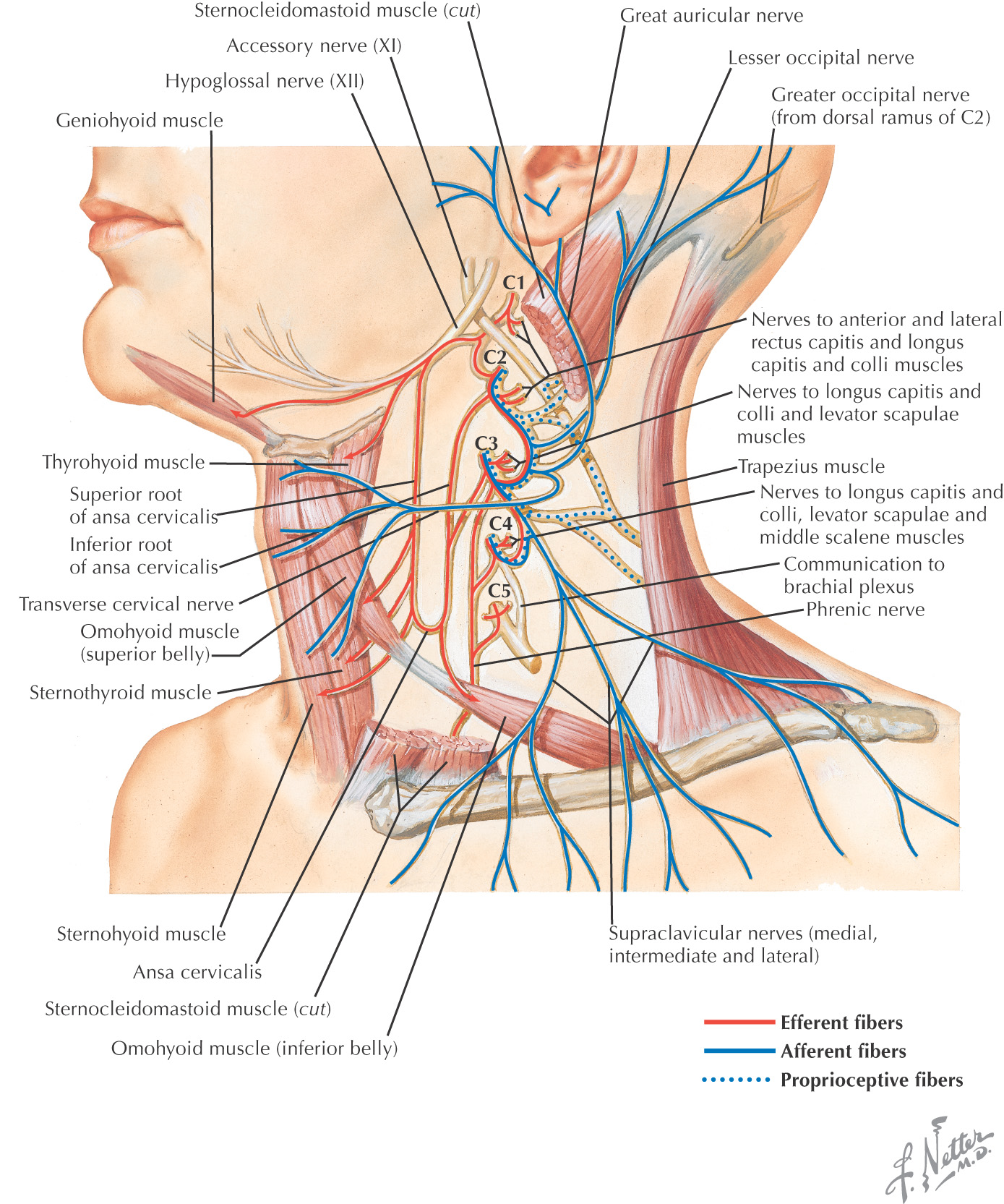
Some sensory branches are from the cervical plexus

Also called tic douloureux
Usually affects the maxillary (V2) or mandibular (V3) division of the trigeminal nerve; rarely affects the ophthalmic division (V1)
Bilateral involvement suggests other factors such as multiple sclerosis
More common in the 5th and 6th decades of life
Cause is unknown–theories involve nerve irritation from abnormal vascularity or tumor compression, or a nerve injury
Periods of intense (lasting 1 to 2 minutes), paroxysmal pain along one of the divisions of the trigeminal nerve
Usually unilateral
Pain normally is initiated by a particular sensory stimulus, such as light touch (putting on makeup, washing the face, shaving, a light breeze), mastication, or brushing teeth
Commonly, trigeminal neuralgia is treated pharmacologically with anticonvulsants, such as carbamazepine (Tegretol)
If drug therapy is unsuccessful, neurosurgery may be required, such as percutaneous radiofrequency rhizotomy of the nerve, glycerol injection of the trigeminal ganglion, or nerve decompression
Alternative and complementary medicine treatments have included acupuncture and meditation
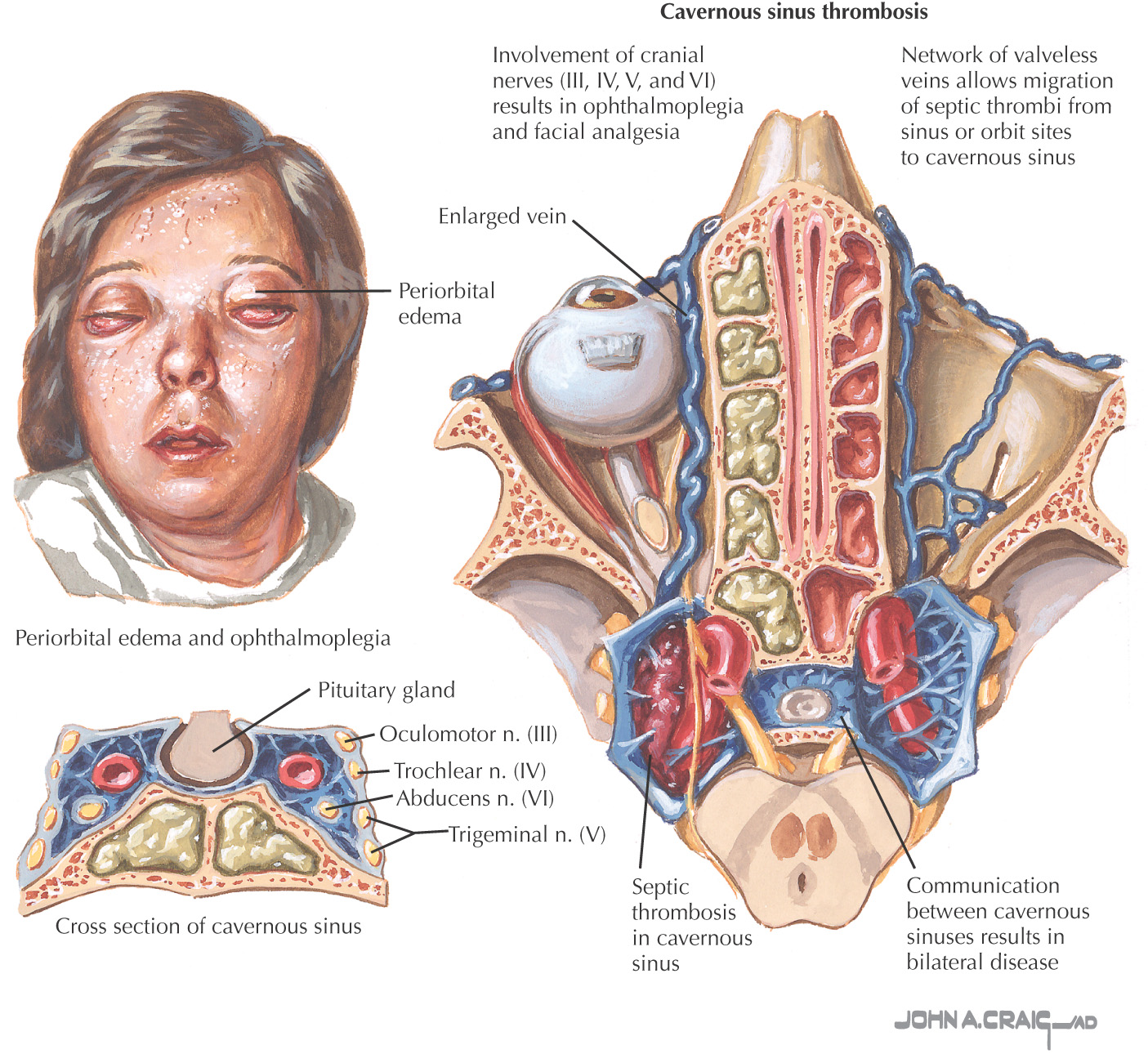
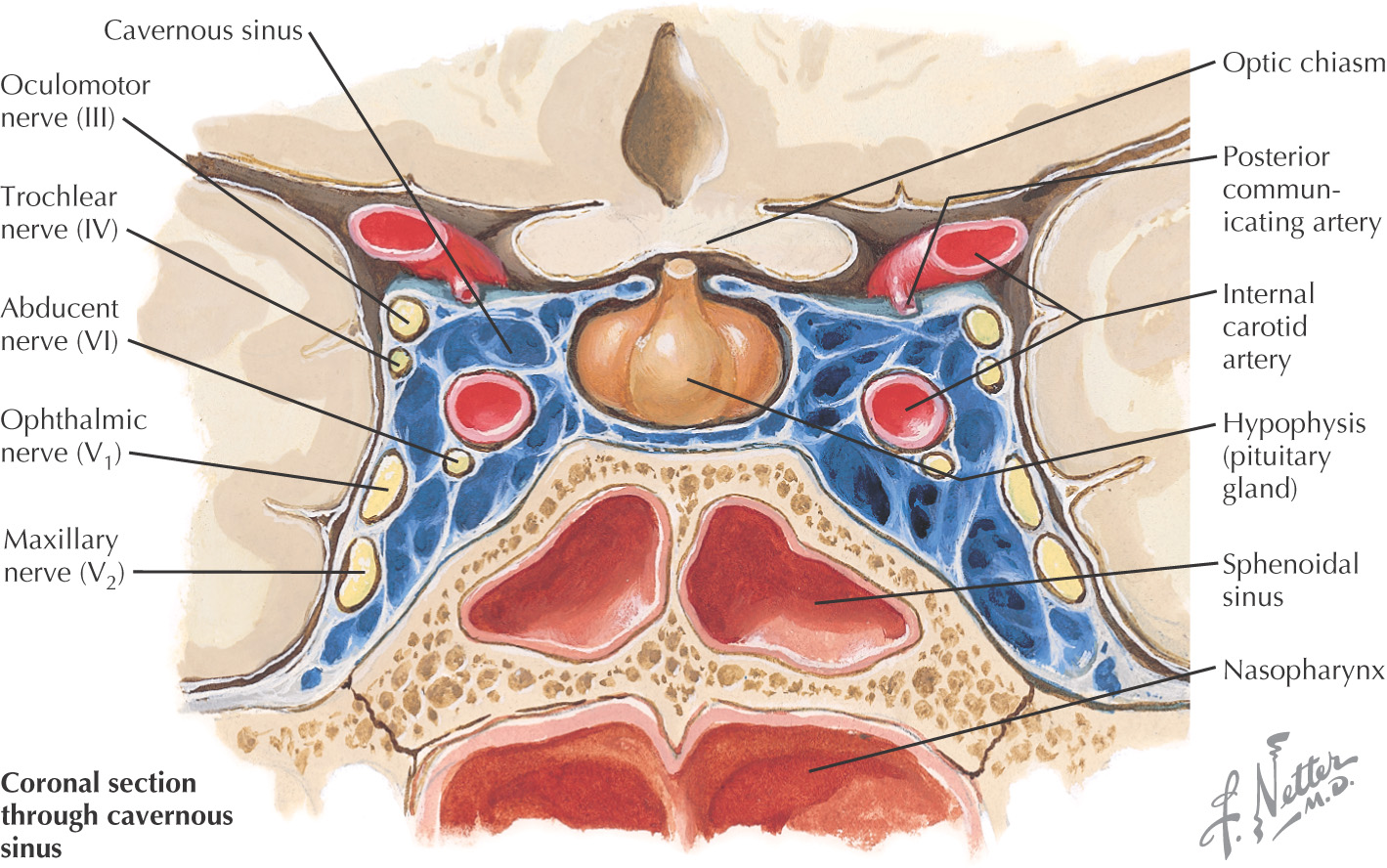
Pathologic condition involving the cavernous sinus that is often caused by a thrombosis, tumor, aneurysm, fistula, or trauma
When caused by a thrombosis, the syndrome usually occurs as a sepsis from the central portion of the face or paranasal sinuses from their connection to the cavernous sinus
Before the advent of antibiotics, death was the normal outcome from the sepsis
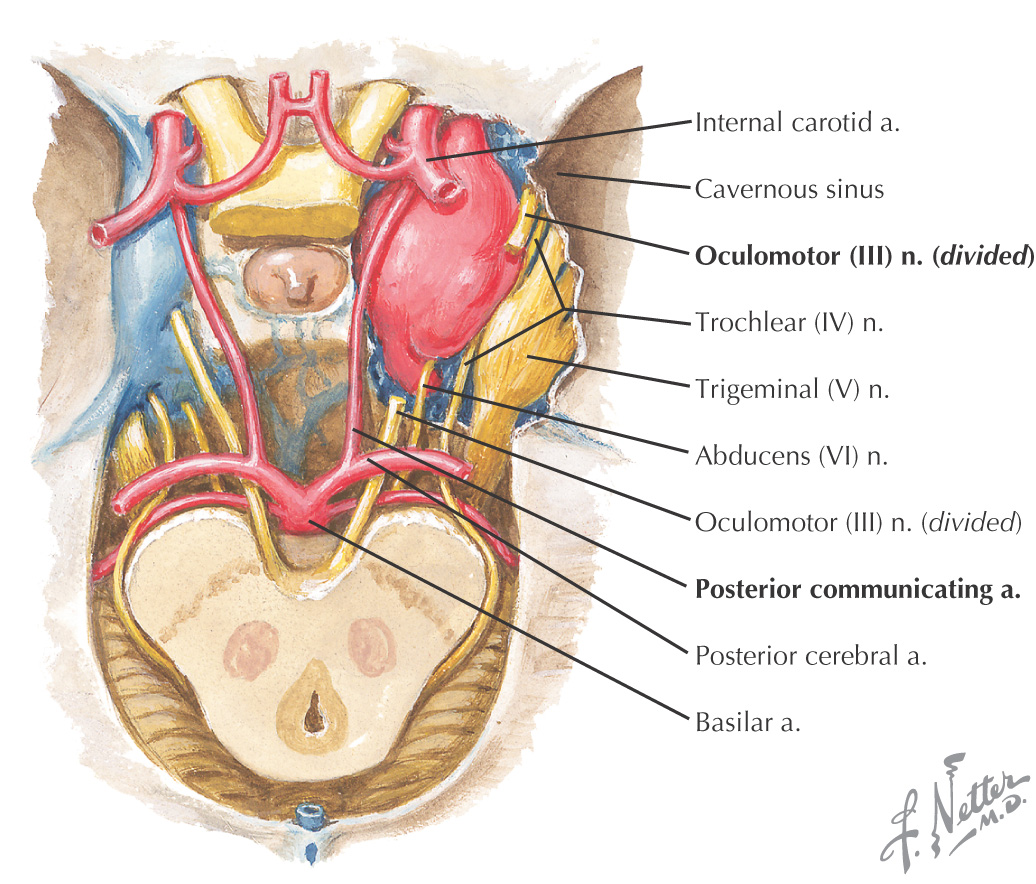
It affects the contents of the cavernous sinus, including:
• Internal carotid artery with sympathetics
Common clinical manifestations include:
• Ophthalmoplegia with diminished pupillary light reflexes
• Venous congestion leading to periorbital edema