Overview and Topographic Anatomy
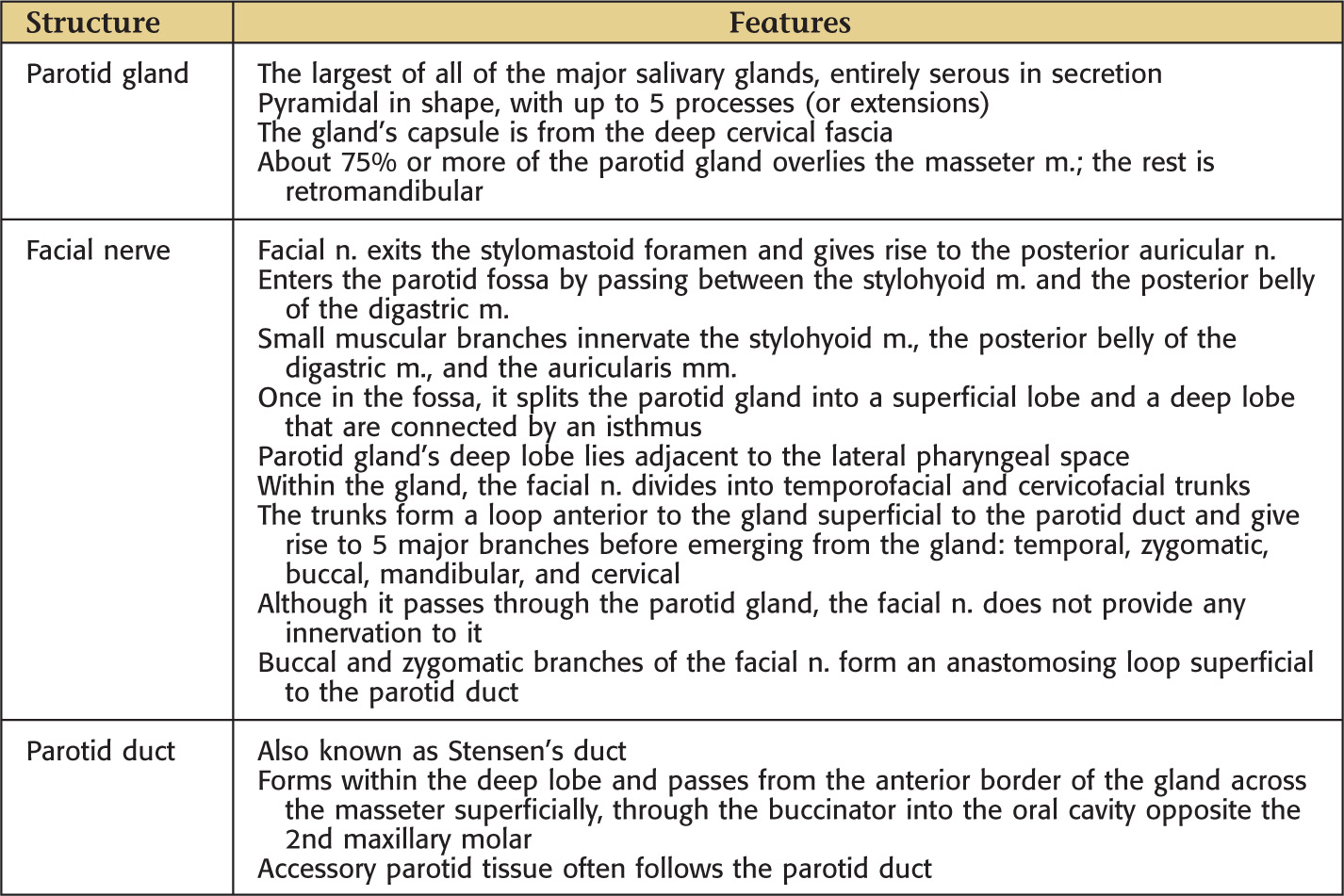
The largest of all the major salivary glands
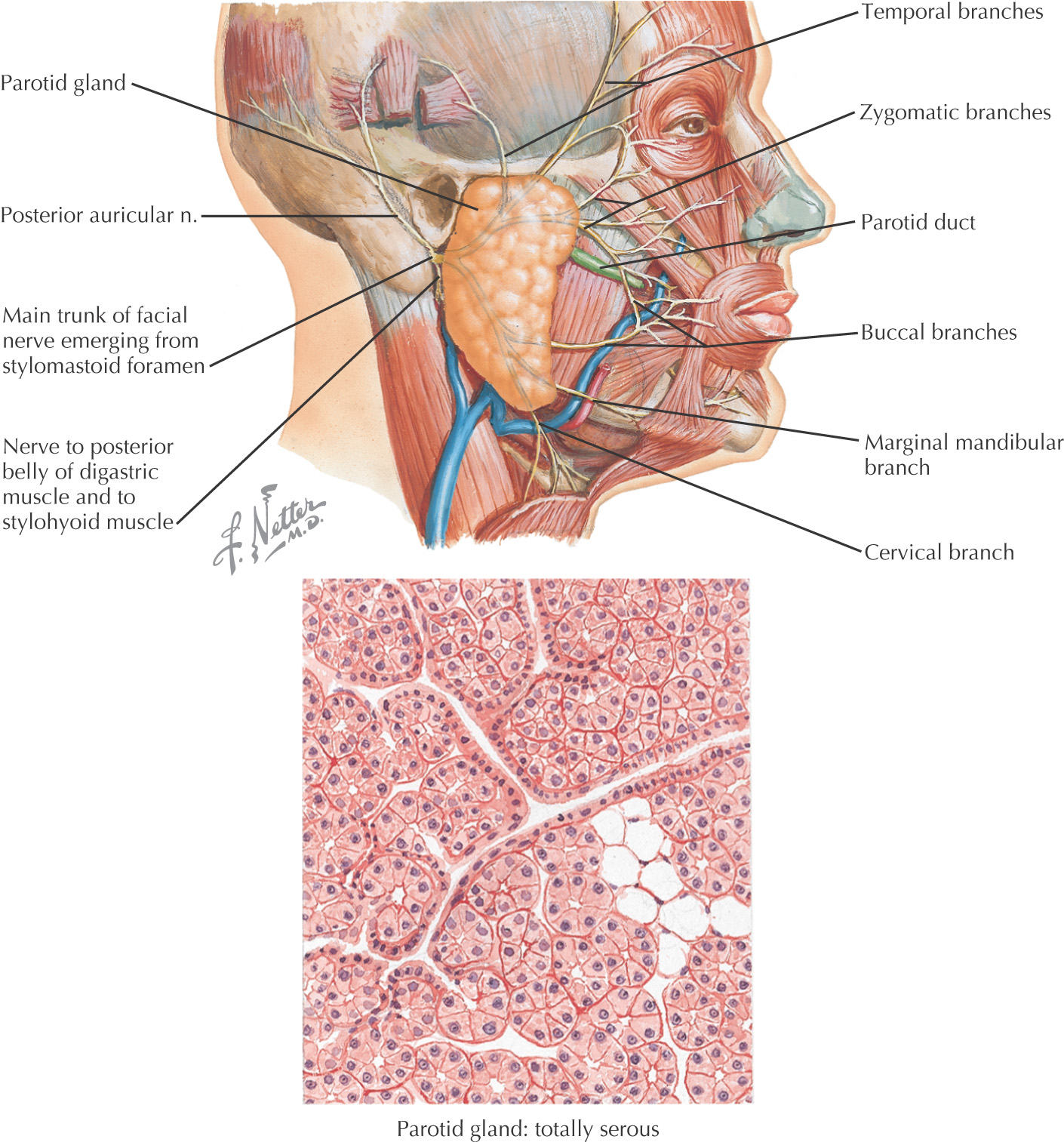
Entirely serous in secretion
Pyramidal in shape, with up to 5 processes (or extensions)
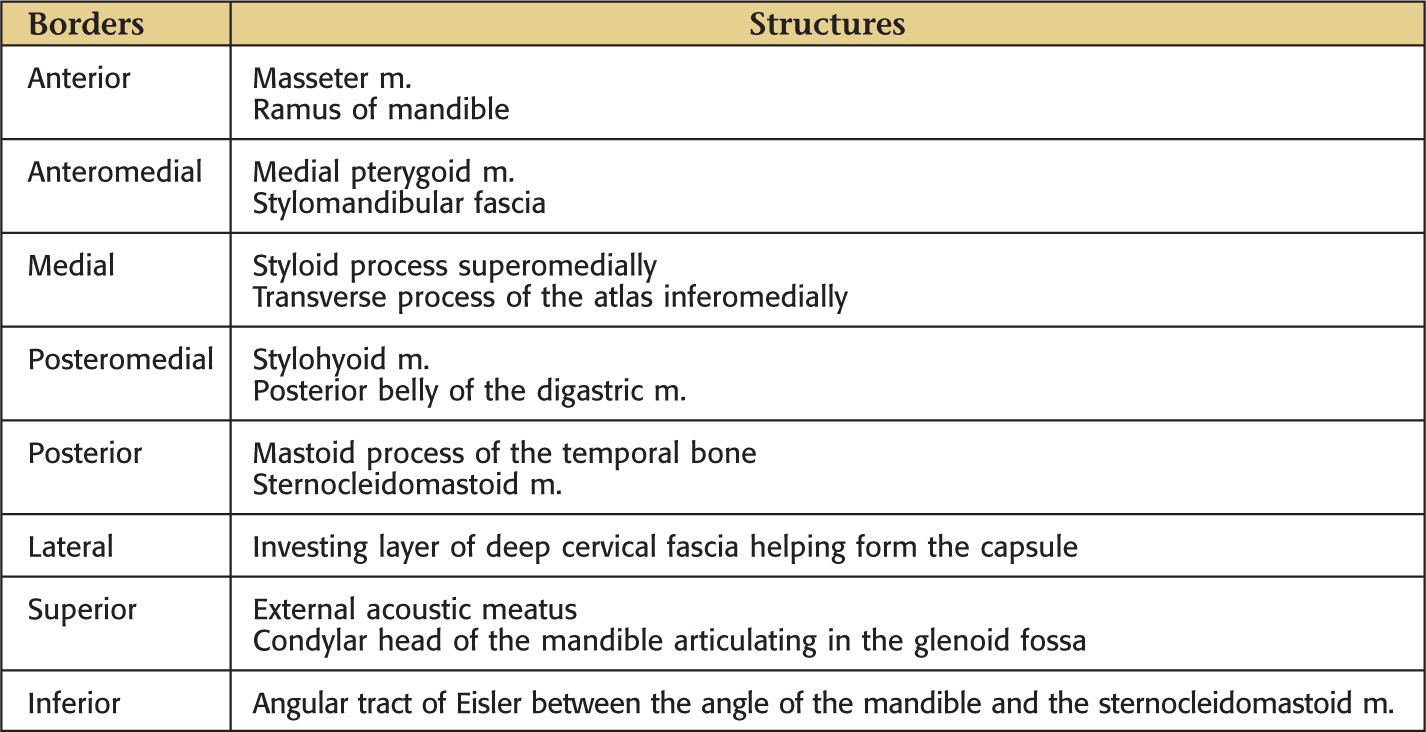
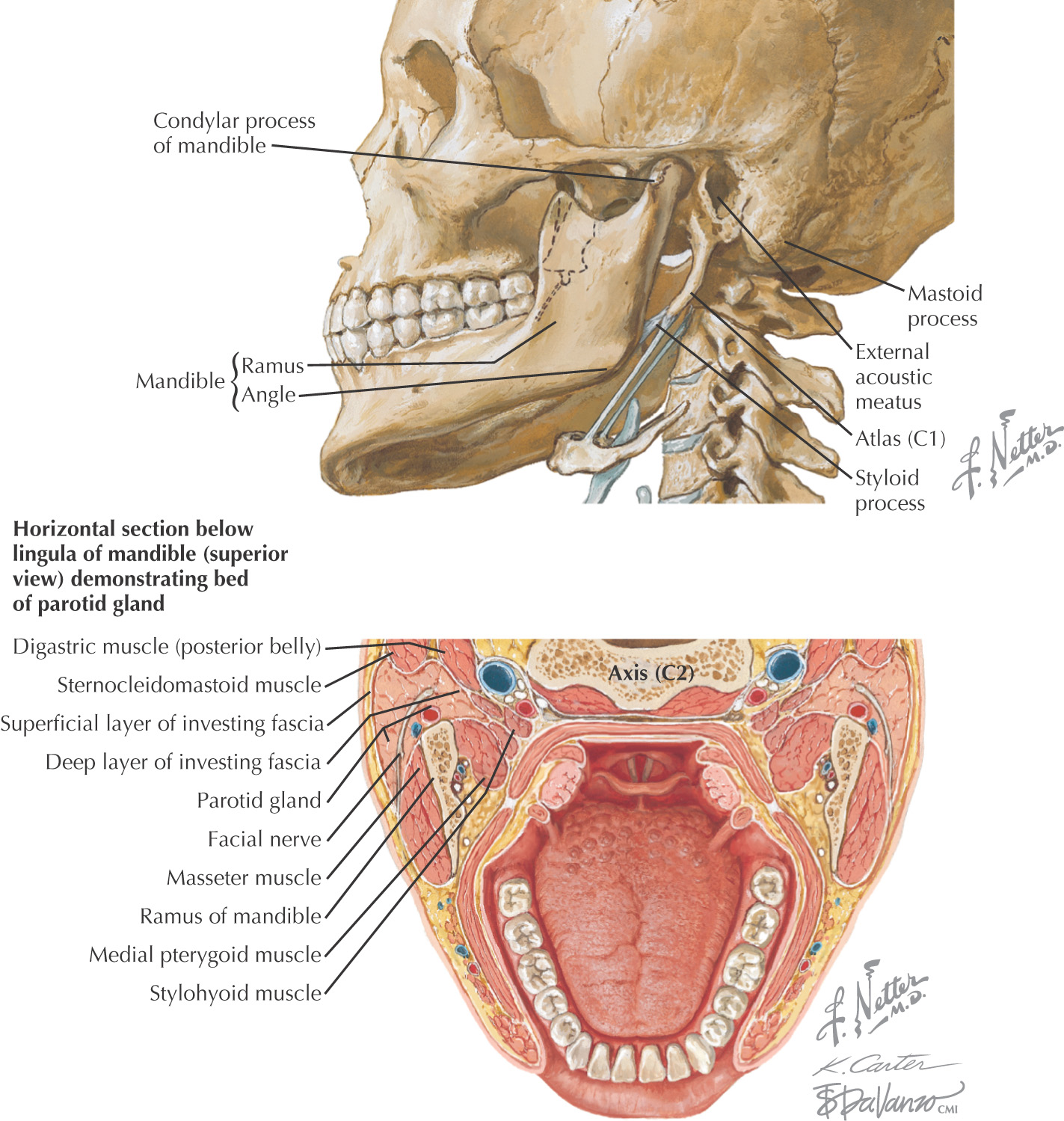
The gland’s capsule is from the deep cervical fascia
Approximately 75% or more of the parotid gland overlies the masseter muscle; the rest is retromandibular
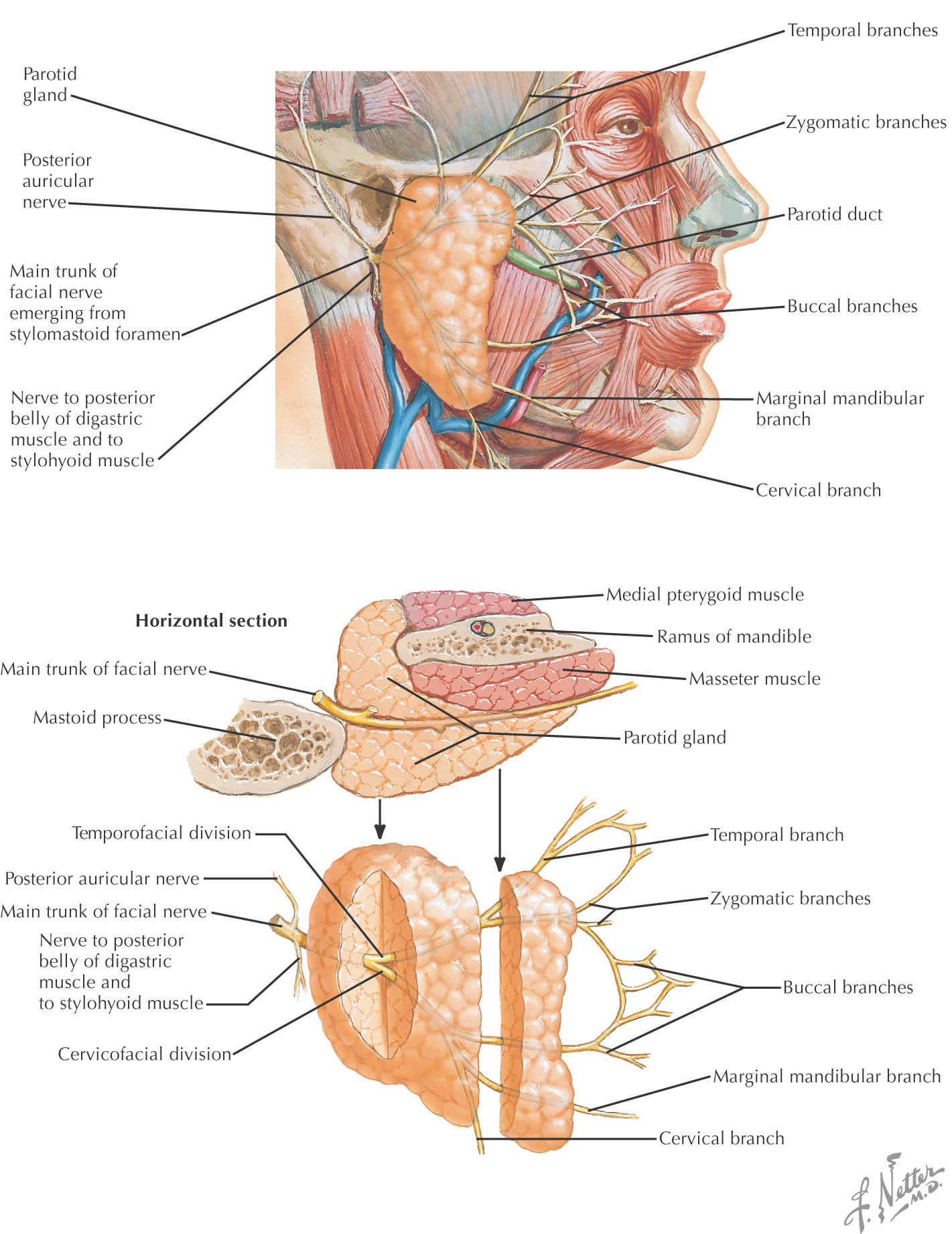
Facial nerve enters the parotid fossa by passing between the stylohyoid muscle and the posterior belly of the digastric muscle, then splits the gland into a superficial lobe and a deep lobe that are connected by an isthmus
Deep lobe lies adjacent to the lateral pharyngeal space
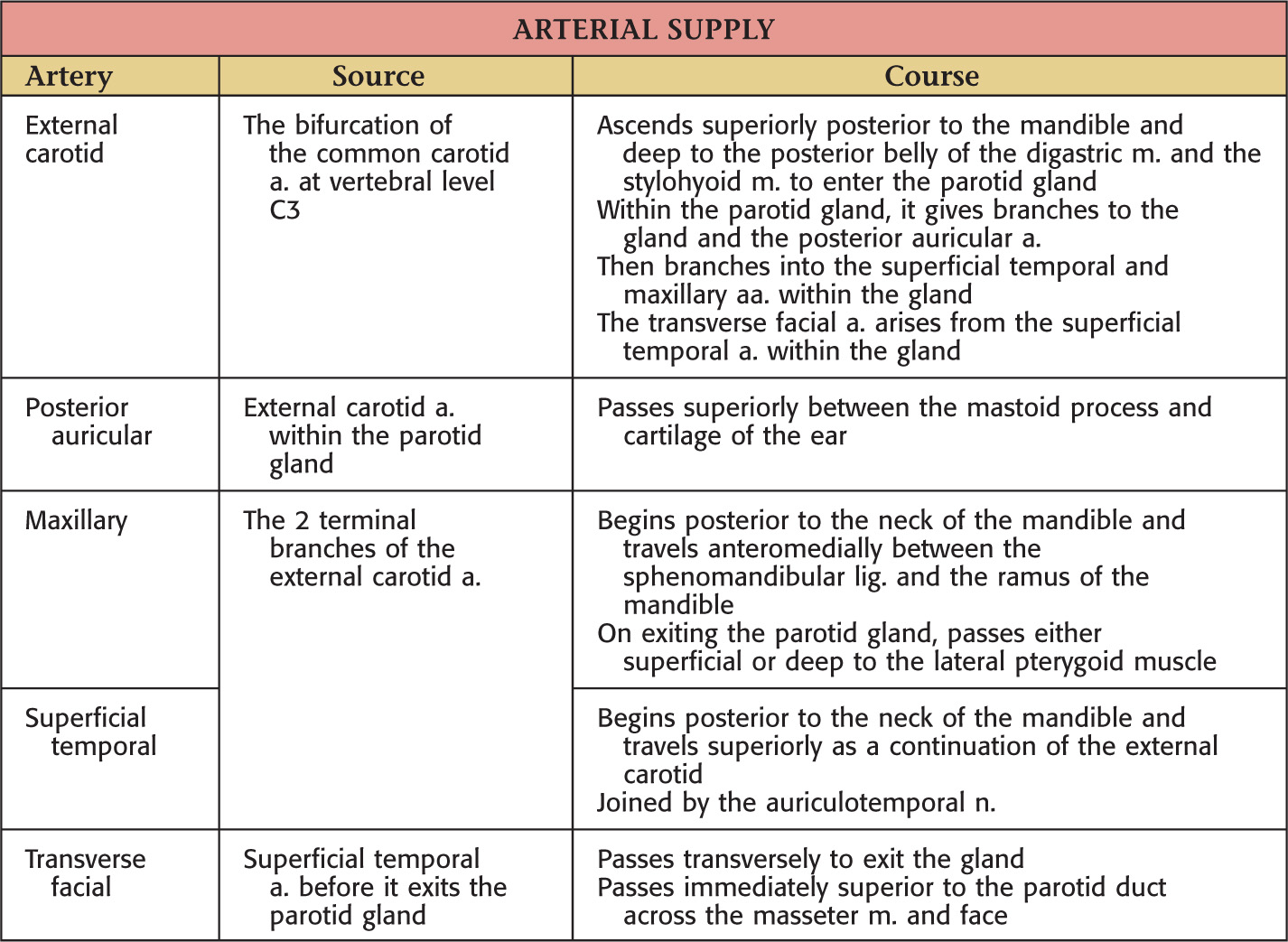
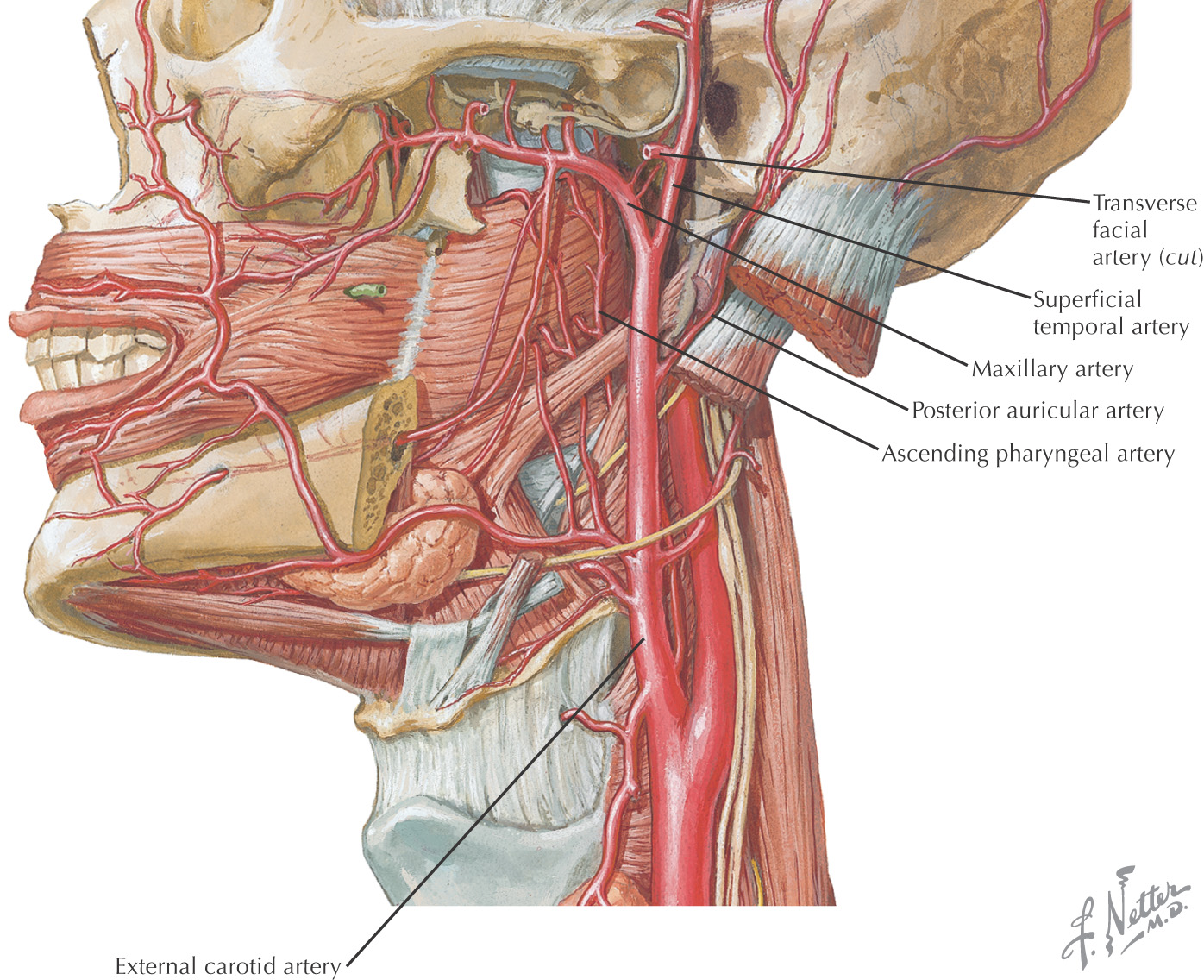
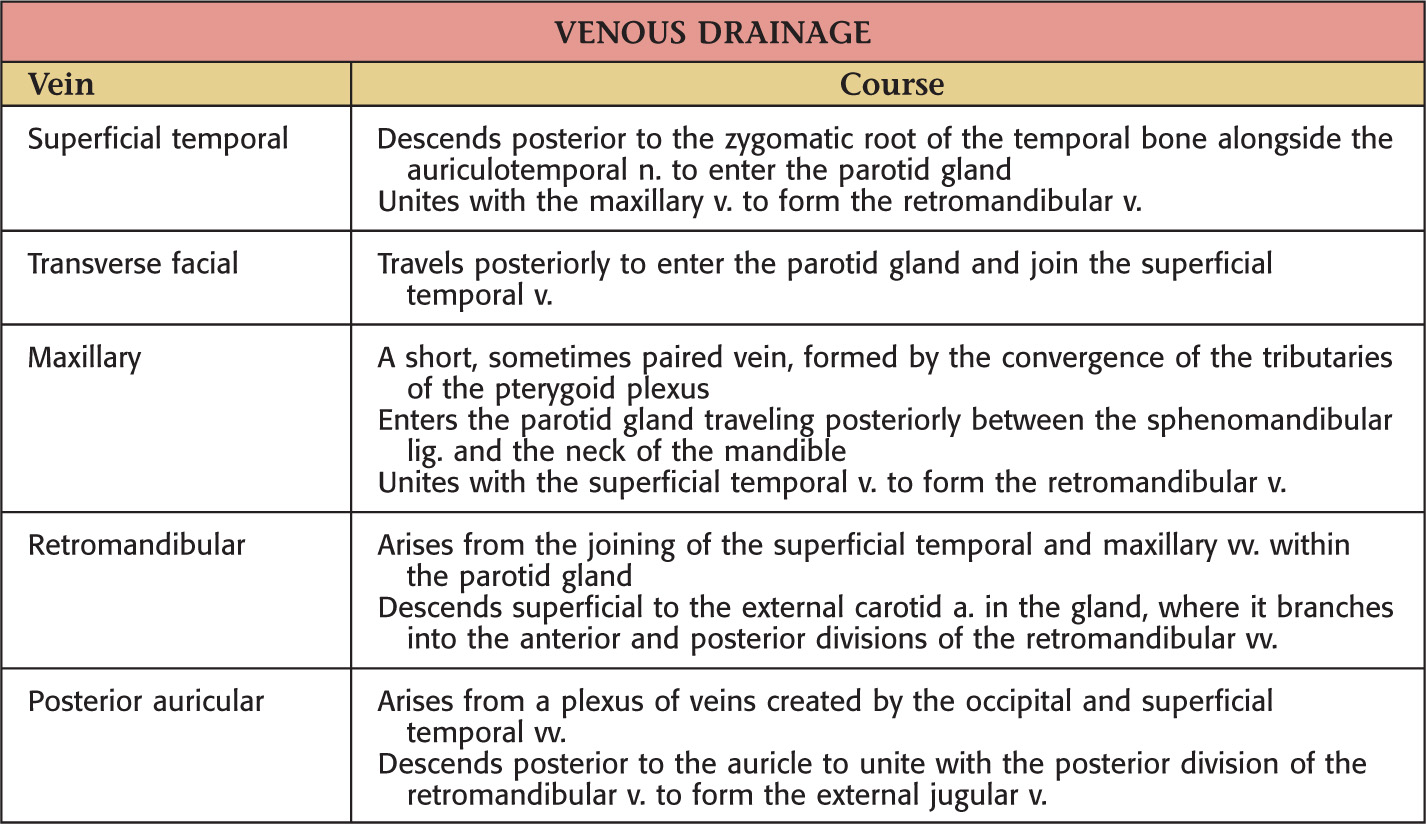
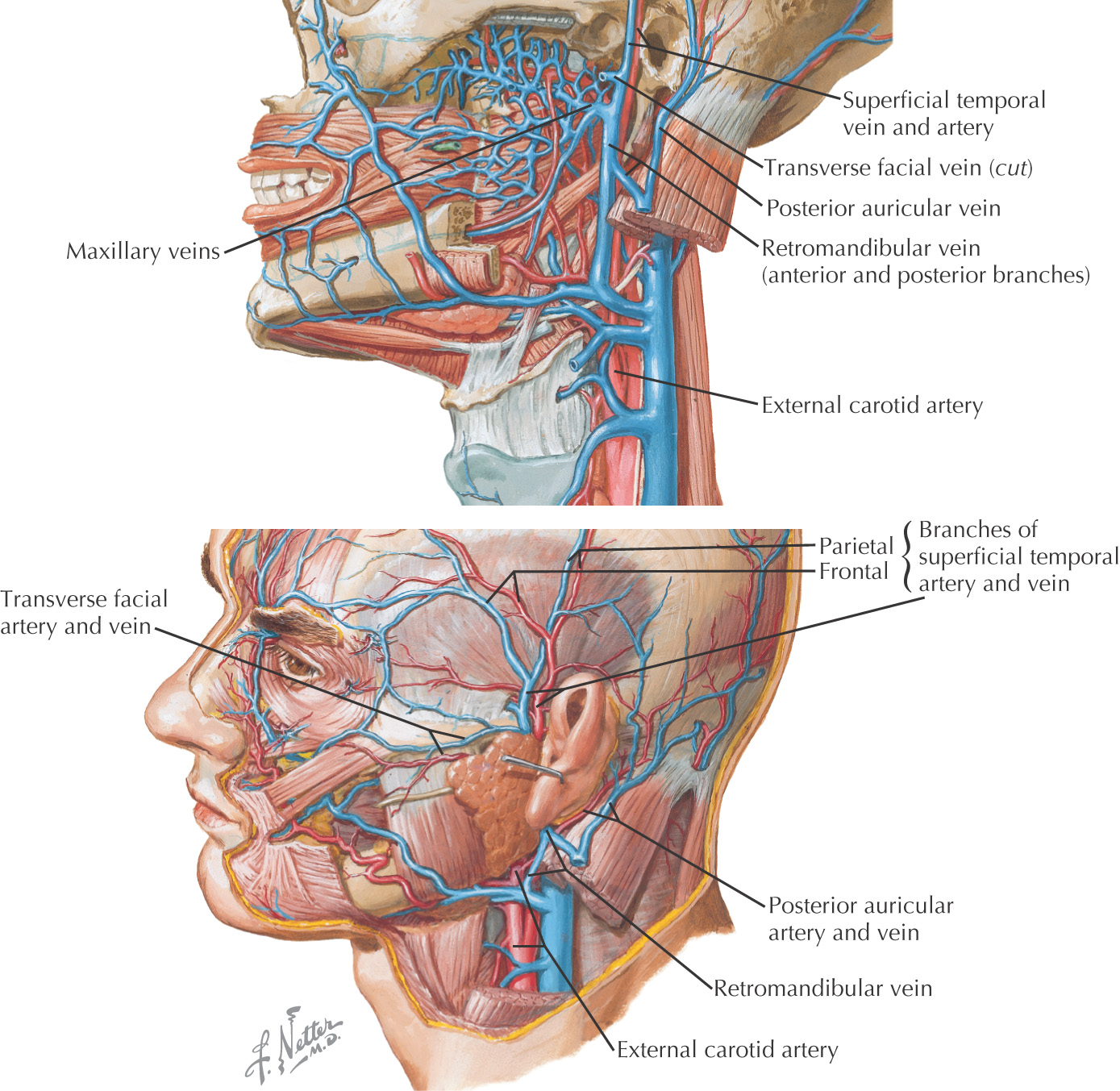
Transverse facial artery parallels the parotid duct slightly superior to the duct
Buccal and zygomatic branches of the facial nerve form an anastomosing loop superficial to the parotid duct
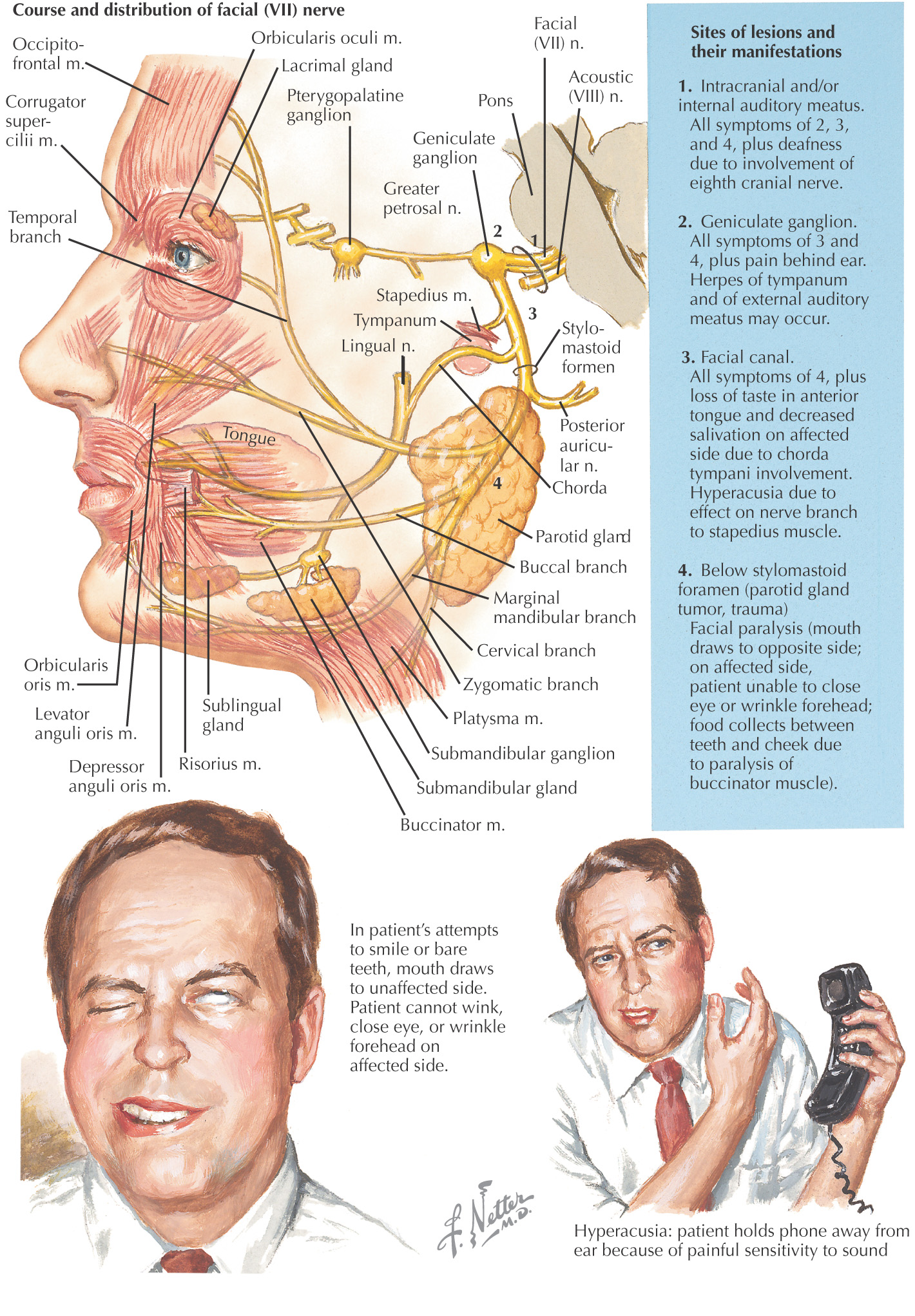
Unilateral facial paralysis from facial nerve (cranial nerve VII) damage
Approximately 80% of cases have unclear etiology
Evidence suggests herpes simplex virus (HSV-1) infection is a cause
• Proposed mechanism: When the virus becomes active at the facial nerve, if the inflammation is in the bony facial canal, limited room for expansion results in nerve compression
Bacterial infections also have been implicated
• In some cases of otitis media, bacteria may enter the facial canal, and any resulting inflammatory response could compress the facial nerve
Temporary Bell’s palsy can result from dental procedures if inferior alveolar nerve block anesthetic is improperly administered in the parotid fossa; signs and symptoms disappear when the anesthetic effects wear off
Mild cases produce a facial nerve neurapraxia; the prognosis for complete recovery is very good, usually within 2 to 3 weeks
In more moderate cases, an axonotmesis may occur, producing wallerian degeneration; full recovery may take 2 to 3 months
In a small percentage of cases, function is never completely recovered
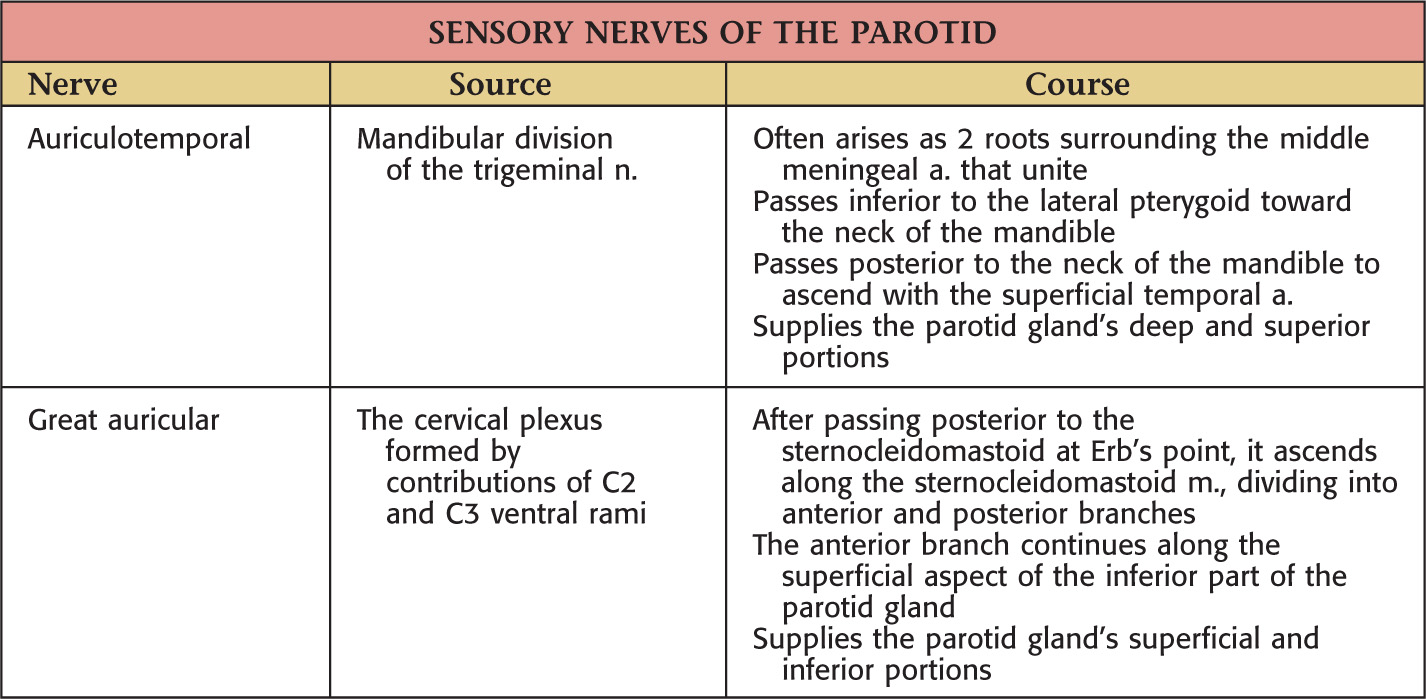
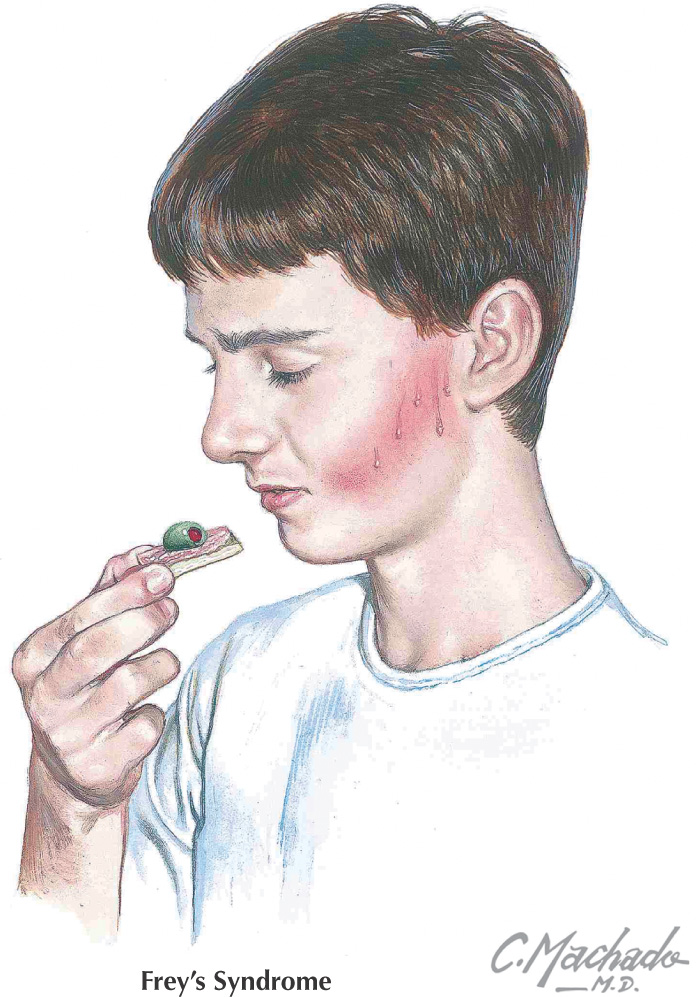
Caused by regeneration of the auriculotemporal autonomic fibers in an abnormal fashion, innervating the sweat glands near the parotid gland after a parotidectomy
Symptoms include sweating and redness in the distribution of the auriculotemporal nerve during eating
Diagnosis is via Minor’s starch iodine test–creates a dark spot over the gustatory sweating area
Treatments include tympanic neurectomy (severing the parasympathetic component) and the topical anticholinergic glycopyrrolate (Robinul)
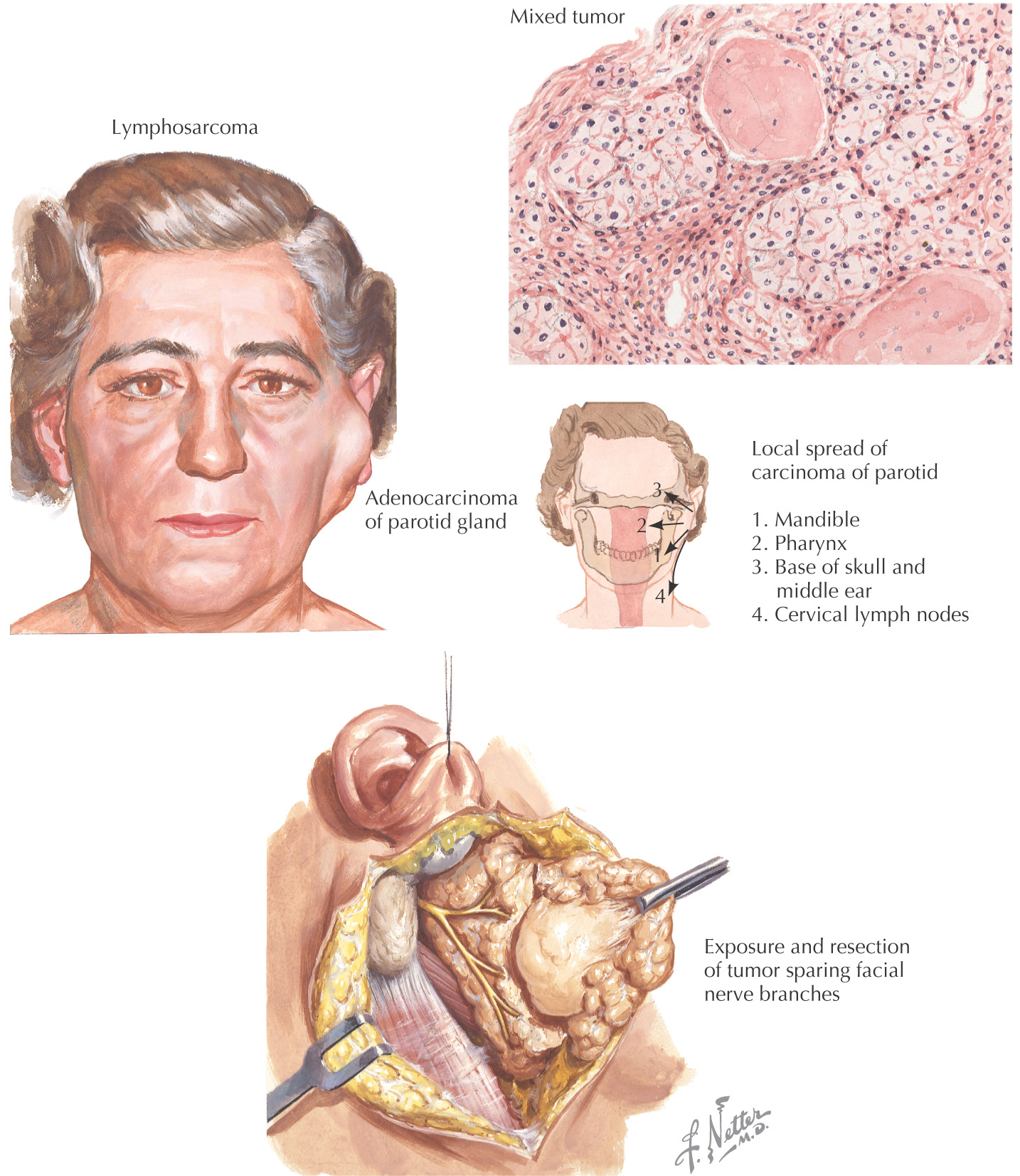
80% of parotid tumors are benign
The most common benign tumor is a pleomorphic adenoma, which, if present for many years, can convert to a highly malignant carcinoma
When pleomorphic adenomas extend through the capsule, they must be removed to reduce recurrence
Because of the proximity, these tumors can extend into the lateral pharyngeal space
Removal of the tumor with its surrounding capsule and tissue is important to obtain a low recurrence rate
• Histologically, pleomorphic adenomas have extensions through the tumor capsule into adjacent tissue, so simple enucleation would allow recurrence from tumor cells left behind
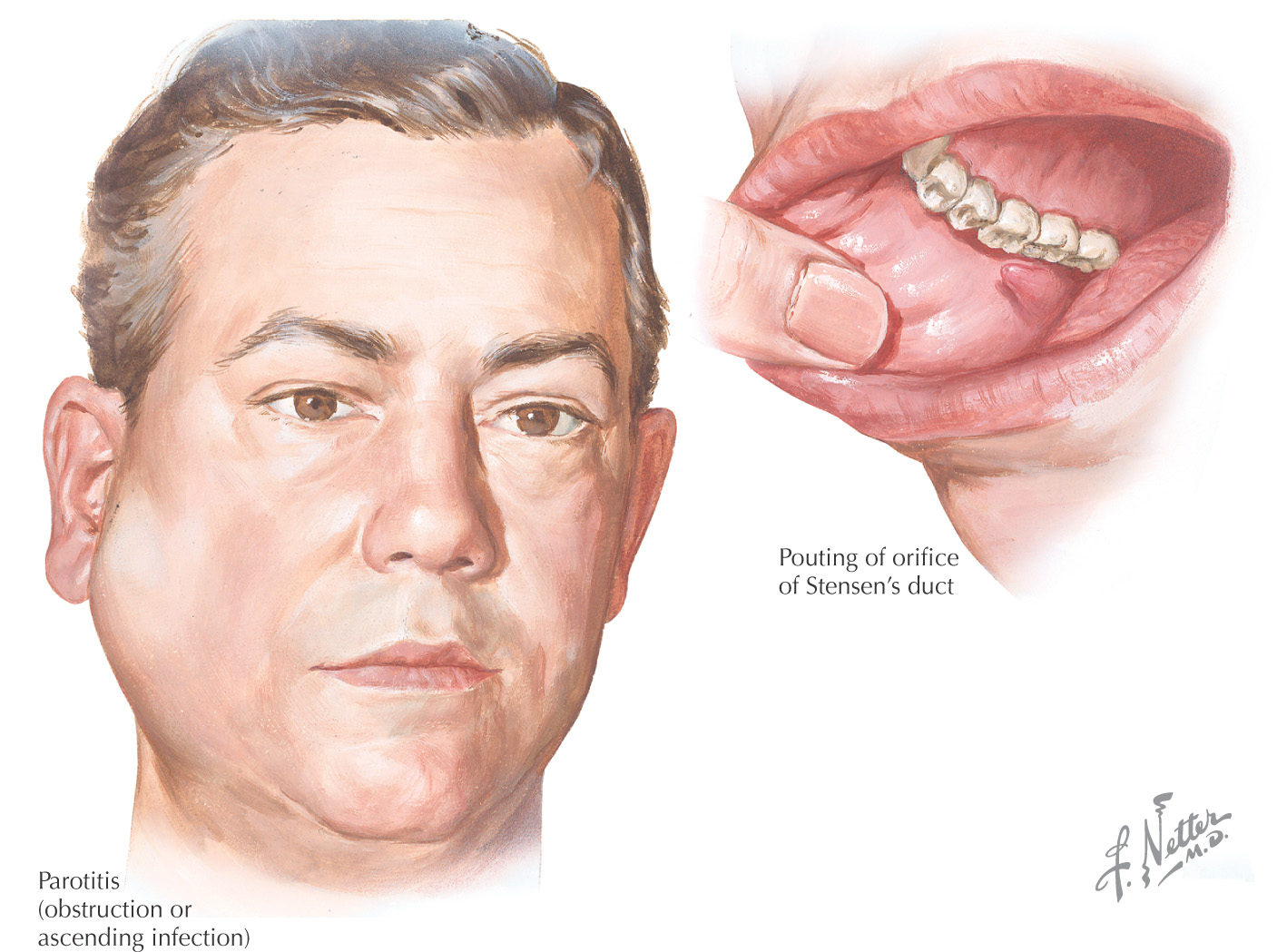
An inflammation of the parotid glands that typically is caused by a bacterial or viral infection
Can also be caused by other diseases, such as Sjögren’s syndrome, tuberculosis, and human immunodeficiency virus (HIV) infection
Pain through mandibular movement is the result of the compression of the deep lobe of the gland by the mandibular ramus
Less common since the introduction of antibiotics, proper hydration, and better oral hygiene
Mortality rate in the early 19th century was as high as 70% to 80%
Most cases now seen in patients on anticholinergic medication, especially the elderly, because it inhibits the salivary flow, which makes it easier for the bacteria to be transported in retrograde fashion along the parotid duct into the gland, where they may settle to cause an infection
Known as mumps
Causative virus is a paramyxovirus that infects different body parts, notably the parotid glands
Usually is spread through saliva, coughing, and sneezing
Parotid glands typically swell and become very painful
With the introduction of mumps vaccination in the 1970s, now rare in most developed nations
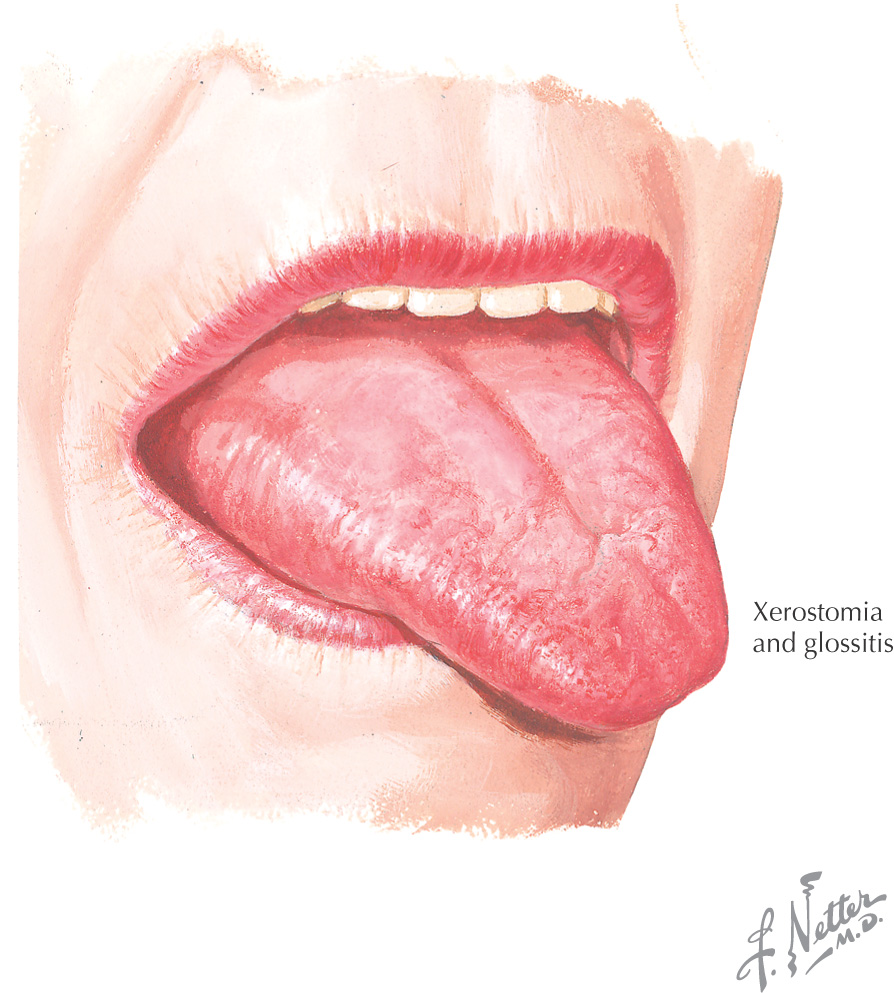
Xerostomia: “dry mouth”
Dry mouth is a symptom that increases the affected person’s susceptibility to dental caries
Can be caused by any medication that reduces salivary outflow, commonly: many antihistamines, antidepressants, chemotherapeutic agents (including radiation therapy), antihypertensives, and analgesics
Occurs in disease processes such as depression, stress, endocrine disorders, Sjögren’s syndrome, and improper nutrition
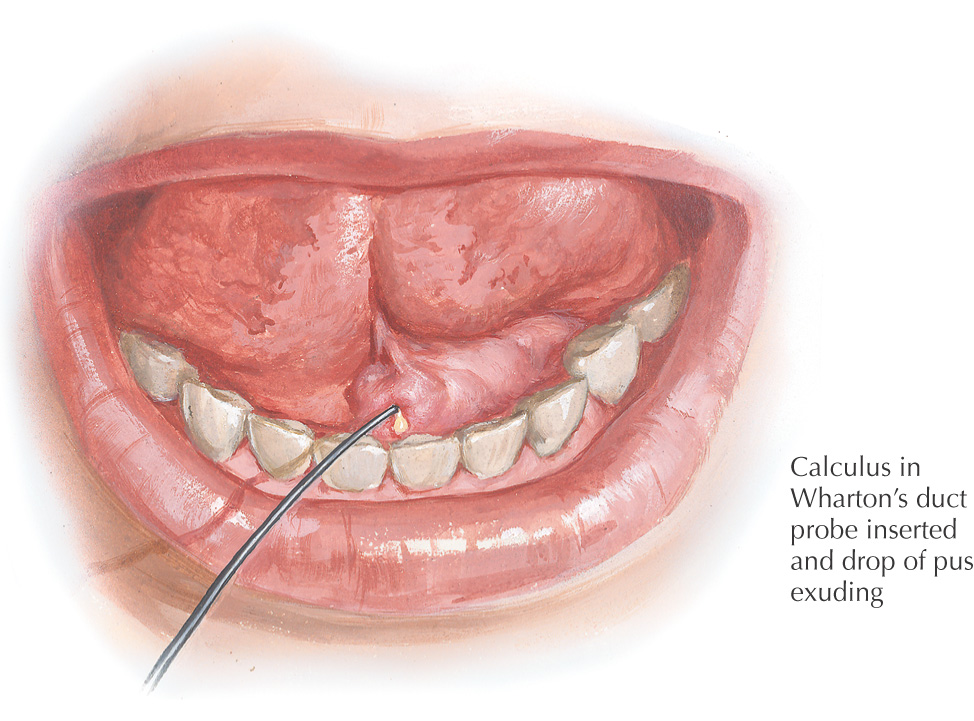
Can lead to the formation of sialoliths, calculi that form in the duct or gland, although they are more commonly associated with infections of the submandibular gland than of the parotid gland and duct
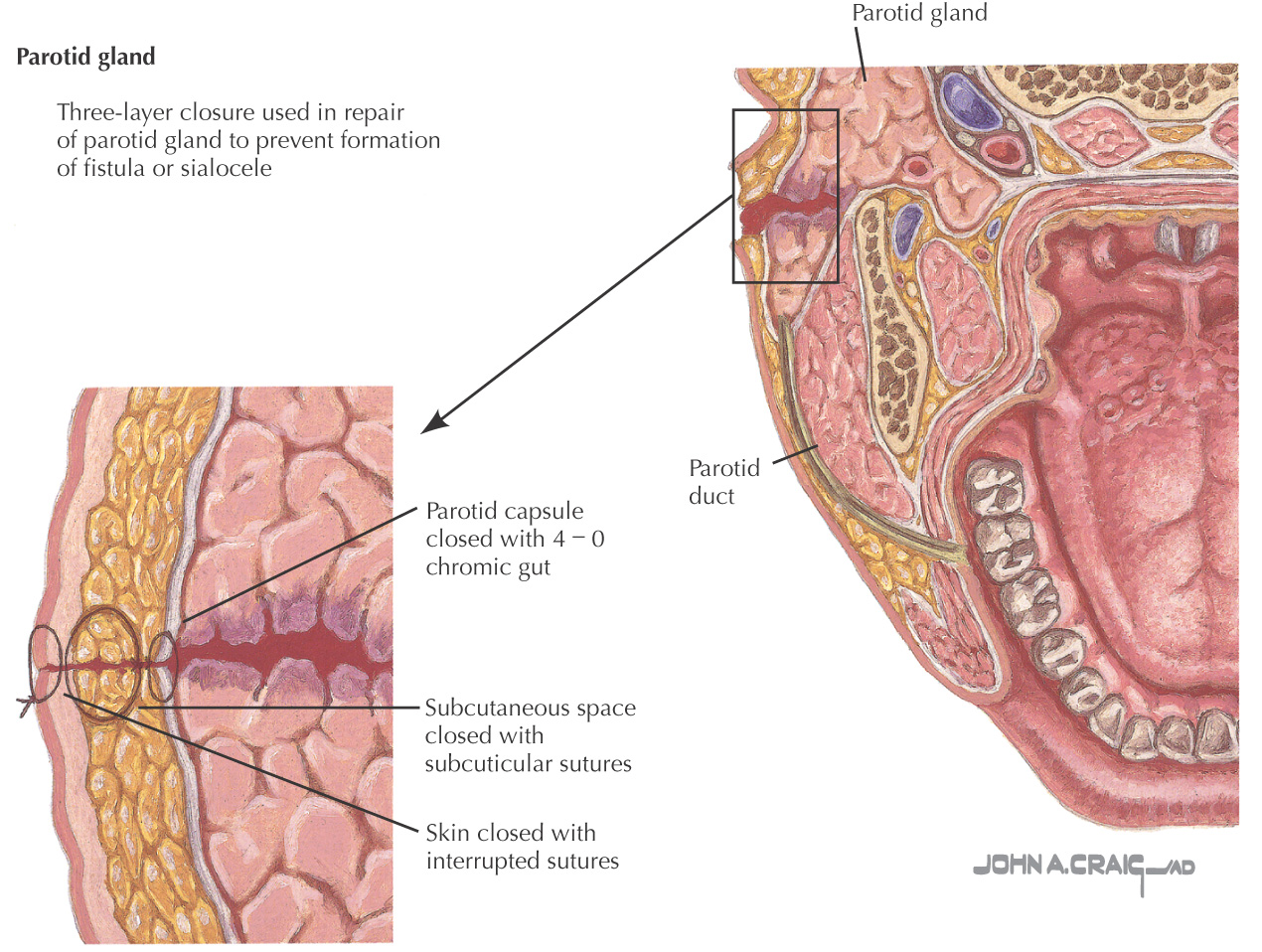
Parotid fistula: a communication between the skin and the parotid gland or duct that may lead to the formation of a sialocele, a cyst filled with a collection of mucoid saliva in the tissues surrounding the gland
Both parotid fistulas and sialoceles often occur as the result of trauma
May also be caused by:
• Section or injury of the duct or one of its branches during operation for cancer of the cheek or face
• Removal of parotid tumors, especially those of the accessory lobe
• Primary or secondary malignant tumors that ulcerate the skin
• Incision and drainage for acute bacterial parotitis
• Ulceration and infection associated with large salivary calculi
• Fistula may develop after a mastoid or fenestration operation
• Infection (actinomycosis, tuberculosis, syphilis, cancrum oris)
Fistulas that lead directly into the oral cavity need no treatment
Fistulas on the skin may or may not need surgical intervention
Anticholinergics are useful agents to diminish the salivation during treatment
Sialoceles often resolve with aspiration or compression and normally do not require drain placement
Injury to the parotid gland or duct should be repaired to prevent formation of fistulas and sialoceles
• Repair of the duct using a stent
• Creating a fistula from the duct into the oral cavity