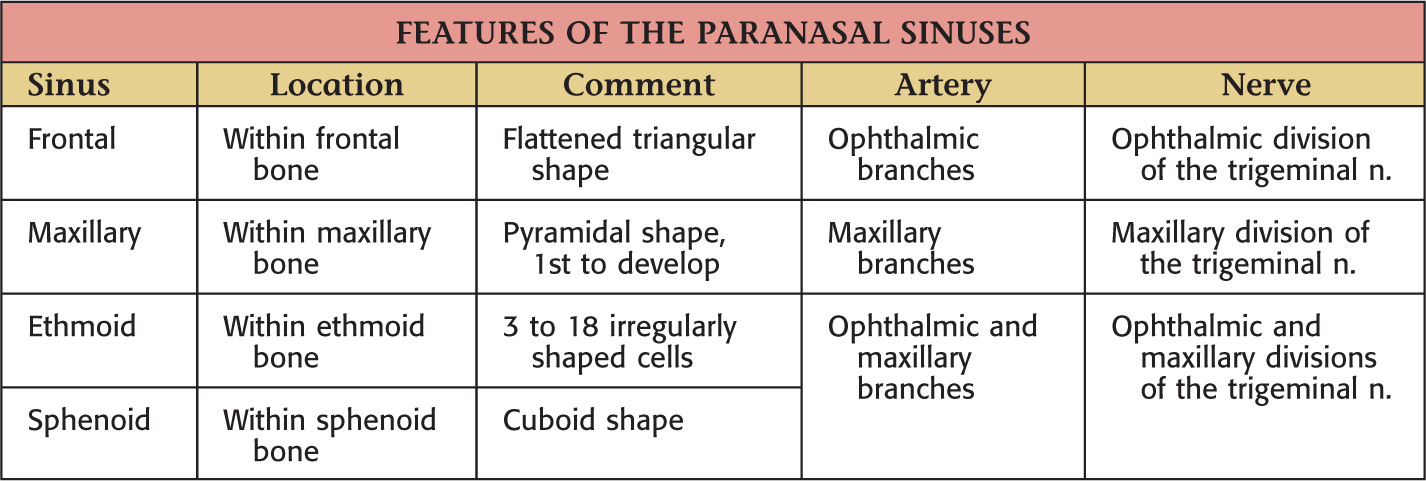
Overview and Topographic Anatomy
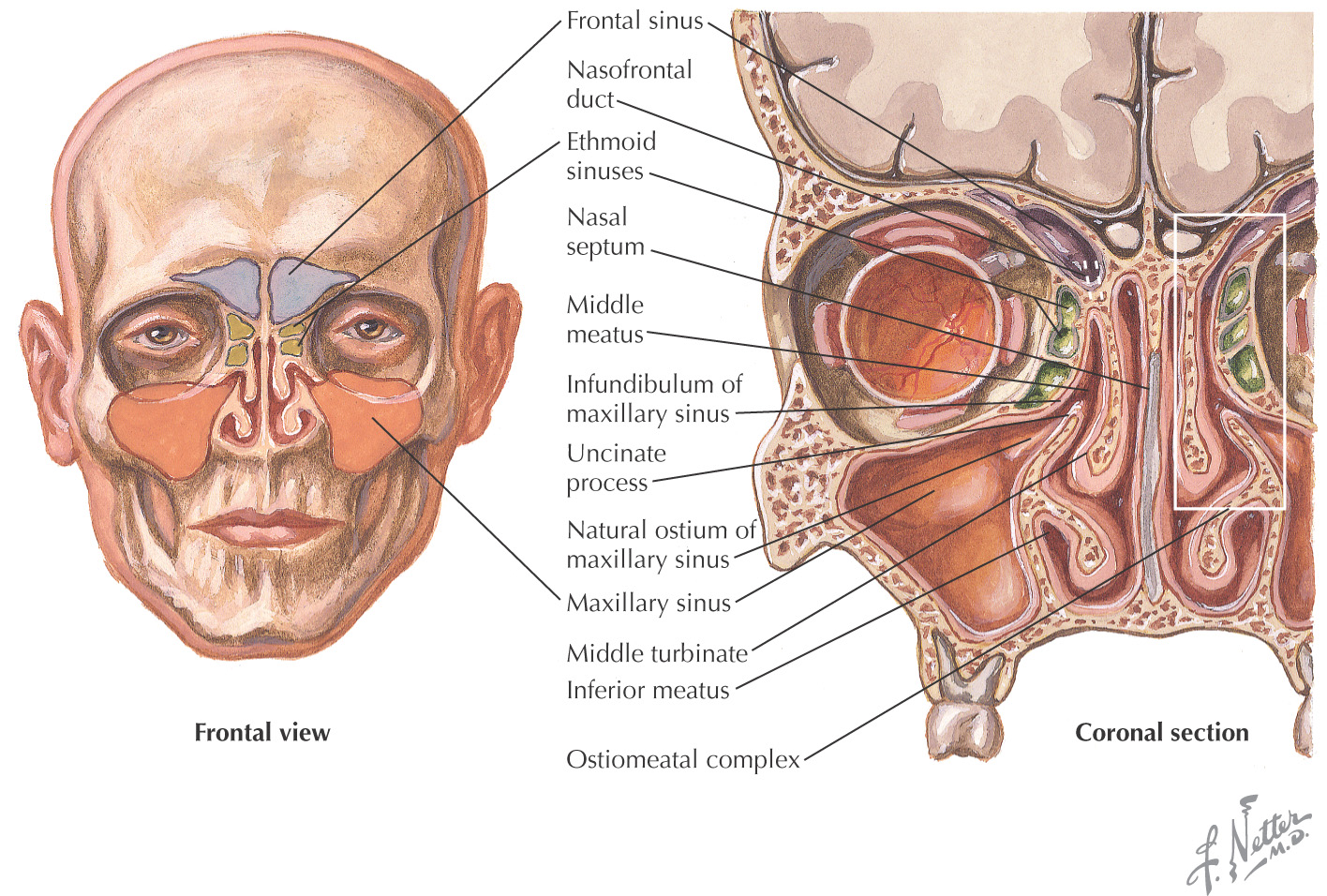
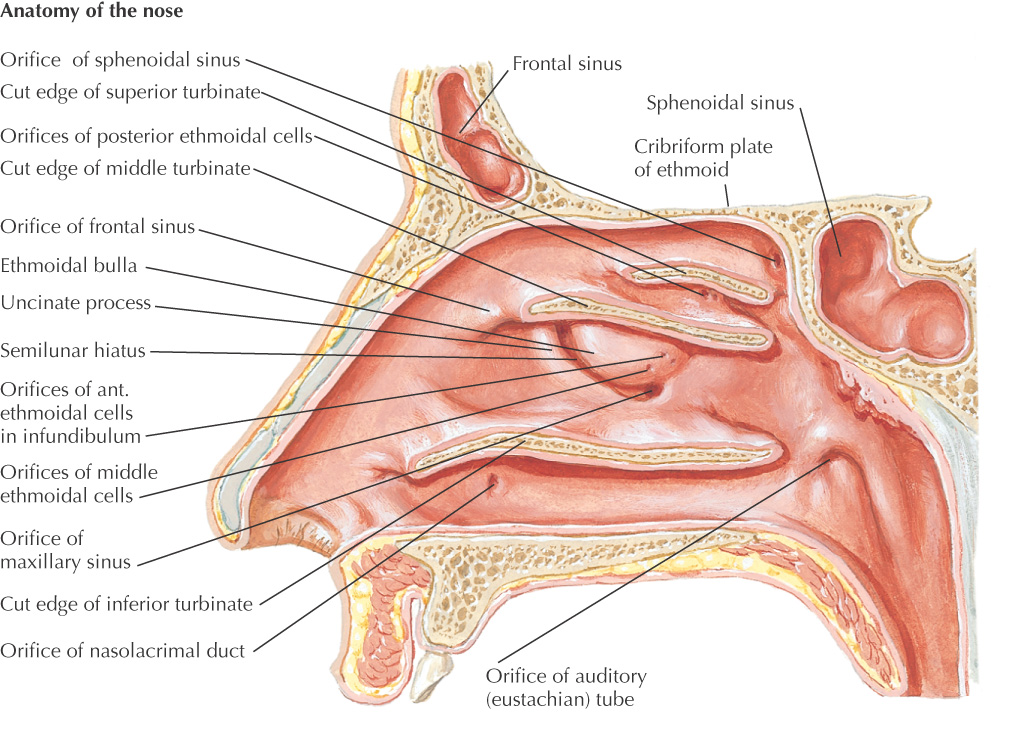
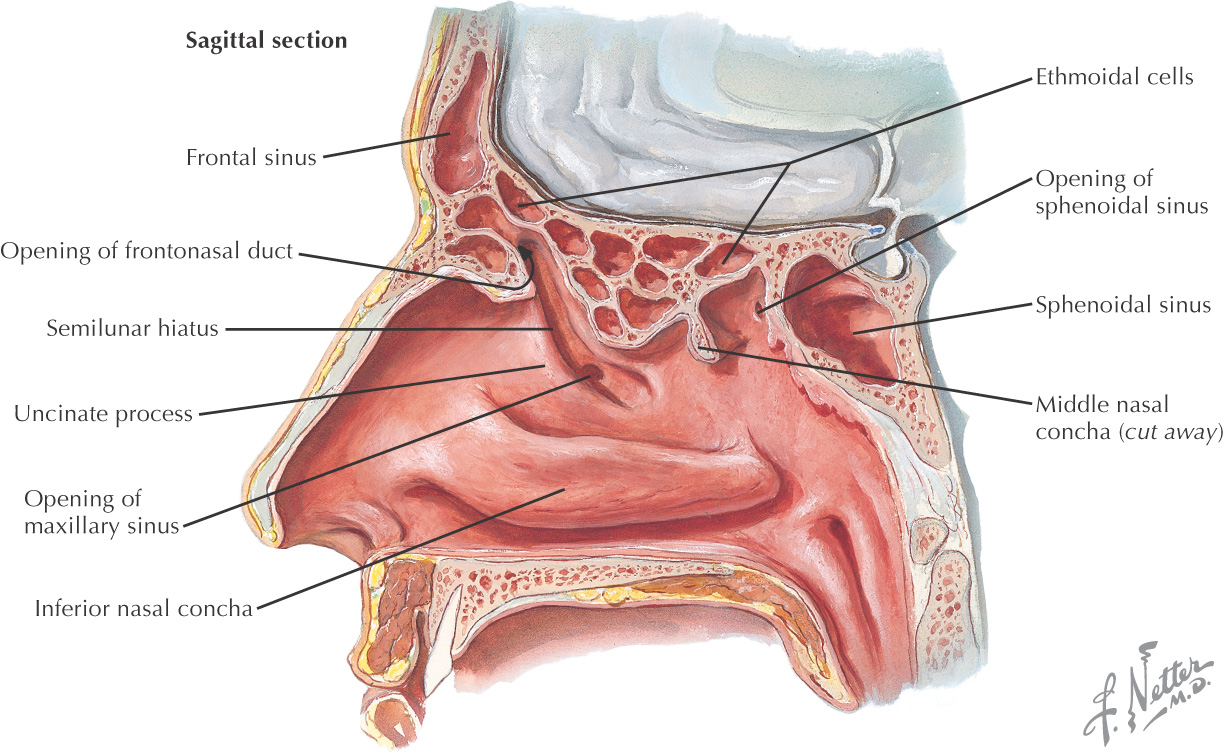
Paranasal sinuses: invaginations from the nasal cavity that drain into spaces associated with the lateral nasal wall
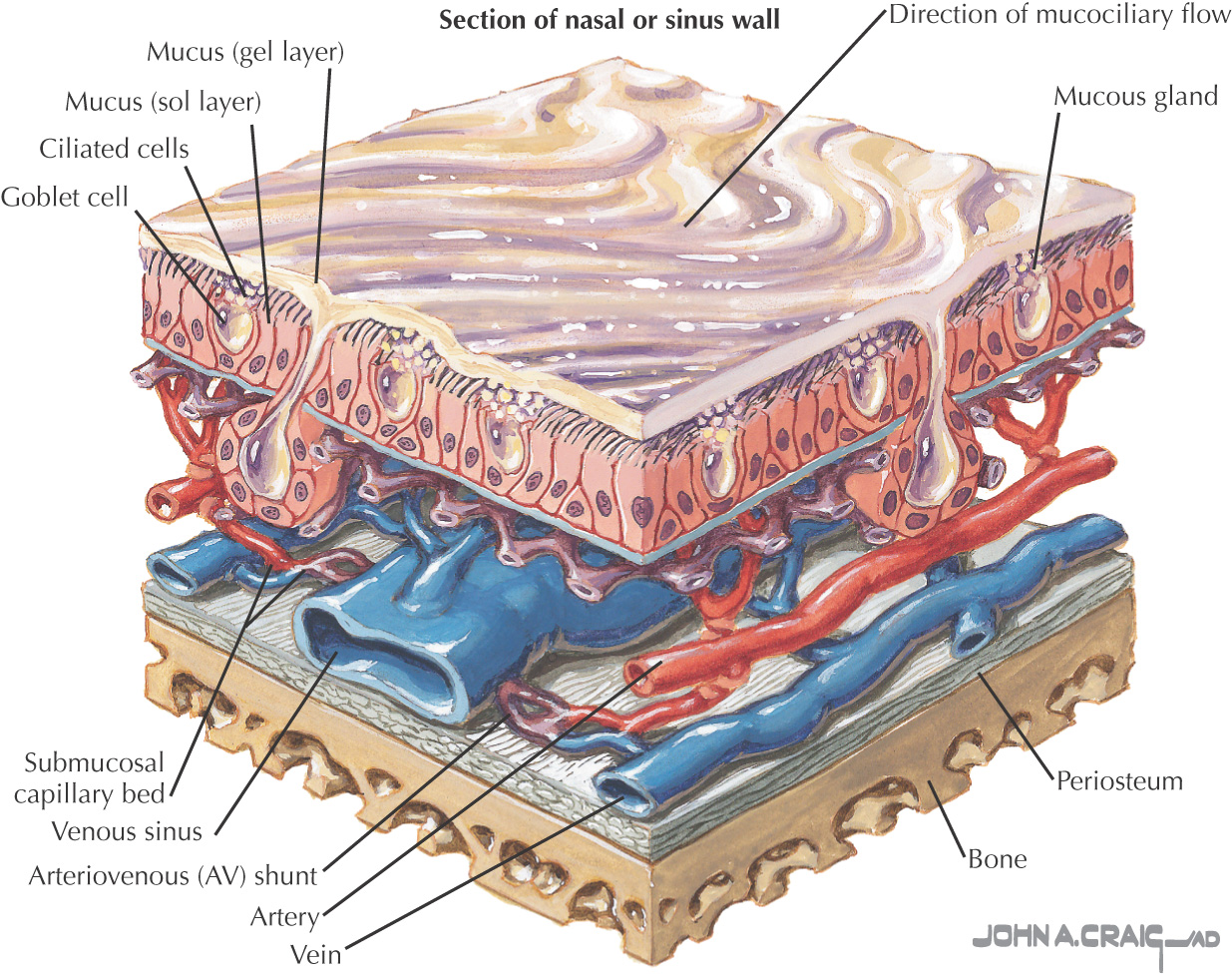
Each is lined by a respiratory epithelium
Morphology of the sinuses is highly variable
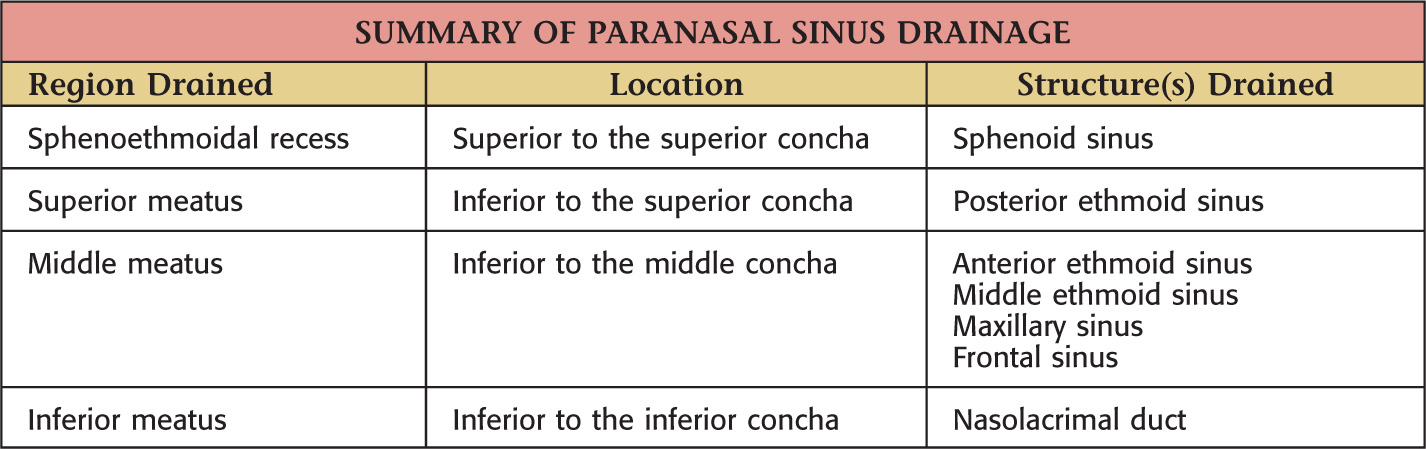
All paranasal sinuses drain into the nasal cavity
Different sinuses serve as drainage conduits for different regions
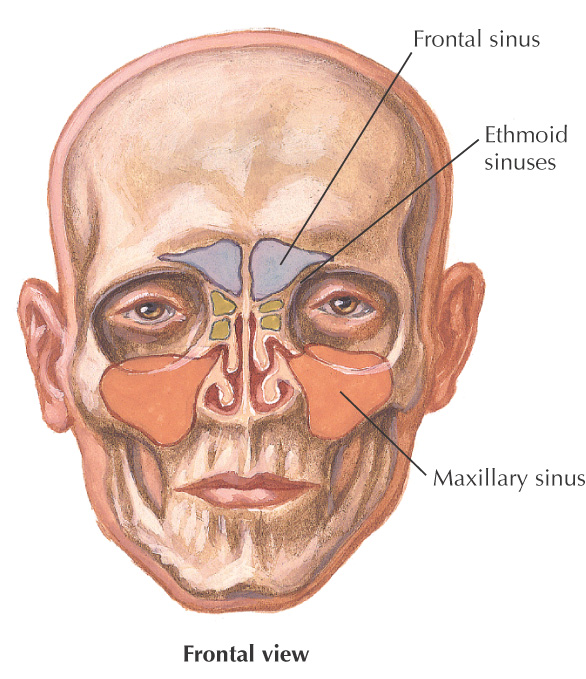
The two frontal sinuses typically are asymmetrical
Rudimentary at birth and usually well-developed by the age of 7 or 8 years
Display a prime expansion when the 1st deciduous molars erupt and another when the permanent molars begin to appear at about age 6
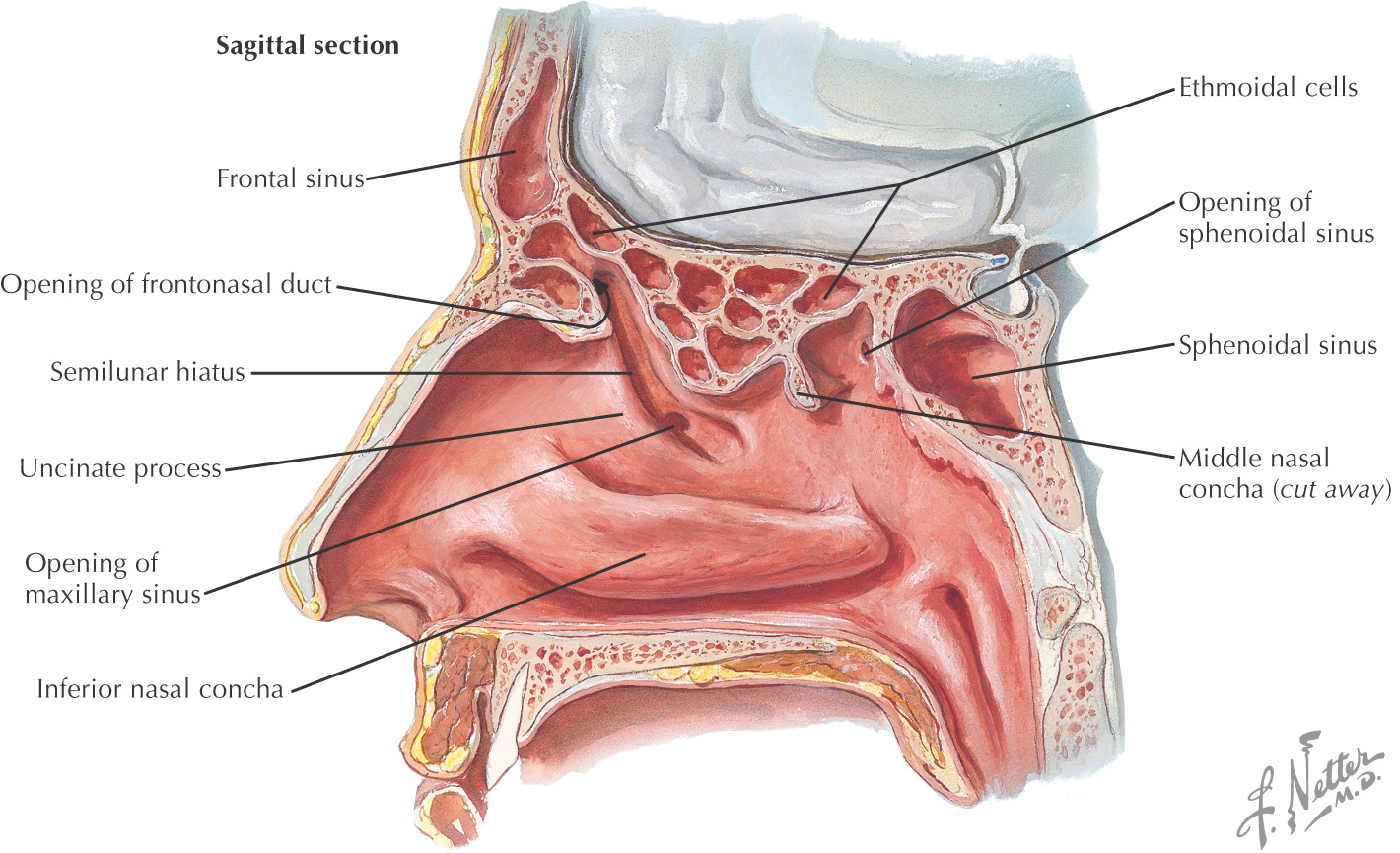
Drainage varies; often drain in front of, above, or into the ethmoidal infundibulum
Primary lymphatic drainage is to the submandibular lymph nodes
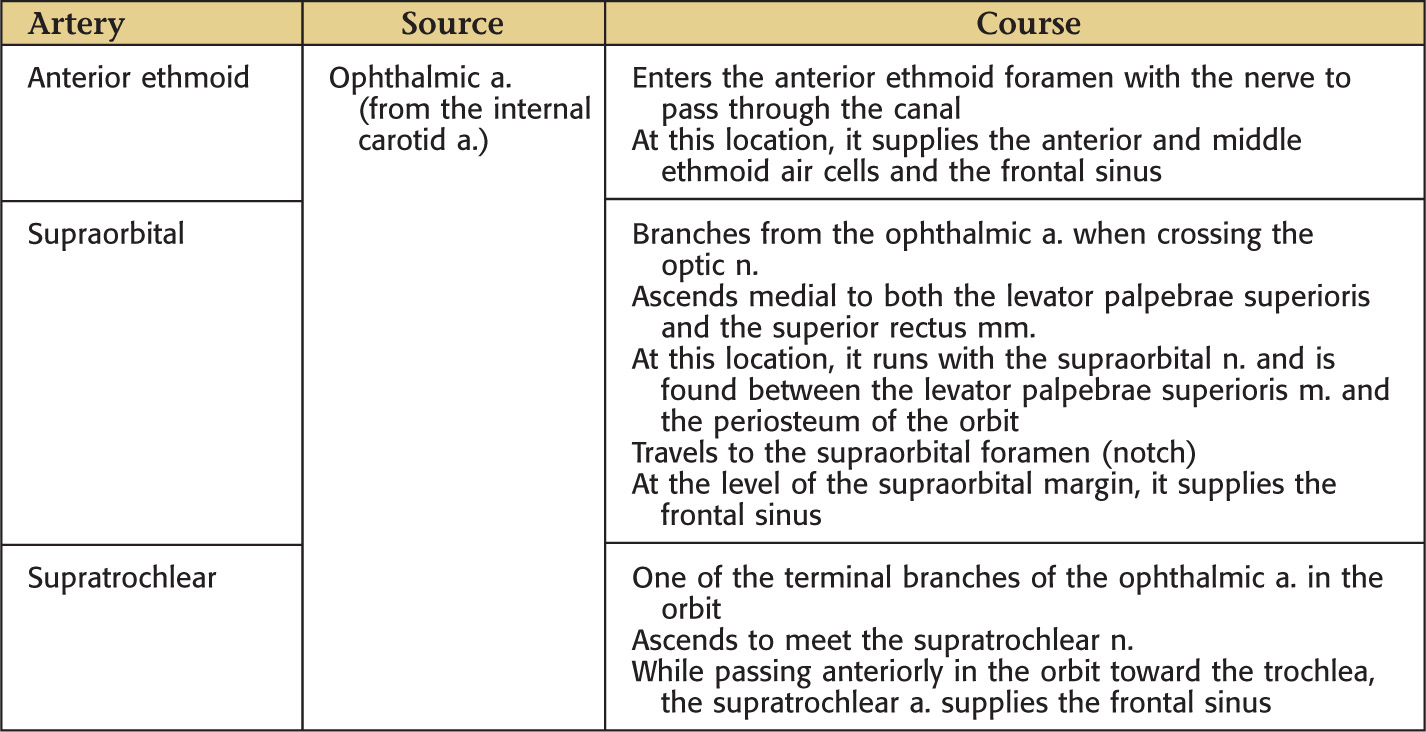
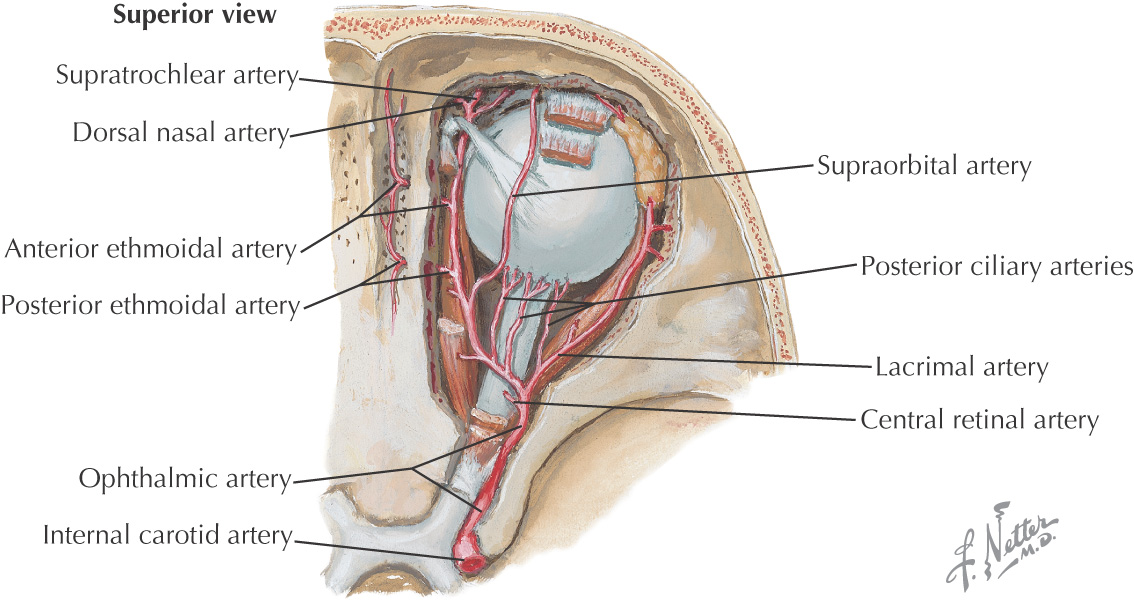
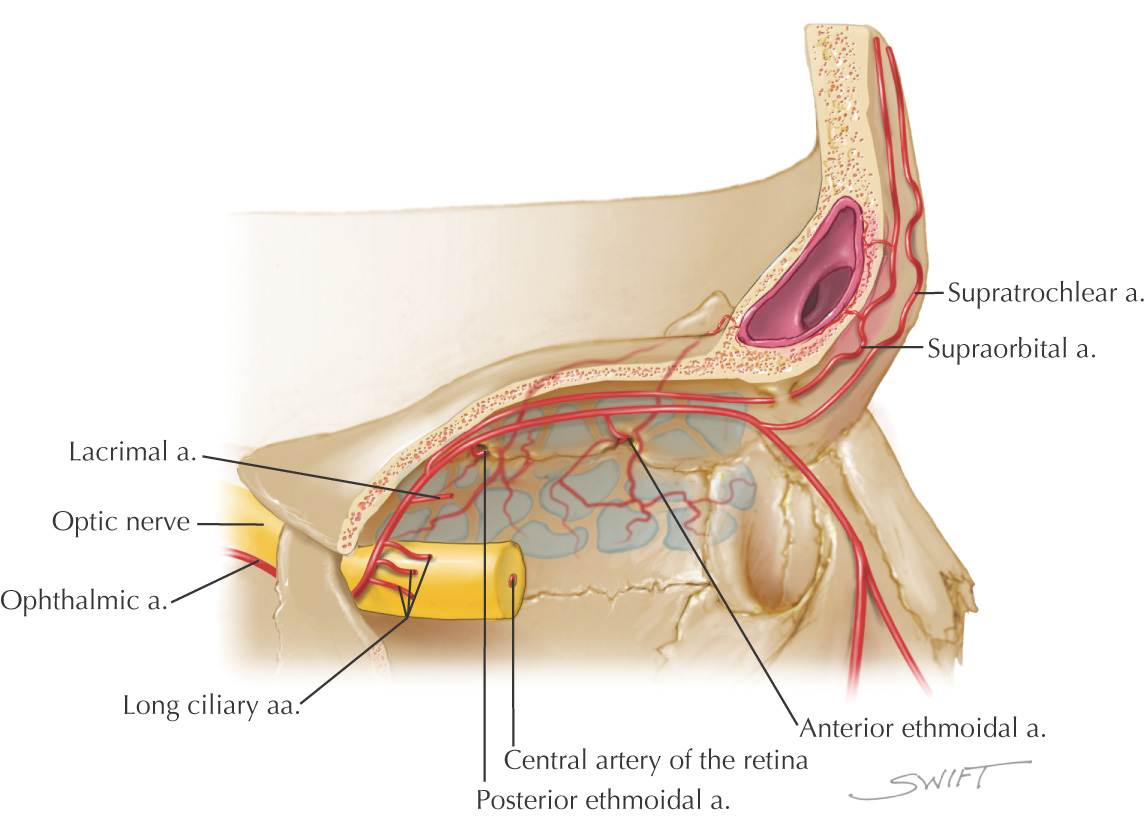
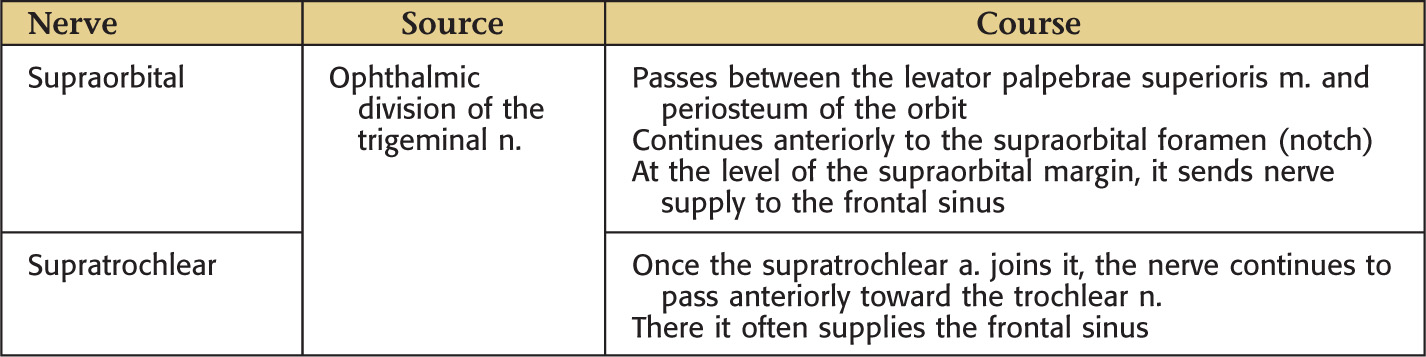
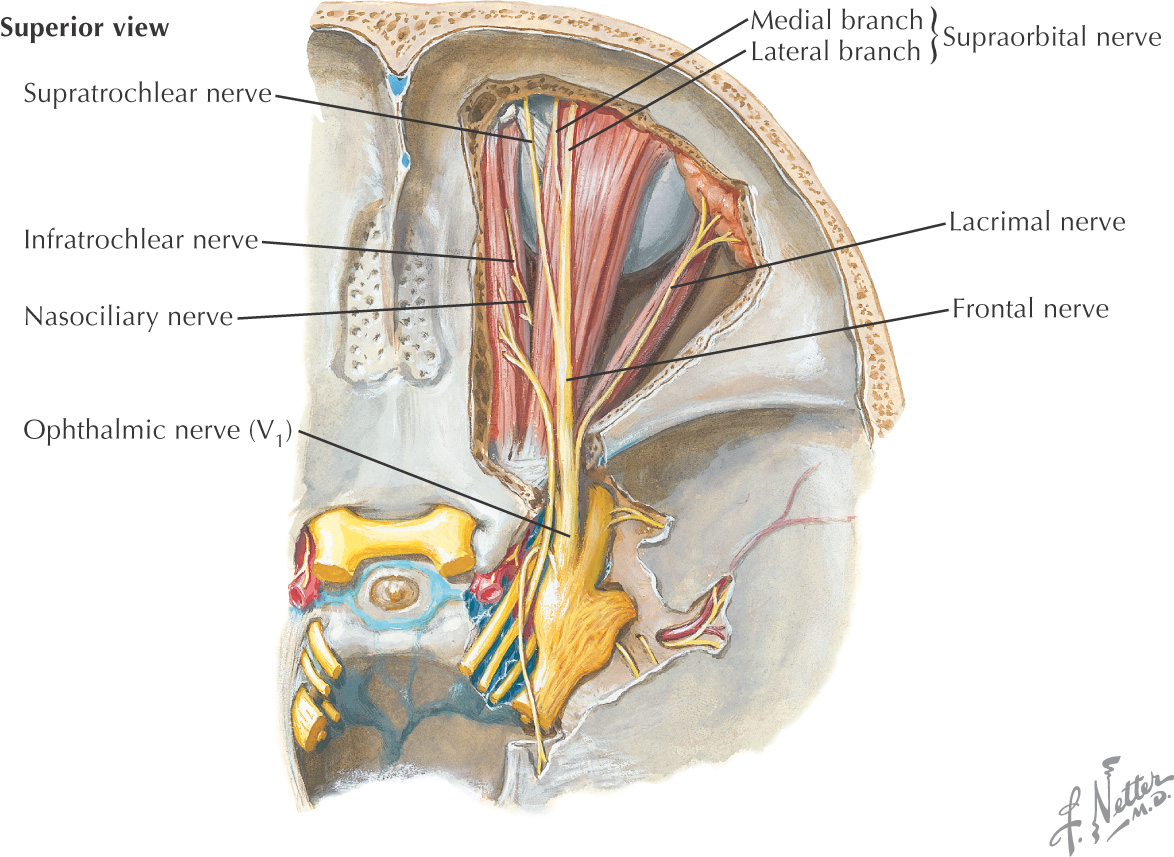
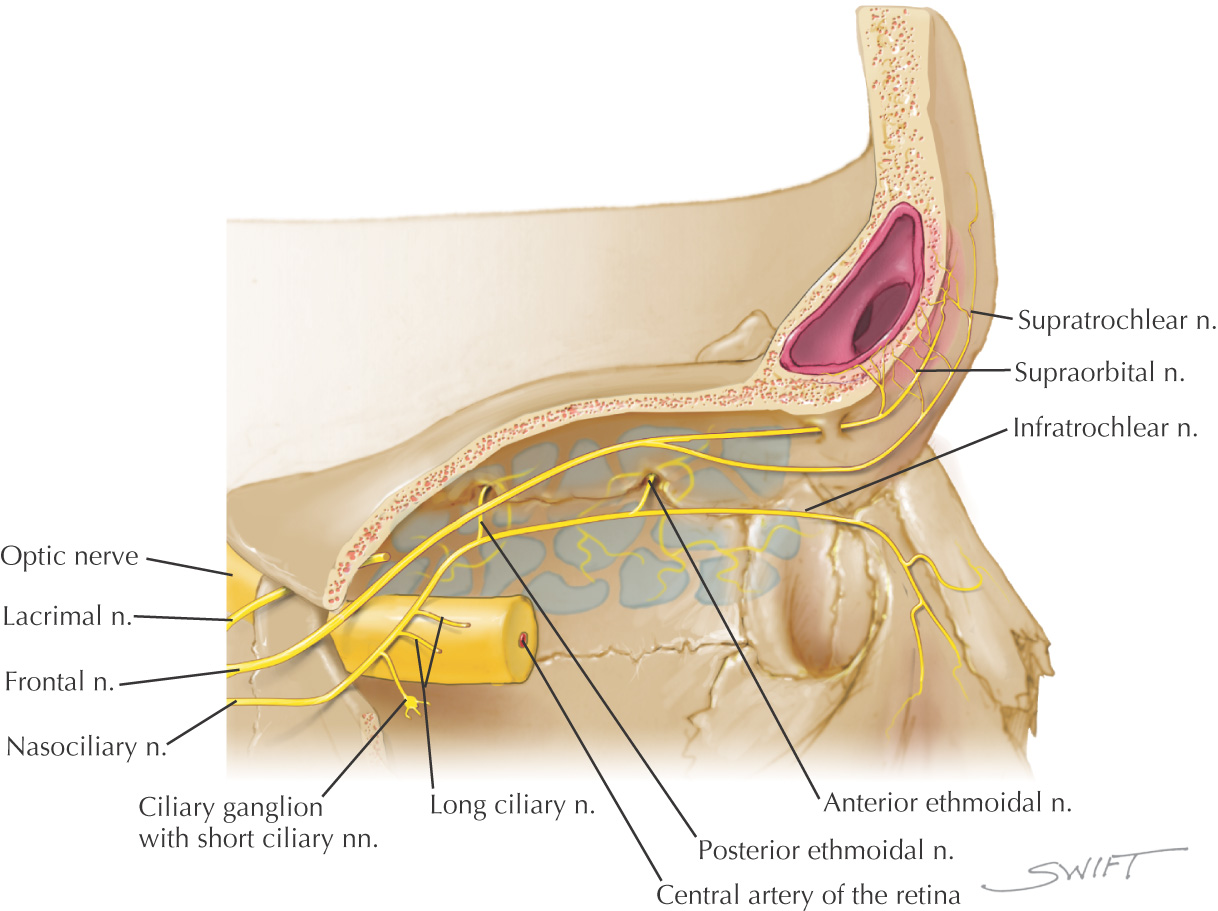
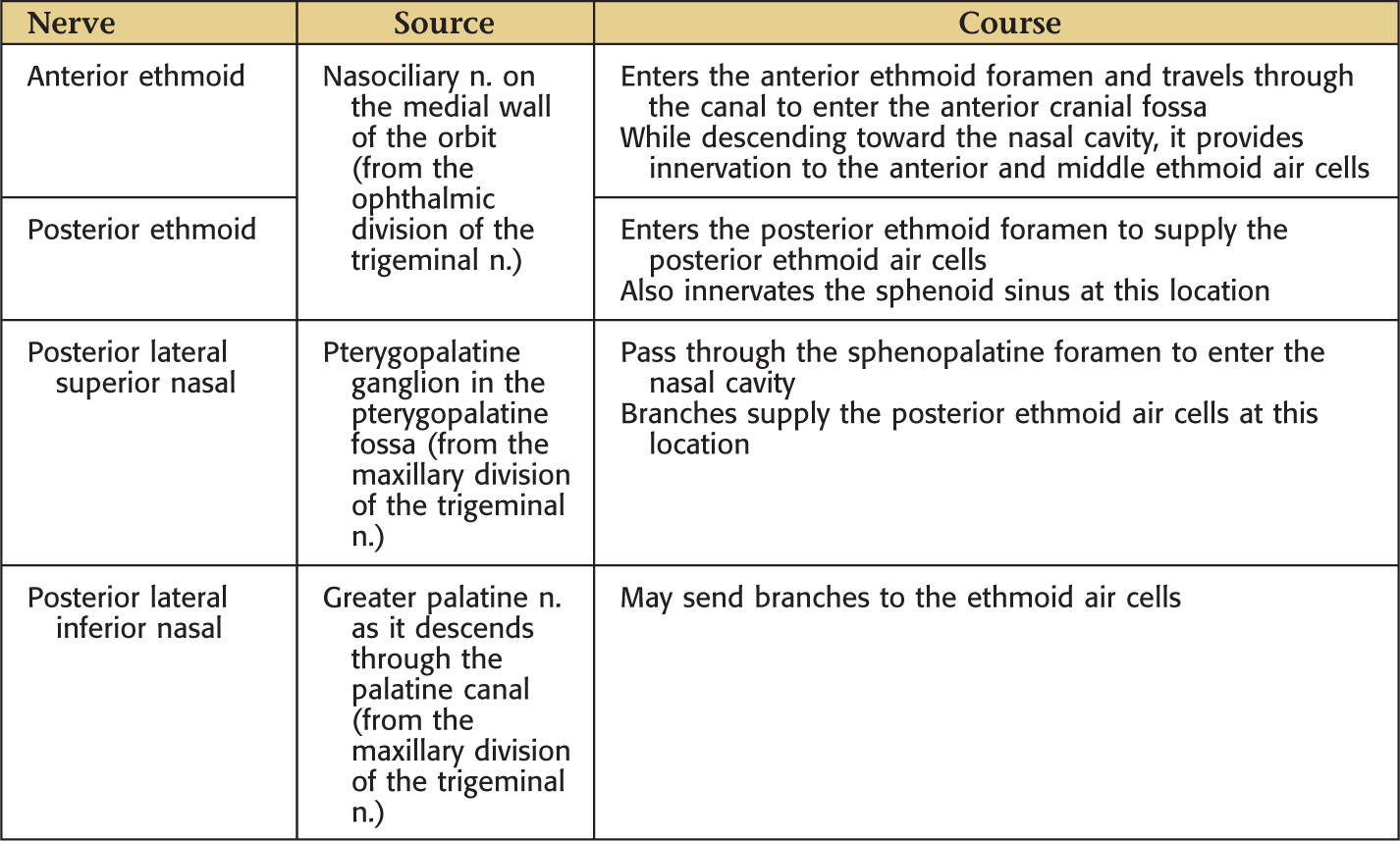
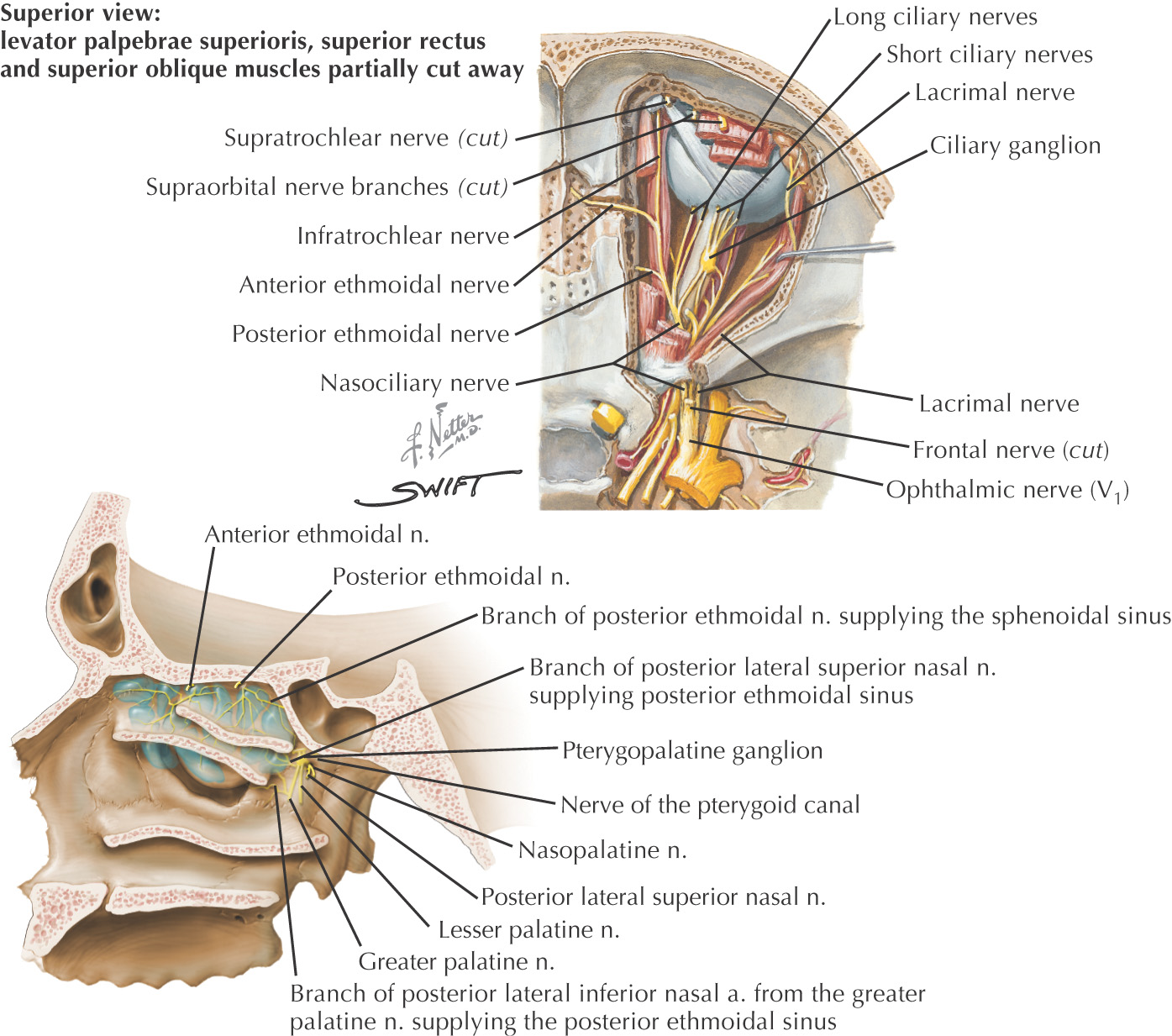
The frontal sinus receives its nerve supply from branches of the ophthalmic division of the trigeminal nerve
• Superior: anterior cranial fossa and contents
• Inferior: orbit, anterior ethmoidal sinuses, nasal cavity
• Anterior: forehead, superciliary arches
• Posterior: anterior cranial fossa and contents
Middle meatus
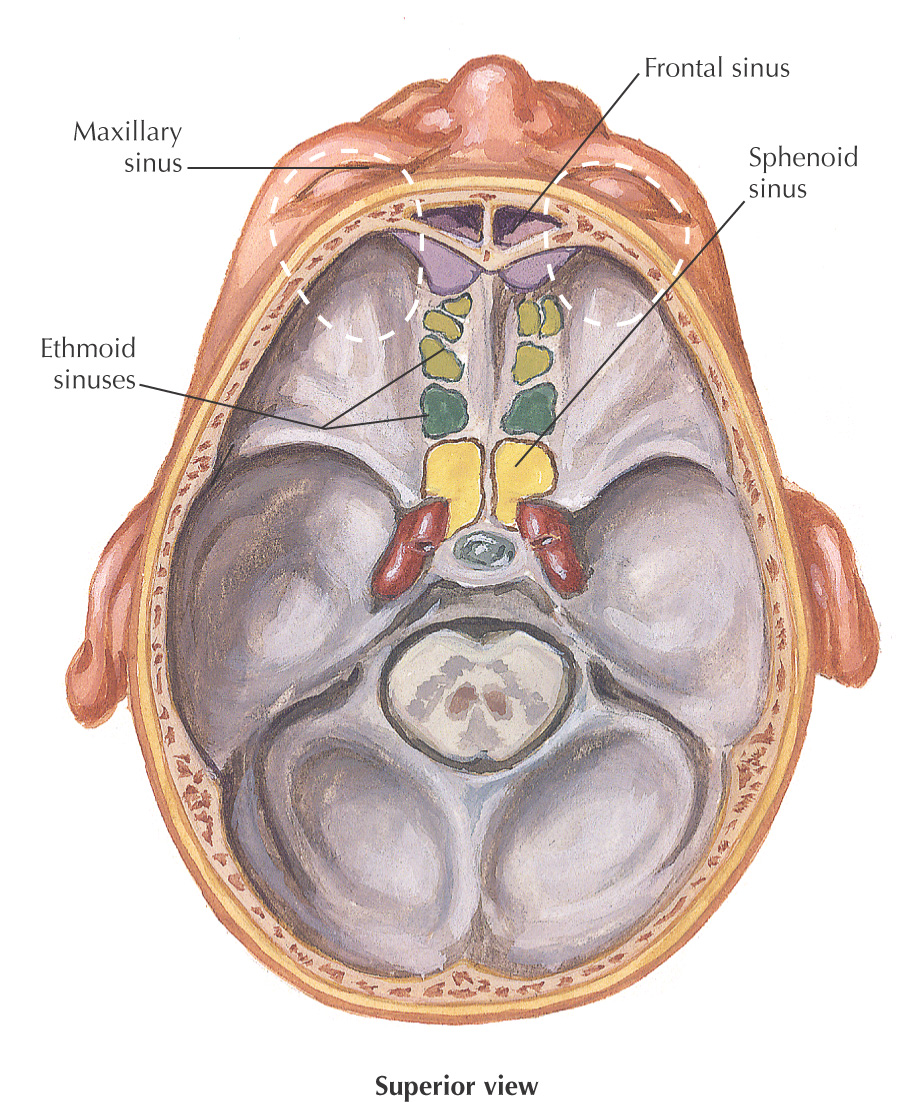
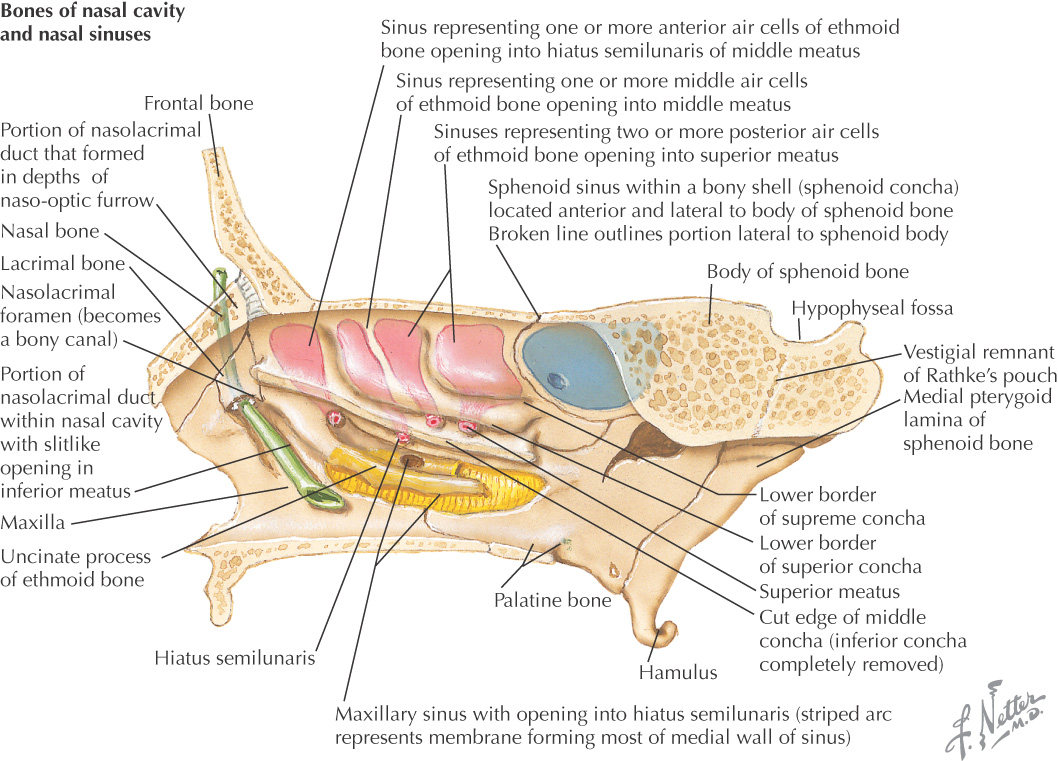
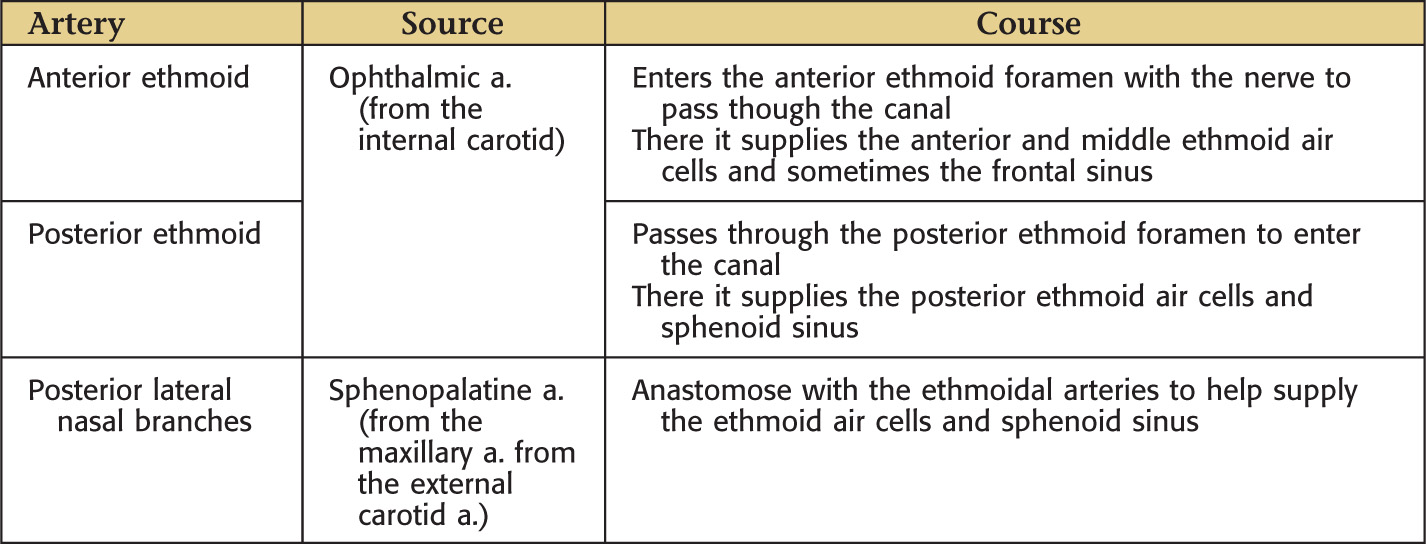
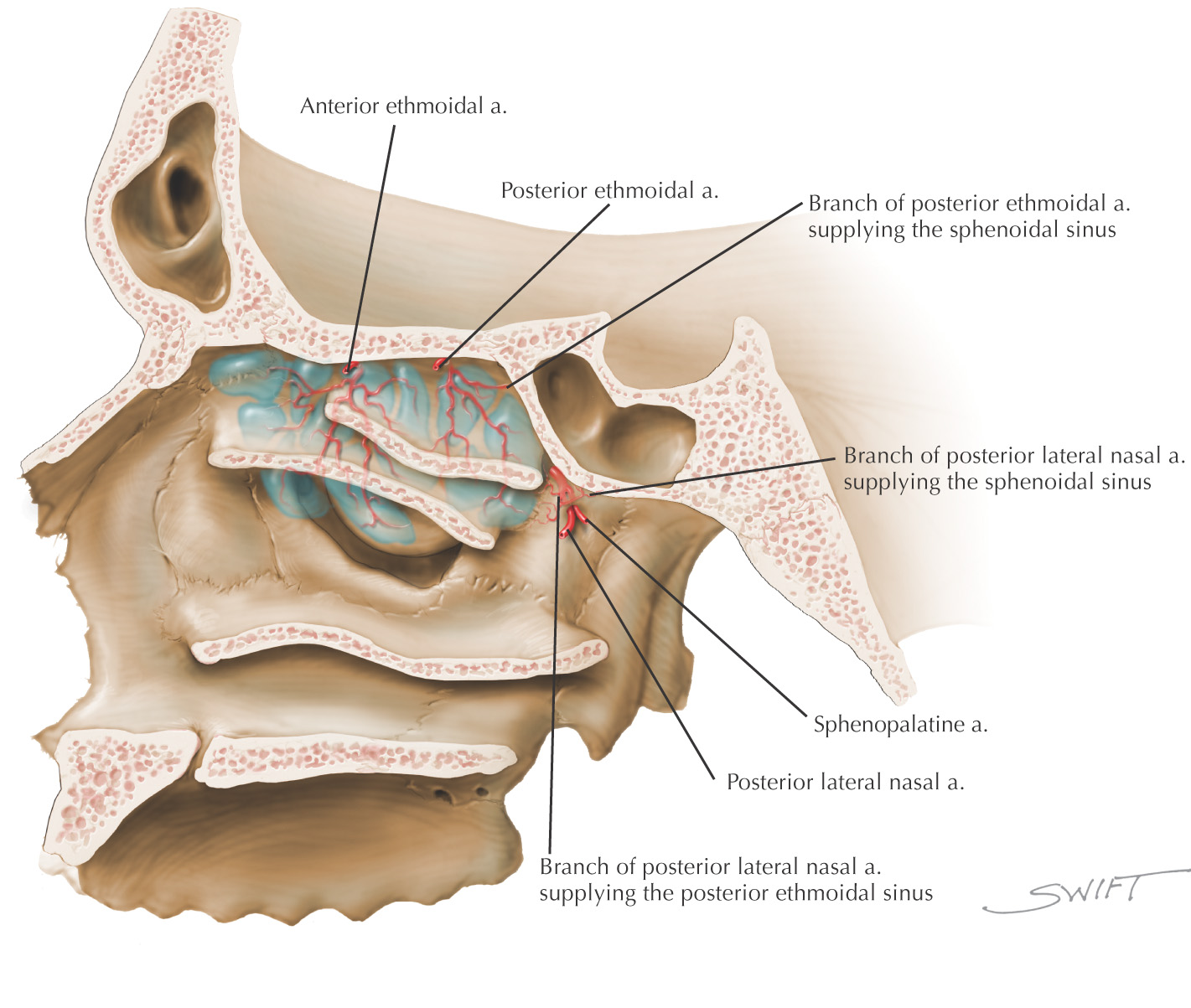
May find 3 to 18 ethmoid air cells on each side
Ethmoid air cells may invade any of the other 3 sinuses
The middle ethmoid air cells produce the swelling on the lateral wall of the middle meatus called the ethmoid bulla
Primary lymphatic drainage is to the submandibular lymph nodes for the anterior and middle ethmoid sinuses; and the retropharyngeal lymph nodes for the posterior ethmoid sinus
• Superior: anterior cranial fossa and contents, frontal bone with sinus
• Anterior: middle meatus (frontonasal duct or ethmoidal infundibulum)
• Middle: middle meatus (on or above ethmoid bulla)

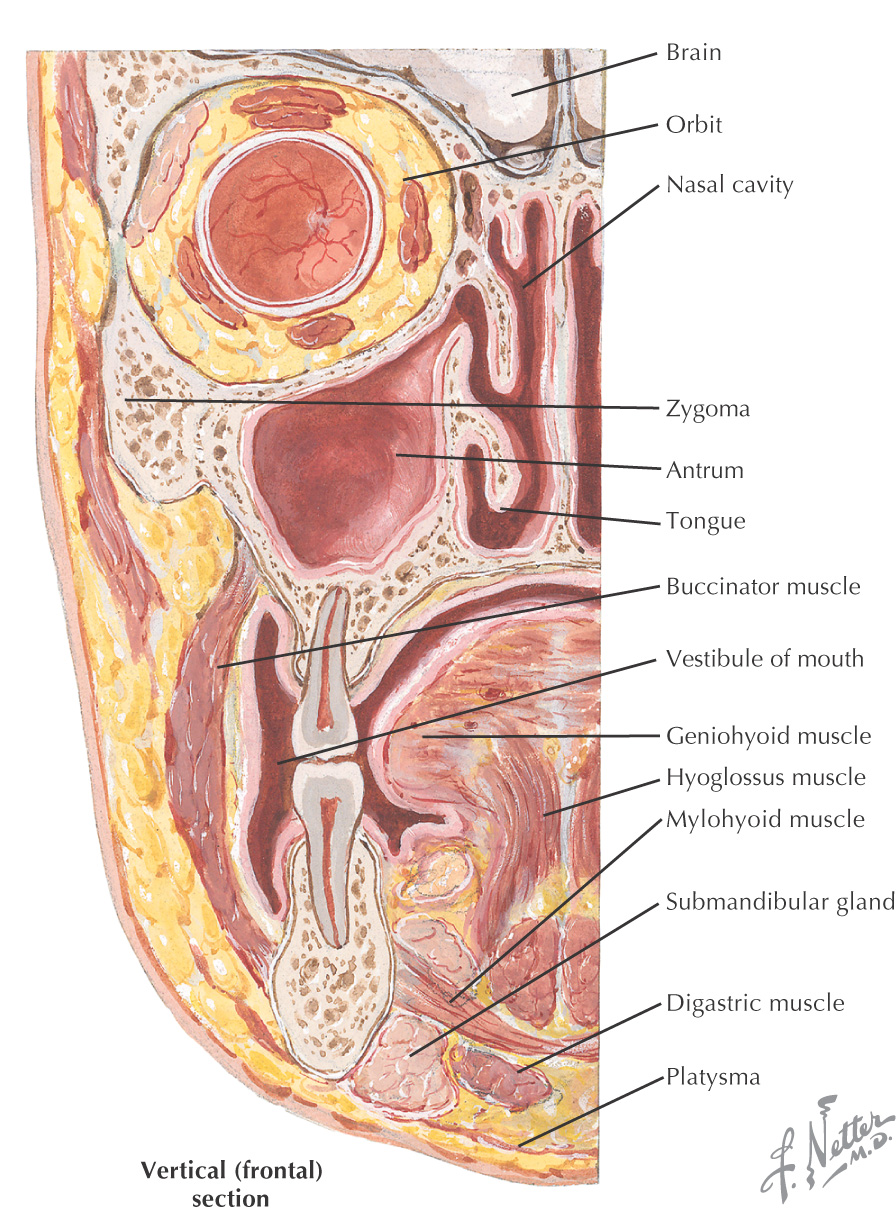
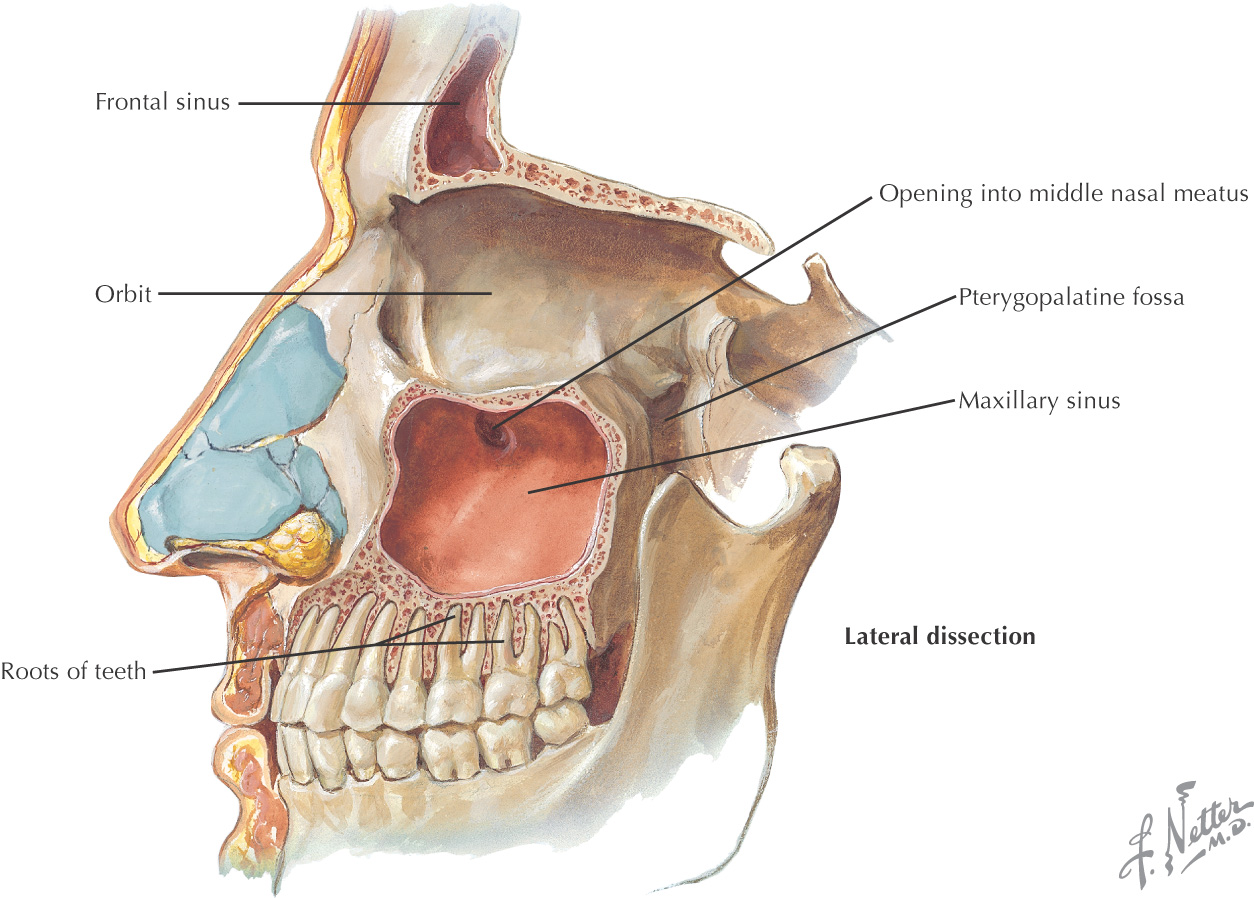
Large pyramidal cavity
Thin walls
Primary lymphatic drainage is to the submandibular lymph nodes
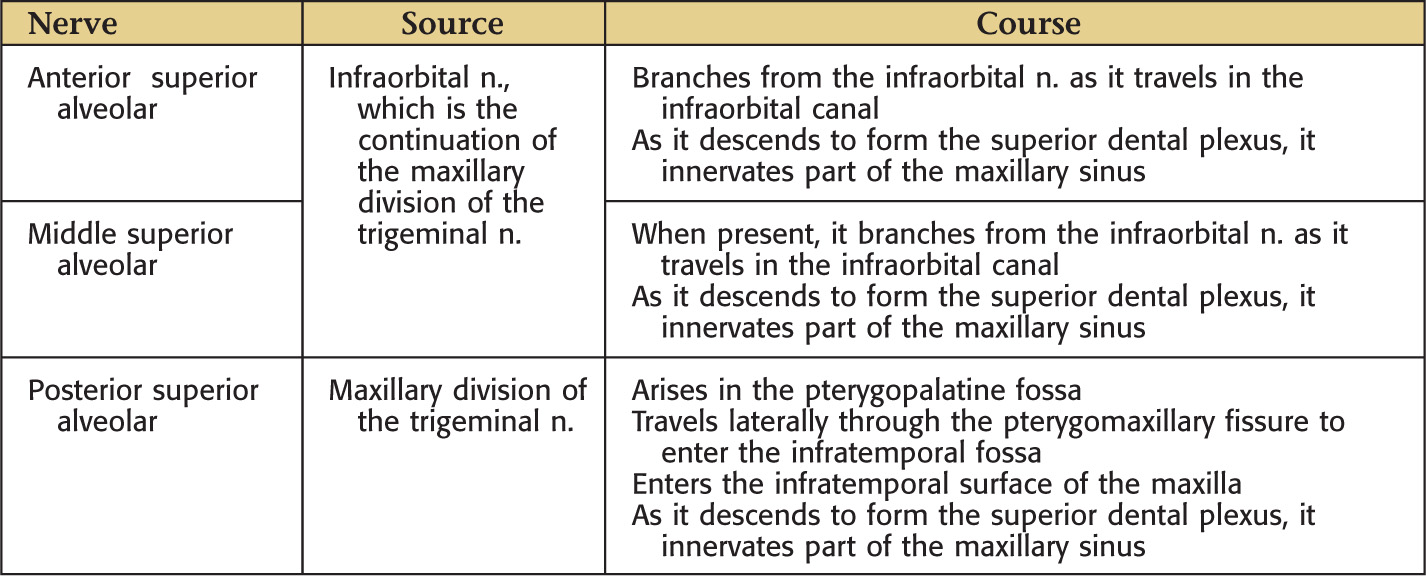
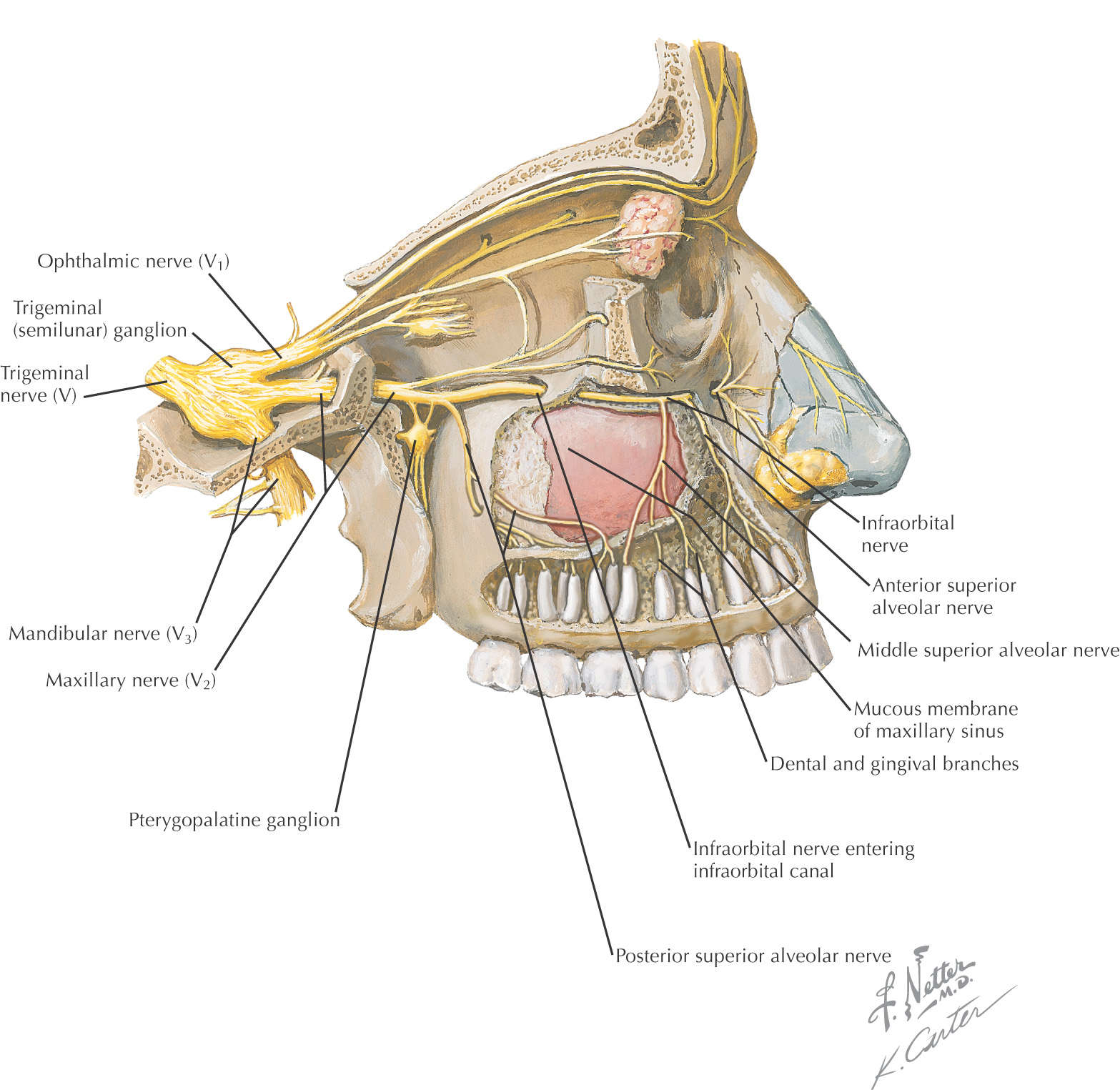
• Superior: orbit, infraorbital nerve and vessels
• Inferior: roots of molars and premolars
• Posterior: infratemporal fossa, pterygopalatine fossa and contents
Middle meatus
Two large, irregularly shaped cavities
Separated by an irregular septum
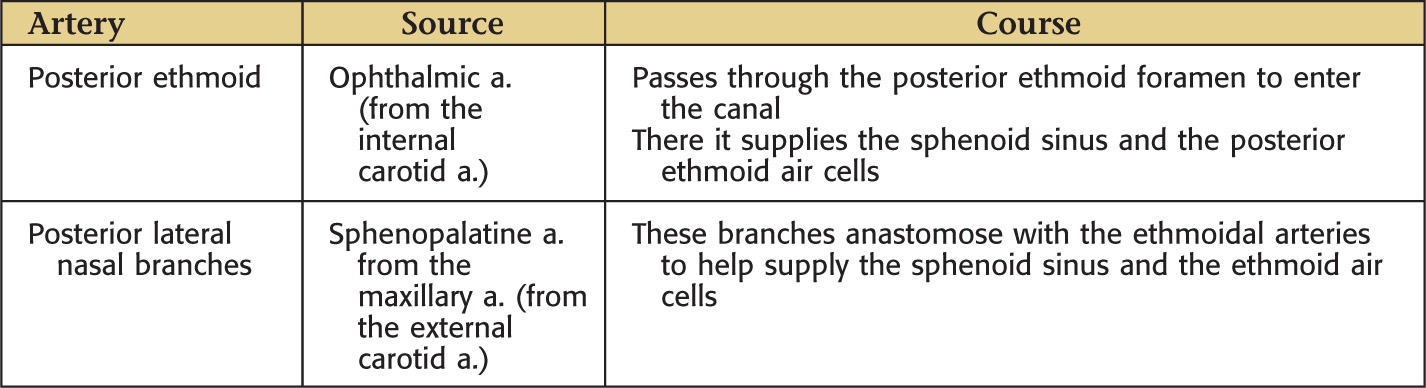
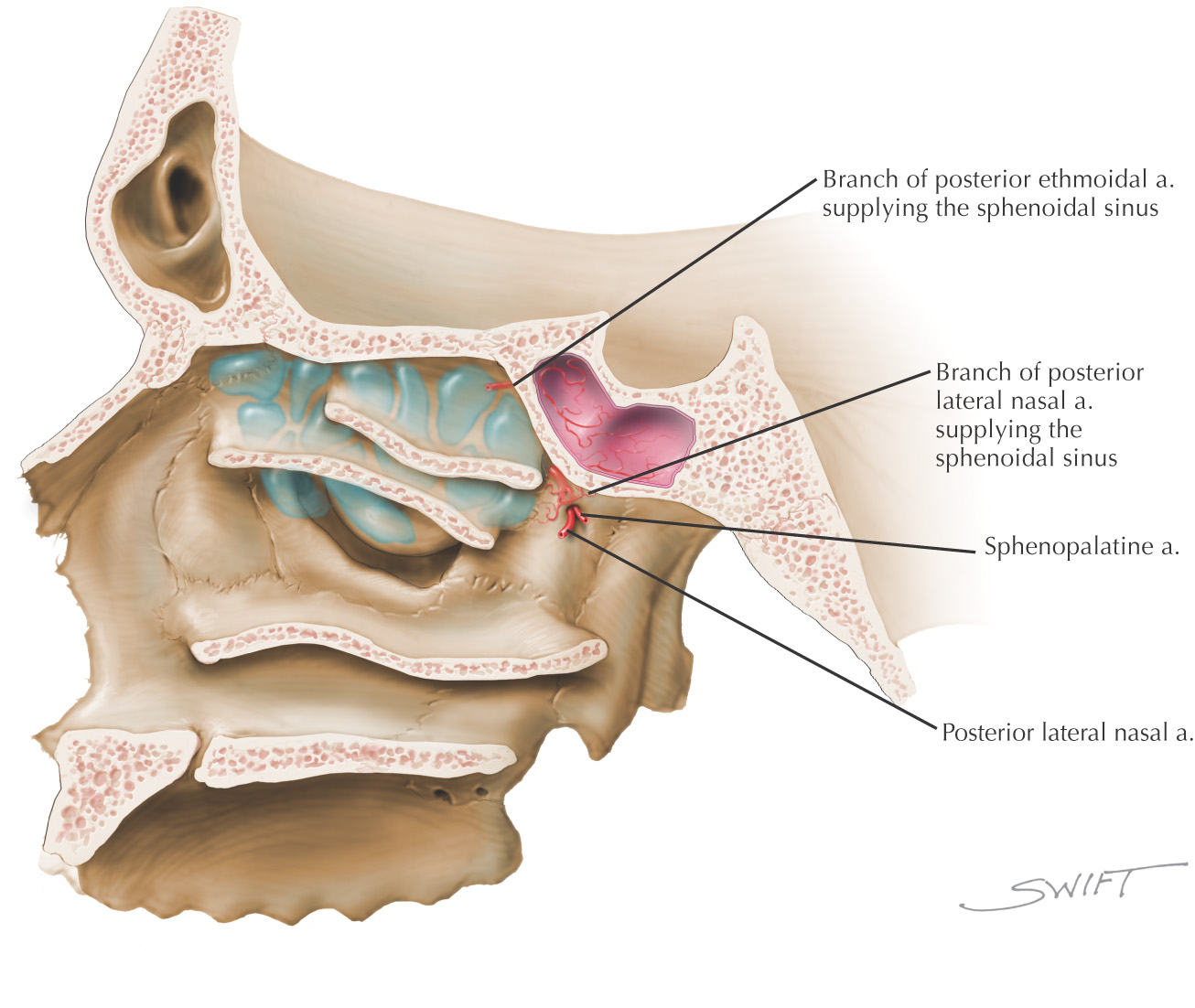
Primary lymphatic drainage is to the retropharyngeal lymph nodes
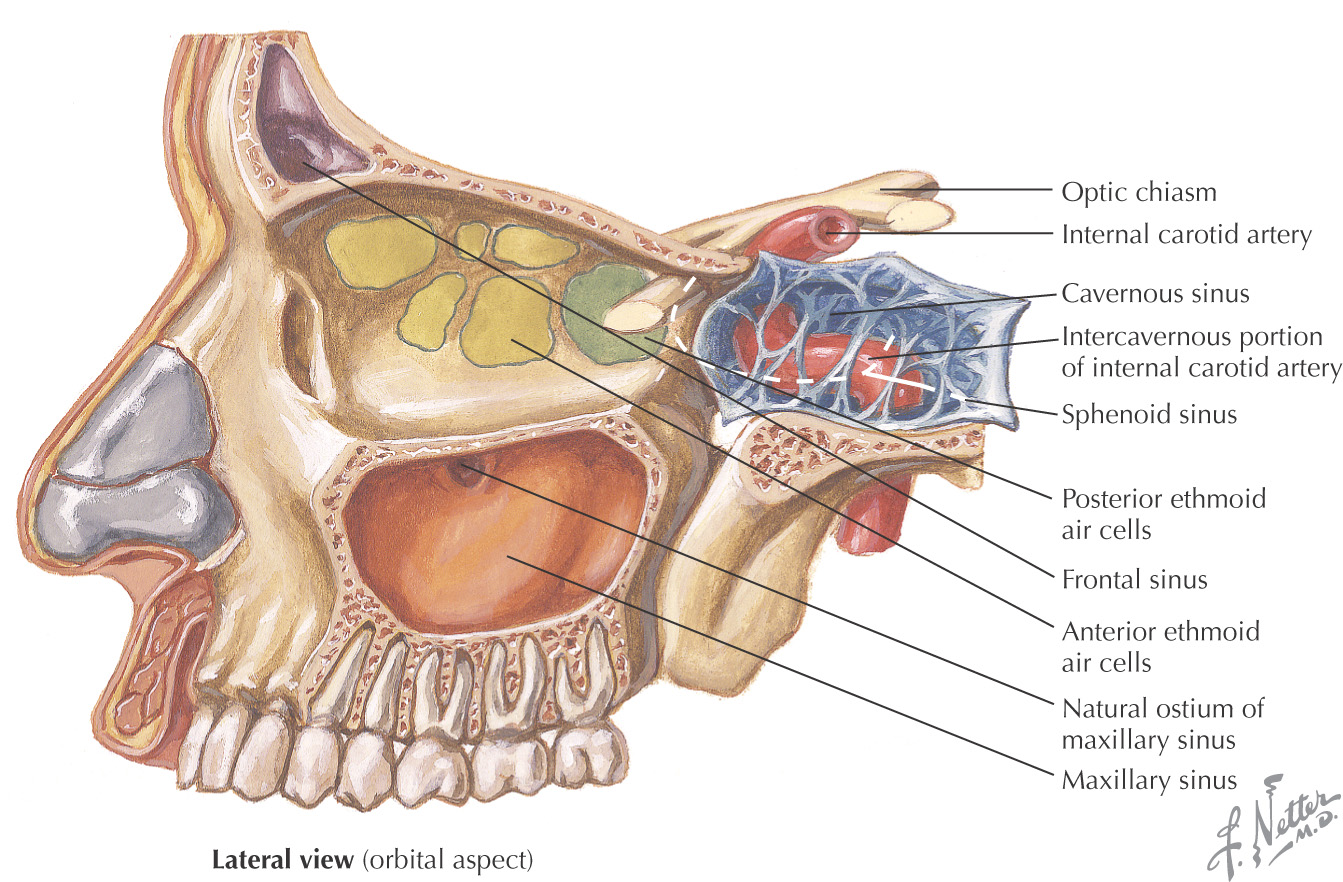
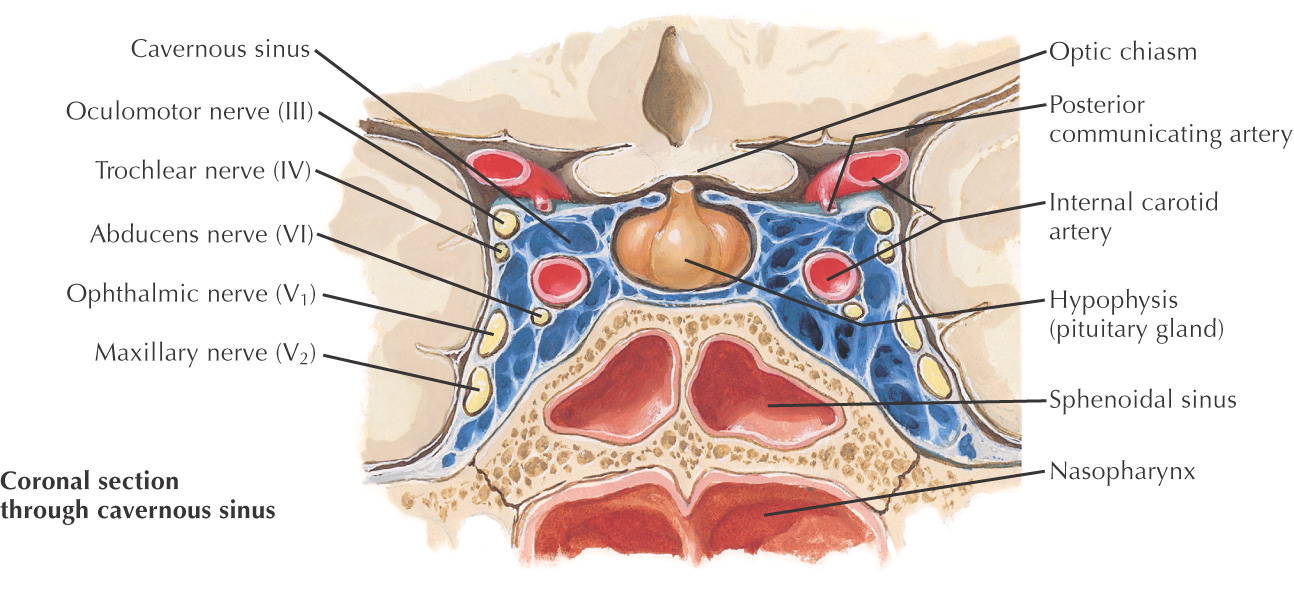
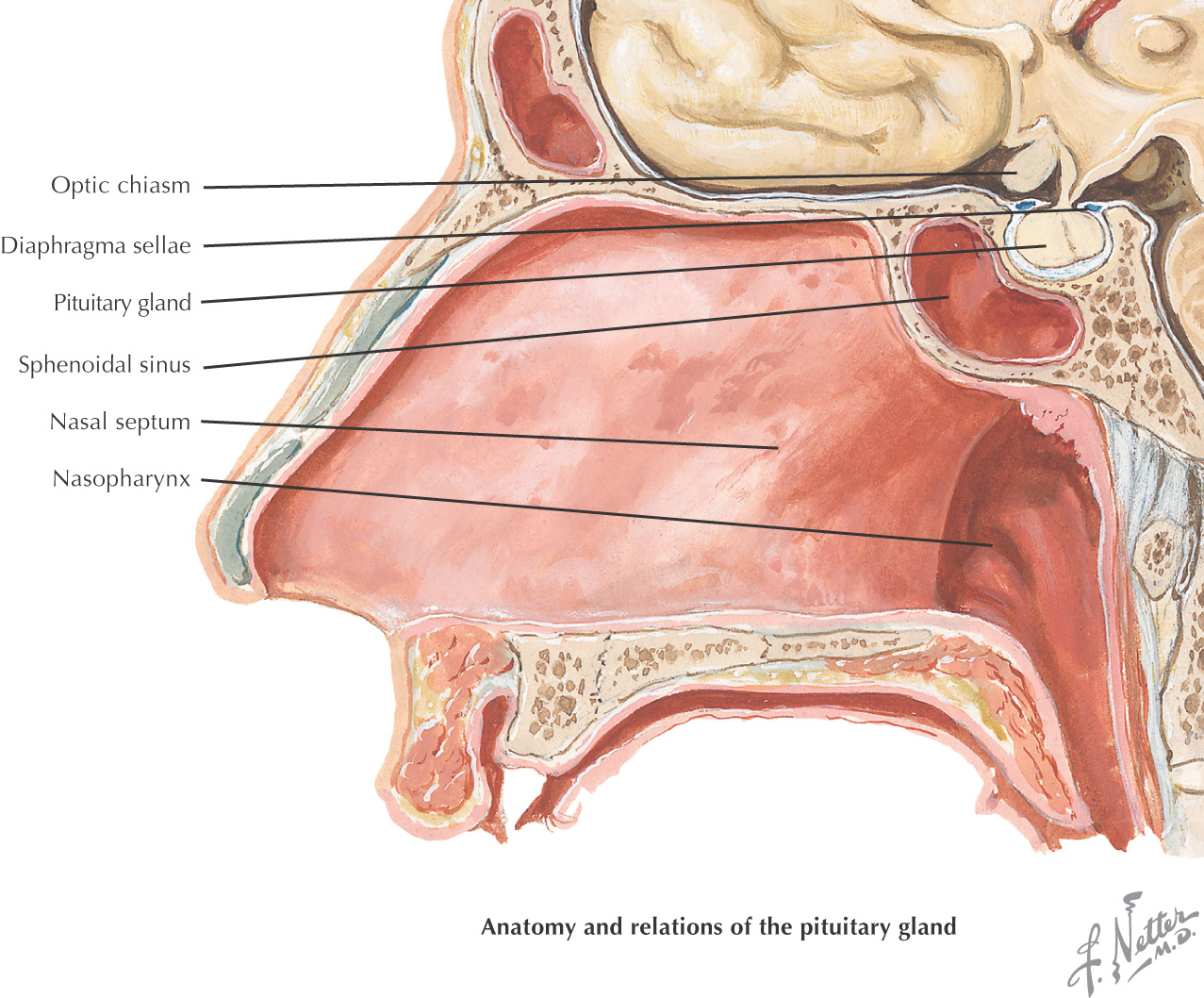
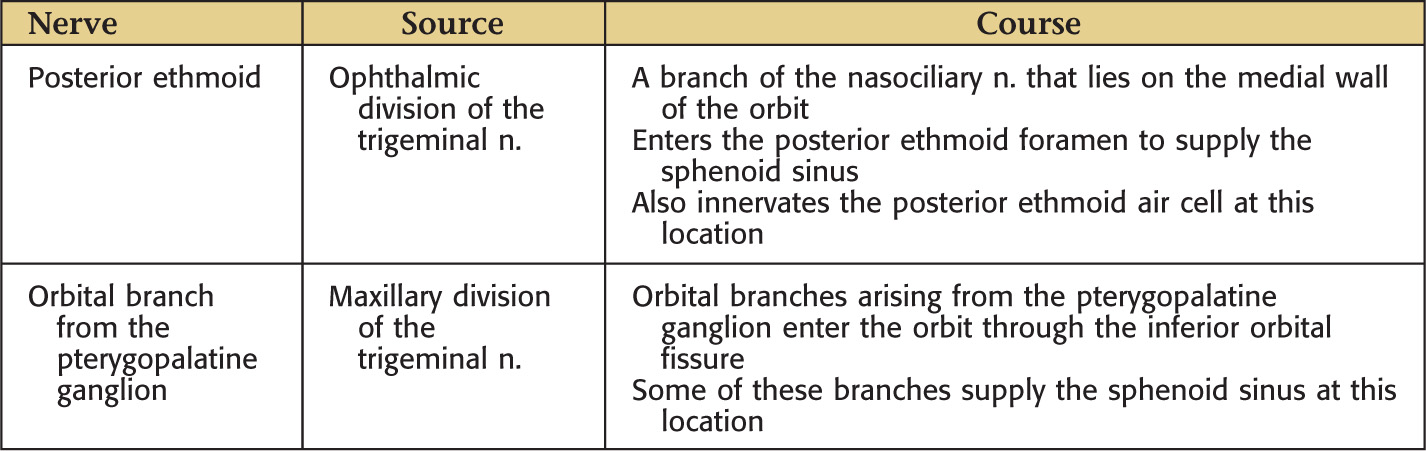
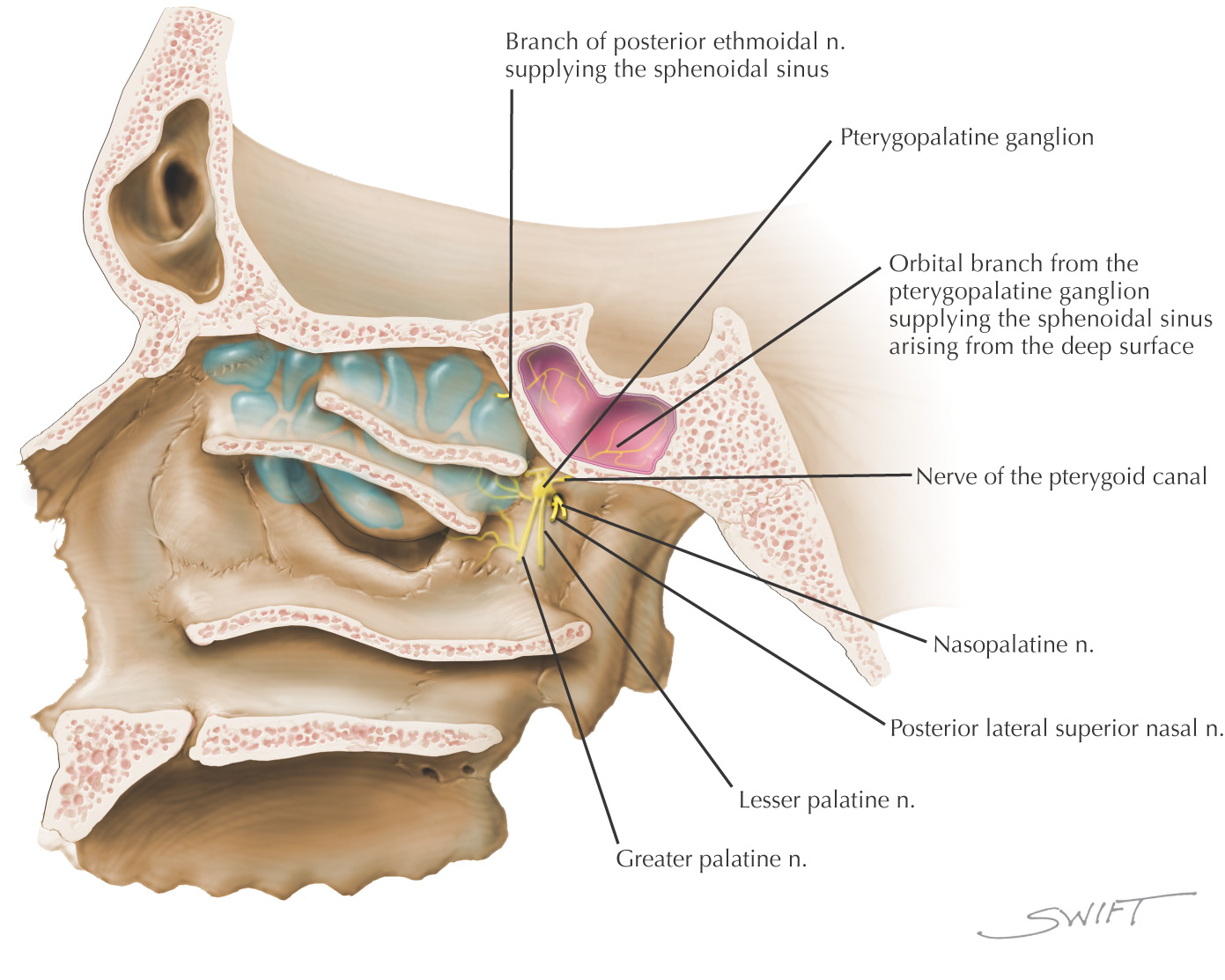
• Superior: hypophyseal fossa, pituitary gland, optic chiasm
• Inferior: nasopharynx, pterygoid canal
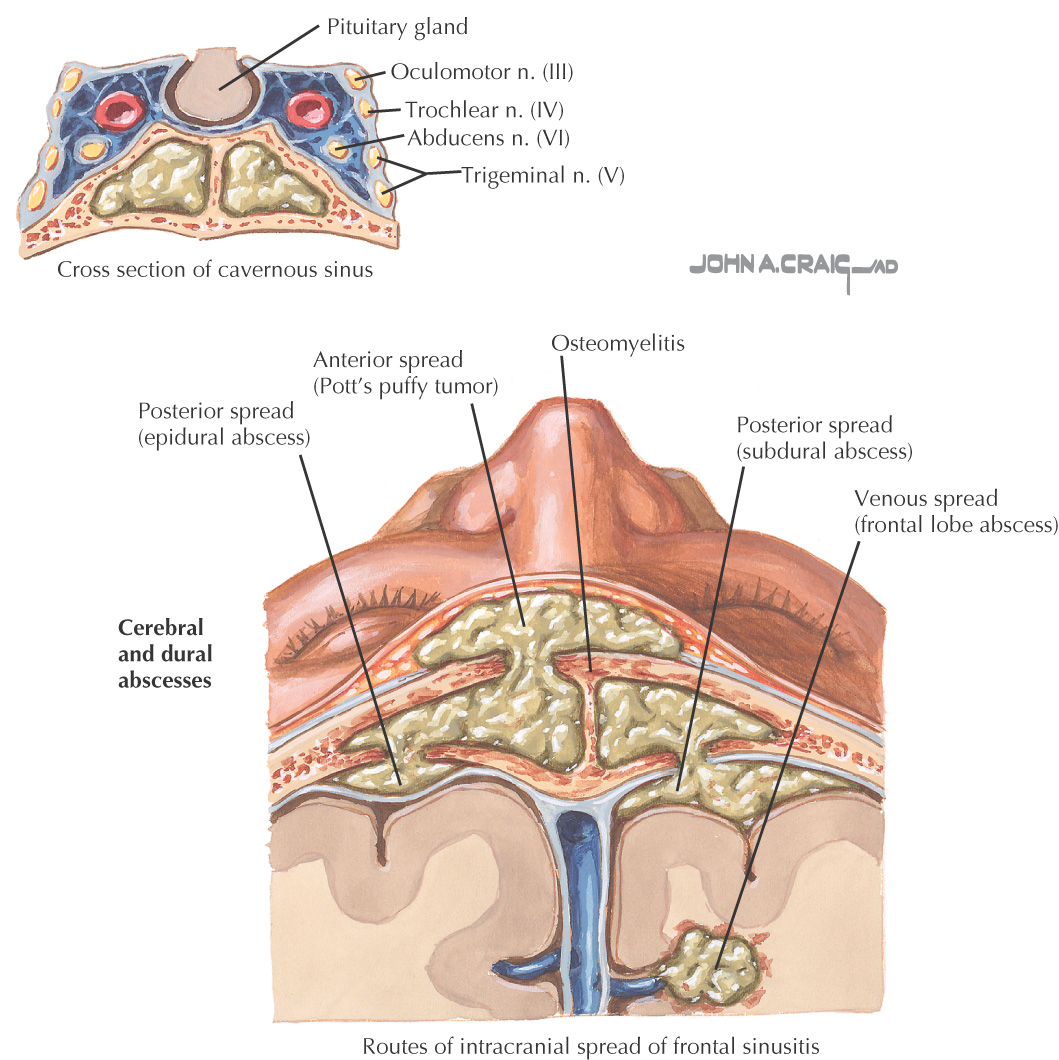
• Lateral: cavernous sinus, internal carotid artery, cranial nerves III, IV, V1, V2, and VI
Sphenoethmoidal recess
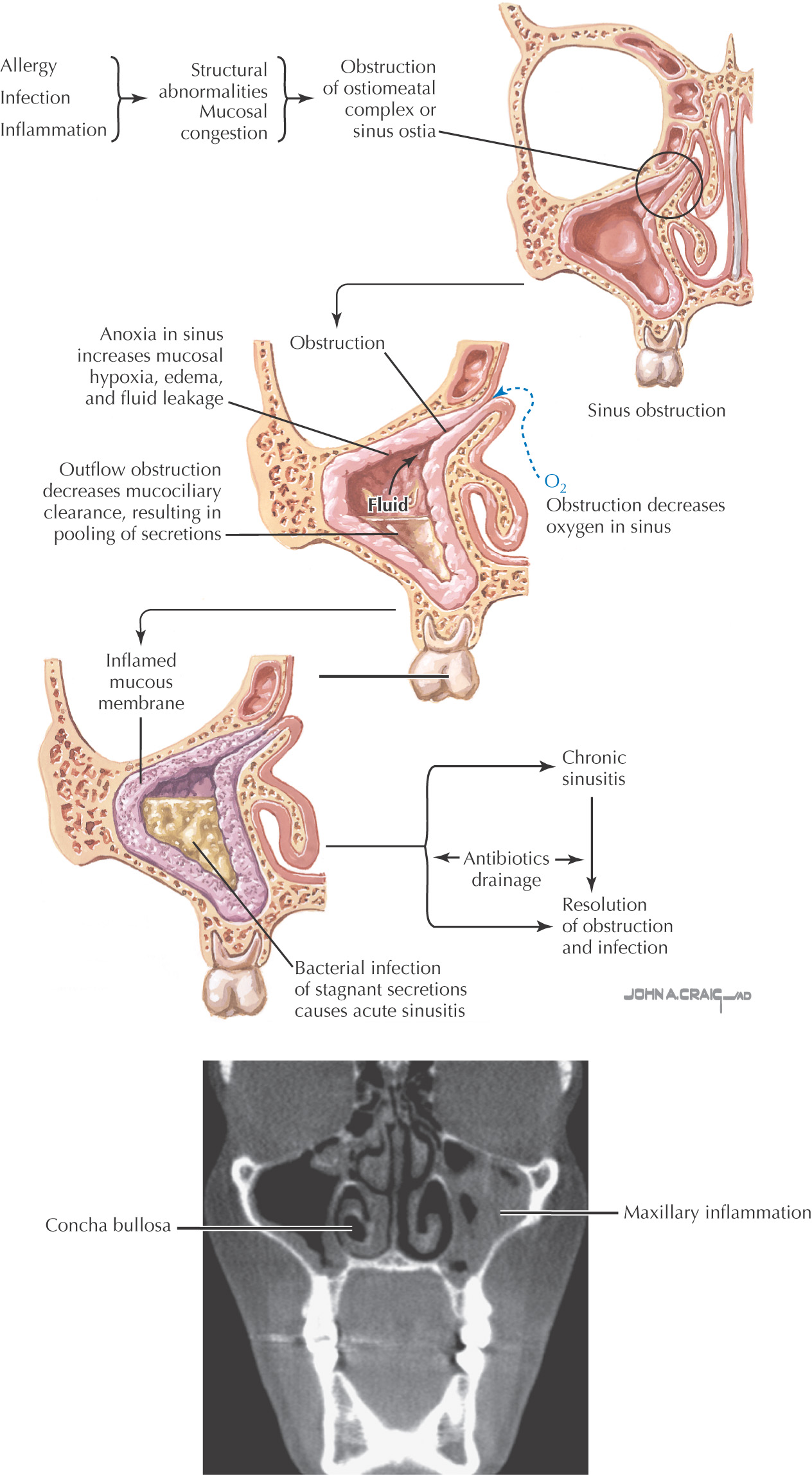
An inflammation of the membrane of the sinus cavities caused by infections (by bacteria or viruses) or noninfectious means (such as allergy)
2 types of sinusitis: acute and chronic
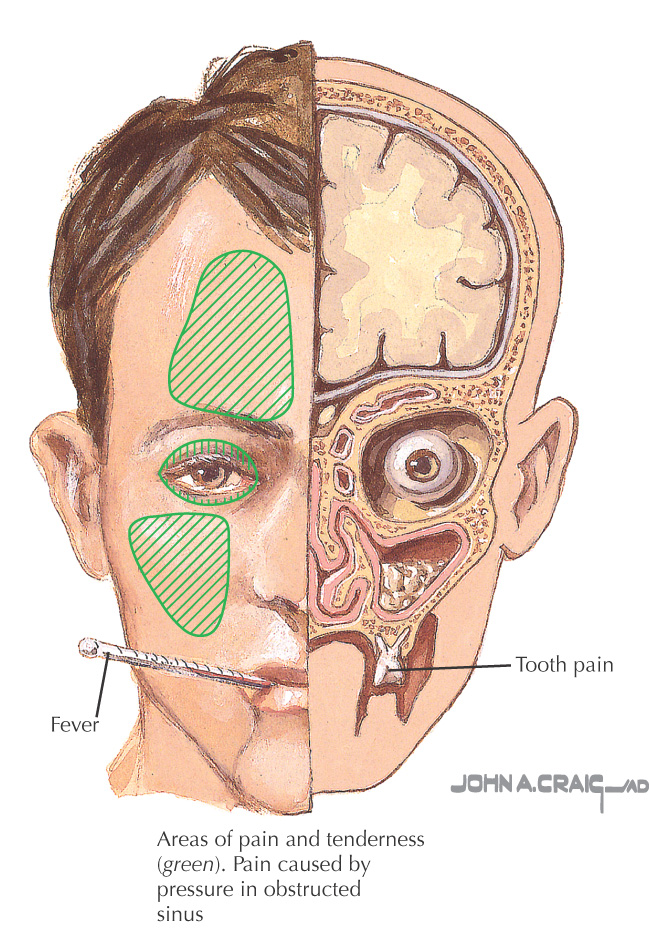
Common clinical manifestations include sinus congestion, discharge, pressure, face pain, headaches
The most common form of sinusitis
Typically caused by a cold that results in inflammation of the sinus membranes
Normally resolves in 1 to 2 weeks
Sometimes a secondary bacterial infection may settle in the passageways after a cold; bacteria normally located in the area (Streptococcus pneumoniae and Haemophilus influenzae) may then begin to increase, producing an acute bacterial sinusitis
An infection of the sinuses that is present for longer than 1 month and requires longer-duration medical therapy
Typically either chronic bacterial sinusitis or chronic noninfectious sinusitis
Chronic bacterial sinusitis is treated with antibiotics
Chronic noninfectious sinusitis often is treated with steroids (topical or oral) and nasal washes
• Maxillary: the most common location for sinusitis; associated with all of the common signs and symptoms but also results in tooth pain, usually in the molar region
• Sphenoid: rare, but in this location can result in problems with the pituitary gland, cavernous sinus syndrome, and meningitis
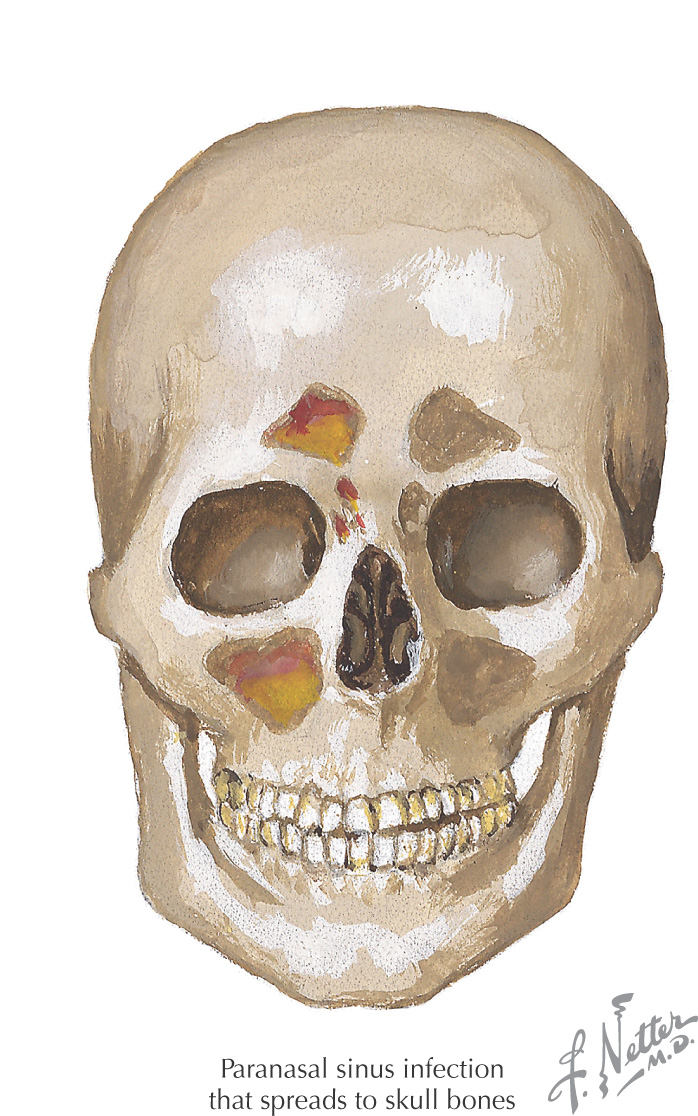
• Frontal: usually associated with pain over the forehead and possibly fever; rare complications include osteomyelitis
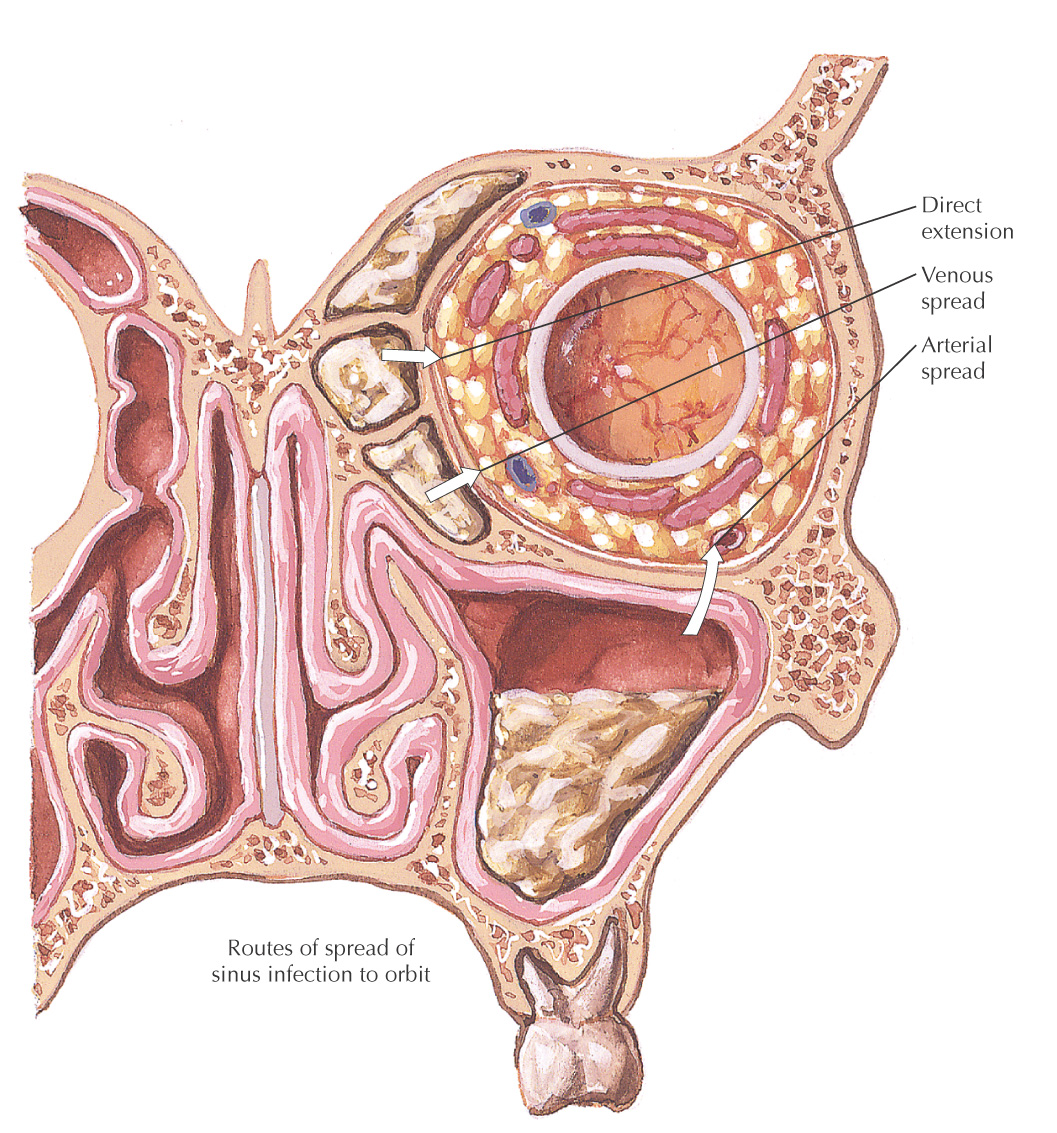
• Ethmoid: potential complications include meningitis and orbital cellulitis
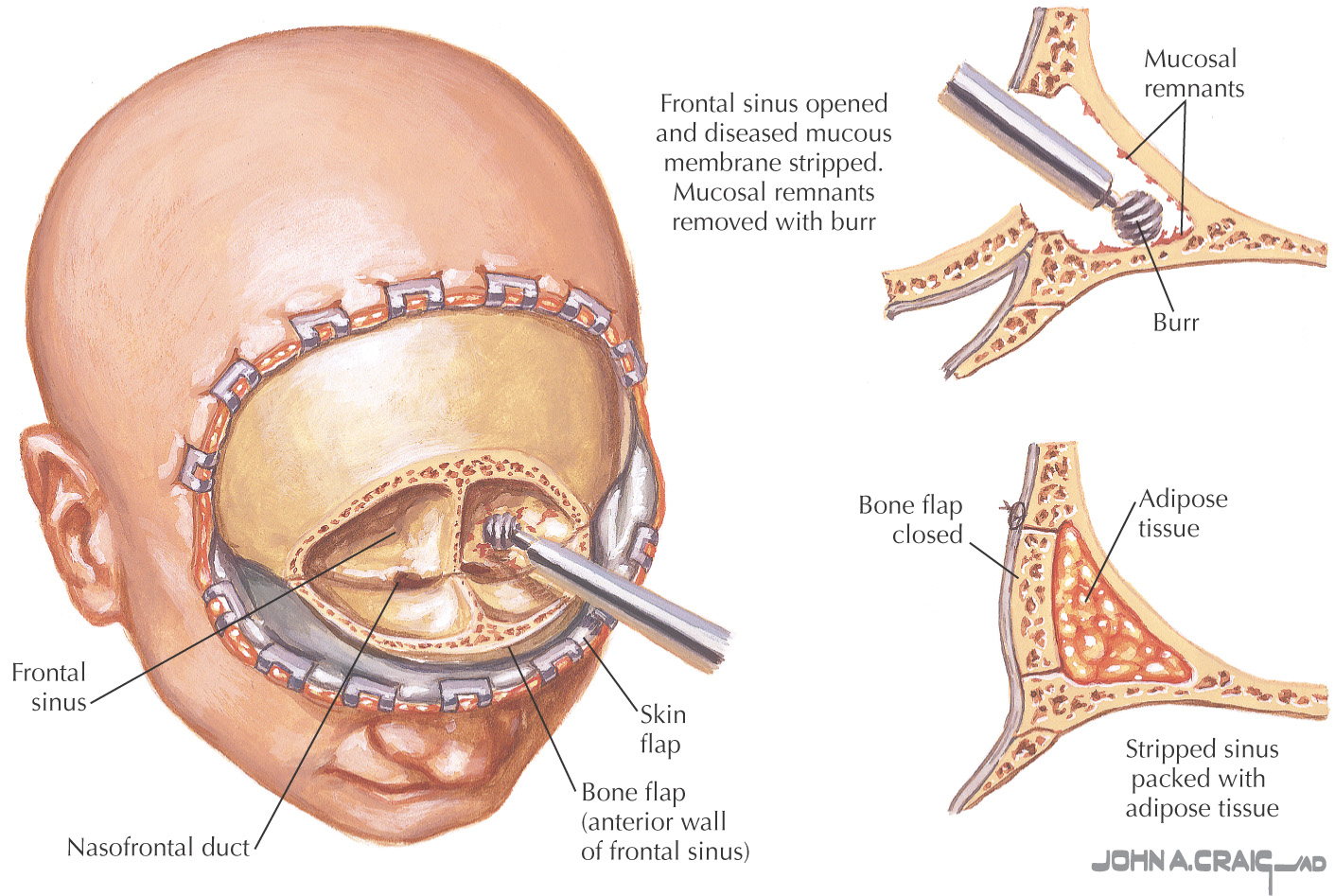
A procedure in which the frontal sinus is completely removed to treat problematic cases of frontal sinus infection, osteomyelitis, and trauma
Once the sinus is opened, all of the sinus membrane is removed with a burr; otherwise, any remaining membrane may form a mucocele
The remaining area often is filled with adipose tissue from the patient because it is thought to impede regrowth of the mucoperiosteum
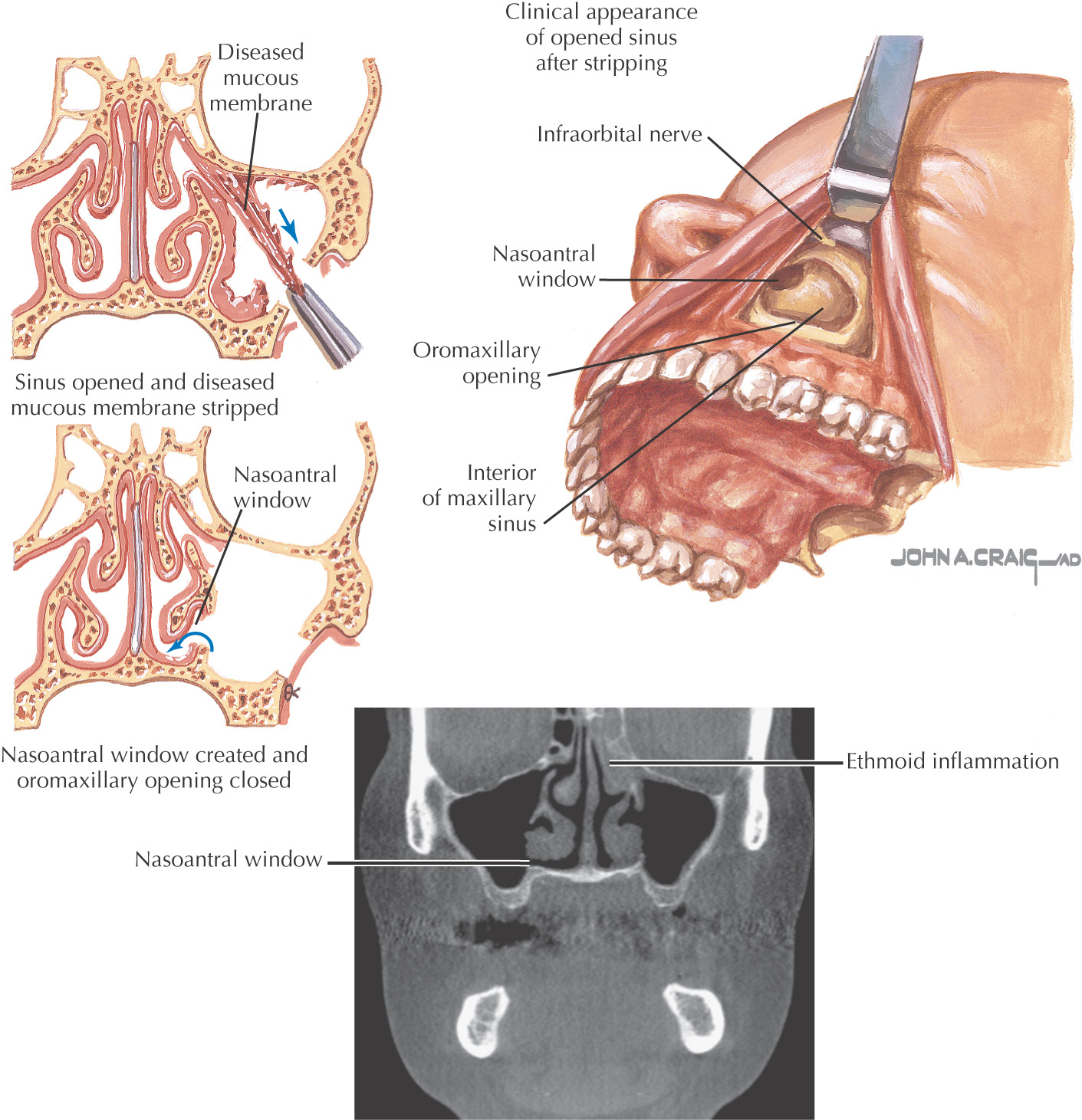
This intraoral procedure allows direct entry into the maxillary sinus
Also provides access to the ethmoid sinus
The maxillary sinus is entered through the canine fossa above the maxillary premolar teeth
The maxillary antrum is opened, the sinus membrane is stripped, and an additional antrostomy is made between the maxillary sinus and the inferior meatus
The antrostomy allows drainage of the maxillary sinus into the nasal cavity
With the advent of functional endoscopic sinus surgery for antrostomies, the Caldwell-Luc procedure often is used for exposure and removal of tumors
Used to be commonly performed to treat chronic maxillary sinusitis
Was also used for procedures such as removal of benign tumors and foreign bodies, access to the pterygopalatine fossa, and closure of dental fistulas into the maxillary sinus
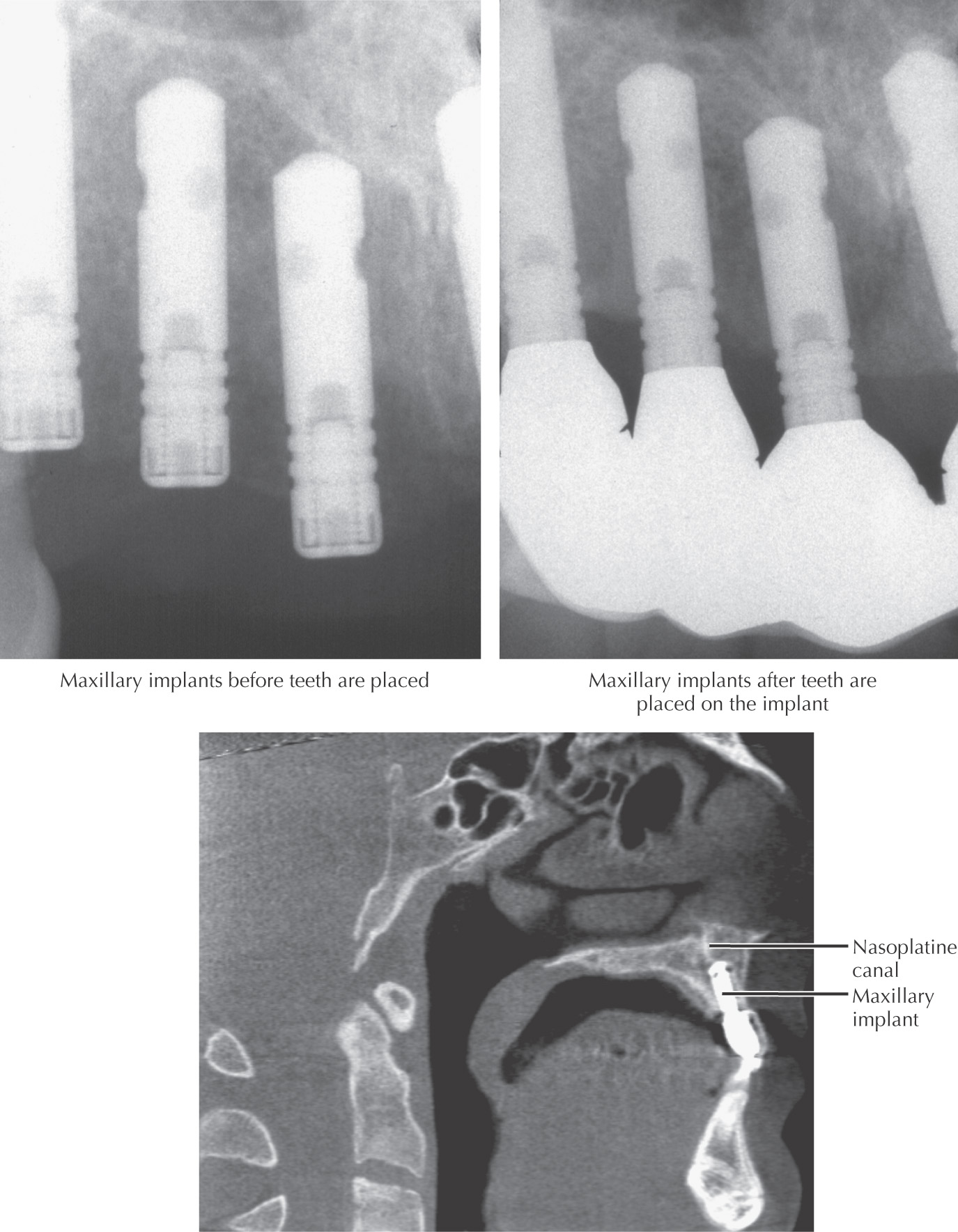
Common dental procedure to add fixed maxillary teeth to the oral cavity
Patient should be in relatively good health
Patient must have sufficient bone in a location suitable for placing an implant
It is becoming more common to use bone grafting before the surgical implant is placed
Bone grafts to provide adequate bed for implants may be harvested from the body or as allografts, or may be supplied as xenografts or synthetic bone substitutes
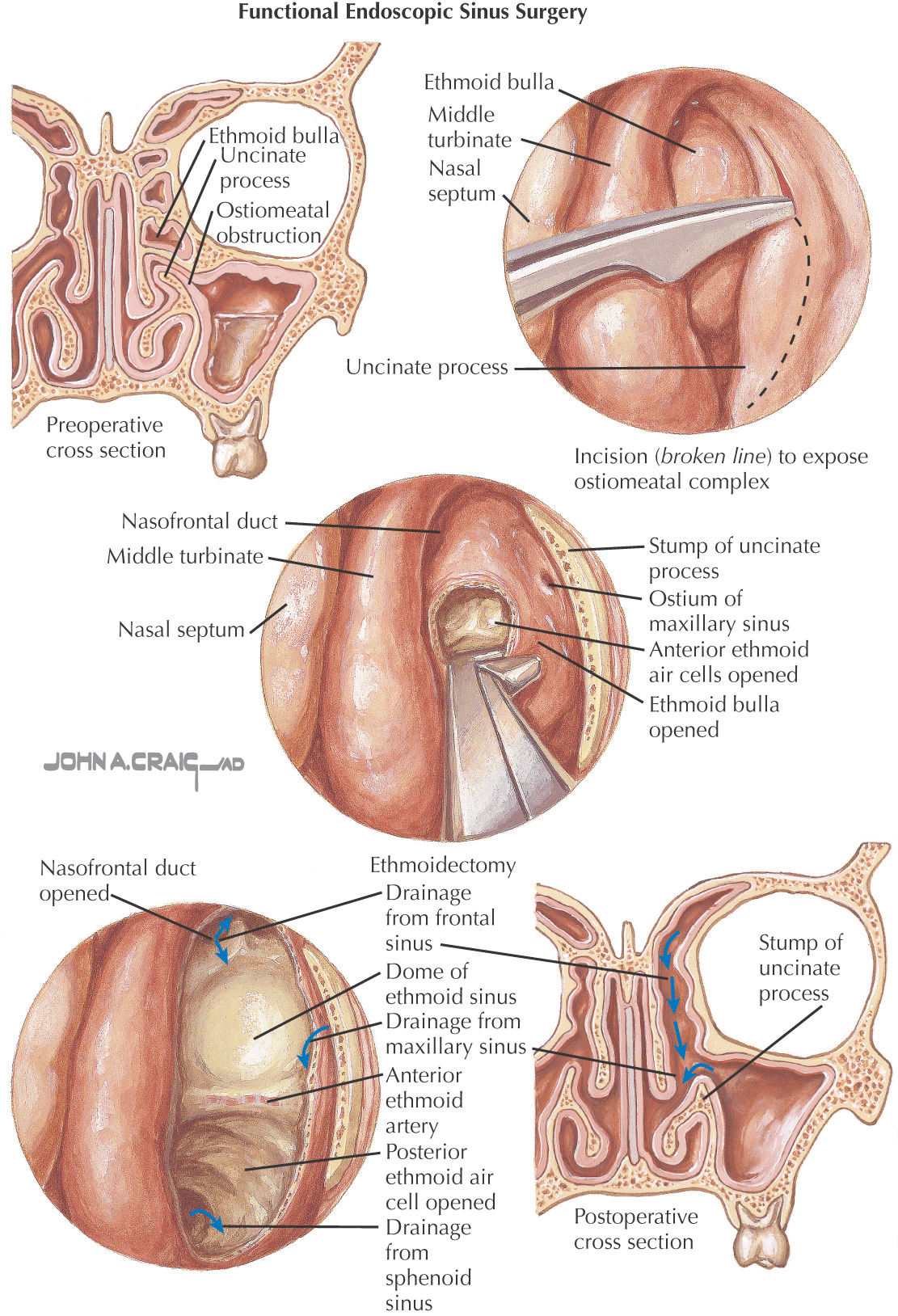
Uses an endoscope inserted into the nose to view the nasal cavity and sinuses, thereby eliminating an external incision
Often an outpatient procedure
Provides increased visualization of the area, making it easier to remove diseased tissue and leave a greater amount of normal tissue intact
Standard surgical treatment for sinusitis for people whose chronic sinus problems do not respond to medical therapy
Also used for removal of polyps, mucoceles, tumors, and foreign bodies and for control of epistaxis