Overview and Topographic Anatomy
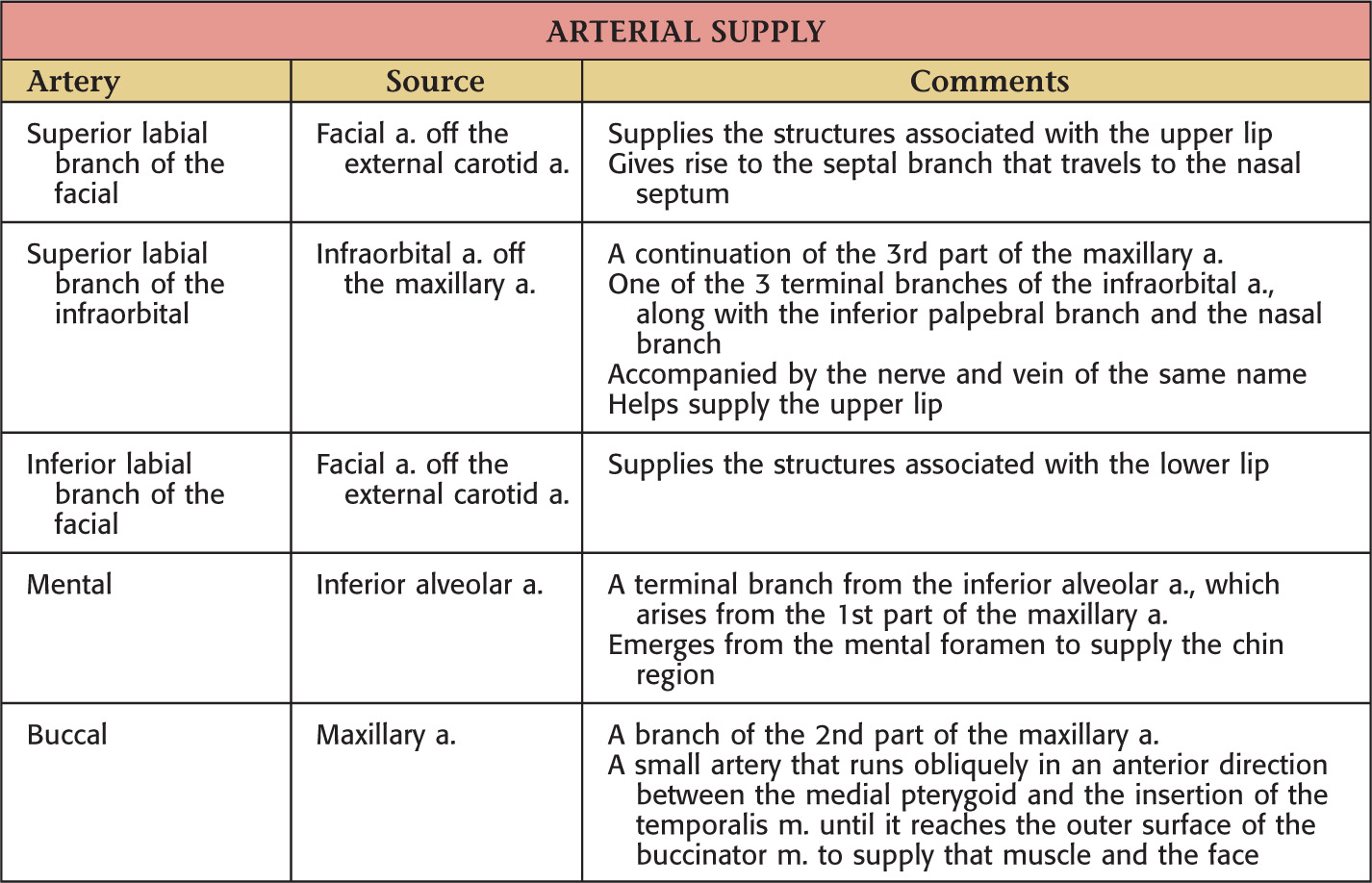
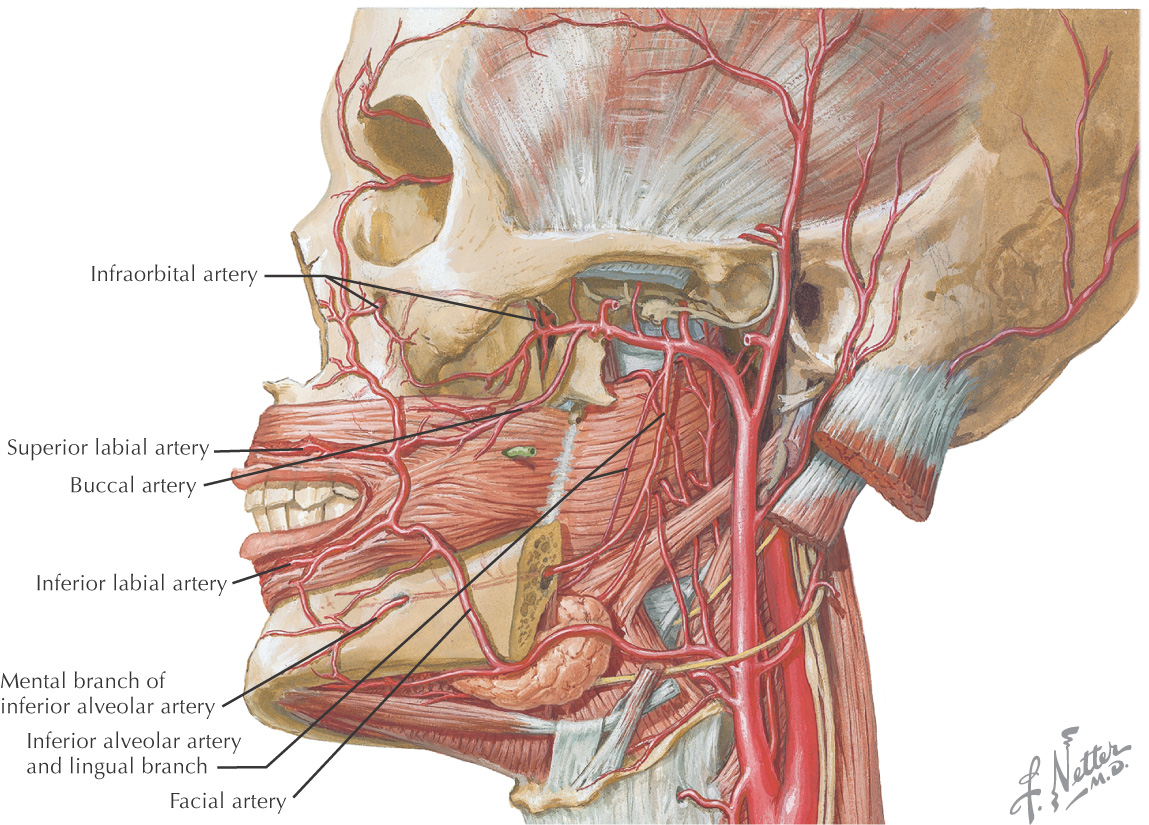
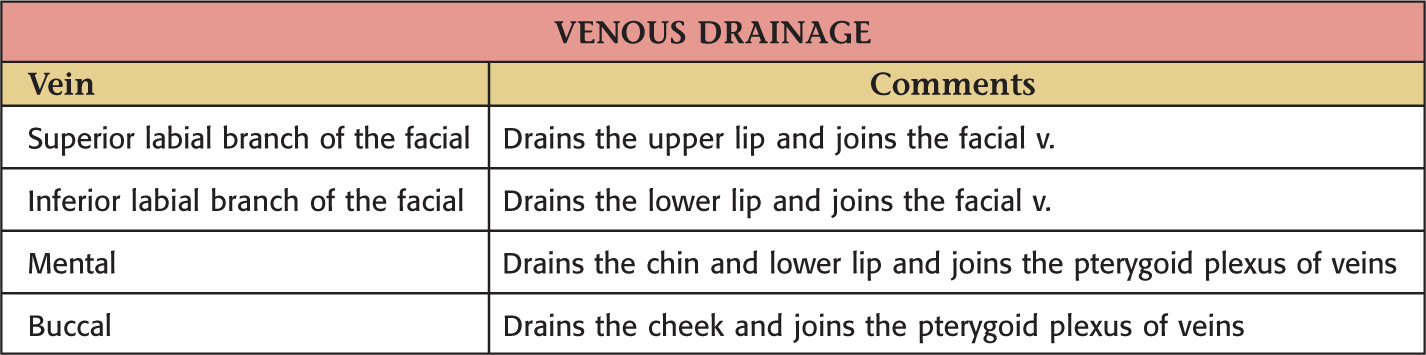
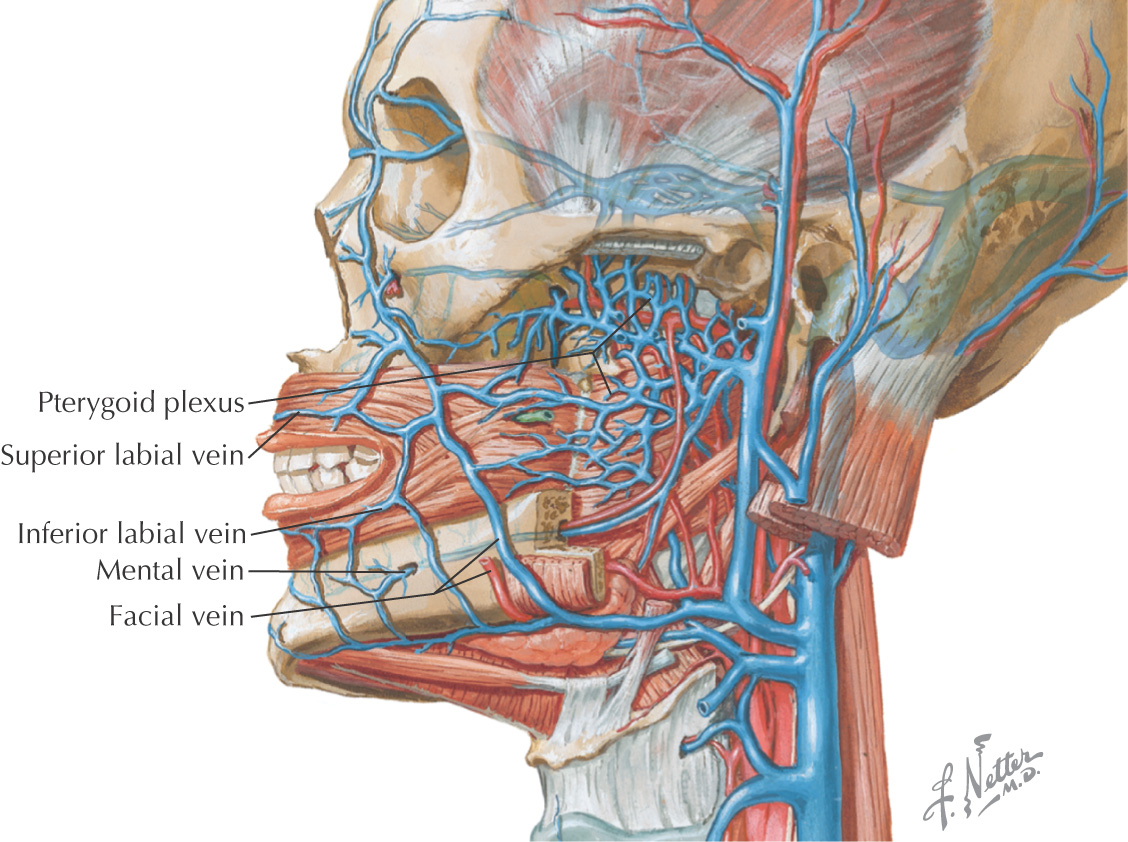
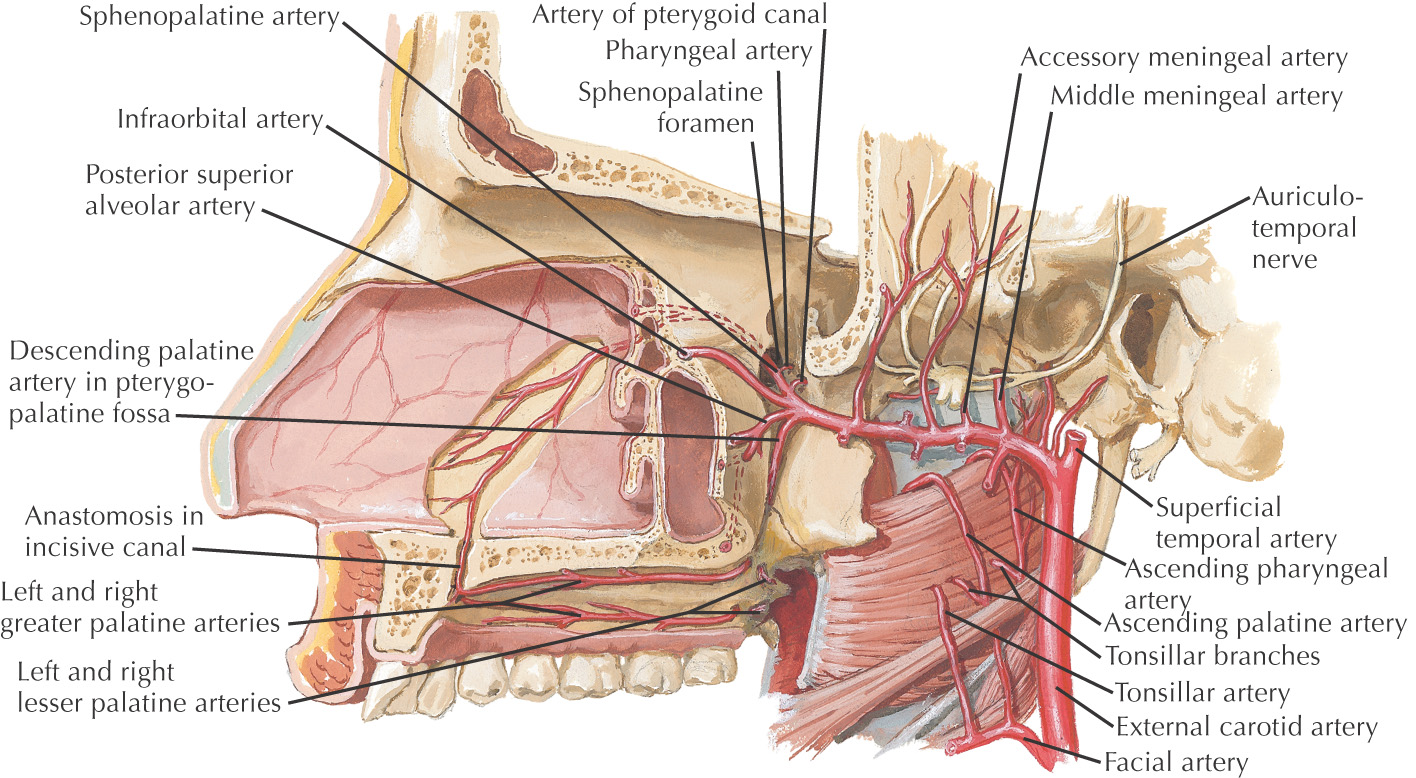
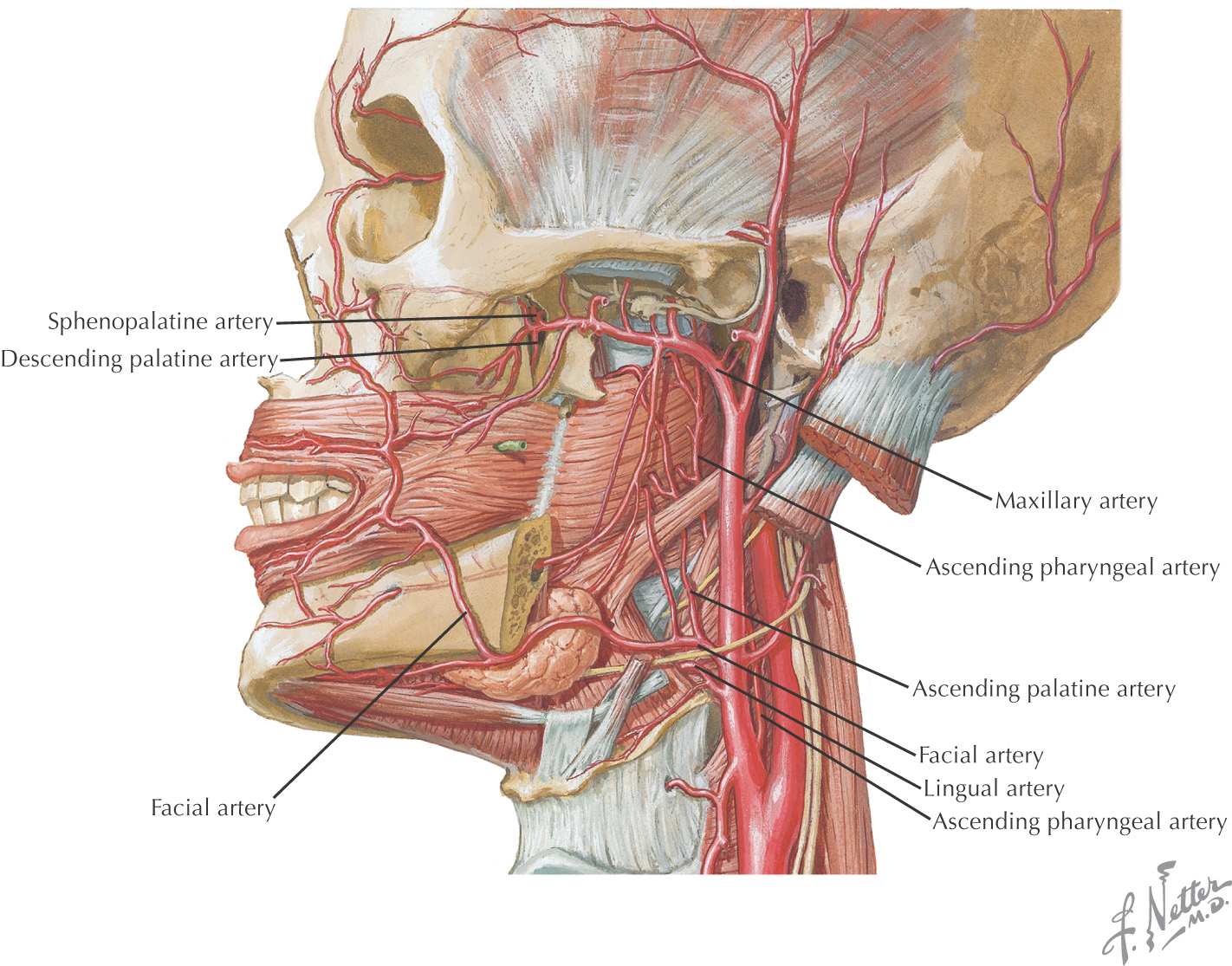
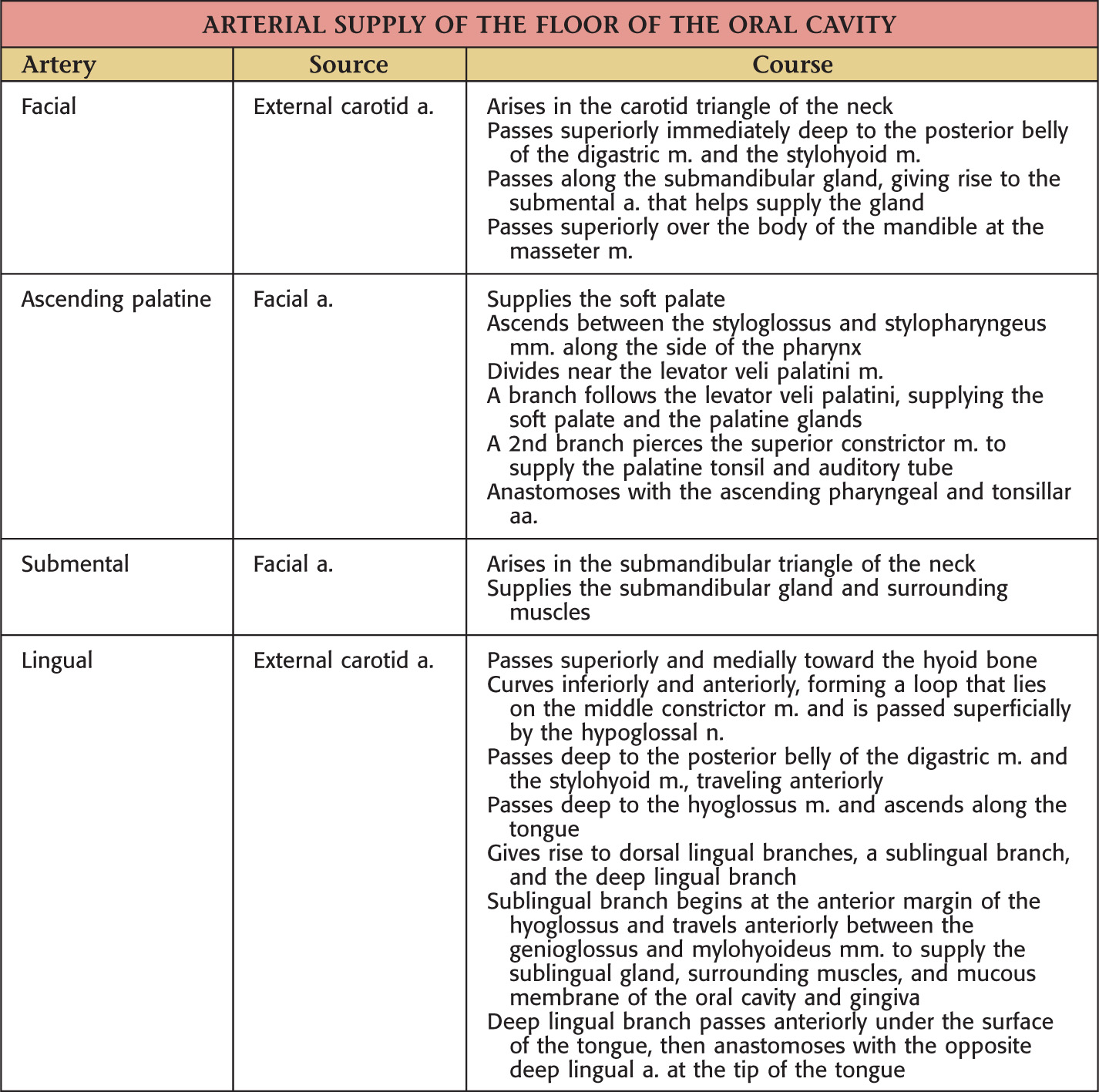
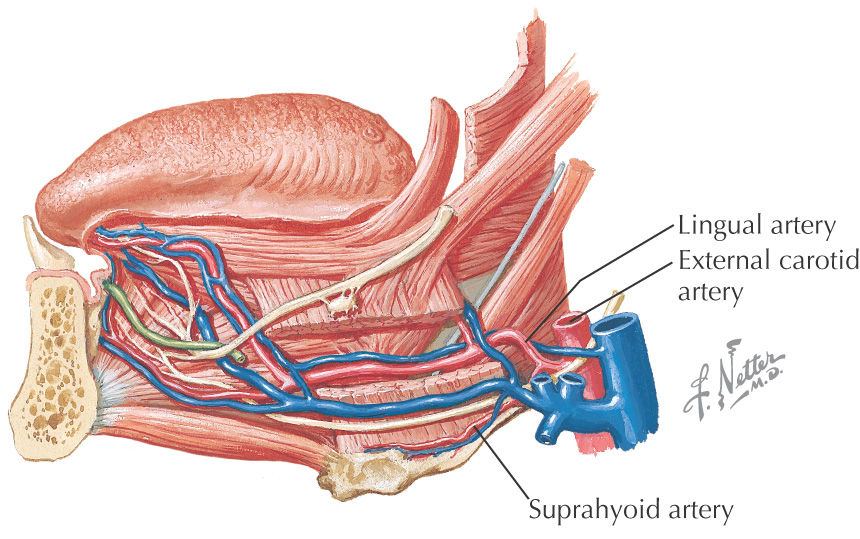
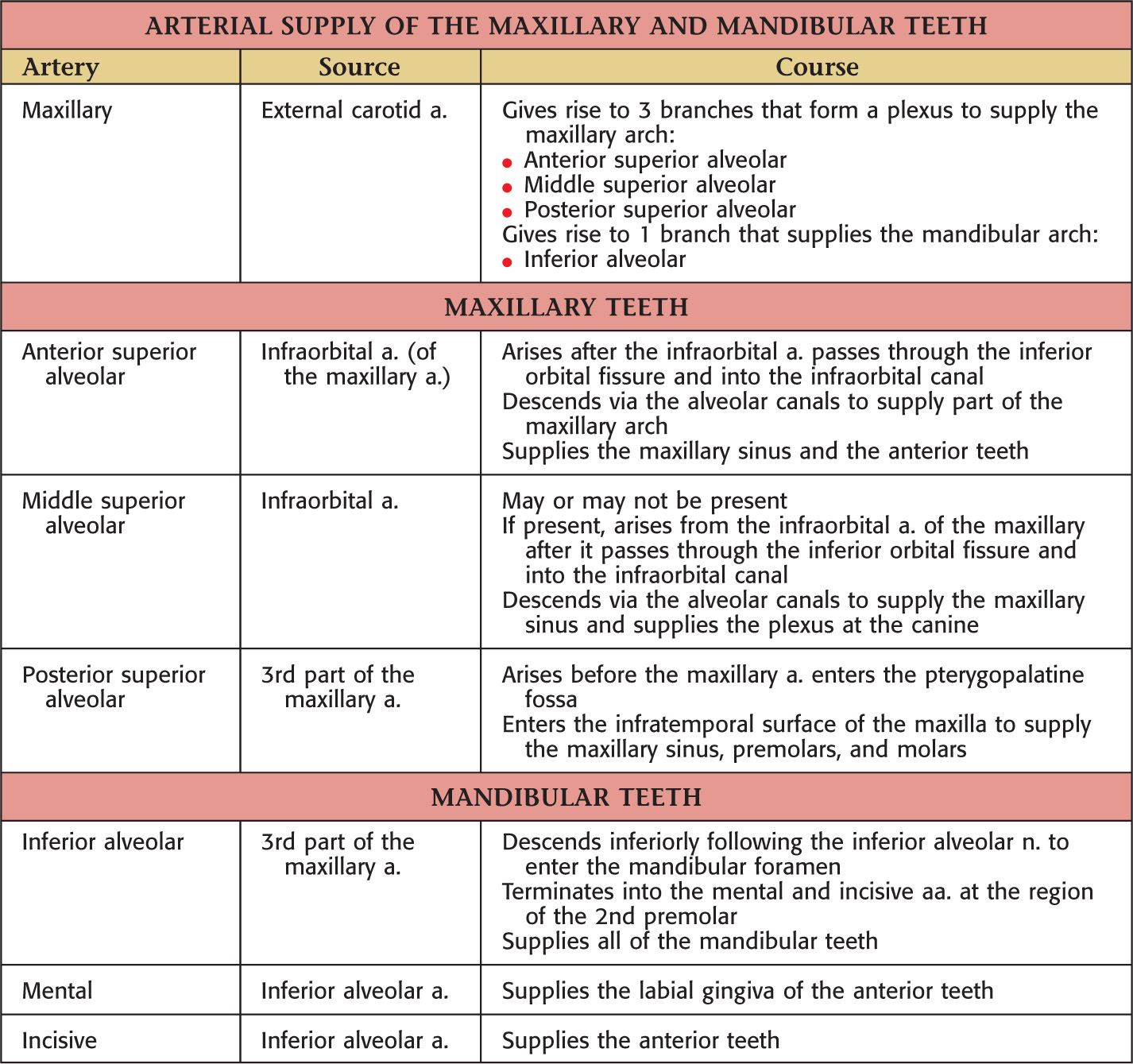
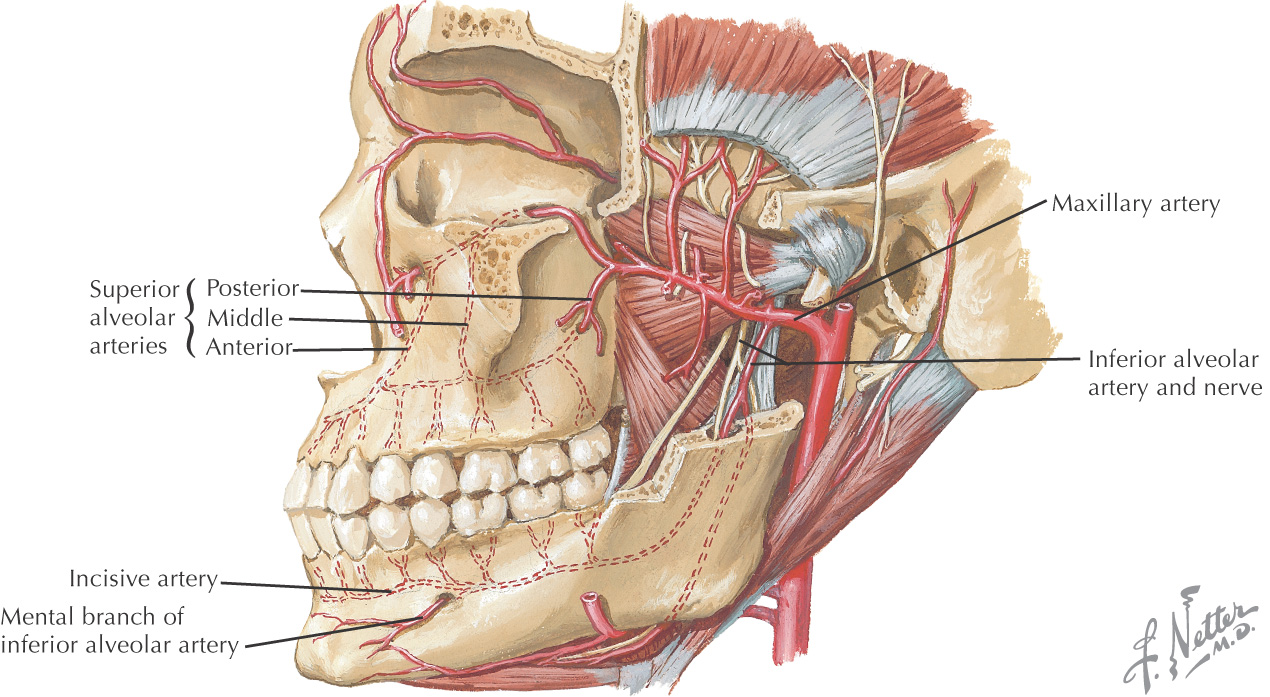
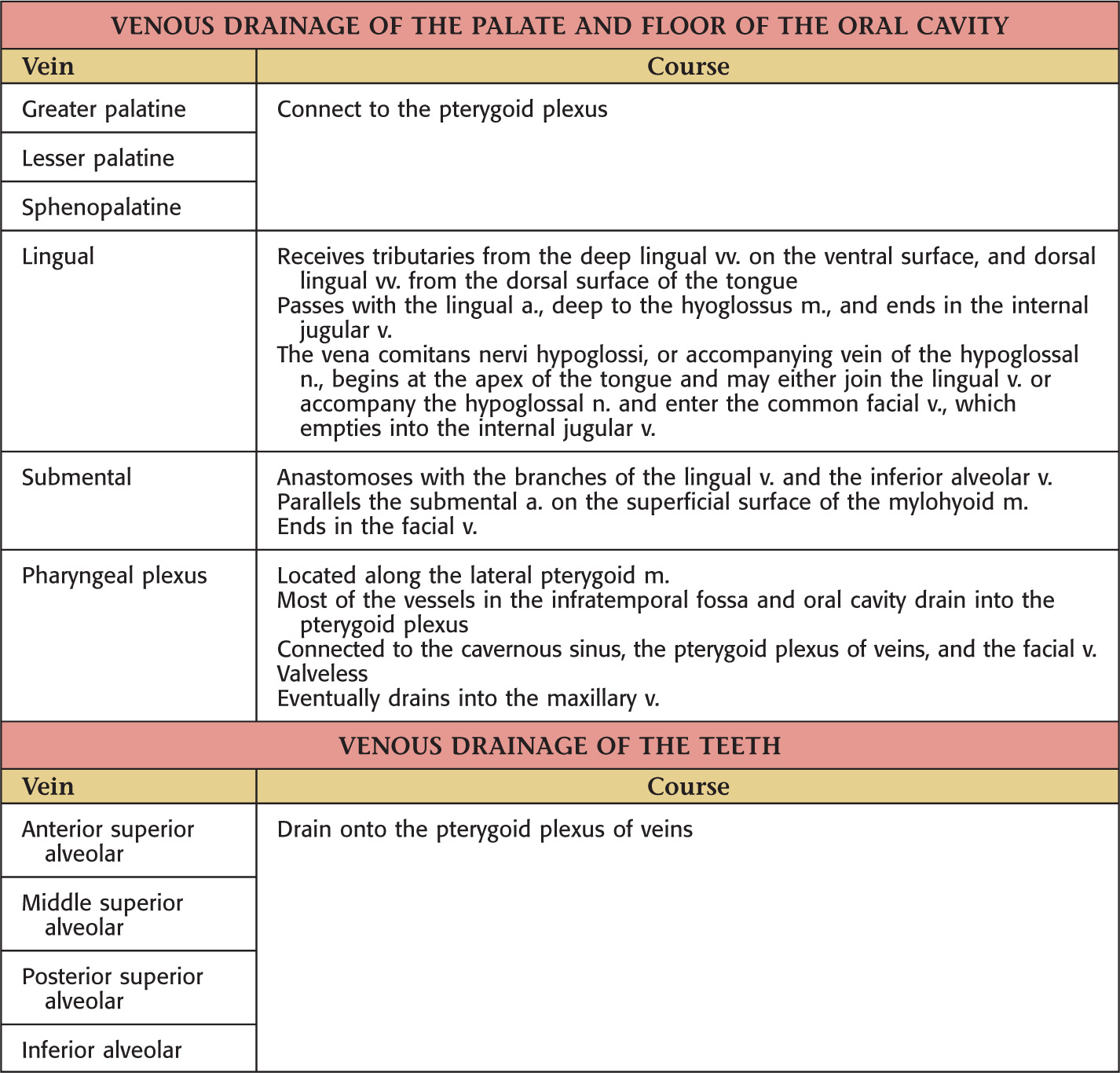
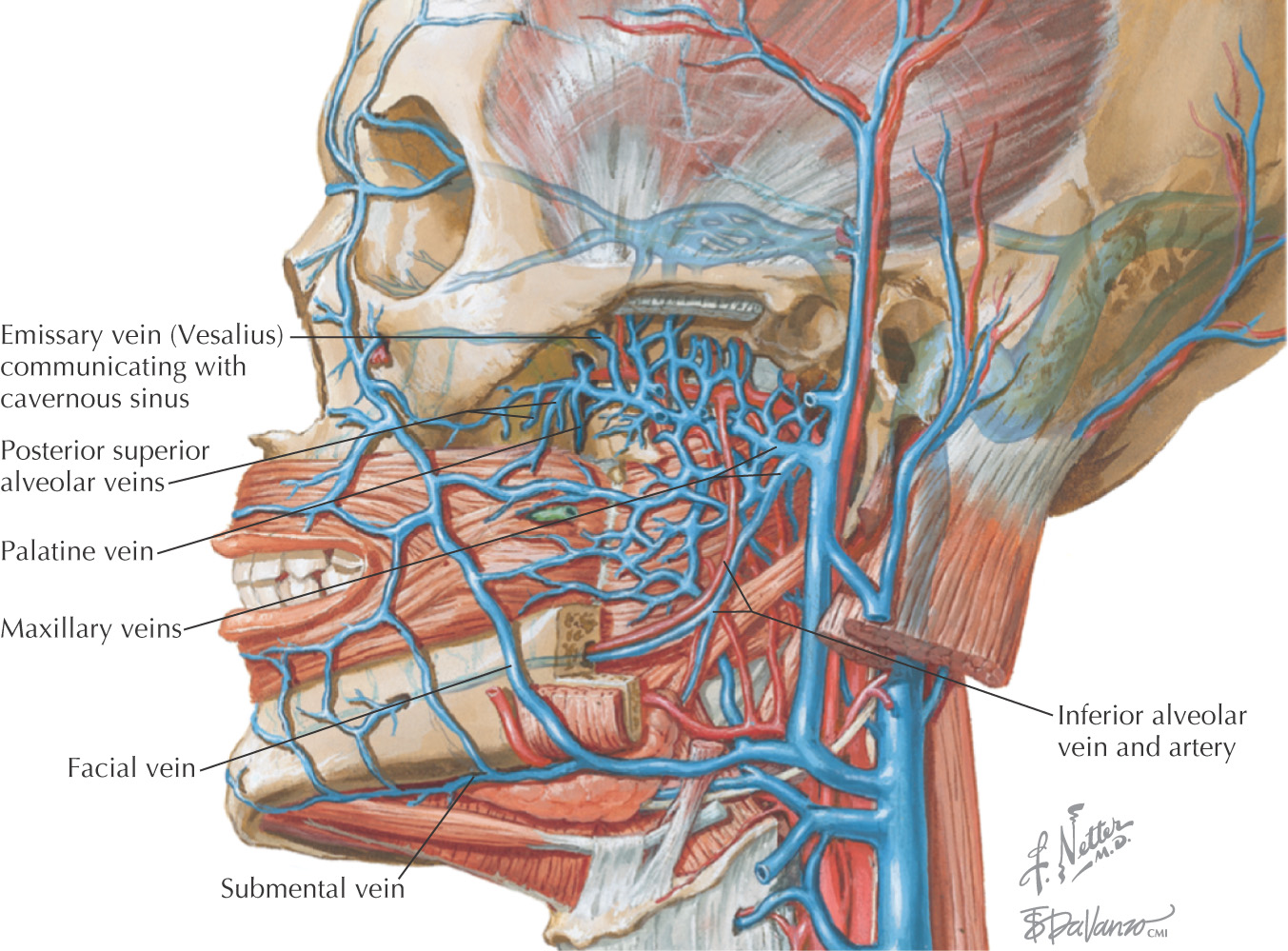
Vascular Supply of the Oral Cavity
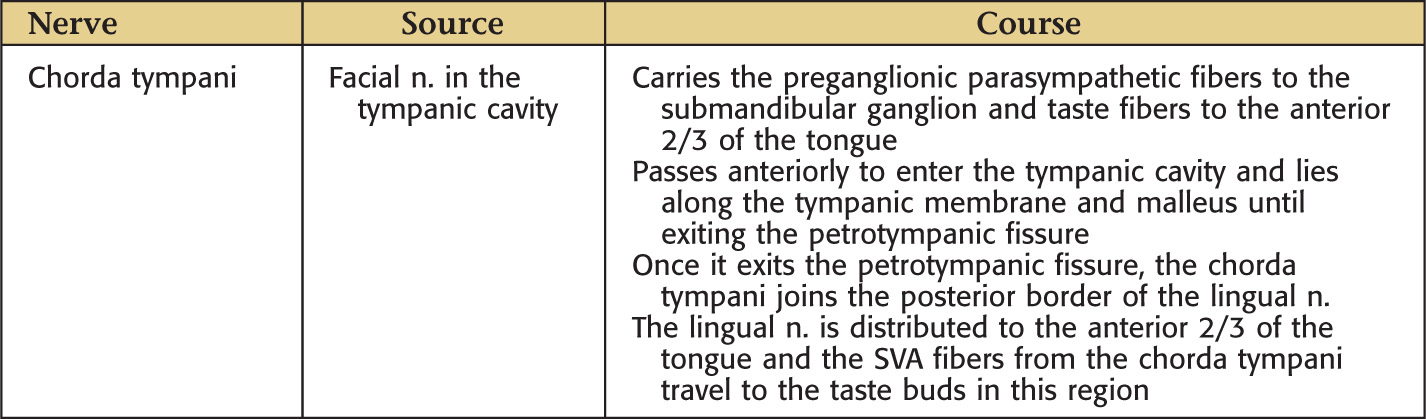
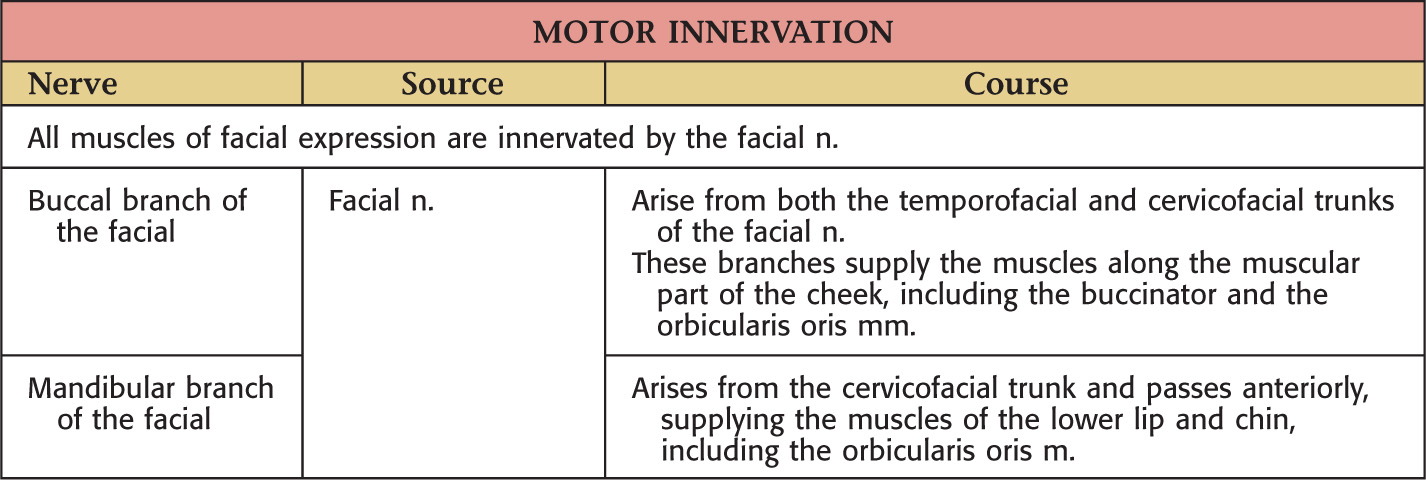
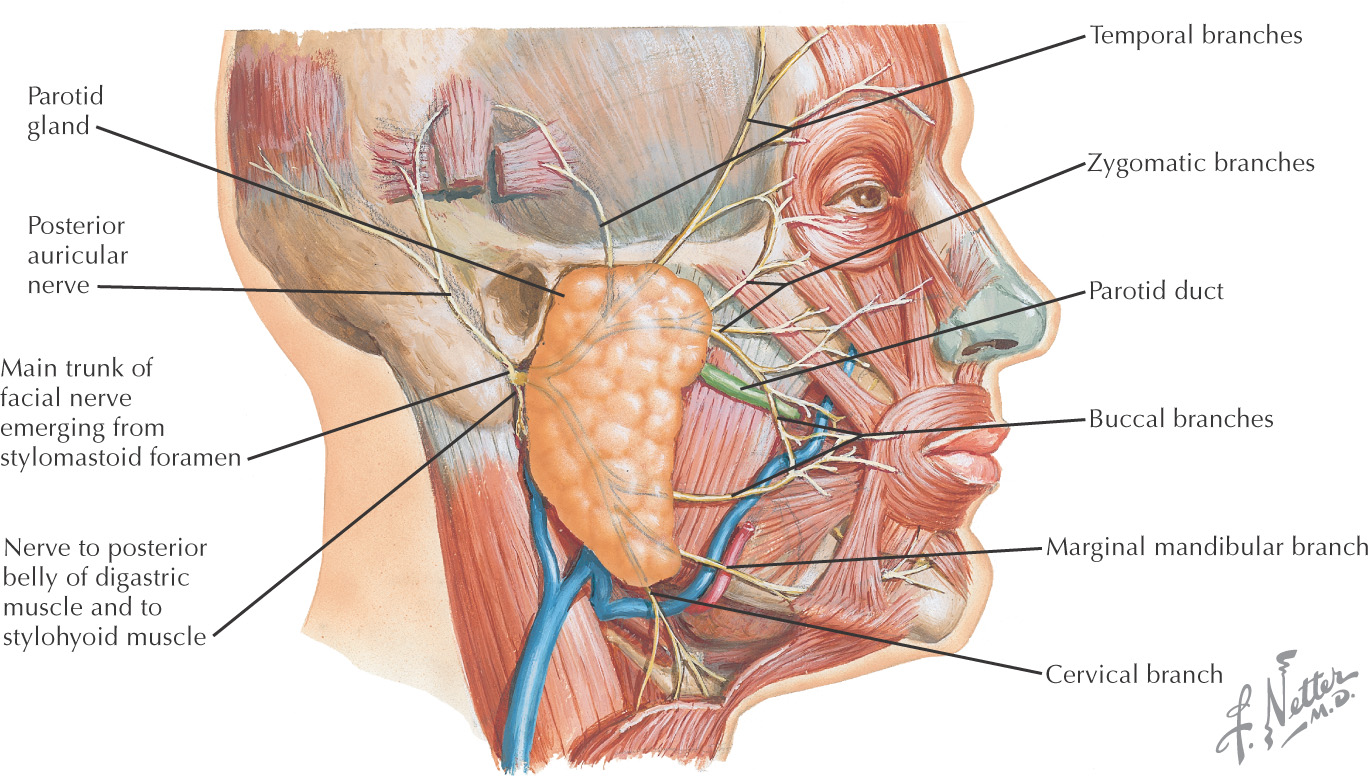
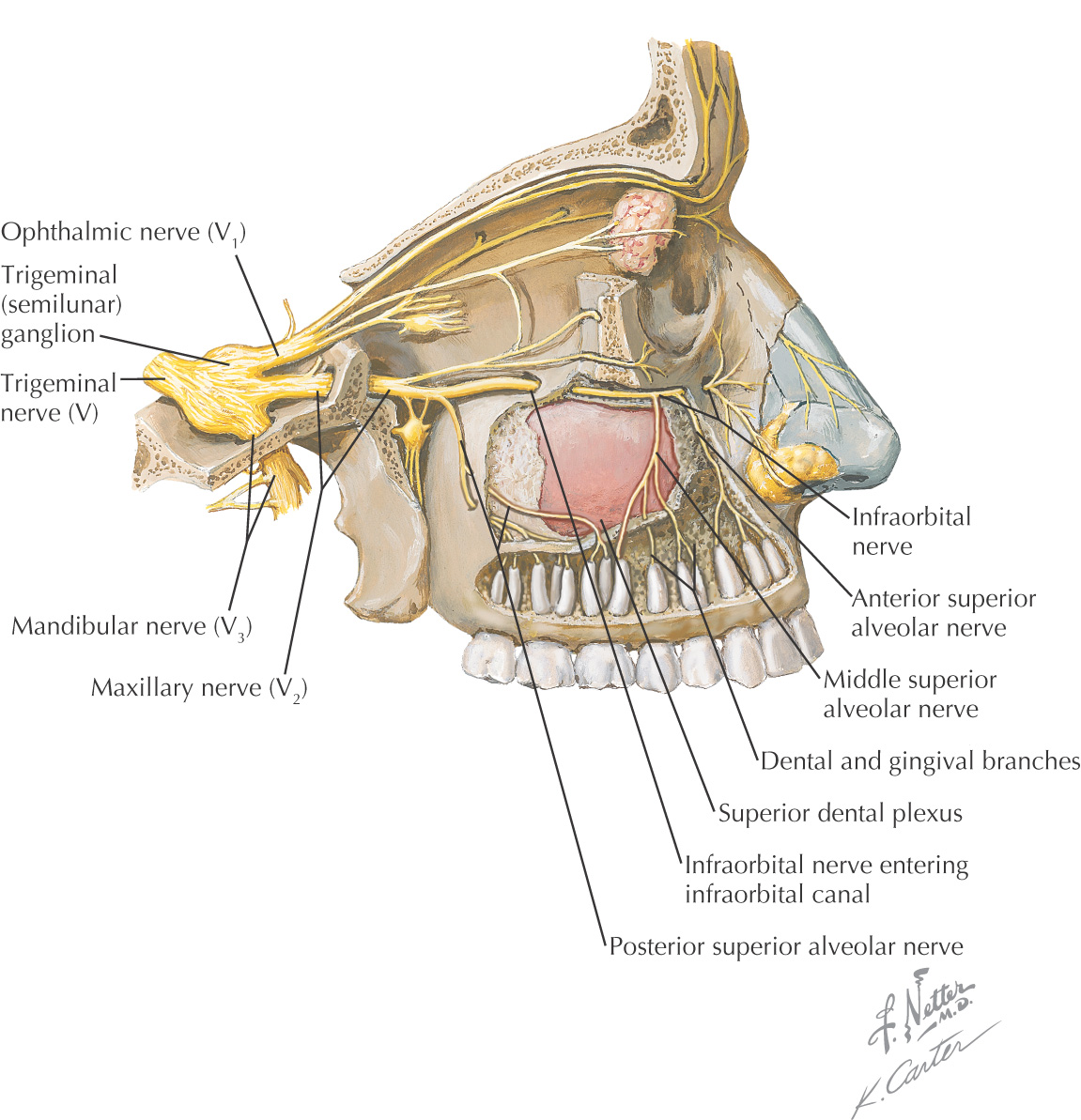
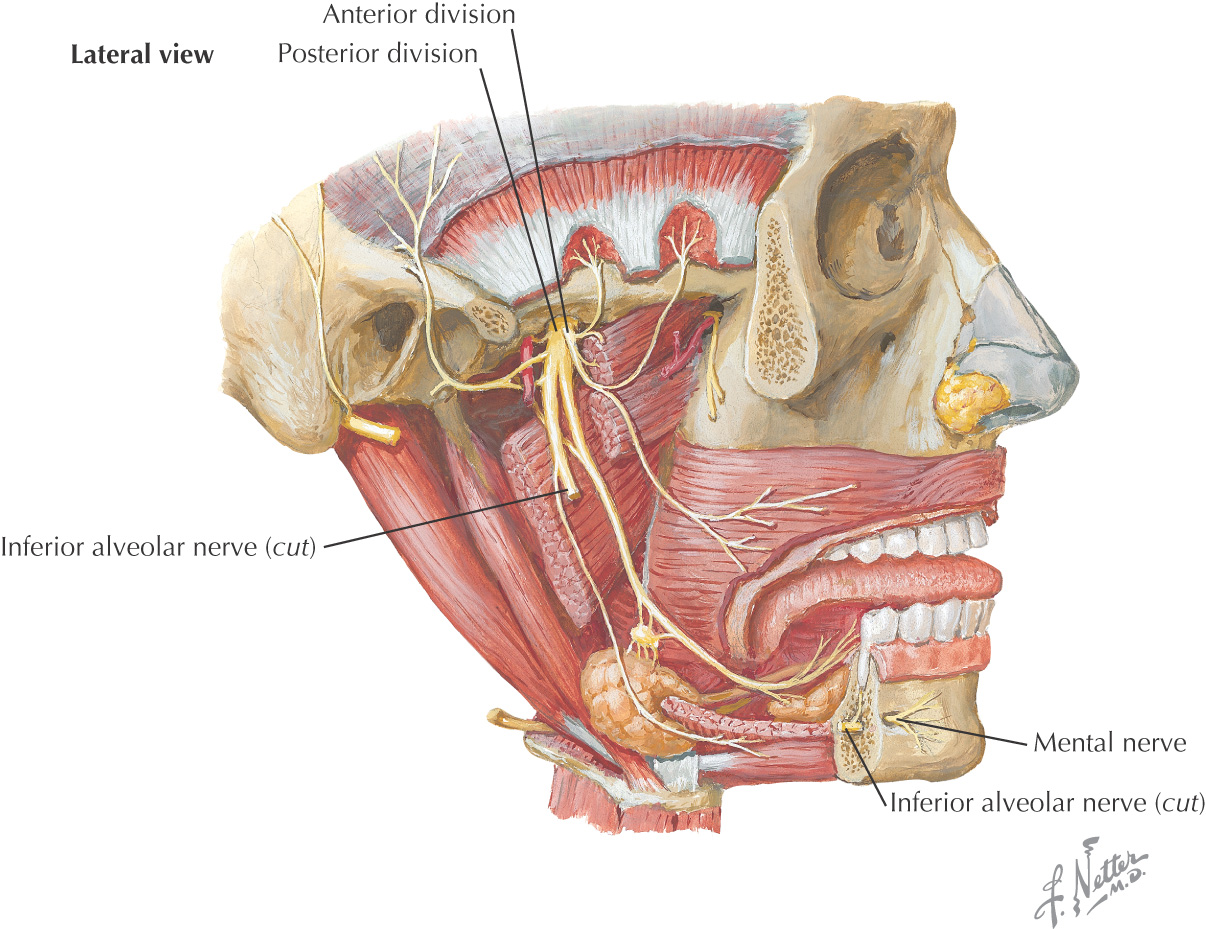
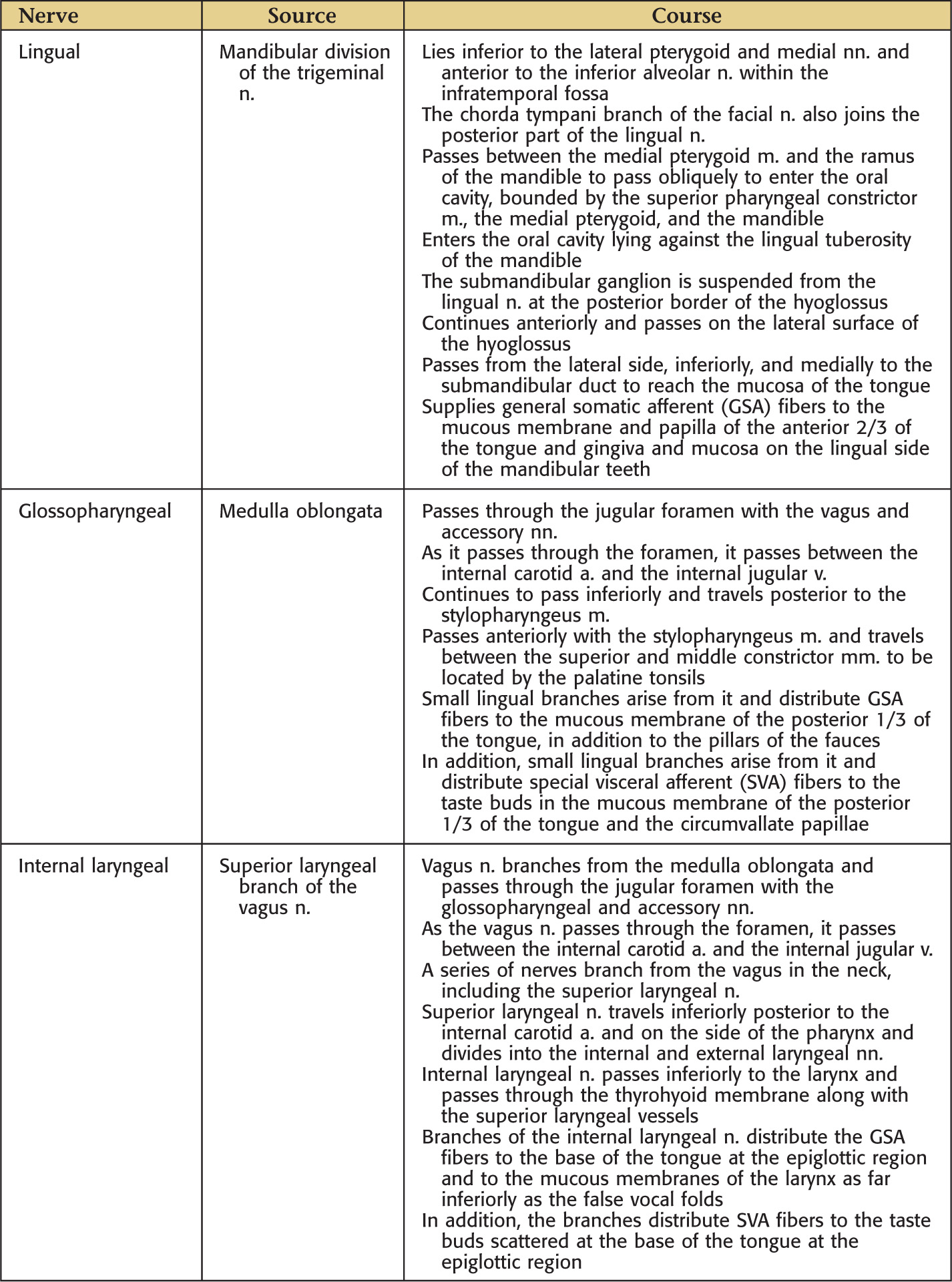
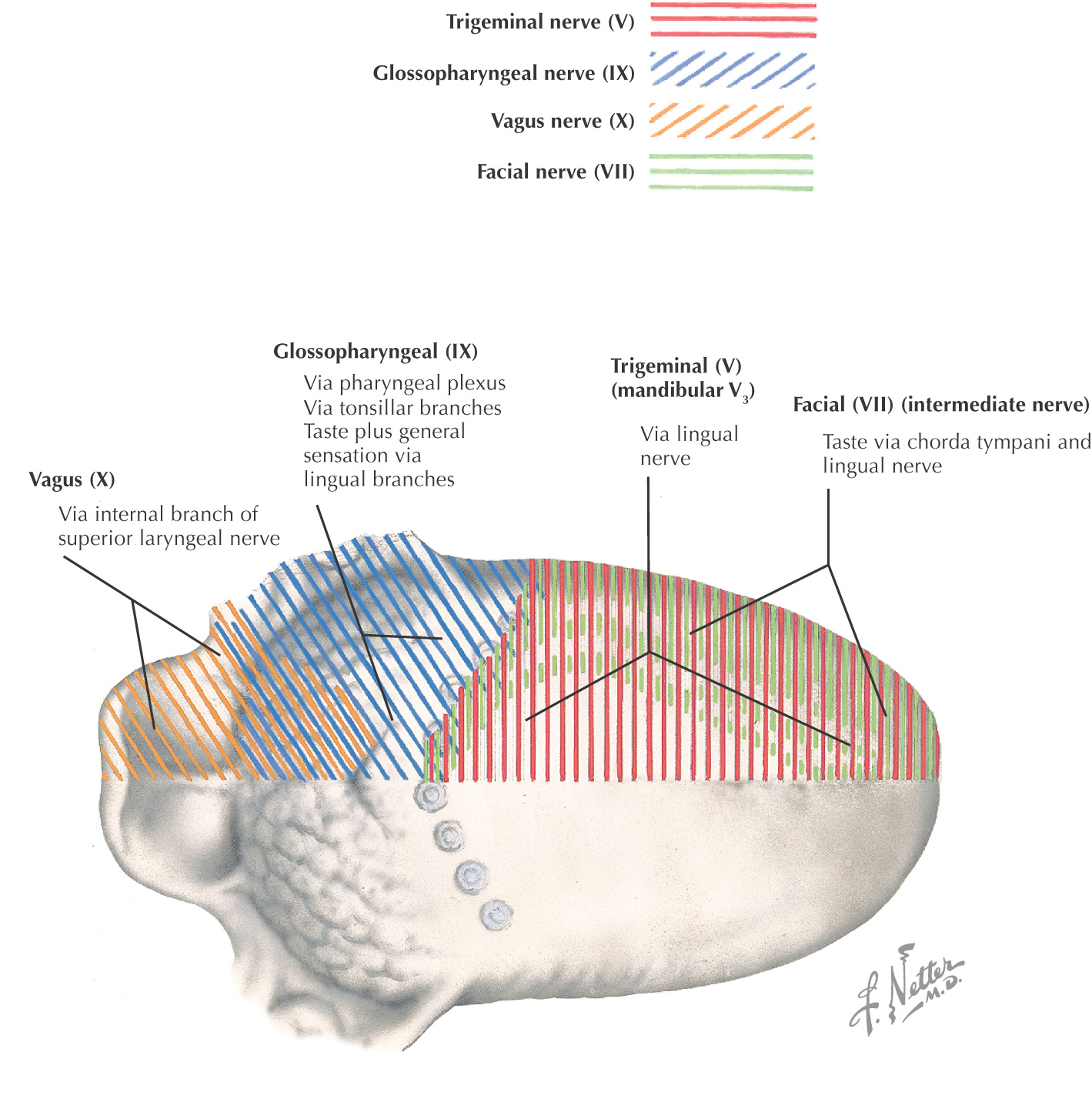
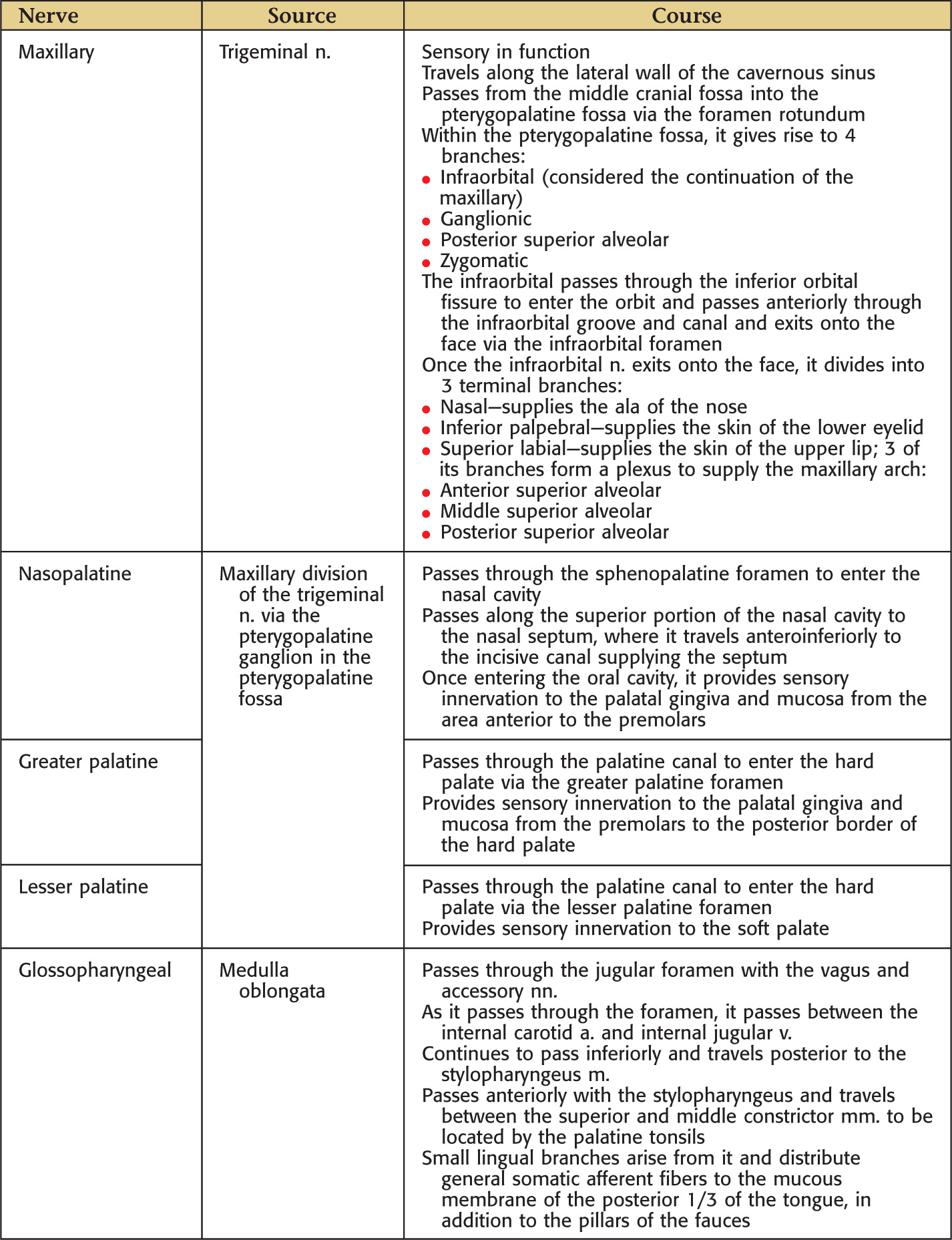
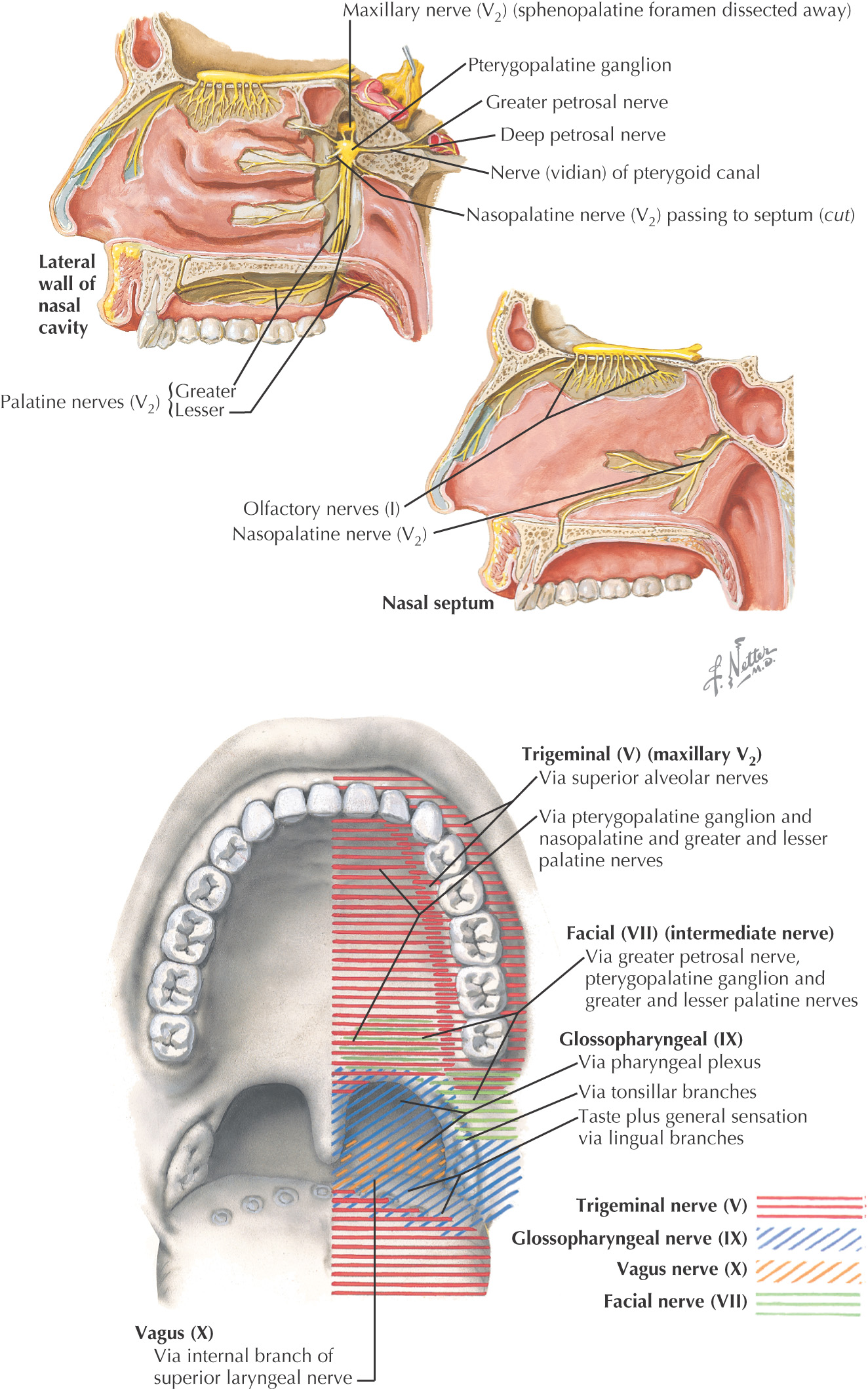
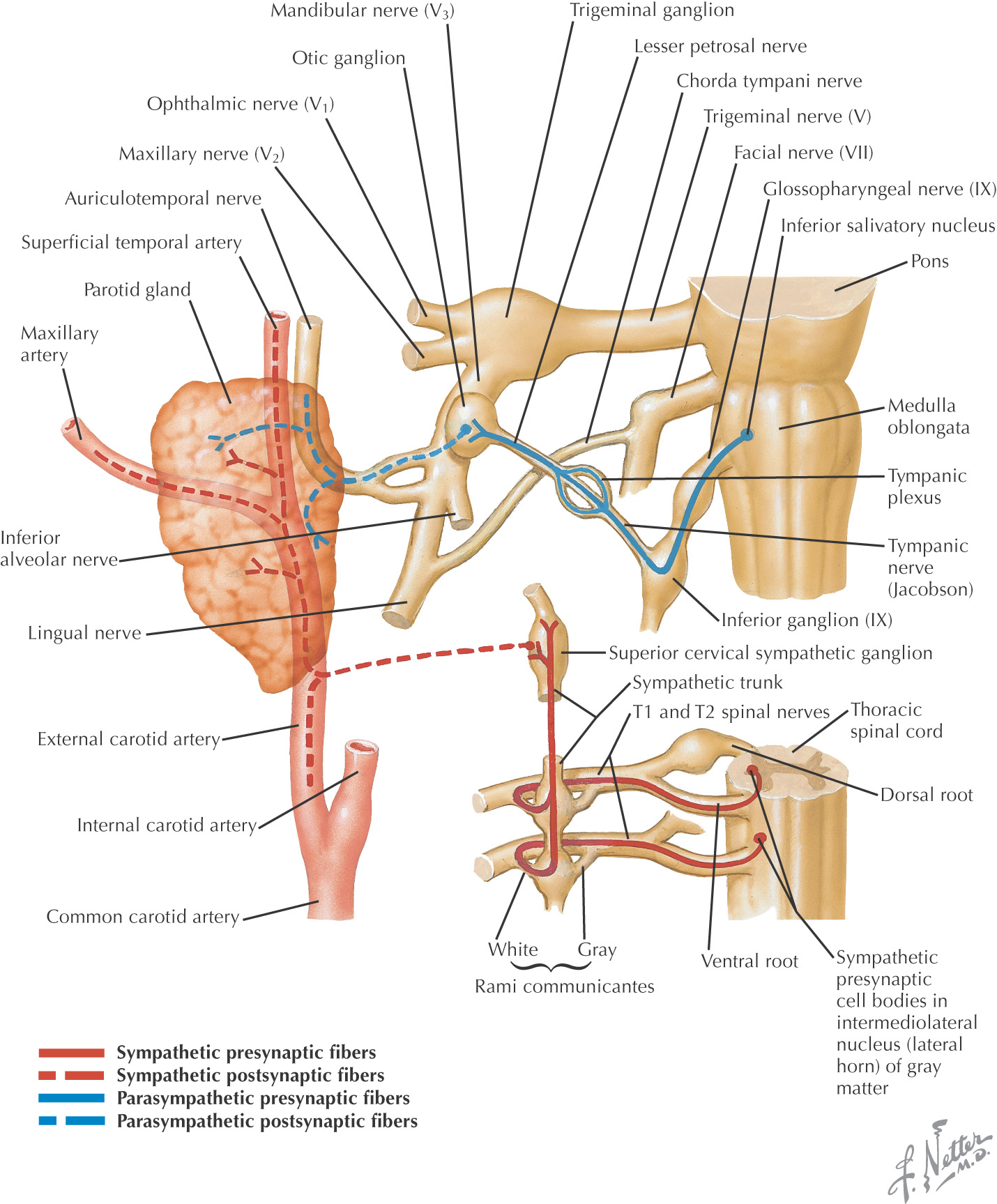
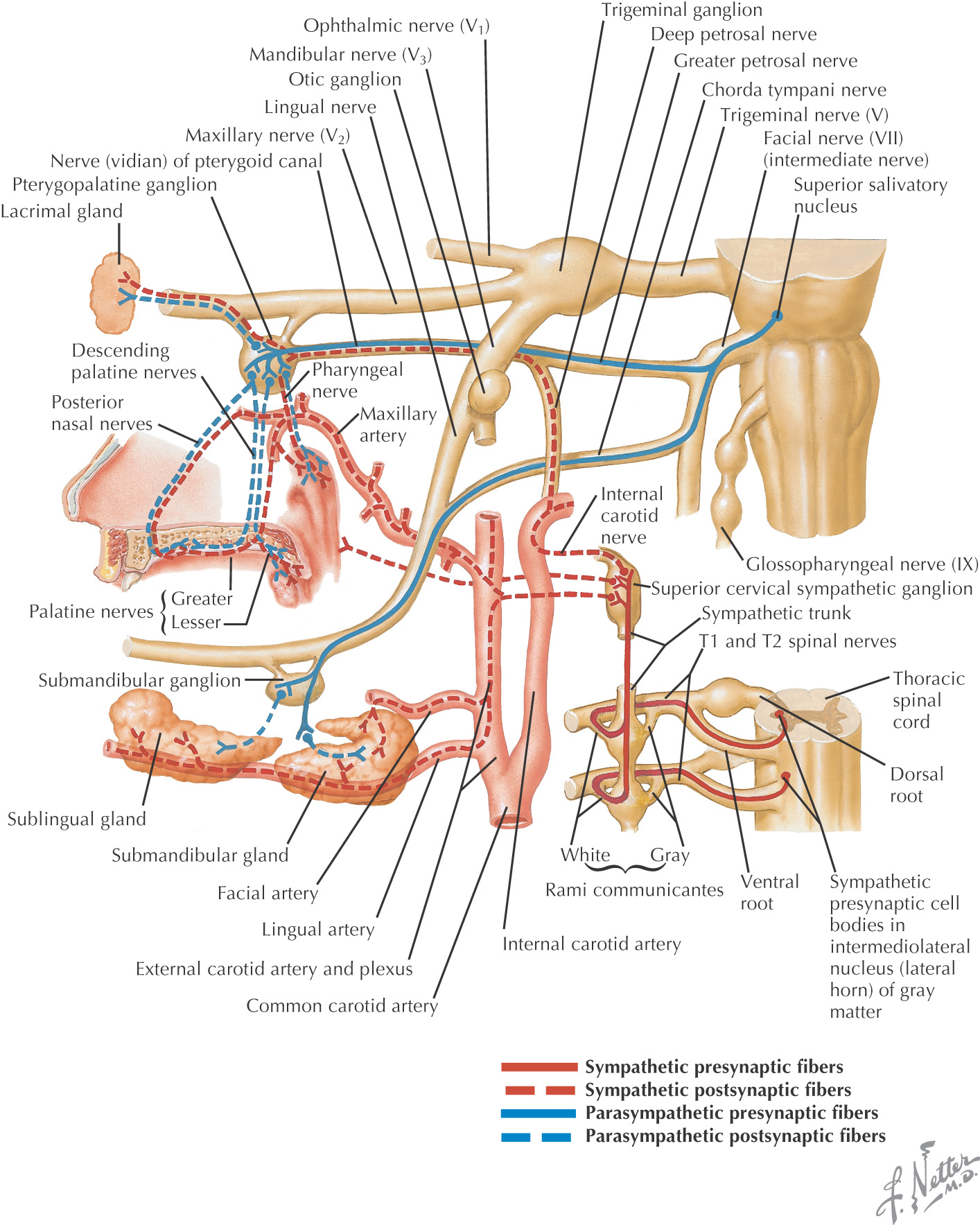
Nerve Supply of the Oral Cavity
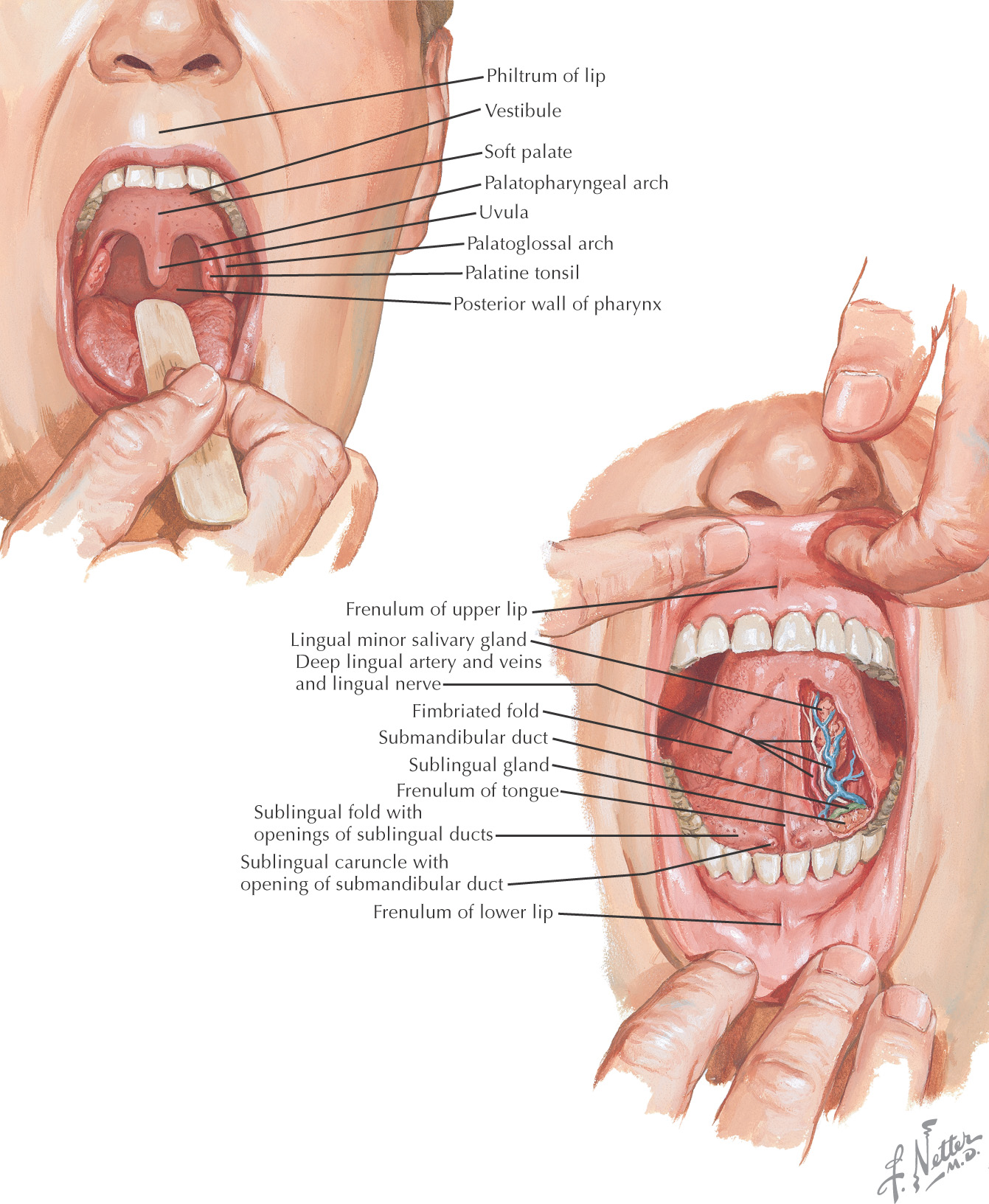
Oral cavity: the space located between the lips and cheeks on the external surface to the palatoglossal fold on the internal surface
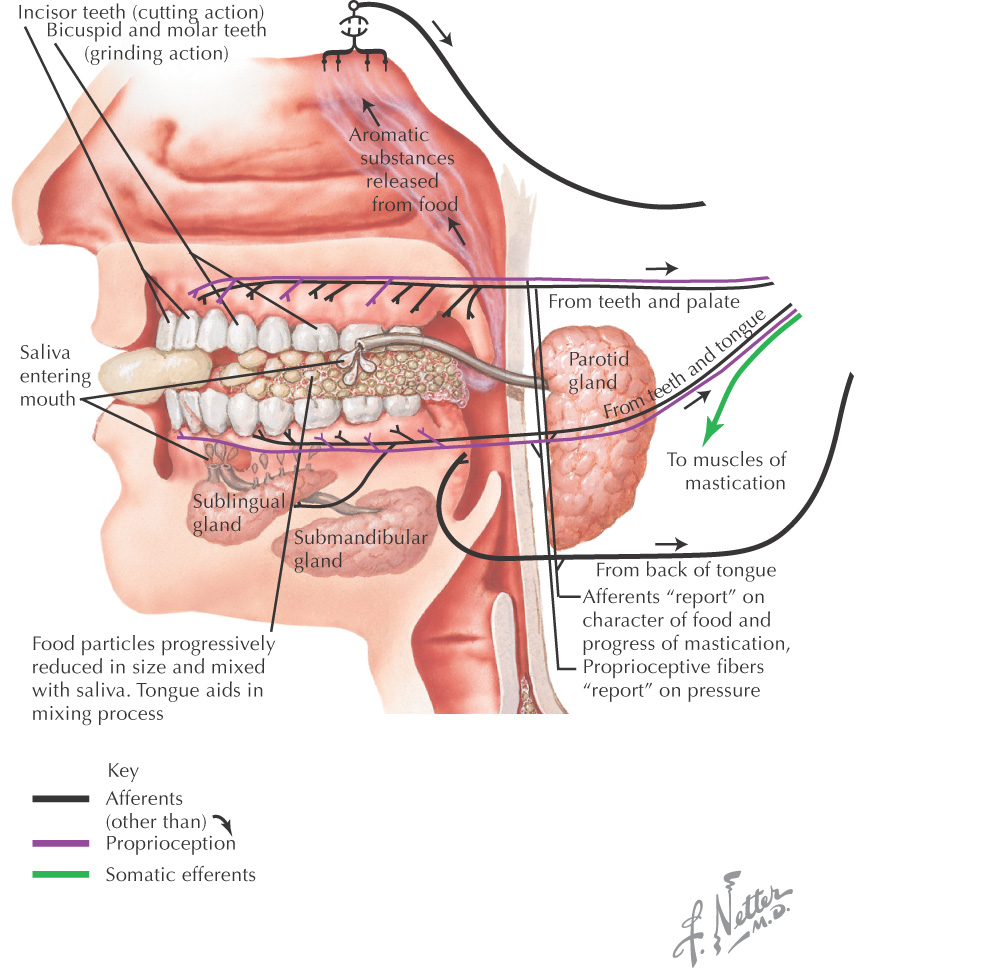
The oral cavity is important in mastication, tasting, and talking
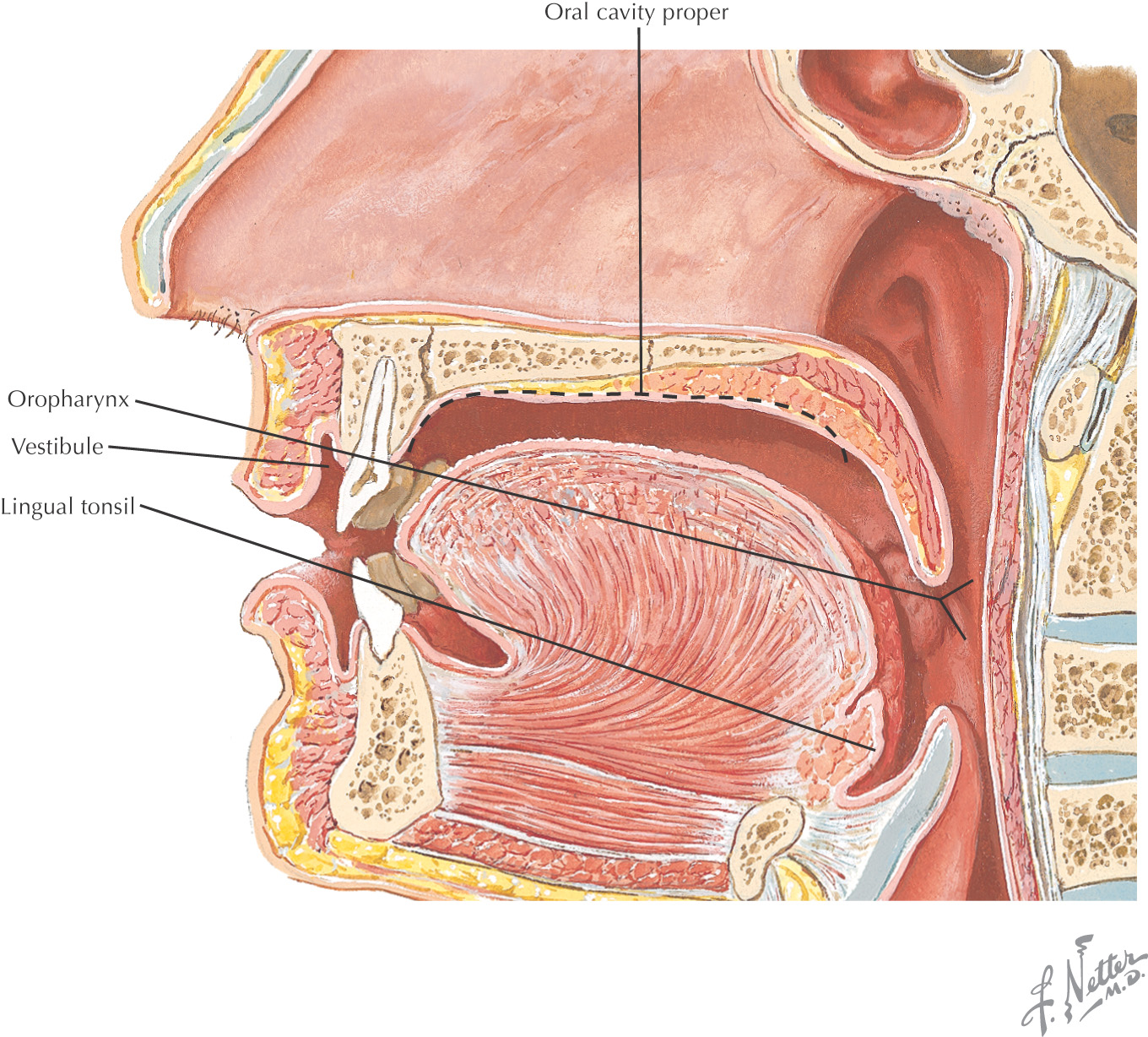
The area of the oral cavity can be divided into:
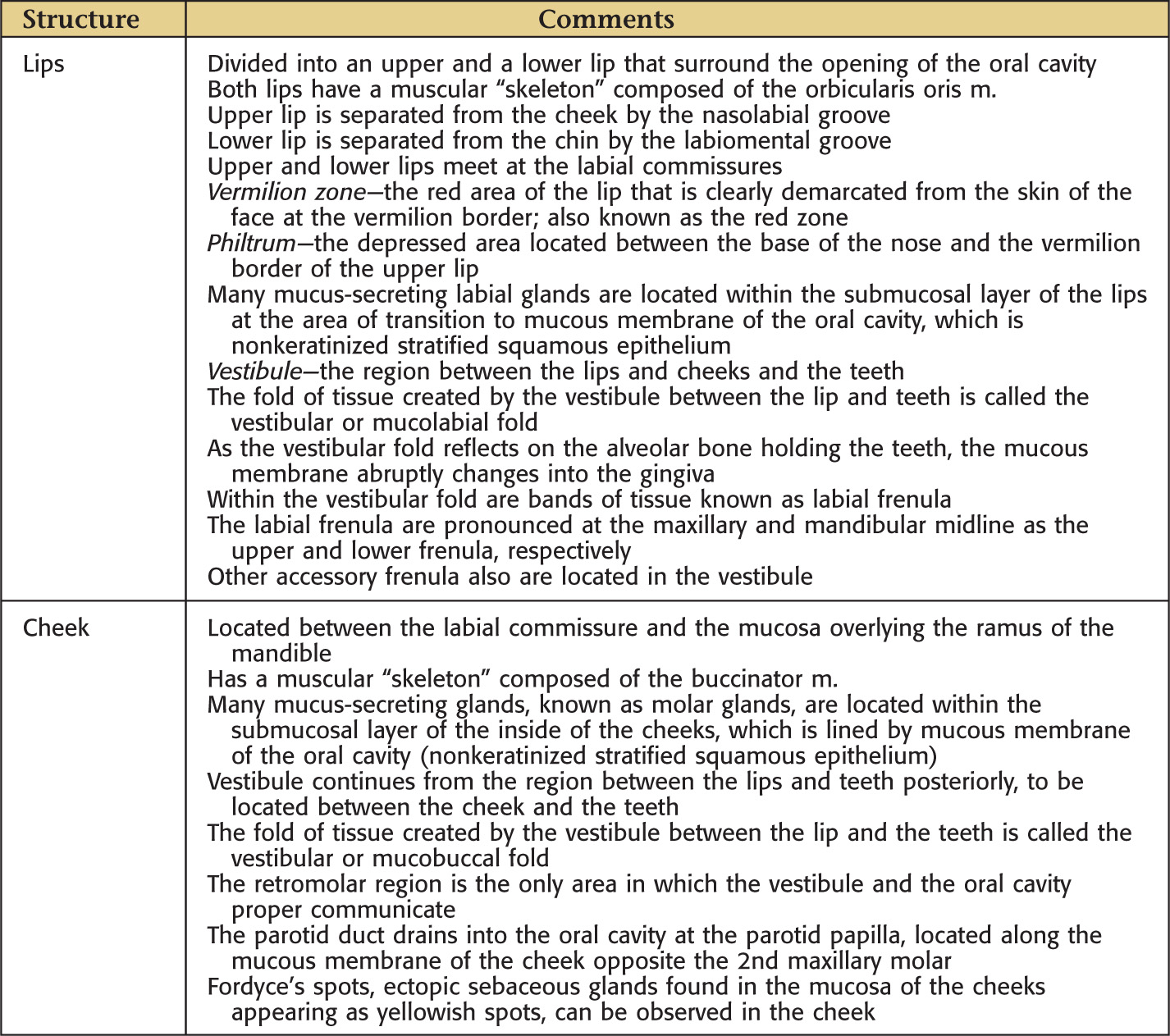
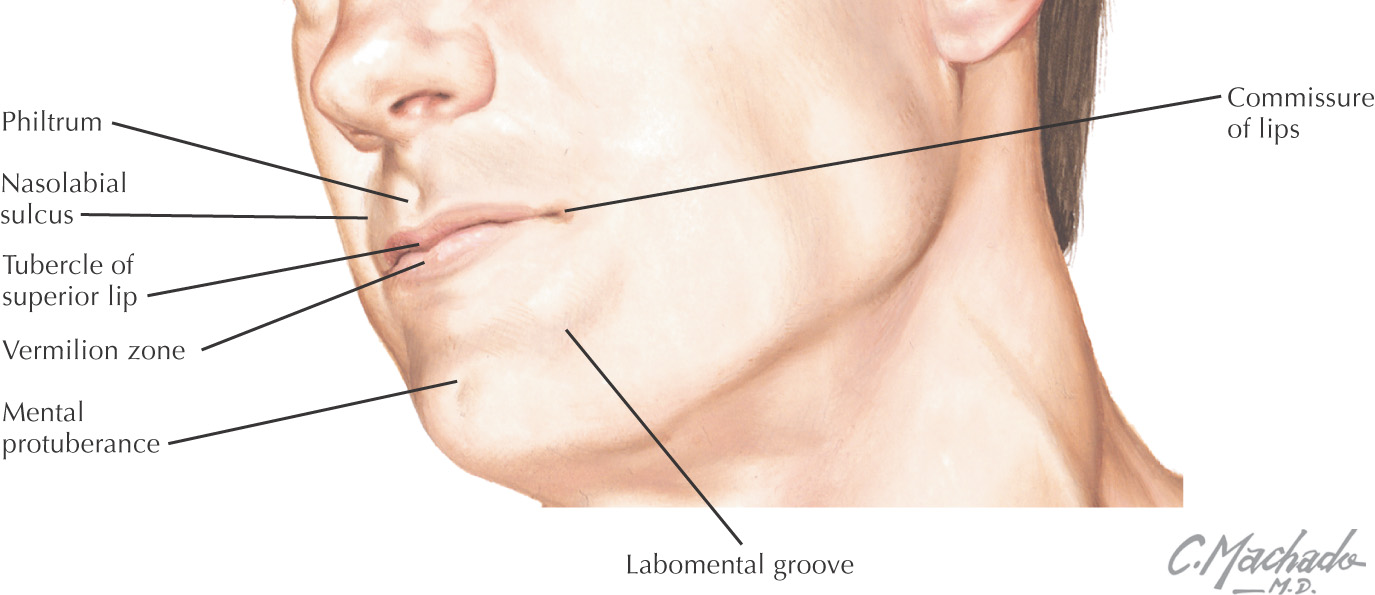
• Vestibule—the area between the teeth and lips or cheek
• Oral cavity proper—the area located internal to the teeth
Posteriorly, the oral cavity is continuous with the oropharynx
The hard palate and the soft palate are important boundaries within the oral cavity
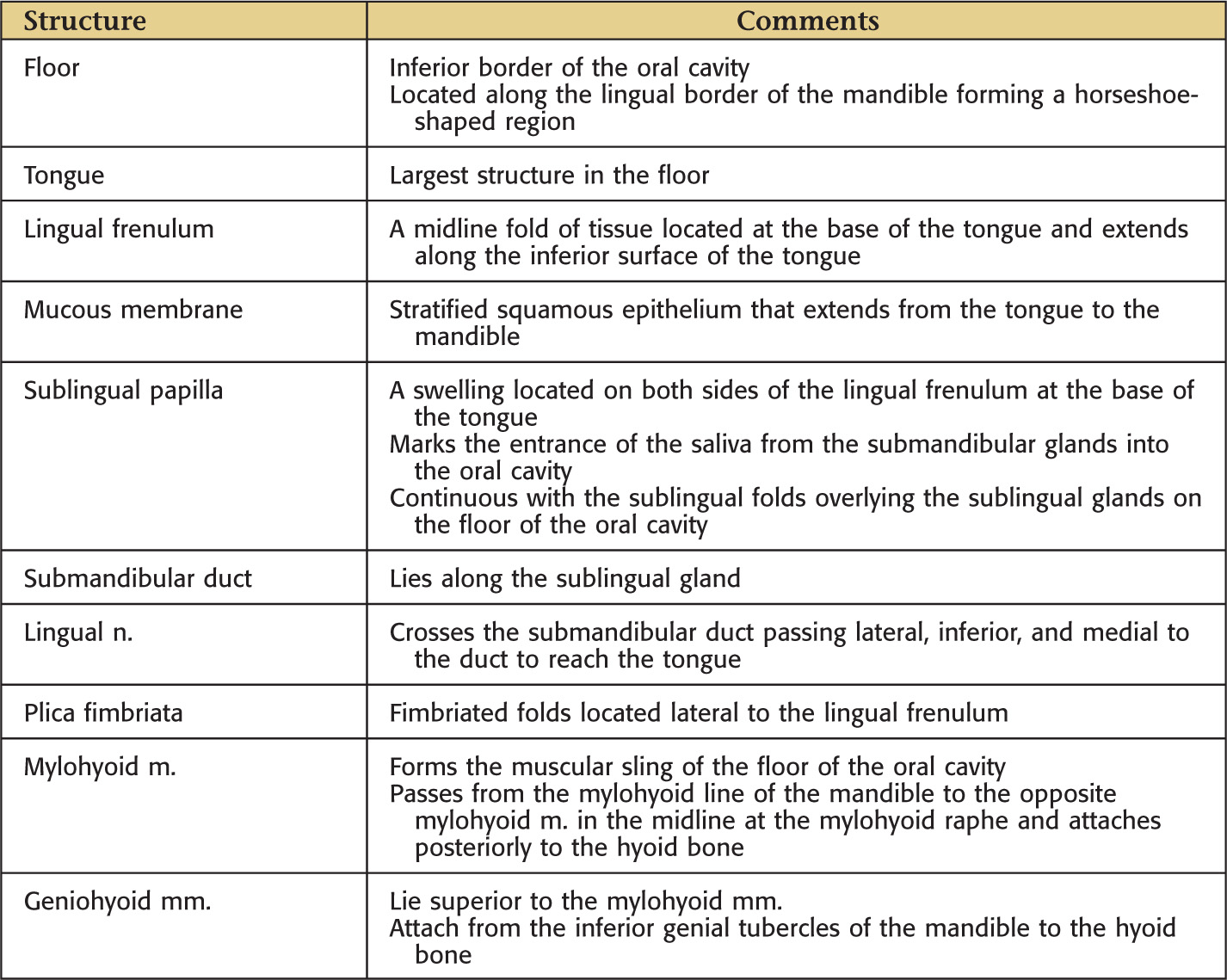
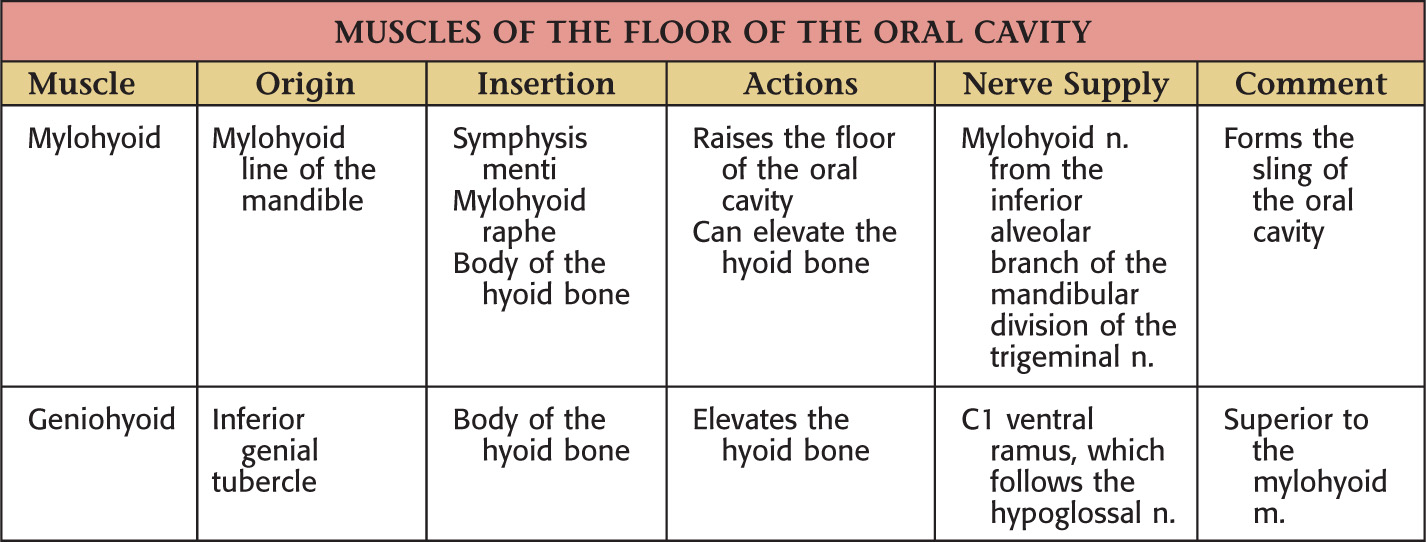
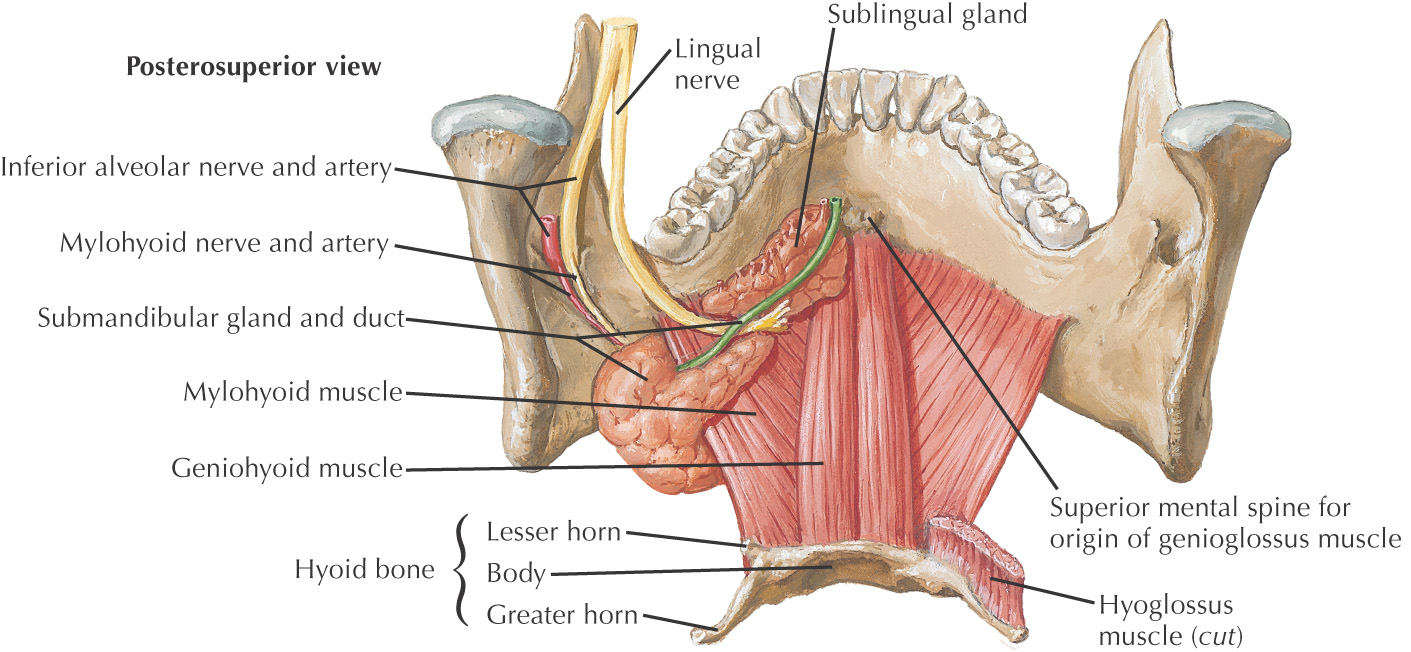
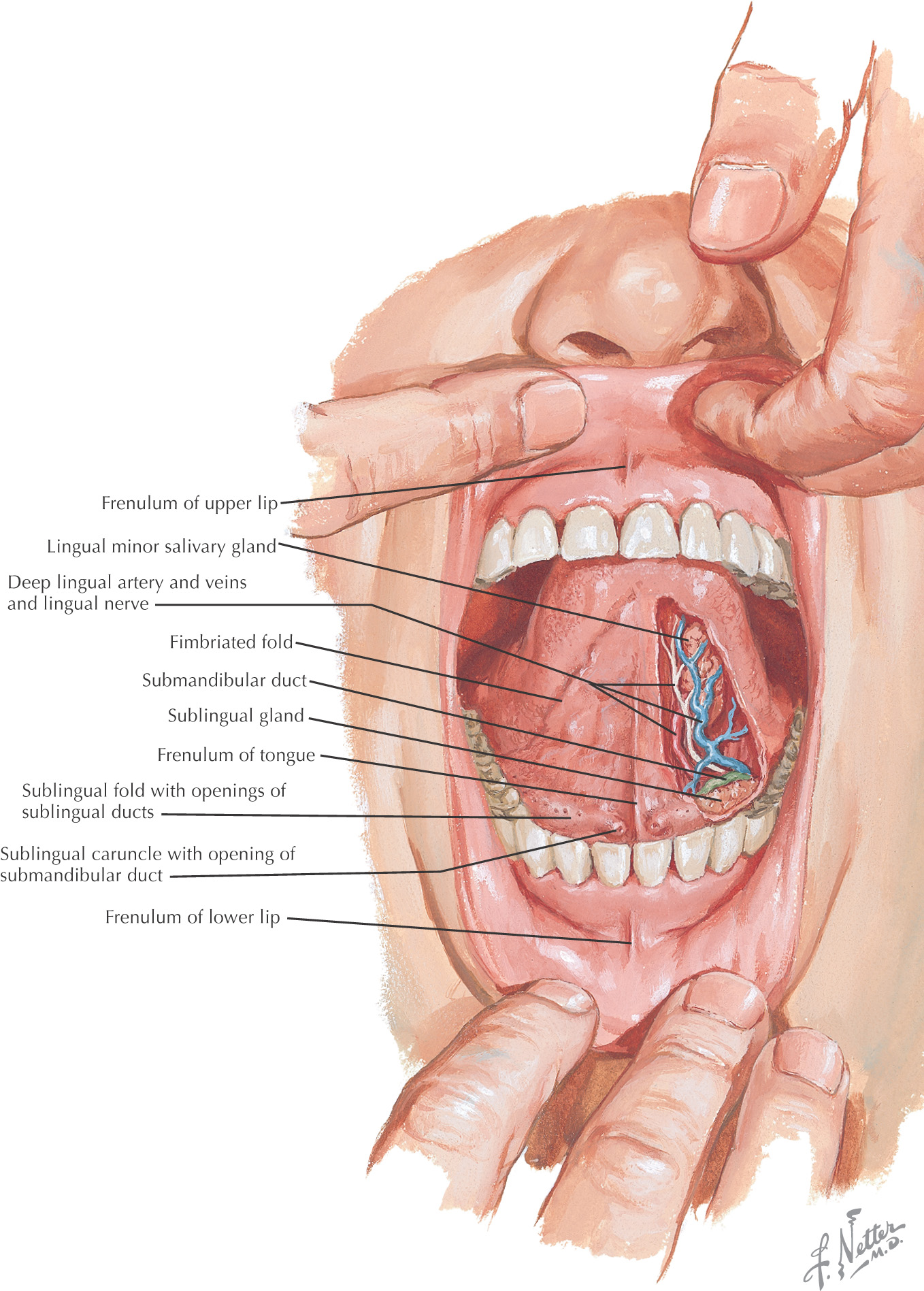
The tongue is a major structure located on the oral cavity floor
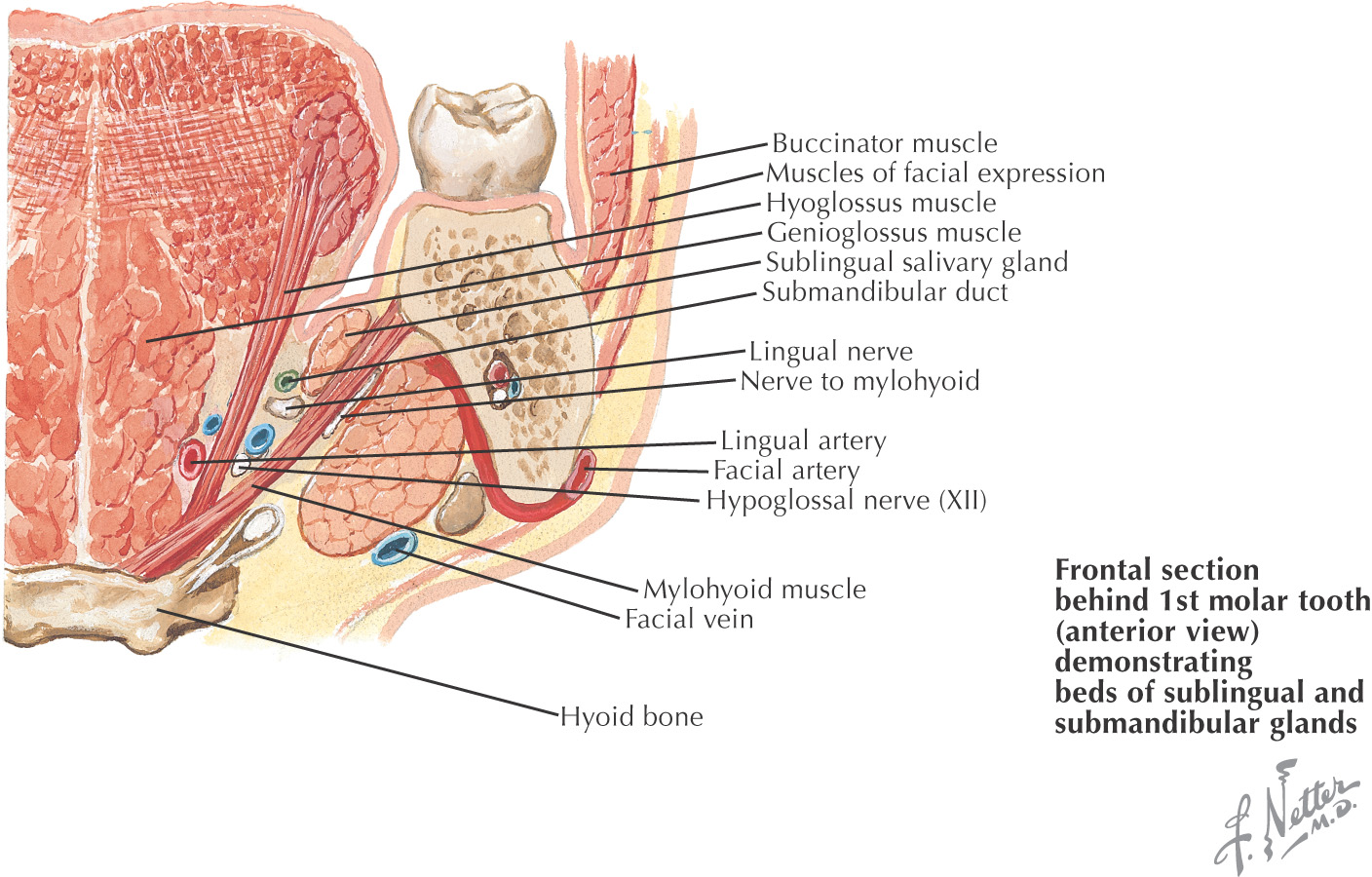
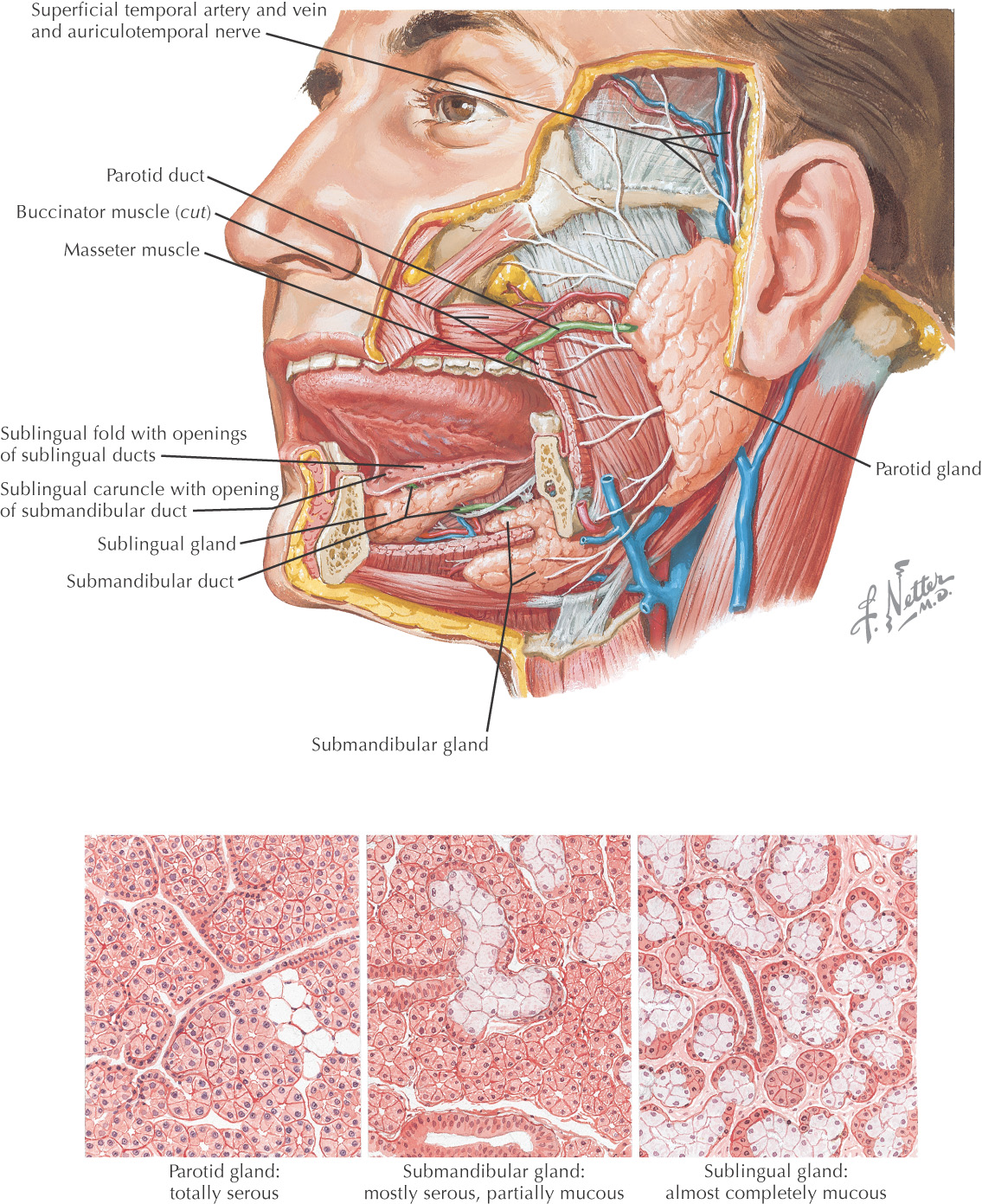
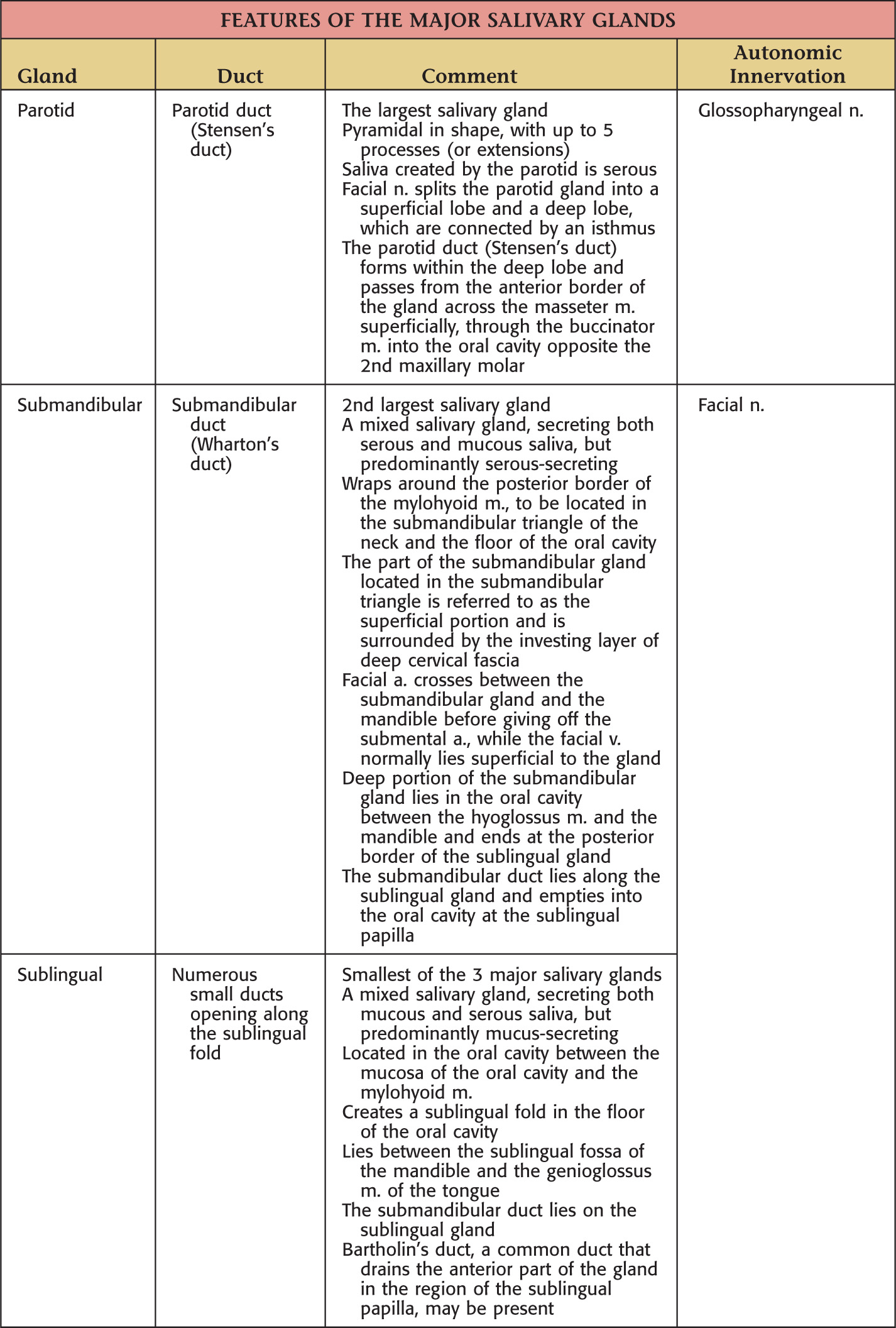
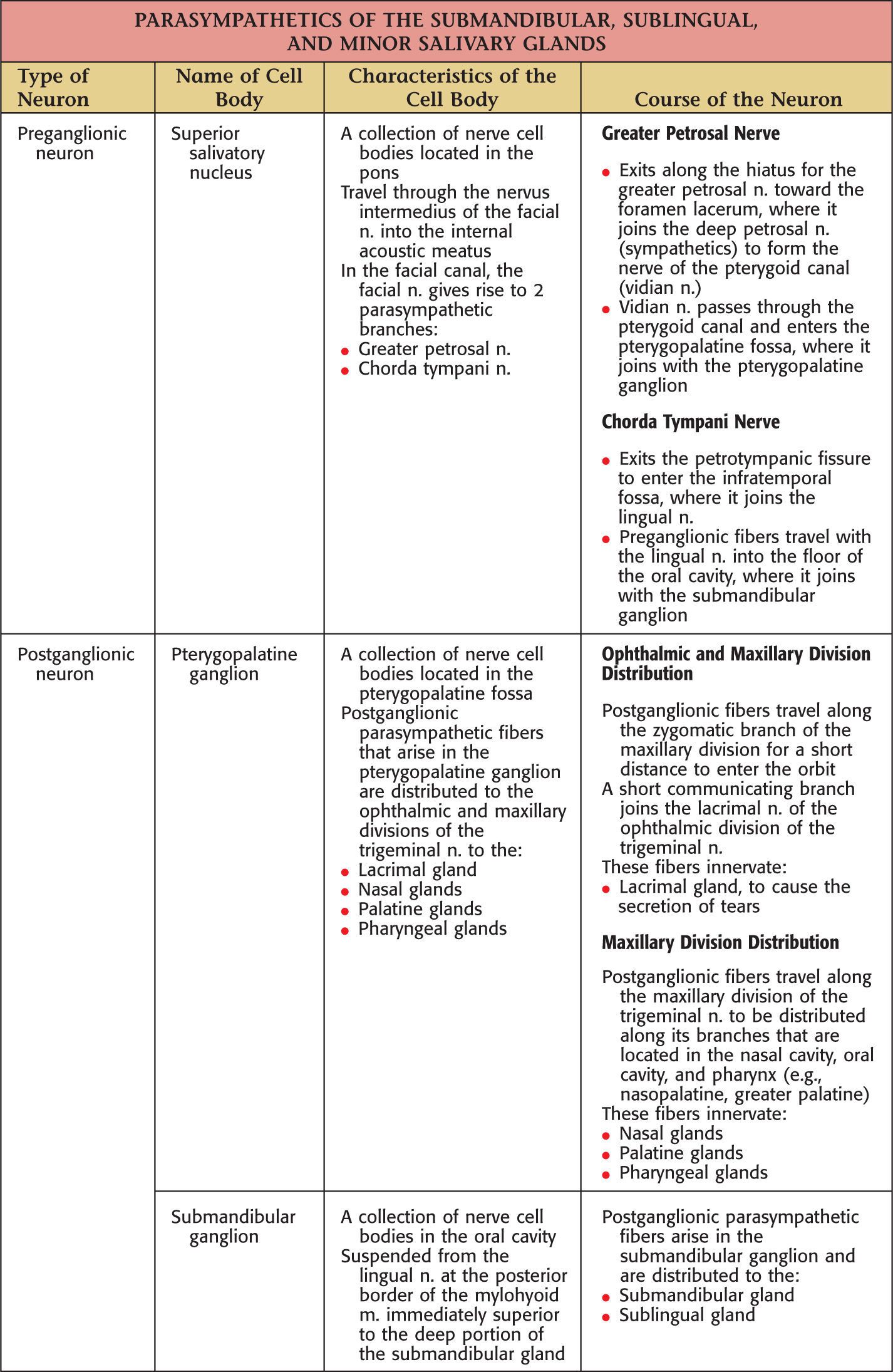
All of the major salivary glands—parotid, submandibular, and sublingual—drain into the oral cavity
Boundary |
Structure |
Superior |
The roof is the hard palate |
Posterosuperior |
Soft palate |
Lateral |
Cheeks |
Inferior |
The floor is located along the lingual border of the mandible forming a horseshoe-shaped region |
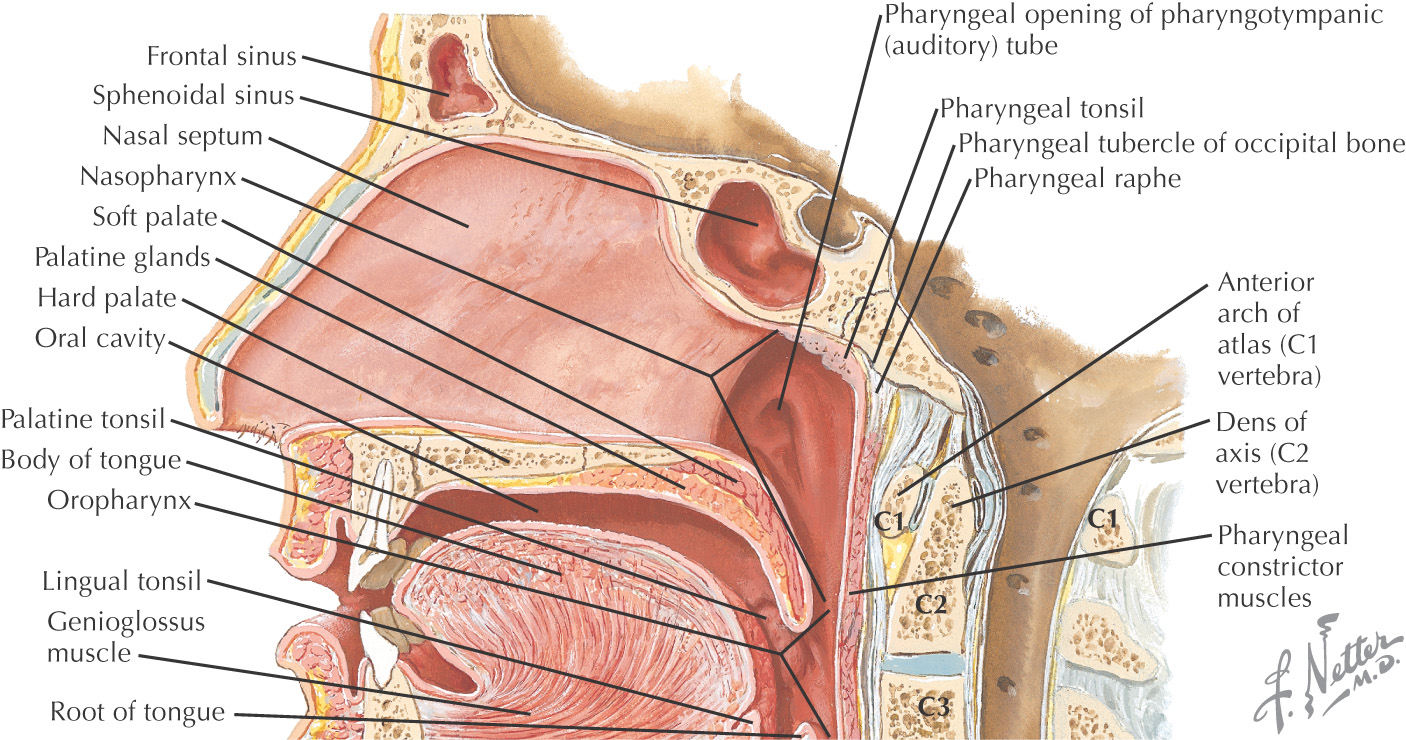
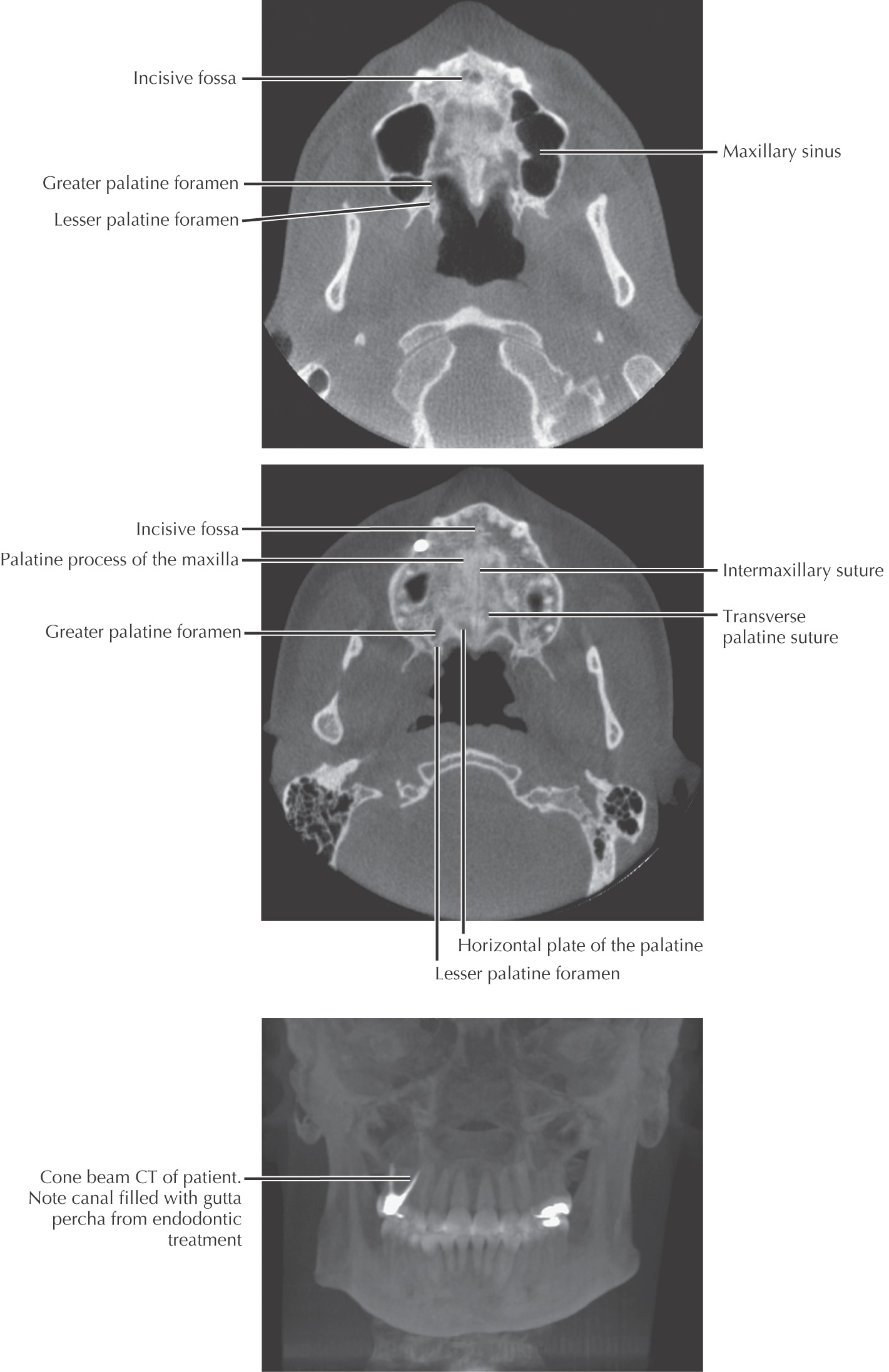
The superior border (or roof) of the oral cavity is the hard palate, comprising the anterior 2/3 of the entire palate
Separates the oral cavity from the nasal cavity
Composed of:
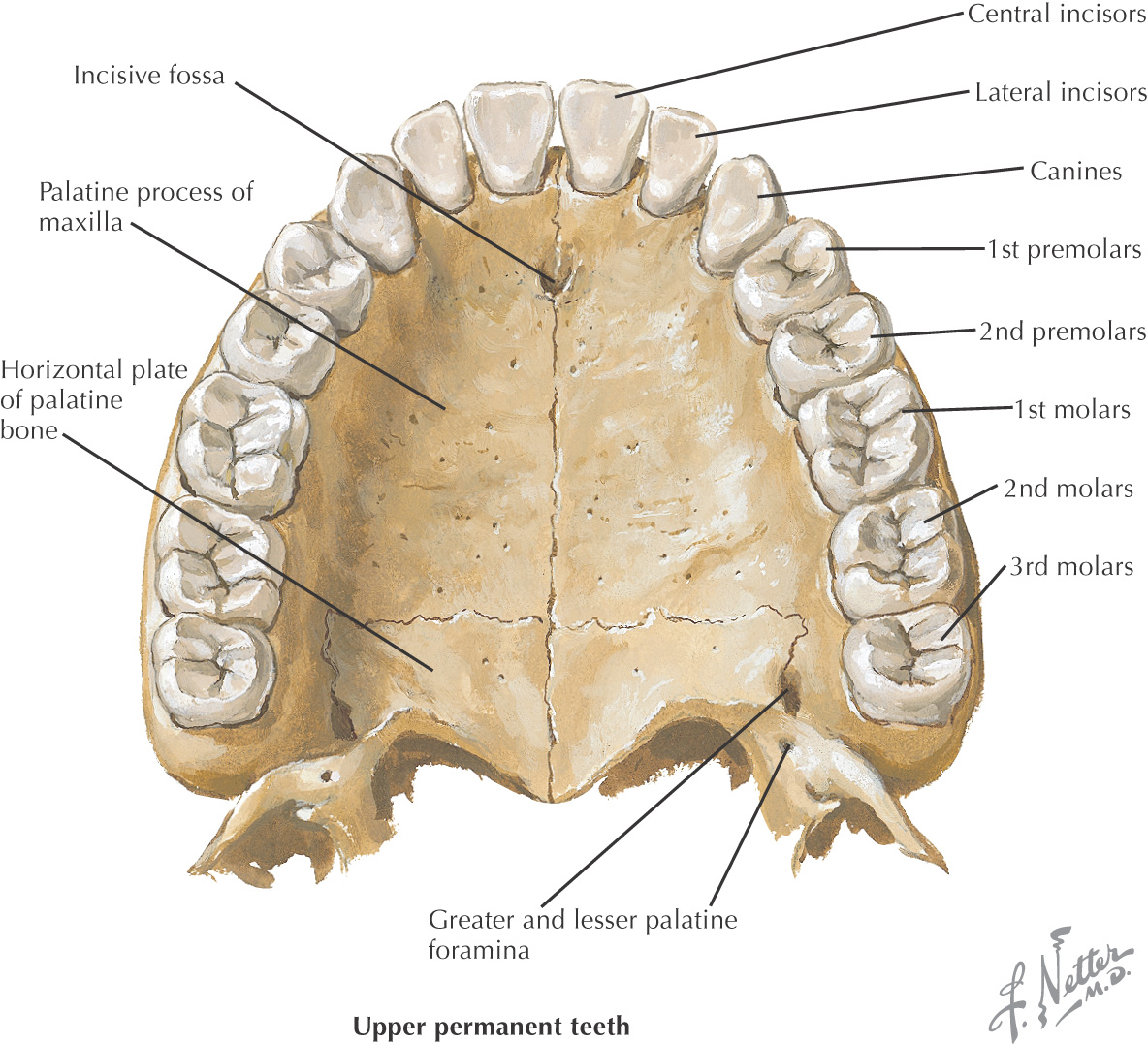
• Palatal process of the maxilla
• Horizontal process of the palatine
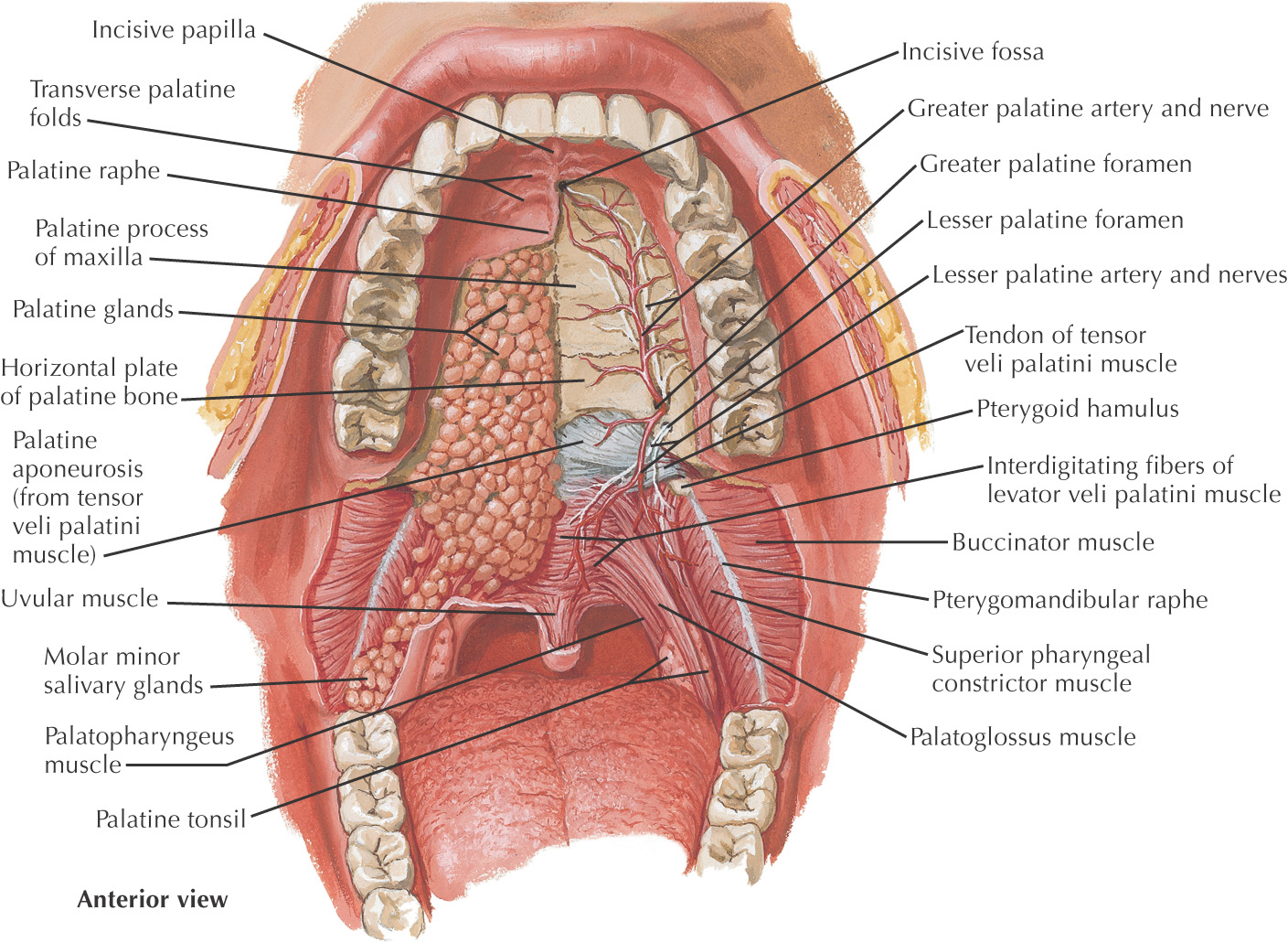
In the anterior midline, an incisive foramen is located on the right and left sides that transmits the terminal branches of the nasopalatine nerve and sphenopalatine vessels
In the posterolateral region of the hard palate, the greater and lesser palatine foramina are located on the right and left sides; these openings transmit the greater and lesser palatine nn. and vessels
The bones of the hard palate are covered by a thick mucous membrane
The mucous membrane has a small elevation in the anterior midline called the incisive papilla that overlies the incisive foramen
Moving posteriorly from the incisive papilla, the mucous membrane has a thick midline palatal raphe
Lateral transverse ridges called transverse rugae (plicae) are located along the mucous membrane of the hard palate
Deep to the mucous membrane of the hard palate are numerous mucus-secreting glands called palatal glands
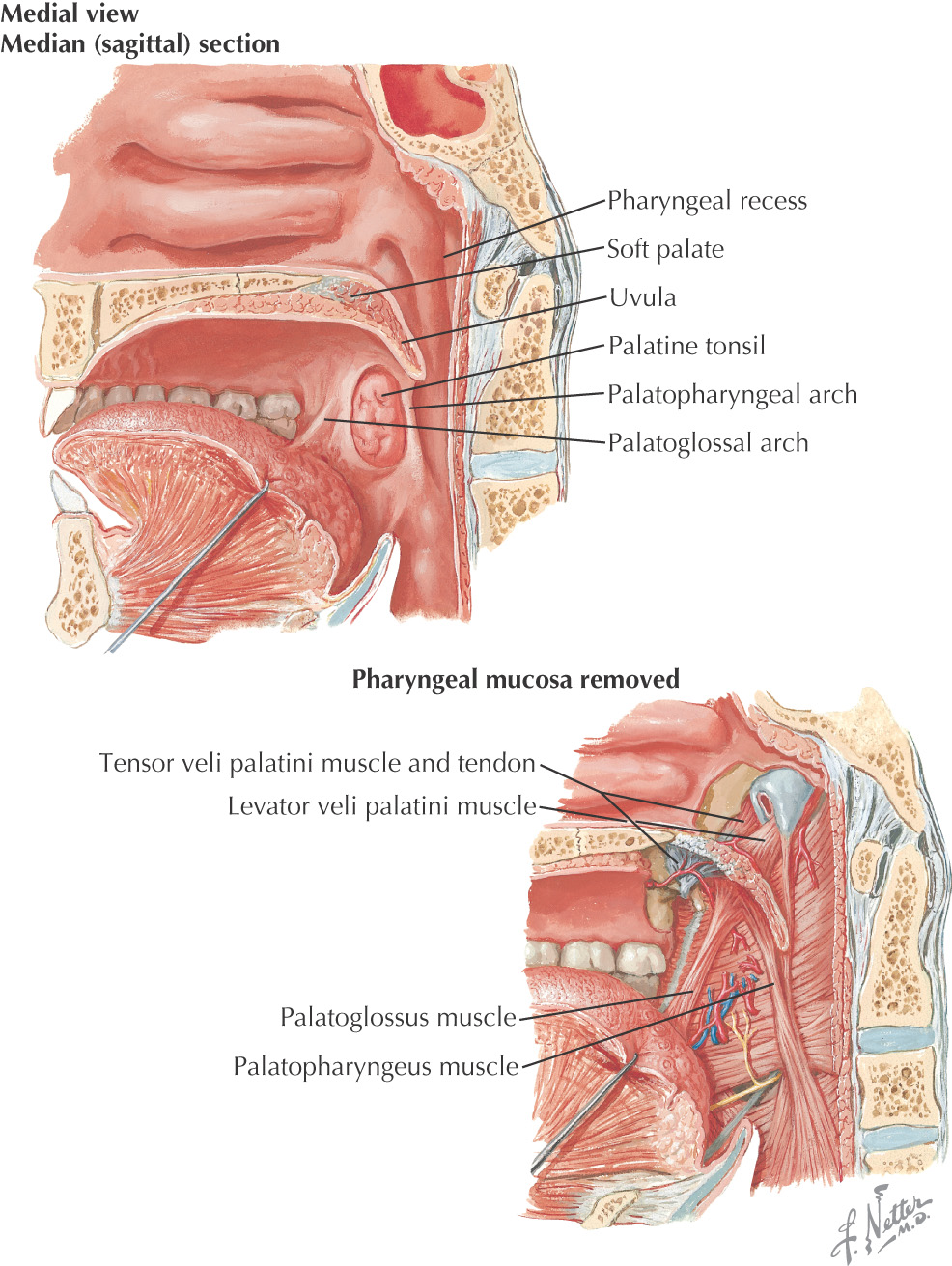
The posterosuperior border of the oral cavity is the soft palate
The soft palate is the continuation of the palate posteriorly and makes up approximately 1/3 of the entire palate
The soft palate separates the oral cavity from the nasopharynx
An abundance of mucus-secreting palatal glands, which are continuous with the hard palate, are located in the soft palate
The soft palate has 3 margins:
• Anteriorly, it is continuous with the hard palate at the vibrating line
• Posterolaterally, it forms the superior portion of the palatoglossal and palatopharyngeal folds
• Posteriorly, the uvula hangs in the center of the posterior free margin
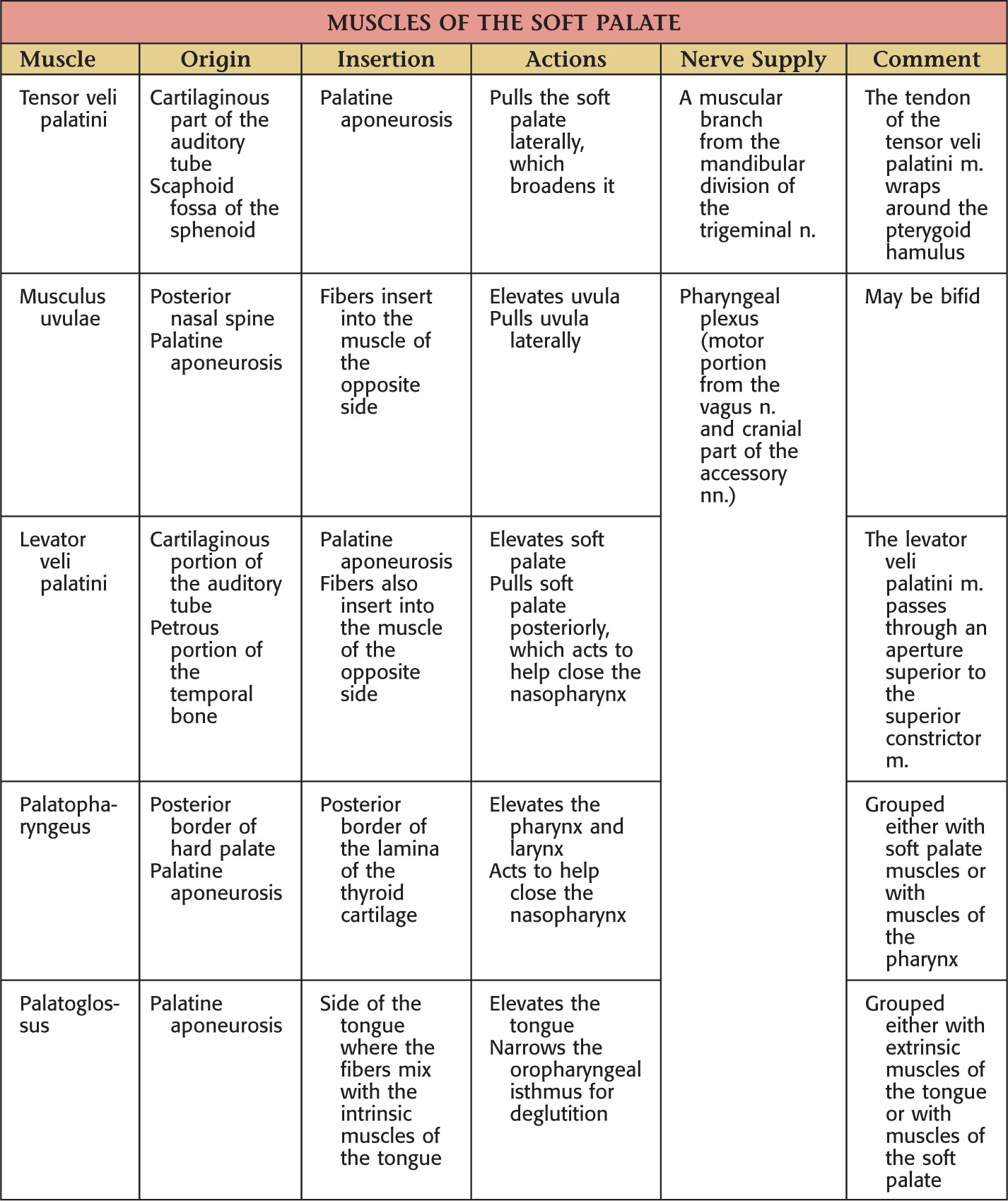
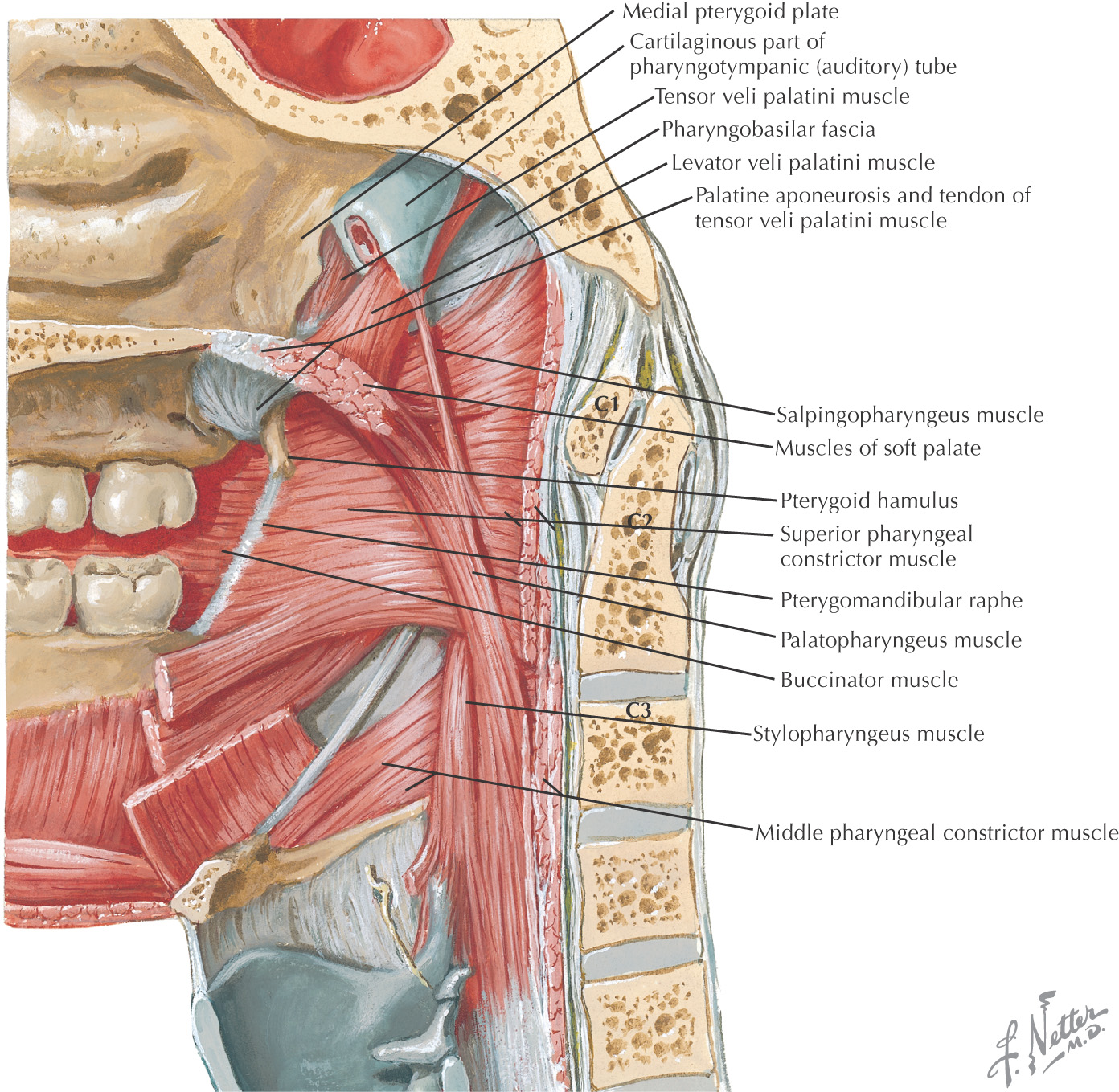
The thick palatine aponeurosis forms the foundation of the soft palate
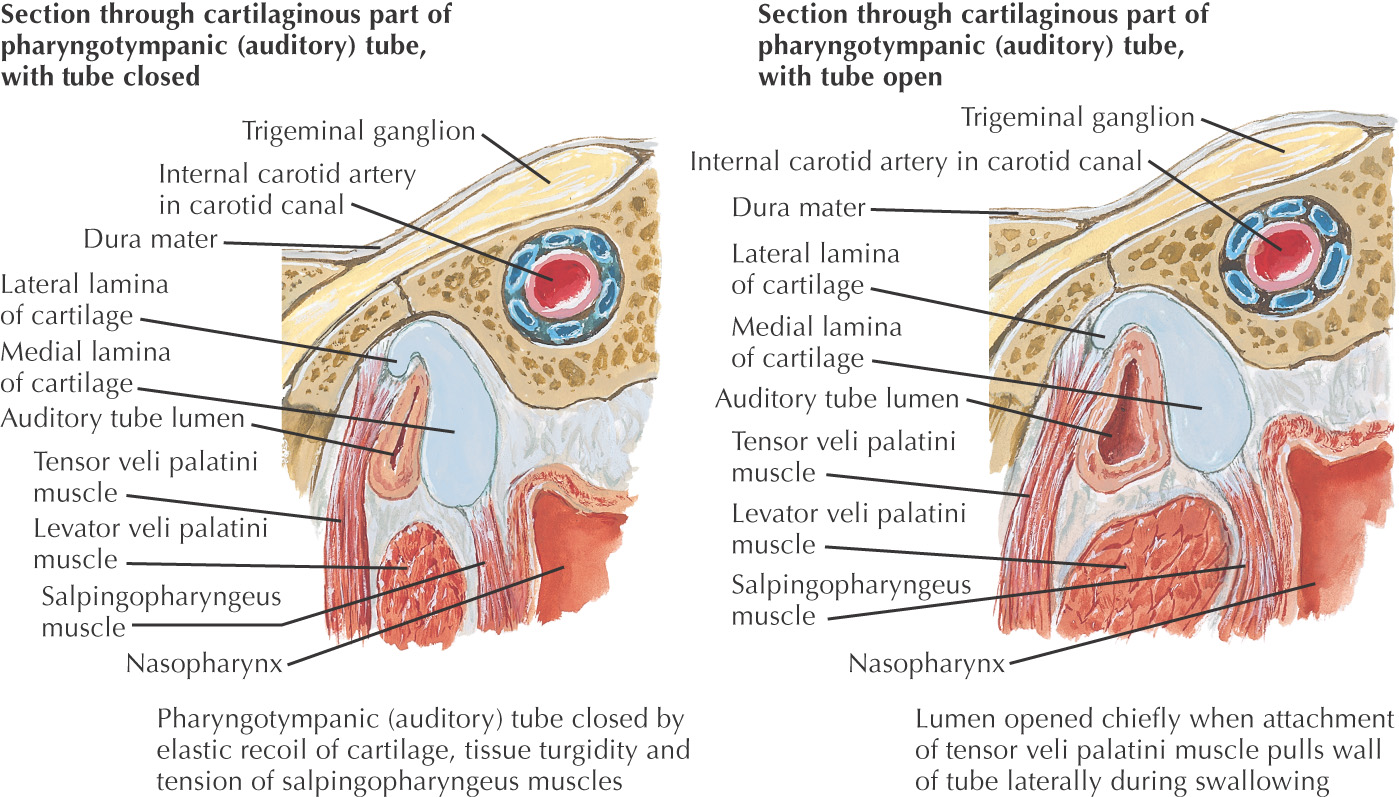
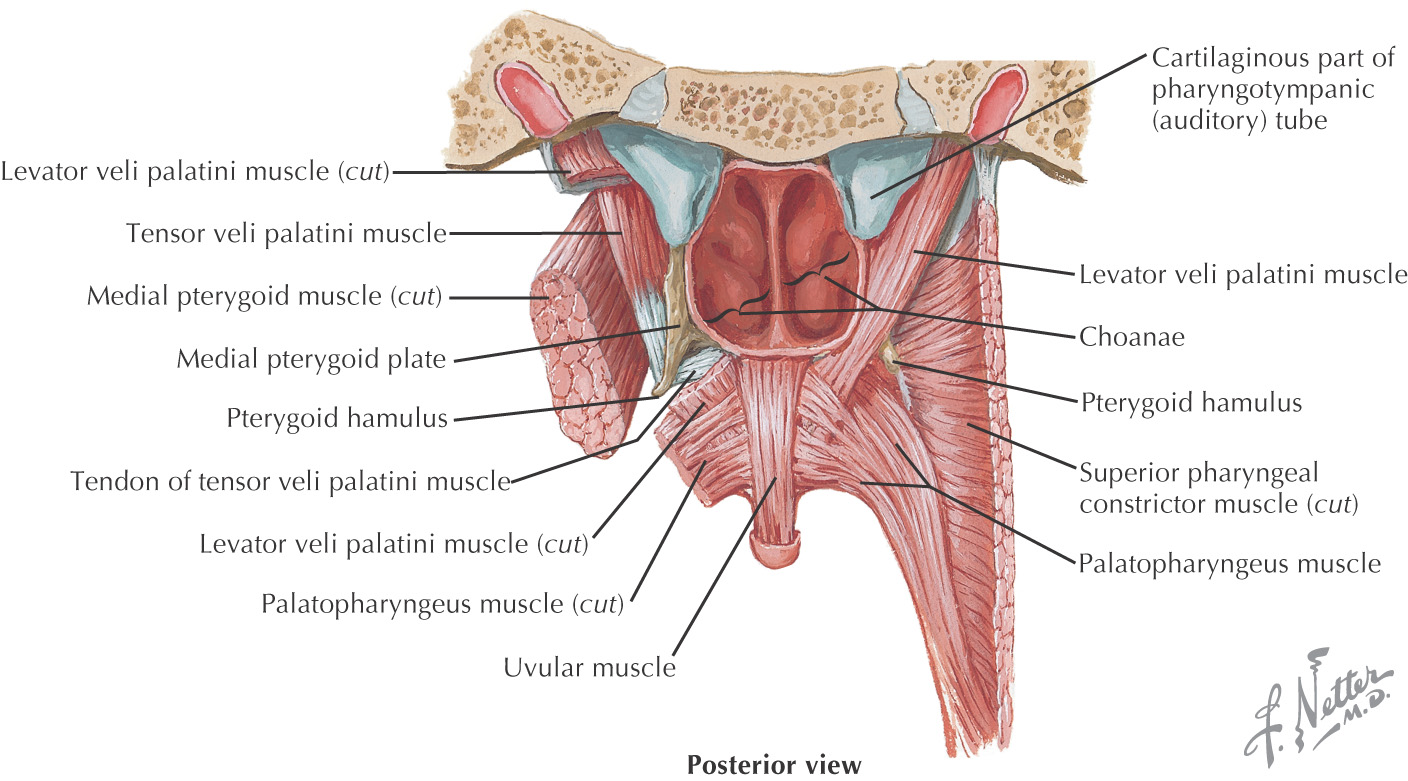
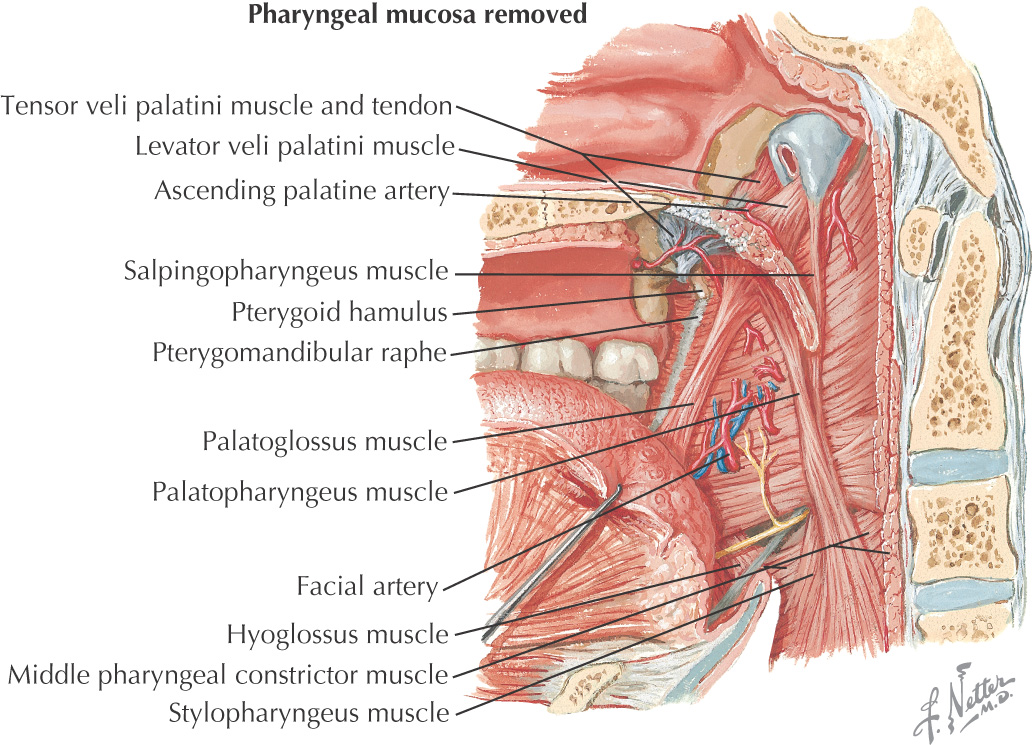
The soft palate is composed of 5 muscles:
• Palatoglossus (sometimes considered in the grouping of tongue muscles)
The soft palate helps close off the nasopharynx during deglutition by forming a seal at the fold of Passavant
The lateral border of the oral cavity extends anteriorly from the labial commissure, posteriorly to the ramus of the mandible
Superior limit of the cheek is the maxillary vestibule; inferior limit is the mandibular vestibule
Mucous membrane of the cheek is stratified squamous epithelium
Fordyce’s spots are ectopic sebaceous glands that may be observed on the inner surface of the cheek
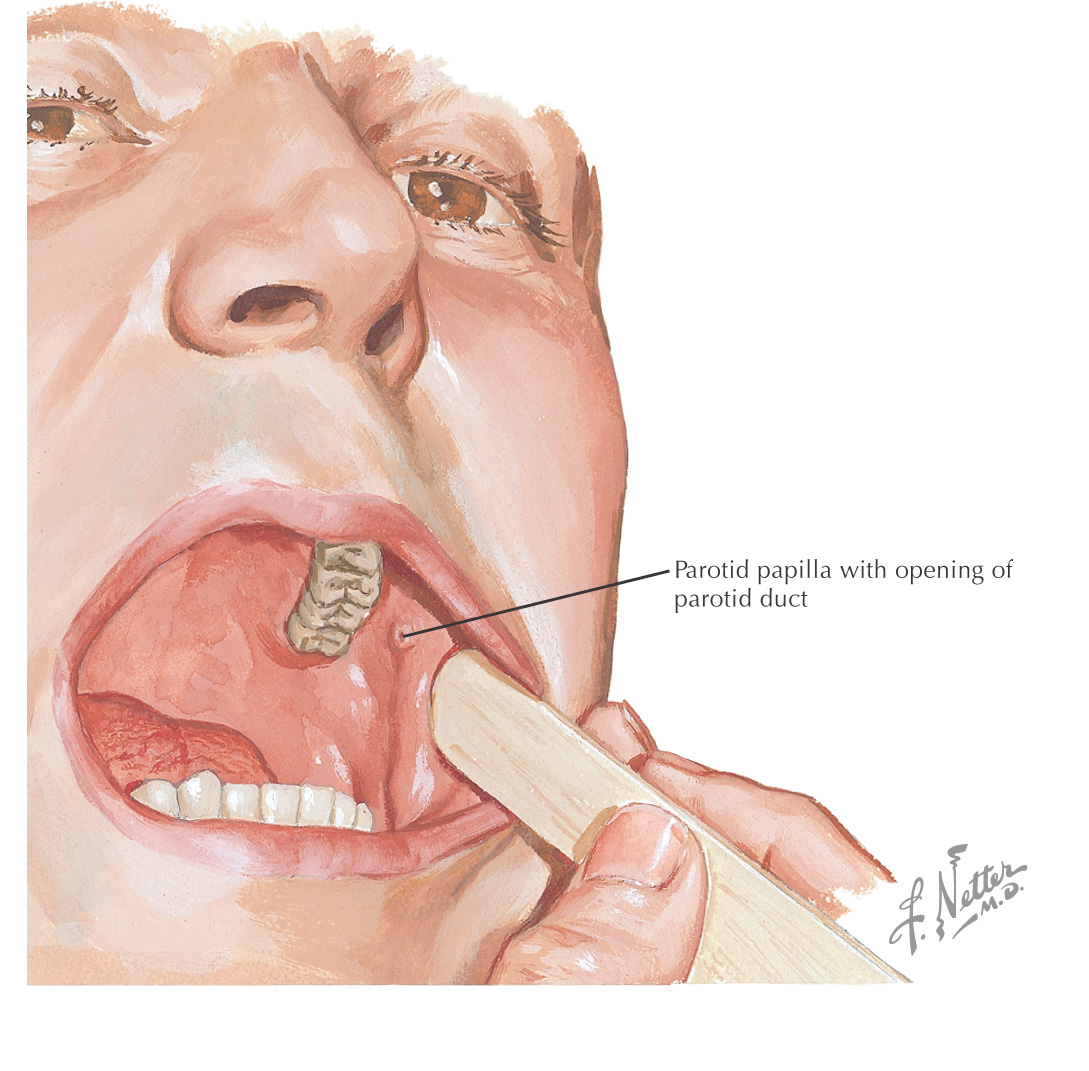
Parotid papilla is located in the cheek opposite the maxillary 2nd molar
Pterygomandibular raphe is located in the posterior portion and serves as a landmark for the pterygomandibular space
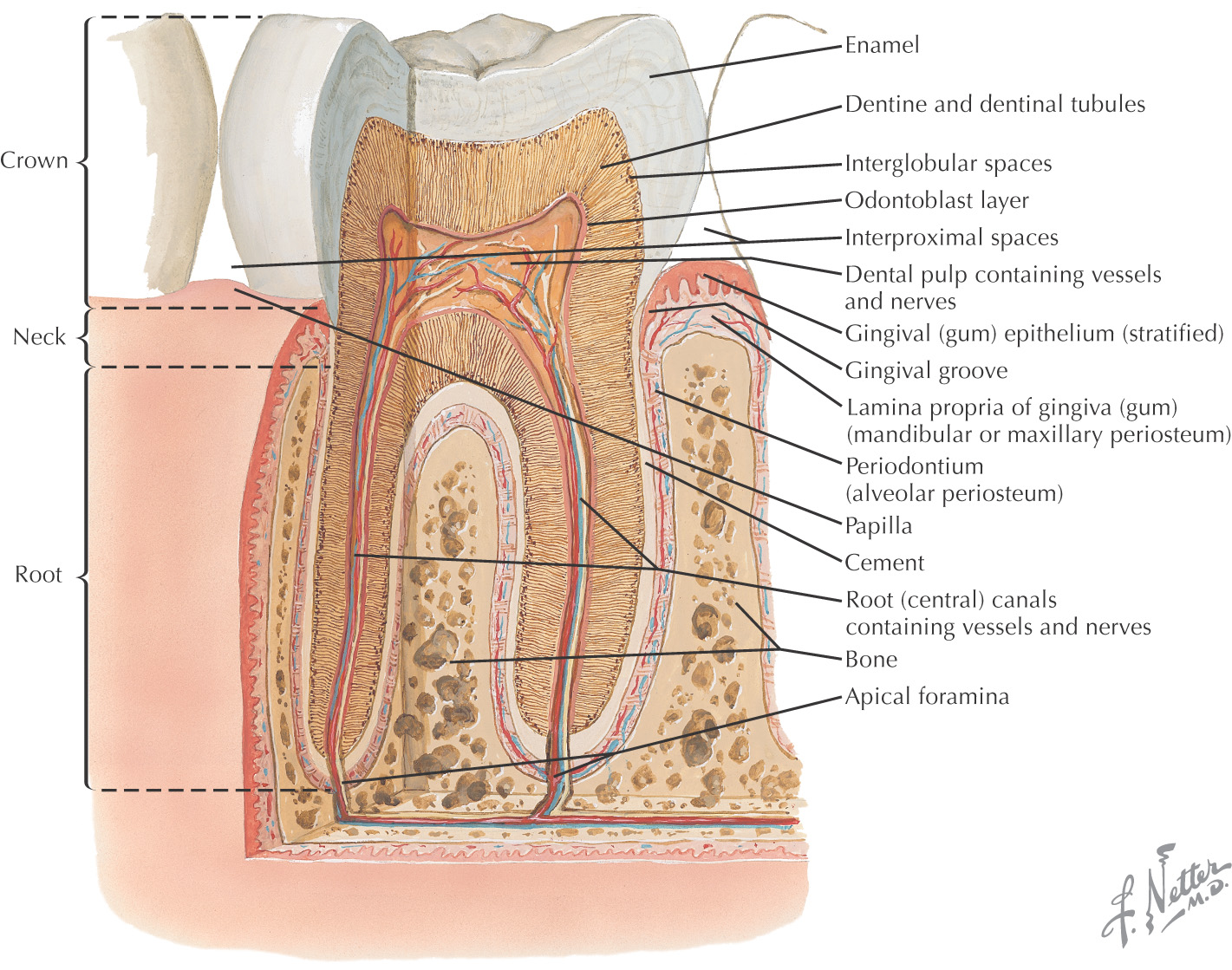
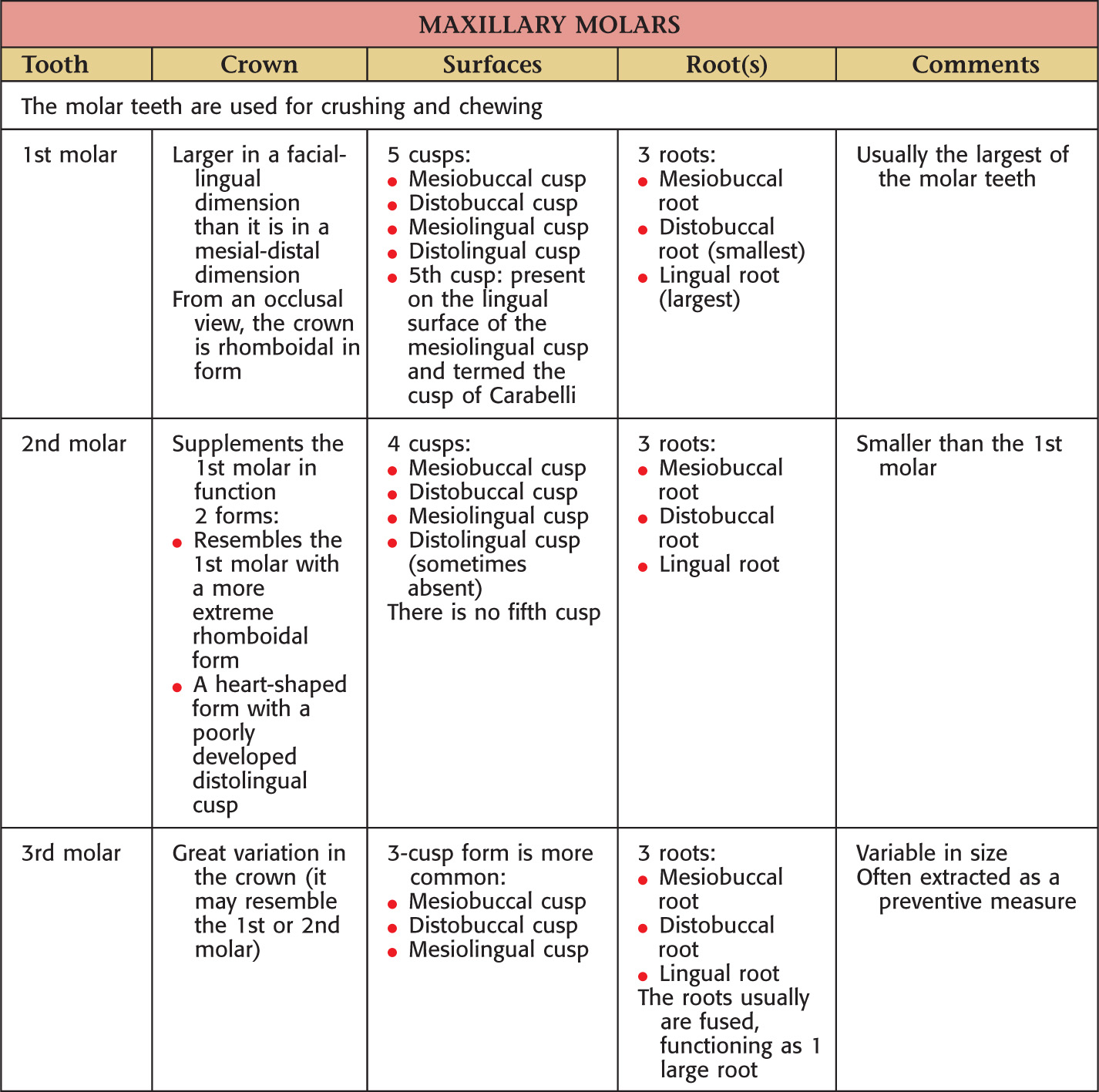
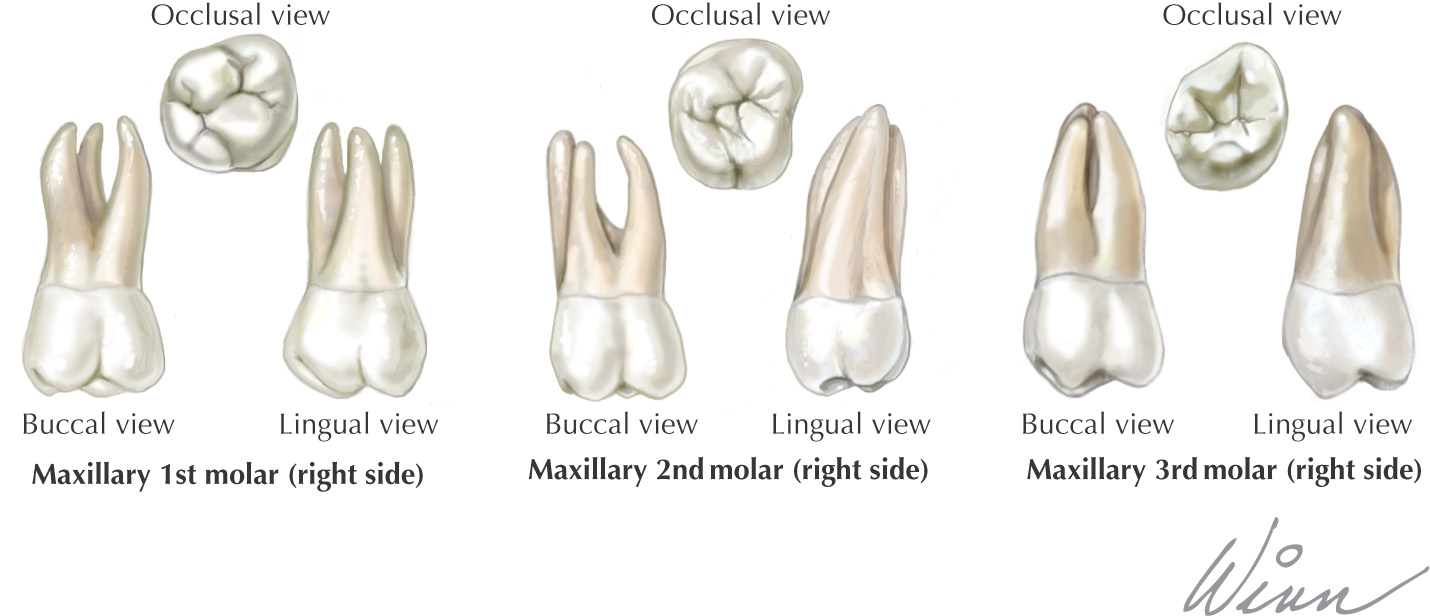
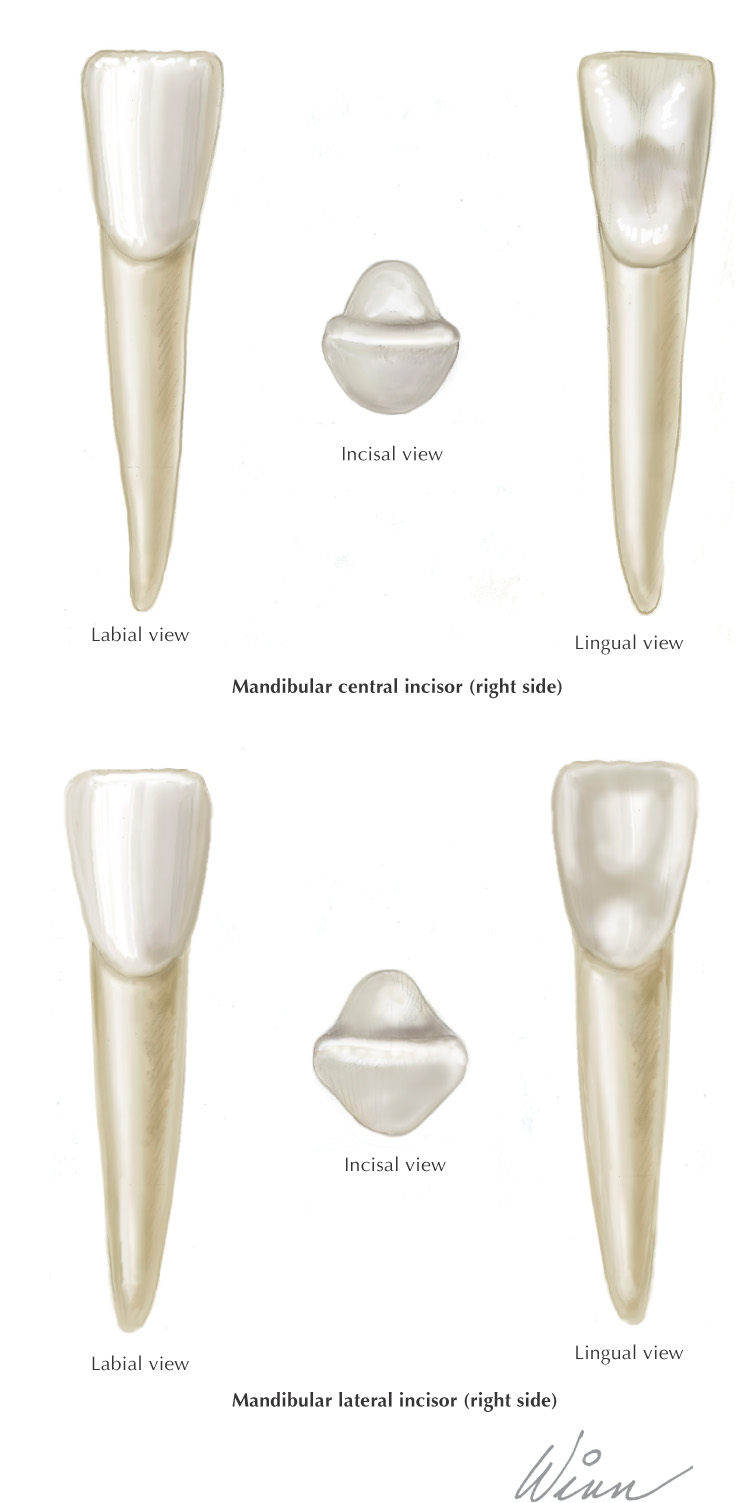
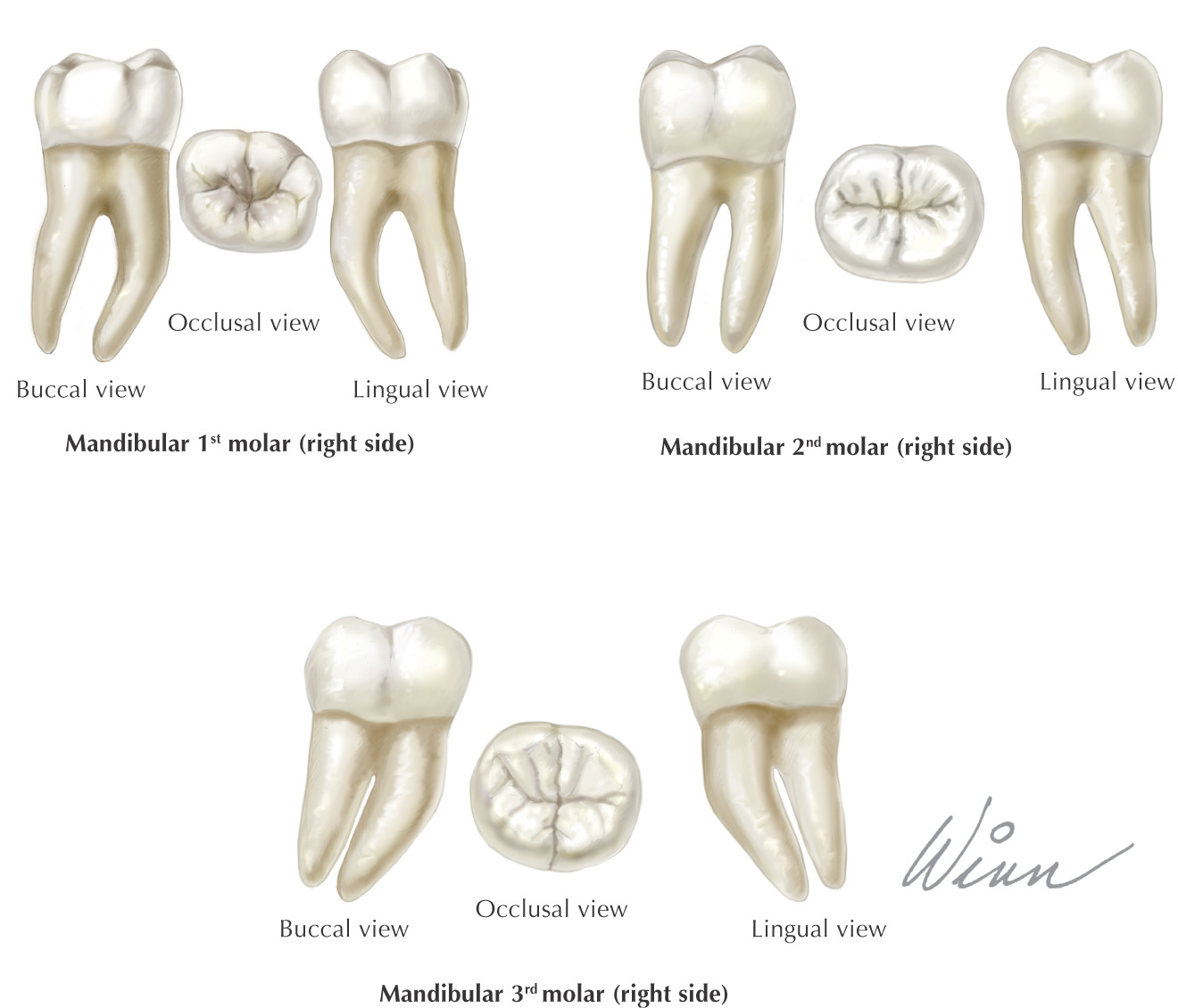
Teeth are hard structures attached to the jaws and involved primarily in eating
2 arches contain the teeth:
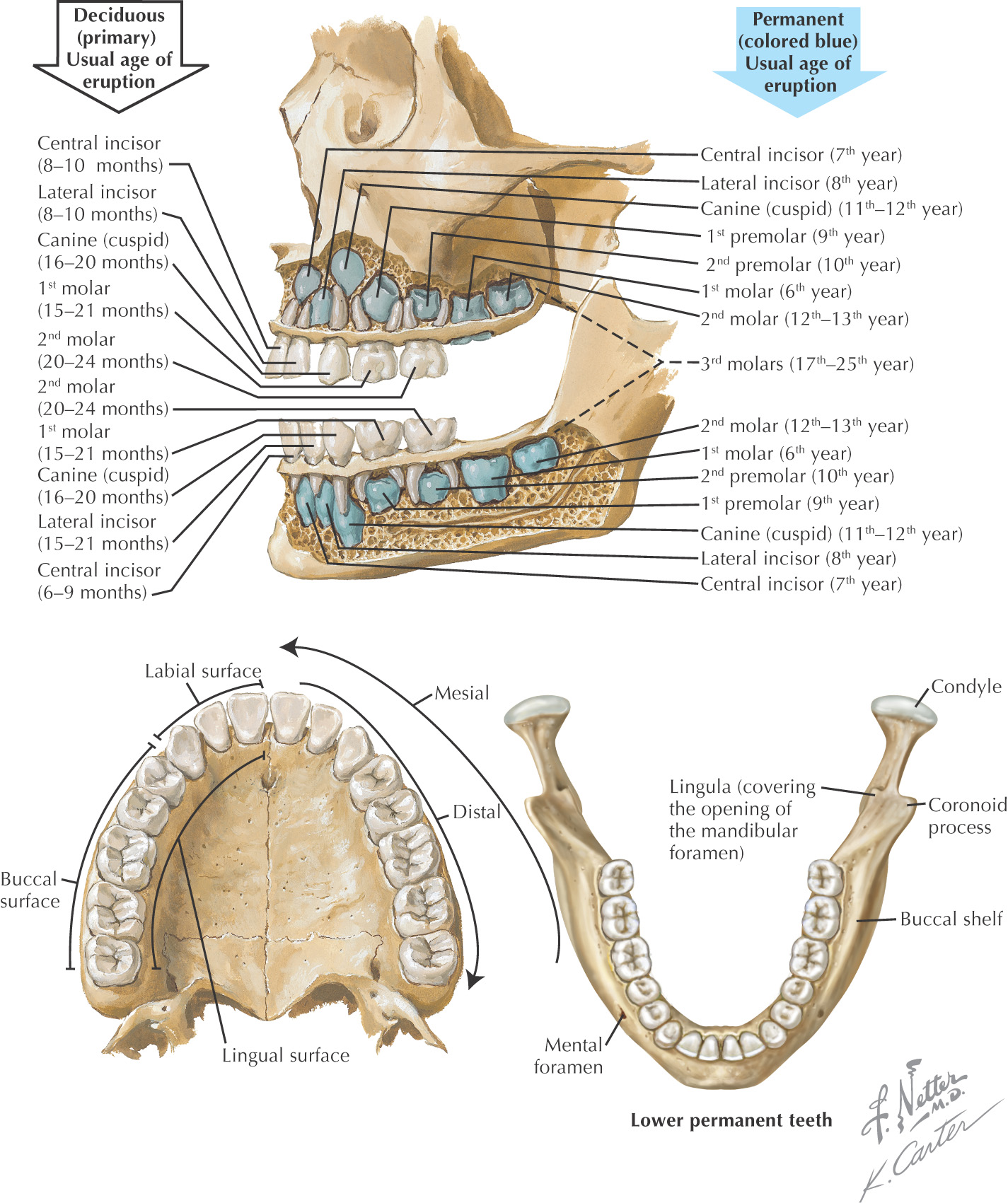
Humans have 2 sets of teeth during a lifetime:
• Deciduous teeth—the primary dentition
• Permanent teeth—the secondary dentition
Between the ages of 6 and 12 years, there is a mixed dentition, in which both primary and permanent teeth are present in the oral cavity at the same time
There are 20 total deciduous teeth: 2 incisors, 1 canine, and 2 molars in each of the 4 quadrants of the oral cavity
The primary dentition is represented by the formula  , which specifies the total number of teeth (10) on each side of the oral cavity
, which specifies the total number of teeth (10) on each side of the oral cavity
No deciduous teeth are present at birth; however, by the 3rd year of life, all 20 deciduous teeth have erupted
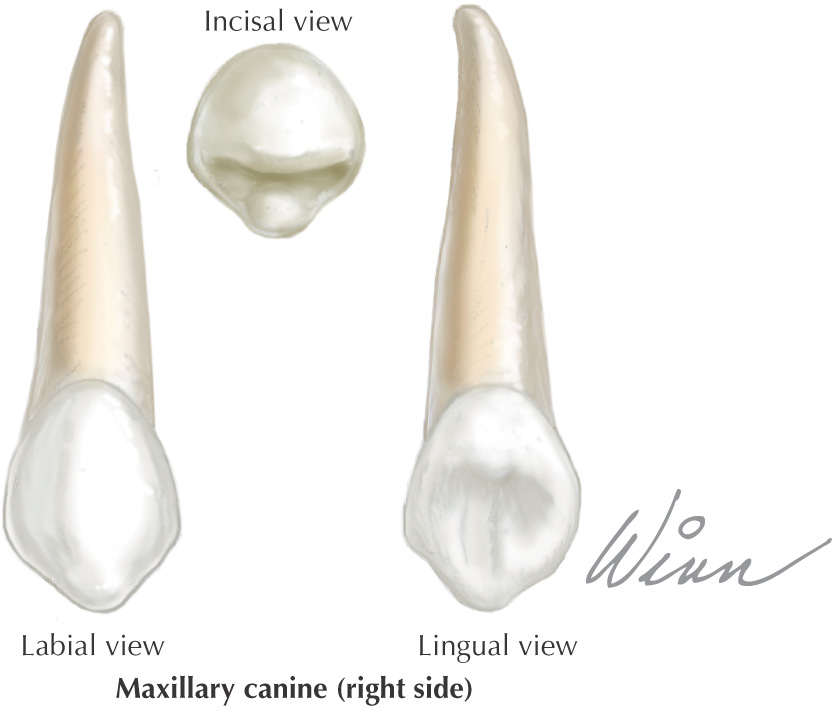
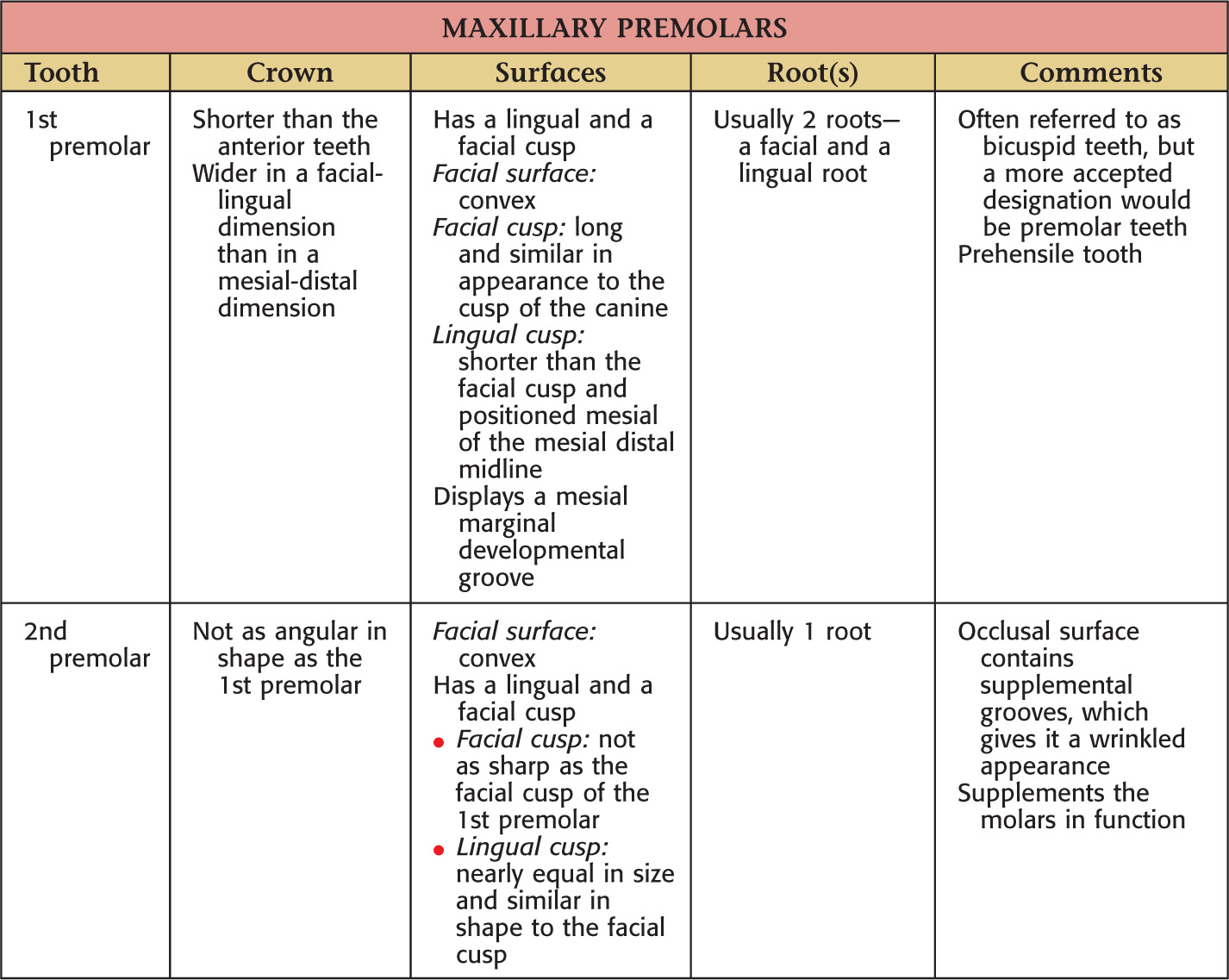
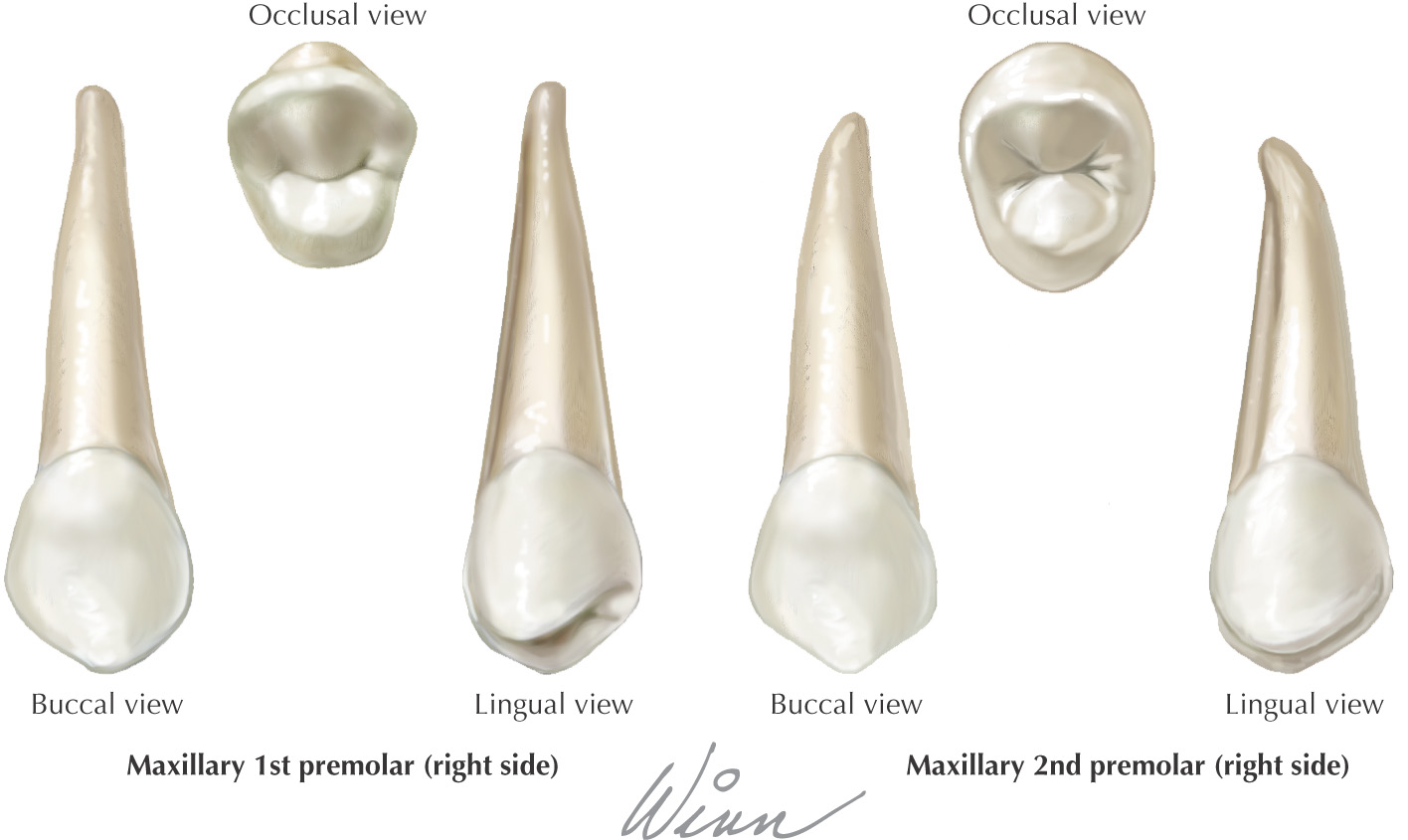
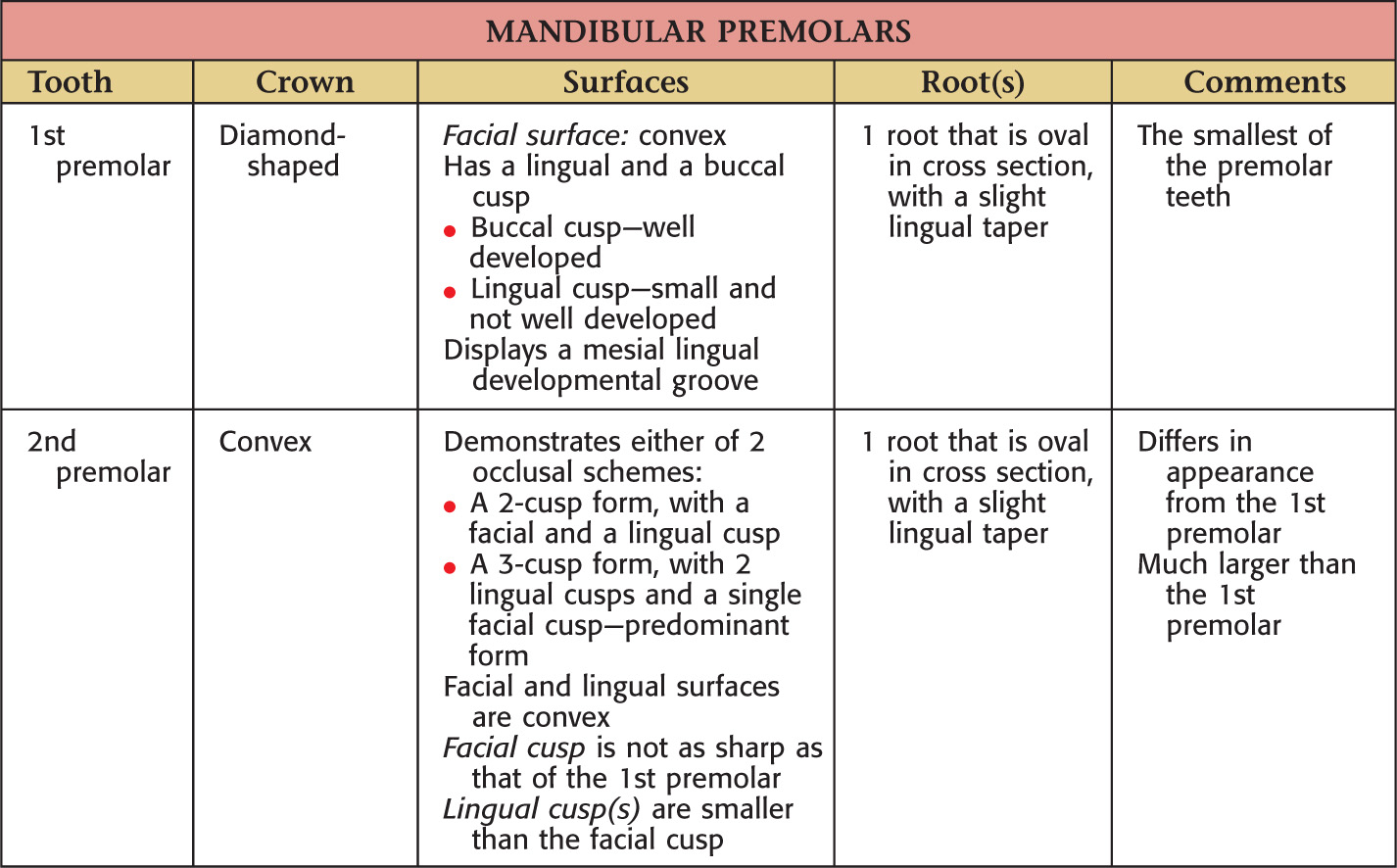
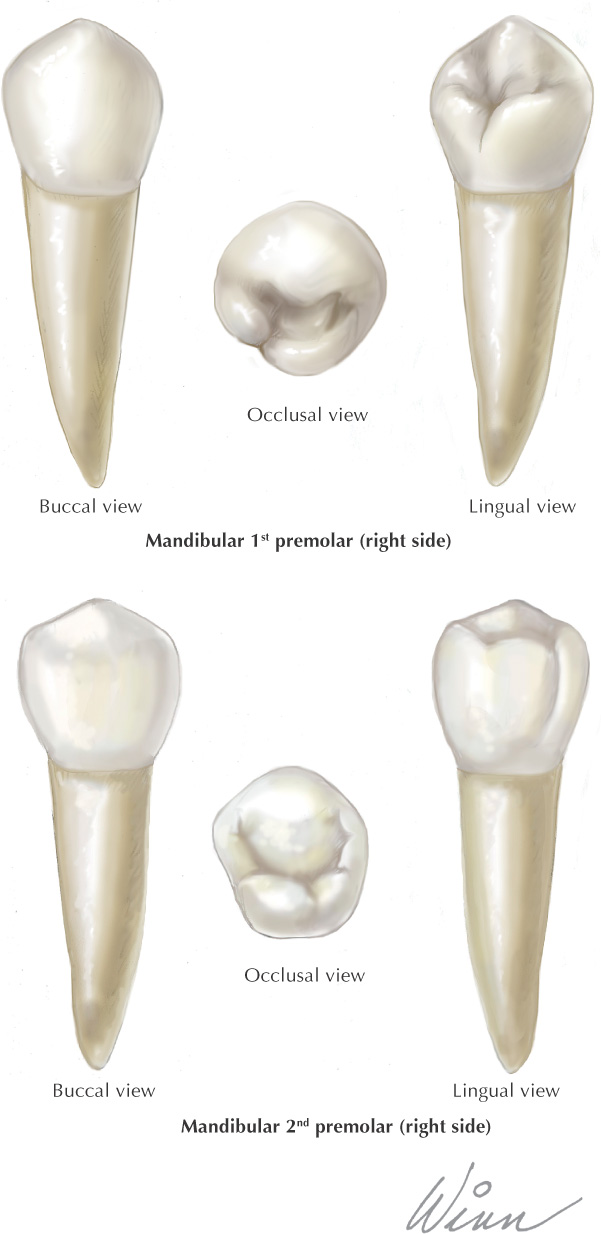
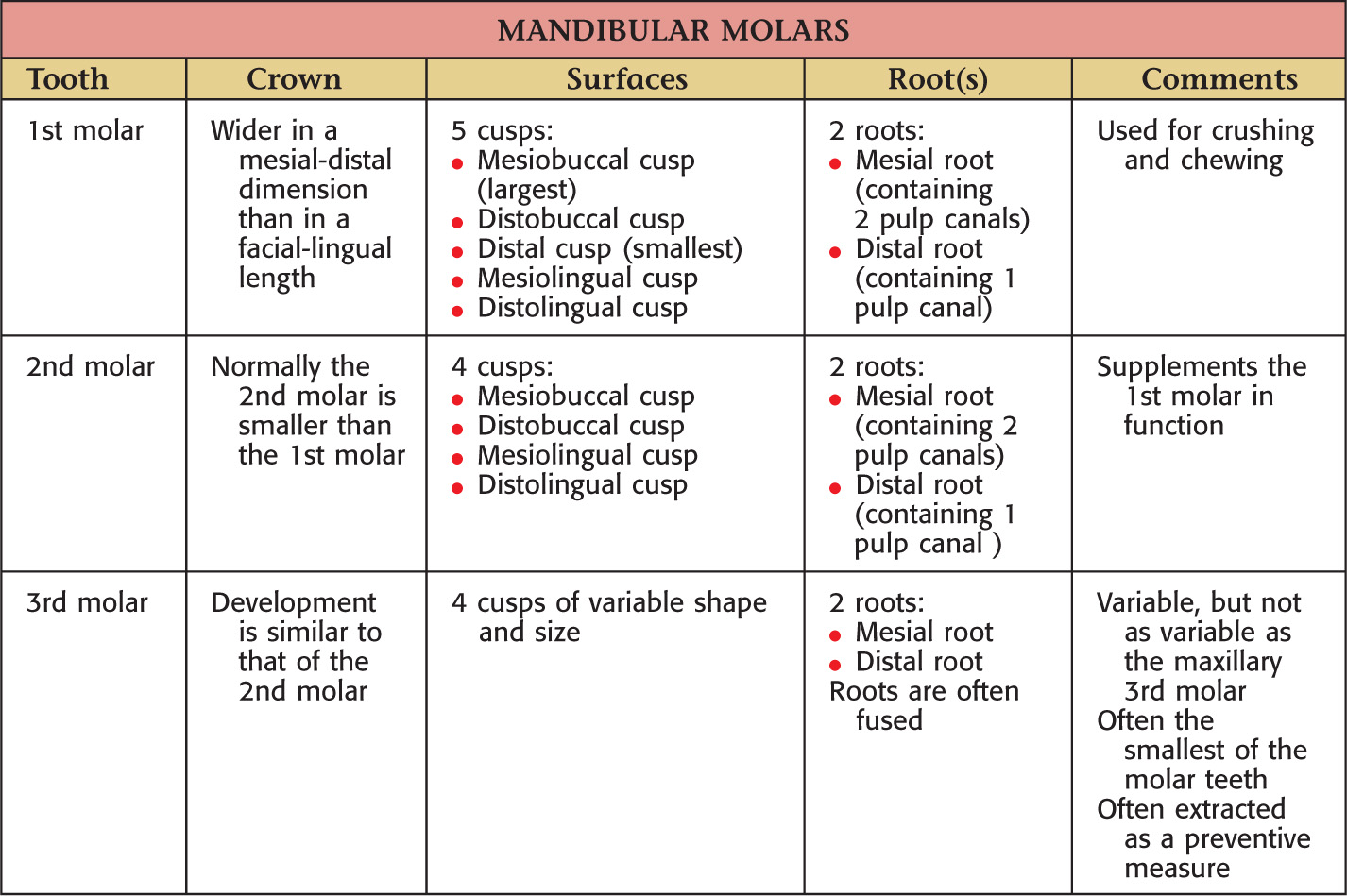
There are 32 total permanent teeth: 2 incisors, 1 canine, 2 premolars, and 3 molars in each of the 4 quadrants of the oral cavity
The permanent dentition is represented by the formula  , which specifies the total number of teeth (16) on each side of the oral cavity
, which specifies the total number of teeth (16) on each side of the oral cavity
The first permanent tooth to erupt into the oral cavity normally is the mandibular 1st molar
• This eruption occurs at about 6 years of age
• It erupts distal to the primary dentition
The primary teeth eventually are replaced by the permanent teeth
The replacement teeth are termed succedaneous teeth
Labial |
The surface of the anterior teeth that is closest to the lip |
Buccal |
The surface of the posterior teeth that is closest to the cheek |
Facial |
Used as a synonym for labial or buccal |
Lingual |
Opposite the tongue in the mandibular arch and opposite the hard palate of the maxillary arch |
Mesial |
Closest to the midline of the dental arch |
Distal |
Farthest from the midline of the dental arch |
Occlusal |
Used for chewing in posterior teeth |
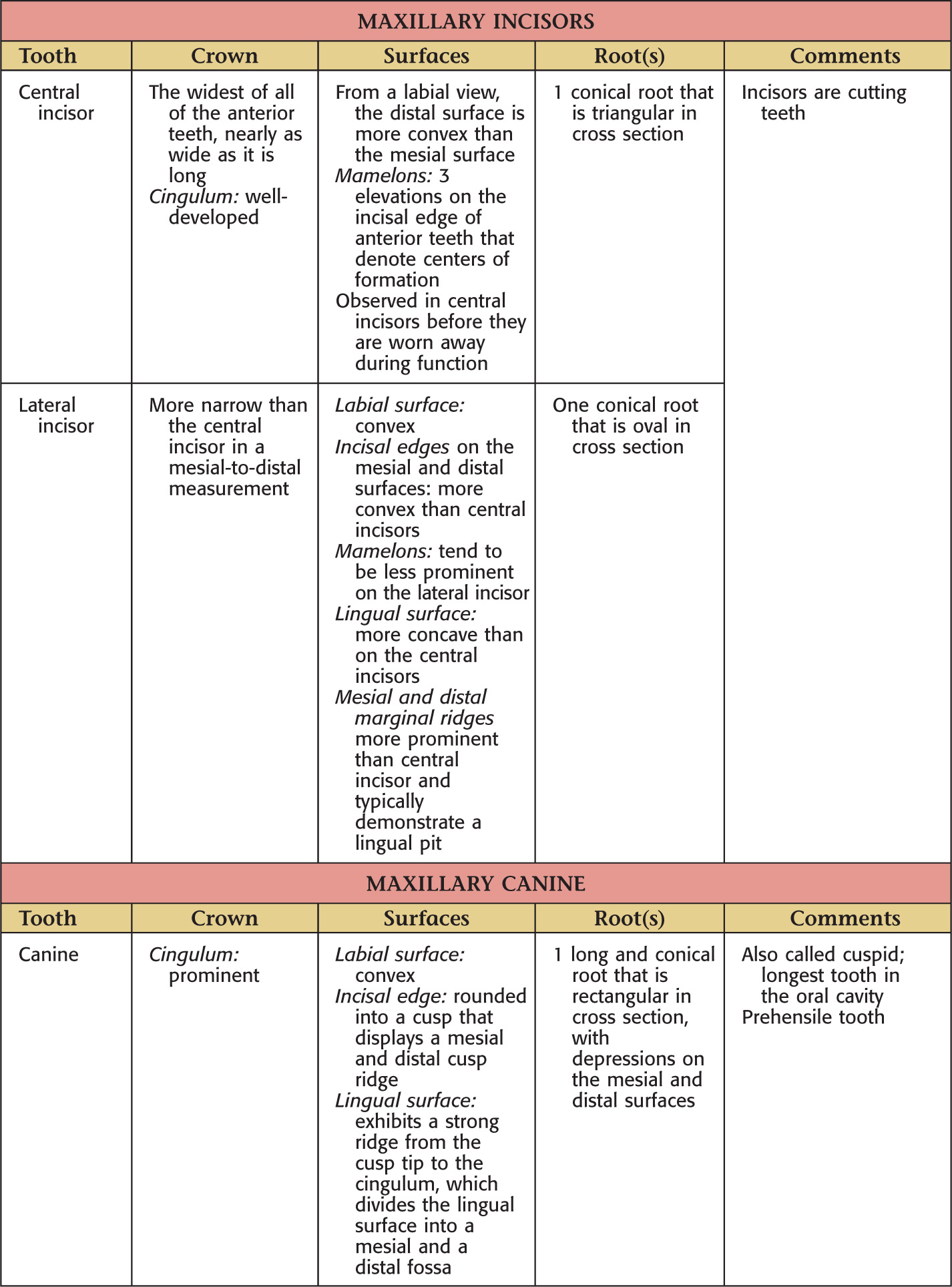
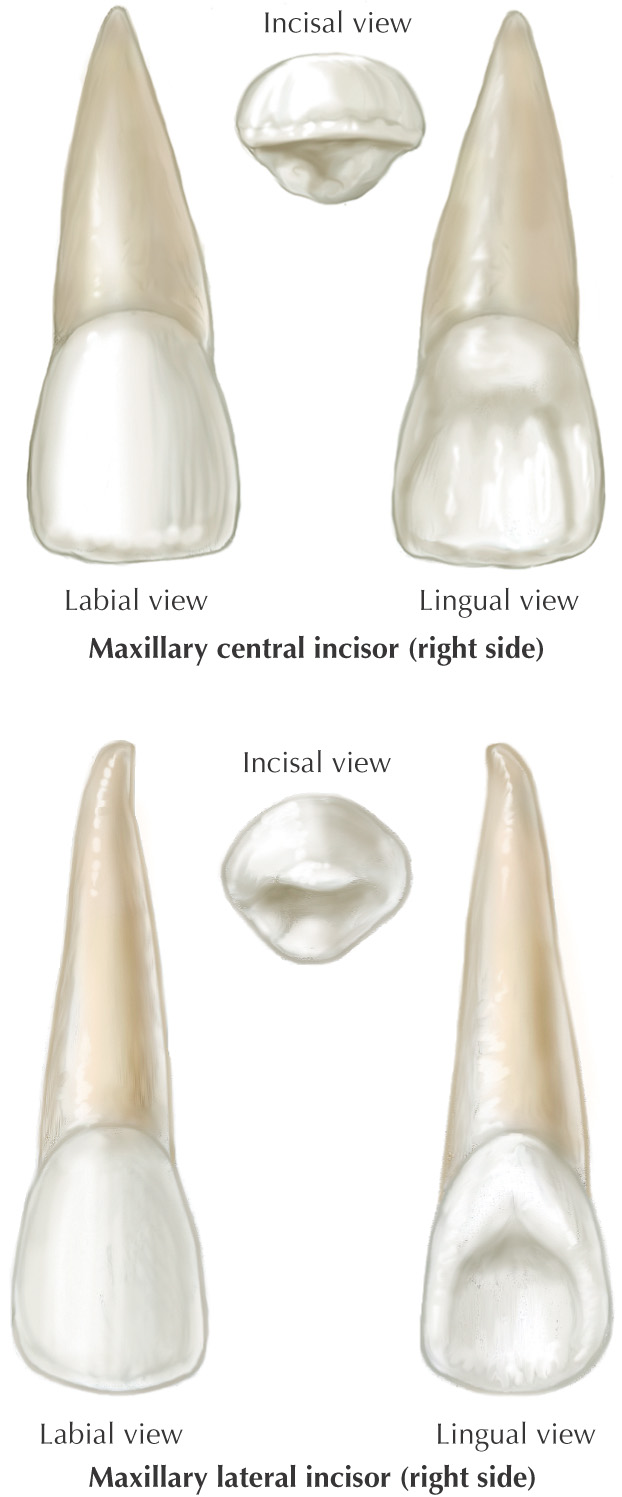
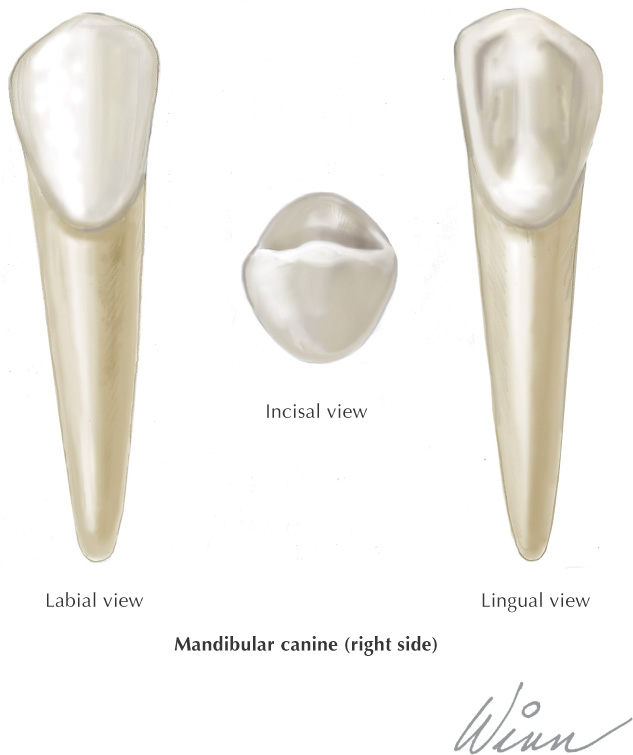
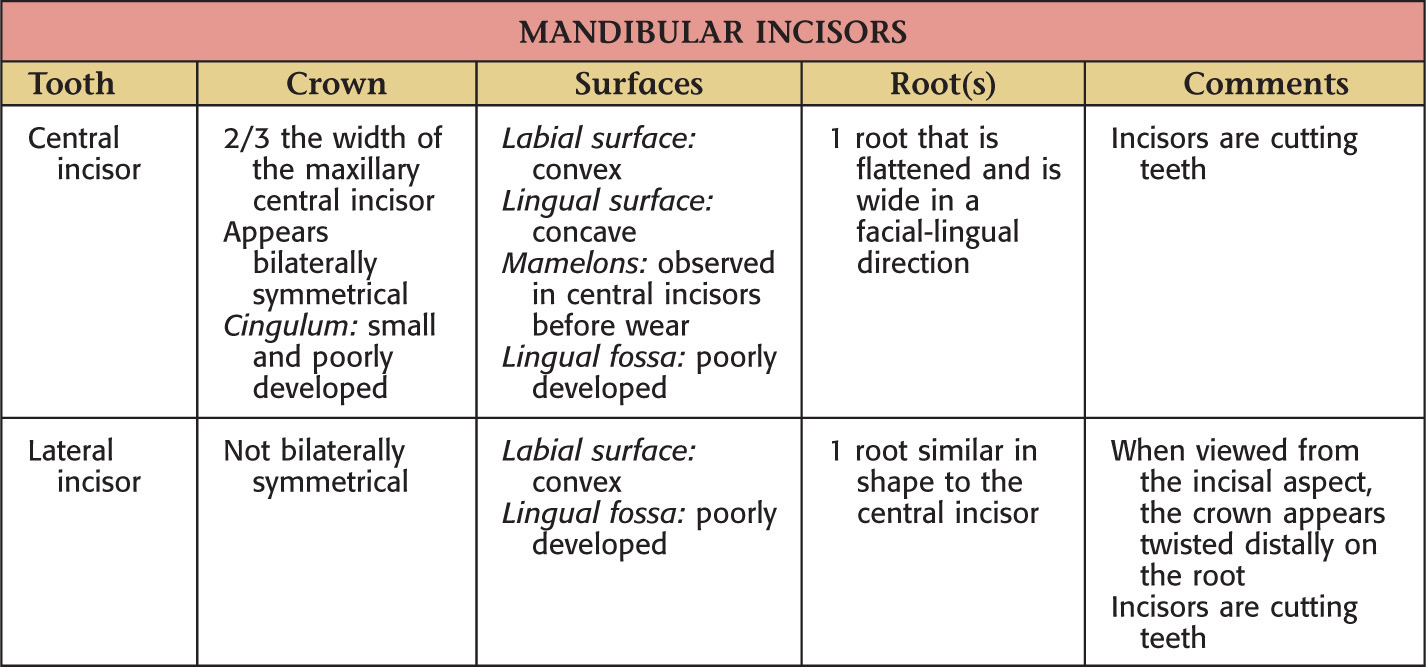
Incisal |
The cutting edge of anterior teeth |


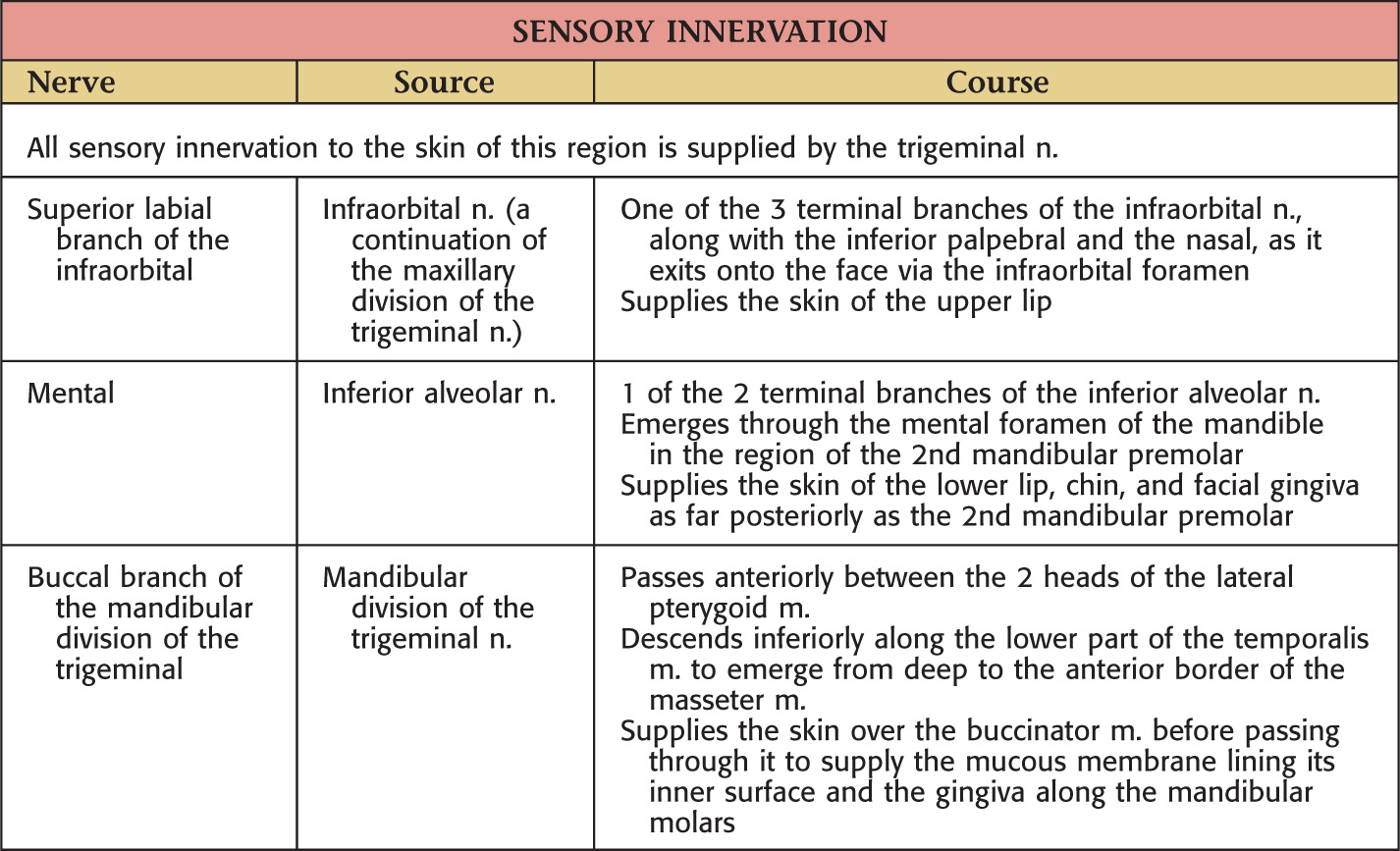
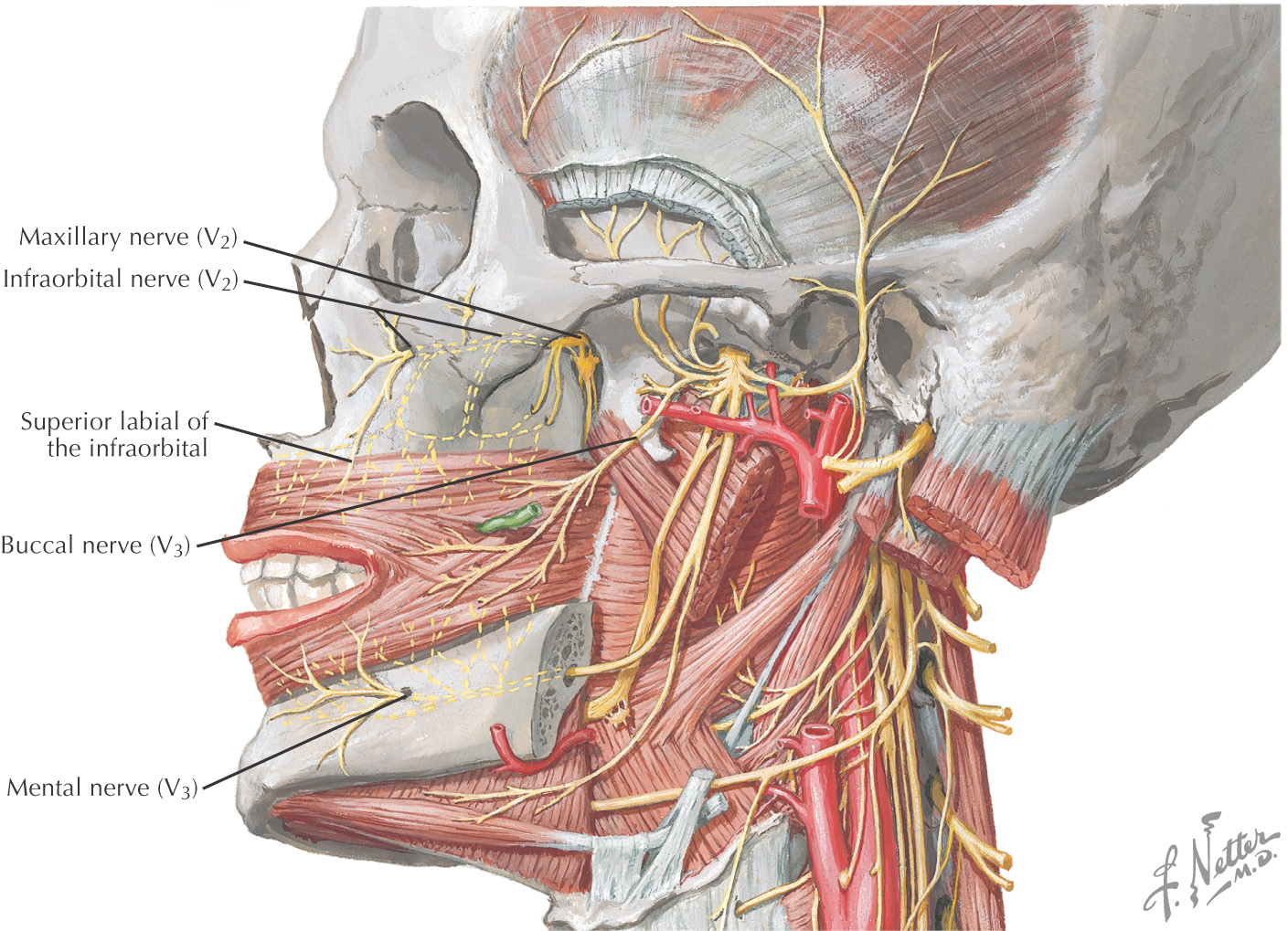
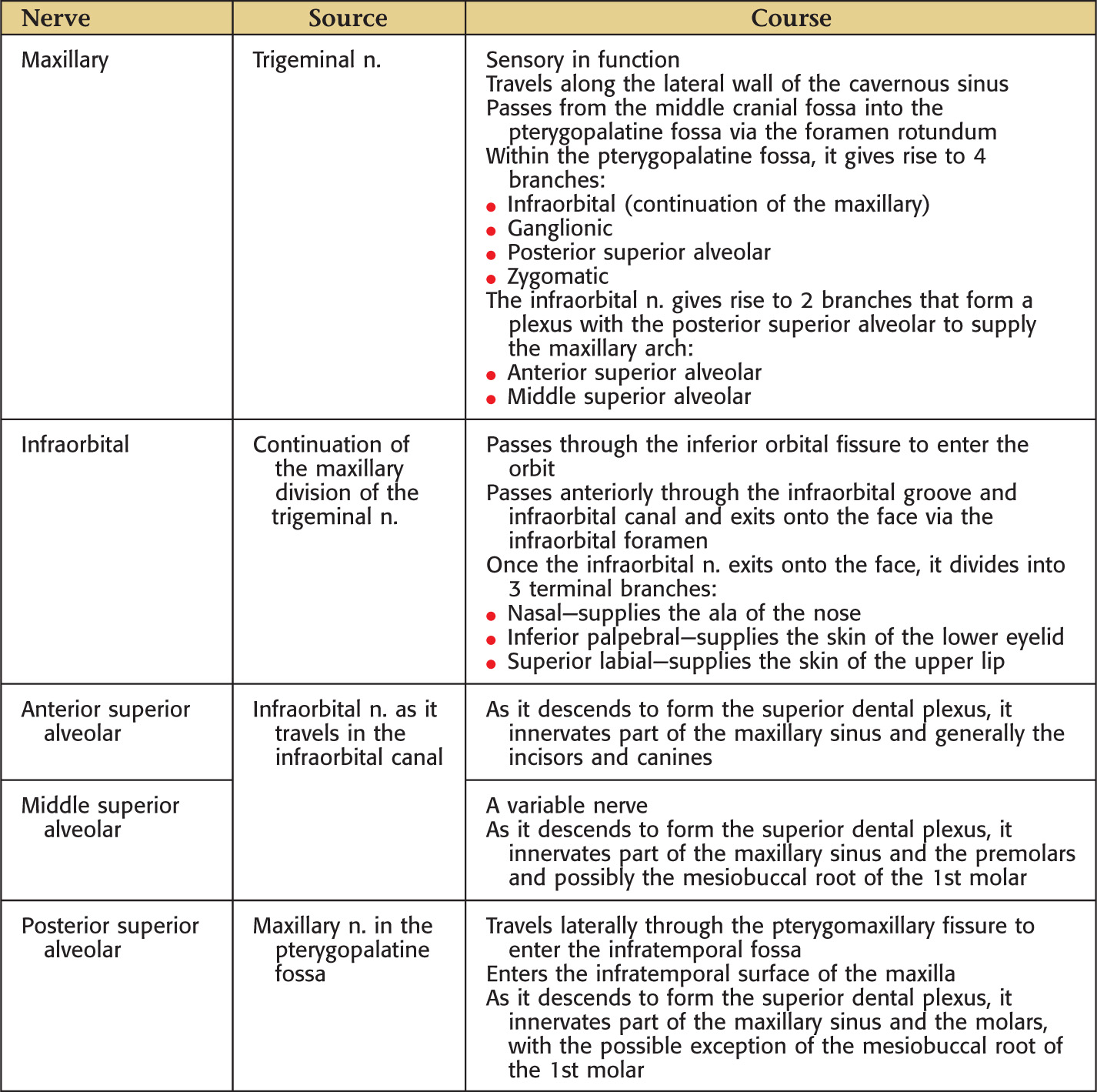
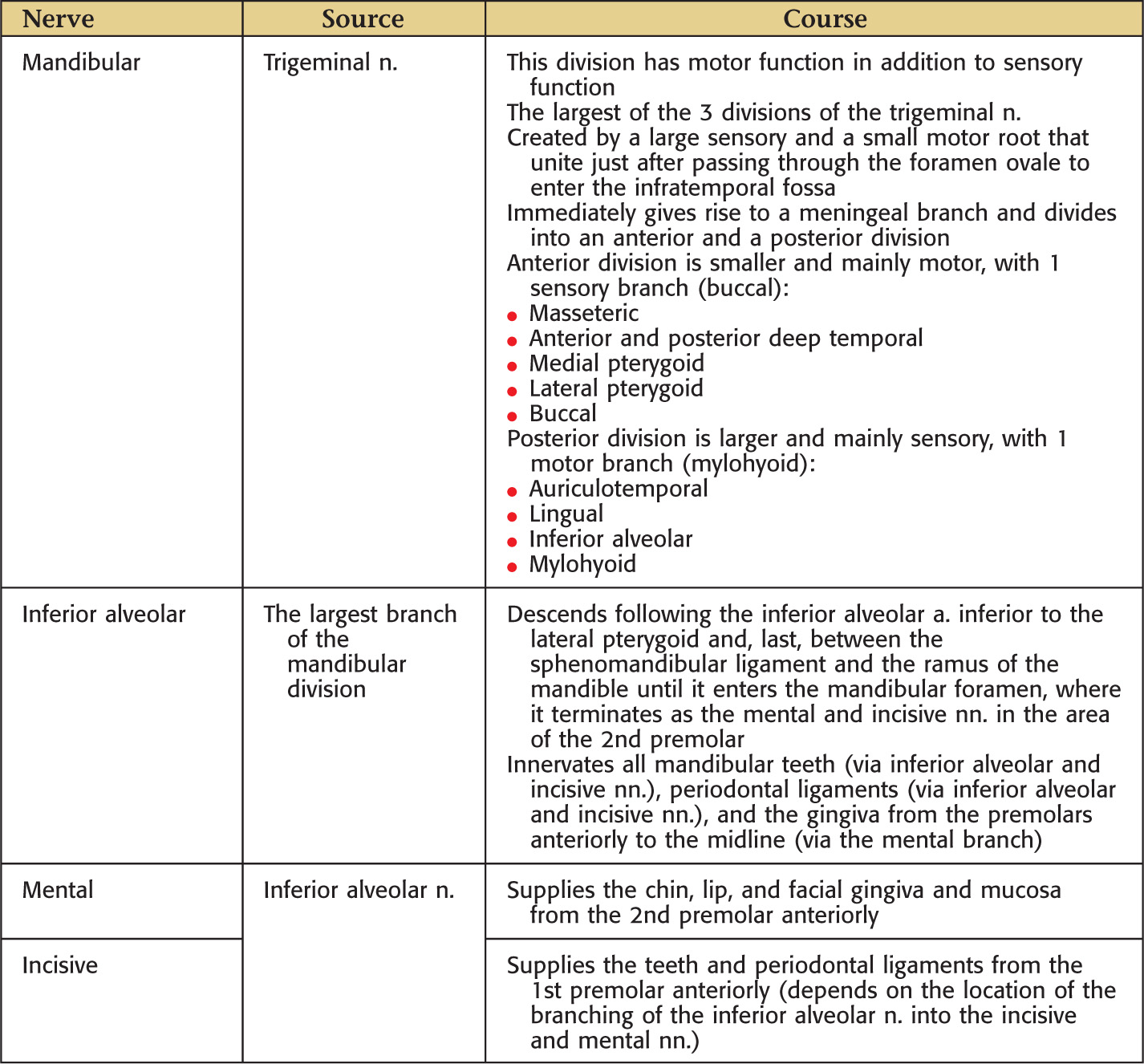
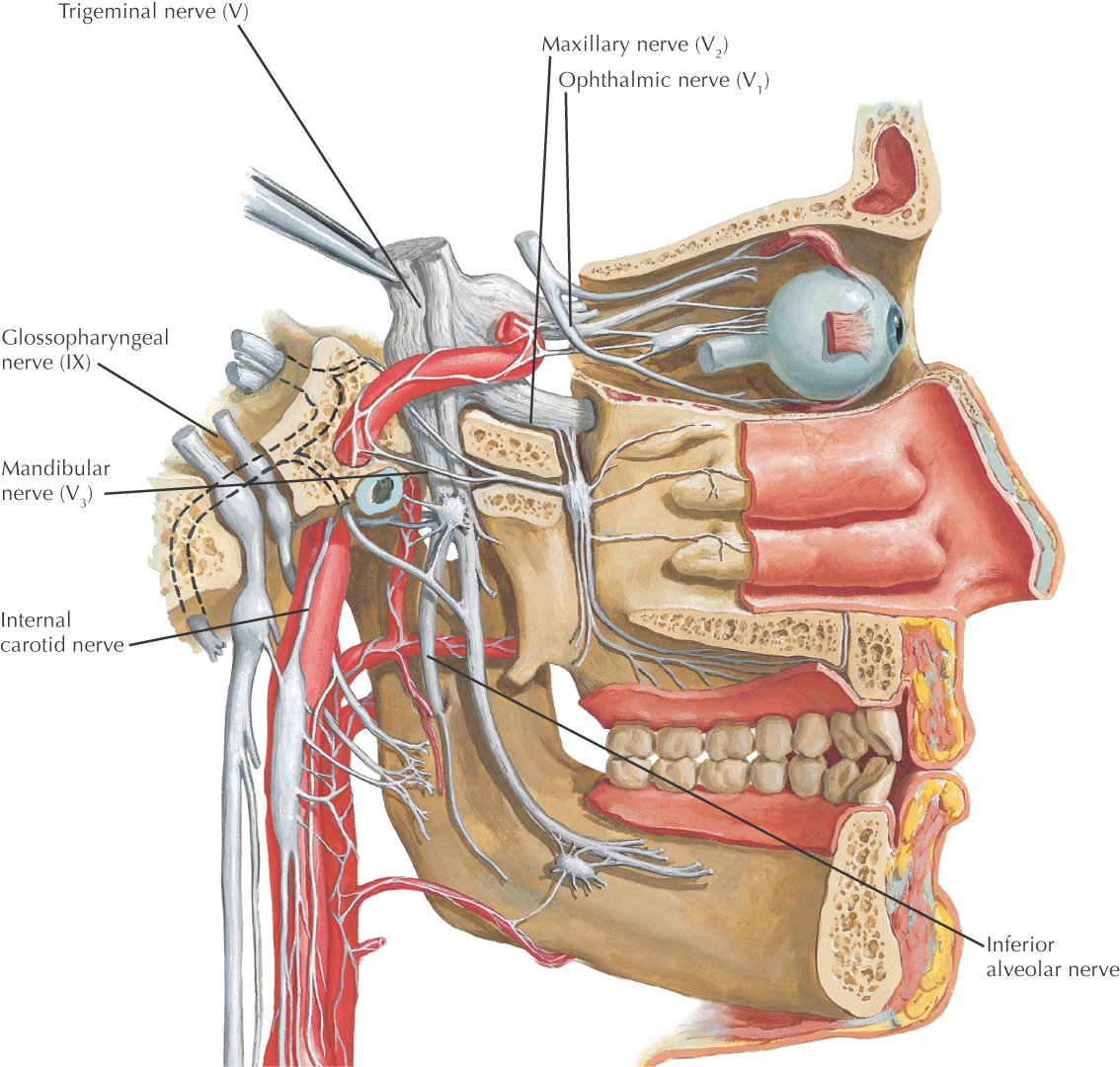
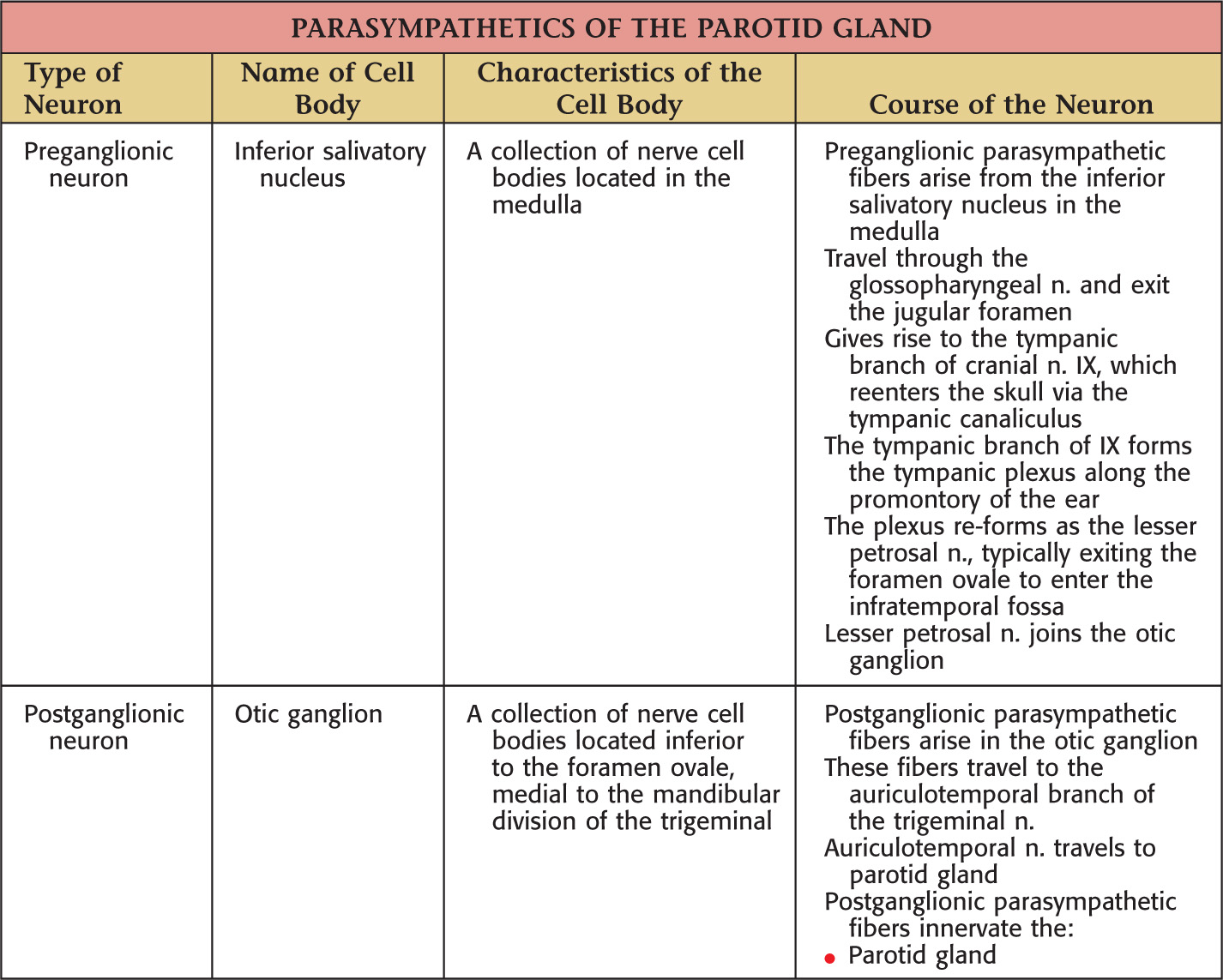
The oral cavity receives its sensory innervation from branches of the maxillary and mandibular divisions of the trigeminal nerve
There are 3 pairs of major salivary glands:
They secrete saliva into the oral cavity to aid in the digestion, mastication, and deglutition of food
Saliva is mucous or serous in consistency
Many minor salivary glands are ubiquitously distributed throughout the oral mucosa of the oral cavity
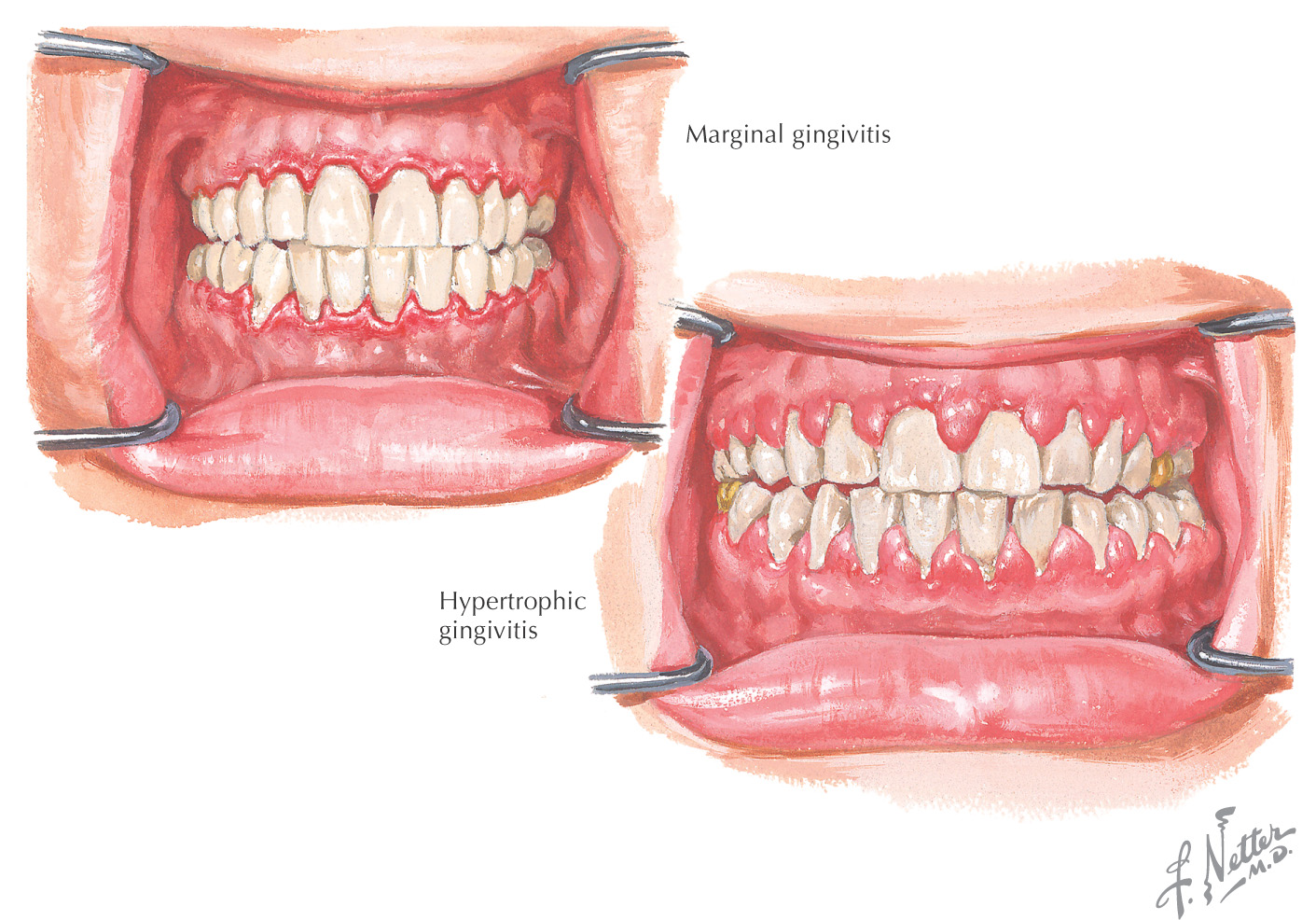
Gingivitis: an inflammation of the gingiva that occurs when bacteria accumulate between the teeth and gingiva
In addition to the inflammation, the gums may demonstrate irritation and bleeding
When plaque (composed of bacteria, food debris, and saliva) is deposited on the teeth, it can form tartar if it is not removed
Plaque and tartar cause irritation to the gingiva, and the bacteria (and their toxins) further irritate the gingiva, leading to bleeding and swelling
If gingivitis remains untreated, it may progress to more serious gingival diseases, such as periodontitis
Long-term untreated gingivitis may lead to damage of bone and loss of teeth
Risk factors for gingivitis include poor dental hygiene, pregnancy, diabetes, illness, and human immunodeficiency virus (HIV) infection
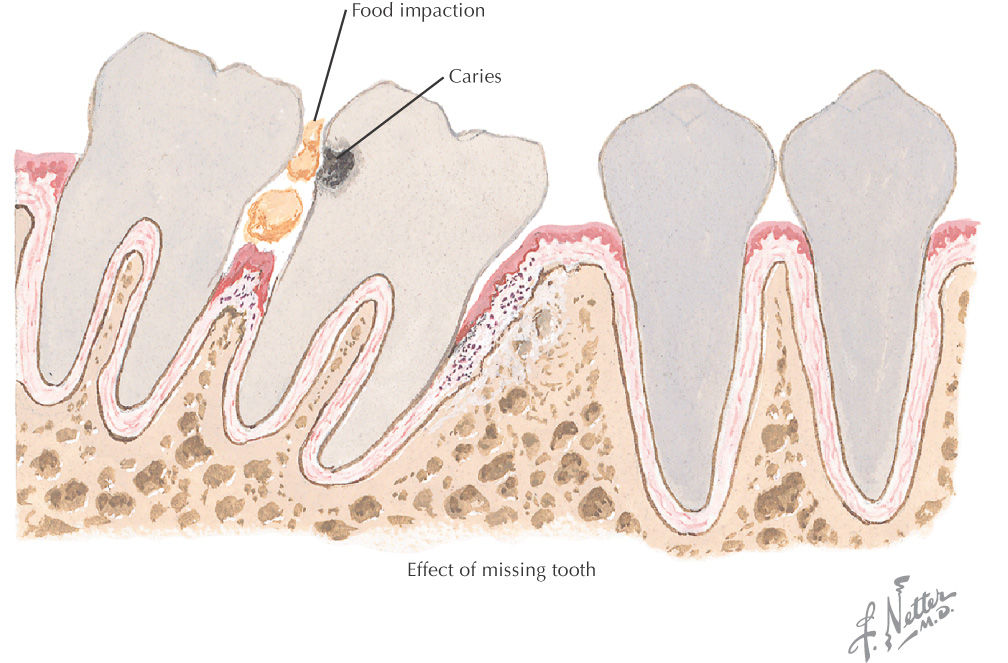
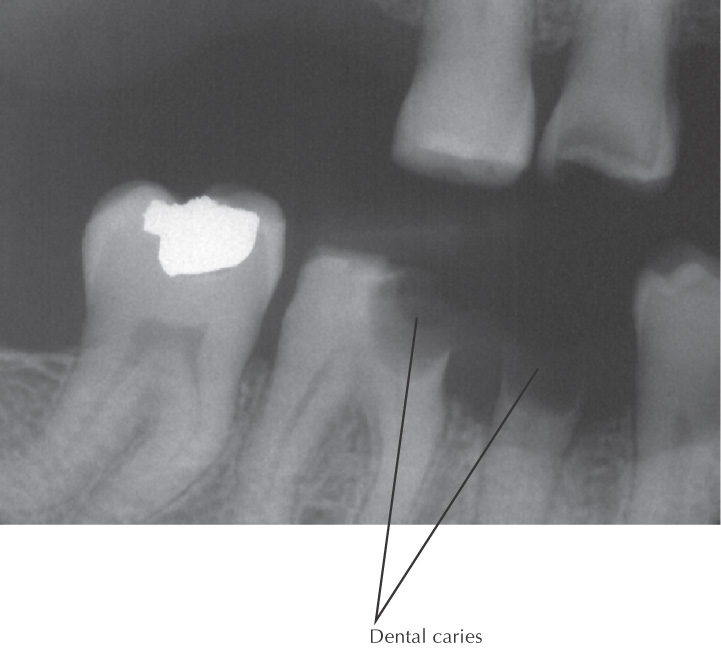
Dental caries (tooth decay), leading to “cavities,” is caused by bacteria in the oral cavity
The bacteria convert foods into acids and help form plaque (made of bacteria, food debris, and saliva), which is deposited on the teeth
Plaque that is not removed from the teeth can mineralize to form tartar
Plaque is most prominent on difficult-to-reach teeth, such as the posterior molars
Acids formed in the plaque begin to erode the enamel on the surface of the tooth, causing a “cavity”
If not treated, the cavity grows in size, with onset of pain as the nerves and blood vessels of the affected teeth become irritated
Consuming foods rich in sugar and starch increases the risk of dental caries
Dental caries can be detected on routine dental examinations
The damage associated with dental caries cannot be repaired by the affected tooth, which now must be restored
Fluoride is used to reduce the risk of dental caries by inhibiting demineralization and promoting remineralization of tooth structure
Saliva helps promote the remineralization process; medications that decrease salivary flow (such as anticholinergics) promote dental caries
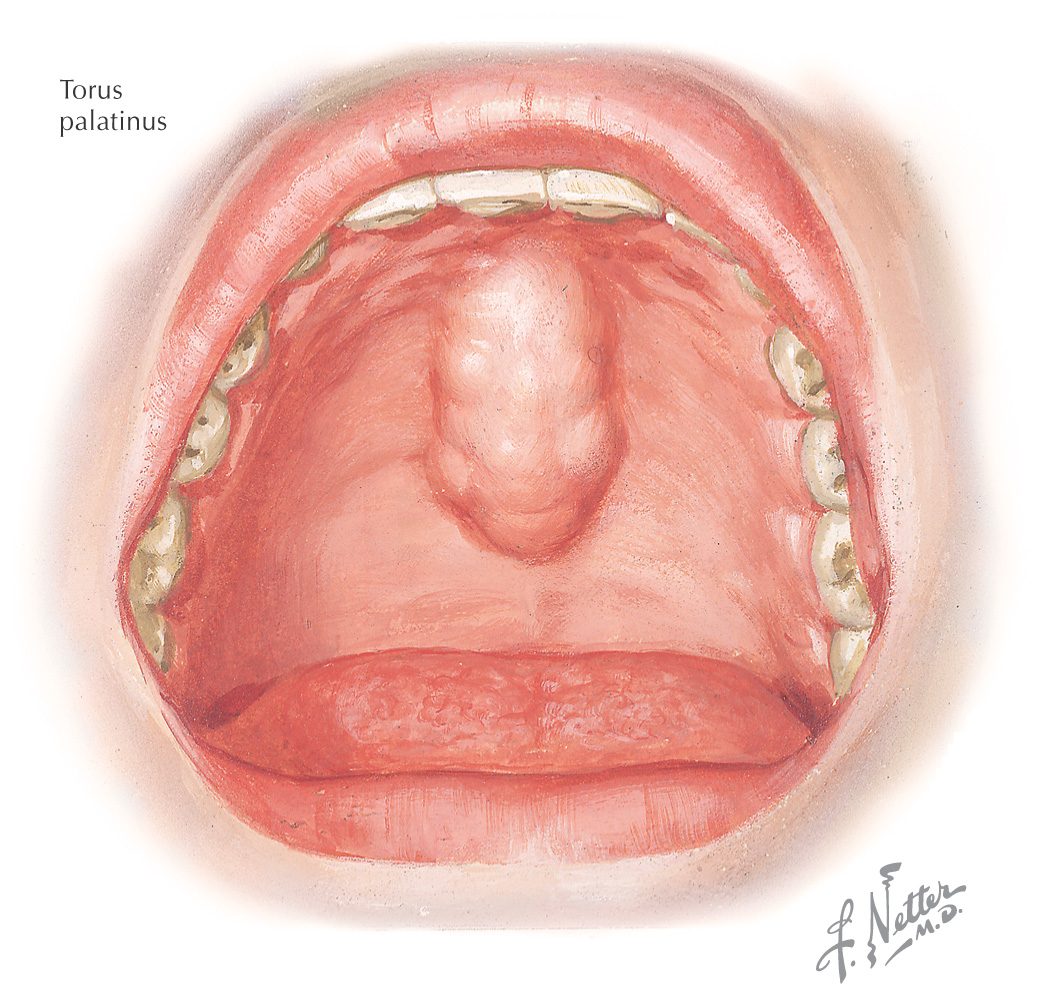
Torus: a nonpathologic bony elevation that occurs in the oral cavity
The presence of a torus does not impede eating or verbal communication but can cause difficulty in the application of a dental appliance, such as a denture
2 major types:
• Palatine—a downgrowth of bone in the midline of the hard palate
• Mandibular—an outgrowth of bone that occurs on the lingual surface of the mandible
A torus does not require treatment unless it interferes with normal function or application of dental appliances
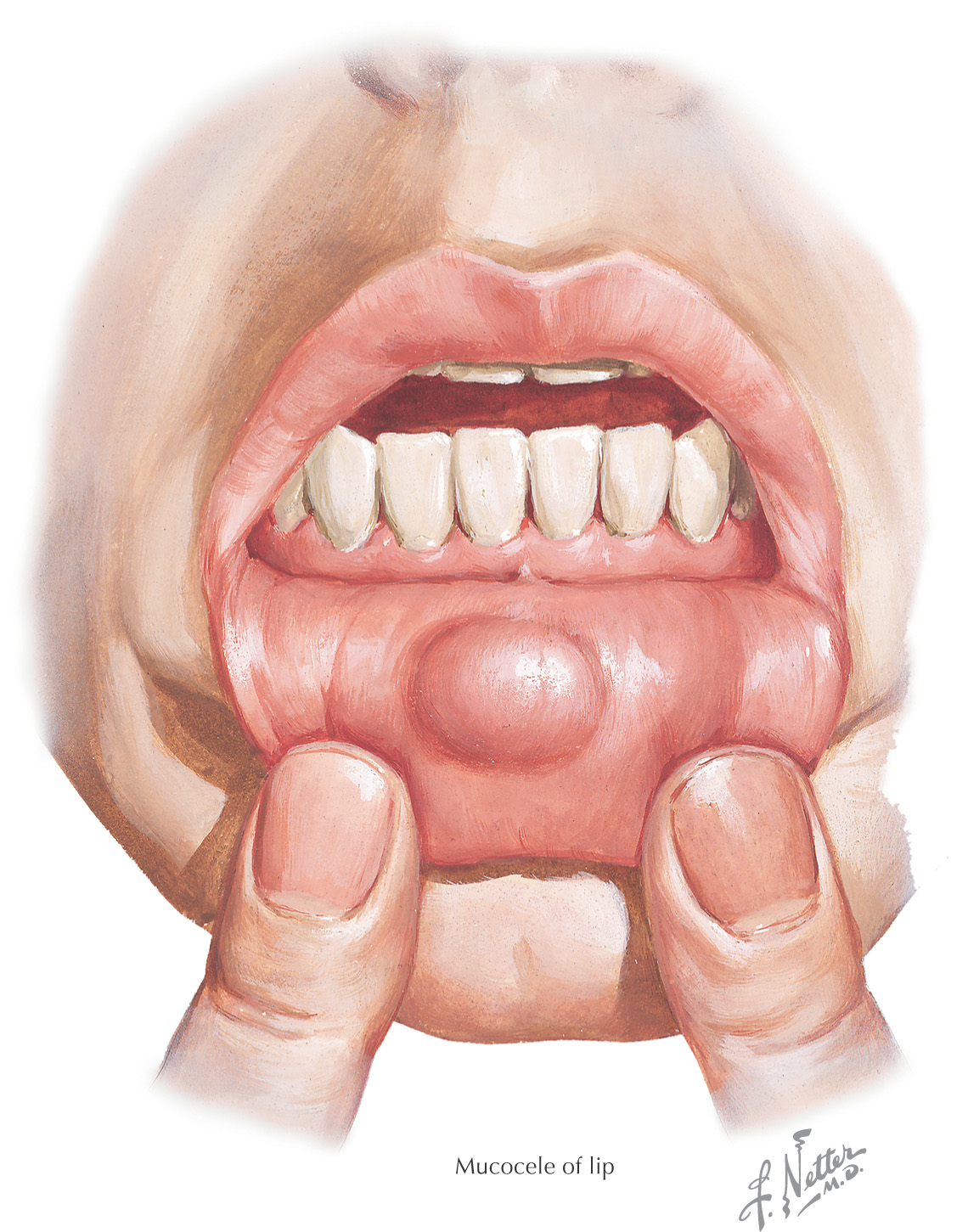
Mucocele: a mucous cyst that results from obstruction of the ducts of minor salivary glands (this lesion also can be associated with blockage of the major salivary glands)
Often caused by trauma to the duct system
Usually located on the lingual aspect of the lip
These lesions contain mucin and granulation tissue
Persistent mucoceles often are excised
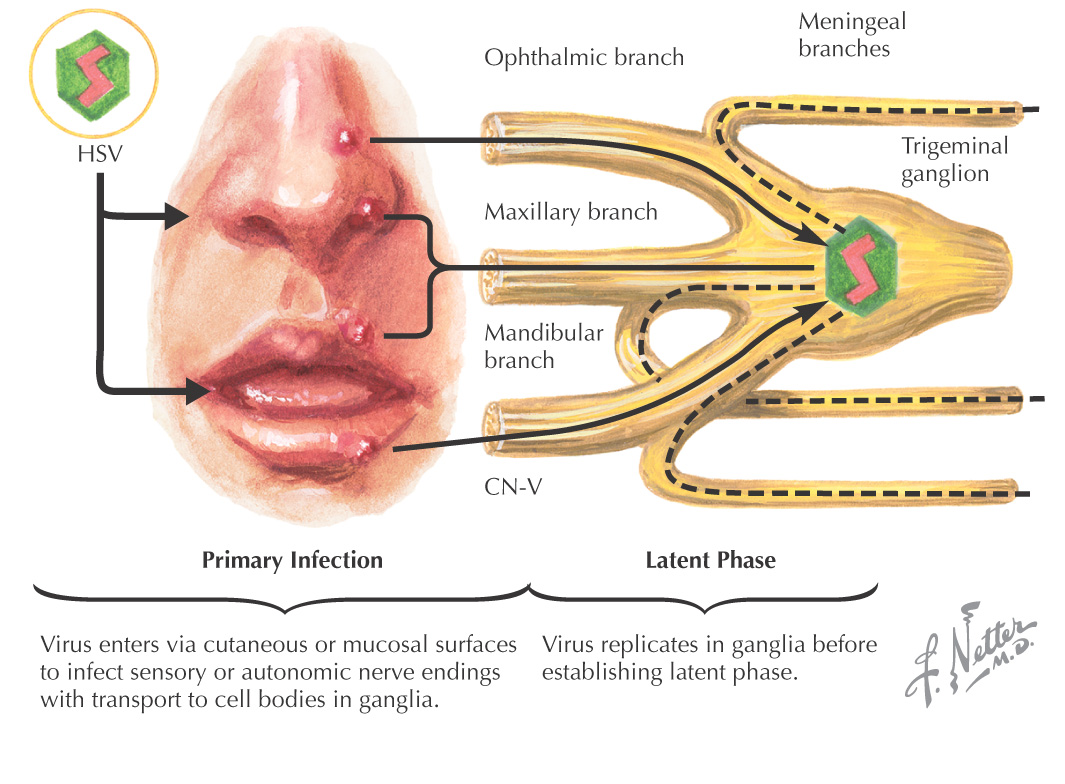
Herpes simplex is the most common cause of viral stomatitis
Caused by exposure to herpes simplex virus type 1 (HSV-1)
HSV-1 usually affects the regions above the waist, causing fever blisters
Most affected people acquire the infection as a child
During the primary infection with HSV-1, multiple vesicles appear on the lips, gingiva, hard palate, and tongue
These vesicles rupture, producing ulcers that heal in 7 to 10 days
After initial exposure, the virus is transported along a retrograde path into the trigeminal ganglion, where it stays inactive and does not replicate
Episodes may recur
Some recurrence triggers:
Infection can be spread through contact with infected lips
Systemic administration of antiviral agents, such as acyclovir, decreases the duration of the recurrent episodes
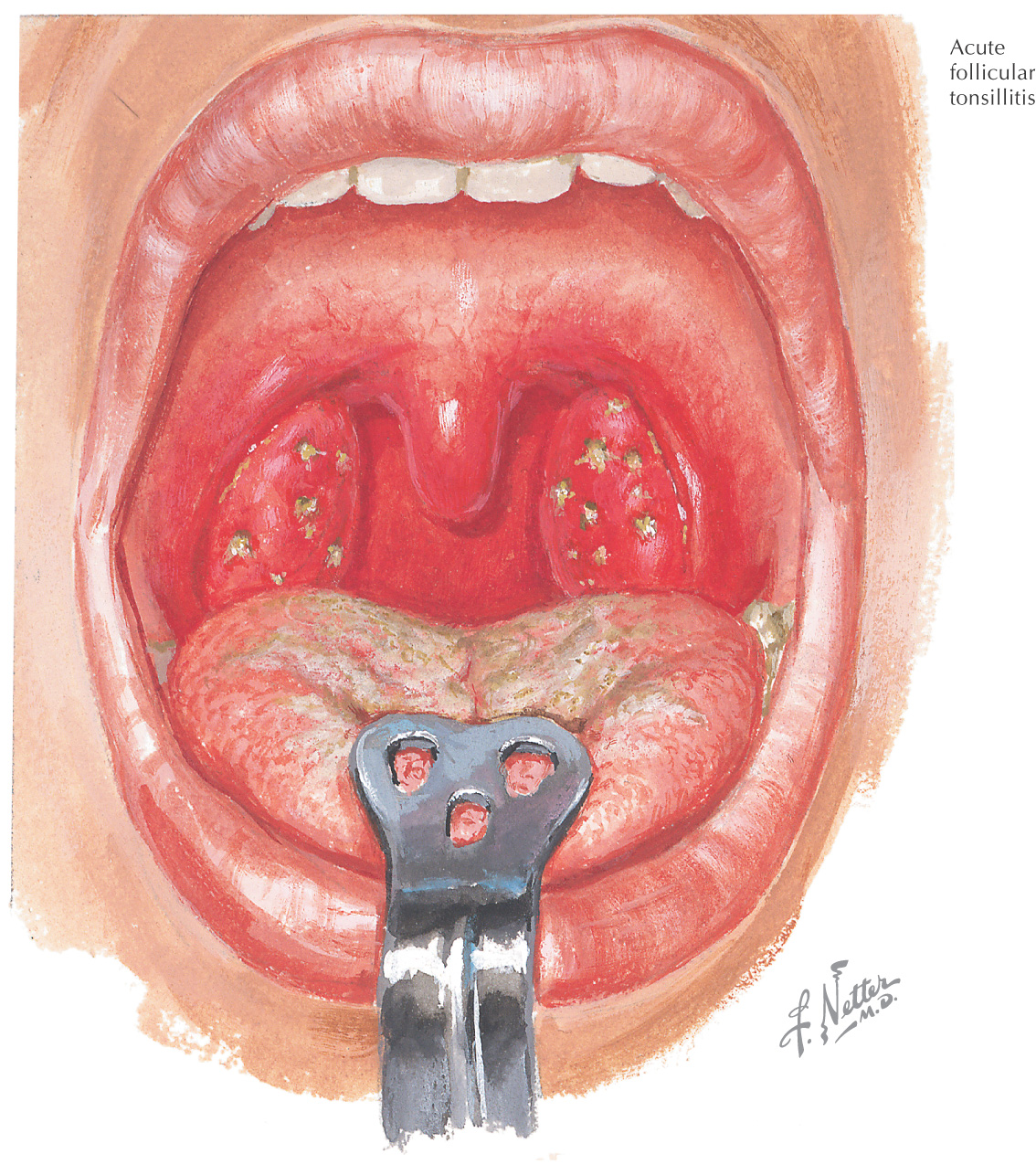
Tonsillitis: an inflammation of the tonsils, the lymph nodes located in the oral cavity and pharynx
There are 3 sets of tonsils:
• Palatine (between the palatoglossal and palatopharyngeal arches)
• Lingual (on posterior 1/3 of the tongue)
These 3 sets of tonsils form Waldeyer’s ring
Symptoms of tonsillitis:
Tonsillitis often is caused by a virus or bacterium
When caused by a bacterial infection, it may be treated by antibiotics
If necessary, a tonsillectomy is performed to remove the tonsils. Palatine tonsils are removed in a tonsillectomy (although the pharyngeal tonsils also may be removed at the same time, especially if they are obstructing nasal breathing)