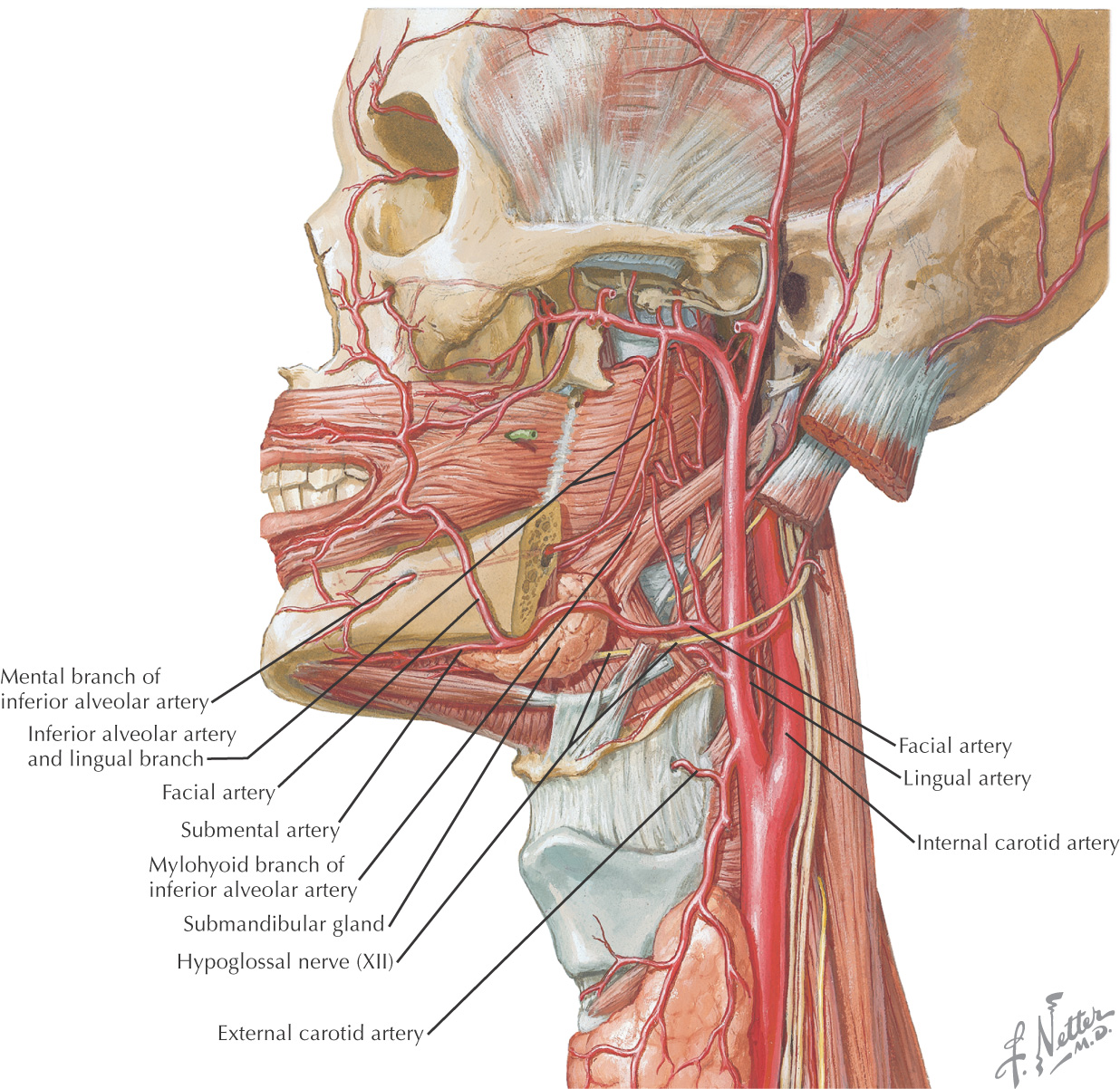
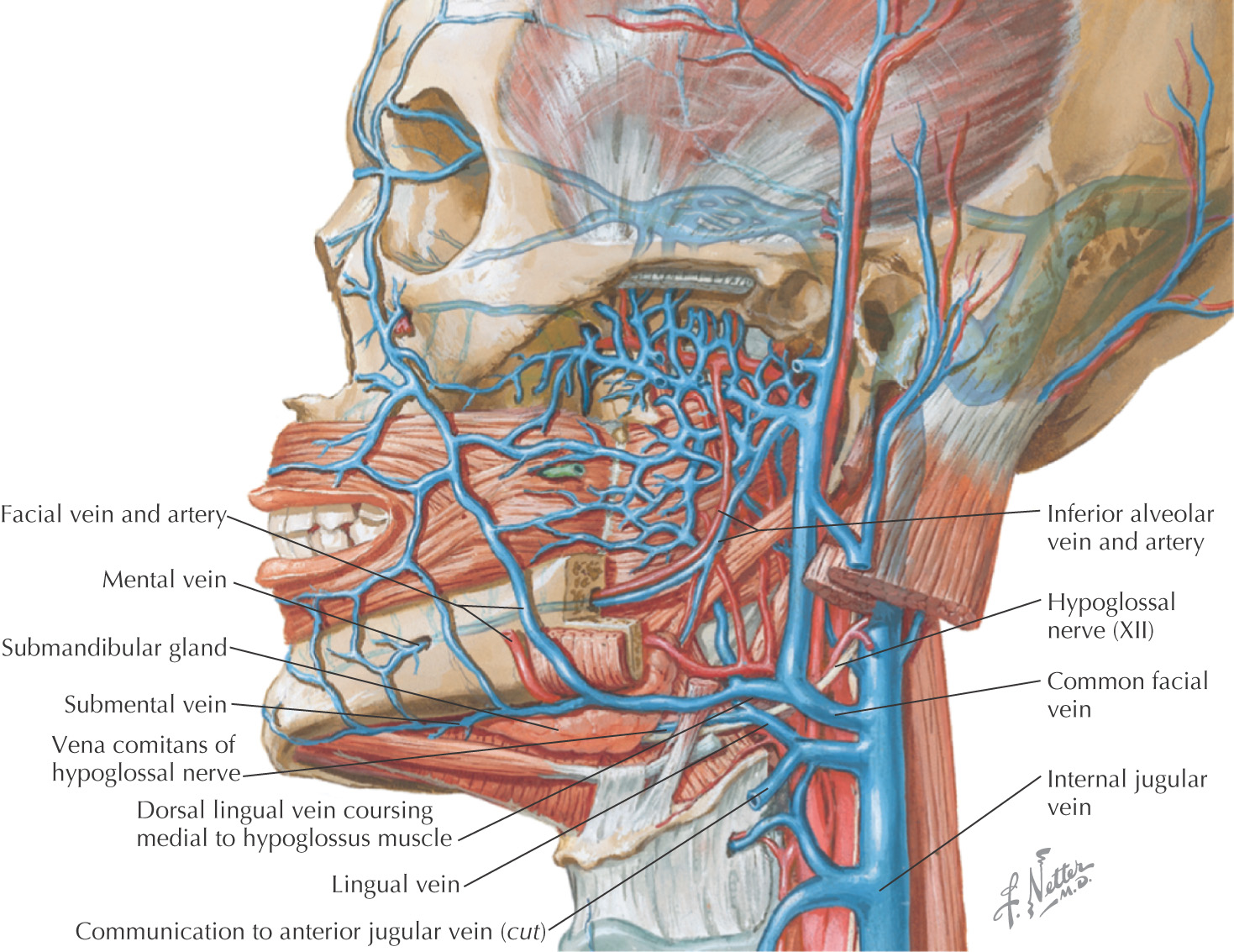
Overview and Topographic Anatomy
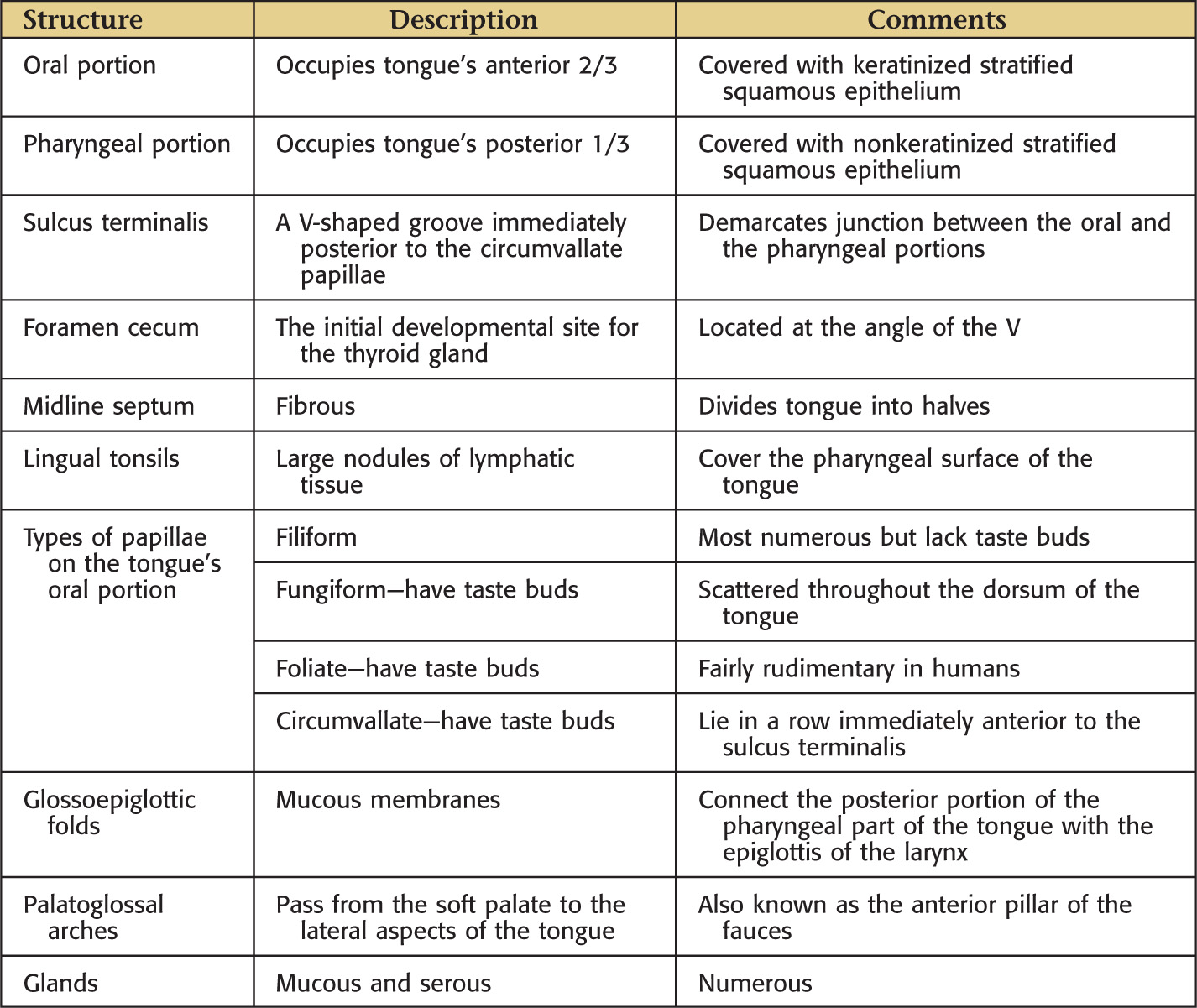
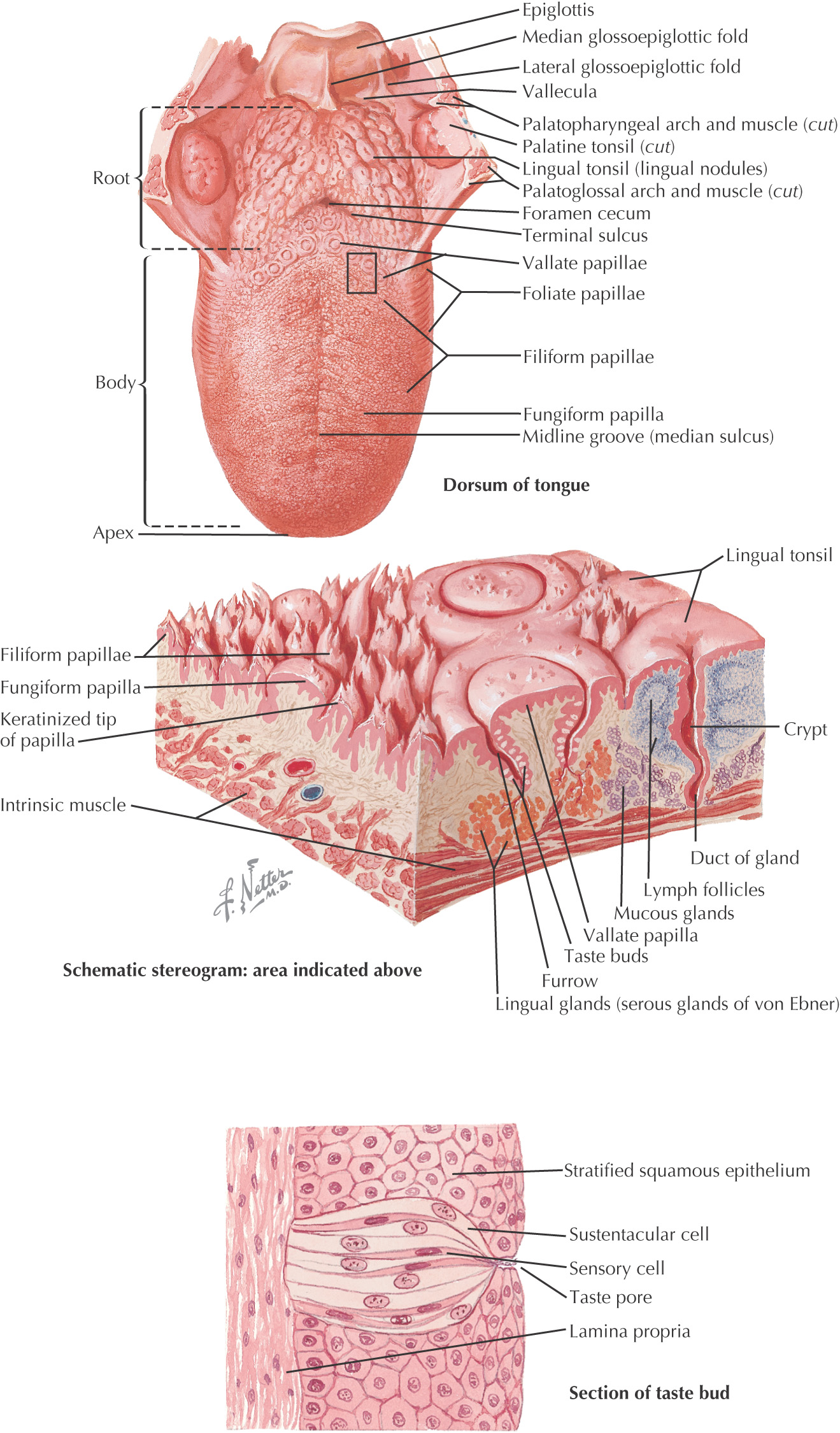
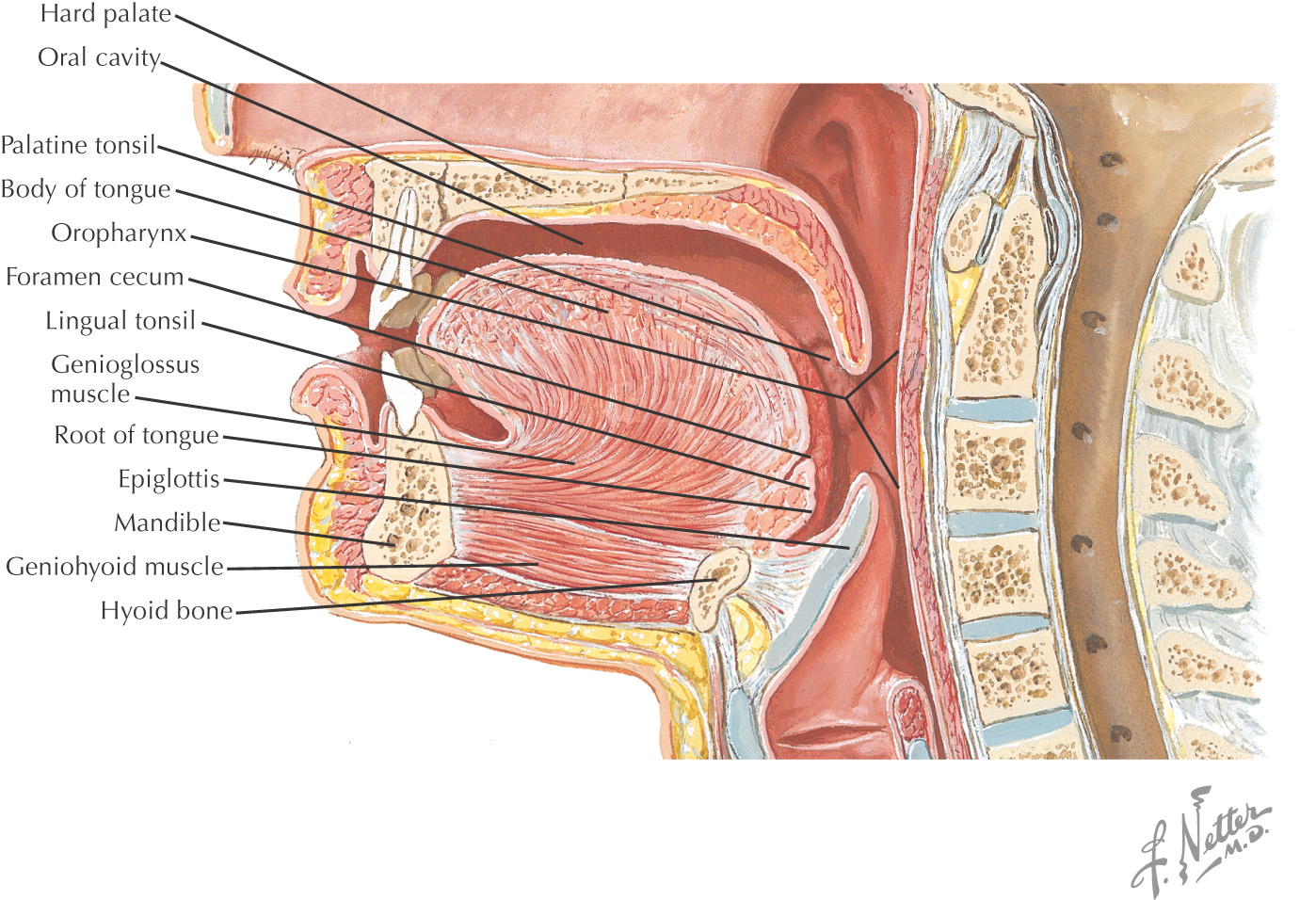
Tongue: a muscular structure in the oral cavity, divided into 2 parts:
Median fibrous septum is thick tissue separating the tongue into halves
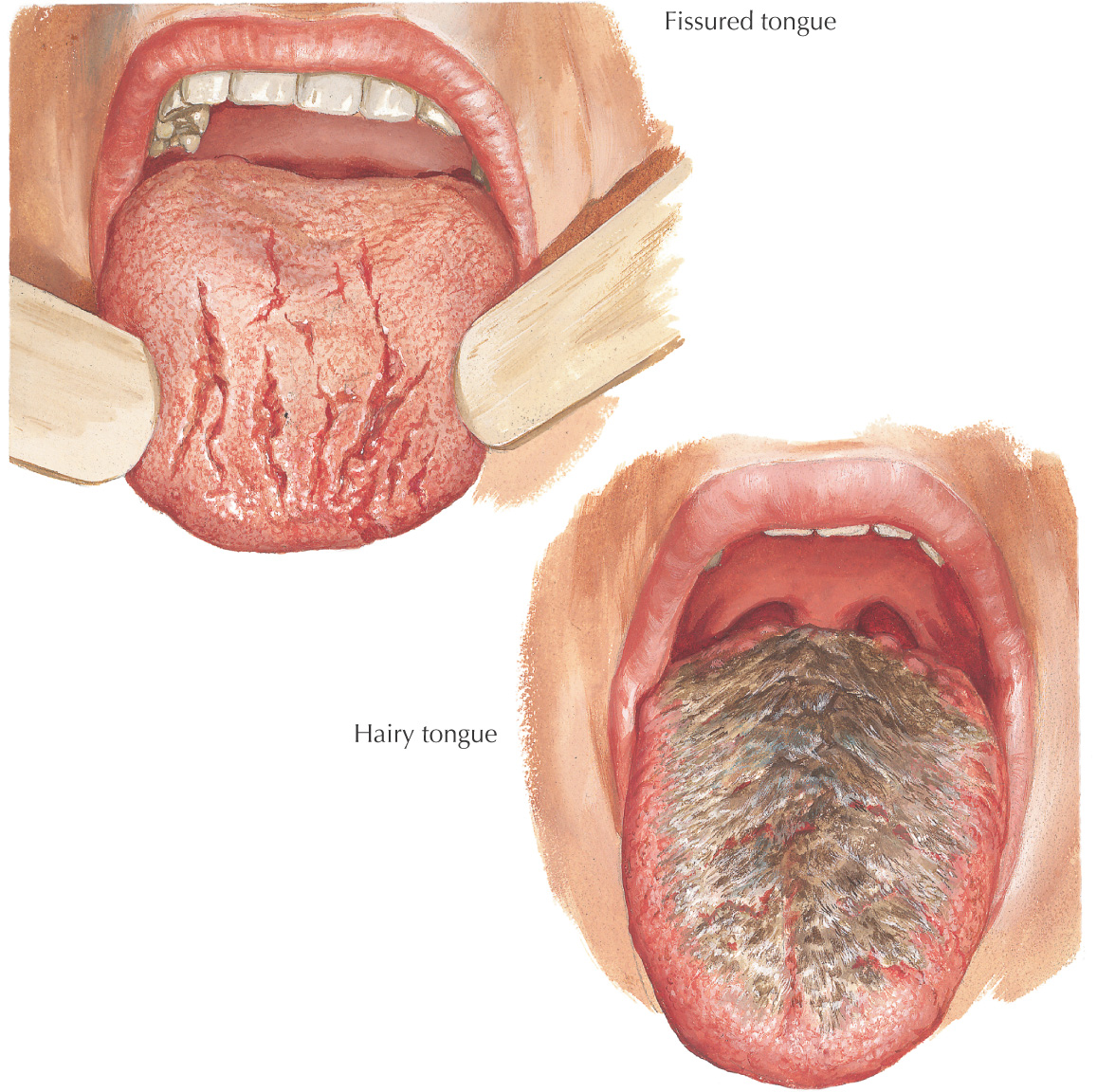
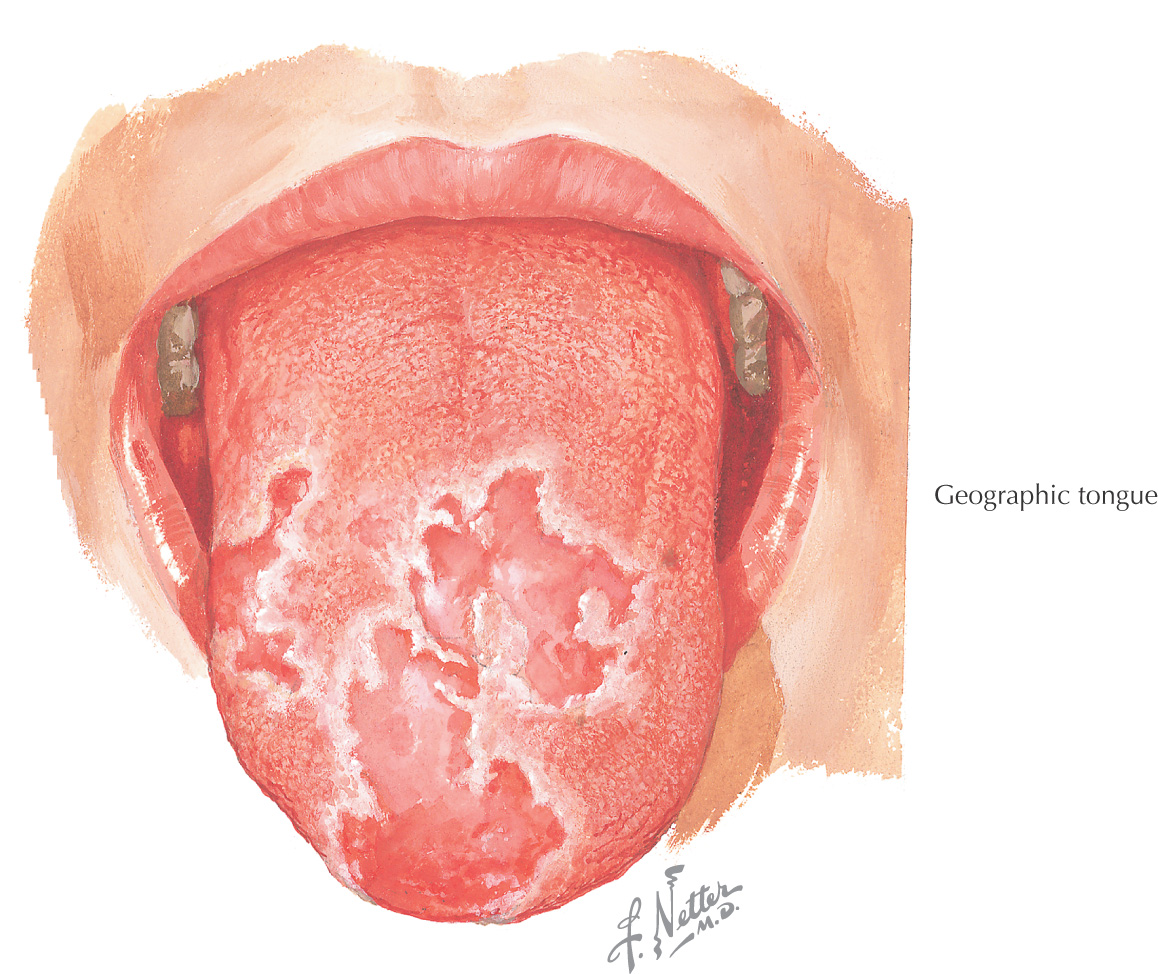
The appearance of the tongue may reflect health problems:
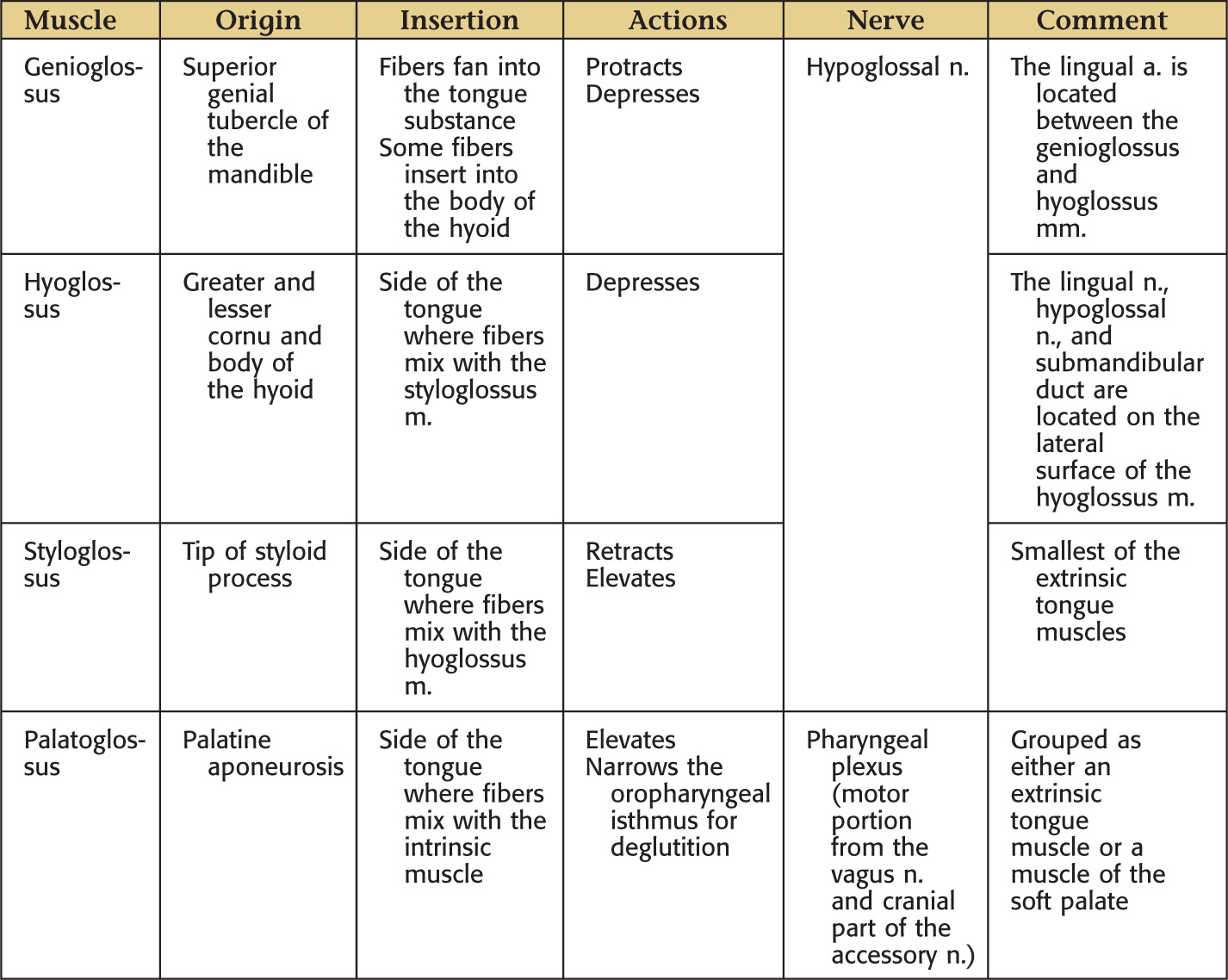
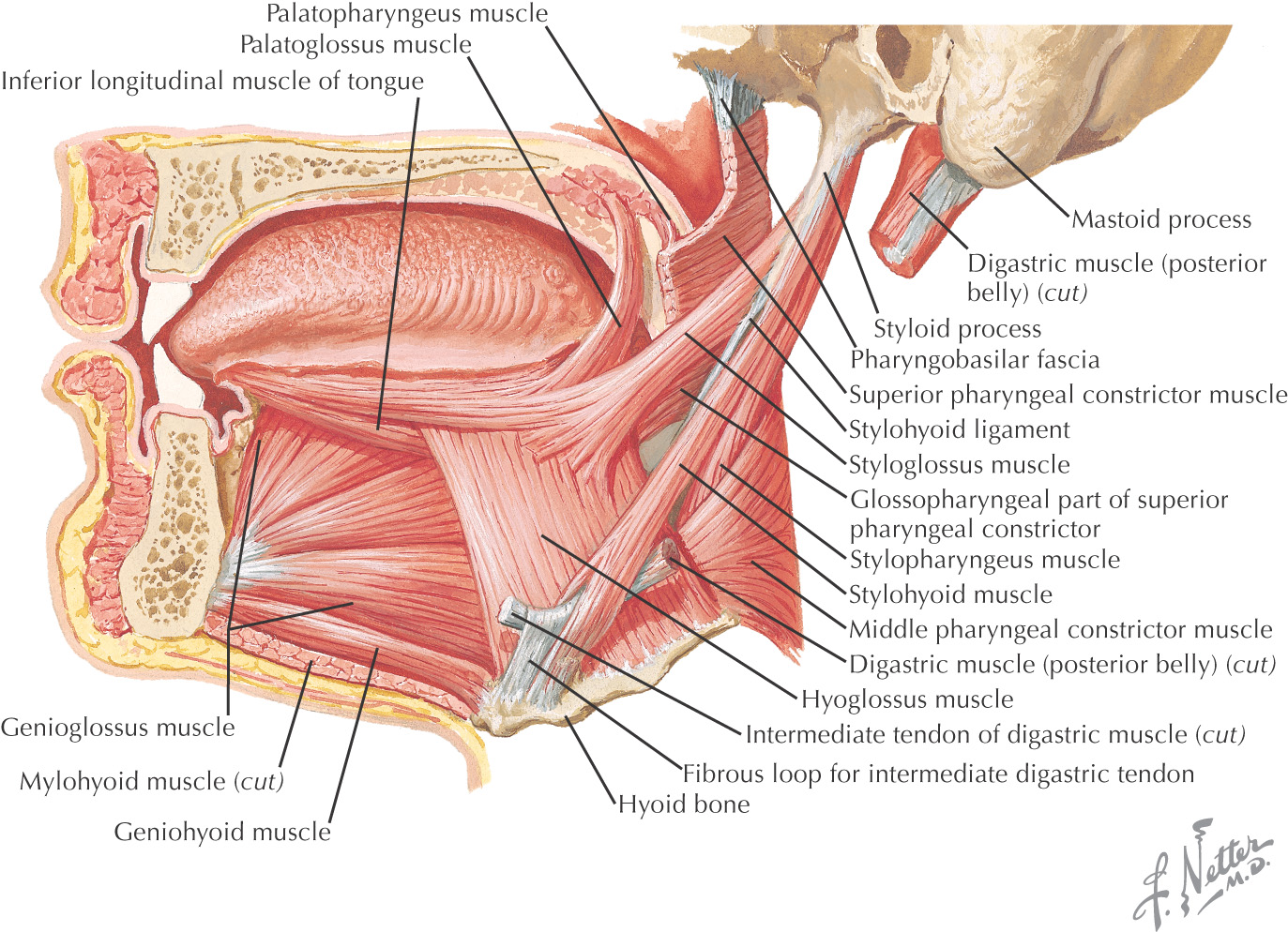
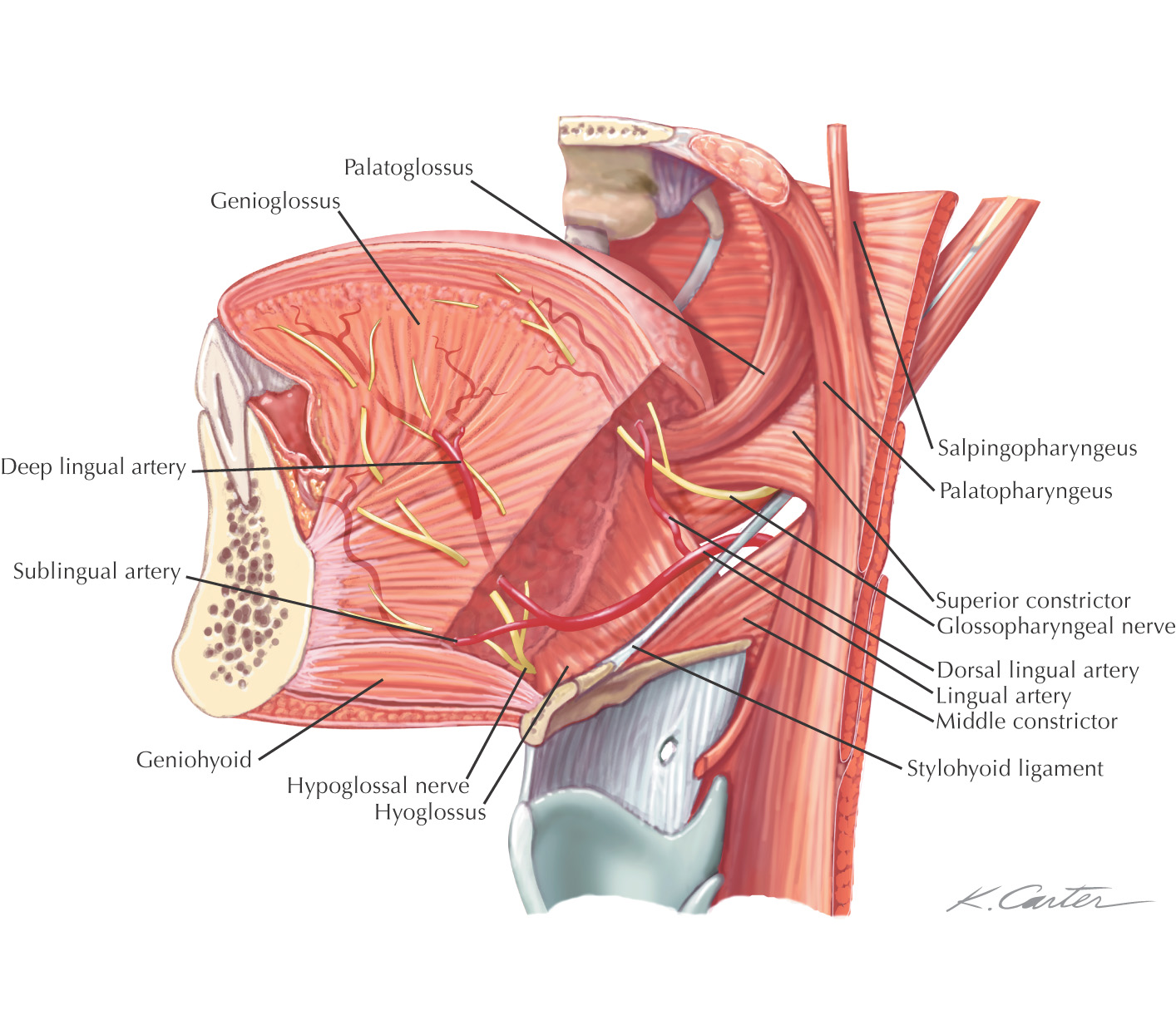
Extrinsic—move the tongue in the oral cavity
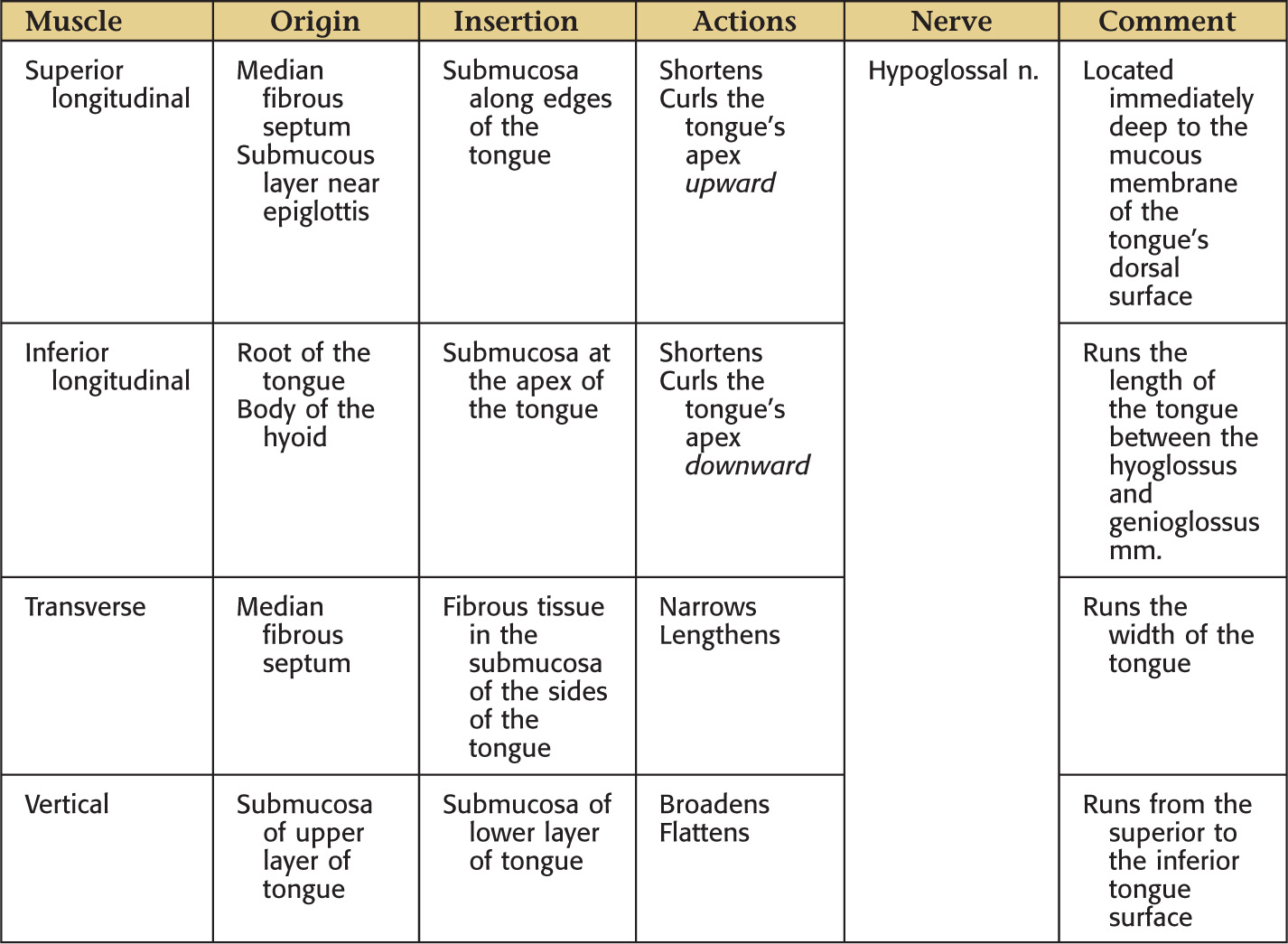
Intrinsic—change the tongue’s shape
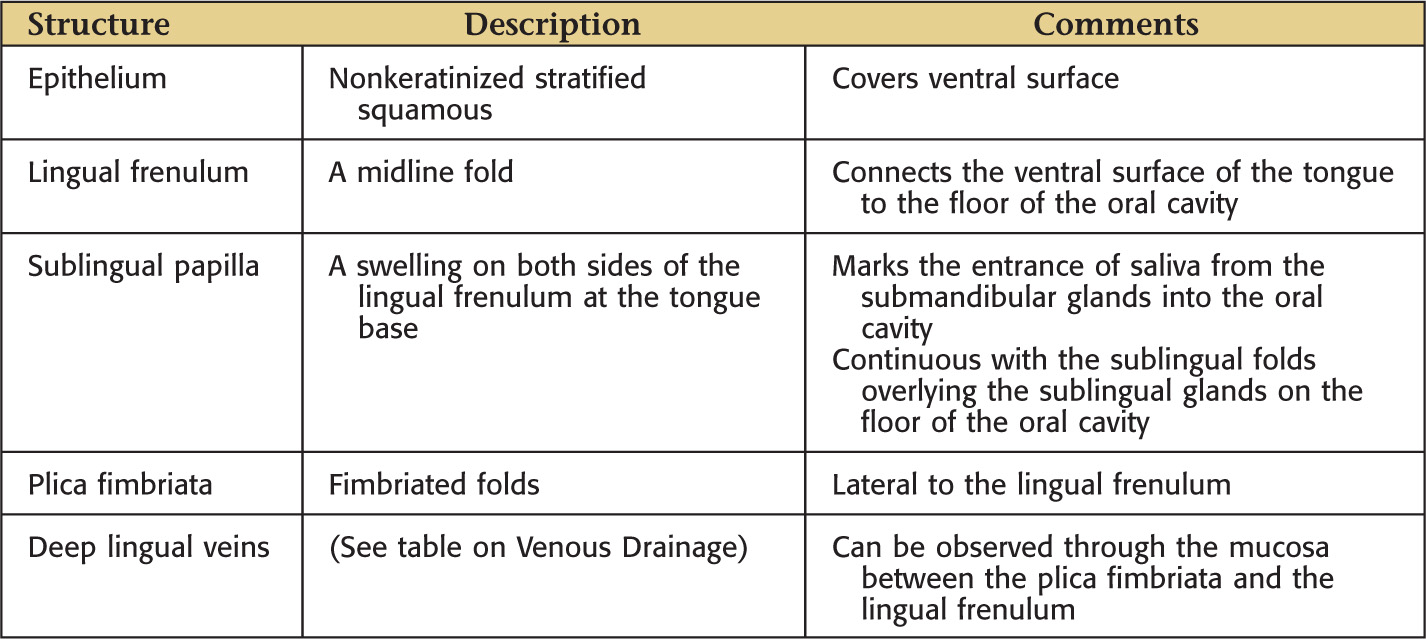
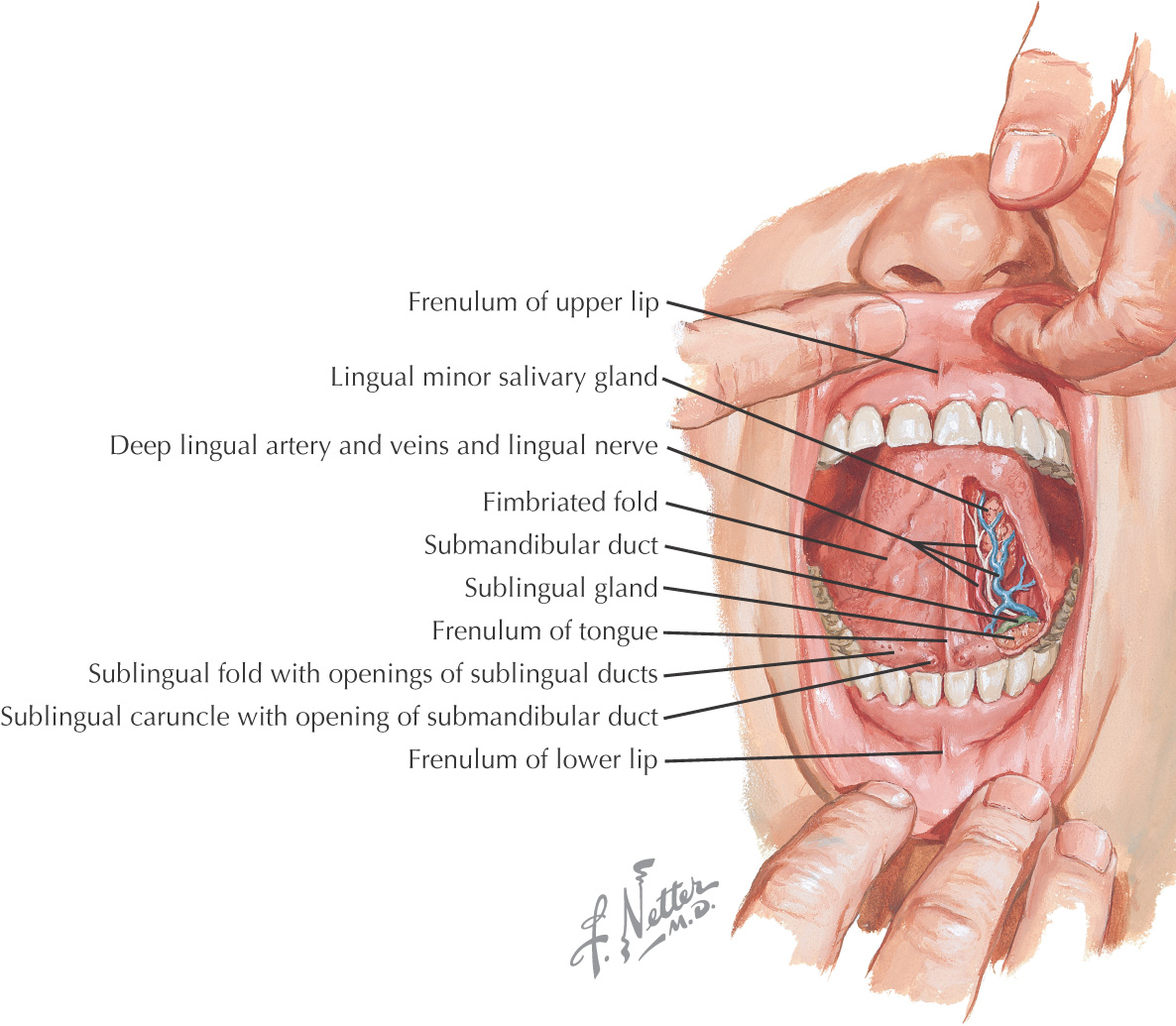
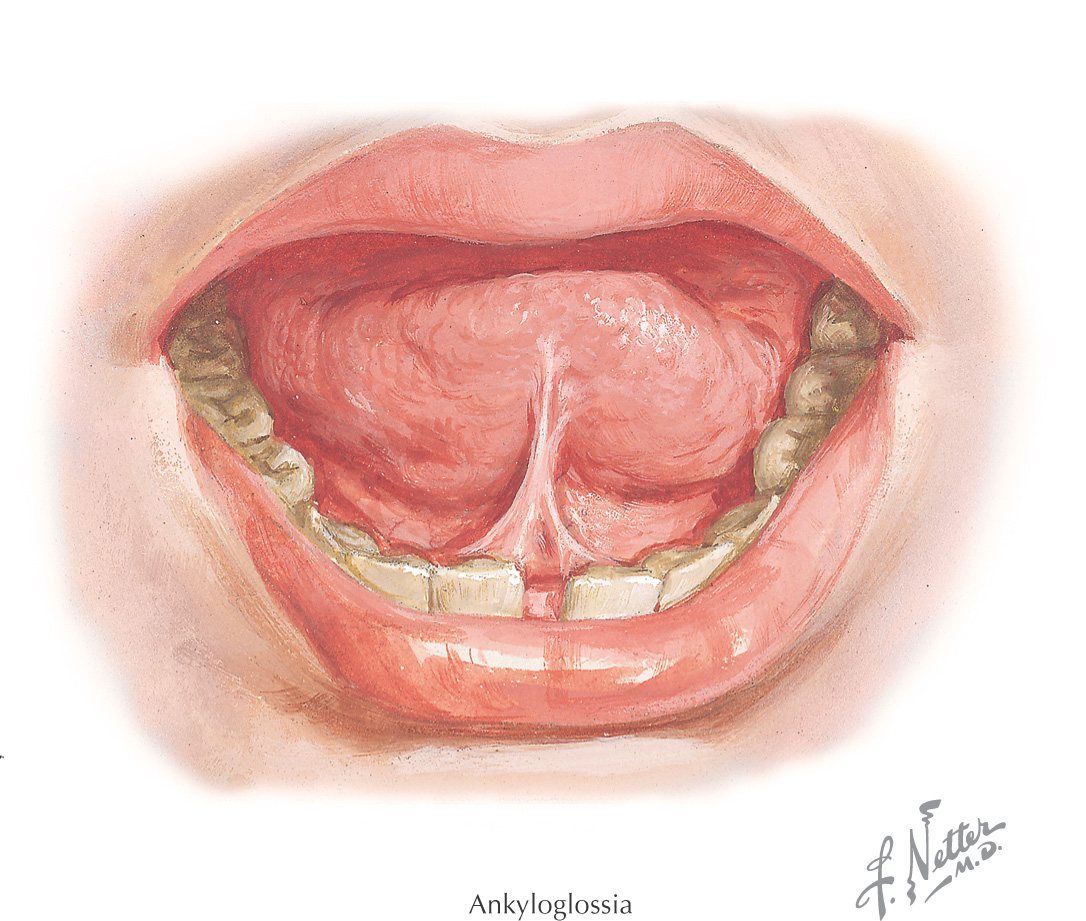
Also known as tongue-tie
Condition in which the lingual frenulum is restricted because of an increase in tissue, which leads to reduced tongue mobility
• Tongue may not be capable of protrusion beyond the incisors
• Tongue may not be capable of touching the palate
• Tongue may manifest a V-shaped notch or may appear bilobed on protrusion
• Causes problems for babies who breastfeed
• If the tongue cannot clear the oral cavity of food, caries, periodontal disease, and halitosis can result
• If condition is severe, can cause a speech impediment
If necessary, the lingual frenulum may be cut (frenectomy)
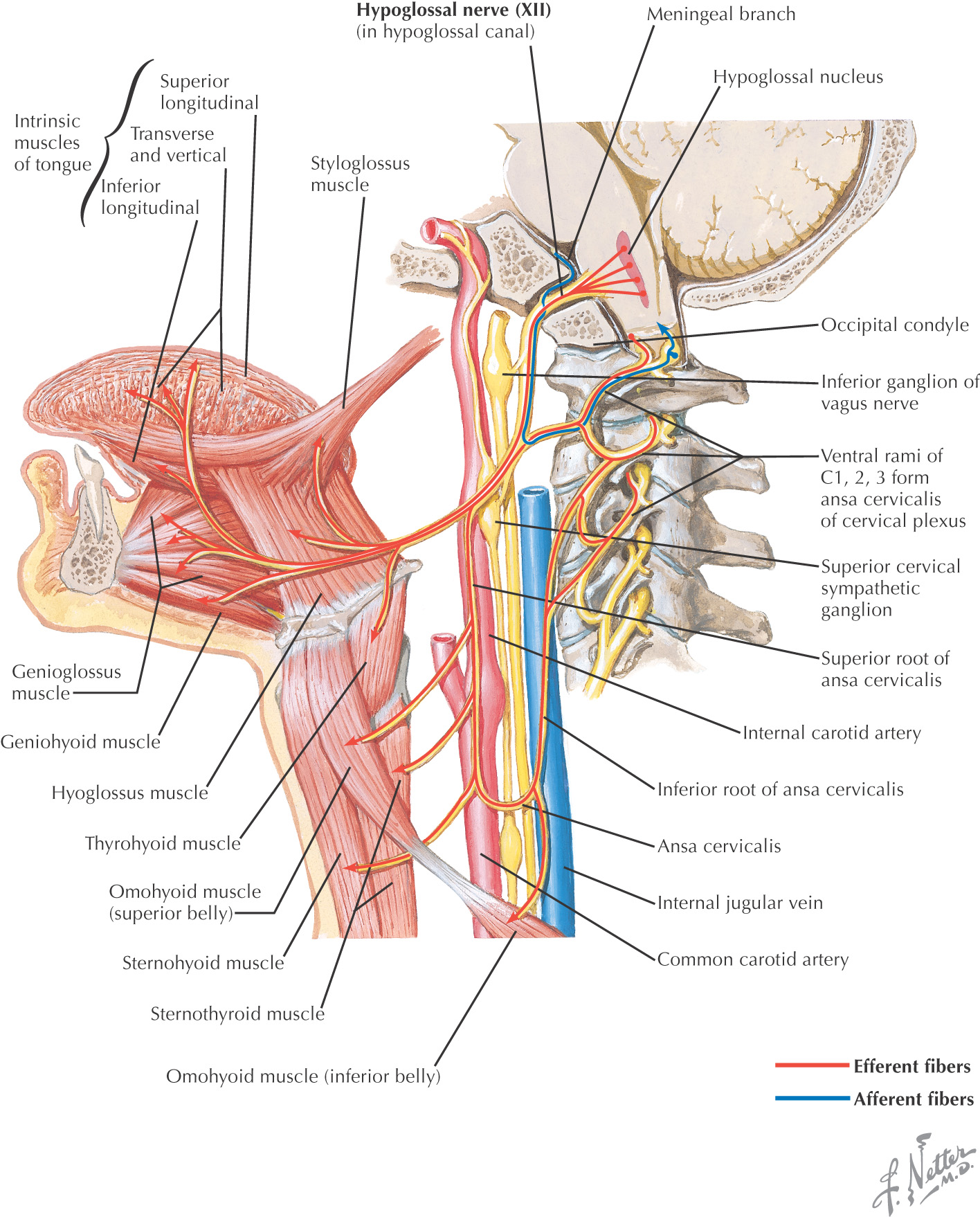
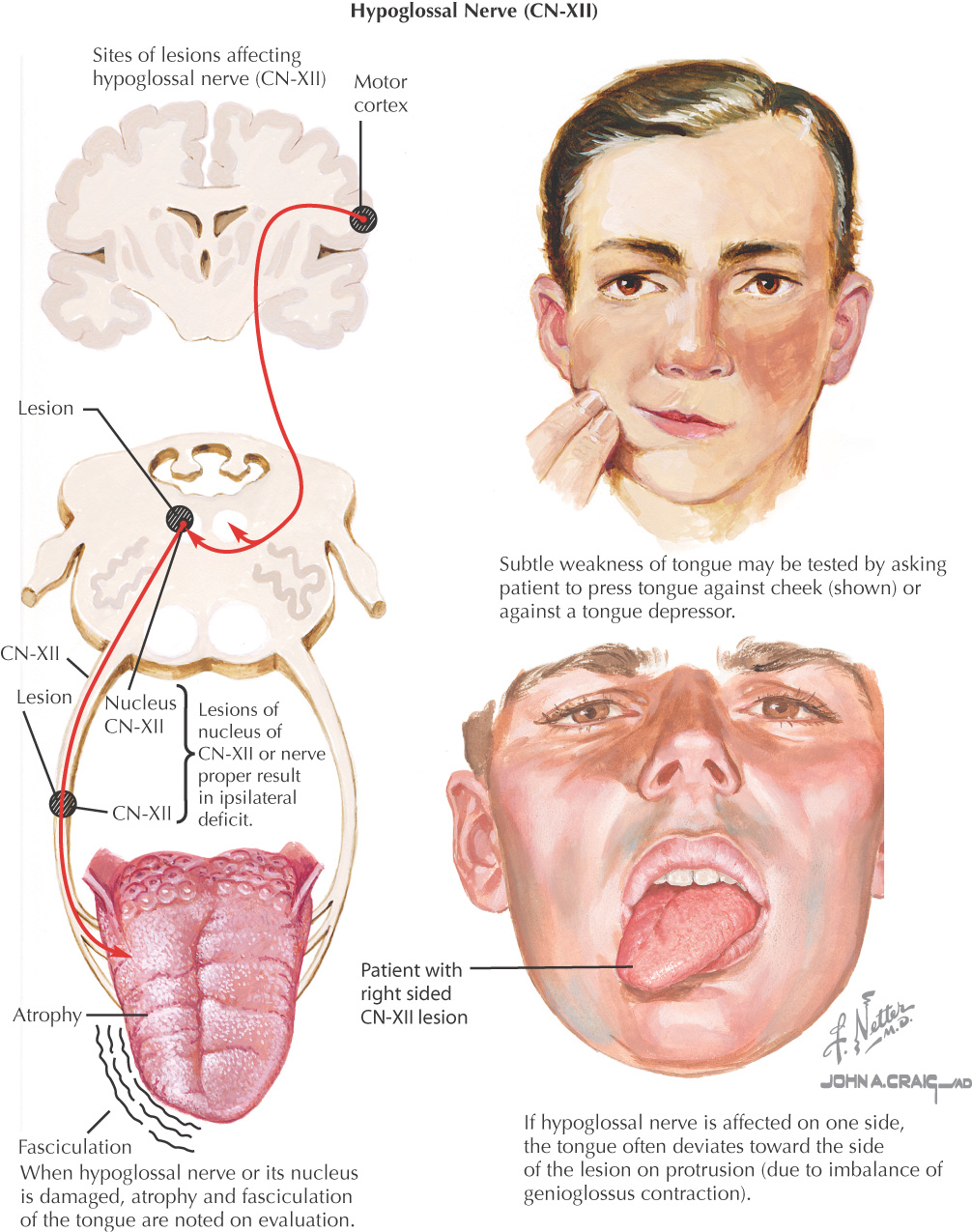
Hypoglossal nerve lesions paralyze the tongue on 1 side
On protrusion, the tongue deviates to the ipsilateral (same) or contralateral side, depending on the lesion site
Lesions to the hypoglossal nerve cause paralysis on the ipsilateral side:
• Tongue deviates to the paralyzed side on protrusion (the paralyzed muscles will lag, causing the tip to deviate)
• Musculature atrophies on the paralyzed side
• Tongue fasciculations occur on the paralyzed side
Example: With a neck wound that cuts the right hypoglossal nerve, the tongue deviates to the right on protrusion, and the right half of the tongue will later demonstrate atrophy and fasciculations
Causes paralysis on the contralateral side:
• Tongue deviates to the side opposite the lesion
• Musculature atrophies on side opposite the lesion
Example: After a stroke on the right side of the brain that affects the right upper motor neurons, the tongue deviates to the left on protrusion, and the left half of the tongue will atrophy
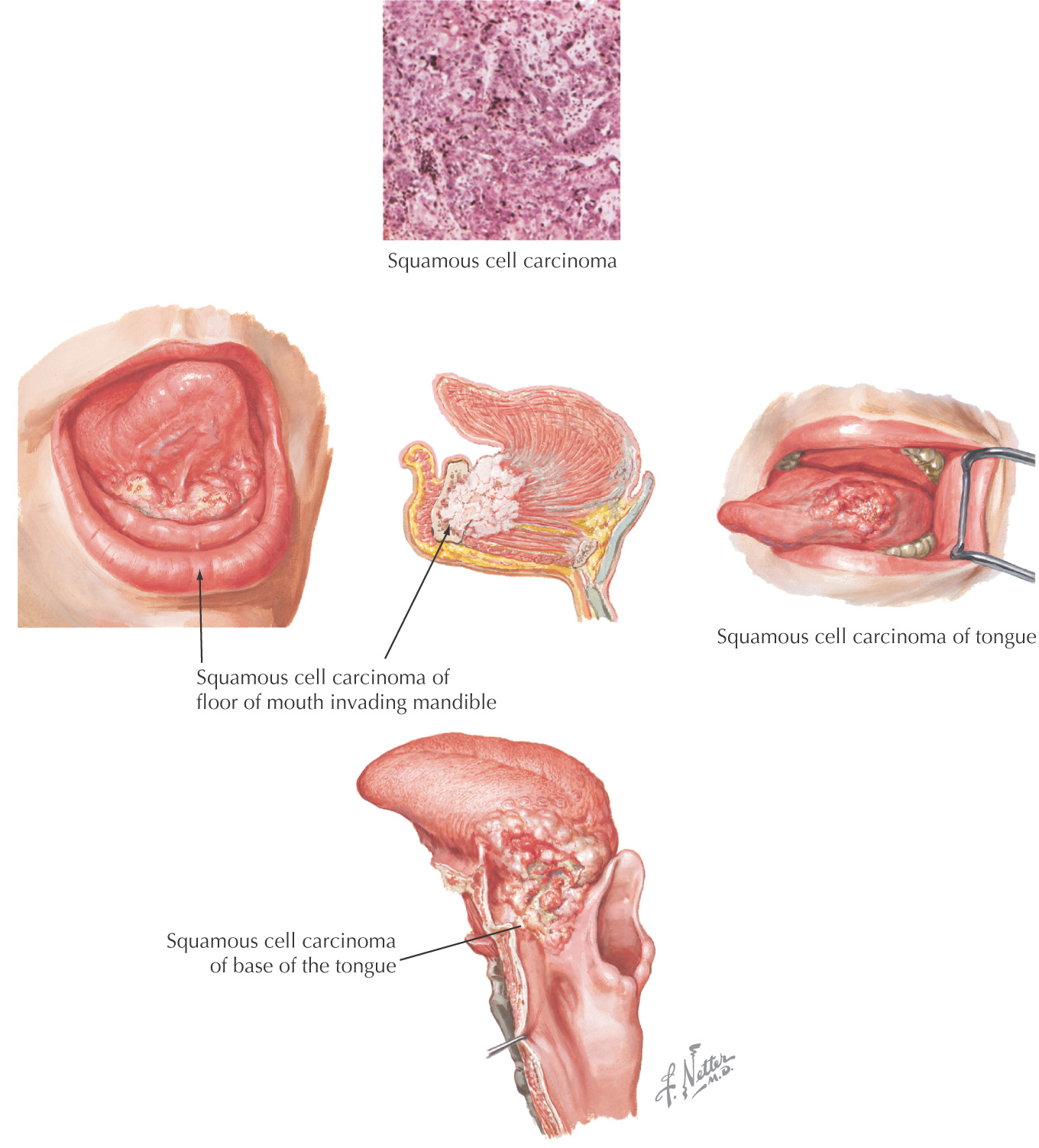
Accounts for most cancers of the oral cavity
In the tongue, usually on the anterolateral aspect
Alcohol and tobacco use are risk factors
Premalignant lesions, such as erythroplasia and leukoplakia, should be identified, because early diagnosis and treatment are paramount in long-term survival
Radiographic imaging helps reveal the tumor’s extent and location
Staging of the tumor guides prognosis
Excision or radiation therapy, or possibly a combination with chemotherapy
If lesion is detected early, excision may suffice
With later tumor stages, a second primary squamous cell carcinoma must be excluded
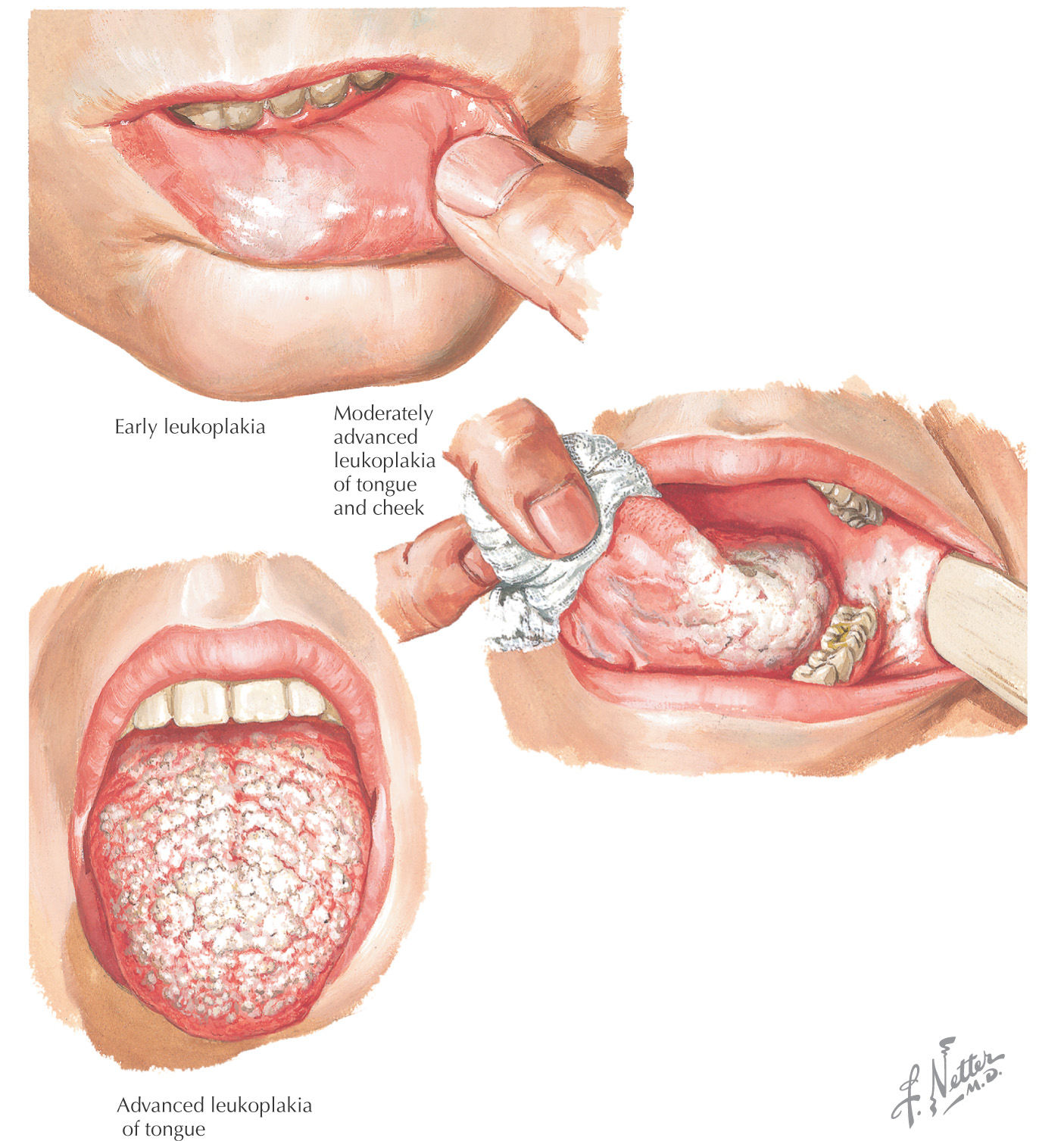
A common premalignant condition of the oral cavity involving the formation of white spots on the mucous membranes of the tongue and inside the mouth
Hairy leukoplakia is a type observed in persons with compromised immune systems
Risk factors:
• Human immunodeficiency virus (HIV) infection
• Epstein-Barr virus infection
Although a precancerous lesion, it may not progress to oral cancer