46 Role of Viruses in Disease
Viruses are obligate intracellular parasites and must replicate in an appropriate host cell to continue to exist. The virus uses the cell’s biochemical machinery to make its components, and then these parts are assembled into new viruses. In many cases, this is lethal to the cell. The cell and innate and immune responses attempt to block the virus replication, kill the infected cell, and prevent the spread of the virus to other sites in the body. Most viral infections cause mild or no symptoms and do not require extensive treatment. When disease occurs, it often results from the spread of the virus to important tissues and the killing of their cells by either virus replication, inflammation, or other host protections. In addition, viruses are excellent inducers of interferon and cytokine production, which results in systemic symptoms, including flulike symptoms.
The common cold, influenza, flulike syndromes, and gastroenteritis are common viral diseases. Other viral infections that target essential tissues and organs can cause serious and even life-threatening disease. In general, the symptoms and severity of a viral infection are determined by (1) the patient’s ability to prevent the spread or rapidly resolve the infection before the virus can reach important organs or cause significant damage, (2) the importance of the target tissue, (3) the virulence of the virus, (4) the extent of immunopathology induced in response to the infection, and (5) the ability of the body to repair the damage.
Immunization by prior infection or vaccination is the best means of protection against viral disease. New vaccines have been developed to allow protection of the populace against even more viruses. Unlike bacteria, there are relatively few targets for the development of antiviral drugs, but drugs are available for certain herpesviruses, for human immunodeficiency virus (HIV), hepatitis B and C viruses (HBV and HCV), and influenza.
In this chapter, viral diseases are discussed with respect to their symptoms, the organ system they target, and the host factors that influence their presentation. Subsequent chapters will discuss the characteristics of the members of specific viral families and the diseases that they cause. A return to this chapter will provide a good review of the viruses.
Viral Diseases
The major sites of viral disease are the respiratory tract; the gastrointestinal tract; the epithelial, mucosal, and endothelial linings of the skin, mouth, and genitalia; the lymphoid tissue; the liver and other organs; and the central nervous system (CNS) (Figure 46-1). The examples given in this chapter represent the more common viral causes of disease.
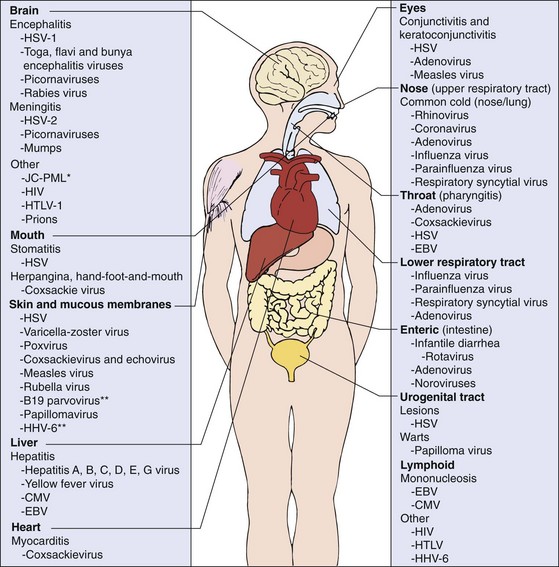
Figure 46-1 Major target tissues of viral disease. Asterisk (*) indicates progressive multifocal leukoencephalopathy. Infection by viruses indicated by double asterisks (**) results in an immune-mediated rash. CMV, Cytomegalovirus; EBV, Epstein-Barr virus; HHV-6, human herpesvirus 6; HIV, human immunodeficiency virus; HSV, herpes simplex virus; HTLV, human T-cell lymphotropic virus; JC-PML, JC papovavirus–induced progressive multifocal leukoencephalopathy.
Oral and Respiratory Tract Infections
The oropharynx and respiratory tract are the most common sites of viral infection and disease (Table 46-1). The viruses are spread in respiratory droplets, aerosols, food, water, and saliva, as well as by close contact and on hands. Similar respiratory symptoms can be caused by several different viruses. For example, bronchiolitis may be caused by respiratory syncytial or parainfluenza virus. Alternatively, one virus may cause different symptoms in different people. Influenza virus can cause a mild upper respiratory tract infection in one person and life-threatening pneumonia in another. Vaccines and antiviral drugs are available for influenza.
Table 46-1 Oral and Respiratory Diseases
| Disease | Etiologic Agent |
|---|---|
| Common cold (including pharyngitis) | Rhinovirus* |
| Coronavirus* | |
| Influenza viruses | |
| Parainfluenza viruses | |
| Respiratory syncytial virus | |
| Metapneumovirus | |
| Adenovirus | |
| Enteroviruses | |
| Pharyngitis | Herpes simplex virus |
| Epstein-Barr virus | |
| Adenovirus* | |
| Coxsackie A virus* (herpangina, hand-foot-and-mouth disease) and other enteroviruses | |
| Croup, tonsillitis, laryngitis, and bronchitis (children younger than 2 years) | Parainfluenza virus 1* |
| Parainfluenza virus 2 | |
| Influenza virus | |
| Adenovirus | |
| Epstein-Barr virus | |
| Bronchiolitis | Respiratory syncytial virus* (infants) |
| Metapneumovirus | |
| Parainfluenza virus 3* (infants and children) | |
| Parainfluenza viruses 1 and 2 | |
| Pneumonia | Respiratory syncytial virus* (infants) |
| Metapneumovirus | |
| Parainfluenza virus* (infants) | |
| Influenza virus* | |
| Adenovirus | |
| Varicella-zoster virus (primary infection of adults or immunocompromised hosts) | |
| Cytomegalovirus (infection of immunocompromised host) | |
| Measles |
Many viral infections start in the oropharynx or respiratory tract, infect the lung, and spread without causing significant respiratory symptoms. Varicella-zoster virus (VZV) and the measles virus initiate infection in the lung and can cause pneumonia but generally cause systemic infections, resulting in an exanthem (rash). Other viruses that establish primary infection of the oropharynx or respiratory tract and then progress to other sites are rubella, mumps, enteroviruses, and several human herpesviruses.
The symptoms and severity of a respiratory viral disease depend on the nature of the virus, the site of infection (upper or lower respiratory tract), and the immune status and age of the person. Conditions such as cystic fibrosis and smoking, which compromise the ciliated and mucoepithelial barriers to infection, increase the risk of serious disease.
Pharyngitis and oral disease are common viral presentations. Most enteroviruses (picornaviruses) infect the oropharynx and then progress by way of a viremia to other target tissues. For example, symptoms such as acute-onset pharyngitis, fever, and oral vesicular lesions are characteristic of Coxsackie A virus infections (herpangina, hand-foot-and-mouth disease) and some Coxsackie B virus and echovirus infections. Adenovirus and the early stages of EBV disease are characterized by sore throat and tonsillitis with exudative membranes; EBV goes on to infect B lymphocytes and cause infectious mononucleosis. HSV causes local primary infections of the oral mucosa and face (gingivostomatitis) and then establishes a latent neuronal infection that can recur in the form of herpes labialis (cold sores, fever blisters). HSV is also a common cause of pharyngitis. HSV and Coxsackie A viruses may also involve the tonsils, but with vesicular lesions.Vesicular lesions on the buccal mucosa (Koplik spots) are an early diagnostic feature of measles infection.
Upper respiratory tract viral infections, including the common cold and pharyngitis, account for at least 50% of absenteeism from schools and the workplace, despite being generally benign. Rhinoviruses and coronaviruses are the predominant causes of upper respiratory tract infections. A runny nose (rhinitis) followed by congestion, cough, sneezing, conjunctivitis, headache, and sore throat are typical symptoms of the common cold. Other causes of the common cold and pharyngitis are specific serotypes of echoviruses and Coxsackie viruses, adenoviruses, influenza viruses, parainfluenza viruses, metapneumovirus, and respiratory syncytial virus.
Tonsillitis, laryngitis, and croup (laryngotracheobronchitis) may accompany certain respiratory tract viral infections. Inflammatory responses to viral infection cause the trachea to narrow below the vocal cords (subglottic area), resulting in laryngitis (adults) and croup (children). This narrowing causes loss of voice; a hoarse, barking cough; and the risk, especially in young children, for a blocked airway and choking. Children infected with parainfluenza viruses are especially at risk for croup.
Lower respiratory tract viral infections can also result in more serious disease. Symptoms of such infections include bronchiolitis (inflammation of the bronchioles), pneumonia, and related diseases. The parainfluenza, metapneumovirus, and respiratory syncytial viruses are major problems for infants and children but cause only asymptomatic infections or common cold symptoms in adults. Parainfluenza 3 virus, and especially respiratory syncytial virus infections, are major causes of life-threatening pneumonia or bronchiolitis in infants younger than 6 months. Infection with these viruses does not provide lifelong immunity.
Influenza virus is probably the best known and most feared of the common respiratory viruses, with the annual introduction of new strains of virus ensuring the presence of immunologically naïve victims. Children are universally susceptible to new strains of virus, whereas older people may have been immunized during a prior outbreak of the annual strain. Despite such immunization, the elderly are especially susceptible to pneumonia caused by new strains of virus because they may not be able to mount a sufficient primary immune response to the new strain of influenza virus or to repair the tissue damage caused by the disease. Influenza infection also increases risk for life-threatening pneumonia by Staphylococcus aureus or streptococcal infections. Other possible viral agents of pneumonia are adenovirus, paramyxoviruses, and primary VZV infections of adults.
Flulike and Systemic Symptoms
Many viral infections cause classic flulike symptoms (e.g., fever, malaise, anorexia, headache, body aches), side effects caused by host responses to the infection. During the viremic phase, many viruses induce the release of interferon and cytokines. In addition to the respiratory viruses, flulike symptoms may accompany infections by arboencephalitis viruses, HSV type 2 (HSV-2), and other viruses.
Arthritis and other inflammatory diseases may result from the cytokine storm and immune hypersensitivity responses induced by the infection or immune complexes containing viral antigen. For example, B19 parvovirus infection of adults, rubella, and infection with some togaviruses elicit arthritis. Immune complex disease that is associated with chronic HBV can result in various presentations, including arthritis and nephritis.
Gastrointestinal Tract Infections
Infections of the gastrointestinal tract can result in gastroenteritis, vomiting, diarrhea, or no symptoms (Box 46-1). Such viruses have a physical structure that can withstand the harsh conditions of the gastrointestinal tract. Norwalk virus, caliciviruses, astroviruses, adenoviruses, reoviruses, and rotaviruses infect the small intestine but not the colon, altering the function or damaging the epithelial lining and the absorptive villi. This leads to the malabsorption of water and an electrolyte imbalance. The resultant diarrhea in older children and adults is generally self-limited and can be treated with rehydration and restoration of the electrolyte balance. These viruses, especially rotavirus, are major problems for adults and children in regions where there is drought and starvation.
Viral gastroenteritis has a more significant effect on infants and may necessitate hospitalization. The extent of tissue damage and consequent loss of fluids and electrolytes may be life threatening. Rotavirus and adenovirus serotypes 40 and 41 are the major causes of infantile gastroenteritis. Vaccines are available for rotavirus.
Fecal-oral spread of the enteric viruses is promoted by poor hygiene and is especially prevalent in day-care centers. Norwalk virus and calicivirus outbreaks affecting older children and adults are generally linked to a common contaminated food or water source. Vomiting usually accompanies diarrhea in patients infected with the Norwalk virus and rotavirus. Although enteroviruses (picornaviruses) are spread by the fecal-oral route, they usually cause only mild or no gastrointestinal symptoms. Instead, these viruses establish a viremia, spread to other target organs, and then cause clinical disease.
Exanthems, Hemorrhagic Fevers, and Arthritides
Virus-induced skin disease (Table 46-2) can result from infection through the mucosa or small cuts or abrasions in the skin (HSV), as a secondary infection after establishment of a viremia (VZV and smallpox) or as a result of the inflammatory response mounted against viral antigens (parvovirus B19). The major classifications of viral rashes are maculopapular, vesicular, nodular, and hemorrhagic. Macules are flat, colored spots. Papules are slightly raised areas of the skin that may result from immune or inflammatory responses rather than the direct effects of the virus. Nodules are larger, raised areas of the skin. Vesicular lesions are blisters and are likely to contain virus. Human papillomaviruses (HPV) cause warts, and molluscum contagiosum causes wartlike growths (nodules) by stimulating the growth of skin cells. There are vaccines for HPV.
| Condition | Etiologic Agent |
|---|---|
| Rash | |
| Rubeola | Measles virus |
| German measles | Rubella virus |
| Roseola infantum | Human herpesvirus 6 |
| Erythema infectiosum | Human parvovirus B19 |
| Boston exanthem | Echovirus 16 |
| Infectious mononucleosis | Epstein-Barr virus, cytomegalovirus |
| Vesicles | |
| Oral or genital herpes | Herpes simplex virus* |
| Chickenpox/shingles | Varicella-zoster virus* |
| Hand-foot-and-mouth disease, herpangina | Coxsackie A virus* |
| Papillomas, etc. | |
| Warts | Papillomavirus* |
| Molluscum | Molluscum contagiosum |
The classic childhood exanthems are roseola infantum (exanthem subitum [HHV-6]), fifth disease (erythema infectiosum [parvovirus B19]), and (in unvaccinated children) varicella, measles, and rubella. The rash follows a viremia and is accompanied by fever. Rashes are also caused by enterovirus, alphavirus, and dengue and other flavivirus infections. They also are occasionally seen in patients with infectious mononucleosis. Vaccines are available for varicella zoster, measles, mumps, and rubella.
The yellow fever virus, dengue virus, Ebola virus, Lassa fever, Sin Nombre virus, and other hemorrhagic fever viruses establish a viremia and infect the endothelial cell lining of the vasculature, possibly compromising the structure of the blood vessel. Viral or immune cytolysis can then lead to greater permeability or rupture of the vessel, producing a hemorrhagic rash with petechiae (pinpoint hemorrhages under the skin) and ecchymoses (massive bruises) and hence internal bleeding, the loss of electrolytes, and shock.
Arthritis can be a consequence of direct infection of the joint or immune responses to viruses such as the togaviruses (e.g., Chikungunya, rubella), parvovirus B19, flaviviruses (e.g., dengue and HCV), HBV, HIV, and human T-cell lymphotropic virus 1 (HTLV-1). Immune complexes containing viral antigen may trigger inflammatory responses, or the virus infection may trigger autoimmune responses, but most viral arthritis is temporary.
Infections of the Eye
Infections of the eye result from direct contact with a virus or from viremic spread (Box 46-2). Conjunctivitis (pinkeye) is a normal feature of many childhood infections and is a characteristic of infections caused by specific adenovirus serotypes (3, 4a, and 7), measles virus, and rubella virus. Keratoconjunctivitis, caused by adenovirus (8, 19a, and 37), HSV, or VZV, involves the cornea and can cause severe damage. HSV disease can recur, causing scarring and blindness. Enterovirus 70 and Coxsackie A24 virus can cause an acute hemorrhagic conjunctivitis. Cataracts are classic features of babies born with congenital rubella syndrome. Chorioretinitis is associated with CMV infection in newborns (congenital) as well as in immunosuppressed people (e.g., those with acquired immunodeficiency syndrome [AIDS]).
Infections of the Organs and Tissues
Infection of the major organs may cause significant disease or may result in further spread or secretion of the virus (see Box 46-2). The symptoms may arise from tissue damage or inflammatory responses.
The liver is a prominent target for many viruses that reach the liver by means of a viremia or the mononuclear phagocyte (reticuloendothelial) system. The liver acts as a source for a secondary viremia but can also be damaged by the infection. The classic symptoms of hepatitis result from infections with hepatitis A, B, C, G, D, and E viruses and yellow fever virus, and they are often associated with EBV infectious mononucleosis and CMV infections. The liver is also a major target in disseminated HSV infection of neonates and infants. Vaccines are available for hepatitis A and B and antiviral drugs for hepatitis B and C.
The heart and other muscles are also susceptible to viral infection and damage. Coxsackie virus can cause myocarditis or pericarditis in newborns, children, and adults. Coxsackie B virus can infect muscle and cause pleurodynia (Bornholm disease). Other viruses (e.g., influenza virus, CMV) can also infect the heart.
Infection of the secretory glands, accessory sexual organs, and mammary glands results in contagious spread of CMV. An inflammatory response to the infection, as occurs in mumps (parotitis, orchitis), may be the cause of the symptoms. CMV infection of the kidney and reactivation are problems for immunosuppressed people and a predominant reason for kidney transplant failure.
Infections of the Central Nervous System
Viral infections of the brain and CNS may cause the most serious viral diseases because of the importance of the CNS and its very limited capacity to repair damage (Box 46-3). Tissue damage is usually caused by a combination of viral pathogenesis and immunopathogenesis. Most neurotropic viral infections do not result in disease, however, because the virus does not reach the brain or does not cause sufficient tissue damage to produce symptoms.
Box 46-3
Central Nervous System Infections
Other
* Most common cause.
Virus may spread to the CNS in blood (arboviruses) or in macrophages (HIV); it may spread from a peripheral infection of the neurons (olfactory), or it may first infect skin (HSV) or muscle (polio, rabies) and then progress to the innervating neurons. The virus may have a predilection for certain sites in the brain. For example, the temporal lobe is targeted in HSV encephalitis, the Ammon horn in rabies, and the anterior horn of the spinal cord and motor neurons for polio.
Viral infections of the CNS are usually distinguished from bacterial infections by the finding of mononuclear cells, low numbers of polymorphonuclear leukocytes, and normal or slightly reduced levels of glucose in the cerebrospinal fluid. Immunoassay detection of specific antigen, polymerase chain reaction detection of viral genomes or messenger RNA, or isolation of the virus from a cerebrospinal fluid or biopsy specimen confirms the diagnosis and identifies the viral agent. The season of the year also facilitates the diagnosis, in that enteroviral and arboviral diseases generally occur during the summer, whereas HSV encephalitis and other viral syndromes may be observed year-round.
Aseptic meningitis is caused by an inflammation and swelling of the meninges that envelopes the brain and spinal cord in response to infection with enteroviruses (especially echoviruses and Coxsackie viruses), HSV-2, the mumps virus, or the lymphocytic choriomeningitis virus. The disease is usually self-limited and, unlike bacterial meningitis, resolves without sequelae unless the virus gains access to and infects neurons or the brain (meningoencephalitis). The viruses gain access to the meninges by means of a viremia.
Encephalitis and myelitis result from a combination of viral pathogenesis and immunopathogenesis in brain tissue and neurons and are either fatal or cause significant damage and permanent neurologic sequelae. HSV, VZV, rabies virus, California encephalitis viruses, West Nile and St. Louis encephalitis viruses, mumps, and measles virus are potential causes of encephalitis. Poliovirus and several other enteroviruses cause paralytic disease (myelitis).
HSV and VZV are ubiquitous and usually cause asymptomatic latent infections of the CNS but can also cause encephalitis. Most arboencephalitis virus infections result in flulike symptoms rather than encephalitis. Postmeasles encephalitis and subacute sclerosing panencephalitis were rare sequelae of measles in the prevaccine era.
Other virus-induced neurologic syndromes are HIV dementia, HTLV-1 tropical spastic paraparesis, JC papovavirus–induced progressive multifocal leukoencephalopathy (PML) in immunosuppressed people, and the prion-associated spongiform encephalopathies (kuru, Creutzfeldt-Jakob disease, Gerstmann-Sträussler-Scheinker disease). PML and the spongiform encephalopathies have long incubation periods.
Hematologic Diseases
Lymphocytes and macrophages are not very permissive for viral replication but are targets for several viruses that establish persistent infections. Viral replication of EBV, HIV, or CMV during the acute phase of infection elicits a large T-cell response, resulting in mononucleosis-like syndromes. In addition, CMV, measles virus, and HIV infections of T cells are immunosuppressive. HIV reduces the numbers of CD4 helper T cells, further compromising the immune system. HTLV-1 infection causes little disease on infection but may lead to adult T-cell leukemia or tropical spastic paraparesis much later in life (Box 46-4).
Macrophages and cells of the macrophage lineage can be infected by many viruses. Macrophages act as vehicles for spreading the virus throughout the body because viruses replicate inefficiently in them, and the cells are generally not lysed by the infection. This process promotes persistent and chronic infections. The macrophage is the primary target cell for the dengue virus. Nonneutralizing antibody can promote uptake of dengue virus and HIV into the cell through Fc receptors. Macrophages and cells of the myeloid lineage are the initial cells infected with HIV and provide a reservoir for the virus and access to the brain. AIDS dementia is thought to result from the actions of HIV-infected macrophages and microglial cells in the brain. Antiviral drugs are available for HIV.
Sexually Transmitted Viral Diseases
Sexual transmission is a major route for the spread of papillomavirus, HSV, CMV, HIV, HTLV-1, HBV, HCV, and hepatitis D virus (HDV) (Box 46-5). Such viruses establish chronic and latent-recurrent infections, with asymptomatic shedding into the semen and vaginal secretions. These viral properties foster dissemination via a route of transmission that is used relatively infrequently and might be avoided during symptomatic disease. The viruses can also be transmitted neonatally or perinatally to infants. Papillomaviruses and HSV establish local primary infections with recurrent disease at the initial site. Lesions and asymptomatic shedding are sources for sexual transmission and for perinatal transmission to the newborn. CMV and HIV infect myeloid and lymphoid cells under the mucosal lining, whereas the hepatitis viruses are delivered to the liver. CMV, HIV, and the hepatitis viruses are present in blood, semen, and vaginal secretions, which can transmit the virus to sexual partners and neonates.
Viruses Spread by Transfusion and Transplantation
HBV, HCV, HDV, HIV, HTLV-1, and CMV are transmitted by blood and organ transplants. These viruses are also present in semen and therefore are sexually transmitted. The chronic nature of the infection, the persistent asymptomatic release of the virus, or the infection of macrophages and lymphocytes promotes transmission by these routes. West Nile encephalitis virus establishes a sufficient viremia for a long enough period that transmission by transfusion has occurred. Screening of the blood supply for HBV, HCV, HIV, and HTLV has controlled transmission of these viruses in blood transfusions (Box 46-6). Blood for babies and organs are screened for CMV, but screening the general blood supply for CMV and other viruses has not been implemented, so the risk for infection remains.
Viruses Spread by Arthropods and Animals
Arthropod-borne viruses (arboviruses) include many of the togaviruses, flaviviruses, bunyaviruses, and the Colorado tick fever reovirus. These viruses establish sufficient viremia in birds or animals (host) to allow their acquisition by mosquitos or ticks (vector) and subsequent transmission to humans when humans enter the habitat of the vector and host. If a virus can establish a sufficient viremia in humans, then the virus, like yellow fever virus, West Nile or St. Louis encephalitis virus, will be spread in an urban setting. Arena, hanta, and rhabdo, viruses are transmitted to humans in saliva, urine, feces or through the bite of an infected animal (Table 46-3). Rabies vaccines are available for individuals whose jobs put them at risk or who are suspected to have been infected with rabies.
Table 46-3 Arboviruses and Zoonoses
| Virus | Family | Reservoir/Vector |
|---|---|---|
| Eastern equine encephalitis | Togaviridae | Birds/Aedes mosquito |
| Western equine encephalitis | Togaviridae | Birds/Culex mosquito |
| West Nile encephalitis | Flaviviridae | Birds/Culex mosquito |
| St. Louis encephalitis | Flaviviridae | Birds/Culex mosquito |
| California encephalitis | Bunyaviridae | Small mammals/Aedes mosquito |
| La Crosse encephalitis | Bunyaviridae | Small mammals/Aedes mosquito |
| Yellow fever | Flaviviridae | Birds/Aedes mosquito |
| Dengue | Flaviviridae | Monkeys/Aedes mosquito |
| Colorado tick fever | Reoviridae | Tick |
| Lymphocytic choriomeningitis | Arenaviridae | Rodents |
| Lassa fever | Arenaviridae | Rodents |
| Sin Nombre hantavirus | Bunyaviridae | Deer mice |
| Ebola | Filoviridae | Unknown |
| Rabies | Rhabdoviridae | Bats, foxes, raccoons, etc. |
| Influenza A | Orthomyxoviridae | Birds, swine, etc. |
Syndromes of Possible Viral Etiology
Several diseases either produce symptoms or have epidemiologic or other characteristics that resemble those of viral infections or may be the sequelae of viral infections (e.g., inflammatory responses to a persistent viral infection). They include multiple sclerosis, Kawasaki disease, arthritis, diabetes, and chronic fatigue syndrome. Also, the strong cytokine response to many virus infections may trigger a loss of tolerance to self-antigens to initiate autoimmune diseases.
Chronic and Potentially Oncogenic Infections
Chronic infections occur when the immune system has difficulty resolving the infection. The DNA viruses (except parvovirus and poxvirus) and the retroviruses cause latent infections with the potential for recurrence. CMV and other herpesviruses; hepatitis B, C, G, and D viruses; and retroviruses cause chronic, productive infections.
HBV, HCV, EBV, HHV-8, HPV, and HTLV-1 are associated with human cancers. EBV, HPV, and HTLV-1 can immortalize cells; after immortalization, cofactors, chromosomal aberrations, or both, enable a clone of virus-containing cells to grow into a cancer. EBV normally causes infectious mononucleosis but is also associated with African Burkitt lymphoma, Hodgkin lymphoma, lymphomas in immunosuppressed individuals, and nasopharyngeal carcinoma; HTLV-1 is associated with human adult T-cell leukemia. Many papillomaviruses induce a simple hyperplasia characterized by the development of a wart; however, several other strains of HPV have been associated with human cancers (e.g., type 16 and 18 are associated with cervical carcinoma). Direct viral action or the inflammation and chronic cell damage and repair in livers infected by HBV or HCV can result in a tumorigenic event leading to hepatocellular carcinoma. HSV-2 has been associated with human cervical carcinoma, most likely as a cofactor. Immunosuppression in patients who have AIDS, patients undergoing cancer chemotherapy, or transplant recipients also allow the production of lymphoma by EBV. HHV-8 infection produces many cytokines to stimulate cell growth, and this growth can progress to Kaposi sarcoma, especially in persons with AIDS.
Vaccines are now available for HBV and high-risk HPV strains. Development of a worldwide vaccine program for HBV not only would reduce the spread of viral hepatitis but also would prevent the occurrence of primary hepatocellular carcinoma. Similarly, the HPV vaccines should also reduce the incidence of cervical carcinoma.
Infections in Immunocompromised Patients
Patients with deficient cell-mediated immunity are generally more susceptible to infection with enveloped viruses (especially the herpesviruses, measles virus, and even the vaccinia virus used for smallpox vaccinations) and to recurrences of infections with latent viruses (herpesviruses and papovaviruses). Severe T-cell deficiencies also affect the antiviral antibody response. Cell-mediated immunodeficiencies can be congenital or acquired. They may result from genetic defects (e.g., Duncan disease, DiGeorge syndrome, Wiskott-Aldrich syndrome), leukemia or lymphoma, infections (e.g., AIDS), or immunosuppressive therapy.
Viruses cause atypical and more severe presentations in immunosuppressed people. For example, infections with herpesviruses (e.g., HSV, CMV, VZV) or the vaccinia smallpox vaccine, which are normally benign and localized, can progress locally or may disseminate and cause visceral and neurologic infections that can be life threatening. A measles infection might cause a giant cell (syncytial) pneumonia rather than the characteristic rash.
People with immunoglobulin A deficiency or hypogammaglobulinemia (antibody deficiency) have more problems with respiratory and gastrointestinal viruses. Hypogammaglobulinemic people are more likely to suffer significant disease after infection by viruses that progress by viremia, which also include the live polio vaccine, echovirus, and VZV.
Congenital, Neonatal, and Perinatal Infections
The development and growth of the fetus are so ordered and rapid that a viral infection can damage or prevent the appropriate formation of important tissues, leading to miscarriage or congenital abnormalities. Infection can occur in utero (prenatal; e.g., rubella, parvovirus B19, CMV, HIV), during transit through the birth canal by contact with lesions or blood (neonatal, e.g., HSV, HBV, CMV, HPV), or soon after birth (postnatal, e.g., HIV, CMV, HBV, HSV, Coxsackie B virus, echovirus).
Neonates depend on the mother’s immunity to protect them from viral infections. They receive maternal antibodies through the placenta and then in the mother’s milk. This type of passive immunity can remain effective for 6 months to a year after birth. Maternal antibodies can (1) protect against spread of virus to the fetus during a viremia (e.g., rubella, B19), (2) protect against many enteric and respiratory tract viral infections, and (3) reduce the severity of other viral diseases after birth. Nevertheless, because the cell-mediated immune system is not mature at birth, newborns are susceptible to viruses that spread by cell-to-cell contact (e.g., respiratory syncytial virus, HSV, VZV, CMV, HIV).
Rubella virus and CMV are examples of teratogenic viruses that can cause congenital infection and severe congenital abnormalities. HIV infection acquired in utero or from mother’s milk initiates a chronic infection, leading to lymphadenopathy, failure to thrive, or encephalopathy within 2 years of birth. HSV can be acquired during passage through an infected birth canal and can result in life-threatening disseminated disease. Nosocomial infection of newborns can result in a similar outcome. If parvovirus B19 is acquired in utero, it can cause spontaneous abortion.
Atkinson W, Wolfe S, Hamborsky J. Epidemiology and prevention of vaccine-preventable diseases, ed 12. Public Health Foundation: Washington, DC, 2011.
Centers for Disease Control and Prevention. Guidelines for prevention of transmission of human immunodeficiency virus and hepatitis B virus to health-care and public-safety workers. MMWR Morb Mortal Wkly Rep. 1989;38(Suppl 6):1–37.
Cohen J, Powderly WG. Infectious diseases, ed 2. St Louis: Mosby; 2004.
Ellner Emond RTD, Rowland HAK, Welsby P. Colour atlas of infectious diseases, ed 4. London: Mosby; 2003.
Gershon AA, Hotez PJ, Katz SL. Krugman’s infectious diseases of children, ed 11. St Louis: Mosby; 2004.
Goering R, et al. Mim’s medical microbiology, ed 4. Edinburgh: Mosby; 2008.
Gorbach SL, Bartlett JG, Blacklow NR. Infectious diseases, ed 3. Philadelphia: WB Saunders; 2004.
Hart CA, Broadhead RL. Color atlas of pediatric infectious diseases. St Louis: Mosby; 1992.
Haukenes G, Haaheim LR, Pattison JR. A practical guide to clinical virology. New York: Wiley; 1989.
Knipe DM, et al. Fields virology, ed 5. Philadelphia: Lippincott Williams & Wilkins; 2006.
Logan SAE, MacMahon E. Viral meningitis. BMJ. 2008;336:36–40.
Mandell GL, Bennet JE, Dolin R. Principles and practice of infectious diseases, ed 6. Philadelphia: Churchill Livingstone; 2005.
Outhred AC, Kok J, Dwyer DE. Viral arthritides. Expert Rev Antiinfect Ther. 2011;9:545–554.
Strauss JM, Strauss EG. Viruses and human disease, ed 2. San Diego: Academic; 2007.
White DO, Fenner FJ. Medical virology, ed 4. Orlando, Fla: Academic; 1994.
All the virology on the WWW. www.virology.net/garryfavweb.html. Accessed May 14, 2012.
The big picture book of viruses. www.virology.net/Big_Virology/BVHomePage.html. Accessed May 14, 2012.
Centers for Disease Control and Prevention. CDC A-Z index. www.cdc.gov/health/diseases.htm. Accessed May 14, 2012
Centers for Disease Control and Prevention. Traveler’s health. www.cdc.gov/travel/diseases.htm. Accessed May 14, 2012
National Center for Infectious Diseases. Infectious disease information A-Z index. www.cdc.gov/ncidod/diseases/index.htm. Accessed May 14, 2012
National Foundation for Infectious Diseases. Fact sheets on diseases. www.nfid.org/factsheets/Default.html. Accessed May 14, 2012
Stannard L. Virus ultra structure. www.uct.ac.za/depts/mmi/stannard/linda.html. Accessed May 14, 2012
World Health Organization. Immunization service delivery. www.who.int/immunization_delivery/en/. Accessed May 14, 2012
World Health Organization. Infectious diseases. www.who.int/topics/infectious_diseases/en/. Accessed May 14, 2012