52 Poxviruses
A goat herder has a large vesicular lesion on his index finger.
1. How does the orf virus infecting this individual resemble smallpox?
2. What was the source, and how was it acquired?
3. How is replication of this virus different from other DNA viruses?
4. Why was it possible to eradicate wild-type smallpox virus?
Answers
1. Orf virus is a poxvirus with a large DNA genome and a complex virion structure; it replicates in the cytoplasm and causes a vesicular lesion. Unlike smallpox, it is a zoonose: it is transmitted by contact and does not spread from the site of infection.
2. Orf virus is the poxvirus of sheep and goats.
3. Poxviruses replicate in the cytoplasm and, as a result, must be able to transcribe its genome in the cytoplasm, which requires encoding of a DNA-dependent RNA polymerase and other enzymes that are present in the nucleus of the host.
4. Wild-type smallpox is strictly a human virus (no animal reservoirs), it always causes disease signs (allows identification of infected individuals), there is only one serotype, and an effective vaccine is available. Immunization with other poxviruses, such as vaccinia virus, protects against smallpox virus.
The poxviruses include the human viruses variola (smallpox) (genus Orthopoxvirus) and molluscum contagiosum (genus Molluscipoxvirus), as well as some viruses that naturally infect animals but can cause incidental infection in humans (zoonosis). Many of these viruses share antigenic determinants with smallpox, allowing the use of an animal poxvirus for a human vaccine.
In 18th century England, smallpox accounted for 7% to 12% of all deaths and the deaths of one third of children. However, the development of the first live vaccine in 1796 and the later worldwide distribution of this vaccine led to the eradication of smallpox by 1980. As a result, reference stocks of smallpox virus in two World Health Organization (WHO) laboratories were destroyed in 1996 after an international agreement to do so was reached. Unfortunately, smallpox did not disappear. Stocks of the virus still exist in the United States and in Russia. Although the world was successfully eliminating natural smallpox, the former Union of Soviet Socialist Republics (U.S.S.R.) was stockpiling immense amounts of weaponized smallpox virus for biowarfare. Smallpox is considered a category A agent by the U.S. Centers for Disease Control and Prevention (CDC), along with anthrax, plague, botulism, tularemia, and viral hemorrhagic fevers, because of their great potential as bioterrorism-biowarfare agents capable of large-scale dissemination and serious disease. The potential for these stocks of smallpox to be acquired and used by a terrorist has been the impetus to renew interest in developing new smallpox vaccine programs and antiviral drugs.
On a positive note, the vaccinia and canarypox viruses have found a beneficial use as gene delivery vectors and for the development of hybrid vaccines. These hybrid viruses contain and express the genes of other infectious agents, and infection results in immunization against both agents.
Structure and Replication
Poxviruses are the largest viruses, almost visible on light microscopy (Box 52-1). They measure 230 × 300 nm and are ovoid to brick shaped with a complex morphology. The poxvirus virion particle must carry many enzymes, including a deoxyribonucleic acid (DNA)-dependent ribonucleic acid (RNA) polymerase, to allow viral messenger RNA (mRNA) synthesis to occur in the cytoplasm. The viral genome consists of a large, double-stranded, linear DNA that is fused at both ends. The structure and replication of vaccinia virus is representative of the other poxviruses (Figure 52-1). The genome of vaccinia virus consists of approximately 189,000 base pairs.
Box 52-1
Unique Properties of Poxviruses
Poxviruses are the largest, most complex viruses.
Poxviruses have complex, oval to brick-shaped morphology with internal structure.
Poxviruses have a linear, double-stranded DNA genome with fused ends.
Poxviruses are DNA viruses that replicate in the cytoplasm.
Virus encodes and carries all proteins necessary for mRNA synthesis.
Virus also encodes proteins for functions such as DNA synthesis, nucleotide scavenging, and immune escape mechanisms.
Virus is assembled in inclusion bodies (Guarnieri bodies; factories), where it acquires its outer membranes.
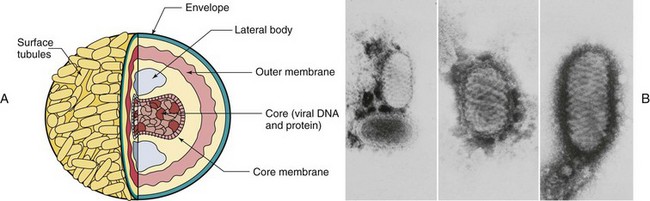
Figure 52-1 A, Structure of the vaccinia virus. Within the virion, the core assumes the shape of a dumbbell because of the large lateral bodies. Virions have a double membrane; the “outer membrane” assembles around the core in the cytoplasm, and the virus leaves the cell by exocytosis or upon cell lysis. B, Electron micrographs of orf virus. Note its complex structure.
The replication of poxviruses is unique among the DNA-containing viruses, in that the entire multiplication cycle takes place within the host cell cytoplasm (Figure 52-2). Thus, poxviruses must encode the enzymes required for mRNA and DNA synthesis, as well as activities other DNA viruses normally obtain from the host cell.
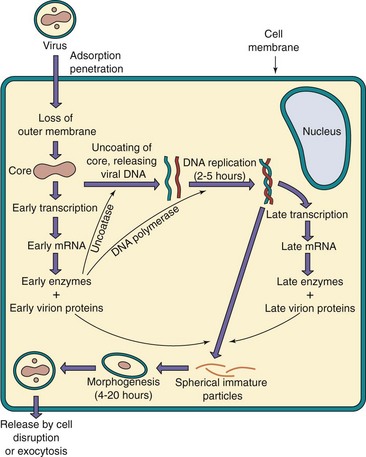
Figure 52-2 Replication of vaccinia virus. The core is released into the cytoplasm, where virion enzymes initiate transcription. A viral-encoded “uncoatase” enzyme then causes the release of DNA. Viral polymerase replicates the genome, and late transcription occurs. DNA and protein are assembled into cores with the core membrane. An outer membrane shrouds the core containing the lateral bodies and the enzymes required for infectivity. The virion buds through the plasma membrane or is released by cell lysis.
After binding to a cell surface receptor, the poxvirus outer envelope fuses with cellular membranes, either at the cell surface or within the cell. Early gene transcription is initiated on removal of the outer membrane. The virion core contains a specific transcriptional activator and all the enzymes necessary for transcription, including a multisubunit RNA polymerase, as well as enzymes for polyadenylate addition and capping mRNA. Among the early proteins produced is an uncoating protein (uncoatase) that removes the core membrane, thereby liberating viral DNA into the cell cytoplasm. Viral DNA then replicates in electron-dense cytoplasmic inclusions (Guarnieri inclusion bodies), referred to as factories. Late viral mRNA for structural, virion, and other proteins is produced after DNA replication. In poxviruses, unlike other viruses, the membranes assemble around the core factories. Approximately 10,000 viral particles are produced per infected cell. Different forms of virus are released by exocytosis or upon cell lysis, but both are infectious.
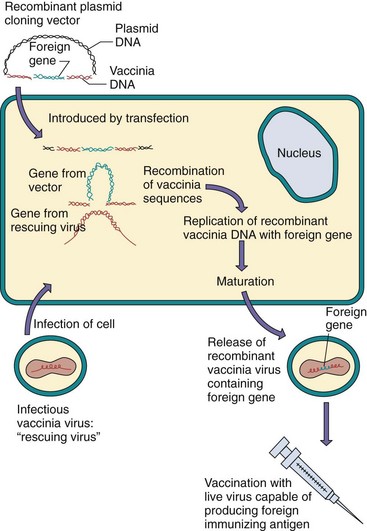
The vaccinia and canarypox viruses are being used as expression vectors to produce live recombinant/hybrid vaccines for more virulent infectious agents (Figure 52-3). For this process, a plasmid is constructed that contains the foreign gene that encodes the immunizing molecule, flanked by specific poxvirus gene sequences to promote recombination. This plasmid is inserted into a host cell, which is then infected with the poxvirus. The foreign gene is incorporated into the “rescuing” poxvirus genome because of the homologous viral sequences included on the plasmid. Immunization with the recombinant poxvirus results from expression of the foreign gene and its presentation to the immune response, almost as if by infection with the other agent. A vaccinia hybrid virus containing the G protein of rabies virus soaked onto a bait food and dropped into forests has been used successfully to immunize raccoons, foxes, and other mammals. Experimental vaccines for human immunodeficiency virus, hepatitis B, influenza, and other viruses have also been prepared using these techniques. The potential for producing other vaccines in this manner is unlimited.
Pathogenesis and Immunity
After being inhaled, smallpox virus replicates in the upper respiratory tract (Figure 52-4). Dissemination occurs via lymphatic and cell-associated viremic spread. Internal and dermal tissues are inoculated after a second, more intense viremia, causing the simultaneous eruption of the characteristic “pocks.” Molluscum contagiosum and the other poxviruses, however, are acquired through direct contact with lesions and do not spread extensively. Molluscum contagiosum causes a wartlike lesion rather than a lytic infection.
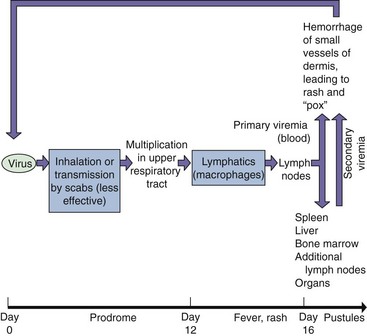
Figure 52-4 Spread of smallpox within the body. The virus enters and replicates in the respiratory tract without causing symptoms or contagion. The virus infects macrophages, which enter the lymphatic system and carry the virus to regional lymph nodes. The virus then replicates and initiates a viremia, causing the infection to spread to the spleen, bone marrow, lymph nodes, liver, and all organs, followed by the skin (rash). A secondary viremia causes the development of additional lesions throughout the host, followed by death or recovery with or without sequelae. Recovery from smallpox was associated with prolonged immunity and lifelong protection.
The poxviruses encode many proteins that facilitate their replication and pathogenesis in the host. They include proteins that initially stimulate host cell growth and then lead to cell lysis and viral spread.
Cell-mediated immunity is essential for resolving a poxvirus infection. However, poxviruses encode activities that help the virus evade immune control. These include the cell-to-cell spread of the virus to avoid antibody and proteins that impede the interferon, complement, and inflammatory, antibody, and cell-mediated protective responses. The disease mechanisms of poxviruses are summarized in Box 52-2.
Box 52-2
Disease Mechanisms of Poxvirus
Smallpox is initiated by respiratory tract infection and is spread mainly by the lymphatic system and cell-associated viremia.
Molluscum contagiosum and other poxviruses are transmitted by contact.
Virus may cause initial stimulation of cell growth and then cell lysis.
Virus encodes immune escape mechanisms.
Cell-mediated immunity and humoral immunity are important for resolution.
Most poxviruses share antigenic determinants, allowing preparation of “safe” live vaccines from animal poxviruses.
Epidemiology
Smallpox and molluscum contagiosum are strictly human viruses. In contrast, the natural hosts for the other poxviruses important to humans are vertebrates other than humans (e.g., cow, sheep, and goats). The viruses infect humans only through accidental or occupational exposure (zoonosis). A recent outbreak of monkeypox in the United States is such an example. The infected individuals had purchased prairie dog pets that had been in contact with Gambian giant rats, which were the probable source of the virus. The revival of smallpox vaccination of military personnel has brought with it incidence of vaccine-mediated (vaccinia) disease in contacts.
Smallpox (variola) was very contagious and, as just noted, was spread primarily by the respiratory route. It was also spread less efficiently through close contact with dried virus on clothes or other materials. Despite the severity of the disease and its tendency to spread, several factors contributed to its elimination, as listed in Box 52-3.
Clinical Syndromes
The diseases associated with poxviruses are listed in Table 52-1.
Smallpox
The two variants of smallpox were variola major, which was associated with a mortality of 15% to 40%, and variola minor, which was associated with a mortality of 1%. Smallpox was usually initiated by infection of the respiratory tract, with subsequent involvement of local lymph glands, which, in turn, led to viremia.
The symptoms and course of the disease are presented in Figure 52-4, and the characteristic rash is shown in Figure 52-5. After a 5- to 17-day incubation period, the infected person experienced high fever, fatigue, severe headache, backache, and malaise, followed by the vesicular rash in the mouth and soon after on the body. Vomiting, diarrhea, and excessive bleeding would quickly follow. The simultaneous outbreak of the vesicular rash distinguishes smallpox from the vesicles of varicella-zoster, which erupt in successive crops.

Smallpox was usually diagnosed clinically but was confirmed by growth of the virus in embryonated eggs or cell cultures. Characteristic lesions (pocks) appeared on the chorioallantoic membrane of embryonated eggs. New polymerase chain reaction and rapid DNA sequencing techniques are available at the CDC.
Smallpox was the first disease to be controlled by immunization, and its eradication is one of the greatest triumphs of medical epidemiology. Eradication resulted from a massive WHO campaign to vaccinate all susceptible people, especially those exposed to anyone with the disease, and thereby interrupt the chain of human-to-human transmission. The campaign began in 1967 and succeeded. The last case of naturally acquired infection was reported in 1977, and eradication of the disease was acknowledged in 1980.
Variolation, an early approach to immunization, involved the inoculation of susceptible people with the virulent smallpox pus. It was first performed in the Far East and later in England. Cotton Mather introduced the practice to America. Variolation was associated with a fatality rate of approximately 1%, a better risk than that associated with smallpox itself. In 1796, Jenner developed and then popularized a vaccine using the less virulent cowpox virus, which shares antigenic determinants with smallpox.
As the eradication program neared its goal, it became apparent that the rate of serious reactions to vaccination (see the following discussion of vaccinia) exceeded the risk of infection in the developed world. Therefore, routine smallpox vaccination began to be discontinued in the 1970s and was totally discontinued after 1980. Newer, safer vaccines are being stockpiled in response to concerns regarding the use of smallpox in biowarfare.
Renewed interest is being paid to antiviral drugs that are effective against smallpox and other poxviruses. Cidofovir, a nucleotide analogue capable of inhibiting the viral DNA polymerase, is effective and approved for treatment of poxvirus infections.
Vaccinia and Vaccine-Related Disease (Clinical Case 52-1)
Vaccinia is the virus used for the smallpox vaccine. Although thought to be derived from cowpox, it may be a hybrid or other poxvirus. The vaccination procedure consisted of scratching live virus into the patient’s skin with a bifurcated needle and then observing for the development of vesicles and pustules to confirm a “take.” As the incidence of smallpox waned, however, it became apparent that there were more complications related to vaccination than cases of smallpox. Several of these complications were severe and even fatal. They included encephalitis and progressive infection (vaccinia necrosum), the latter occurring occasionally in immunocompromised patients who were inadvertently vaccinated. Recent cases of vaccine-related disease have been noted in family members of immunized military personnel. These individuals are treated with vaccinia immune globulin and antiviral drugs.
Clinical Case 52-1
Vaccinia Infection in Vaccinated Contacts
The Centers for Disease Control and Prevention (CDC) (MMWR Morb Mortal Wkly Rep 56:417–419, 2007) described the case of a woman who visited the public health clinic in Alaska because the pain from vaginal tears had increased over the course of 10 days. There was no fever, itching, or dysuria. Clinical examination showed two shallow ulcers, redness, and vaginal discharge. There was no inguinal lymphadenopathy. A viral specimen from the lesion was identified by the CDC as the vaccine strain of vaccinia virus. Presence of the virus was identified by a variation of a polymerase chain reaction test, which produces characteristic vaccinia DNA fragments from the genome. Although she routinely insists on using condoms during sex, a condom broke during vaginal intercourse with a new male sex partner. The male partner was in the U.S. Military and had been vaccinated for smallpox 3 days before initiating his relationship with the woman. Although routine smallpox immunization had been stopped because of elimination of the virus, increased numbers of military and other personnel are receiving vaccinia immunization for protection against weaponized smallpox. This increases the potential for unintentional transmission of the vaccinia vaccine virus. Other cases of vaccine-related vaccinia infection include infants and individuals with atopic dermatitis, who had more severe consequences.
Orf, Cowpox, and Monkeypox
Human infection with the orf (poxvirus of sheep and goat) or cowpox (vaccinia) virus is usually an occupational hazard resulting from direct contact with the lesions on the animal. A single nodular lesion usually forms on the point of contact, such as the fingers, hand, or forearm, and is hemorrhagic (cowpox) or granulomatous (orf or pseudocowpox) (Figure 52-6). Vesicular lesions frequently develop and then regress in 25 to 35 days, generally without scar formation. The lesions may be mistaken for anthrax. The virus can be grown in culture or seen directly with electron microscopy but is usually diagnosed from the symptoms and patient history.

The more than 100 cases of illnesses resembling smallpox have been attributed to the monkeypox virus. Except for the outbreak in Illinois, Indiana, and Wisconsin in 2003, they all have occurred in western and central Africa, especially Zaire. Monkeypox causes a milder version of smallpox disease, including the pocklike rash.
Molluscum Contagiosum (Box 52-4)
The lesions of molluscum contagiosum differ significantly from pox lesions in being nodular to wartlike (Figure 52-7A). They begin as papules and then become pearl-like, umbilicated nodules that are 2 to 10 mm in diameter and have a central caseous plug that can be squeezed out. They are most common on the trunk, genitalia, and proximal extremities and usually occur in a cluster of 5 to 20 nodules. The incubation period for molluscum contagiosum is 2 to 8 weeks, and the disease is spread by direct contact (e.g., sexual contact, wrestling) or fomites (e.g., towels). The disease is more common in children than adults, but its incidence is increasing in sexually active and immunocompromised individuals.
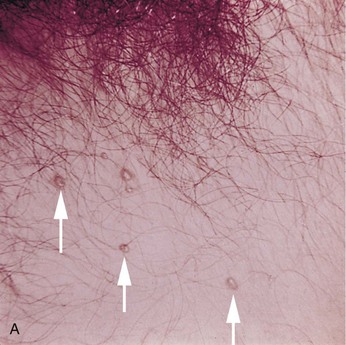
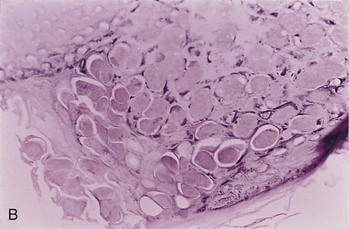
Figure 52-7 Molluscum contagiosum. A, Skin lesions. B, Microscopic view; epidermis is filled with molluscum bodies (magnification 100×).
The diagnosis of molluscum contagiosum is confirmed histologically by the finding of characteristic large, eosinophilic, cytoplasmic inclusions (molluscum bodies) in epithelial cells (Figure 52-7B). These bodies can be seen in biopsy specimens or in the expressed caseous core of a nodule. The molluscum contagiosum virus cannot be grown in tissue culture or animal models.
Lesions of molluscum contagiosum disappear in 2 to 12 months, presumably as a result of immune responses. The nodules can be removed by curettage (scraping) or the application of liquid nitrogen or iodine solutions.
1. The structure of poxviruses is more complex than that of most other viruses. What problems does this complexity create for viral replication?
2. Poxviruses replicate in the cytoplasm. What problems does this feature create for viral replication?
3. How does the immune response to smallpox infection in an immunologically naïve person differ from that in a vaccinated person? When is antibody present in each case? What stage or stages of viral dissemination are blocked in each case?
4. What characteristics of smallpox facilitated its elimination?
5. Vaccinia virus is being used as a vector for the development of hybrid vaccines. Why is vaccinia virus well suited to this task? Which infectious agents would be appropriate for a vaccinia hybrid vaccine, and why?
1. Poxviruses have a large, complex structure with several membranes, lateral bodies, and other structures. Synthesis and assembly of complex structures are difficult.
2. Poxviruses are DNA viruses. Replication of a DNA virus in the cytoplasm requires that the virus supply and encode the enzymes required for mRNA synthesis (e.g., DNA-dependent RNA polymerase, capping enzymes) and for DNA synthesis (DNA-dependent DNA polymerase), enzymes that are normally present in the nucleus.
3. Immunity to smallpox infection develops from the local innate responses to the more systemic antibody and T-cell responses. The immune responses do not develop until 6 to 10 days after infection, too late to stop the spread of the virus. Because the virus has spread throughout the body by this time and infected many tissues, the immune response (especially cell-mediated immunity) can cause great damage when trying to eliminate the infected cells.
In a vaccinated person, antibody is present in the bloodstream to block the spread of the virus by viremia. T-cell responses are activated within 2 to 4 days from memory cells, and these responses can successfully limit and resolve the infection.
4. Elimination of smallpox was made possible by an excellent vaccine that leaves evidence of vaccination, a very active World Health Organization, and because the virus has the following properties: exclusive human host range (no animal vectors to control); single serotype shared with animal viruses, such as vaccinia; and presence of symptoms in every infected individual, which facilitated quarantine procedures.
5. Vaccinia has been developed into an attenuated virus that will not cause human disease (in immunocompetent hosts). The genome contains many genes that are not necessary for virus replication and which can be replaced with genes from other viruses or microbes. If the appropriate gene is incorporated into a vaccinia hybrid, the vaccine would establish a natural immune response, including CD8 T cells and memory cells, that would be appropriate for those viruses requiring TH1 immune responses for immune control.
The vaccinia hybrid vaccine would also be appropriate for viruses that cannot be grown outside of a human, for viruses that would have questionable safety because of potential reversion, and for viruses that have oncogenic potential. Appropriate viruses include human immunodeficiency virus (HIV), herpes simplex virus (HSV), cytomegalovirus (CMV), Epstein-Barr virus (EBV), and other viruses.