Bony Thorax
 Oblique sternum (R)
Oblique sternum (R)Bony Thorax—Positioning Considerations
The routine for a sternum generally includes a lateral and an oblique wherein the sternum is shifted to the left of the spine and is superimposed over the homogeneous heart shadow. A 15°–20° RAO achieves this best. An orthostatic-breathing technique generally is used to blur out the lung markings and the ribs overlying the sternum. If preferred, exposure can also be made on suspended expiration.
Ribs
Each technologist should determine the preferred routine for his or her department.
Two-Image Routine
One suggested two-image routine is an AP or PA with the area of injury closest to the image receptor (IR) (above or below diaphragm) and an oblique projection of the axillary ribs on the side of injury. Therefore the oblique for this routine on an injury to the left anterior ribs would be an RAO shifting the spine away from the area of injury and to increase visibility of the left axillary ribs. The oblique for an injury to the right posterior ribs would be an RPO wherein the spine again is rotated away from the area of injury.
Three-Image Routine
Another three-image routine required in some departments for all rib trauma consists of AP above diaphragm or AP below diaphragm and RPO and LPO of the site of injury.
Above and Below Diaphragm
The location of the injury site in relationship to the diaphragm is important for all routines. Those injuries above the diaphragm require less exposure (nearer to a chest technique) when taken on inspiration and those below the diaphragm require an exposure nearer to that of an abdomen technique when taken on expiration.
Right Anterior Oblique (RAO) Sternum*


Lateral Sternum*

• 24 × 30 cm L.W. (10 × 12″) or 30 × 35 cm (11 × 14″)
• Place lead blocker anterior to sternum (for recumbent position)



Lateral Sternum
Sternoclavicular Joints PA and Anterior Oblique Projections*



Position
Oblique:
Rotate thorax 10°–15° to shift vertebrae away from sternum (best visualizes downside SC joint). RAO will demonstrate the right SC joint. LAO will demonstrate the left SC joint.
Less obliquity (5°–10°) will best visualize the upside SC joint next to spine.
Sternoclavicular (SC) Joints—PA

SC Joints—Anterior Oblique

AP or PA (Bilateral) Ribs—Above Diaphragm*
Generally taken as AP for posterior ribs and PA for anterior ribs.

AP Ribs (Bilateral)—Below Diaphragm*


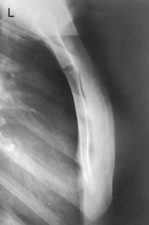
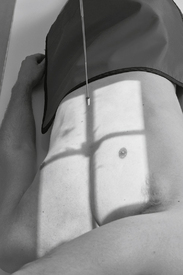
Anterior Oblique Upper Axillary Ribs—RAO*

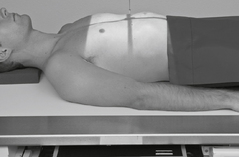
Fig. 7-13 45° RAO above diaphragm—bilateral, right anterior injury (to shift spine away from injury).
Position
• Erect, or recumbent if needed (erect preferred)
• Oblique 45°, rotate spine away from area of interest
• Involved region of thorax is centered to IR with top of IR ≈4 cm (1.5″) above shoulders
Posterior Oblique Lower Axillary Ribs—LPO*
Anterior or Posterior Oblique Axillary Ribs


*Bontrager Textbook, 8th ed, p. 362.
*Bontrager Textbook, 8th ed, p. 363.
*Bontrager Textbook, 8th ed, pp. 364 and 365.
*Bontrager Textbook, 8th ed, pp. 366 and 368.
*Bontrager Textbook, 8th ed, pp. 366 and 368.
*Bontrager Textbook, 8th ed, pp. 369 and 370.
*Bontrager Textbook, 8th ed, pp. 369 and 370.