Mobile (Portables) and Surgical Procedures
 AP chest (supine and semierect)
AP chest (supine and semierect)Essential Principles for Trauma and Mobile Radiography
The following three principles must be observed for trauma and mobile procedures:
• Two projections 90° to each other (minimum): Trauma radiography generally requires two projections taken at 90° (or right angles to each other) while true CR-part-IR alignment is maintained.
• Entire anatomic structure or trauma area on image receptor: Trauma radiography mandates that the entire structure being examined should be included on the radiographic image to ensure that no pathologic condition is missed. Additional projections must be taken if the entire structure is not seen on the initial image.
• Maintain the safety of the patient, health care workers, and the public: Technologist must maintain the safety and well-being of patients, family/friends, and other health workers during a trauma or mobile radiographic procedure. Safe handling of patients and radiation protection of the patient and others in the immediate vicinity of the exposure is the responsibility of the technologist.
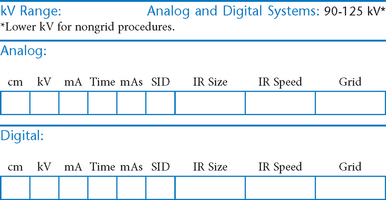
Mobile—AP Chest*


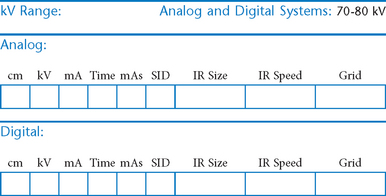
Mobile—AP Abdomen (KUB)*

Mobile—Lateral Decubitus*
Left lateral best demonstrates free air in right upper abdomen. Must include diaphragm.

Position
Mobile—AP Pelvis or Hip*



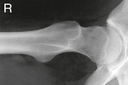
Mobile—Axiolateral Hip*


Position
• Place folded towels or support under affected hip.
• Place vertical grid against patient’s side with top of IR just above iliac crest with face of grid parallel to femoral neck and perpendicular to CR.
• Elevate opposite leg (Do NOT support leg/foot on collimator or tube because of risk for burns or electrical shock.)
• Internally rotate affected leg only if unsecured hip fracture is not suspected.
Mobile—Modified Axiolateral Hip and Proximal Femur*

Alternative projection if both limbs have limited movement and the inferosuperior projection cannot be obtained

Position
• Patient supine, affected side near edge of table with both legs fully extended
• Provide pillow for head, and place arms across superior chest.
• Maintain leg in neutral (anatomic) position.
• Rest IR on extended Bucky tray, which places the bottom edge of the IR about 2″ (5 cm) below the level of the tabletop.
• Tilt IR approximately 15° from vertical and adjust alignment of IR to ensure that face of IR is perpendicular to CR to prevent grid cutoff.
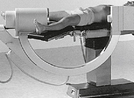
Surgical (Mobile) C-Arm

C-Arm Lateral Hip
Surgical or Mobile Procedures
Procedure Notes:
______________________________________________________________
______________________________________________________________
______________________________________________________________
______________________________________________________________
______________________________________________________________
______________________________________________________________
______________________________________________________________
______________________________________________________________
______________________________________________________________
______________________________________________________________
______________________________________________________________
______________________________________________________________
______________________________________________________________
______________________________________________________________
______________________________________________________________
______________________________________________________________
______________________________________________________________
______________________________________________________________
______________________________________________________________
______________________________________________________________
______________________________________________________________
______________________________________________________________
______________________________________________________________
______________________________________________________________
______________________________________________________________
______________________________________________________________
______________________________________________________________
______________________________________________________________