18 Fibula
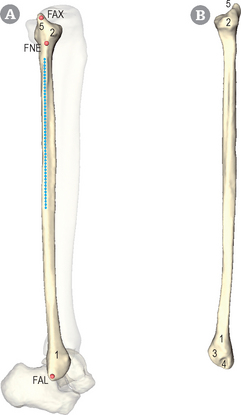
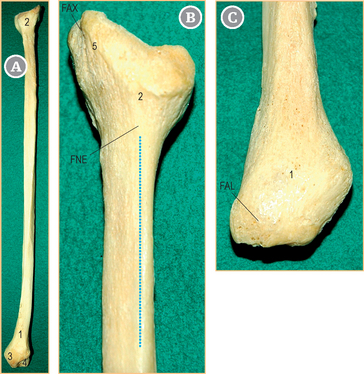
Orientation and general presentation (Figs 18.1 & 18.2)
The fibula is lateral and posterior to the tibia. The distal epiphysis (1) is flatter than the proximal epiphysis (2). The distal epiphysis shows the lateral malleolus (FAL). The articular facet of the talofibular joint (3) is oriented medially, whereas the malleolar fossa (4) of the lateral malleolus is located behind the joint surface. The proximal epiphysis, or fibula head (2), is separated from the diaphysis by the neck of the fibula (FNE). The fibula head has a styloid process (5) pointing upwards and showing a sharp fibula apex (FAX). Vertically below the lateral aspect of the head, the lateral edge (blue line) runs downwards.
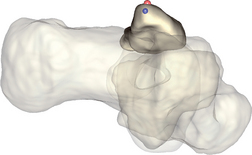
Fibula – ApeX of the styloid process (FAX)[R,L]
Landmark FAX
Bony eminence located on the dorsal aspect of the fibula head (see Fig. 18.1, structure 2). Both the biceps femoris muscle and the fibular collateral ligament insert on the head next to the styloid process (see Figs 18.1 & 18.2).

 Subject lying: The subject is lying supine, knee flexed (about 90°), with the palpator standing slightly laterally in front of the knee.
Subject lying: The subject is lying supine, knee flexed (about 90°), with the palpator standing slightly laterally in front of the knee.
Subject standing: The palpator kneels, facing the flexed knee of the subject, who is asked to put his or her bodyweight on the limb that is not being palpated.
Follow the tendon of the biceps femoris muscle (blue arrow) with your index finger until you reach its insertion.

 FAX is the most lateral and posterior part of the fibula head, next to the tendon.
FAX is the most lateral and posterior part of the fibula head, next to the tendon.

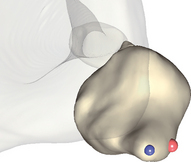
The manually palpated point is not strictly speaking the real apex of the fibula head, as this is located deeper under the tendon of the biceps femoris muscle. This must be kept in mind if virtual palpation is performed in parallel; in this case, the red landmark must be selected. If you wish to perform virtual palpation of the real apex, select the blue landmark.

Fibula – NEck (FNE)[R,L] 
Landmark FNE
Intermediate area between the fibula head and the fibula diaphysis (see Figs 18.1 & 18.2).

Subject lying: The subject is lying supine, knee flexed (about 90°), with the palpator standing slightly laterally in front of the knee.
Subject standing: The palpator kneels, facing the flexed knee of the subject, who is asked to put his or her bodyweight on the limb that is not being palpated.
Place the forefinger on the fibula head slightly more anteriorly and distally in relation to FAX (see p. 154).
Glide your finger downwards towards the fibula head.

The junction, or fibular neck, between the head and the diaphysis is usually readily palpable.

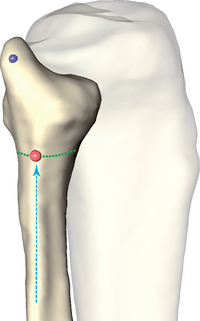 Locate the lateral edge and follow it up (blue arrow) to the fibula neck (green curve). Select the intersection point between the neck and the lateral edge (FAX, in blue; see p. 154).
Locate the lateral edge and follow it up (blue arrow) to the fibula neck (green curve). Select the intersection point between the neck and the lateral edge (FAX, in blue; see p. 154).
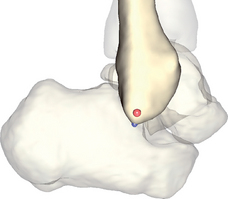
Fibula – Apex of the Lateral malleolus (FAL)[R,L] ISB H|Anim
Landmark FAL
The lateral malleolus has a triangular prismatic form with anterior and posterior edges, which join at the apex of the malleolus (see Figs 18.1 & 18.2). In the neutral position of the foot, the lateral malleolus is about 2 cm lower than the medial malleolus.

Subject lying: The subject is lying supine, knee extended, with the palpator at the subject’s ankle.
Subject standing: The palpator kneels next to the extended lower limb of the subject, who is asked to put his or her bodyweight on the limb that is not being palpated.
Place your forefinger and thumb on the posterior edge of the malleolus and the anterior edge of the lateral malleolus, respectively.
Move both fingers distally along the edges of the malleolus until they meet at the distal aspect of the lateral malleolus.

At that location, gently push the forefinger into the soft tissue, towards the apex of the malleolus (FAL).
The manually palpated point is not strictly speaking the real apex of the malleolus, which is located deeper in the soft tissue. This must be kept in mind if virtual palpation is performed in parallel; in this case, the red landmark must be selected. If you wish to perform virtual palpation of the real apex, select the blue landmark.