Chapter 8 The urinary system
Morphologically, the urinary and genital or reproductive systems may be considered as one (the urogenital (UG) system) because of their common embryological origins, and because both systems share common ducts. Aside from the germ cells the bulk of the UG system is derived from the intra-embryonic mesoderm. Despite this commonality it is easier to consider the system in its two major functional divisions: the urinary and genital (or reproductive) systems.
Common aspects
The initial structures that develop in the UG system have excretory functions. Subsequently, a number of those structures become adapted for reproductive function, losing their excretory roles. The remaining excretory structures continue to develop as the definitive urinary organs and their associated ducts.
Origins
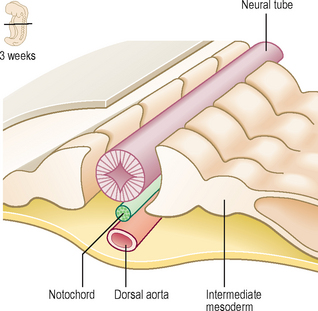
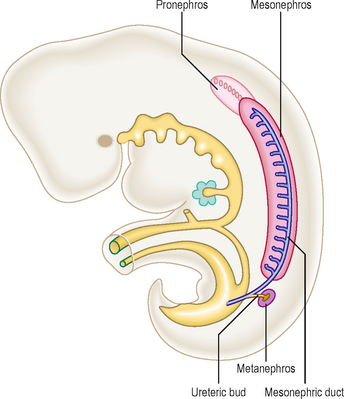
The UG system originates from the bilateral intermediate cell masses of the intra-embryonic mesoderm (Fig. 8.1). Each cell mass develops craniocaudally in the trunk of the embryo as the nephrogenic cord that underlies the urogenital ridge, the bulge formed by the underlying differentiating mesenchymal tissue. Cavities appear in the mass at each segmental level, beginning at the most cranial end, which are primitive kidney tubules. On each side, the most cranial components constitute the pronephros and these develop first, then the mesonephros develops and finally the metanephros appears most caudally (Fig. 8.2). The pronephros is non-functional and temporary, whereas the mesonephros and metanephros produce urine. There is a common pattern for kidney development within vertebrates generally, though the extent to which the pronephros, mesonephros and metanephros subsequently develop varies within different species. The metanephros becomes the definitive human adult kidney.
The urinary system
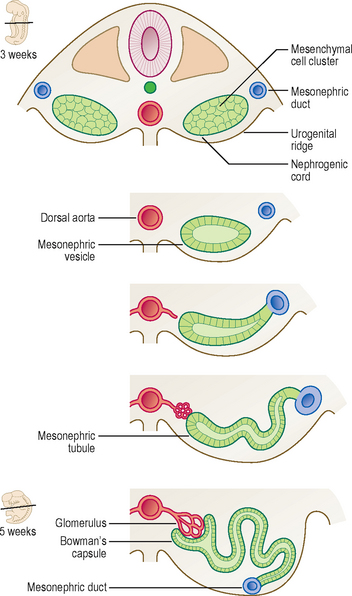
Two components are necessary for the development of an excretory system: a capillary bed from which the filtration product is derived and a tubule to conduct filtration products to the exterior (Fig. 8.3). The tubule begins as a blind-ended cup-like structure invaginating the capillary bed (or glomerulus) and opens into the exterior (via a convergent series of tubes into the urinary bladder). Thus, there is a nephric vesicle (becoming known as either mesonephric or metanephric as differentiation proceeds) and an excretory duct developing from the mesenchymal cells of the intermediate cell mass. The nephric vesicle is the initial part of the tubular system into which the glomerulus invaginates. The tubule opens into the duct (Fig. 8.3) and this pattern occurs at each segmental level. Each tubule lengthens and therefore becomes convoluted, especially so in the metanephros in which the definitive adult nephrons develop.
Kidneys and ureters
Three pairs of successive kidneys develop in a craniocaudal sequence. The pronephros develops at the most cranial end of the nephrogenic cord, but because it is non-functional and is only a short-lived structure in humans it will not be considered further.
The mesonephros begins to develop in the lower thoracic and lumbar segments of the embryo. The cavities, which appear in the mesonephros, become the tubules and connect laterally with the mesonephric duct, which also forms from the intermediate mesoderm. The duct lies longitudinally in the embryo draining into the primitive urogenital sinus, the future urinary bladder. The urogenital sinus is closed inferiorly by the cloacal membrane (see Chapters 1 and 7), which is derived from the ectoderm and endoderm that lie in contact with each other to form a closure. In some vertebrate species the mesonephros persists as the adult kidney, though not in humans. Parts of the duct system do persist in humans, however, as components of the reproductive system in the male, as the ductus deferens and the efferent ductules of the testis. In the female the mesonephric duct largely disappears though unimportant remnants may be found between the layers of the broad ligament.
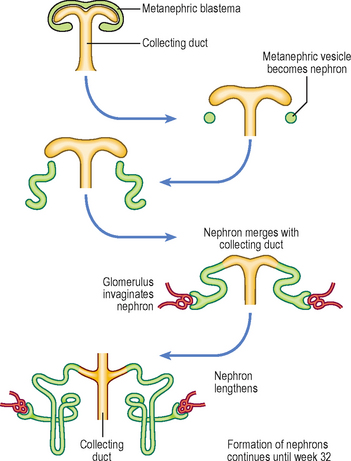
The metanephros (Fig. 8.4) develops at the most caudal end of the nephrogenic cord. The metanephric diverticulum or ureteric bud arises as an outgrowth from the caudal end of the mesonephric duct. The ureteric bud grows into the nephrogenic cord, the tissue of which condenses around it to form the metanephric blastema (Fig. 8.4). The tip of the developing ureter (the ureteric bud) continues to divide to form the collecting ducts and the calyces, each division becoming surrounded by a metanephric blastema. The ureteric bud also forms the definitive adult ureter. The cells in the blastema go on to form the nephrons. These developments are longer and more complex than those of the mesonephros. The blind-ended portion of the tubule, as in the mesonephros, receives an invagination of the glomerular capillaries (Fig. 8.5). The mesonephric duct distal to the ureteric bud is incorporated into the wall of the urinary bladder as the trigone, and also forms the ductus deferens.
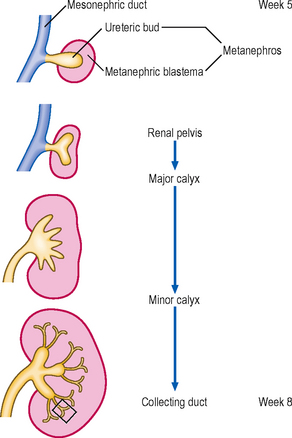
Fig. 8.4 The development of the metanephros and its duct system between 5 and 8 weeks. The area enclosed by a box is enlarged in Figure 8.5.
The kidneys come to occupy their adult lumbar position later in development, apparently having ascended from their pelvic origin (Fig. 8.6). This is because of the differential growth rates of the abdominal walls and the kidneys, and the regression of the enlarged suprarenal glands.
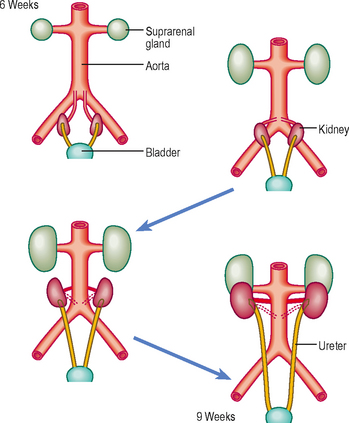
Fig. 8.6 The ascent of the kidneys from the sacral to the lumbar position between 6 and 9 weeks. Note the relatively large size of the suprarenal glands which regress at a later stage.
 Clinical box
Clinical boxThe developing kidneys are subject to a range of developmental anomalies ranging from agenesis to dysplasia, or to cyst formation. There are also some possible positional malformations. If the kidneys do not ‘ascend’ from their pelvic origin then a pelvic kidney results. Sometimes both kidneys become so close during their ascent that their lower poles (usually) fuse, a so-called horseshoe kidney. This can lead to pressure on the inferior vena cava and oedema of the lower limbs. In cystic, pelvic or horseshoe kidneys, presenting symptoms may include haematuria and recurrent renal infections.
As a consequence of the ascending kidneys a successive series of arterial blood supplies arise from the abdominal aorta. The persistence of an accessory renal artery supplying the lower pole of the kidney as well as the renal artery proper is commonly observed.
The metanephric kidney is functional from week 10 and the urine produced at this stage passes into the amniotic fluid. The amniotic fluid is swallowed by the fetus, thus recirculating the water content. However, it is the placenta which removes fetal waste at this stage of development.
Urinary bladder and urethra
The urinary bladder arises after the cloaca has been divided by the urorectal septum. The anterior part is the urogenital sinus, and the posterior component is the anorectal canal (see Chapter 7). In both sexes, the upper part of the urogenital sinus forms the bladder. In males, the pelvic part becomes the prostatic and membranous parts of the urethra and the lower phallic part becomes the penile urethra. In females, the middle and lower parts of the urogenital sinus become the entire urethra. Initially the bladder is continuous with the allantois, but the allantois regresses to form the urachus and then the median umbilical ligament after birth.
In the severe birth defect known as exstrophy of the bladder the urinary bladder is exposed on the surface of the anterior abdominal wall. Partial or complete duplication of the ureteric bud gives rise to a bifid ureter or separate ureters. These anomalies may result in reflux of urine and urinary tract infections. A number of abnormalities can occur if part or the entire allantois fails to become obliterated, resulting in urachal cysts, a urachal sinus or a urachal fistula. In cases of an urachal fistula the allantois remains patent and urine leaks from the umbilicus.
 The UG system is considered as one morphologically because of the common embryological origin and shared elements of the duct systems. The initial structures that develop in the UG system are associated with excretory functions, some of which lose those functions and become adapted for reproductive roles. Cavities appear in the intermediate cell mass and differentiation proceeds in a craniocaudal direction, and thus the nephrogenic cord develops along the length of the trunk of the embryo, underlying the urogenital ridges. In each embryonic segment an excretory tubule and a nephric vesicle develop from which the urinary tubules arise. The glomerulus is invaginated into the nephric vesicle. The metanephroi become the definitive adult kidneys the ureteric bud grows out of the caudal end of the mesonephric duct into the nephrogenic cord, thus forming a metanephric blastema. The metanephroi appear to ascend the posterior abdominal wall to achieve their adult position, as a consequence of differential growth rates.
The UG system is considered as one morphologically because of the common embryological origin and shared elements of the duct systems. The initial structures that develop in the UG system are associated with excretory functions, some of which lose those functions and become adapted for reproductive roles. Cavities appear in the intermediate cell mass and differentiation proceeds in a craniocaudal direction, and thus the nephrogenic cord develops along the length of the trunk of the embryo, underlying the urogenital ridges. In each embryonic segment an excretory tubule and a nephric vesicle develop from which the urinary tubules arise. The glomerulus is invaginated into the nephric vesicle. The metanephroi become the definitive adult kidneys the ureteric bud grows out of the caudal end of the mesonephric duct into the nephrogenic cord, thus forming a metanephric blastema. The metanephroi appear to ascend the posterior abdominal wall to achieve their adult position, as a consequence of differential growth rates.