Chapter 13 Health promotion in schools
Overview
The view that schools can promote the health and welfare of children and young people has a long history. The development of a school health service, the requirement for school boards to provide meals and, more recently, the inclusion of physical education in the national curriculum and the setting of nutritional standards for school meals are examples of how the school was seen as a key setting in which a captive audience could be encouraged to adopt lifestyles conducive to good health.
The World Health Organization has defined a health-promoting school (HPS) as: ‘one in which all members of the school community work together to provide pupils with integrated, positive experiences and structures which promote and protect health. This includes both the formal and informal curriculum in health, the creation of a safe and healthy school environment, the provision of appropriate health services and the involvement of the family and the wider community in efforts to promote health’ (World Health Organization 1995). The school is seen as a total environment in which many aspects affect the health of its pupils and staff, including its organization, ethos and culture and its layout, in addition to any teaching about health issues and the provision of medical and nursing services. Schools also act as referral agencies, signposting children and parents to other health, welfare and voluntary services when appropriate.
This chapter looks at the physical, mental and social well-being of children and young people and how schools can be powerful agents in the promotion of good health through the curriculum and everyday practices.
Why the school is a key setting for health promotion
Education is a resource for health. This is recognized by the World Health Organization, and the United Nations included ‘achieving universal primary education’ as one of its eight millennium development goals. Equally, health is a prerequisite for education: ‘Children who face violence, hunger, substance abuse, and despair cannot possibly focus on academic excellence. There is no curriculum brilliant enough to compensate for a hungry stomach or distracted mind’ (National Action Plan for Comprehensive School Health Education 1992).
School is seen as an important context for health promotion, principally because it reaches a large proportion of the population for many years. The emphasis on schools is also a recognition that the learning of health-related knowledge, attitudes and behaviour begins at an early age.
 BOX 13.1
BOX 13.1Reflect on your own experience of health promotion when you were at school. Do you regard your experience as adequate and appropriate?
 BOX 13.2
BOX 13.2Consider each of the following statements about the aims for health promotion for young people and indicate how important you would rate each (very important/important/not very important/not important at all).
What factors would you identify as important in promoting a health-enhancing lifestyle for young people?
Childhood and adolescence is a time of great change, when young people often acquire lifetime habits and attitudes. One function of a healthy school environment is to enable children to develop healthy behaviours. Part of growing up is risk-taking, but problems arise when young people are unaware of the scale of risk involved. The effects of smoking, excessive alcohol consumption, drug use and low levels of exercise may not become apparent until later life. There is some evidence that risk-taking behaviour in one area can lead to risk-taking behaviour in other areas. A recent study of 15-year-olds found that the odds of someone having used cannabis in the last month were 12 times higher for those who had drunk alcohol in the last week compared with those who hadn’t, and 8 times higher for those who had smoked in the last week (National Centre for Social Research and the National Foundation for Educational Research 2005). Similarly, two-fifths of sexually active 13- and 14-year-olds said they were under the influence of alcohol or cannabis the first time they had sexual intercourse (Wight et al 2000). Whilst adolescence is characterized by powerful peer group attachments, the school setting provides an opportunity to communicate with young people and provides learning opportunities and a safe environment to practise new skills.
There is a relationship between health and education and the ability to learn. Young people’s experiences in school influence the development of their self-esteem, self-perception and their health behaviours. Pupils with low school performance and educational aspirations and high levels of absence from school are more likely to engage in earlier risk-taking behaviour such as drug use (Canning et al 2004). School attendance is particularly important and provision of food at school, e.g. through breakfast clubs, can improve attendance rates. Equally, health can have an impact on educational performance. There is evidence that providing good nutrition in school can improve attention, concentration and overall cognitive development (Powney et al 2000).
Health promotion in schools
The development of health education and promotion in schools has reflected many approaches to health promotion. Health education has tended to reflect the medical view of health and in many countries is almost exclusively concerned with hygiene, nutrition and fitness. In the 1960s education saw a swing to being child-centred and educational methods sought to develop autonomy and responsibility through discovery learning. Health education emerged as a complex theme of well-being and fulfilment of maximum potential. Health promotion in schools is now closely linked to personal and social development, and delivered in the curriculum as personal and social health education (PSHE). The aim is for young people to be in charge of their own lives and the role of the school is to develop self-esteem and self-awareness. Emphasis is placed on the process of education, and finding teaching and learning strategies which encourage reflection and personal awareness. The direction and organization of the health promotion programme also aim to reflect the needs of the children and young people. The provision of PSHE in schools remains patchy and often focuses on knowledge rather than skills and attitudes. There are many reasons for this, including the lack of training for teachers in this subject and mixed messages from government as to the importance of PSHE within the curriculum (PSHE is not mandatory but is strongly encouraged).
Alongside these attempts to promote autonomy and decision-making skills are more traditional information-giving approaches. Behind such an approach is the simple assumption that people are rational decision-makers whose behaviour will change once they have information about how to live more healthily. Much health promotion in schools therefore entails the provision of information about the health-damaging effects of certain behaviours, such as smoking and taking drugs.
The provision of sex education in schools reflects these views of health promotion. Sex education is now commonly referred to as ‘sex and relationships education’ in recognition of the need to move away from a focus on biology to a focus on emotional health, values and life skills.
 BOX 13.5
BOX 13.5Sex and relationship education
Following revisions to the English National Curriculum in 1999, a new personal social and health education (PSHE) framework for schools, and the Social Exclusion Unit’s report on teenage pregnancy, schools were provided with specific guidance on the provision of sex and relationships education (SRE) in schools (Department for Children, Schools and Families 2000). The guidance requires that:
The health-promoting school
The HPS is an international approach to addressing the health of pupils and teachers in a comprehensive and strategic manner (Fig. 13.1). If education for the health of young people is to focus on more than individual behaviour and be health promotion, it needs to acknowledge the influence of the school itself as a health-promoting environment and as part of a wider community.
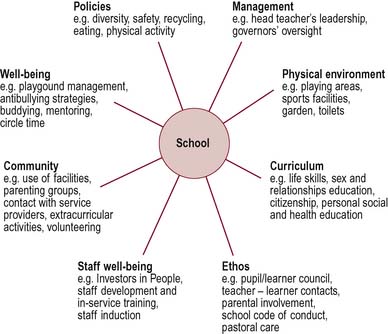
The whole school context includes its ethos, organization, management structures, relationships and physical environment as well as the taught curriculum. In the HPS all these aspects will reinforce and support each other, leading to a synergistic effect. In reality, different aspects of the school often give conflicting messages. Many aspects of school can be health-promoting or health-inhibiting. Educationalists have long talked of a ‘hidden curriculum’ and the way in which messages can be transmitted through children and young people’s daily experience of their surroundings and relationships at school. For example, the state of many school toilets might suggest that hygiene is not valued or that the pupils do not require (or deserve) cleanliness or care. Knowing that someone (e.g. personal tutor, school nurse) is always available to talk to about any personal concerns or incidents at school such as bullying or teasing is important for mental health and well-being.
The European Network of Health Promoting Schools (ENHPS) was launched in 1992 as an initiative of the World Health Organization. The principles of HPS have been identified as:
In common with other settings, effective health promotion in schools happens when it is coordinated and takes place within structured frameworks. In the UK the National Healthy Schools Standard was launched in 2002. As with other award schemes for hospitals and workplaces, the scheme encourages institutions to work towards specific targets. A basic level is to ensure that systems are in place so that specific aspects of health can be incorporated into a school.
The National Healthy Schools Programme (NHSP) is a government initiative to improve the health and achievements of children and young people. The NHSP focuses on four key themes:
The NHSP adopts a whole-school approach and aims to:
The government has set a target that by 2009 all schools will be participating in the NHSP and that 75% will have achieved National Healthy School status (www.healthyschools.gov.uk).
Policies and practices
The policies that a school develops represent its values. Schools may have policies on equal opportunities, discipline and rewards, health and safety, bullying, healthy food and various curriculum issues, including sex education. Policies may be merely ‘paper exercises’ unless they have been influenced by wide consultation within the school and community, have been clearly written and disseminated and are consistently applied. The practices of a school can be evidenced in its daily life and the ways in which decisions are taken. Democratic participation by pupils is a key element in an HPS.
The Ottawa Charter describes health promotion as a process of ‘enabling people to take more control over and improve their health’ (World Health Organization 1986). How can pupils in schools be enabled to make decisions about their education and their health?
Social environment
The quality of social interactions among pupils, between staff and pupils and between the staff contributes to the ethos or climate in a school. Increasingly, schools are recognizing that healthy schools which value positive relationships, prioritize learning and build self-esteem also drive up educational standards.
Curriculum
The formal curriculum includes knowledge and understanding of health-related topics (e.g. biology and nutrition) at a level appropriate for pupils’ age, social and cognitive development. The informal curriculum refers to areas not formally taught or examined, including pastoral care and extracurricular activities in areas such as sports and arts. In the UK there is no statutory provision for health promotion and its integration into the curriculum is patchy.
Physical environment
The physical environment and layout of a school may be stimulating or depressing. Schools should provide a clean and safe environment with no litter or graffiti, clean toilets and a welcoming but secure entrance. There should be areas for play, for social interaction and for quiet study or reading. In many countries the provision of basic amenities such as sanitation, water availability and air cleanliness may be priorities.
Links with the community
How well the school communicates and connects with its local community, where its pupils and their families live, is an important criterion for the HPS. Partnerships with parents may vary from information about school events and fund-raising requests, consultation about uniform or meals provision to the active involvement of all parents in decision-making about the curriculum, pastoral care and resource issues. Parents may also become involved in school life through reading schemes, practical parenting classes and breakfast clubs. A survey of parents’ views on health education and promotion found that many parents did not know what schools were doing and had not been consulted about health promotion despite the fact that they saw school as a major influence on young people’s health awareness (National Foundation for Educational Research 1997).
‘Society School’
A school in Belgium identified the need to integrate its diverse ethnic groups socially. One way to do this was to involve parents in school activities. The school took the approach of celebrating its multiculturalism by asking parents to prepare a snack food from their traditional foods for all the children in the school. Many parents participated, also providing decorations and music. All parents were invited to the school for a free meal. Parents reported that this project broke down their initial hesitation about coming into the school and enabled them to build relationships with other parents (European Network of Health Promoting Schools 1997).
Schools are also part of a wider community and should be open to that community. Many agencies and services can provide support to schools. For example, the police and emergency services often provide educational sessions concerning accident prevention.
HPS and ‘school connectedness’ in Queensland, Australia
The Western Gateway project in Ipswich, Queensland aimed to encourage students’ connectedness with school in order to promote mental health and act as a protective factor reducing the incidence of violence and substance abuse. Ten schools were supported over a 3-year period. Activities undertaken included health weeks, breakfast and lunchtime programmes, smoke-free toilet blocks, healthier tuckshops, comprehensive curriculum programmes, cultural days, parent information sessions and increased participation in physical activity within the school. Evaluation suggested activities improved pupils’ connectedness with school and increased community participation and ownership in school activities (Queensland Government 2005a, b).
Effective interventions
Health promotion interventions in schools differ substantially in their nature, ranging from programmes providing physiological information to life skills to abstinence-oriented programmes, in addition to the comprehensive whole-school approaches outlined above. Many curriculum programmes aim to have outcomes relevant to risk reduction, such as increased knowledge or changes in behaviour. Programmes may thus be specific to a particular health issue (e.g. smoking education) or more generic life skills programmes aiming to develop self-esteem and social and communication skills. They may target pupils only, or extend their reach to include teachers, parents and the wider community.
Schools are dynamic communities and there are many varied influences on young people both within and outside the school setting, so demonstrating the particular effect of health promotion is extremely difficult. The majority of interventions aim to develop health-enhancing behaviours. These health outcomes will not be apparent until later in life. For example, the Australian ‘no hat – no play’ policy will not demonstrate an effect on skin cancer rates until well into adulthood. Evidence shows that increasing children’s knowledge is feasible, but changing their attitudes and behaviour, even in the short term, is far more difficult (Lister-Sharp et al 1999). A recent study by the World Health Organization into the evidence of effectiveness of health promotion in schools and the HPS approach found that mental health promotion programmes were amongst the most effective. Factors associated with increased effectiveness included: long duration, high intensity and involvement of the whole school, a focus on the school environment, multifactoral interventions and peer-led health promotion (Stewart-Brown 2006). There is evidence that integrated, holistic and strategic programmes are more effective than classroom education programmes (St Leger 2005).
Promoting mental health in schools
Schools should promote positive mental health and emphasize well-being as well as targeting those with particular needs. In this way, schools can help to disseminate the idea of mental health as everyone’s business and tackle problems of stigma and denial. Research has shown that the following characteristics are associated with effective mental health programmes in schools:
Conclusion
Schools are widely seen as having a key role in health promotion. Young people are a key target group for the provision of information and encouragement of responsible and health-promoting attitudes and behaviour. The habits acquired in childhood and adolescence may prove influential for the rest of one’s lifespan. Adolescence is also a time of development and risk-taking, and a fine balance needs to be struck between encouraging the development of autonomy alongside responsible and health-promoting attitudes and behaviour. However health, personal and social education has always been marginalized within the formal curriculum. Currently PSHE is not a mandatory subject, although its inclusion is encouraged. Research suggests that narrow information-based programmes are less effective than broader programmes that address the school as a whole. This is the direction taken by the HPS initiative, which seeks to promote a whole-school approach, encompassing not just the formal curriculum but also the informal curriculum, the school’s physical and social environment and its links with its community. The evolving evidence base suggests that the HPS approach is effective and contributes to children’s and young people’s health, education and welfare.