CHAPTER 15 Dental restraint and anesthesia
Sedation
Surgical and diagnostic dental procedures are often performed with the horse sedated because this eliminates the risks associated with general anesthesia. In addition, performing dental procedures with the horse sedated, rather than anesthetized, incurs less expense and time. Problems associated with performing surgical and diagnostic dental procedures with the horse sedated include over-sedation, which can result in excessive ataxia, insufficient analgesia to safely complete the procedure, excessive movement complicating the procedure, and increased risk to personnel. Analgesia can be augmented by administering local or regional anesthesia, but for some procedures, such as extraction of wolf teeth, sedation alone may sometimes be sufficient.
Sedation can be maintained either with bolus injections of a sedative, alone or in combination with an opioid, or by constant rate infusion (CRI) of the sedative, alone or in combination with an opioid. A bolus injection of the sedative is the more common mode of administering sedation. Alpha-2 agonists commonly administered as a bolus include detomidine (0.005–0.02 mg/kg, IV), xylazine (0.3–1.0 mg/kg, IV), medetomidine (0.0035–0.007 mg/kg, IV), and romifidine (0.03–0.1 mg/kg, IV). The duration of sedation achieved by administration of xylazine is short when compared to the duration of sedation imparted by detomidine, medetomidine, or romifidine. When administered intramuscularly, the sedative should be administered at least 15 minutes before surgery, and the dose of the drug should be at least double that of the intravenous dose to achieve the same effect. To minimize movement, the horse can be re-sedated during surgery with the same or another sedative (xylazine [0.5 mg/kg, IV]; detomidine [0.01 mg/kg, IV]; medetomidine [0.002 mg/kg, IV]; or romifidine [0.06 mg/kg, IV]).
Butorphanol (0.02–0.05 mg/kg, IV) is the most common opioid administered in conjunction with a sedative. Other opioids administered include methadone (0.1 mg/kg, IV) and morphine (0.15 mg/kg, IV). Sedation with an alpha-2 agonist should precede administration of the opioid to avoid opioid-induced excitement. Reducing the initial dose of an alpha-2 agonist and administering subsequent doses to effect is prudent to avoid over-sedation when using combinations of drugs. A heavily sedated horse may need the support of a stocks partition, or wall to prevent it from falling. On some occasions, reversing an alpha-2 agonist to speed the recovery of the horse from sedation may be desirable. This is generally necessary only if a large dose of detomidine or romifidine was administered. Yohimbine (0.15 mg/kg, IV), even though it is a weak antagonist, is usually effective. Alternatively, atipamezole (0.15 mg/kg, IV), a more potent antagonist, can be used as a reversal agent. The antagonist should be infused slowly to diminish the likelihood of the reversal agent causing excitation.
If a long procedure is anticipated, sedation can be maintained at a more constant level using a CRI of one or more sedatives after a loading bolus of the sedative has been administered. Drugs commonly administered by CRI include detomidine alone (0.02 mg/kg/hour) or in combination with either butorphanol (0.012 mg/kg/h) or morphine (0.15 mg/kg/h). To avoid inducing excitement when using an opioid in combination with an alpha-2 agonist, a loading dose of the alpha-2 agonist (e.g., detomidine [0.008 mg/kg]) should be administered initially before a loading dose of butorphanol (0.02 mg/kg) or morphine (0.15 mg/kg) is administered.
Nerve blocks of the head
The portion of the head subjected to a dental procedure can be desensitized by using a regional nerve block. Regional nerve blocks of the head include the maxillary, infraorbital, mandibular, mandibular alveolar, and mental nerve blocks. A regional nerve block is administered most easily after the horse has been sedated, and administering the block with the horse sedated enhances the safety of the horse and the operator. Application of a nose twitch often facilitates administration of the block.
Maxillary nerve block
Anesthetizing the maxillary nerve at the pterygopalatine fossa, where the nerve enters the infraorbital canal to become the infraorbital nerve, desensitizes all the ipsilateral dental structures of the maxilla and premaxilla, the paranasal sinuses, and nasal cavity. To anesthetize the maxillary nerve at the pterygopalatine fossa, the point of a 20- to 22-gauge, 3.5 inch (8.9 cm), spinal needle is inserted just ventral to the zygomatic process and dorsal to the transverse facial vessels at the level of the caudal third of the orbit (Fig. 15.1).1 The tip of the needle is inserted perpendicular to the longitudinal axis of the head so that it enters the pterygopalatine fossa just caudal to the maxillary tuberosity at a depth of approximately 2–2.5 inches (5.0–6.5 cm). The horse may jerk its head if the tip of the needle contacts the nerve. An alternative method of anesthetizing the maxillary nerve at the pterygopalatine fossa is to insert the point of a 6 inch (15.2 cm) needle ventral to the most dorsal aspect of zygomatic process, directing the needle rostrally and ventrally, aiming toward the rostral edge of the contralateral facial crest, until the needle strikes bone (Fig. 15.2).

Fig. 15.1 The maxillary nerve can be anesthetized at the pterygopalatine fossa, by inserting a 20- to 22-gauge, 3.5-inch (8.9 cm), spinal needle just ventral to the zygomatic process and dorsal to the transverse facial vessels at the level of the caudal third of the orbit. 15–20 ml of local anesthetic solution is deposited after the needle strikes bone.

Fig. 15.2 The maxillary nerve can be anesthetized at the pterygopalatine fossa by inserting a 6-inch (15.2-cm) needle ventral to the most dorsal aspect of the zygomatic process and directing the needle rostrally and ventrally, aiming toward the rostral edge of the contralateral facial crest, until the needle strikes bone.
Regardless of the technique used, 15 to 20 ml of local anesthetic solution is instilled after the needle strikes bone and as the needle is withdrawn slightly. Structures innervated by the maxillary nerve are desensitized within 15 minutes.
Infraorbital nerve block
The infraorbital nerve block is useful for performing surgery of the nose or maxillary and premaxillary dental structures. When the infraorbital nerve is anesthetized rostral to the infraorbital foramen, where it emerges from the infraorbital canal, the area desensitized includes the skin of the ipsilateral lip, nostril, and face, up to the level of the infraorbital foramen. When the infraorbital nerve is anesthetized within the infraorbital canal, additional structures desensitized include the ipsilateral maxillary and premaxillary teeth, and associated alveoli and gingiva. The effect is the same as that achieved with a maxillary nerve block, provided that the local anesthetic solution completely fills the infraorbital canal.
To locate the infraorbital foramen, a thumb (or middle finger) is placed in the notch formed by the nasal bone and premaxilla, and the middle finger (or thumb) is placed on the rostral aspect of the facial crest. The foramen is located with the index finger halfway between and 1 to 3 cm caudal to an imaginary line connecting the thumb and middle finger (Fig. 15.3). The ridge of the foramen is palpated beneath the ventral margin of the levator labii superioris muscle. To anesthetize the infraorbital nerve within the infraorbital canal, a 21- or 22-gauge,  -inch (3.8-cm) needle is inserted through the skin about
-inch (3.8-cm) needle is inserted through the skin about  inch (1.3 cm) rostral to the foramen after elevating the ventral edge of the levator labii superioris muscle. The point of the needle is advanced along the surface of the maxilla and inserted about 1 inch (2.5 cm) into the canal. Four to 8 ml of local anesthetic solution is deposited within the canal.
inch (1.3 cm) rostral to the foramen after elevating the ventral edge of the levator labii superioris muscle. The point of the needle is advanced along the surface of the maxilla and inserted about 1 inch (2.5 cm) into the canal. Four to 8 ml of local anesthetic solution is deposited within the canal.

Fig. 15.3 The infraorbital foramen is located by placing a thumb (or middle finger) in the notch formed by the nasal bone and premaxilla and the middle finger (or thumb) on the rostral aspect of the facial crest. The foramen can be palpated with the index finger halfway between 1 and 3 cm caudal to an imaginary line connecting the thumb and middle finger after elevating the ventral margin of levator labii superioris muscle with the index finger.
Filling the infraorbital canal with a large volume of local anesthetic solution likely desensitizes all the same structures that the maxillary nerve block desensitizes because the local anesthetic solution anesthetizes the infraorbital nerve as far caudally as the maxillary foramen. The advantage of the infraorbital nerve block over the maxillary nerve block is that instilling local anesthetic solution within the infraorbital canal assures that the infraorbital nerve has been anesthetized. The infraorbital nerve block is tolerated poorly by the horse, however, because the point of the needle inevitably contacts the infraorbital nerve directly, so adequate restraint and great care should be taken during its administration.
Mandibular nerve block
Anesthetizing the mandibular nerve at the mandibular foramen, where it enters the mandibular canal to become the mandibular alveolar nerve, desensitizes the ipsilateral side of the mandible and all its dental structures. The mandibular foramen is located on the medial aspect of the vertical ramus of the mandible where an imaginary line that extends along and caudal to the occlusal surface of the mandibular cheek teeth intersects with another imaginary line that passes perpendicular to the first line from the lateral canthus of the eye. To anesthetize the mandibular nerve, the point of a 20- to 22-gauge, 6–8-inch (15.2–20.3-cm) spinal needle is inserted at the ventral border of the ramus, just rostral to the angle of the mandible and aimed dorsally (Fig. 15.4), or a  -inch (8.9-cm) spinal needle is inserted at the angle formed by the intersection of the vertical and horizontal rami of the mandible and aimed rostrally and dorsally (Fig. 15.5). The point of the needle is advanced along the medial surface of the ramus toward the mandibular foramen, and 15 to 20 ml of local anesthetic solution is deposited.
-inch (8.9-cm) spinal needle is inserted at the angle formed by the intersection of the vertical and horizontal rami of the mandible and aimed rostrally and dorsally (Fig. 15.5). The point of the needle is advanced along the medial surface of the ramus toward the mandibular foramen, and 15 to 20 ml of local anesthetic solution is deposited.
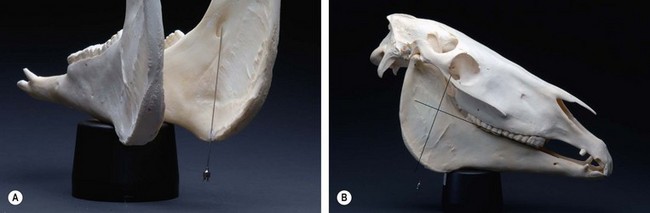
Fig. 15.4 (A) To anesthetize the mandibular nerve, a 20- to 22-gauge, 6–8-inch (15.2–20.3-cm) spinal needle is inserted at the ventral border of the ramus, just rostral to the angle of the mandible and aimed dorsally, along the medial aspect of the vertical ramus of the mandible, toward the mandibular foramen. 15–20 ml of local anesthetic solution is deposited. (B) The mandibular foramen is located at a point where an imaginary line that extends along and caudal to the occlusal surface of the mandibular cheek teeth intersects with another imaginary line that passes from the lateral canthus of the eye perpendicular to the first line.

Fig. 15.5 To anesthetize the mandibular nerve, a  inch (8.9 cm) spinal needle is inserted along the medial surface of the vertical ramus of the mandible at the angle formed by the intersection of the vertical and horizontal rami and aimed rostrally and dorsally toward the mandibular foramen, the location of which is described in the legend for Fig. 15.4.
inch (8.9 cm) spinal needle is inserted along the medial surface of the vertical ramus of the mandible at the angle formed by the intersection of the vertical and horizontal rami and aimed rostrally and dorsally toward the mandibular foramen, the location of which is described in the legend for Fig. 15.4.
Inserting the needle to a point slightly dorsal to the estimated location of the foramen helps to ensure that local anesthetic solution contacts the mandibular nerve because the nerve courses ventrally from a dorsal location to enter the foramen. A second needle of the same length applied to the lateral surface of the mandible can be used to judge the depth of the insertion of the first needle. Structures innervated by the mandibular nerve are desensitized within 15–30 minutes.
Mental nerve block
The mandibular alveolar nerve traverses the mandibular canal to emerge at the mental foramen as the mental nerve. Anesthetizing the mental nerve rostral to where it exits the mental foramen desensitizes the skin of the ipsilateral lip and chin. The mandibular canine, incisor, and cheek teeth and associated alveoli and gingiva are innervated by branches of the mandibular alveolar nerve, which lie within the mandibular canal, and so, to desensitize these structures, local anesthetic solution must be instilled into the mandibular canal. Anesthetizing either the mental nerve at the mental foramen or the mandibular alveolar nerve within the mandibular canal is termed a mental nerve block.
The mental foramen is located on the lateral aspect of the horizontal ramus of the mandible in the interalveolar space directly below the commissure of the lips (Fig. 15.6). The mental foramen lies beneath the tendon of the depressor labii inferioris muscle, and so to palpate the ridge of the mental foramen, this tendon must be elevated dorsally. To anesthetize the mandibular alveolar nerve within the rostral aspect of the mandibular canal, a 21- or 22-gauge,  -inch (3.8-cm) needle is inserted through the skin about
-inch (3.8-cm) needle is inserted through the skin about  inch (1.3 cm) rostral to the mental foramen after elevating the tendon of the depressor labii inferioris muscle. Creating a bend in the shaft of the needle aids its insertion. The needle is inserted into the mandibular canal as far as possible, and 5–10 ml of anesthetic solution is deposited.
inch (1.3 cm) rostral to the mental foramen after elevating the tendon of the depressor labii inferioris muscle. Creating a bend in the shaft of the needle aids its insertion. The needle is inserted into the mandibular canal as far as possible, and 5–10 ml of anesthetic solution is deposited.

Fig. 15.6 The mental foramen can be palpated with an index finger on the lateral aspect of the horizontal ramus of the mandible in the interalveolar space directly below the commissure of the lips by elevating the tendon of the depressor labii inferioris muscle with the index finger. To anesthetize the mandibular alveolar nerve, a 21- or 22-gauge,  -inch (3.8-cm) needle is inserted into the mandibular canal about
-inch (3.8-cm) needle is inserted into the mandibular canal about  inch (1.3 cm) rostral to the mental foramen after elevating the tendon of the depressor labii inferioris muscle.
inch (1.3 cm) rostral to the mental foramen after elevating the tendon of the depressor labii inferioris muscle.
Filling the mandibular canal with a large volume of local anesthetic solution (i.e., >10 ml) likely desensitizes all the same structures that the mandibular nerve block desensitizes because the local anesthetic solution anesthetizes the mandibular alveolar nerve as far caudally as the mandibular foramen. The mental nerve block is tolerated poorly by the horse because the point of the needle inevitably contacts the mandibular alveolar nerve directly.
Analgesia of the temporomandibular joint
Analgesia of the temporomandibular (TM) joint is sometimes used for diagnostic purposes, e.g., to determine if a TM joint is infected or if disease of one or both TM joints could be the cause of clinical signs of disease displayed by the horse. The TM joint is the articulation between the base of the zygomatic process of the temporal bone and the mandibular condyle of the mandible.2 A fibrocartilaginous disc separates the joint into a large, dorsal compartment, with a rostral and caudal pouch, and a smaller ventral compartment. Whether or not the dorsal and ventral compartments communicate is disputed.2,3
The mandibular condyle is palpated as a smooth protrusion approximately midway between the base of the ear and the lateral canthus of the eye. Its identity can be confirmed by palpating the protrusion while an assistant moves the mandible. The zygomatic process of the temporal bone is identified several centimeters dorsal to the mandibular condyle. The site of centesis of the caudal pouch of the dorsal compartment is located midway between and  to
to  inch (0.64 to 1.3 cm) caudal to an imaginary line connecting these structures (Fig. 15.7).3 The needle is inserted at this site, with the horse sedated, in a rostral and ventral direction to a depth of about 1 inch (2.5 cm). Fluid may fill the hub of the needle when the needle is inserted into the pouch. The pouch is infused with 2–3 ml of local anesthetic solution. Even if the dorsal and ventral compartments do not communicate, the local anesthetic solution likely diffuses into the ventral compartment in sufficient concentration to provide analgesia of structures contained within that compartment.
inch (0.64 to 1.3 cm) caudal to an imaginary line connecting these structures (Fig. 15.7).3 The needle is inserted at this site, with the horse sedated, in a rostral and ventral direction to a depth of about 1 inch (2.5 cm). Fluid may fill the hub of the needle when the needle is inserted into the pouch. The pouch is infused with 2–3 ml of local anesthetic solution. Even if the dorsal and ventral compartments do not communicate, the local anesthetic solution likely diffuses into the ventral compartment in sufficient concentration to provide analgesia of structures contained within that compartment.

Fig. 15.7 The site of centesis of the caudal pouch of the dorsal compartment of the TM joint is located midway between  and
and  inch (0.64–1.3 cm) caudal to an imaginary line connecting the mandibular condyle and the zygomatic process. The needle is inserted in a rostral and ventral direction to a depth of about 1 inch (2.5 cm), and 2–3 ml of local anesthetic solution is infused into the pouch.
inch (0.64–1.3 cm) caudal to an imaginary line connecting the mandibular condyle and the zygomatic process. The needle is inserted in a rostral and ventral direction to a depth of about 1 inch (2.5 cm), and 2–3 ml of local anesthetic solution is infused into the pouch.
1 Fletcher BW. How to perform effective equine dental nerve blocks. In Proceedings, 50th Annual Convention of American Association of Equine Practitioners 2004; 233–236
2 Weller R, Taylor S, Maierl J, et al. Ultrasonographic anatomy of the equine temporomandibular joint. Equine Vet J. 1999;31:529–532.
3 Rosenstein DS, Bullock MF, Ocello PJ, et al. Arthrocentesis of the temporomandibular joint in adult horses. Am J Vet Res. 2001;62:729–733.