CHAPTER 23 The temporomandibular joint
Introduction
Disorders of the temporomandibular joint (TMJ) are common in human beings, having a reported prevalence of up to 80 %.1 In contrast, reports of horses affected with disease of the TMJ are sparse and are limited to reports of horses with advanced disease, perhaps not because the prevalence of the disease is low, but because definitively diagnosing disease of the TMJ of horses is difficult. In this chapter, we describe the anatomy and function of the TMJ, diseases of the TMJ, and options for medical and surgical management of horses affected with disease of the TMJ.
Anatomy
The equine TMJ is a synovial joint formed by the zygomatic process of the temporal bone and the condylar process, or condyle, of the mandible (Fig. 23.1).2,3 It is an incongruent joint and is divided completely into two separate compartments by an L-shaped, centrally concave, fibrocartilagenous disc (Fig. 23.1).2,4–7 The disc attaches circumferentially to the mandibular condyle, temporal bone, and joint capsule.5,6 The dorsal, discotemporal compartment is wider than the ventral, discomandibular compartment and apparently does not usually communicate with it,2,4–8 though in one study, communication between the compartments was demonstrated in three of seven cadaver heads injected with dye, indicating that in at least a small percentage of horses, they do communicate.9 Each compartment has a rostral and a caudal recess. The caudal recess of the discotemporal compartment is larger than the rostral recess, and the rostral recess of the discomandibular compartment is larger than the caudal recess.5,6,8 The joint capsule is reinforced by the lateral and caudal ligaments.5,6,8
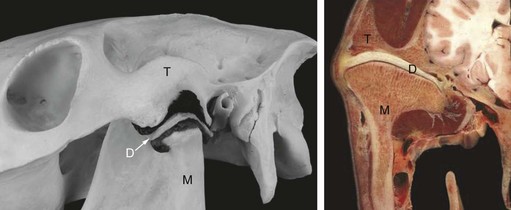
Fig. 23.1 Anatomy of the temporomandibular joint (TMJ). The image on the left shows the skeletal components of the TMJ and a corrosion cast of the dorsal and ventral compartments with the fibrocartilagenous disk wedged between them. The right image shows a transverse section through the TMJ in a frozen cadaver specimen. T, temporal bone; M, mandibular bone; D, intra-articular disc.
Muscles of mastication associated with the equine TMJ include the temporalis muscle, which attaches to the medial and rostral aspects of the joint capsule, the masseter muscle, which attaches rostrally and laterally to the joint capsule, and the lateral and medial pterygoid muscles, which attach laterally and medially to the joint capsule.3,5,6
The blood supply to the TMJ arises from the transverse facial, superficial and deep temporal, and tympanic arteries.5 The transverse facial vessels pass ventral to the TMJ, and the superficial temporal artery and vein run caudal to the TMJ. The zygomatic branch of the auriculopalpebral nerve passes caudal and dorsal to the TMJ to reach the zygomatic arch.5,6 The caudal aspect of the TMJ is covered by the rostrodorsal aspect of the parotid salivary gland, which also covers the superficial temporal artery, vein, and auriculopalpebral nerve.5,6
Function
The primary function of the TMJ is to permit mastication. Unlike ruminants, which regurgitate their food, horses only have one cycle to masticate feed to a small particle size to allow efficient microbial digestion.10 Unlike carnivores, whose power stroke of mastication is primarily vertical, the equine masticatory cycle has three distinct phases that allow for effective grinding of feed: the opening, vertical stroke; the closing, vertical stroke; and the powerful, lateral power stroke, during which feed is ground.4,11–13 The configuration of the TMJ allows this lateral movement of the mandible, which is initiated by the pterygoideus muscle. The side-to-side movement of the mandible within the joint capsule is coupled with rostrocaudal movement, with one side of the mandible gliding rostrally, and the other side of the mandible gliding caudally.4,11–13 Dental occlusion13 and type of feed12 have been found to have a significant influence on motion of the TMJ.
Diseases of the TMJ
The equine TMJ is afflicted by the same diseases that afflict other synovial joints and include acute septic arthritis,14–17 (sub)luxation,18,19 osteoarthritis,16,20 and congenital dysplasia (H. Gerhards, personal communication). Tearing of the intra-articular disc has been reported.16
Septic arthritis
Septic arthritis of the TMJ has occurred in association with open fractures and wounds that communicate with the joint or from spread of infection from surrounding tissue (e.g., from tissue infected with Streptococcus equi var. equi in horses suffering from strangles).15 In many cases, an underlying cause cannot be established, and the horses are presented because of a masticatory problem, swelling of the TMJ, or a discharging tract.14,17,21,22
Horses suffering from sepsis of the TMJ are presented for examination because they have a swelling, often painful, over the affected TMJ and are dull and have difficulty eating (Fig. 23.2).14,17,21,22 In some cases, a fistulous tract may be evident.17 Typically, the demeanor and masticatory function of horses suffering from sepsis of the TMJ improves while the horse is receiving antimicrobial therapy, but dullness and difficulty eating recur when antimicrobial therapy ceases.

Fig. 23.2 A horse affected with infectious osteoarthritis of the TMJ. The horse had a marked swelling of its left TMJ, which when palpated caused the horse to show signs of pain. A teat cannula was positioned in the caudal recess of the discotemporal compartment of the TMJ for lavage of this compartment performed with the horse sedated. The picture on the right shows the placement of a Penrose drain into a distal portal.
Unless sepsis is accompanied by fracture, luxation, or subluxation, radiographic examination of the TMJ is often inconclusive, and another imaging modality, such as ultrasonography, scintigraphy, or computed tomography, is needed to diagnose septic osteoarthritis.17,23 Arthrocentesis of a septic TMJ typically yields abnormal-appearing synovial fluid that contains an increased nucleated cell count.14 Streptococcus zooepidemicus is often cultured from an infected TMJ.14,17,22
(Sub)luxation
The TMJ can become luxated or subluxated, with or without fracture of the mandible.18,19,24 Affected horses usually have evidence of trauma to the head. Clinical signs depend on the degree of luxation and may include acute swelling of the region of the TMJ, rostral displacement of the mandible, decreased lateral range of movement of the mandible, an inability to open the mouth, difficult mastication, and rupture of an eye. Horses with a luxated or subluxated TMJ may develop osteoarthritis regardless of whether or not they are treated.
Osteoarthritis
Clinical signs of disease displayed by horses with osteoarthritis of the TMJ are often similar to signs of disease displayed by horses with septic arthritis of that joint, though the clinical signs displayed by horses with osteoarthritis are often less severe and their onset is more insidious.16,23,24 Affected horses typically show a decreased range of mandibular motion and masticate preferentially on the non-affected side of the mandible. Joint distension and bony swelling are usually present over the affected TMJ, and if the disease is chronic, atrophy of the masseter muscles may be evident.
A strong association between disorders of the TMJ and dental malocclusion has been demonstrated in human beings,25 and this same association is noted in horses chronically affected with osteoarthritis of the TMJ. The incisor arcades of horses chronically affected may become slanted, and the molar arcade on the affected side of the head may wear at an extremely steep angle, causing shear mouth. Determining whether disease of the TMJ is a result or a cause of abnormality of the incisor arcades may be difficult. Osteoarthritis has occurred secondary to rupture of the articular disc, but most commonly, no underlying cause is identified.16
Identifying arthritis of the TMJ radiographically is often difficult, and other methods of imaging the joint, such as ultrasonography or scintigraphy, may be more useful. Ultrasonographic features of an arthritic TMJ include an irregular contour to both the temporal and mandibular components of the joint and an abnormally large volume of synovial fluid (Fig. 23.3). Typical scintigraphic findings include a mild to moderate increase in radiopharmaceutical uptake over the affected joint compared to the unaffected, contralateral TMJ. Arthrocentesis of the arthritic TMJ yields synovial fluid that is less viscous than normal and that has a normal nucleated cell count and a normal or mildly elevated concentration of protein. Proliferative new bone formation and cartilage loss are features observed during arthroscopic examination of the joint (Fig. 23.4).


Diagnosis of disease of the TMJ
Clinical examination
Clinical signs associated with disorders of the TMJ range from very specific (e.g., swelling over the joint, a discharging sinus tract from the joint, or displacement of the mandible) to non-specific (e.g., headshaking, head-tilt, reluctance to be ridden, and weight loss). Clinical examination should start with observing the horse for signs of disease reported by the owner. If signs of disease are vague, examination of multiple body systems may be necessary before the TMJ is incriminated as the source of these vague signs.
Examination of a horse suspected of having a disorder of the TMJ should include careful inspection of the horse while it masticates rough feed, and special attention should be paid to the symmetry of the side-to-side movement of the jaw. The TMJs work as a functional unit, and in normal horses, the grinding motion is symmetrical. Pain or mechanical impairment at the TMJ results in a reduced range of motion of the mandible on the affected side. If disease of a TMJ is suspected, the dental arcades should be examined because disease of one or both TMJs commonly results in malocclusion.20,26
Systematic palpation of the TMJ region may cause the horse to demonstrate signs of pain or may reveal a swelling of soft tissue or bony consistency (Fig. 23.2). The TMJ is located by following the mandibular ramus dorsally. The palpable depression representing the neck of the mandibular condyle should not be mistaken for the TMJ. The joint space lies dorsal to the mandibular condyle, the lateral aspect of which can be palpated as a smooth projection lying halfway between the lateral canthus of the eye and the base of the ipsilateral ear. Making the horse move its mandible while palpating this region helps to locate the mandibular condyle. In our experience, findings during palpation vary widely between horses, depending on the breed and condition of the horse. In some horses, the pouches of the joint capsule, especially the caudal pouch of the discotemporal compartment, are very prominent, but the pouches of the discomandibular compartment cannot be palpated. The lateral aspect of the mandibular condyle of some horses is very prominent, but that of others is very difficult to palpate. Even though the palpable portion of the TMJs varies in morphology, the left and right regions of the TMJ should be symmetrical. To better appreciate function of the joint, the joint can be palpated while the horse chews.
Intra-articular anesthesia and arthrocentesis
Because the TMJ is separated completely into two compartments by the articular disc, each compartment probably must be injected separately to completely desensitize the entire joint. No studies have examined the likelihood of local anesthetic solution diffusing in a high enough concentration from one compartment to the other to result in desensitization of both compartments. Centesis of the TMJ performed directly over the joint is difficult because articular cartilage and the meniscus primarily occupy this space, and consequently centesis is most reliably performed over the caudal pouch of the dorsal compartment. The technique of arthrocentesis was thoroughly described by Rosenstein et al (2001)9 and Weller et al (2002).27 Using the approach to the caudal pouch of the dorsal compartment (i.e., the discotemporal compartment) described by Rosenstein et al (2001),9 the mandibular condyle is identified as a smooth protrusion approximately midway between the lateral canthus of the eye and the base of the ear. The zygomatic process of the temporal bone is palpated 1–2 cm dorsal to the condyle, and a line is imagined between these structures. The site of centesis is a depression midway between these structures and  to 1 cm caudal to the imagined line. The discotemporal compartment is desensitized with 2–2.5 ml of local anesthetic solution (Fig. 23.2). The ventral compartment (i.e., the discomandibular compartment) is injected with 1–1.5 ml of local anesthetic solution by walking the needle off the rostral aspect of the mandibular condyle.
to 1 cm caudal to the imagined line. The discotemporal compartment is desensitized with 2–2.5 ml of local anesthetic solution (Fig. 23.2). The ventral compartment (i.e., the discomandibular compartment) is injected with 1–1.5 ml of local anesthetic solution by walking the needle off the rostral aspect of the mandibular condyle.
Although the capsule of both pouches is relatively superficial, care must be taken not to inject the anesthetic solution outside the joint capsule where it may anesthetize branches of one of the cranial nerves in this area. In some cases, performing the procedure under ultrasonographic control may be beneficial. In our experience, the clinical signs of disease displayed by the majority of horses with TMJ disorders, such as decreased range of mandibular motion, resolve while the TMJ is temporarily desensitized. If the joint has advanced osteoarthritis, mobility of the mandible may be mechanically impaired.
Radiography
Radiographic evaluation of the TMJ is challenging, largely because the complexity of this area results in numerous superimpositions over the joint.28–30 To alleviate the problem of superimposition, the TMJ can be examined radiographically using special projections. To obtain the radiographic projection described by Pommer (1948),31 the X-ray cassette is placed 120 cm lateral to the TMJ of interest, and the X-ray beam is directed toward the contralateral TMJ (Fig. 23.5). Using this technique, the TMJ of interest is magnified to such a degree that evaluation of that joint is enhanced. This technique exposes the horse to a high concentration of radiation and consequently, the eye of the horse nearest the X-ray tube should be protected with a lead shield.
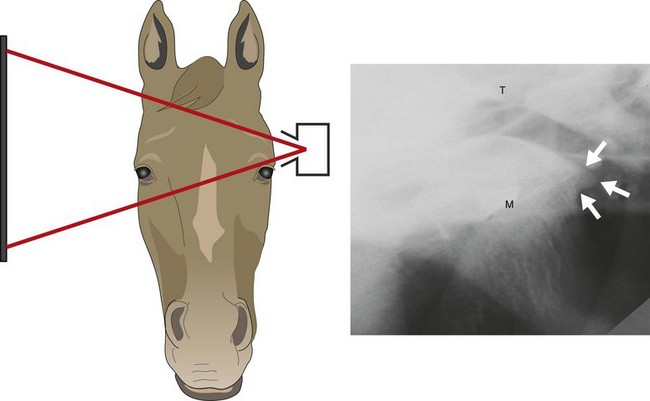
Fig. 23.5 Radiographic projection of the TMJ. The image shows a projection of the left TMJ of a 23-year-old horse. This projection, described by Pommer (1948),31 allows evaluation of the TMJ of interest by magnifying the superimposed contralateral TMJ. Note the osteophyte on the caudal aspect of the mandibular condyle (arrows), which is commonly seen in old horses.
Recently, two oblique projections have been described that allow evaluation of the TMJ and surrounding osseous structures without superimposition of contralateral structures.32,33 For one of these projections, the X-ray cassette is placed above the horse’s poll in a horizontal position, with the horse’s head fully extended, and the X-ray beam centered on the ipsilateral TMJ and directed caudally at a 35° angle to the long axis of the head and 50° dorsally.32 For the other projection, the horse’s head is held in a neutral position, and the cassette is placed parallel to the sagittal plane next to the TMJ of interest. The X-ray beam is directed caudodorsally to rostroventrally, from the contralateral side, to the TMJ of interest (Fig. 23.6).33 If the TMJ of interest is the left TMJ, this projection is termed a right, caudodorsal-to-left, rostroventral oblique (Rt15Cd70D-LeRVO). Both projections allow evaluation of subchondral bone, a feature not allowed by other radiographic projections.
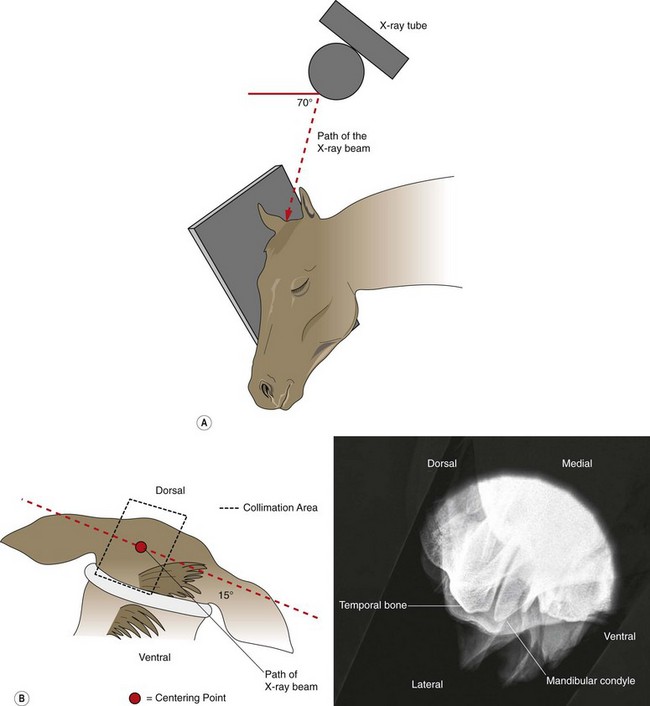
Fig. 23.6 Tangential projection of the equine TMJ described by Townsend (2009).33 (A) This schematic drawing illustrates the X-ray beam angle at 70° to the dorsal plane and cassette; (B) Dorsal view of the radiographic projection showing the beam angle at 15° to the centering point and the collimation area. The radiographic image on the right is the result of this projection.
A luxation or subluxation of the TMJ, with or without a fracture(s), is usually easily identified on radiographs as an incongruence of the bony surfaces of the TMJ and an incongruence of the occlusal surfaces of the incisors and cheek teeth. Osteoarthritic changes are much more difficult to appreciate radiographically. If osteoarthritis is severe, an irregular outline of the bones forming the joint, as well as periarticular new bone formation and changes in the width of the joint, can be appreciated. In our experience, the majority of old horses have some degree of osteophyte formation on the caudal aspect of the mandibular condyle (Fig. 23.5) yet show no clinical signs of disease of the TMJ, indicating that osteophytes in this area may not be clinically significant. Mild changes of osteoarthritis are difficult to appreciate during radiographic examination of the TMJ.
Scintigraphy
Scintigraphy is an imaging modality that portrays function rather than morphological changes. It is the most sensitive of all imaging modalities for a variety of diseases, including dental disorders.27 To examine the TMJs of a horse scintigraphically, the horse is injected intravenously with 5 MBq/kg 99mTc-phosphonate. This dosage equates to half the dose usually used for imaging other parts of the horse, but in our experience, this reduced dose is sufficient to evaluate the head. We have found that the vascular and soft tissue phases are not useful for this area, and therefore we perform only a bone phase, usually about three hours after injection. Left and right lateral projections and a dorsal projection, each centered over the TMJ of interest, are acquired. Both TMJs should be adjacent to the camera during acquisition of images to avoid differences in radiopharmaceutical uptake caused by distance attenuation of the gamma radiation.
The resulting images should be evaluated visually, as well as quantitatively, by defining regions of interest (ROI) over the TMJs. On the dorsal projection the ROIs are compared directly, whereas on the lateral projections reference ROIs are defined over the ramus of the mandible (Fig. 23.7). The ratio between the ROI over the TMJ and the reference ROI is calculated and compared between sides. Radiopharmaceutical uptake by structures of the head, including the TMJs, varies with the age of the horse. The TMJs of young horses take up considerably more of the radiopharmaceutical drug than does the relatively inactive rest of the mandible, whereas the TMJs of old horses often cannot be differentiated from the surrounding tissues (Fig. 23.8). In our experience, a difference in radiopharmaceutical uptake by a TMJ of more than 25 % is indicative of disease of that joint.
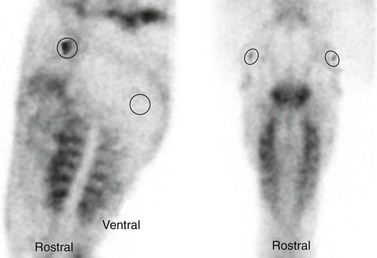
Fig. 23.7 Lateral (left image) and dorsal (right image) scintigrams of the TMJs of a horse, 3 hours after the horse was injected with TC99m-methylendiphosphonate. Regions of interest are drawn around the TMJs, and reference regions of interest (ROIs) are defined over the ramus of the mandible. The ratio between the ROI over the TMJ and the reference ROI is calculated and compared between sides.
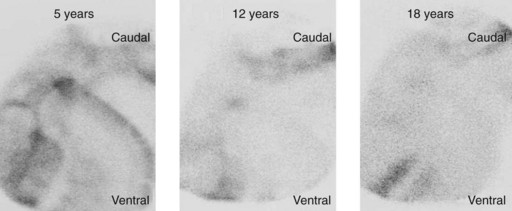
Fig. 23.8 Left lateral scintigrams of the TMJs of three horses of different ages, 3 hours after injection of TC99m-methylendiphosphonate. The uptake of the radiopharmaceutical drug decreases remarkably as horses age.
The left and right TMJs are structurally linked and, therefore, function as a unit. Disorders of the TMJ of human beings resulting from malocclusion are often bilateral, and we believe disorders of the TMJ of horses are likewise bilateral. Marked radiopharmaceutical uptake over both TMJs in an old horse may be suggestive of disease of both TMJs.
Ultrasonography
Ultrasonographic examination of the TMJs is easily performed with the horse standing and is usually well tolerated by the horse.7,34 To obtain optimal quality of the image, hair over the TMJ to be examined should be clipped, but the procedure can sometimes be performed adequately without clipping the hair. The area is cleansed and covered with a coupling gel. Both TMJs should be examined for comparison. A 7.5 MHz (or higher) linear array transducer provides sufficient depth to image the TMJ, while still providing excellent resolution of the images.
The transducer should be positioned perpendicular to the joint space to acquire transverse images of the joint, and so, to keep the transducer perpendicular to the curved outline of the lateral aspect of the joint, the transducer must be rotated as the joint is examined. To examine the TMJ ultrasonographically, we follow the mandible dorsally with the transducer orientated approximately parallel to the dorsal outline of the horse’s nose until the caudal aspect of the joint can be imaged. To image the medial aspect of the joint, the transducer is rotated dorsorostrally by 45°. To image the rostral part of the joint, the transducer is rotated another 30°in the same direction while applying slight rostroventral translation. A stand-off is usually not required, but may be useful if the horse is thin.
The ultrasonographic examination allows evaluation of the bony surfaces of the joint, the fibrocartilagenous disc, and the joint capsule, and quantification of the amount of synovial fluid within the joint. The surface of the bones should appear as smooth, hyperechogenic lines. The disc appears as a homogenous wedge, the base of which is located laterally and the apex of which points medially, between the surface of the zygomatic process of the temporal bone and the surface of the mandibular condyle and is similar in echogenicity to the menisci in the stifle. The caudal recess of the discotemporal compartment of the TMJ is filled with synovial villi and is difficult to distinguish ultrasonographically from the disc. The joint capsule is visible as an interface between the disc and the parotid salivary gland, which overlies it on the caudal part of the joint, or subcutaneous tissue, which overlies it on the rostral part of the joint. No synovial fluid, or only a very minimal amount, is visible if the TMJ is normal. Changes in the TMJ seen ultrasonographically that are pathognomonic for disease of the joint include irregular outline of the bony surfaces, increased amount of synovial fluid, hyperechogenicity of the synovial fluid, disruption of the homogenous appearance of the disc, or thickening of the joint capsule (Fig. 23.3).
Computed tomography
Computed tomography (CT) is the method of imaging of choice for diagnosing disorders of the TMJ of human beings and small animals.35 It allows the medial components of the joint to be evaluated without superimposition of other structures. Computed tomographic anatomy of the normal TMJ of horses has been described,36 and CT has been used to diagnose septic arthritis of the TMJ of a horse.17 Until recently, to image the head of a horse using CT, the horse had to be anesthetized, which increased the costs and risks of the procedure. Now, some equine referral centers can perform CT scans of the head with the horse sedated, which has led to a wider use of this modality for diagnosing disorders of the equine head.
Treatment
Horses with a disorder of the TMJ can be treated conservatively or surgically, according to the type of disorder.
Conservative treatment
Conservative treatments available for horses with a disorder of the TMJ are similar to those available for a horse with a disorder of any other similarly affected joint with similar likelihood of success. Intra-articular injection of a corticosteroid has been used successfully to treat horses with non-septic osteoarthritis of the TMJ.16 We have observed good, long-term outcome after administering methylprednisolone acetate into the TMJ of horses affected with osteoarthritis of that joint. Those horses that did not respond to treatment had evidence of advanced osteoarthritis seen during post-mortem examination (Fig. 23.4). We have had limited success in resolving clinical signs of osteoarthritis of the TMJ after administering a glycosaminoglycan and hyaluronic acid into the TMJ.
Dental malocclusion accompanies disease of the TMJ of human beings and likely also accompanies disease of the TMJ of horses. Determining whether disease of the TMJ is a result or a cause of abnormal malocclusion may be difficult. Horses affected with disease of a TMJ should be carefully examined for dental malocclusion, and any occlusal abnormalities, such as shear mouth and slant mouth, should be corrected.
Surgical treatment
There are few reports of surgical management of horses with disease of the TMJ. Rostral luxation of a TMJ of one horse was successfully corrected, with the horse anesthetized, by placing a metal mouth gag between the cheek teeth on the affected side and placing pressure on the rostral aspect of the mandible and on the rostral aspect of the maxillae to close the mouth.19 After recovering from anesthesia, the horse was able to masticate food, though the horse was permanently blind in the ipsilateral eye, probably from damage to the eye inflicted by the coronoid process of the mandible when it displaced rostrally.
Arthroscopic evaluation of osteoarthritic TMJs and arthroscopic lavage of septic TMJs have been described.8,14,16 Due to the bipartite nature of the TMJ, the discotemporal and discomandibular compartments of the TMJ must be evaluated through individual arthroscopic portals, but only the lateral aspect of the discotemporal joint can be evaluated fully because the curvature of the mandibular condyle renders the rest of the joint inaccessible.6,8 Authors of one report declared the discomandibular joint to be inaccessible because of the position of the transverse facial artery and vein;8 other authors reported it to be accessible, though difficult to evaluate due to obstruction of vision by synovial villi and poor maneuverability.6
To examine the TMJ joint arthroscopically, the horse is anesthetized and positioned in lateral recumbency with the affected TMJ uppermost. The horse can be positioned in dorsal recumbency if both TMJs are to be arthroscopically examined. After preparing the region of the TMJ for aseptic surgery, the TMJ is distended with sterile, isotonic saline solution after inserting a needle into the compartment of the joint using a technique described above, with or without ultrasonographic guidance. The needle is left in place, and a longitudinal, 5 mm long, skin incision is made adjacent to it. An arthroscopic sleeve and blunt obturator are introduced into the joint, through the incision, in a rostromedial direction. The obturator is replaced with a 4-mm diameter, 30°, forward arthroscope, and the joint is distended, through the arthroscope, with sterile, isotonic saline solution. A needle can be placed into the joint further rostrally to allow egress of fluid, which is important for improving visualization if the original penetration by the obturator caused intra-articular hemorrhage, and for providing continuous lavage of the joint.
A septic discotemporal compartment can be lavaged with the horse standing and sedated if financial constraints imposed by the owner make performing the procedure with the horse anesthetized unfeasible. The region of the affected TMJ is prepared for aseptic surgery, and local anesthetic solution is infiltrated subcutaneously at the site for arthrocentesis of the caudal recess of the discotemporal compartment described above. This is a palpable depression just dorsal and caudal to the mandibular condyle, which lies halfway between the lateral canthus of the eye and the base of the ipsilateral ear. A needle is placed into the discotemporal compartment, and the joint is distended with 10–25 ml of sterile, isotonic saline solution. A 5-mm long, longitudinal incision is made in the skin at this site with a no. 15 blade. A 10-cm long, blunt, teat cannula with obturator is placed through this incision and directed rostromedially into the joint (Fig. 23.2). Egress of fluid confirms that the cannula has been placed into the joint. A 16-gauge, 2.54-cm (1-inch) needle is placed in the most dependent part of the distended TMJ, and a 5-mm long, longitudinal skin incision made adjacent to it. A second teat cannula is placed through this incision into the compartment to allow egress of fluid introduced into the joint through the other teat cannula. After the joint has been lavaged, a Penrose drain can be placed into the TMJ through the ventral skin incision (Fig. 23.2) and maintained, with a suture, for several days before it is removed.
Unilateral, mandibular condylectomy and meniscectomy has been reported to be a successful treatment for horses with severe septic or non-septic osteoarthritis of the TMJ.22,24,37 When mandibular condylectomy was performed bilaterally, more severe and longer-lasting abnormalities of mastication were observed.37 Deviation of the mandible toward the non-treated side was reported to occur after unilateral condylectomy and meniscectomy.37 Deviation was thought to be caused by a temporary lack of stability of the joint and atrophy of the masseter muscle on the treated side. A horse in a more recent report, however, did not experience deviation of the mandible after unilateral condylectomy and meniscectomy and had immediate improvement in its ability to open its mouth and to masticate.22
1 Rugh JD, Solberg WK. Oral health status in the Unites States: temporomandibular joint disorders. Journal of Dental Education. 1985;49:398–405.
2 Barone R. Articulation temporo-mandibulaire. Paris: Vigot; 1989.
3 Hillman DJ, ed. Scisson and Grossman’s Anatomy of the domestic species. Philadelphia: W.B. Saunders, 1975.
4 Baker GJ. Equine temporomandibular joints (tmj): morphology, function and clinical disease. Proceedings AAEP. 2002;48:442–447.
5 Rodriguez MJ, Agut A, Gil F, Latorre R. Anatomy of the equine temporomandibular joint: study by gross dissection, vascular injection and section. Equine Vet J. 2006;38(2):143–147.
6 Weller R, Maierl J, Bowen IM, et al. The arthroscopic approach and intra-articular anatomy of the equine temporomandibular joint. Equine Vet J. 2002;34(4):421–424.
7 Weller R, Taylor S, Maierl J, et al. Ultrasonographic anatomy of the equine temporomandibular joint. Equine Vet J. 1999;31(6):529–532.
8 May KA, Moll HD, Howard RD, et al. Arthroscopic anatomy of the equine temporomandibular joint. Vet Surg. 2001;30(6):564–571.
9 Rosenstein DS, Bullock MF, Ocello PJ, Clayton HM. Arthrocentesis of the temporomandibular joint in adult horses. Am J Vet Res. 2001;62(5):729–733.
10 Dixon PM. Dental anatomy. In: Baker GE, Easley J. Equine dentistry. 2nd edn. Edinburgh: Elsevier; 2005:25–48.
11 Bonin SJ, Clayton HM, Lanovaz JL, Johnson TJ. Kinematics of the equine temporomandibular joint. Am J Vet Res. 2006;67(3):423–428.
12 Bonin SJ, Clayton HM, Lanovaz JL, Johnston T. Comparison of mandibular motion in horses chewing hay and pellets. Equine Veterinary Journal. 2007;39(3):258–262.
13 Simhofer H, Anen C, Niederl M, et al. Comparison of the Masticatory Cycles of Horses Before and after Dental Treatment Using Kinematic Analysis. In: 6th international Conference on Equine Locomotion. France: Cabourg; 2008. p. 19
14 Carmalt JL, Wilson DG. Arthroscopic treatment of temporomandibular joint sepsis in a horse. Vet Surg. 2005;34(1):55–58.
15 Silbersiepe E. Die Entzündung des Kiefergelenkes. In: Silbersiepe E, Berge E, Müller H. Lehrbuch der Speziellen Chirurgie für Tierärzte und Studierende. Stuttgart: Ferdinand Enke Verlag; 1986:119–120.
16 Stadtbäumer G, Boening KJ. Diagnostische und arthroskopische Verfahren am Kiefergelenk des Pferdes. Tierärztl Prax. 2002;30:99–106.
17 Warmerdam EP, Klein WR, van Herpen BP. Infectious temporomandibular joint disease in the horse: computed tomographic diagnosis and treatment of two cases. Vet Rec. 1997;141(7):172–174.
18 Hardy J, Shiroma JT. What is your diagnosis? Rostral luxation of the right temporomandibular joint. J Am Vet Med Assoc. 1991;198:1663–1664.
19 Hurtig MB, Barber SM, Farrow CS. Temporomandibular joint luxation in a horse. J Am Vet Med Assoc. 1984;185(1):78–80.
20 Grosse G. Die Veränderungen am Kiefergelenk des Pferdes in Verbindung mit Zahn- und Gebißanomalien, Veterinärmedizinische Dissertation. Leipzig: Justus Liebig Universität; 1938.
21 Devine DV, Moll HD, Bahr RJ. Fracture, luxation, and chronic septic arthritis of the temporomandibular joint in a juvenile horse. Journal of Veterinary Dentistry. 2005;22(2):96–99.
22 Nagy AD, Simhofer H. Mandibular condylectomy and meniscectomy for the treatment of septic temporomandibular joint arthritis in a horse. Vet Surg. 2006;35(7):663–668.
23 Weller R, Cauvin ER, Bowen IM, May SA. Comparison of radiography, scintigraphy and ultrasonography in the diagnosis of a case of temporomandibular joint arthropathy in a horse. Vet Rec. 1999;144(14):377–379.
24 Patterson LJ, Shappell KK, Hurtig MB. Mandibular condylectomy in a horse. J Am Vet Med Assoc. 1989;195(1):101–102.
25 Payne M, Nakielny RA. Temporomandibular joint imaging. Clin Radiol. 1996;51(1):1–10.
26 May KJ. Incisor problems that may result in inflammation of the temporomandibular joint. Pferdeheilkunde. 1996;12:716.
27 Weller R, Livesey L, Maierl J, et al. Comparison of radiography and scintigraphy in the diagnosis of dental disorders in the horse. Equine Vet J. 2002;33(1):49–58.
28 Gibbs C, Lane JG. Radiographic examination of the facial, nasal and paranasal sinus regions of the horse. II. Radiological findings. Equine Vet J. 1987;19(5):474–482.
29 Park RD. Radiographic examination of the equine head. Vet Clin North Am Equine Pract. 1993;9(1):49–74.
30 Wyn-Jones G. Interpreting radiographs 6: Radiology of the equine head (Part 2). Equine Vet J. 1985;17(6):417–425.
31 Pommer A. Die röntgenologische Darstellung des Kiefergelenkes des Pferdes. Wiener Tierärztliche Wochenschrift. 1994;36:230.
32 Ramzan PH, Marr CM, Meehan J, Thompson A. Novel oblique radiographic projection of the temporomandibular articulation of horses. Vet Rec. 2008;162(22):714–716.
33 Townsend NB, Cotton JC, Barakzai SZ. A tangential radiographic projection for investigation of the equine temporomandibular joint. Vet Surg. 2009;38(5):601–606.
34 Rodriguez MJ, Soler M, Latorre R, et al. Ultrasonographic anatomy of the temporomandibular joint in healthy pure-bred Spanish horses. Vet Radiol Ultrasound. 2007;48(2):149–154.
35 Schwarz T, Weller R, Dickie AM, et al. Imaging of the canine and feline temporomandibular joint: a review. Vet Radiol Ultrasound. 2002;43(2):85–97.
36 Rodriguez MJ, Latorre R, Lopez-Albors O, et al. Computed tomographic anatomy of the temporomandibular joint in the young horse. Equine Vet J. 2008;40(6):566–571.
37 Barber SM, Doige CE, Humphreys SG. Mandibular condylectomy – Technique and results in normal horses. Veterinary Surgery. 1985;14(2):79–86.