1 The history of frequency-specific microcurrent
The history of electromagnetic therapies
Starting in the late 1800s there was a tremendous upwelling of interest in electromagnetism and electrical effects. In the early 1900s, medical physicians and osteopaths were interested in using electromagnetic therapies and frequencies as a way of treating patients. The devices and techniques were used by thousands of doctors but were not accepted by the medical establishment. Albert Abrams, MD used electromagnetic therapies in his San Francisco clinic from 1914 until his death in 1937. He founded the Electromedical Society and the journal Electromedical Digest as a way for practitioners to communicate and share their research and treatment findings (ERA 1980). In 1934 the American Medical Association, in its efforts to standardize medical education and treatments, decreed that drugs and surgery were the accepted tools of medicine and anyone using electromagnetic therapies would lose their license to practice which at that time was granted by the AMA. The research and clinical use of electromagnetic therapies in medicine came to a halt and by the early 1950s the necessary devices were rendered illegal in the United States by the FDA, after which, electromedical practice gradually died out although the early devices remained in use in private medical and osteopathic practices around the US, Canada and England.
Where the frequencies came from
In the late 1940s, after his service in World War II, Harry Van Gelder, an osteopath and naturopath trained in England and Australia bought a small private osteopathic practice in Vancouver BC that came with one of these early electromedical machines and a list of frequencies. He taught himself to use the machine and apply the frequencies, and achieved a degree of notoriety as a successful healer. Using the machine, the frequencies, osteopathic manipulation, homeopathy and nutrition he treated patients from all over Canada and the US for ailments ranging from back pain to cancer and his fame grew along with his success. In 1955 he moved his practice and his family back to Australia, returning in 1972, to practice in Ojai, California. Using the same tools and achieving the same level of success, his notoriety grew and patients once again found him from all over the US and Canada.
In 1980 a chiropractic student named George Douglas heard about Dr. Van Gelder’s practice in Ojai and spent three months working with him to learn his methods. Dr. Douglas came home with the list of frequencies and put them in a drawer as a memento. After graduating from Western States Chiropractic College in Portland Oregon in 1983, he began teaching in the student health center where I met him in 1991 when I was a third year chiropractic student. In 1992 Dr. Douglas purchased a Precision Microcurrent instrument because it had two channels, as did Dr. Van Gelder’s antiquated machine, and he had the idea that it might be useful as a way of delivering the frequencies.
First uses of microcurrent and the frequencies
Microcurrent was introduced in the United States as a physical therapy modality in the late 1970s by a chiropractor and acupuncturist Dr. Thomas Wing. Dr. Wing used four low frequencies such as .3Hz, .6Hz, 10Hz, and 30Hz delivered with single channel microcurrent unit using cotton tipped probes and eventually a double channel microcurrent called the “Myomatic I” (I = interferential). Because of its ability to increase ATP production (Cheng 1982) microcurrent was being used by Dr. Wing and others to increase the rate of healing in injured athletes, to control pain, to increase the rate of fracture repair and wound healing and to treat myofascial pain.
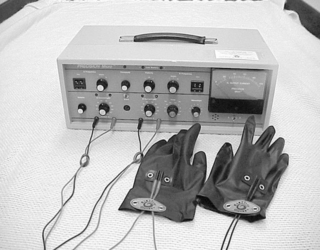
Figure 1.2 • The original Precision Microcurrent could deliver frequencies accurate only to two digits. If the switch was set to 19 the .1, 1, and 10 multiplier could form 1.9, 19, and 190 but not 191, which was needed for tendons or 195 which was used for the bursa. The two-digit specific unit gave way to the three-digit unit in 1999.
Microcurrent delivers subsensory current in millionths of an ampere compared to the milliamps current, one thousand times stronger, used in other widely used electrotherapies such as interferential and TENS which makes muscles contract and can be felt as a buzzing or pulsing. One micro amp (μA) is the same 1/1000 of a milliamp (mA). The current cannot be felt and is the same level of current that the body itself produces in every cell and tissue.
Microcurrent and the frequencies were used on family and friends for two years starting in 1993 when I graduated from Chiropractic College producing some positive response and no negative effects from use of the frequencies or the current. I bought a small chiropractic practice in 1994 and introduced microcurrent into my practice in 1995 as a way of treating fibromyalgia and myofascial pain patients. We used standard adhesive electrode pads to connect the machine to the patient and set the microcurrent machine for various frequencies and observed the responses. Not all of the frequencies produced beneficial results but none of them produced any adverse effects so we felt comfortable exploring further to see what was possible.
Open-minded friends interested in the treatment concept volunteered to be treated. A family friend came over one afternoon and after hearing about our new discovery asked us to try treating his back. Twenty years previously he had fallen off of a ladder and landed flat on his back creating a massive bruise the length of his trunk. His back was still sore and tender to touch 20 years after the injury and he wanted to see if it could be changed. The muscles in his back felt stiff, hardened and almost crunchy as the adhesive electrode pads were applied on the four corners of his torso and microcurrent and the frequencies on Van Gelder’s list for reducing fibrosis, “deep old bruise” and mineral deposits were used on the injured tissue. Much to our surprise, the pain disappeared and the tissue became soft, non-tender and pliable in 30 minutes giving a glimmer of what was to come.
Clinical practice using frequencies
By 1996, I had a typical suburban chiropractic practice focused on musculoskeletal pain and injury. The joint manipulation, adjusting, massage and manual trigger point therapy taught in Chiropractic College were the tools available to treat patients. I was a new practitioner in a small practice, seeing about 35 patients a week, and wanting to expand my patient services, I bought a microcurrent device used by estheticians intended to provide facial anti-aging skin treatments. This skin care microcurrent used a pair of graphite conducting gloves to carry the current to the patient’s skin. Before and after photographs showed dramatic improvement in lines, wrinkles and jowls, and it was likely that patients would pay cash for such treatments and increase the practice revenue. I never suspected where it would end up.
In January 1996, one of the afternoon patients was a crane operator who had been injured in an auto accident four months before. His job required that he look down from his control station at the top of the crane and turn his head as he moved train cars and ship containers around a large freight yard. The auto accident had injured the muscles in his neck and created myofascial trigger points that made him dizzy when he activated these muscles. He had a sturdy thick neck, and three months of manual trigger point therapy had produced only minimal improvement in symptoms. His neck muscles felt firm, hardened and almost crunchy. In fact, they felt exactly like my friend Chuck’s chronically painful, long-ago injured back muscles had felt the week before.
The similarity between the feeling of the neck muscles and Chuck’s back muscles made me think of using the frequencies and microcurrent. The graphite gloves were attached to the skin care microcurrent unit across the hall and fit perfectly when moved to the leads on the two-channel Precision Microcurrent machine in the patient’s treatment room. I wondered out loud if the frequencies would have the same effect on this patient’s neck muscles as they had on Chuck’s back muscles. The patient asked whether it would hurt, and when told that it wouldn’t, he encouraged me to give it a try.
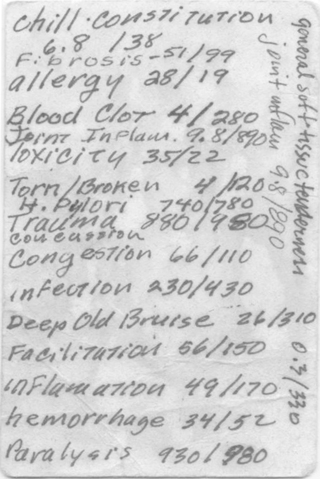
The frequencies we used to treat our friends and family were written on the back of a business card stored in the top of the machine. The frequencies were set on the machine, it was turned on, the gloves were moistened to allow proper conduction of the imperceptible current and the gloves were placed on the patient’s neck. The treatment had the immediate and totally unexpected effect of making the muscles go completely soft or “smooshy”. It was as if the tissue changed state from a solid to a gel. The taut bands disappeared instantly, as did the patient’s pain, and the treatment was complete in 30 minutes. In five years of training and practice doing manual massage and trigger point therapy no tissue had ever changed the way this tissue did. Surprise and disbelief were replaced by curiosity when the effects proved to be permanent and the symptoms resolved completely in one additional treatment.
The next patient who came in with pain from myofascial trigger points had the same positive response to the same frequencies. The muscle went smoosh, the taut bands disappeared, the pain went away and the changes became permanent in a very few treatments. Within the week every patient who came in was being treated for their muscle pain with microcurrent and frequencies. In every case muscles went smoosh, taut bands disappeared, pain went away and the changes were sometimes permanent and sometimes not. Local doctors began referring their fibromyalgia and myofascial pain patients to the clinic after hearing me speak at a continuing education course on fibromyalgia offered at Portland State University in 1995. The small chiropractic clinic became the Fibromyalgia and Myofascial Pain Clinic of Portland, developing a reputation and a client base of difficult to treat chronic pain patients. Soon, every patient who came into the clinic with pain was being treated with the graphite gloves and the frequencies and the positive responses grew more consistent. By March, dozens of patients had responded well and there was some real excitement about our results. Then quite suddenly, two people changed the practice forever.
FSM clinical practice expands
Dr. Paul Puziss, an open minded orthopedic surgeon specializing in arthroscopic shoulder surgery, worked well with chiropractic physicians and had an appreciation for the effects of myofascial trigger points as pain generators. Dr. Puziss operated on a clinic patient and, following the six-week surgical recovery, Dr. Puziss sent him back for what he thought would be months of standard manual trigger point therapy. Dr. Puziss saw the patient for his follow-up after only two microcurrent treatments and called the clinic immediately asking, “What did you do? I have never seen anyone recover motion so quickly after a surgery!” He listened to the explanation of the new treatment method and responded by sending every failed shoulder pain patient in his practice to the clinic in the spring of 1996. Shoulder patients, as it turns out, have very particular patterns of muscle, nerve and joint dysfunction and learning the techniques to treat them successfully took the better part of a year. The lessons learned from these early patients formed the basis of what has been taught in FSM seminars ever since.
In March 1996, a colleague at a local continuing education seminar asked politely, “How are things going?” She listened to the stories of our incredible success using microcurrent to treat myofascial trigger points, and within weeks she started referring patients. Over the next six months she referred dozens of her most difficult, impossible-to-treat, post-injury, chronic pain patients and their response to frequencies and current taught us how to use FSM.
In 60 days, the small chiropractic practice became a chronic pain clinic, doubled in size from 45 patients a week to 90 patients a week, and maintained this pace for the next four years. The lessons learned about treating chronic pain patients during that period are the foundation of what is taught today as Frequency-specific Microcurrent.
Developing the protocols
The results produced in treating simple myofascial trigger points were nothing short of miraculous and the patients for whom it was not effective eventually became the exception not the rule. Patients who had been helped told friends and family and the practice continued to grow. Assistants were needed to keep the office working efficiently. In June of 1996, Kristi Hawkes, a student at the National College of Naturopathic Medicine (NCNM) in Portland, began working ten hours a week in the clinic, helping with FSM treatments as a student “preceptor”. We wanted to demonstrate to ourselves that our positive results were not due to the placebo effect from the patient’s or the doctor’s positive expectation. We set up an ongoing experiment where Kristi operated the machine and the patients were treated with the machine facing away from me. For a few months, nothing was said in the treatment room that would give the patient encouragement and in some cases somewhat discouraging comments were made to see if expectation made a difference. Some treatments were started with the machine turned off to see if there was a noticeable difference in tissue response. Each time the machine was off the usual softening of the muscles did not occur and it was noticed immediately. The pain reduction and tissue softening response only happened when the machine was on and never happened if the machine was off. It became apparent that it was not any positive expectation or magic hands that produced the changes in tissue. It had to be the treatment itself, and we closed that experiment.
The technique needed to be fine tuned and standardized. There were frequencies to remove pathologies such as inflammation, fibrosis, chronic inflammation, toxicity and scar tissue and frequencies for tissues such as muscle, fascia and nerve. The machine had two channels that could deliver frequencies. Channel A fired 2 milliseconds before channel B fired. Which frequency went on which channel? Did it matter? In what order did we need to run them to achieve optimal results? What conditions would respond and what conditions would not? In June of 1996 none of these questions had answers. The clinic spent three months trying different combinations of tissue and condition frequencies on A and B channels in different patients on different days until we found that we achieved the best responses with the condition on channel A and the tissue on channel B.
The results became more consistent but patients still needed ten or fifteen treatments before the improvements became permanent. How could we get faster, more long lasting results? One of the interns went to the rare book room at the National College of Naturopathic Medicine (NCNM) and looked up frequencies in Electromedical Digest. This journal was published from 1920 to 1951 and had articles by physicians who treated patients with electromagnetic therapies. One of the interns, Ryan Wilson, found a list of frequencies used by Albert Abrams in his San Francisco clinic in the back of a 1927 issue of the magazine.
Albert Abrams was a controversial figure in his day but attracted the attention and support of the famous muckraking writer Upton Sinclair. Sinclair went to San Francisco in 1922 intending to write about Abrams and expose him as a fraud and a quack. What he saw in Abram’s clinic caused him to write an article for Pearson’s magazine titled “House of Wonders”. He saw Abrams diagnose and successfully treat pain and lethal conditions of the day such as tuberculosis, cancer, pneumonia, and influenza. Abrams founded the Electromedical Society and Electromedical Digest and funded them until his death in 1937. When we added Abrams’ frequencies for tissue fibrosis at the beginning of the myofascial trigger point treatments, our outcomes improved and patients began to recover more quickly.
Why use graphite gloves?
Wanting to find out if the way the current was applied made a difference, we tried adhesive electrode pads such as those used on TENS devices and we tried the graphite conducting gloves that came with the facial microcurrent machine to connect the leads from the machine to the patient. The two red, or positive current, leads were plugged into the jacks on the back of one of the graphite gloves and the two black, or negative current, leads were plugged into the jacks on the back of the other graphite glove. The practitioner wore latex gloves inside the graphite gloves to prevent the current from going through the doctor instead of the patient.
The graphite gloves consistently produced a better response than the adhesive electrode pads for reasons that are still not clear. There is a theory but there is not an easy way to test it so it will remain a theory. The graphite gloves are effectively cylinders of conductive material that allow the electrons in the current to flow around them before going into the patient. Physics tells us that moving electrons create a magnetic field that is perpendicular to their path. When the current flows through the gloves the electron path is circular and the magnetic field created has to be passing through the patient. Adhesive electrodes create a point of current entry on a flat surface and do not create a circular path. It seems likely that the magnetic field from the circular path creates the enhanced effect seen with the graphite gloves but not everyone agrees with this theory.
The first FSM course
By October of 1996, it was apparent that this treatment technique was extremely promising. But was it real? Could the results be reproduced or was there some complex placebo effect operating in our clinic that had not been discovered? In a fee-for-service clinic you cannot ethically conduct the double-blind placebo-controlled studies that are the medical gold standard for proving efficacy of a treatment. Patients and insurance companies pay for treatment, not research, and there wasn’t enough clinical data to attempt university collaboration or grant funding for a controlled research trial even if we had known how to apply for one.
The most obvious way to tell if the treatment was reproducible was to teach it and see if people new to the technique could achieve the same results. There were some hurdles before we could teach the technique and make equipment available. The graphite gloves were only available to the purchasers of the $7000 facial toning machine sold by Bio-Therapeutics. David Suzuki, president of Bio-Therapeutics and Microcurrent Technologies finally relented in the face of impassioned pleading and agreed to sell the graphite gloves to practitioners who took the FSM course.
A logo and a name for this new technique had to be created so the flyers to advertise the course would look professional. On a Friday night in November, Ryan Wilson and Kristi Hawks joined me for a brainstorming session at a local pub at the end of a long and busy week. With the noisy Friday night happy hour crowd chattering in the background, Frequency-specific Microcurrent emerged from the long list of crossed off names on the pad as the simplest and most descriptive. As the three of us talked, Ryan doodled on napkins with a felt tipped pen. Variations on a theme were tried and discarded until the current form of the Frequency-specific Microcurrent logo took shape and was voted in. A grateful patient who owned a sign shop took the napkin and turned it into a graphics file and “FSM” had a name and a face.

Figure 1.4 • The FSM logo was devised in felt pen on the back of a napkin in a local pub on a Friday night in November of 1996. A patient with a graphics business turned it into the FSM logo used today.
The first FSM seminar was scheduled in mid-January 1997 at NCNM, the Portland Naturopathic College. We sent out flyers to licensed chiropractors, naturopaths and naturopathic students in Oregon. Twenty-five students attended the first one-day course. The syllabus totaled 17 typed pages. Part of that syllabus presented the early microcurrent applications promoted by Dr. Thomas Wing when he introduced microcurrent to the US in the 1970s. The most commonly used frequencies were .3Hz, for increasing healing, .6Hz for stimulation of acupuncture points, 30Hz for pain control, and 300Hz for reducing edema and stimulating lymphatic flow. Dr. Wing’s protocols were all included in the first syllabus.
The flyers, syllabus and frequency summary sheet were created on the clinic computer at night after patients had gone home and the flyers were folded, sealed and stamped at home on the kitchen table. The copy shop printed the ten page syllabus the day before the seminar and the summary sheet was two short columns on one side a sheet of paper. The first class was taught on a chalk board and included demonstrations, a practice session and a very nervous instructor. Dr. Douglas purchased a fruit platter at a local grocery store for the snack breaks, and brought an electric tea kettle, paper cups and tea bags from home for warm drinks. We made it up as we went along and somehow got through the day. A few attendees caught the bug and contacted the local distributor for Precision Microcurrent to purchase a machine and began using the technique. By June of 1997 the answer to our question appeared in the form of practitioners reporting successful, reproducible results. The frequency-specific response was real.
Teaching the seminars
FSM was first taught to discover whether it was reproducible. The classes continued because it would have been immoral to stop teaching them. So many pain patients were helped with FSM in the clinic that it seemed important to train other practitioners so they could pass along this relief to many more pain patients. The seminars became easier and attracted more students when we gained approval for continuing education credit in Oregon for chiropractors and naturopaths later in 1997.
The two-day seminars were presented as a low key home grown event four times a year in Portland at the National College of Naturopathic Medicine until 2000. NCNM resides in a grand 1900s vintage brick building tucked away on a side street in central Portland. Sometimes the boiler didn’t work in the winter and we wore coats and gloves in the frigid lecture room, sometimes the guard would forget to open the building on Saturday morning and the group would stand in the rain for 30 minutes awaiting his arrival. But the room rental price was right, the staff was friendly and supportive and the school setting was familiar and comforting. The syllabus grew to 40 typed pages, the summary sheet increased to two columns of frequencies and protocols on both sides of a sheet of paper; Dr. Wing’s material was deleted and only FSM treatment protocols were presented.
The practice became overwhelmingly busy with more and more difficult patients referred from chiropractic, medical and naturopathic physicians all over Oregon. Every patient we helped seemed to know six people like themselves and they sent their friends and family in droves. It was the perfect learning environment and a wonderful, if hectic, place to practice and gather experience. Interns, assistants and associates came and went. In 1997, Kristi Hawks, now Dr. Kristi Hughes, moved back home to Minnesota to set up practice and eventually became a captivating teacher and lecturer and one of the busiest most knowledgeable naturopathic physicians in the country.
The first collected case report presentation
In February 1997, a Chiropractor who belonged to the American Back Society (ABS) heard me talking about FSM at a medical meeting and suggested that our results would be perfect for a workshop presentation at the ABS national meeting in San Francisco in December 1997. FSM outcomes in the treatment of myofascial trigger points were collected for the year and the following is an excerpt from the resulting paper.
Results in clinical practice – 1996
250 new patients were treated in 1996 and the results in 137 cases of “simple” chronic myofascial pain in various body regions uncomplicated by disc injury, neuropathy, or severe arthridities, most due to prior trauma or chronic overuse were examined. Symptom duration ranged from 8 months to 22 years. The majority of patients had been treated by one or more prior therapies including prescription drugs, physical therapy, surgery, chiropractic, acupuncture, trigger point therapy and massage. Of those 137 patients, 128 completed treatment. Pain was reduced in 126 of those 128 from an average 5–8/10 to a 0–2/10. Two patients had pain reduced from the 5–8/10 range to 3–4/10 range. Treatment duration varied between 6 and 60 visits depending on the severity, complexity and chronicity of the case. Patients were told to return if the pain reoccurred or motion became limited. Only six patients have returned for occasional follow-up treatments. The results seem to be long lasting and possibly permanent. No follow-up questionnaires were sent so the exact long-term results cannot be documented.
Results in clinical practice – 1997
Further refinements in treatment techniques and frequencies resulted in improved patient response and reduced the number of treatments required. Data was retrieved from the charts of 100 new patients seen between January and June of 1997 and the results are quite encouraging. There were 50 patients with head, neck or face pain resulting from chronic myofascial complaints. There were five acute cervical and 21 with chronic low back complaints. The rest were shoulder, other extremity or thoracic pain. Most of the patients were referred to the clinic by a medical physician, chiropractor, naturopathic physician or another patient. We defined chronic as pain lasting longer than 90 days after the precipitating trauma.
The outcomes were described as simple averages. The average chronicity was 4.7 years in head, neck and face pain and after 11.2 treatments over a 7.9 weeks treatment period the average pain levels decreased from a 6.8/10 to 1.5/10. There was no control group but the patients in some sense served as their own control since 88% (44/50) had failed with some other therapy. Seventy-five percent of patients (33/44) had failed with medical care, 54% (24/44) had failed with chiropractic, 38% (17/44) had failed with physical therapy, 11% (5/44) with naturopathic care, and 6% (3/44) with acupuncture. Many patients had used two or more of these therapies with minimal to no permanent relief.
The outcomes were better in low back pain than in neck pain group even though the low back pain was more chronic at 8.4 years versus 4.7 years in the neck pain group. Patients with myofascial trigger points in the low back muscles were treated an average of 5.9 times in 6 weeks and the average pain was reduced from 6.8/10 to 1.6/10.
In general, patients were treated twice a week with FSM, manipulation and massage. As they improved, their treatments were reduced to once a week, then once every two weeks. Half the neck pain patients took 10 or more treatments to obtain maximum improvement. It took two years to learn that cervical patient recovery took 11 treatments in 8 weeks compared to the low back patient’s 6 treatments in 6 weeks because their myofascial pain was complicated by or perpetuated by nerve irritation, disc and facet joint injuries and ligamentous laxity from trauma or degeneration. The low back patients all had simple myofascial pain due to trigger points with no complicating factors.
This was the next lesson in the specificity of response. Trigger points perpetuated by nerves, discs, facets and ligaments do not respond to the treatments for trigger points directed solely at the muscle. When the treatment protocols for nerves, discs, facets and ligaments were developed two years later and used with an accurate assessment and diagnosis, patient recovery became more efficient and consistent.
At the American Back Society national meeting in December 1997, 450 people attended a plenary lecture in the morning by an orthopedic surgeon who stated that myofascial pain from trigger points must be the result of emotional conversion since these patients never improved. The speaker was polite and curious and asked for a copy of the paper when he was told that myofascial pain and trigger points were treated easily and effectively with this new method. In general, FSM and the clinical outcomes were well received by clinicians and skeptically assessed by researchers and this first exposure to the world of medical meetings turned out to be a good education.
FSM goes public
Shortly after the American Back Society meeting, there was a call for papers in the area of head, neck and face pain from a peer reviewed journal called “Topics in Clinical Chiropractic” (TICC) which accepted case reports. I decided to write up the cervical cases that had been presented at the American Back Society meeting and submit them to this journal. The paper was accepted and in August 1998 FSM had its first publication (McMakin 1998).
In July of 1998, I was correcting the galley proofs of the TICC paper while sitting in the back row listening to a lecture by Jeff Bland, PhD. Dr. Bland gave seminars all over the US presenting the biochemical and physiologic mediators of health and illness and a new concept he called “Functional Medicine”. He was one of my favorite speakers and his annual hour-long lectures were a must. When he saw the galley proofs of the article he asked for a reprint when it was published.
When he received the reprint Jeff called and asked if I would agree to be interviewed as a “Clinician of the Month” for his tape series called “Functional Medicine Update” that went out to over 5000 subscribers in the US and around the world. The interview was taped in February of 1999 and distributed in April 1999. Jeff Bland and that interview started a process that would change FSM forever.
There were 400 calls to the clinic requesting information and the FSM seminar, now two days long but still written on a chalk board, began attracting medical physicians and chiropractors from all over the United States. Shirley Hartman MD, a general practitioner and acupuncturist, flew from Florida to Portland to take the seminar and was the first one ever or since to have all of the frequencies memorized by Sunday afternoon. She loved the seminar but spent $85 in cab fare being lost and trying to find NCNM in its obscure location in downtown Portland. After that, the seminars moved to a small hotel near the airport for the next five years. Dana Pletcher a chiropractor from Chicago and Catherine Willner, MD a neurologist from Durango, Colorado heard the functional medicine update interview and took the seminar in the early years. Dr. Pletcher sponsored the FSM seminar in Chicago and Dr. Hartman brought FSM to Jacksonville Florida for the next four years. Dr. Willner ended up pioneering FSM treatments for the nervous system, lectures on FSM and the nervous system at the FSM Advanced course and has become an ardent supporter and friend.
New discoveries – treating nerve pain
In 1996 and 1997 the treatments for myofascial pain and trigger points were developed. In 1998 we discovered nerve pain could be treated. A patient came in with arm pain that was clearly from nerve irritation instead of trigger points and said, “For goodness sake, think of something and try something, anything to get rid of this.” It was a matter of thinking it through. There was a frequency to remove inflammation and a frequency from Van Gelder’s list of tissues for the nerve. It seemed reasonable that nerve pain would come from inflammation in the nerve. Using the basic technique of removing “pathology” from a tissue, we used 40Hz on channel A to remove inflammation and 390Hz on channel B to direct the effect to the nerve as a tissue. In 1998 the Precision Microcurrent could only deliver frequencies accurate to two places. It had two digits and a three place multiplier of .1, 1 and 10. So if the two digit switch was set at 39 and the multiplier was set at 10 the frequency delivered was 390Hz. The frequency for the nerve from Van Gelder’s list was 396Hz – 390Hz was as close as we could get and it seemed to work fairly well.
The DC current is delivered as a ramped square wave pulse that can be alternating or polarized positive or negative. In his book, The Body Electric, Robert Becker (1985) described the human body as having a natural polarity more positive at the top and negative at the feet, more positive in the middle and negative at the ends of the hands and feet. In physical therapy classes at the Chiropractic College, they taught us that positive polarized current sedates nerves and causes vasoconstriction. It seemed reasonable to sedate painful nerves and to follow the normal polarization of the body by using a positive polarized current.
The glove with the two positive red colored leads was placed at the neck and the glove with the negative black colored leads was placed at the hand for nerve pain in the arm, with the current polarized positive. The patient’s pain dropped from 7 out of 10 to a zero in 30 minutes and the patient went home pain free and acting as if she was a little “stoned”. Unlike treatments for muscles, treating the nerve created an induced euphoria that became as predictable as it was profound. The response to the first nerve pain treatment was even more amazing and unexpected than the response to the first myofascial treatment since nerve pain is otherwise very difficult or impossible to treat.
But there were no laurels to rest on; nerve pain did not stay gone like myofascial trigger points. It came back, especially if the patient lifted anything or spent time with the neck or the low back flexed forward. Once the pain could be eliminated, the bar was raised to see if the relief could be made permanent. This meant that the team had to learn how to rehabilitate the discs in the neck and low back that were causing the nerve inflammation.
There were frequencies for the discs so we began treating the discs with FSM and found that disc pain and nerve pain resolved more quickly when both tissues were treated. Often, patients with disc and nerve pain in the neck or low back also had local low back or neck pain that was coming from the posterior joints in the spine called facet joints. The facet joint symptoms improved only when the frequencies to remove inflammation and scar tissue from the joint tissues were used in treatments. The patients were wonderful teachers. One day when his facet joints were being treated a patient said, “It feels as if the pain is in the bone!” When the frequencies to reduce inflammation in the bone and its outer covering, the periosteum, were added to the treatment his back pain went away. This discovery began the next steep learning curve.
Improving clinical skills
Because the treatments were so specific, the diagnosis had to be correct for the treatment to be effective. We discovered over time that if the treatment was effective the diagnosis was correct. If the treatment was ineffective the diagnosis was refined and a new treatment was designed based on the new assessment. Sometimes an effective treatment for one problem led to the resolution of that problem only to reveal a different underlying problem that had been hidden by the first.
For example, a patient injured three years previously in an auto accident would present with neck and midscapular, shoulder and arm pain. When treatment resolved the myofascial trigger points and softened the tight painful neck muscles, neck range of motion increased and arm pain improved but then the local neck pain and midscapular pain became much worse. After numerous repetitions of this pattern, we eventually discovered that an x-ray taken from the side with the neck flexed forward and then extended back revealed the problem. The flexion–extension x-ray showed that the ligaments holding the vertebra together had been stretched and injured in the accident. The lax ligaments at C5–6 which had been splinted by the tight muscles were now unsupported because the muscles were relaxed and the upper of the two vertebra was sliding forward on the lower one each time the patient flexed the neck forward. The increased movement at the segment was irritating the facet joints in the posterior spine, creating inflammation in the disc and in the ligaments and resulting in increased pain in the neck and midscapular area. Each case was unique and challenging but the clinical training in differential diagnosis was invaluable.
The clinic developed a reputation for treating chronic pain of all types and treated more and more difficult, chronic and complicated pain patients every year from 1998 until the clinic closed in 2007. Most but not all patients recovered as we searched to find the combination of approaches that make the difference between success and failure.
Discovering the treatment team
We found that a team approach to treatment was the key. Successful disc rehabilitation in the neck, thoracic spine and low back depended on reduction of inflammation, reduction of nerve pain and enhanced tissue repair from FSM. But exercise rehabilitation to strengthen and stabilize the spine was crucial to create lasting results – the problem was finding a physical therapist that understood complicated patients and would not make them worse with heavy weights or inappropriate therapies. A chance conversation in a beachside pizza parlor led to the discovery of the second member of the team. The Ola Grimsby Institute (OGI) trained physical therapists specializing in spinal stabilization at New Heights Physical Therapy clinic and created appropriate exercises with light weights on pulleys individualized for each patient to strengthen the muscles, improve circulation at the spine, and correct poor biomechanics and posture.
The third member of the team appeared when we found Dr. Roy Slack, a physiatrist or physical medicine physician, who specialized in spinal injections. He was well trained, compassionate and exquisitely skilled. He used light anesthesia and was sensitive to the patient’s comfort during the procedure. There were times when an injection of steroids and Marcaine into a facet joint or the epidural space near an injured disc was the only way to make a dramatic reduction in inflammation and allow the patient to tolerate exercises at the PT clinic and benefit from the FSM therapies for nerve and muscle at our clinic. The team was in place and results continued to improve.
None of this should suggest that every patient recovered completely. Quite the contrary, as the patients and their problems became more and more complex the percentage permanently “cured” seemed to decline. The physical, emotional and financial hurdles to be overcome were often insurmountable and many patients left treatment still in pain. But most patients left with some improvement and all had a better understanding of their condition.
Discovering the treatment for fibromyalgia from spine trauma
In 1999, Advanced Pain Management Group (APMG), Portland’s only multidisciplinary medical pain management clinic, decided to include a chiropractor and FSM. At APMG between March and December of 1999 the patients who required prescribed narcotics, injections, spinal morphine pumps or spinal electrical stimulators and who had pain problems that were orders of magnitude more difficult to treat than patients seen by the average chiropractor provided the beginning of the next leap on the learning curve.
In April 1999, an APMG patient presented with severe full body pain following a series of physical traumas in the preceding seven years. She had pain in the neck, arms, and hands, mid back, low back, legs and feet that she rated as a 7–8/10. She did not tolerate narcotics for various reasons and was sent for FSM as a last resort.
All of the muscles in her neck and upper back were taut and exquisitely tender to touch – even light touch would make her flinch and break into a sweat. It could not be the muscles, discs or facet joints. After treating those conditions for three years it was obvious that they were not capable of creating such intense widespread pain and muscle tension. The only tissue that could possibly cause such widespread neck to foot pain was the spinal cord and it seemed likely that the pathology creating the spinal cord irritation would be inflammation. Since we had a frequency from Van Gelder’s list for the spinal cord (10Hz) and a frequency to reduce inflammation (40Hz) there was a way to test the hypothesis with a treatment. Robert Becker’s description of the body’s polarity dictated that the positive leads be placed at her neck, the negative leads at her feet and the current be polarized positive.

Figure 1.5 • The first patients treated with the fibromyalgia protocol had one graphite glove wrapped in a wet towel around the neck and another towel wrapped in a wet glove around the feet. Clinic associate, Sonja Pettersen, ND helped with the seminars and modeled for this photograph.
The response was immediate and surprising. The patient began to relax and the neck and back muscles gradually softened. The pain began to recede first in the feet and legs and then the back and neck and finally the arms were pain free. In 30 minutes the induced euphoria response we had come to expect with nerve pain treatment was more profound than any ever seen. The patient stopped talking, closed her eyes and began to breathe more slowly and deeply. She could be roused but would not talk willingly. At the end of 90 minutes she was completely pain free. What had happened, how it worked and how long it would last were all mysteries. As it turned out, her pain stayed down from a 7/10 to a 3–5/10 for three days after each treatment and then gradually returned. The patient lived three hours drive from the clinic and came in to be treated three times. She had to borrow money to pay for the gasoline to get to Portland from the coast for the third treatment. It was her final treatment and we both knew the relief was not likely to last. She brushed off my apology and said she was content because her pain would be down for her daughter’s birthday party the next day.
Over the next few months there were ten patients with similar pain patterns and similar history of trauma who had the same response to the same treatment. The pain would be gone in 60 to 90 minutes, the patient would get so stoned that she could not talk and the pain would come back within one to two days. Dr. Eric Long, well known for his skill in doing nerve conduction studies, differential diagnosis and treatment of chronic pain, referred a patient because he heard that “something different” was being done for pain patients. Her case was particularly challenging and her stoicism and courage in the face of intractable pain was inspiring. She was treated with the new protocol and at the end of an hour she was pain free, peaceful and looked years younger. She was grateful for the temporary relief and was told that we were working on finding a way to create more permanent improvement.
We had no idea how the spinal cord influenced full body pain and no idea how we were influencing it with frequencies and current. More important, after the experience with medical skeptics at the American Back Society meeting, it was clear that no one would believe the results unless we had objective data to prove that something measurable was changing. Dr. Long was glad that his patient had been helped but said that nerve conduction testing was much too imprecise to document such changes and he had absolutely no idea of how to document what had happened. The excitement about the successful treatment was matched only by the frustration of having no idea what exactly was happening, how it worked or how to make it permanent.
By the end of 1999, 25 patients with this pain pattern and history had been treated. The diagnosis was “fibromyalgia” associated with some sort of physical trauma affecting the spine. Patients were told that the trauma had injured a disc in the neck and created inflammation in the spinal cord and that the inflammation was amplifying the impulses coming up pain pathways in the spinal cord from the arms and legs. The pain level was usually high, rated by the patient as being between a 5 and 9/10 even if the patient was on narcotics. The patients, mostly female, had a history of auto accidents or falls, surgeries that involved intubation for general anesthesia or lifting injuries. The pain diagrams began to look familiar. There were always x’s or circles at the front and back of the neck, points of the shoulders, arms, elbows, hands, midscapular area, back, low back, legs and feet. A patient whose fibromyalgia did not begin with some sort of trauma never complained of pain in the hands or feet.
The physical examination findings were always similar. The knee reflexes were always hyperactive, indicating a significant degree of irritation in the spinal cord. (Normal knee or patellar tendon reflexes are normal because descending inhibitory impulses from the brain come down to the L3 nerve root in the spine in time to dampen the reflex arc. If the conduction of descending inhibitory nerve impulses in the spinal cord is reduced due to inflammation in the spinal cord the reflex has enough time to become hyperactive but not enough time for clonus to develop as happens in upper motor neuron injuries.) Patients whose fibromyalgia did not begin with some trauma had normal or even reduced patellar reflexes. There was always hypersensitivity at specific nerve roots, usually in nerves coming from the neck. Only patients whose fibromyalgia started with trauma had these findings and only these patients responded to the 40Hz and 10Hz frequencies applied with polarized positive current from neck to feet treatment protocol. The key to successful treatment was once again accurate diagnosis.
Understanding the CTF treatment – developing the model
In June of 1999, I met an old friend at a medical meeting in Canada who had moved from Portland to England to teach at Anglo European Chiropractic College (AECC) in Bournemouth. He was very pleased to hear about the positive results with this very difficult group of pain patients and asked that the outcomes and model be presented in March 2000 at the joint spring conference of Anglo European Chiropractic College and the British Chiropractic Association whose topic was “Cervical Trauma and Chronic Pain”. The paper, due in January, had to answer the questions: How would a disc injury create amplification of the pain impulses going up the spinal cord from the hands and feet? What happened to discs when they were injured but not herniated? What effect do injured discs have on the nerve and the spinal cord? Why do they have hyperactive reflexes? Why doesn’t it heal?
In December, a colleague who knew about the AECC presentation sent me a reprint of Taylor & Twomey’s (1993) article documenting damage to the spine found on autopsy in patients killed in auto accidents from non spine trauma. One of the requirements for inclusion in the study was an x-ray and an MRI read as “normal”. Upon autopsy, the patients were found to have cracks in the vertebral end plates, fractures between the end plate and the disc, tears in the disc annulus, and small bulges that allowed the disc nucleus to contact the end plate or the damaged disc annulus none of which appeared on spinal imaging. She followed this up by sending two papers each from Olmarker (1993, 1995) and Ozaktay (1995, 1998) showing that the nucleus pulposus of the disc is not only inflammatory but neurotoxic. The nucleus pulposus material did not amplify pain impulses in the spinal cord or nerves; it stopped them. The original model was wrong.
If impulses in the spinal cord pain pathways were slowed or stopped what would happen to pain signals? Principles of Neural Science by Kandel & Schwartz (1985) would have the answer in the section on pain processing. The text opened to the paragraph that explained what we were seeing. “Central pain can arise not only from pathologic lesions in the thalamus but also from lesions placed anywhere along the nociceptive pathway from the spinal cord and brain stem to the thalamus.”
The next paragraph listed pain descriptors used by patients to describe central pain and they were exactly word for word the descriptors used by cervical trauma fibromyalgia patients to describe their pain. Burning, aching, stinging, stabbing, sharp, dull were all circled on the intake forms the fibromyalgia patients filled out in the office. No other patients circled all of the pain descriptors. The text commented that central pain was particularly bothersome emotionally and this matched the distress unique to this patient group. The disc injuries were damaging the pain pathways in the spinal cord and causing central pain. The questions were answered, the model fell into place and the paper was ready to present at the AECC meeting.
Speaking at NIH – presenting the model
The next week Dr. Jay Shah, a physiatrist working at The National Institutes of Health (NIH), called because he was in charge of recruiting speakers for Grand Rounds presentations at NIH and needed a speaker to replace someone who had canceled at the last minute. He asked if I was interested in presenting the data and the model for treating fibromyalgia from cervical trauma at a Grand Rounds presentation in April 2000. Dr. Shah is one of the world’s experts in myofascial trigger points and he took the FSM seminar in 1999 to see if it could be effective for his patients. During that seminar he heard about the results being produced in fibromyalgia patients and wanted to expose his colleagues at NIH to this new therapy. The answer was an enthusiastic but slightly intimidated, “Yes!” The next few weeks were a whirlwind of seeing patients during the week and learning how to make Power Point slides on the weekends.
Two weeks later Dr. Jeffrey Bland called and asked for a presentation on the topic “Energy Medicine in Clinical Practice” to be presented at the Institute for Functional Medicine International Symposium to be held in May of 2000. That talk would once again present the frequency-specific response and our outcomes in the treatment of cervical trauma induced fibromyalgia and the concept that one specific frequency combination had specific effects in treatment.
The AECC presentation went well. The next month Dr. Shah helped fine tune the presentation for the much more sophisticated and demanding audience of physicians at NIH. At the end of the NIH lecture, the assembled audience of thirty physicians and PhDs were asked to help find something that could be measured to document objectively what was changing besides pain as we treated this group of patients. Terry Phillips, a PhD immunochemist recently recruited from George Washington University to bring his expertise in micro immunochemistry to the NIH, came up after the lecture and said that if he had spots of the patient’s blood on pieces of blotter paper taken at different times during the treatment he could tell me what was changing. He sent the blotter paper in the mail and when it arrived, the ideal patient was called.
The volunteer and the cytokine data
MK was a delightful young woman who had been treated unsuccessfully in the clinic for widespread myofascial pain, neck and arm pain for four months in 1998. She eventually had neck surgery in 1999 to fuse two herniated discs that were the source of the trouble but told us that her pain had generalized to the full body and became worse after the surgery. When she answered the phone she said yes her hands and feet did hurt and wondered why we wanted to know. Delighted but skeptical when she was told that there was a new treatment that might help her she said she would be happy to donate five drops of blood to help us find out what was happening during the treatment.
The session started with a physical examination. She had hyperactive patellar reflexes and the cervical nerve roots were hypersensitive to sharp stimulation. Her pain was a 7–8/10 and she had stopped taking narcotics because they did not help the pain. She had the 11 out of 18 tender points tender to less than 4 lbs/in2 pressure, full body pain and disturbed sleep that are diagnostic for fibromyalgia. A finger stick from a diabetes blood tester gave us the blood spot for the first small strip of blotter paper. The microcurrent machine was set to deliver 40Hz on channel A and 10Hz on channel B, the graphite gloves were placed at her neck and feet with the current polarized positive and the treatment began. In a few minutes her neck muscles started to relax and soften, the pain started decreasing in her feet and legs and we knew the treatment would be effective.
After 30 minutes of treatment she opened her eyes sleepily and asked incredulously, “Is this legal?” The euphoric effect is something like that produced by morphine or Versed and very profound on the first treatment. Her pain was down to a 4/10 after 40 minutes and dropping fast. We took blood samples every 30 minutes. When her pain was down to 0/10, the frequency was changed to the frequency combinations that Van Gelder used to reduce “nervous tension”, “emotional tension” and “concussion” for 20 minutes. The last blood sample was taken and MK went home pain free for the first time in four years. The paper strips dried overnight, went into a plastic container and were mailed to Terry Phillips at NIH the next day.
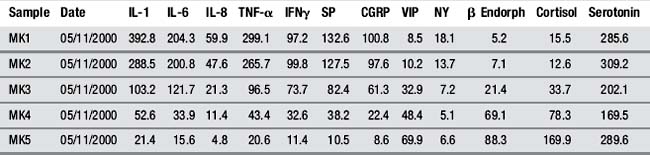
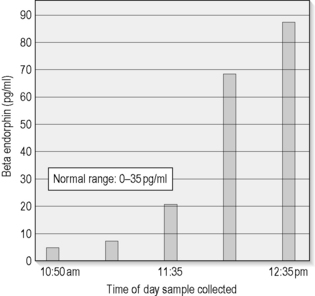
The busy weeks at the clinic flew by and the IFM Symposium was two days away when the fax machine started clattering and out slipped a page with columns of data listing the substances from each blood spot taken during the treatment. There were substances called IL-1 (Interleukin-1), IL-6, IL-8, TNF-α, CGRP (calcitonin gene related peptide), which were all inflammatory peptides called cytokines, and substance-P, endorphins, cortisol, and serotonin.
Dr. Phillips and his miraculous testing equipment had discovered in great and minute detail what was changing. The numbers, measured in nano and pico liters, changed dramatically by factors of 10–20 times between the first and last readings. The function of most of the peptides was a mystery but it was apparent that such dramatic changes had to be significant. Every pain specialist knows that substance-P is produced in the spinal cord and that the huge changes in substance-P could only mean that the treatment did indeed affect spinal cord function. The dramatic reductions in the inflammatory cytokines had to mean that the treatment reduced inflammation, and the huge increases in endorphins had to be the explanation for the induced euphoria. The treatment success was no longer subjective changes in pain scores. Objective data showed that something very real was changing (McMakin 2004).
Presenting the cytokine data
Dr. Bland greeted us as we arrived at the Phoenix resort where the meeting was being held. He took the offered data sheets and when his hand started to tremble, it was clear the numbers were as good as they appeared. He said, “This is going to knock their socks off.”
The 2:00pm workshop lecture “Energy Medicine in Clinical Practice” the next day had to be moved twice to accommodate new registrants and the audience of more than 200 people filled every chair, sat on the floor and stood along the sides and the back of the room. The lecture was timed to the minute but there was time to include the new data slides at the end. The room was totally silent as the bar graphs showed inflammation and substance-P plummeting and endorphins rising by factors of 10–20 times. The physicians in the audience knew better than the speaker that these rates of change had never been seen before and were not possible to create by any other known method of treatment.
The last sample taken after the pain was zero showed every parameter continuing to move in exactly the same direction except for serotonin. Serotonin dropped during the treatment that reduced the pain and when the frequency was changed to the combinations used to reduce nervous tension, emotional tension and concussion, serotonin turned around and doubled itself in 20 minutes. This was energy medicine in practice and the audience sat in stunned silence until they burst into applause.
The Australia connection
Mike Curley, the director of HealthWorld, a nutritional supplement distributor in Australia, was sitting in the back of that workshop room listening to the lecture. He decided to bring FSM to his practitioners in Australia. We made the arrangements and scheduled the first Australian FSM seminar for September 19, 2001. Mike promoted the seminar by flying all over Australia during the spring and summer (Australia’s fall and winter) of 2001 promoting the course and recruiting a very large and enthusiastic group. September 11, 2001 closed US airports, changed the face of international air travel and postponed the seminar into October.
The first course, held in Sydney was presented on a white board projected to a large video screen in a huge hotel ballroom to 60 medical physicians, chiropractors and naturopathic doctors. Considering that the US course had never had a class larger than 25, teaching a group this size was a challenge. The practicum sessions were barely controlled chaos with a group this size and the Australian students proved to be exuberant and intense learners. The yearly five-day Australian seminars continued with large and enthusiastic groups each year until 2007 when Mike retired. The Australian connection led to the next big leap in FSM development.
FSM animal research
In 2002 Wayne Reilly, a research associate with HealthWorld, arranged for an experiment to be done at University of Sydney by his friend and colleague, Dr. Vivienne Reeve. Dr. Reeve studies drugs and processes that reduce inflammation in a mouse model and together they designed a study that would test the effect of frequencies to reduce inflammation. The process is simple. The researchers paint arachidonic acid on the mouse’s ears, which creates inflammation at a predictable rate and then measure the swelling with a caliper in millimeters. They administer some drug before or after the exposure and see if it reduces the swelling compared to an untreated control group.

Figure 1.7 • Reduction in Cytokine IL-1. Interleukin 1 was reduced from 392.8 pg/ml to 21.4 pg/ml in 90 minutes in a peripheral blood sample. The normal range is 0-25 pg/ml. Cytokines are known to be difficult to change and change only slowly, when they change at all, making this data even more remarkable. The reduction in cytokines correlated to the reduction in pain.
Dr. Reilly chose the frequencies to be tested in the experiment. When the first batch of ten mice was treated with 40Hz on channel A and 116Hz on channel B to “reduce inflammation in the immune system” the swelling went down by 70% in four minutes in every animal treated. Dr. Reeve stopped the study because in 18 years of research on anti-inflammatory drugs she had never seen any prescription or non-prescription drug that reduced swelling by more than 45%. She “blinded” everyone in the lab by moving each process into a separate room and not allowing anyone working on any part of the study to know whether the mouse being treated was in the active treatment group or the sham group. She turned the machine around so that the person treating the mice didn’t know if it was running and she put a sham frequency in the protocol. The treated mice still had a 62% reduction in swelling compared to the untreated and the sham groups. And it was a four minute time-dependent response. Half of the effect is present at two minutes, the full effect is present at four minutes and every one of the 20 animals treated responded (Reilly 2004).
They tested three different frequency combinations from the FSM list. No other frequency combination reduced inflammation at all. They were each equivalent to placebo.

Figure 1.8 • Wayne Reilly held each mouse for four minutes as they were being treated. Notice that the gloves contact the mouse where it is being held on the back and at the tail and not on the ears where the reduction in swelling was measured.
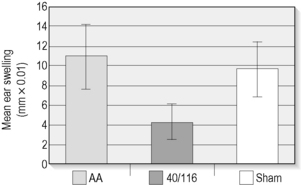
Figure 1.9 • Arachidonic acid was painted on the ears of hairless mice. 40Hz/116Hz reduced by an average of 62% in four minutes in every animal tested and the sham frequency shown on the far right had no effect on swelling.
Then they exposed the hairless mice to a measured dose of ultraviolet light, just enough to create a mild sunburn, make the ears swell and create immune system suppression. One half of the mice were treated immediately after the sunburn with 40Hz and 116Hz and the other group was treated two hours after the exposure. The group treated immediately had no decrease in swelling but the group treated at two hours had a small (0.01) but significant decrease in swelling.
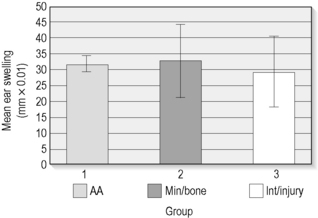
Figure 1.10 • The researchers tested three different frequency combinations including the frequency to “remove minerals” in “bone” and a group of three frequencies for injury and none of them had any effect in reducing inflammation. They were equivalent to placebo.
Before the sunburn the mice were painted on a hind leg with a substance, called oxazolone, which they would be allergic to on the second exposure if the immune system was operating normally. Sunburn suppresses the immune system so mice that have been sunburned do not swell as much as normal mice when their ears are painted with oxazolone two weeks after the first exposure.
The results of the FSM study were fascinating. The untreated mice had ear swelling of 30 units (0.01 x mm) when exposed to oxazolone the second time. The sunburned, untreated mice had the swelling reduced, and the immune system suppressed by 63.4% as expected. The group treated with FSM at two hours, that had the best reduction in swelling, had their immune system suppression reduced slightly from 63.4% to 57.5%. But the group treated immediately after the sunburn, that had no significant reduction in swelling, had their immune system suppression reduced by half from 63.4% to 31.05%.
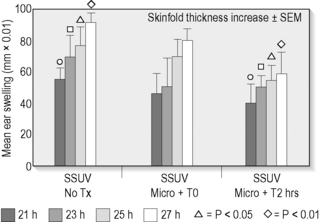
Figure 1.11 • The mice were exposed to UV light creating immune suppression and swelling. The mice treated immediately with microcurrent had no reduction in swelling but the mice treated at two hours had a small but statistically significant reduction in swelling caused by sunburn.
The implications of this portion of the trial were staggering. The application of one frequency combination for four minutes changed an immune system response when measured two weeks after the application of the frequency. The change to the immune system was effectively permanent.
Dr. Reeve is an established, well-published, conservative PhD in a tenured university research position. She wanted to repeat the study with a larger group of mice but would never accept funding for the project. Dr. Reilly presented a brief abstract at a medical conference but the data has never been published.
FSM seminars go national
Throughout 2000, 2001 and 2002 the practice and the US seminars continued to grow. The seminars were now two and a half days long and still presented by writing on a white board with a felt marker in a hotel meeting room in Portland, Chicago or Jacksonville Florida. The syllabus expanded to 60 typed pages and the summary of frequencies and treatment protocols filled two full columns on both sides of a laminated sheet. The conditions treated successfully with FSM continued to grow as the practice increased and the cases accumulated from practitioners around the country.
There was one frequency combination that turned out to be effective for reversing shingles and both oral and genital herpes. The pain disappeared after ten minutes of treatment and 60 minutes of treatment each day for three days would prevent the blisters from appearing if delivered in the painful pre-shingles prodrome. Sixty minutes of treatment would eliminate the pain and clear up the blisters in five days instead of five weeks if treatment started after the blisters appeared. That frequency combination was not useful for any other condition and everyone treated so far with these conditions has responded positively. In 2002, one frequency combination was found to be effective in eliminating kidney stone pain; it did nothing for the stone, it just stopped the pain within minutes in every one of the 25 patients treated that year. Some frequencies treated new injuries and accelerated the healing by three to four times if treatment was administered in the first four hours after injury. Any condition from asthma to irritable bowel syndrome that involved inflammation or scar tissue seemed to respond dramatically.
In 2002 Jeff Katke, the president and CEO of Metagenics, Inc., a large nutriceutical company providing professional grade nutritional supplements to physicians, suggested a collaboration. Metagenics would promote FSM seminars and the FSM seminar would recommend Metagenics supplements to be used to support the changes created with FSM treatment. In fact, this is how treatments were done at the clinic. Those patients with proper nutrition and a stable state to support the changes made by FSM treatment recovered more quickly and had better outcomes than patients who did not have good nutrition or take supplements. It seemed to be a reasonable way to get the FSM information out to more people.
By this time Dr. Kristi Hughes, the naturopathic physician who helped when FSM was being developed, was now a speaker for Metagenics giving lectures around the country about functional medicine approaches to health. Metagenics sponsored nine FSM seminars in 2003 and Dr. Hughes lecture series preceded the FSM seminars by six to eight weeks in most cities. Any time she talked about her results using FSM and nutrition to treat pain patients, people signed up for the FSM seminars in droves.
Travels with Dr. Bland
In addition to his position at the Institute for Functional Medicine, Dr. Jeffrey Bland was also the chief science officer for Metagenics and gave day-long lectures in 18 cities around the country in the spring of each year, describing the biochemistry and science behind nutritional approaches to improve health and prevent disease. The FSM display booth and I joined Dr. Bland on his 18 city tour from January through April. On most Fridays we traveled to the city where he would lecture on Saturday. He lectured from 8:30 to 4:30 and Saturday night we flew on to the next city. He lectured on Sunday and we traveled home either immediately afterward or on Monday morning. Tuesday, Wednesday and Thursday found me back at work at the clinic until we left again on Friday. Jeff was gracious and generous and made my first experience with national seminar travel as painless as possible.
Doctors attending the day’s lecture could be treated at the FSM booth during the breaks as FSM was discussed and demonstrated. One physician had been injured 14 years previously when she rode her bicycle into a 20-foot deep unmarked construction trench on her way home from the hospital one night. She was pacing at the back room and had the facial expression of someone in pain. At the break, I asked about her history and then inquired if her hands and feet hurt. She replied that they did and agreed to sit in the back of the room and be treated. Cloth napkins from the refreshment table combined with warm water from the tea service became makeshift electrodes with the graphite gloves wrapped inside and were wrapped around her neck and feet. The experience gained from treating 25 patients a year for four years made the treatment faster and the relief longer lasting. In 60 minutes this physician was pain free for the first time in 14 years and after a few more treatments the pain was permanently eliminated. She took the FSM seminar in Detroit that year and is a skilled and successful FSM practitioner in Toronto to this day.
The FSM course began to make the transition from typed text to Power Point slides in January 2003. The first FSM seminar was scheduled for mid-February 2003 and somehow 60 pages of text became 742 power point slides in six weeks. The FSM seminars in 2003 were so well attended that the number of practitioners in the US doubled from 150 to 300 in ten months.
New equipment – new possibilities
The Precision Microcurrent had always been a two-digit specific device with two numbers set on the frequency switch and 0.1, 1, and 10 multiplier switch to turn 0.68 into 6.8, 68, and 680. The frequencies came in three digits: for example the frequency for tendon is 191Hz, the frequency for the bursa is 195Hz. With only two digits the treatment could not be specific enough to target important tissues. Glen Smith, the engineer-designer and owner of Precision Microcurrent, responded reluctantly to the request for a three-digit specific machine in 1999 saying he didn’t think it could possibly make a difference. It not only made a difference; it made a huge difference in the patient’s response. After 1999, he made only three-digit specific devices for Frequency-specific Microcurrent practitioners.
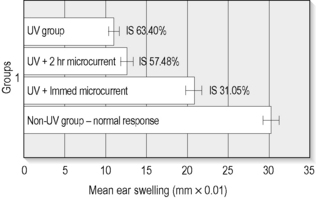
Figure 1.12 • UV exposure to the point of sunburn reduces immune system response. The mice were painted on the hind leg with a sensitizing chemical at the time of UV exposure and painted again on the ear two weeks later. Normal mice who had not been exposed to UV responded two weeks later with 30 units of swelling. The swelling is a normal response. Sunburned mice had their immune system suppressed (IS) by 63.4% from exposure to UV. Mice treated with FSM two hours after the UV exposure had the best reduction in swelling and had immune system suppression reduced from 63.4% to 57.48%. The mice treated immediately with FSM had immune system suppression reduced by half from 63.4% to 31.05%. A single four minute treatment created a change in immune system response lasting two weeks and assumed to be permanent.
There were now enough FSM practitioners and patients that Microcurrent Technologies agreed to develop an automated unit that would run sequences of frequencies in treatment protocols for various conditions. The first “AutoCare” allowed the standard routine protocols to be applied more efficiently in the office. The clinic staff who had been changing frequencies every two minutes on the Precision Microcurrent cheered when the first automated unit arrived. The AutoCare was upgraded in 2004 and again in 2006 to become the AutoCarePlus running 83 automated frequency protocols. The HomeCare, released in 2004 finally made it possible for a fibromyalgia patient to be treated at home under a practitioner’s direction and become pain free at will. The HomeCare unit made recovery from fibromyalgia possible.
Practitioners wanted a HomeCare pocket sized unit they could program from a computer. Microcurrent technologies took the leap and developed the CustomCare in 2007. Patients with the most complex conditions can now maintain treatment and find relief at home with protocols designed for them by the FSM practitioner.
In 2003, athletic trainers came from all over the country for the first FSM Sports seminar in Phoenix in June. Because of their body size, muscle mass and injury profile, athletes require higher current levels and different frequency treatment protocols than the average person. Microcurrent Technologies developed the first SportsCare unit specifically designed for athletes in July of 2003.
Precision Distributing provides the three-digit specific Precision Microcurrent and all of the automated units to practitioners who have attended the FSM Core seminar but any microcurrent device that can deliver one frequency on each of two channels in a ramped square wave pulse can be used for a Frequency-specific Microcurrent treatment. Many students took the course and used their own equipment when they went home to practice.

Figure 1.13 • Three Digit Precision Microcurrent. Glen Smith, the engineer who designed the original Precision Microcurrent, created the first three-digit specific Precision Microcurrent in 1999 convinced that the specificity would not make a difference. The improvement in results made such a difference that soon three-digit machines were used exclusively. Any three digit specific device can be used for treatment.
The Sports Care and the Precision Microcurrent made their NFL debut when Keith Pyne, DC arranged for us to work in the Oakland Raiders training room for the day after our July 2003 San Francisco Core seminar and we treated most of the defensive team including legendary figures such as Bill Romanowski. Buddy Prim, a private trainer for NFL athletes, heard about FSM and brought most of the offensive line from the San Francisco 49er’s to a treatment room set up in an airport hotel on the next day. Reducing inflammation, scar tissue and mineral deposits in men whose job required determined performance and incredible conditioning was a real learning experience. The world of professional sports had discovered FSM.
After FSM made it possible for Terrell Owens, a well known wide receiver for the Philadelphia Eagles, to recover from surgery and heal torn ankle ligaments and a fibular fracture in six weeks instead of the predicted 18 weeks so he could play in the Super Bowl, the word spread throughout the NFL about FSM. The SportsCare, CustomCare, and Precision Microcurrent became training room standards for a few teams and hundreds of players. Through the efforts of skilled athletic trainers like Jeff Spencer, Mike Hatrack, Mark Lindsay and many others, FSM has treated US Postal and Lance Armstrong as they won the Tour de France, helped Tiger Woods recover from knee surgery, and helped Lashinda Demus heal her hamstring injury and win the US National women’s 400 meter hurdles.
The first FSM symposium
The FSM Advanced Course presented new frequencies and advanced treatment concepts every fall since 1999. Students asked for a symposium where FSM outcomes and research could be shared. The 2003 FSM Advanced course was held on Friday afternoon and Saturday morning and the first FSM Symposium was held on Saturday afternoon and all day Sunday in a beautiful ballroom in a downtown Portland hotel. Ninety practitioners attended all four days and it was a joyous celebration.
Jim Oschman, PhD a bio-physicist and author of Energy Medicine; the Scientific Basis (Oschman 2000) was our guest speaker. His task was to explain why the tissue softens so dramatically and why the graphite gloves became warm when the frequency is correct for the patient’s condition. “Why does it get warm; why does it go smoosh?” His explanations mesmerized the attendees and at the end of his lecture he had everyone stand and tone to demonstrate the power of a resonance field.
To complete the demonstration everyone in the room was connected to the microcurrent unit by putting the red leads contact on one side of the aisle and the black leads contact on the other side of the aisle and then having everyone hold hands on each side and across the back to complete the circuit. The frequencies to “restore joy” pulsed through 90 people and the induced euphoria in the room was an experience that everyone still talks about.
The Advanced FSM course and workshops are held every year in February. The symposium is held every two years and includes presentations from practitioners in the US, Ireland and Australia and Dr. Oschman and other speakers still join us every year to try to explain why and how it works.
The low back myofascial pain cases from the American Back Society presentation were published as “Microcurrent Therapy: A novel treatment method for chronic low back myofascial pain” in the Journal of Body Work and Movement Therapies (JBMT) in April 2004. The cytokine data and the cases of successful treatment of fibromyalgia caused by spine trauma were published as “Cytokine changes with microcurrent treatment in fibromyalgia associated with cervical trauma” in JBMT in July 2005. FSM now had three published papers and a track record of incredible case reports. And this is just the beginning.
Crohn’s disease case report
The practitioner case reports at this symposium were an astonishing demonstration of the versatility of the resonance response, the ability of microcurrent to increase the rate of healing and the commitment of the FSM practitioners to patient care and clinical research.
Scott Bergman, DC took his first FSM Core Seminar in Portland in February 2003. The FSM course teaches the frequencies for the digestive system and the frequencies thought to reduce inflammation, chronic inflammation and histamine among others. At the symposium he reported the results of his FSM treatment of a 14-year-old girl with Crohn’s disease. She had a history of being hospitalized with an episode of Crohn’s every spring and every fall for two years in spite of ideal diet, appropriate nutritional support and the best medical care. She was on the path to her first hospitalization of the year when the gastroenterologist told her on Monday morning to collect her school work and be prepared to be hospitalized on Thursday for about one week of the standard treatment for Crohn’s.
Dr. Bergman treated her on Monday afternoon when she and her mom returned from the gastroenterologist looking for some alternative to four days in the ICU. When the treatment started her abdomen was painful and distended, she was nauseous and her appetite was gone. Dr. Bergman combined his knowledge of Crohn’s disease with the tools he gathered from FSM and created a treatment protocol. At the end of one hour’s treatment, her abdomen was non-tender and flat, she was pain free and she was hungry. Each day for four days she was treated. Each day her symptoms were less than they were the day before. And each day when she left, the pain and bloating were gone, her abdomen was non-tender and she was hungry. She never did check into the hospital. She still gets treated once a month, her Crohn’s disease remains in remission and she has never again been in the hospital for Crohn’s.
This and the other case reports at the 2003 symposium were just the beginning of the “miracle stories” that FSM practitioners would document in presentations at every advanced course and symposium.
FSM and the future
At each symposium since 2003 practitioners report on successful treatment of conditions that no one would have thought of treating with frequencies and microcurrent 10 years ago. Incomplete spinal cord injuries, disc herniations and reflex sympathetic dystrophy, Alzheimer’s and Parkinson’s, PTSD (post-traumatic stress disorder), anxiety and obsessive compulsive disorder, sports injuries, post-operative pain and wound healing, skin anti-aging, interstitial cystitis, diabetic neuropathies, uterine fibroids and ovarian cysts and others are presented as cases by practitioners who have treated them successfully.
It has been 12 years now and there are 1200 FSM practitioners in the US, 165 in Australia and 45 in Ireland, 1 in the Netherlands, 1 in Germany, 1 in Spain, 2 in England, 1 in South Africa, and 1 in Hong Kong. The practitioners are an enthusiastic varied interdisciplinary group made up of MDs, DCs, DOs, NDs, NPs, PTs, OTs, LMTs, PhDs, and licensed acupuncturists. The treatment protocols are more refined and more efficient and attending the Core seminar is still like learning a new language in three days.
There are controlled trials planned in medical facilities to study the effects of FSM in the treatment of diabetic wounds and peripheral neuropathies, oral and genital herpes, shingles and in postoperative wound healing and pain control and in dental applications including orthodontics, periodontics and post-operative healing. There doesn’t seem to be any end in sight for what can be accomplished by resonance in the hands of dedicated and caring practitioners.
Cheng N. The effect of electric currents on ATP generation, protein synthesis, and membrane transport in rat skin. Clinical Orthopedics. 1982;171:264-272.
Electronic reactions of Dr. Abrams. Republished articles from Electronic Medical Digest 1980. Vista CA: Borderland Sciences Research Foundation, 1980.
Kandel E., Schwartz J. Principles of neural science, second ed., New York: Elsevier; 1985:331-336.
McMakin C. Microcurrent treatment of myofascial pain in the head, neck and face. Topics in Clinical Chiropractic. 1998;5(1):29-35.
McMakin C. Microcurrent therapy: a novel treatment method for chronic low back myofascial pain. Journal of Bodywork and Movement Therapies. 2004;8:143-153.
McMakin C., Gregory W., Phillips T. Cytokine changes with microcurrent treatment of fibromyalgia associated with cervical spine trauma. Journal of Bodywork and Movement Therapies. 2005;9:169-176.
Olmarker K., Rydevik B., Nordberg C. Autologous nucleus pulposus induces neurophysiologic and histologic changes in porcine cauda equina nerve roots. Spine. 1993;18:1425-1432.
Olmarker K., Blomquist J., Stromberg J., et al. Inflammatogenic properties of nucleus pulposus. Spine. 1995;20:665-669.
Oschman J. Energy medicine: the scientific basis. Edinburgh: Churchill Livingstone, 2000.
Ozaktay A.C., Cavanaugh J.M., Blagoev D.C. Phospholipase A2-induced electrophysiologic and histologic changes in rabbit dorsal lumbar spine tissues. Spine. 1995;20:2659-2668.
Ozaktay A.C., Kallakuri S., Cavanaugh J.M. Phospholipase A2 sensitivity of the dorsal root and dorsal root ganglion. Spine. 1998;23:1297-1306.
Reilly W., Reeve V.E., Quinn C. Anti-inflammatory effects of interferential, frequency-specific applied microcurrent. Proceedings of the Australian Health and Medical Research Congress. 2004.
Taylor J.R., Twomey L.T. Acute injuries to cervical joints, an autopsy study of neck pain. Spine. 1993;18:1115-1122.