13 Massage in sport
Introduction
Massage and soft tissue mobilisation have become accepted modalities in the overall musculoskeletal management of recreational and high performance athletes alike, as both athletes and their coaches explore all avenues to achieve optimal performance and sporting success.
Previous chapters have already discussed the effects of therapeutic massage. This chapter will present some of the current issues in massage and soft tissue mobilisation in relation to the athlete and athletic performance.
The term athlete in this chapter refers to any regular participant in sport and fitness training. It encompasses a range of levels and involvement (Fig. 13.1).
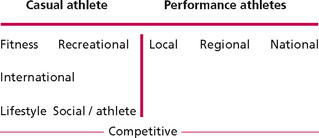
The casual athlete category includes those individuals who have adopted a fitness lifestyle balancing all aspects of physical and mental and spiritual life to achieve for themselves the highest quality of life, wellness and adaptive capacity. Exercise and activity play a major part in the life of these individuals. Massage for this group would focus on enhancing the feelings of well being. They would be unlikely to seek out a specialist sports massage.
A second group of casual athlete is the recreational athlete. These are participants who engage in sport as a social rather than competitive activity. Participation is often irregular and training between games is minimal or absent. This group is likely only to seek out sports massage when injury prevents participation.
Athletes in the performance group differ from the casual social athlete in that for the performance athlete the outcome of competition is seen as a measure of success and failure and where training for specific performance achievement is essential. For the performance athlete, massage and soft tissue mobilisation are part of their regular maintenance routine. Sports massage for this group of athletes should focus on achieving and maintaining peak performance. This is achieved through the application of techniques to facilitate optimal neuromuscular movement patterns, limiting the negative impact of compensatory patterns and aiding physiological and psychological recovery from training and competition stress.
What is sports massage?
Sports massage, rather than being a single technique, can be more appropriately considered as a combination of soft tissue mobilising techniques integrated and applied to the athlete to enhance the positive benefits of physical performance and to minimise the negative effect of the physical stress of training and competition.
Techniques commonly used in sports massage practice are:
• Traditional Swedish massage—effleurage, petrissage, and tapotment;
• Massage with movement—lengthening and broadening;
• Soft tissue release—utilising passive, active or weight-bearing movement;

The range of techniques available and the integrated mode of application in sports massage practice has made research in to the efficacy of sports massage challenging. This challenge is as yet unresolved. Currently only the components of Swedish massage have been evaluated in relation to the efficacy of sports massage with equivocal results (Weerapong et al 2005). Evidence based on well-designed clinical research is more authoritative than that based on consensus and experience and views of recognised experts. In the field of sports massage there has been only limited well-designed clinical research, leaving consensus and the views of recognised experts as the best evidence available (Best et al 2008).
The empirical success of sports massage application lies in the selection of appropriate technique(s), positioning of the target tissue and accuracy of application to meet the specific needs of the individual athlete. Sports massage practice like all other manual therapies must be based on thorough assessment and sound clinical reasoning.
To be successful the sports massage practitioner must not only be skilled in the application of massage techniques but must have an understanding of the theory underpinning practice. This should include a sound knowledge of functional anatomy coupled with an appreciation of the biomechanics of specific sports skill. It is important that there is an understanding of how the soft tissue responds and adapts to the imposed stress of training and competition including the response to trauma, inflammation and repair.
Soft tissue response to training and recovery
Athletic performance is dependent on the synergistic interaction of the whole body musculoskeletal system. To be successful the performance athlete needs to develop sports-specific skill and ability of the highest quality and efficiency. This is dependent on training specificity, skill repetition and motor learning ability and genetic predisposition to achieve the physiological changes, neuromuscular movement patterns and compensatory soft tissue adaptations necessary for optimal performance.
Training for improved performance is based on the established specific adaptation to imposed demand (SAID) principle (Baechle & Earle 2008) (Fig. 13.2). To affect a change in the body system or tissue the demand must be sufficient to provoke an adaptation response. The demand must be specific to the skill pattern(s) required if it is to carry over into performance. It is important to remember that to provoke adaptation the body system needs to be stressed, often inducing a microtrauma response in the tissue. Adaptation is a time-dependent process; therefore sufficient time between loading events needs to be given to allow the adaptation process to occur. A period of recovery between loading events is therefore an essential component of optimal training design (Baechle & Earle 2008).
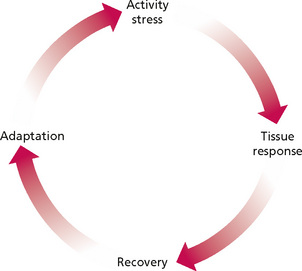
Figure 13.2 • • Cycle of SAID training response.
Reprinted from Anatomy and Physiology 6e, Thibodeau & Patton (2007) with permission from Elsevier.
The SAID approach to training while facilitating the development and maintenance of the optimal capacity of the major body systems exposes the athlete to the risk of injury when the tissue load exceeds the adaptive and reparative capacity of the tissues. It should be remembered that not all tissues respond in the same way and the response is stepwise rather than linear.
Regular sports participants demonstrate tissue changes in response to sport-specific movement patterns and training demand. Increases in the strength of the ligaments and tendons have been identified in response to repeated loading; however, in early training there is some structural weakening before the strength gain (Archambault et al 1995). This may be the reason athletes new to sport or suddenly increasing their training are prone to overuse injury affecting the tendons.
Fascia is an interconnecting fibrous connective tissue found throughout the body. It forms the sheaths around the muscles, forming separation between individual muscles, and allows the smooth gliding between the adjacent muscles. The interconnecting fascial planes also provide pathways for neural and vascular structures. Trauma or overload of fascial tissue can result in loss of elasticity and tissue congestion.
The stress response of the supporting fascia to real or perceived threat is tissue thickening. Repeated stress on the fascia produces fibrotic thickening which can spread over time across the fascial sheath, resulting in reduced mobility and further dysfunction. The functional integration of fascial sheaths connecting the lower and upper limbs via ‘slings’ crossing the trunk can lead to body-wide compensatory shifts (Myers 2009, Vleeming et al 2007). The integration of the fascial sheaths requires the massage practitioner to consider the whole body movement pattern compensations in response to local tissue stress when designing massage applications. Massage application should be aimed at influencing the mobility of the fascia.
Fritz (2005) reports application of slow gliding movements with a degree of tissue ‘drag’ producing a slow sustained pressure or tension can be effective in influencing the pliability of the tissue and increasing blood flow. Application of massage strokes should include mobilising the fibres longitudinally, diagonally and cross fibre to mirror the multiplanar and multidirectional demand of sport. Soft tissue release with passive or active movement can be incorporated to focus on more localised areas of thickening or tissue resistance (Sanderson 1999).
Training has been shown to enhance the physiological responses to physical demand with changes seen in the vascular network and local muscle physiology to meet increased metabolic demand (Baechle & Earle 2008). Aubert et al (2003) identified that high intensity exercise and training produced an autonomic imbalance characterised by an increase in resting heart rate often considered to be an indicator of overtraining in an athlete (Holzer 2007). Arroyo-Morales et al (2008) report that whole body myofascial release in conjunction with active recovery aided in the restoration of autonomic nervous system balance; however, the method of application of the myofascial release was unclear.
Regular training and sports skill performance will also lead to a refining of neural patterning through responsive change in cortical plasticity (Tyc et al 2005) and the integration of feedback and feed forward mechanisms in response to task specificity, resulting in enhanced movement efficiency (van Vliet & Henegan 2006).
Changes in the cortical response have been shown to occur relatively quickly (Tyc et al 2005). The development of these preferential pathways will result in high repeatability of motor skill which will increase performance skill. The inter-relationship of the feedback and feed forward mechanisms are essential for ensuring that the body employs the most efficient movement pattern optimising muscle balance and joint position.
The altered movement patterns seen in the athlete in response to injury and subclinical tissue changes provoke a rapid adaptive response in the central nervous system. Left unchecked these adaptations may lead to muscle imbalance and subsequent alteration in joint motion, giving rise to repeated suboptimal loading of the supporting tissues, leaving them vulnerable to overuse injury.
The anticipatory feed forward mechanisms essential for functional stability have been shown to be compromised by pain (Gowan 2004, Hodges et al 2003) and isometric muscle fatigue (Allison & Henry 2002). Sports massage application aimed at reducing pain and minimising the effect of fatigue may be influential in maintaining feedback feed forward balance and thus reducing the risk of injury.
Many sports skills require the athlete to develop a performance-specific functional asymmetry. Functional asymmetry is seen as an excessive range of motion at a joint or joints in order to achieve a specific performance demand. Consider the excessive external shoulder rotation seen at the shoulder during the tennis serve or the javelin throw at the end of the take back. It is important that the sports massage practitioner appreciates the role of functional asymmetry and facilitates its controlled development rather that trying to prevent it. Focus should rather be on preventing unwanted compensatory changes in other structures.
Sports skill demand
Many sports skills are multiplanar and multidirectional, requiring force transmission across several joints, often combining extreme ranges of motion and muscle strength. They are often unpredictable in nature and performed in a changing environment. The athlete needs the capacity to respond appropriately at all times. To ensure that these demands can be met the athlete needs to have access to full range of motion along and across the body chain. This will require optimal muscle length, mobility of and between the supporting fascial sheaths and integrity of the neural control systems. When planning sports massage intervention, it is important to consider the demand of the sports’ skills and specific movement patterns on the individual athlete. Some of the considerations are presented in Table 13.1.
Table 13.1 Consideration of specific movement pattern on the individual athlete
| Specific movement pattern | Sport | Consider |
|---|---|---|
| Running | Athletics; football; rugby | Changes in speed: acceleration and deceleration Changes in direction: forwards backwards; cutting; pivoting |
| Propelling | Balls; implements | Kicking Throwing Hitting Through water e.g. swimming; rowing |
| Take off and landing | Netball; basketball; gymnastics | Take off from one foot or two Landing and stopping Landing and rebounding Changes of direction Aerial skill between take off and landing |
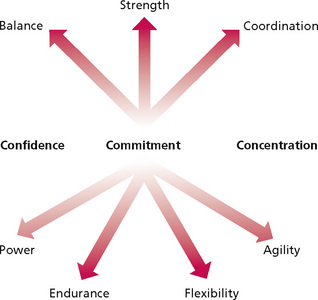
Individual sports skills and performance are based on a combination of factors: see Figure 13.3. The interplay between mobility and stability mechanisms needs to be understood by the sports massage practitioner so that work on one element does not compromise another. The influence of the psychological status of the athlete cannot be discounted as this is often central to performance (Hemmings 2000a, b).
Sports massage application
Massage in competition
Galloway and Watt (2004) identified that sports physiotherapists at major games devoted approximately 45% of their time to massage. Athletes at major competitions present for massage for a variety of reasons: as part of their routine maintenance, as part of their warm-up routine, to help alleviate pre-competition anxiety, to aid recovery between bouts of activity and to minimise the effects of fatigue and or muscle soreness over several days of competition. Techniques and applications will therefore need to be adapted to the demand of the circumstance, timing of events and the practitioner's evaluation of the soft tissue status of the individual.
Recovery between bouts of strenuous activity is a major requirement for the performance athlete especially during periods of competition at a major event. Research activity in relation to sports massage for recovery has focused on delayed onset muscle soreness and fatigue (Barnett 2006, Best et al 2008, Cheung et al 2003, Hemmings et al 2000, Hilbert et al 2003, Howatson & Van Someren 2008, Mancinelli et al 2006, Weerapong 2005, Zainuddin et al 2005)
Muscle fatigue has to date been poorly explored in published studies. Fatigue has been defined as any exercise-induced reduction in the ability to exert muscle force or power (Powers & Howley 2009) with both peripheral and central mechanisms reported to contribute to muscle fatigue. The specific mechanisms of muscle fatigue have not yet been established although chemical, neural, vascular and mechanical factors are all implicated. Fatigue has also been found to have a detrimental effect on motor pattern, resulting in an increased potential for suboptimal performance and injury. Kernozek et al (2008) identified altered landing mechanics following neuromuscular fatigue while Givoni et al (2007) demonstrated altered proprioception in response to fatigue of the quadriceps. Fatigue has also been identified as a contributor to reduction in shock attenuation resulting in increasing loading on the skeleton (Nordin & Frankel 2001), which may contribute to the development of stress fractures.
In many sports such as gymnastics, throwing and jumping in track and field and weightlifting, rest and recovery time between fatiguing bouts of activity are short. Rapid recovery is therefore an important factor in maintaining optimal performance throughout the duration of the competition. The focus of massage in this context is to enhance the clearance of metabolites, and to gain reduction in post exercise muscle tension. Early studies focused on the increase of circulation and the clearance of post activity lactate acid (Bale & James 1991, Monedero & Donne 2000); however, these studies did not address the short duration applications necessary in the context of sport competition.
Application of coarse vibrations and shaking to the whole limb can produce alteration in muscle tone via overload of neural input into the central nervous system from the mechanoreceptors. Vibration and shaking in combination with effleurage may have a more positive influence on the circulation helping to clear post activity metabolites. Effleurage in this context should be varied in depth and rhythm to avoid a sedating effect and to maintain the athletes concentration and focus. There are as yet no published studies that evaluate the depth and rhythm of effleurage nor are there any that consider the effect of coarse vibration and shaking on recovery of muscle performance. A study by Hemmings (2000a) found that although massage had no effect on recovery of muscle power, it did have a positive influence on the athletes' perception of recovery.
Post activity massage
Massage after activity is often linked to the prevention of muscle soreness and the associated loss of function. It is in the area of delayed onset muscle soreness that most of the research relating to sport has taken place.
Delayed onset muscle soreness (DOMS) is a complex phenomenon. Cheung et al (2003) present six proposed causal mechanisms for DOMS: lactic acid; muscle spasm; connective tissue damage; muscle damage; inflammation and calcium release. It is, however, unlikely that any one of these is responsible in isolation.
DOMS is associated with sudden change in activity or increased training load predominantly in association with eccentric muscle work (Jonhagen et al 2004). Eccentric loading has been associated with structural damage to both muscle and connective tissue leading to oedema and localised inflammatory response. Nosaka et al (2002) found that the level of indicators of muscle damage did not correspond to the intensity or course of DOMS, thereby suggesting that DOMS may be present with minimal muscle damage and that muscle damage may occur with minimal DOMS. Zainuddin et al (2005) therefore suggest that some interventions may be effective for enhancing recovery of muscle function without affecting DOMS or vice versa.
Increased muscle soreness and swelling are common features of DOMS and are well recognised by athletes but the accompanying temporary decrease in muscle function is less well recognised (Jonhagen et al 2004). Previous research has reported changes in joint kinematics, muscle function and gait in the presence of DOMS (Harris et al 1990, Weber et al 1994) and muscle damage (Paschalis et al 2007); however, Saxton et al (1995) report that athletes’ perception of the subsequent physical impairment is often disturbed, which may in turn lead to an increased risk of injury. Moraska (2005) reports that while concentric and isometric muscle function recovers within 4 days, eccentric force production may take up to 10 days.
Studies relating to DOMS have focused predominantly on the removal of lactate following exercise and on increasing circulation. The role of lactate levels in DOMS has now been largely discounted. Early research reviewed by Ernst (1998), carried out on active population but not specifically on performance athletes indicated that massage may have a positive effect on DOMS. This is in contrast to the review by Tiidus (1997) who found no evidence to support the use of massage in the management of DOMS. In one of the few randomised control trials Frey Law et al (2008) found that deep massage had a positive effect on reducing pain associated with DOMS, whereas superficial touch had little or no effect. Much of this conflict in the evidence is due to the methodological variations in design, subjects, massage technique and skill of the therapist, making comparison between studies almost impossible.
It is important to remind ourselves that DOMS is associated with a change in intensity or nature of activity. Performance athletes are for the most part highly trained and therefore their susceptibility and response to DOMS is significantly lessened compared to the recreational athlete.
Out of competition maintenance massage
The application of massage and soft tissue mobilisation for maintenance of health, well being and optimal performance forms the major part of the work of the sports massage practitioner. To be effective in this phase of athlete management the emphasis must be on normalisation of the body tissues and movement patterns.
Massage for maintenance focuses on addressing and managing some of the ‘silent’ subclinical contributors to musculoskeletal dysfunction. Progression of excessive tissue loading to dysfunction occurs over time (Fig. 13.4).
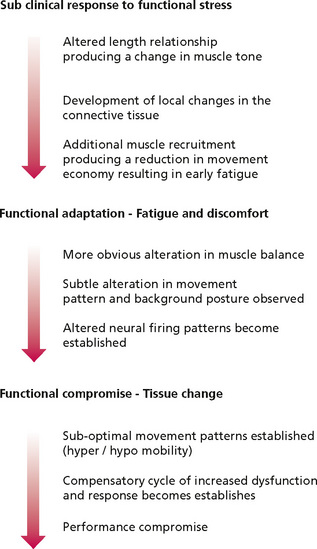
Judicious application of sport massage techniques can minimise or reverse this process. The specific direction, duration, depth and emphasis will depend on the palpation findings and the tissue response throughout the treatment.
Many athletes in regular training will seek out prophylactic sports massage as part of their training and recovery plan rather than wait for injury to strike. The specific benefit of this prehabilitative massage interventions is hard to quantify and therefore difficult to research.
The practitioner needs to evaluate both the primary performance pattern (specific skill pattern) of the individual and the associated secondary pattern looking at the background movement control of posture and balance. The interplay of the background adjustment and the primary movement intent are essential for optimal movement performance. An imbalance of this interplay may lead to the development of a less than optimal compensatory pattern which if left unchecked can lead to a compensatory movements resulting in tissue dysfunction.
It is important to consider that the more elite high-performance athlete is likely to have skill levels that are highly repeatable which can produce for consistent loading on specific tissues. The less skilled performer tends to have a more variable skill pattern which produces a more variable loading pattern. The high-performance athlete is therefore vulnerable to repetition overload especially if there are alterations in tissue as a consequence of fatigue or prior injury. The variable loading pattern of the less skilled athlete may spread the tissue load but there will also be a reduction in the adaptive strengthening of the ligaments and tendons. This may give rise to an increased injury potential especially on sudden unguarded movements.
Specific sports massage application
Athletes have unique physiognomy and as a result respond to training and performance in a highly individual way. Sports massage must be responsive to the specific needs of the individual.
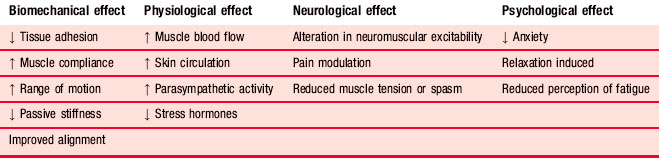
Although evidence is limited the proposed benefits of sports massage can be considered under four headings when planning intervention (see Table 13.2).
Swedish massage theory and application has already been presented elsewhere in this text so only specific adaptations in relation to sport application are presented here. Other adjunct techniques are briefly outlined. For further detail on application the reader is directed to Chaitow & Walker Delany (2001, 2002).
Effleurage
One of the key roles of introductory effleurage and/or palpation examination is to identify area of tissue change, local tenderness and sites of pain. When an area is found to be tender on palpation it can be considered to be responding to or associated with disturbance of normal muscle balance, altered reflex activity or soft tissue dysfunction.
Effleurage with active movement is an effective method of increasing muscle length. This can be specifically targeted to areas of local thickening and tissue bind found longitudinally along the line of muscle fibre orientation. It is a useful approach in warming up an area of post muscle strain injury repair prior to stretching or activity.
Effleurage can also be coupled with movement to achieve a broadening or spreading of fibres. This is a useful method of loosening adhesions across the fibres of the target muscle. It is beneficial in restoring muscle extensibility following resolution of intramuscular haematoma.
Positional release techniques
Chaitow (1996) defines ‘positional release’ as the positioning of the body or part of the body in such a way as to facilitate a resolution of musculoskeletal dysfunction. The literature has identified several approaches to positional release (Jones 1981: strain counterstrain; Bowles 1981: functional technique) but there is a degree of commonality as all require that the client be positioned in such a way that the implicated tissues are placed away from any resistance and towards a position of comfort.
This approach has value in sport where sport skill demand places excessive repetition and loading on the tissues, resulting in their inability to fully relax back into the neutral state after the functional stress is removed. Failure to return to this state after activity results in local spasm with or without local tenderness. If this suboptimal position is maintained over time the normal flow of proprioceptive information is disturbed, resulting in an alteration in resting muscle length with one component becoming hypershortened. Any sudden stretching of this shortened structure causes a further reflex shortening of the already shortened muscle. Unless this reflex response is addressed, the response continues, producing an increased pain response.
The massage practitioner can assist in the management of this response as a preliminary to other massage applications. The body or the local body part is positioned by the practitioner away from any resistance towards a position of ease. This can be identified by monitoring the tone in the stressed tissue. As the position of ease is achieved and maintained there is a palpable reduction in tone. As the tone reduces, the body or body part can be moved into a more neutral; position and other techniques applied as indicated.
Muscle energy techniques
The reciprocal innervation of the neuromusuloskeletal system forms the basis of the muscle energy approach to management of the athlete. It is dependent on the interaction between muscle spindle and Golgi tendon organ to influence change in the length and tension of the target muscles. Post isometric relaxation (PIR) and reciprocal inhibition (RI) are the two methods of applications of muscle energy techniques.
PIR is an effective tool in increasing range of motion in a shortened muscle. The athlete is carefully positioned to ensure that the target muscle can be taken to the point of restriction. At this point the practitioner resists isometric contraction of the muscle. Following the release of the contraction there is a refractory period before the muscle is able to contract again. This period is used to move the limb further into range until a new point of restriction is encountered. The process is then repeated until range is restored.
In situations where pain is inhibiting the target muscle RI may be the best approach for improving range. The athlete is positioned so that the antagonist of the target muscle can be isometrically contracted; this will provoke relaxation in the target muscle through the mechanism of reciprocal innervation. Following this inhibition there is an immediate demonstrable reduction in tone, allowing an increased movement potential in the target muscle (Chaitow & Walker Delany 2001).
Clinical increase in range of the target tissue is well accepted among practitioners; however, there are as yet no randomised control trials to evaluate the efficacy of muscle energy approaches in an athlete population.
Acute soft tissue injury management
Following trauma to the soft tissues fibrin-rich inflammatory exudates often pool in the anatomical spaces. If left unchecked, fibrous adhesions can begin to form, leading to adhesions between normally friction-free gliding surfaces. The sports massage practitioner must address this problem respecting the healing status of the directly traumatised tissue and associated tissue to help facilitate the early restoration of normal function and to assist in creating an optimal environment for further repair.
Working in conjunction with the normal PRICE (protect, rest, ice, compression and elevation) protocol (CSP 1999) , an example of this would be management of the acutely sprained ankle. Effleurage massage, sweeping through the anatomical space around the posterior margins of the malleoli and up to the popliteal fossa performed with the limb in elevation, can significantly reduce swelling following ankle sprain. Gentle ‘box massage’ can also be incorporated to assist in fluid movement. Begin with general effleurage strokes to the proximal area of the limb, directing the stroke into the femoral triangle to assist in the lymphatic drainage, and minimise any congestion in the proximal structures. This approach can be begun 24 hours after injury and repeated at regular intervals. It is important at this stage to avoid over-vigorous application directly over the traumatised structure(s) so as not to disturb the initial clot formation. A supporting brace should be maintained between massage interventions.
Managing muscular haematomas
Muscular haematomas are a problem in contact and implement sports. They can be divided into two categories—intermuscular and intramuscular haematoma—depending on their presentation and underlying tissue damage.
Intermuscular haematoma
Intermuscular haematoma forms when a direct blow to the muscle causes disruption of the fascia surrounding the traumatised muscle fibres, allowing bleeding to occur freely between and around neighbouring tissues. This results in an often spectacular display of superficial discolouration along with local tenderness at the site of trauma and some loss of range of motion at the joints over which the affected muscle acts.
While these injuries are spectacular to look at they are relatively easy to manage. In the first 48 to 72 hours following injury any massage intervention would be gentle; clearance stroking in the area proximal to the trauma site is all that is initially required from the sports massage practitioner at this stage. As recovery and resolution of the haematoma progresses, massage focus is shifted to ensuring that no compensatory movement patterns are left to develop. For the lower limb this will involve addressing the trunk and pelvis as well as the contralateral limb and the distal area of the ipsilateral limb. Once resolution has been achieved effleurage with lengthening can be employed to ensure that the local extensibility is restored at the site of the repaired tissue. RI can be employed after the initial clot has stabilised to encourage relaxation in the fibres surrounding the injury site and to encourage range of motion. PIR can be employed as healing continues to restore extensibility and range in the muscle. This may need to continue during the rehabilitation phase to ensure normal function is restored.
Intramuscular haematoma
By contrast an intramuscular haematoma has little to show in the initial stages. In the type of injury the direct blow to the muscle is sufficient to cause a significant crush injury to the muscle fibres but the fascial sheath surrounding the muscle remains intact. The consequence of this is that bleeding from the crush injury builds up within the muscle being unable to escape from the enclosing fascia. The pressure from the bleeding causes pain as it stretches against pain-sensitive structures. This increase in pressure will also compromise the vascular supply to the surrounding area and especially to the focal point of the trauma. Chemical pain will add to the pain presentation from the local ischaemia and subsequent hypoxia and buildup of metabolites. At the initial presentation this is often seen as a ‘target area’: white in the centre due to compromised blood supply and red around the outside where blood is pooling from the intact supply.
A palpable very firm tender mass is detected at the site of the primary blow. The athlete is likely to have a significant loss of function of the implicated muscle as a consequence of both the local swelling and secondary protective muscle spasm provoked by the pain. Resolution of this type of injury can be slow as blood supply essential for the inflammatory and healing process is severely compromised. Overzealous treatment can result in the development of calcification within the haematoma.
The sports massage practitioner must make every effort to avoid increasing tension in the already tense area by avoiding any contact directly over the affected area. Gentle finger massage around the periphery of the area may assist in reducing local pressure and normalising blood supply.
Proximal clearance utilising slow gently effleurage strokes may be beneficial and can be introduced as soon as the clot has stabilized. As resolution continues gentle effleurage can be re-introduced to the injured muscle, avoiding direct pressure over the injury site. Management of secondary compensations through fascia mobilisation and muscle balancing through the use of RI and PIR techniques can begin as soon as the patient can tolerate it.
Once the area of healing is stable (usually after 14–21 days), work can be focused on restoring local tissue extensibility within the injured muscle. Local soft tissue release and effleurage with lengthening and broadening are particularly valuable here. Techniques focusing on normalisation of muscle tone and encouraging extensibility should be continued as the athlete returns to training and competition.
Muscle strain
Hamstring complex
Two joint muscles are vulnerable to muscle tear with the hamstring complex being the most commonly injured in sprint athletes (Drezner 2003, Hoskins & Pollard 2005). Orchard (2001) identified that previous injury is the major contributor to future recurrence. Prevention of injury must therefore be a major component in the management of the sprint athlete. The challenge for the practitioner is to recognise the individual athletes predisposing risk factors that contribute to hamstring injury.
The biarticular nature of the hamstring complex across the knee and hip require the practitioner to consider the stresses arising from above and below. This is especially the case during sprinting when the hamstring must adapt rapidly from concentric to eccentric action during the swing phase and initial foot contact of gait to maintain efficient forward momentum.
The distal expansions of the hamstrings provide lateral (biceps femoris) and medial support (semi membranosis and semitendinois) for the knee joint. The distal attachment of the biceps femoris also has a fascial connection to the peroneus longus (Stranding et al 2005). Alteration of the biomechanics of the foot and lower leg may place additional stress on the hamstrings, especially the biceps femoris. Running biomechanics must therefore be considered in the assessment and management of the sprint athlete.
Proximally the hamstring complex attaches to the ischial tubersity. Biceps femoris via a fascial expansion is connected to the sacrotuberous ligament of the sacroiliac joint which in turn has a facial connection with the thoracolumbar fascia (Vleeming et al 2007). The extensive nature of muscular attachments to the thoracolumbar fascia provide a functional connection between the hamstrings and the pelvis, the trunk, upper torso and the shoulder girdle. This integration of function requires the practitioner to evaluate the overall posture and alignment of the athlete.
Management of hamstring injury will follow a pattern similar to that proposed for the intermuscular haematoma. Consideration must also be given to the complex functional role of the thoracolumbar fascia. Soft tissue release to the thoracolumbar fascia should be included to ensure optimal mobility is maintained. It is also important to reduce any muscle imbalance across the hip and pelvis to ensure normal pelvic tilt can be maintained to reduce the stress on the proximal attachment of the hamstrings.
Overuse injury in running sports
The evolution of mass participation in charity running events over the past two decades has brought with it a large number of recreational athletes who take on the challenge of training and running distances up to a marathon. This increased participation has also produced an increase in injury. In the early 1990s there were reports that between 25 and 50% of runners experienced an injury that was severe enough to cause a break in training or an alteration in performance.
Training and running up to and beyond marathon distances brings with it high repetition loading with a relatively constant pace resulting in a high level of cyclic loading, leaving tissue vulnerable to overuse and overload failure, especially in the poorly vascularised tendons. Cavanagh and La Fortune (1980) identified that each kilometre run required 600 foot strikes Many team sports involve running, often requiring rapid changes of pace and direction while running at speed with sudden stops and starts which produce additional stress on the muscles and the supporting and stabilising connective tissue. As a result of running-related activity, exercise-related lower limb leg pain has (ERLLP) has become an increasingly common overuse problem presenting to the sports massage practitioner.
ERLLP encompasses some of the more enigmatic sports injuries including anterior knee pain syndrome, iliotibial band syndrome, ‘shin splints’, medial tibial stress syndrome, compartment syndrome and stress fracture. In order to effectively manage these often challenging and long-lasting conditions it is necessary for the sports massage practitioner to have an appreciation of the contributing factors.
In a review of risk factors for lower limb injuries Murphy et al (2003) found that there was limited agreement and understanding of causative factors. Several studies have put forward a range of potential causation. These can be roughly divided into intrinsic and extrinsic factors and are presented in Table 13.3.
Table 13.3 Intrinsic and extrinsic factors in musculoskeletal injury
| Intrinsic | Extrinsic |
|---|---|
| Individual structural anatomy Foot posture Pronated foot (low medial arch) Supinated foot Knee alignment Valgus Varus Hip position Anteverted (toe in) Retroverted (toe out) Tissue load history Previous injury Preferred posture habit Poor physical condition Age |
Changes in training load Activity, intensity load, frequency Surface and footwear Terrain Regular irregular Incline/decline camber |
These factors need to be considered by the practitioner in the clinical reasoning and decision-making prior to assessment and treatment of the athlete.
Prospective studies investigating the cause and effect relationship of intrinsic biomechanical risk factors were lacking prior to the study of Willems et al (2006). In a study of 400 PE students Willems et al found that those subjects who developed ERLLP had a running pattern that differed from those who remained injury free. The common findings in the ERLLP subjects were a more central heel strike at initial contact, a more everted foot with increased loading under the medial aspect of the forefoot in mid-stance and an increase in extension range of motion at the first metacarpophalangeal joint, the most clinically significant finding of the three being increased eversion of the foot in mid-stance. The functional linkage between the foot and knee would tend to produce an increase in internal rotation of the tibia in response to the more everted foot, along with an increase in the passive and dynamic stabilising demand of the soft tissues at the hip and knee to limiting internal rotation. The failure of the tissues to meet this increased stabilising demand has been suggested as a cause of mal-tracking of the patella, provoking patellofemoral pain syndrome and increased load on the iliotibial band, resulting in the development of iliotibila band syndrome.
Transition from walking to running occurs as the double stance phase in the walking gait cycle is replaced by a float phase between each foot contact in running. With this comes an increased demand on the limb at foot contact. There is an increased stability demand at the hip, knee and foot and ankle along with increased impact force from 0.7 (walking) × body weight to 2–3 (running) × body weight.
As running speed increases, initial foot strike moves from the hind foot to the forefoot. This shift reduces the contact area that accompanies mid-stance. This resulting reduction in base of support will require increased stability throughout the support limb. Increased running speed will also reduce contact time with the ground, reducing the time for force dissipation. The time between each foot contact reduces as speed increases, reducing recovery time between each loading event. Any muscle weakness or imbalance at the hip, knee or ankle must therefore be minimised or eliminated to ensure optimal loading (Novacheck 1998).
Patellofemoral pain syndrome
Patellofemoral pain syndrome is a catch-all term for anterior knee pain located around the patella margins. It has been related to hyperpronation of the foot during gait with associated increased medial rotation of the tibia and a tendency towards an increased valgus stress of the knee with increased stress on the lateral aspect of the patella and the soft tissue support of the lateral aspect of the knee, namely the iliotibial band and the distal biceps femoris. Shortening of any of these can restrict patella glide, increasing the stress on the lateral margin of the patella. These altered kinematics have been attributed to poor foot mechanics and also to weakness of the ipsilateral gluteus medius (Powers 1998).
Massage can play a significant part in both the prevention and management of this condition utilising a combination of applications including general effleurage to the quadriceps and hamstrings, muscle energy release of tensor fascia lata and gluteus maximus to optimise the mobility of the iliotibial band and petrissage, wringing and bending of biceps femoris to increase extensibility. The practitioner should also consider the tissues of the lower leg and foot as well as those of the pelvis and low back.
The shoulder complex
Cools et al (2003) reports that chronic shoulder pain is probably the most common upper extremity problem in athletes involved in overhead sports.
It is commonly recognised that symptoms of glenohumeral impingement in the overhead athlete are often related to instability in the shoulder complex (Borsa et al 2008, Meister 2000). Instability of the shoulder complex is often insidious and difficult to demonstrate on clinical testing.
The quality of shoulder movement depends on the interaction between the scapular and glenohumeral kinematics. The posture of the head, neck and upper torso also play a part as they form the attachment points for the major scapular muscles, namely trapezius (upper middle and lower fibres), levator scapulae rhomboids and serratus anterior. For optimal function of the glenohumeral joint, the head of the humerus needs to be centred into the glenoid fossa of the scapula. In overhead sports skills the scapular needs to rotate on the thorax to position the glenoid to form a platform for the humerus. Muscle balance and timing of the muscles acting on the scapula is essential to ensure that this can be achieved.
Sports-specific throwing skills often require the acquisition of a functional asymmetry in range of motion. In the javelin thrower for example there is a requirement for an excessive range of external rotation with horizontal extension in the throwing shoulder. To achieve this, the athlete needs to have optimal extensibility of the anterior glenohumeral capsule and the supporting anterior structures, and balance of control between the infraspinatus and subscapularis to control the position of the head of the humerus in the glenoid. An increased length in the ipsilateral pectoralis major and pectoral fascia along with the contralateral abdominal fascia is also required to allow the shoulder girdle and trunk to rotate effectively against the pelvis to gain an efficient pre-load position. In order to achieve this position there must be sufficient rotation at the pelvis, side flexion of the trunk and hip extension on the leading leg. All of these factors need to be addressed in the massage planning.
The deep-seated tendon of supraspinatus, the commonest site of impingement, is not accessible for massage under the acromion and therefore treatment should be aimed at normalising the function of the shoulder girdle. Sports massage can play a major part in optimising the position of the scapula, and the function of the glenohumeral joint through management of posture and muscle balance across the head, neck and shoulder girdle. Soft tissue releases of the major facial sheaths should also be included to ensure optimal length across the trunk. Local application to optimise the function of individual muscles should be included.
Sports massage in the management of athletes with disabilities
Over the past 60 years there have been major advances in sport participation by athletes with disabilities. The televising of the Paralympic Games has been a major driving force for encouraging more people with disabilities into sport. The participation level and commitment to sport is the same as is seen in Figure 13.1 but unlike their able-bodied counterparts, athletes with disability often have an underlying medical condition that may have a negative impact on sporting performance.
At the elite end of performance for athletes with disability the Paralympic Games now boast over 4000 participants across a range of sports categorised into three major categories of disability:
Each category brings its own challenge for the massage practitioner working with athletes with disabilities. Associated problems with cognitive ability and social skills are often present and may require a more flexible approach to communication and handling to ensure optimal compliance with treatment.
Categorisation is made for convenience but athletes do not fall neatly into each. The sports massage practitioner working with athletes with disability will need to understand the complexity and impact of any coexisting medical conditions in order to design appropriate interventions.
Athletes with visual impairment
Athletes with visual impairment often present with altered or increased postural stress as a result of their response to performing with a guide, as in such sports as track athletics and tandem cycling. Many may also develop altered movement patterns as they utilise enhanced senses of hearing and touch to optimise their performance. Running athletes often have an altered gait pattern that if not effectively managed can result in overuse injury. Prophylactic massage application can play a major part in the overall management of the visually impaired performance athlete. The massage practitioner must consider any compensatory mechanisms alongside the individual's physical profile and the specific sports skill demand when designing massage intervention for this group of athletes. The application of techniques should not require adaptation but it is important that the practitioner takes care to minimise the risk of skin irritation as the athlete may not be able to monitor this for themselves.
Athletes with intellectual impairment
Intellectual impairment may accompany some of the physical disability categories within the Paralympic sports. This should not be confused with those athletes with frank learning disabilities that currently compete in the Special Olympics. Working with athletes with intellectual impairment and those with learning difficulties demands care in communication and chaperoning to ensure that the athlete understands and consents to the massage intervention and feels comfortable with the modes of application. Formal consent may need to be obtained from a parent or guardian. The massage practitioner should also be aware of any accompanying physical problems, for example associated hypermobility, poor muscle tone and altered proprioception often found in Down's Syndrome. Athletes with intellectual impairment may also have associated medical conditions; for example, athletes whose intellectual disability resulting from head trauma may have accompanying epilepsy. In the management of these athletes the massage practitioner should ensure that they have a full medical history in order to identify any specific cautions and or contraindications.
Athletes with physical disabilities
In order to allow athletes with physical disability to compete in a fair and equitable manner they are further arranged into four subcategories:
Each category brings with its own specific challenges for the massage practitioner.
Spinal cord injury
Spinal cord lesions may be either acquired through trauma or disease or as a consequence of a congenital condition such as spina bifida. The level of the spinal lesion determines the classification for these athletes but also gives the massage practitioner guidance on accompanying problems that need to be considered in the treatment design. Thermoregulation is a challenge for athletes with spinal cord injury. Dissipation of any heat generated by the massage application may be compromised especially if the massage is being applied in a hot environment. Conversely athletes may also experience difficulties in maintaining body temperature in a cold environment. The massage practitioner needs to consider this relation to skin exposure and draping when working in a low ambient temperature.
The loss of skin sensation below the level of the lesion makes the spinal-injured athlete vulnerable to skin abrasions and pressure sores. Care must be taken when positioning the athlete for massage. The pattern of application should be considered in advance to ensure optimal positioning and regular change of posture to avoid unnecessary pressure buildup. Care of any insensitive area during handling is essential for minimising the risk of abrasion.
Altered sensation below the level of the lesion prevents the normal pain response in athletes with spinal injury. The lack of pain response may be the trigger for the potentially life-threatening response of autonomic dysreflexia. In the spinal-injured patient any nociceptive input below the level of the lesion can result in an inappropriate level of noradrenaline (norepinephrine) secretion, producing hypertension, sweating and skin blotching above the level of the lesion. The individual will also complain of a pounding headache. The massage practitioner must be aware of the potential for this condition and take care in handling and positioning of the insensitive region below the level of the lesion. If the practitioner suspects the onset of this condition it is essential to act promptly as the elevated blood pressure, if not managed, can result in cerebral haemorrhage or even death.
Spinal cord-injured athletes, as a consequence of the paralysis-related immobility and loss of weight-bearing activity, also suffer from progressive loss of bone mineral density, leaving them vulnerable to osteoporotic fracture in the lower limbs and the spine. Fracture in this population may result from minimal trauma. The massage practitioner should maintain a high level of suspicion for fracture when assessing the athlete if the athlete is involved in contact sport or reports a fall from their wheelchair. Once again handling and positioning must respect the risk of fracture.
Wheelchair-based athletes are exposed to significant risk of overuse injury to their shoulder and the functioning levels of the trunk. As in the management of other athletes successful massage application must be based on a sound individual physical profile and an appreciation of the sport-specific skill performance. Optimising posture and managing muscle imbalance are the main focus of intervention in this group of athletes.
Athletes with limb deficiency
Limb deficiency may be acquired or congenital. Limb-deficient athletes are classified for performance according to functional capacity rather than on specific limb deficiency. The potential for muscle power and strength and proprioception of the intact limbs and trunk are normal. Limb deficiency does, however, cause an alteration in the positioning of the centre of gravity and line of gravity, creating a challenge to balance and coordination that the athlete needs to accommodate. These challenges will have an impact on the movement patterns and physical adaptations of the individual athlete. The massage practitioner needs to evaluate these adaptations when designing their intervention. The massage application for this group of athletes needs no specific adaptation.
Athletes with cerebral palsy
The nature of cerebral palsy provides a significant challenge for the sports massage practitioner. Athletes in this category of disability have all movement deficiency classified by the limbs affected and the nature of the movement disorder. Alteration in normal tone is the common physical feature but the severity and nature of the tone change will vary from individual to individual. Alteration in tone will also have a marked impact on posture. Care must be taken in the application of massage to this group. The spasticity (increased tone) may play an important role in the joint stability in these athletes; therefore massage application that reduces tone prior to training or competition may have a negative impact on the athlete, increasing the risk of injury.
‘Les Autres’
This is a complex group of athletes with physical disabilities arising from a range of syndromes that do not fit into any other classification. To work effectively with this group the massage practitioner must be sure that they have a clear understanding of the complexity of the specific syndrome.
Management of athletes with disabilities is a highly specialised area of sports massage. The massage techniques are in common to those of other athletes but the selection and design of the application requires careful planning.
Summary
The variety of context and application techniques routinely employed in sports massage have made the construction of objective research difficult, leaving the efficacy of massage in sport unsubstantiated.
Many of the available studies have been highly dependent on subjective criteria for the diagnosis, treatment application and outcome measure. The effect of touch is unique between practitioner and client, making control and standardisation almost impossible. Design and progression of sports massage application is often guided by the athlete's report of ‘tightness’ or ‘niggles’ and by the practitioner's interpretation of soft tissue ‘feel’, adding to the challenge of standardisation.
Overall evidence for massage in sport has been limited with the major emphasis on post exercise recovery and prevention of delayed onset muscle soreness. The studies have usually had only a small cohort and have been undertaken on non-elite athletes, limiting the validity of any outcome.
Best et al (2008) attempted a meta-analysis to investigate the effectiveness of sport massage for recovery of skeletal muscle following strenuous exercise but it proved impossible due to the large variation in the research method and in the application of the massage intervention. Subjects are predominantly normal healthy subjects or recreational athletes. Studies on performance athletes are minimal. Research is often limited to only a single massage application and to only one limb or part of a limb. The continued value that both athletes and coaches place on benefit of sports massage suggests that future clinical research is needed within the performance sport environment to establish the mechanisms of efficacy.
Key points
• Sports massage is not a single technique. It is the integration of several soft tissue mobilising techniques.
• Successful sports massage is dependent of appropriate technique(s), positioning and accuracy of application to meet the specific needs of the individual athlete.
• Understanding soft tissue response to the stress of training and competition is essential for successful sports massage practice.
• Functional integration of the fascial sheaths requires the practitioner to consider whole body movement patterns and compensations in response to local tissue stress when designing massage applications.
• Mobility and stability mechanisms need to be understood to ensure that treatment of one element does not compromise another.
• Working with athletes with disability requires the practitioner to understand the complexity and impact of any coexisting medical conditions in order to design appropriate interventions.
Allison G.T., Henry S.M. The influence of fatigue on trunk muscle responses to sudden arm movements: a pilot study. Clin. Biomech. (Bristol, Avon). 2002;17(5):414-417.
Archambault J.M., Wiley J.P., Bray R.C. Exercise loading of tendons and the development of overuse injuries: a review of current literature. Sports Med.. 1995;20(2):77-89.
Arroyo-Morales M., Olea N., Martinez M., et al. Effects of myofascial release after high intensity exercise: a randomised control trial. J. Manipulative. Physiol. Ther.. 2008;31(3):217-223.
Aubert A.E., Seps B., Beckers F. Heart rate variability in athletes. Sports Med.. 2003;33(12):889-919.
Baechle T.R., Earle R.W., editors. Essentials of strength training and conditioning, third ed, Champaign, IL: Human Kinetics, 2008.
Bale P., James H. Massage warmdown and rest as recuperative measures after short-term intense exercise. Physiotherapy in Sport. 1991;13(2):4-7.
Barnett A. Using recovery modalities between retraining sessions in elite athletes: does it help? Sports Med.. 2006;36(9):781-796.
Best T.M., Hunter R.D.C., Wilcox A., et al. The effectiveness of sports massage for recovery of skeletal muscle from strenuous exercise. Clin. J. Sport. Med.. 2008;18(5):446-460.
Bowles C. Functional technique - a modern perspective. J. Am. Osteopath. Assoc.. 1981;80(3):326-331. Cited in:Chaitow L. Positional release techniques. Edinburgh: Churchill Livingstone; 1996.
Borsa P.A., Laudner K.G., Sauers E.L. Mobility and stability adaptations in the shoulder of the overhead athlete: a theoretical and evidence-based prespective. Sports Med.. 2008;38(1):17-36.
Cavanagh P.R., La Fortune M.A. Ground reaction forces in distance running. J. Biomech.. 1980;13:397-406.
Chaitow L. Positional release techniques. Edinburgh: Churchill Livingstone, 1996.
Chaitow L., Walker Delany J. Clinical application of neuromuscular techniques, volume 1 The upper body. Edinburgh: Churchill Livingstone, 2001.
Chaitow L., Walker Delany J. Clinical application of neuromuscular techniques, vol. 2. The lower body. Edinburgh: Churchill Livingstone, 2002.
Cheung K., Hume P.A., Maxwell L. Delayed onset muscle soreness. Treatment strategies and performance factors. Sports Med.. 2003;33(2):145-164.
Cools A.M., Witvrouw E.E., Declercq G.A., et al. Scapular muscle recruitment patterns: trapezius latency with and without impingement symptoms. Am. J. Sports Med.. 2003;31(4):542-549.
Cowan S.M., Schache A.G., Brukner P., et al. Delayed onset of transversus abdominus in long-standing groin pain. Med. Sci. Sports Exerc.. 2004;36(12):2040-2045.
CSP. Guidelines for the management of soft tissue (musculoskeletal) injury with protection, rest, ice, compression and elevation (PRICE) during the first 72 hours. Chartered Society of Physiotherapy. 1999.
Drezner J.A. Practical management: hamstring muscle injuries. Clin. J. Sport. Med.. 2003;13:48-52.
Ernst E. Does post-exercise massage treatment reduce delayed onset muscle soreness? A systematic review. J. Sports Med.. 1998;32(3):212-214.
Frey Law L.A., Evans S., Knudtson J., et al. Massage reduced pain perception and hyperalgesia in experimental muscle pain: a randomised control trial. J. Pain. 2008;9(8):714-721.
Fritz S. Sports and exercise massage: comprehensive care in athletics, fitness and rehabilitation. St Louis: Elsevier Mosby, 2005.
Galloway S.D., Watt J.M. Massage provision by physiotherapists at major athletic events between 1987 and 1998. Br. J. Sports Med.. 2004;38(2):235-236.
Givoni N.J., Pham T., Allen T.J., et al. The effect of quadriceps muscle fatigue on position mating at the knee. J. Physiol.. 2007;584(1):111-119.
Harris C., Wilcox A., Smith G., et al. The effect of delayed onset muscle soreness (DOMS) on running kinematics. Med. Sci. Sports Exerc.. 1990;22(2):S200.
Hemmings B. Sports massage and psychological regeneration. Br. J. Sports Med.. 2000;7:184-188.
Hemmings B. Psychological and immunological effects of massage after sport. Br. J. Sports Med.. 2000;7(12):516-519.
Hemmings B., Smith M., Graydon J., et al. Effects of massage on physiological restoration, perceived recovery and repeated sports performance. Br. J. Sports Med.. 2000;34(2):109-114.
Hilbert J.E., Sforzo G.A., Swensen T. The effects of massage on delayed onset muscle soreness. Br. J. Sports Med.. 2003;37(1):72-75.
Hodges P.W., Moseley G.L., Gabrielsson A., et al. Experimental muscle pain changes feedforward postural responses of the trunk muscles. Exp. Brain Res.. 2003;151(2):262-271.
Holzer K. The tired athlete. In Brukner P., Khan K., editors: Clinical sports medicine, third ed, North Ryde, NSW: McGraw-Hill, 2007.
Hoskins W., Pollard H. The management of hamstring injury—Part 1: Issues in diagnosis. Man. Ther.. 2005;10:96-107.
Howatson G., van Someren K.A. The prevention and treatment of exercise induced muscle damage. Sports. Med.. 2008;38(6):483-503.
Jones L. Strain and counterstrain. Colorado Springs: Academy of Applied Osteopathy; 1996. Cited in: Chaitow L. Positional release techniques. Edinburgh: Churchill Livingstone, 1996.
Jonhagen S., Ackernann P., Eriksson T., et al. Sports massage after eccentric exercise. Am. J. Sports Med.. 2004;32(6):1499-1503.
Kernozek T.W., Torry M.R., Iwasaki M. Gender differences in lower extremity landing mechanics caused by neuromuscular fatigue. Am. J. Sports Med.. 2008;36(3):554-565.
Mancinelli C.A., Davis D.S., Aboulhosn L., et al. The effects of massage on delayed onset muscle soreness and physical performance in female college athletes. Phys. Ther. Sport. 2006;7:5-13.
Meister K. Injuries to the shoulder in the throwing athlete. Am. J. Sports Med.. 2000;28:265-275.
Monedero J., Donne B. Effect of recovery interventions on lactate removal and subsequent performance. Int. J. Sports Med.. 2000;21(8):593-597.
Moraska A. Sports massage: a comprehensive review. J. Sports Med. Phys. Fitness. 2005;45(3):370-381.
Murphy D.F., Connolly D.A.J., Benyonn B.D. Risk factors for lower extremity injury: A review of the literature. Br. J. Sports Med.. 2003;37:13-29.
Myers T.M. Anatomy trains: myofascial meridians for manual movement therapists, second ed. Edinburgh: Churchill Livingstone, 2009.
Nordin M., Frankel V.H. Basic biomechanics of the musculoskeletal system, third ed. Philadelphia: Lippincott Williams and Wilkins, 2001.
Nosaka K., Newton M., Sacco P. Delayed-onset muscle soreness does not reflect the magnitude of eccentric exercise-induced muscle damage. Scand. J. Med. Sci. Sports. 2002;12(6):337-346.
Novacheck T.F. The biomechanics of running. Gait Posture. 1998;7(1):77-95.
Orchard J.W. Intrinsic and extrinsic risk factors for muscle strains in Australian football. Am. J. Sports Med.. 2001;29(3):300-303.
Paschalis V., Giakas G., Baltzopoulos V., et al. The effects of muscle damage following eccentric exercise on gait biomechanics. Gait Posture. 2007;25(2):236-242.
Powers C. Rehabilitation of patellofemoral joint disorders: a critical review. J. Orthop. Sports Phys. Ther.. 1998;28(5):345-354.
Powers S.K., Howley E.T. Exercise physiology: theory and application to fitness and performance, seventh ed. Boston: McGraw-Hill, 2009.
Sanderson M. Soft tissue release: a practical handbook for physical therapists. Corpus Publishing, 1999.
Saxton J.M., Clarkson P.M., James R. Neuromuscular dysfunction following eccentric exercise. Med. Sci. Sports Exerc.. 1995;27(8):1185-1193.
Stranding S., Ellis H., Healy J.C., et al. Gray's anatomy: the anatomical basis of clinical practice, thirtyninth ed, Edinburgh: Elsevier Churchill Livingstone; 2005:1825-1861.
Tiidus P.M. Manual massage and recovery of muscle function following exercise: a literature review. J. Orthop. Sports Phys. Ther.. 1997;25(2):107-112.
Tyc F., Boyadjian A., Devanne H. Motor cortex plasticity induced by extensive training revealed by transcranial magnetic stimulation in humans. Eur. J. Neurosci.. 2005;21(1):259-266.
Van Vliet P.M., Heneghen N.R. Motor control and the management of musculoskeletal dysfunction. Man. Ther.. 2006;11:208-213.
Vleeming A., Mooney V., Stoeckart R. Movement stability and lumbopelvic pain, second ed. Edinburgh: Churchill Livingstone, 2007.
Weber M.D., Servedis F.J., Woodall W.R. The effects of three modalities on delayed onset muscle soreness. J. Orthop. Sports Phys. Ther.. 1994;20:236-242.
Weerapong P., Hume P.A., Kolt G.S. The mechanisms of massage effects on performance, muscle recovery and injury prevention. Sports Med.. 2005;35(3):235-256.
Willems T.M., DeClecq D., Delbaere K. A prospective study of gait related risk factors for exercise related lower leg pain. Gait Posture. 2006;23(1):91-98.
Zainuddin Z., Newton M., Sacco P., et al. Effects of massage on delayed-onset muscle soreness, and recovery of muscle function. J. Athl. Train.. 2005;40(3):174-180.