Communicating with Clients in Crisis
At the end of the chapter, the reader will be able to:
1 Define crisis and related concepts.
2 Discuss theoretical frameworks related to crisis and crisis intervention.
3 Identify and apply structured crisis intervention strategies in the care of clients experiencing a crisis state.
4 Apply crisis intervention strategies to mental health emergencies.
5 Discuss crisis management strategies in disaster and mass trauma situations.
This chapter describes nurse-client relationships in crisis situations and discusses related communication strategies. The chapter focuses on the nature of crisis and presents crisis intervention guidelines nurses can use with clients and families in clinical and community settings. Included are theoretical frameworks that guide the process of crisis intervention. The application section provides practical guidelines nurses can use with clients in crisis, mental health emergencies, and disaster management.
Basic concepts
Crisis
Flannery and Everly (2000) state, “A crisis occurs when a stressful life event overwhelms an individual’s ability to cope effectively in the face of a perceived challenge or threat” (p. 119). People in crisis experience an actual or perceived overwhelming threat to self-concept, or a loss that conventional coping measures cannot handle. Unabated, the resulting tension continues to increase, creating major personality disorganization and a crisis state.
The word crisis comes from the Greek root word krisis, meaning “turning point.” The Chinese ideograph used to represent crisis consists of one character for danger and another for opportunity (Roberts, 2005). Personal responses to crisis can be adaptive or maladaptive. Successfully working through a crisis strengthens people’s coping responses and sense of self-efficacy. People can learn new coping skills, expand their support system, and raise their level of functioning. Maladaptive responses can result in the development of acute or chronic psychiatric symptoms requiring professional treatment.
Crisis State
Everly (2000) defines a crisis state as an acute normal human response to severely abnormal circumstances; it is not a mental illness. Because a crisis state represents a personal response, two people experiencing the same crisis event will respond differently to it. Understanding the person who is experiencing the crisis rather than an objective crisis stressor is critical to successful crisis intervention.
A crisis state creates a temporary disconnect from attachment to others, loss of meaning, and a disruption of previous mastery skills (Flannery & Everly, 2000). Individuals feel vulnerable. People in crisis are open to but also need a goal-directed approach to resolve a crisis state. Crisis intervention strategies are designed to help support people experiencing crisis achieve psychological homeostasis. A favorable outcome depends on the person’s interpretation of the crisis, perception of coping ability, resources, and level of social support.
Types of crisis
A crisis is commonly classified as developmental or situational. Erik Erikson’s (1982) stage model of psychosocial development forms the basis for understanding developmental crisis. Each stage is associated with a psychosocial crisis to be resolved. Successful resolution of each maturational stage leaves a person better able to meet the interpersonal challenges and stressors of the next. Examples of critical incidents associated with developmental crises include marriage, pregnancy and birth of a child, midlife crisis, retirement, meaning in aging, and so on.
Erikson’s (1982) descriptions of normative psychosocial crisis are used as benchmarks for assessing signs and symptoms of developmental crisis. When a situational crisis is superimposed on a normative developmental crisis, the crisis experience can be more intense. For example, a woman losing a spouse at the same time she is going through menopause experiences the double impact of a situational crisis and a normal maturational crisis associated with midlife.
Situational Crises
A situational crisis refers to an unusually stressful life event that exceeds a person’s resources and coping skills. Examples include unexpected illness or injury, rape, car accident, loss of home, spouse, job, and so forth. In health care settings, most crises are situational.
A situational crisis is not defined by the life event itself (Hoff, 2009). Rather, it is the person’s experience of the event—its origin and meaning to an individual, plus combined individual and social factors that influence a person’s perception of the event as a crisis. Common factors influencing how successfully a person responds to a crisis include:
Adventitious Crisis
An adventitious crisis is not a part of everyday experience. It is unplanned, unusual, horrific, and beyond anyone’s control. Examples of adventitious crisis include:
• Natural disasters such as floods, earthquakes, fires, mudslides
• National disasters such as terrorism, riots, wars
• Crimes of violence such as rape, child abuse, assault, or murder (Boyd, 2008)
Disasters are catastrophic for large groups of people or whole communities simultaneously (Michalopoulos & Michalopoulos, 2009).
Other Classifications
Roberts and Yeager (2009) differentiate between a private and public crisis. A private crisis affects individuals and families, but not the community at large. Examples include suicide, terminal diagnosis, a car crash, rape, or the death of a family member. A public crisis event, more commonly referred to as a disaster, affects a whole community or large groups of people simultaneously. People are acutely aware of the precipitating events, for example, with Hurricane Katrina and terrorist attacks.
James (2008) describes two additional types of crisis. An existential crisis occurs when a person questions the meaning of his or her life, and whether it has any value. Midlife crisis falls into this category. Environmental crises are associated with major changes in the ecosystem, such as global warming, volcanic eruptions, disease epidemics, wars, and severe economic depression. Table 21-1 presents the Burgess and Roberts continuum of the different levels of crisis (Roberts & Yeager, 2009).
TABLE 21-1
Burgess and Roberts’ Stress-Crisis-Trauma Continuum
| Levels | Type | Actions/Approach |
| Levels 1 and 2 | Somatic distress crisis and transitional stress crisis | Brief crisis intervention and primary outpatient mental health care/treatment |
| Level 3 | Traumatic stress crisis | Traumatic and group crisis–oriented therapy |
| Level 4 | Family crises | Individual, couple, or family therapy, case management, and crisis intervention focus with forensic intervention |
| Level 5 | Mentally ill persons in crisis | Crisis intervention, psychopharmacology, case and medication monitoring, day treatment, and community support |
| Level 6 | Psychiatric emergencies | Crisis stabilization, outpatient treatment, inpatient hospitalization, and/or legal intervention |
| Level 7 | Catastrophic traumatic stress crises | Application of multiple levels of crisis/trauma intervention inclusive of all previously listed intervention strategies |
From Roberts A, Yeager K: Pocket guide to crisis intervention (p. 15), New York, 2009, Oxford University Press.
Crisis intervention
Crisis intervention represents a systematic application of theory-based problem-solving strategies designed to help individuals and families resolve a crisis situation quickly and successfully, with an anticipated outcome of achieving precrisis level functional capacity (Roberts & Yeager 2009). Each person’s experience of a crisis is unique to that person and situation. Crisis intervention strategies should be adapted to fit each client’s preferences, beliefs, values, and individual circumstances.
Crisis intervention is a time-limited treatment modality. Four to six weeks is considered the standard time frame for crisis resolution, although full recovery can take a much longer period of time, particularly from a disaster crisis (Callahan, 1998).
Strategies are focused on immediate problem solving and strengthening the personal resources of clients and their families. Nurses function as advocate, resource, partner, and guide in the crisis intervention process. There should be a strong focus on helping clients mobilize personal resources and use support resources effectively (Hoff, 2009). The goal of crisis intervention is to return the client to his or her previous level of functioning. Specific goals include:
• Stabilization of distress symptoms
• Reduction of distress symptoms
• Restoration of functional capabilities
• Referrals for follow-up support care, if indicated (Everly, 2000, pp. 1–2)
Theoretical frameworks
Erich Lindemann (1944) and Gerald Caplan (1964, 1989) are considered primary contributors to the development of crisis theory. Lindemann’s study of bereavement in survivors coping with the crisis of death of a loved one or experiencing a disaster provided an initial frame of reference for understanding the stages involved in resolving emotional crisis and bereavement. His findings suggest, “Proper psychiatric management of grief reactions may prevent prolonged and serious alterations in the patient’s social adjustment, as well as potential medical disease” (p. 147).
Caplan broadened Lindemann’s model to include developmental crisis and personal crisis (Roberts, 2005). Although the direct focus of crisis intervention is on secondary prevention because the crisis state is already in motion, Caplan applied concepts of primary, secondary, and tertiary prevention to crisis intervention. His model of preventive psychiatry incorporates reducing the incidence of mental disorders in the community, limiting the duration of mental upset, and reducing impairment from clinical symptoms. Consistent with Caplan’s ideas was the development of practical crisis intervention strategies related to crisis telephone lines, training for community workers, and crisis response strategies. Caplan viewed nurses as key service providers in crisis intervention.
Caplan (1964) described the initial response to a crisis situation as shock, with variations in emotions ranging from anger, laughing, hysterics, crying, and acute anxiety to social withdrawal. Then follows an extended period of adjustment, a period of recoil. This period can last from 2 to 3 weeks. Client behaviors can appear normal to outsiders, but the person often describes nightmares, phobic reactions, and flashbacks of the crisis event.
Caplan uses the term restoration or reconstruction to describe the final phase of crisis intervention. This phase involves taking constructive actions to face and resolve the reality issues present in a crisis situation. If successfully negotiated, the person achieves precrisis functioning or better. When people use self-destructive coping strategies such as drug or alcohol use, violence, or avoidance, restoration is delayed and/or the person is at risk for development of physical or mental symptoms.
Donna Aguilera (1998) developed a nursing model identifying how a crisis develops and corresponding factors needed for resolution. The model proposes that a crisis state occurs in response to a potentially life-changing event because of a distorted perception of a situation or because the client lacks the resources to cope successfully with it. Balancing factors include a realistic perception of the event, the client’s internal resources (beliefs or attitudes), and the client’s external (environmental) supports. These factors can reduce the impact of the stressor, leading to the resolution of the crisis, and can help minimize overreactions.
The absence of adequate situational support and coping skills and/or a distorted perception of the crisis event can result in a crisis state, leaving individuals and families feeling overwhelmed and unable to cope. Interventions are designed to increase the balancing factors needed to restore the person to precrisis functioning. Exercise 21-1 provides insight into the nature of crisis.
Applications
Structuring crisis intervention strategies
Roberts (2005) provides a seven-stage sequential blueprint for clinical intervention, which can be used to structure the crisis intervention process in nurse-client relationships. This model is compatible with the nursing process sequencing of assessment, planning, implementation, and evaluation.
Step 1 (assessment): Assessing lethality and mental status
Safety should be the foremost assessment in any crisis situation. Assessment should focus on determining the severity of the crisis state, and the client’s current danger potential—both to self and to others. If a person’s crisis state is induced or complicated by physiologic factors, the person should be treated as a medical emergency first and then as a psychiatric emergency. Assessment for suicide and homicide should be part of every crisis care assessment.
Nurses need to evaluate the client’s mental status if there is any reason to suspect unsafe or unusual thoughts and behaviors. Clients who are psychotic, under the influence of drugs, severely agitated, or temporarily out of control for medical reasons will require immediate triage to stabilize their physical condition. Close one-to-one observation is critical until the situation is brought under control. Table 21-2 provides guidelines for communicating with a client who is unable to cooperate with assessment or treatment. Family and significant others can provide additional assessment data related to the current crisis state (e.g., documenting changes in behavior, ingestion of drugs, or medical history) if the client is unable to do so.
TABLE 21-2
Guidelines for Working with Uncooperative Clients in the Emergency Department
| Stage | Client Behavior | Nurse Actions |
| 1. Environmental trigger | Stress response | Encourage venting: avoid challenge; speak calmly, clearly; offer alternative |
| 2. Escalation period | Movement toward loss of control | Take control: maintain safe distance, acknowledge behavior, medicate if appropriate, remove to quiet area, "show force" if necessary |
| 3. Crisis period | Emotional/physical discharge | Apply external control: implement emergency protocol, initiate confinement, give focused intensive care |
| 4. Recovery | Cool down | Reassure: support; no retaliation; encourage to discuss behavior and alternative; release when in control; assess reaction to environment; conduct sessions for staff to process all areas of incident |
| 5. Postcrisis and letdown | Reconciliatory | Demonstrate acceptance while continuing clarification of unit standards and expectations |
From Steele RL: Staff attitudes toward seclusion and restraint: anything new? Perspect Psychiatr Care 29(3):28, 1993. Reprinted by permission of Nursecom, Inc.
Step 2: Establishing rapport and engaging the client
• A simple introductory statement can quickly orient the client to the purpose of the crisis questions and how the information will be used. Health Insurance Portability and Accountability Act (HIPAA) of 1996 regulations require confidentiality. If clients expect family members to give or receive information to health providers when the client is not present, they will need to sign a consent form. Clients in crisis look to health professionals to structure interactions.
• Providing professional support to help the client and family feel more comfortable helps reduce anxiety in crisis situations. Clients and families experiencing a crisis state require a compassionate, flexible, but clearly directive calm approach from nurses. The client should be placed in a quiet, lighted room with no shadows, away from the mainstream of activity.
• Only a minimum number of people should be involved with the client, until he or she is stabilized. If the client is unable to cooperate, for safety reasons, more than one professional may be needed. Ideally, one nurse should be the primary contact for information. Depending on the nature of the crisis and client’s personal responses, family members may be included or asked to return when the client is stabilized. The condition, as well as the preferences of the client, should be determining factors.
• In the early stages of crisis, people need to be listened to, rather than being given elaborate information (Artean & Williams, 1998). It is important to find out the client’s perception of the crisis—how it developed, how it impacts on a person’s life, is this a first encounter with a serious crisis, or one of many that the client has experienced? Questions to assess the client’s perception of the client’s emotional coping strength are important. James (2008) suggests asking question such as “How were you feeling about this before the crisis got so bad?” “Where do you see yourself headed with this problem?” (p. 51).
Let clients tell you what they are experiencing. Listen for facts and associated feelings. Use a reflective listening response to identify applicable feelings (e.g., “It sounds as if you are feeling very sad [angry, lonely] right now.”). You can help clients focus on relevant points by repeating a phrase found in the dialogue, asking for validation of its importance, or asking for clarification to focus further thought. Exercise 21-2 offers an opportunity to understand reflection as a listening response in crisis situations.
Step 3 (assessment): Identifying major problems
The following are guidelines for identifying major problems:
• Ask for a general outline of how the client has experienced the crisis, and note the sequential order of the crisis.
• Keep the focus on the here and now. Questions should be short and relevant to the crisis.
• Request more specific details (e.g., ask who was involved, what happened, and when it happened) if this information is not easily forthcoming from the client.
• Ask about the feelings associated with the immediate crisis.
• Responses to clients should be brief, empathetic, and clearly related to the client’s story.
• Note changes in expression, body posture, and vocal inflections as clients tell their story and at what points they occur.
• Identify central emotional themes in the client’s story (e.g., powerlessness, shame, hopelessness) to provide a focus for intervention.
• Periodically summarize content so that you and your client simultaneously arrive at the same place with a comprehensive understanding of major issues.
Dealing with Feelings
People do not necessarily link a crisis event to their feelings about it. Nurses can call the client’s attention to the linkage by specifically connecting crisis data with observations about client response (e.g., “I wonder if because you think your son is using drugs [precipitating event], you feel helpless and confused [client emotional response], and it seems you don’t know what to do next [client behavioral reaction].”). Checking in with clients helps ensure that your interpretations represent the client’s truth.
Clients in crisis often feel that their emotional reactions to a situation are abnormal because they are intense or uncomfortable. It is helpful to point out that most people will experience a variety of powerful feelings in crisis situations.
Recognizing Personal Strengths
In a crisis, people have a tendency to focus on what is wrong, which stimulates negative thinking patterns. Empowering clients to identify existing personal strengths through compassionate witnessing is an important strategy. Compassionate witnessing is defined as “noticing and feeling empathy for others” (Powley, 2009, p. 1303). When combined with social supports and community resources, compassionate witnessing of personal strengths can significantly enhance coping skills. For example, having a job, financial resources, and knowledge about accessing health care services are critical assets people can use in crisis situations. In the heat of the moment, clients may not recognize their value. Reinforce strengths as you observe them or as the client identifies them. Exercise 21-3 provides an opportunity to experience the value of personal support systems in crisis situations.
Providing Truth in Information
Being truthful about what is known and unknown, and updating information as you learn about it is a critical strategy for building trust with clients in crisis. Explain what is going to happen, step by step. Letting clients know as much as possible about progress, treatment, and consequences of choosing different alternatives allows clients to make informed decisions and reduces the heightened anxiety associated with a crisis situation.
Step 5 (planning): Exploring alternative options and partial solutions
People in crisis often develop tunnel vision (Dass-Brailsford, 2010) and feel they have no resolution of their problem. Finding viable solutions to seemingly impossible problems challenges this assumption, and helping clients to develop targeted alternative strategies increases self-efficacy. Problems not related to the crisis can be handled later.
Clients in crisis generally feel powerless. Nurses can introduce alternative methods that the client may not have considered. Helping a client examine the consequences of proposed solutions and breaking tasks down into small, achievable parts empowers clients. Proposed solutions should accommodate both the problem and client resources. Its helpful to assist clients in discussing the consequences, costs, and benefits of choosing of one action versus another (e.g., “What would happen if you choose this course of action as compared with…?” or “What is the worst that could happen if you decided to…?”).
The locus of control for decision making should always remain with the client to whatever extent is possible. Making autonomous choices encourages clients to become invested in the solution-finding process and hopeful about finding a resolution to a crisis situation.
Involving Social Support Systems
Positive social supports and available community resources act as a buffer to the intensity of a crisis state. Evaluating the availability and ability of a client’s support system to be involved is a critical assessment. Support networks provide practical advice and a sense of security. Equally important, they are a source of encouragement that can reaffirm a client’s worth and help defuse anxiety associated with the uncertainty present in most crisis situations.
Not everyone in a client’s support system holds equal or positive resource value for the client or family. It is important to ask not only about the number and variety of people in the client’s support network, but “who does the client and/or family trust,” and “who would they be most comfortable telling about their situation.” In crisis situations, many clients and families temporarily withdraw from natural support systems and may need encouragement to reconnect.
Step 6 (planning): Developing a realistic action plan
Crisis intervention “is action-oriented and situation focused” (Dass-Brailsford, 2010, p. 56). Formulating a realistic action plan starts with prioritizing identified problems. An effective crisis plan should have a practical, here-and-now, therapeutic, short-term focus and should reflect the client’s choices about best options. Keep in mind the overarching goal of crisis intervention: to restore the functional capabilities of the individuals to their precrisis state.
Introduce consideration of immediate small steps to encourage stabilization. Provide instructions as clearly and simply as possible, explain what is going to happen step by step, and have clients repeat instructions back to you to ensure mutual understanding.
Focusing on the Present
Help your clients to think in terms of short time intervals and immediate next steps (e.g., “What can you do with the rest of today just to get through it better”?) Examples include getting more information, gathering essential data, taking a walk, calling a family member, taking time for self. When people begin to take even the smallest step, they gain a sense of control, and this stimulates hope for future mastery of the crisis situation. Thinking about crisis resolution as a whole is counterproductive.
Incorporate Previously Successful Coping Strategies
People with a record of resiliency and creativity in other aspects of their lives are more likely to weather a crisis satisfactorily. Looking at past coping strategies can reveal skills that can be used in a current crisis situation and offer hope that the current crisis also is resolvable. Ask, “What do you usually do when you have a problem?” or “To whom do you turn when you are in trouble?”
Explore the nature of tension-reducing strategies the client has used in the past (e.g., aerobics, Bible study, calling a friend). If the client seems immobilized and unable to give an answer about usual coping strategies, the nurse can offer prompts such as “Some people talk to their friends, bang walls, pray, go to church…” Usually, with verbal encouragement, clients begin to identify successful coping mechanisms, which can be built on, for use in resolving the current crisis.
Step 6 (implementation): Developing an action plan
Developing realistic goals is a critical component of crisis intervention. This process includes becoming aware of choices, letting go of ideas that are toxic or self-defeating, and making the best choice among the viable options. Goal-directed activities should reflect the client’s strengths, values, capabilities, beliefs, and preferences.
Achievable goals give clients and families hope that they can get to a different place with their emotional and physical pain. Goals that have meaning to the client are more likely to be accomplished. Crisis offers clients an opportunity to discover and develop new self-awareness about things that are important to them and skills.
Designing Achievable Tasks
Help clients choose tasks that are within their capabilities, circumstances, and energy level. Achievable tasks can be as simple as getting more information or making time for self. You can suggest, “What do you think needs to happen first?” or “Let’s look at what you might be able to do quickly.” Engaging clients in simple problem solving can help with crisis-related feelings of helplessness and hopelessness. Problem-solving tasks that strengthen the client’s realistic perception of the crisis event, incorporate a client’s beliefs and values, and integrate social and environmental supports offer the best chance for success. Greene, Lee, Trask and Rheinscheld (2005) suggest that helping clients tap into and use their personal resources to achieve goals facilitates crisis resolution and provides individuals with tools for further personal development.
Providing Structure and Encouragement
Clients need structure and encouragement as they perform the tasks that will move them forward. Making a commitment to achieve a small task related to crisis resolution helps clients see crisis resolution as a process they can master and stimulates hope. Setting time limits and monitoring task achievement is important.
Resolving a crisis state is not experienced as only steady movement forward. There will be setbacks. Clients need ongoing affirmation of their efforts. Supportive reinforcement includes validation of the struggles clients are coping with, anticipatory guidance regarding what to expect, the normalcy of ambivalent feelings, uncertainty, and discussion of fears surrounding the process. Comparing current functioning with baseline admission presentations helps nurses and their clients mutually evaluate progress, foresee areas of necessary focus, and measure achievement of treatment goals.
Providing Support for Families
Part of crisis intervention strategies includes providing support for family members. Crisis for the family can be experienced collectively as a direct strike in a disaster, or as a secondary individual response to the illness or injury of a family member. Family members supporting individuals in crisis are coping not only with the acute emotional fallout brought about by the client’s crisis, but with the management of an unstable home environment created by the client’s absence or inability to function in previous roles. There may be legal or safety issues that family members have to address.
Bluhm (1987) suggests an image of a family in crisis as “a group of people standing together, with arms interlocked. What happens if one family member becomes seriously ill and can no longer stand? The other family members will attempt to carry their loved one, each person shifting his weight to accommodate the additional burden” (p. 44).
Individual family members will experience the crisis in diverse ways, so different levels of information and support will be required. Giving families an opportunity to talk about the meaning of the crisis for each family member, and offering practical guidance about resources they can use to support the client and take care of themselves are important strategies nurses can use with families. Communication strategies the nurse can use to help families in crisis are presented in Box 21-1.
Step 7 (evaluation): Developing a termination and follow-up protocol
Kavan, Guck, and Barone (2006) note, “Follow up provides patients with a lifeline and improves the likelihood that they still follow through with the action plan (p. 1164). All clients should receive verbal instructions, and written discharge or follow-up directives, with phone numbers to call for added help or clarification. Although acute symptoms may subside with standard crisis intervention strategies, some clients will need follow-up for residual clinical issues. Many agencies include a follow-up call to the client or family to check on how things are going after crisis discharge.
Mobilizing resources in the community often is necessary in helping clients maintain continued mastery of health care situations. Community agency resources can provide clients with essential supports. An important piece of assessment data is whether the client is willing to use outside resources, and if so, which ones. Some clients are reluctant to use social services, medications, or mental health services, even short term, because of the stigma they feel about their use. Nurses can help clients and families sort out their concerns, assess their practicality, and develop viable contacts.
If indicated, nurses can facilitate the referral process by sharing information with community agencies and by giving clients enough information to follow through on getting additional assistance. Having written referral information available regarding eligibility requirements, location, cost, and accessibility can make a difference in compliance. Exercise 21-4 provides an opportunity to practice crisis intervention skills.
Mental health emergencies
Mental health emergencies present significant challenges for nurses. Whether encountered in the community or admitted to an emergency department, these clients often present as a danger to themselves or others. These clients present with chaotic distress behaviors, which are not under the client’s control. Many communities have trained first responders in methods of dealing with individuals experiencing psychiatric crisis and have crisis response teams.
The client who presents as a mental health emergency is generally unable to participate in his or her care. Although mental health emergencies share some similarities with other types of crisis, they usually require a higher, more immediate level of assessment and intervention to protect the client from harming himself or others. Examples of a mental health emergency include suicidal, homicidal, or threatening behavior, self-injury, severe drug or alcohol impairment, and highly erratic or unusual behavior associated with serious mental disorders. Nurses can find it difficult to tolerate the intensity of the relationship associated with mental health emergencies.
Myer (2006) describes a triage assessment system (TAS) for mental health crises that can help nurses understand a client’s responses across 3 domains: affective, behavioral, and cognitive. He suggests that clinicians identify the primary affective reaction, for example, anger, fear, or sadness. Next the client’s behavioral reaction is assessed related to mobility, avoidance, or approach. The client’s immediate perception of a transgression, threat, or loss in relation to the crisis event constitutes the cognitive domain. Treatment should focus on the most severe reaction.
This is where you should begin. Think about what the client sees. Remember that although defensive behaviors seem threatening, usually these clients feel vulnerable. Clients may feel they are in acute danger. They are not in control of their behavior or capable of logical reasoning. Keep communication short, compassionate and well defined. Do not be intimidated, but avoid intimidation. Find out where the fear is coming from. Go slow and avoid sudden movements. Box 21-2 provides de-escalation tips developed by Scott Davis of the Montgomery Police Department (2010) for use with clients presenting in the community with mental health emergencies.
Clinicians need to be respectful and avoid traumatizing individuals who are already experiencing a chaotic, distressed state. Patient-centered care requires assessment and treatment approaches that are compassionate, and as acceptable to the client as is possible. Whenever possible, offer simple choices with structured coaching.
Psychiatric emergency clients usually require medication for stabilization of symptoms and close supervision. Whereas crisis intervention represents a short-term response, a mental health emergency requires an immediate coordinated response designed to alleviate the potential for harm and restore basic stability.
Types of mental health emergencies
Callahan (1998) identifies three types of mental health emergencies in health care: violence, suicide, and psychosis.
Violence
Violence is a mental health emergency that can create a critical challenge to the safety, well-being, and health of the clients and others in their environment. Officer Scott Davis, crisis intervention team coordinator with the Montgomery County Police Department shares a field expedient tool, using the acronym “DANGEROUS PERSON” (Box 21-3), to assess dangerousness to self or others in clients presenting as mental health emergency.
Nurses should assume an organic component (drugs, alcohol, psychosis, or delirium) underlying the aggression in clients presenting with disorganized impulsive or violent behaviors, until proven otherwise. Violent clients must be stabilized immediately for the protection of themselves and others. Perry and Jagger (2003) advise that at least two health care providers should be present at the bedside for all procedures if the client is suicidal, delirious, or under the influence of drugs or alcohol.
The client’s body language often offers the nurse clues to escalating anxiety, which can end in violent behavior if left unchecked. Table 21-3 presents characteristic indicators of increasing tension leading to violence. A history of violence, childhood abuse, substance abuse, mental retardation, problems with impulse control, and psychosis, particularly when accompanied by command hallucinations, are common contributing factors.
TABLE 21-3
Behavioral Indicators of Potential Violence
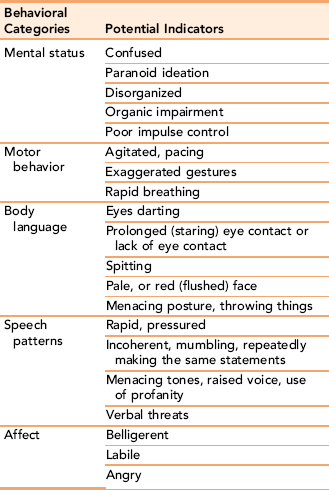
Data from: Keely B: Recognition and prevention of hospital violence. Dimens Crit Care Nurs, 21(6): 236-241, 2002; Luck L, Jackson D, Usher K. STAMP: components of observable behaviour that indicate potential for patient violence in emergency departments. Journal of Advanced Nursing. 59(1): 11-19, 2007.
Treatment of violent clients consists of providing a safe, nonstimulating environment for the client. Often clients calm down if taken to an area with less sensory input. The client should be checked thoroughly for potential weapons and physically disarmed, if necessary. Short-term medication is usually indicated to help defuse potentially harmful behaviors.
Communication strategies to defuse violent behaviors are useful adjuncts to treatment, and can prevent escalation of violent behavior. The nurse can use simple strategies such as calling the client by name; using a low, calm tone of voice; or presenting a show of force if necessary to help the client defuse tension. Encouraging the client to physically walk and to vent emotions verbally can be helpful.
Organically impaired clients may perceive necessary medical procedures as being intrusive and threatening. Perry and Jagger (2003) advise that, before you start any procedure, you should tell the client exactly what you are going to do and why the procedure is necessary, with a request to cooperate. If the client refuses, don’t insist, but explain the reason for doing the procedure in a calm, quiet voice. If you help your client regain a sense of control, he or she will be more likely to cooperate with you. Your movements should be calm, firm, and respectful.
Suicide
Suicide is the ultimate personal crisis. People turn to suicide as an option in times of acute distress, when under the influence of drugs, or when they believe there are no other alternatives. A major goal in evaluating suicidal risk is to assess whether the client is in imminent danger of doing harm to self (Stellrecht, Gordon,Van Orden et al., 2006).
It is a myth that people who talk about harming themselves are at less risk. Every suicidal statement, however indirect, should be taken seriously. Even with clients who have indicated that they are “just kidding,” the fact that they have verbalized the threat places them at greater risk. Verbal indicators of potential suicide include statements such as “I don’t think I can go on without …” “I sometimes wish I wasn’t here,” or “People would be better off without me.” Less direct indicators include statements like “I don’t see anything good in my life.” Any of these statements requires further clarification (e.g., “You say you can’t go on any longer. Can you tell me more about what you mean?”).
• Are you thinking of hurting yourself? (include frequency and intensity of thoughts)
• Do you have a plan? (If the person indicates a plan, additional inquiry about the methods and availability of the method is needed.) Inquiring if the client has a plan is essential. Individuals with a detailed plan and the means to carry it out are at greatest risk for suicide, particularly if they do not have a reliable support system. In assessing the lethality of the plan, inquire about the method, and the client’s knowledge and skills about its use (Roberts, Monferrari, & Yeager, 2008).
• What do you hope to accomplish with the suicide attempt? (look for hopelessness, including severity and duration)
• Have you thought about when you might do this? (immediate vs. chronic thinking)
• Who are you able to turn to when you are in trouble? (social support)
Behavioral indicators of escalating suicidal ideation include giving away possessions, apologizing for previous bad behaviors, writing letters to significant people, intense sharing of personal data from people who do not normally share with others, and frequent accidents.
Irrational behaviors, drug and alcohol abuse, previous suicide attempts, and verbal threats are matters of concern, as is a sudden mood change, especially if the client demonstrates much more energy. Clients with certain mental illnesses such as bipolar disorder or schizophrenia with command hallucinations are more at risk. Antisocial and borderline personality disorders are associated with increased suicide attempts. Suicide rates are greater for older adults, especially for white men, and among adolescents, particularly male African Americans. Men are more likely to complete suicide, whereas more women attempt suicide (American Psychiatric Association, 2003). Clients who verbalize or behaviorally demonstrate “a weight being lifted off the shoulders” should be watched carefully.
Other high-risk factors include:
Most clients are ambivalent about ending their life and experience relief that the decision has been taken out of their hands. Introduce the idea of psychiatric evaluation after disclosure of suicidal ideation in a calm, compassionate manner with a simple statement: “I’m worried that you might harm yourself because of how you say you are feeling right now. You have several of the factors that place you at high risk for suicide. I would like you to see Dr. Jones for an evaluation.”
Stabilization and safety of the client is the most immediate concern with clients experiencing suicidal crisis. Clients exhibiting high-risk behaviors require one-to-one constant staff observation, and a potentially suicidal client should never be left alone. Possible weapons (e.g., mirrors, belts, knitting needles, scissors, razors, medications, clothes hangers) should be confiscated. When taking these items, explain in a calm, compassionate manner the general reason why the items should not be in the client’s possession, and where they will be kept. The client needs to be compassionately informed of the reason unsafe items are being removed. They need to be assured that the items will be returned when the danger of self-harm resolves.
Documentation of the suicidal risk assessment, interventions, and client responses is essential. Included in the documentation should be any quotes made by the client, details of observed behavior, review of identified risk factors, and client responses to initial crisis intervention strategies. The names and times of anyone you notified and contacts with family should be incorporated in the narrative note. These data provide direction for future clinicians involved in the client’s care. The Joint Commission requires that any death that is not consistent with a client’s disease process or any permanent loss of function occurring as a consequence of an attempted suicide in a hospital be reported as a sentinel event (Captain, 2006).
Most inpatient settings have written suicide precaution protocols that must be followed with clients presenting with suicidal ideation. Observational monitoring of acutely suicidal clients ranges from constant 1:1 observation, to 15- or 30-minute observational checks. Less restrictive checks can include supervised bathroom, unit restriction or restriction to public areas, and supervised sharps (Jacobs, 2007). The frequency and type of observation is dependent on the suicidal assessment of the client.
After the initial focus of suicide intervention on stabilizing acute distress, helping the client identify triggers, and understand the reasons that led to suicidal ideation and/or suicide attempt becomes important. Helping people reestablish a reason for living and getting others involved as a support system are critical interventions.
Acceptance of the client is a critical element of rapport. Nurses need to explore their own feelings about suicide behaviors as the basis for understanding the client in danger of self-injury. Consistent with a high risk for suicidal behavior is a sense of hopelessness, lack of meaningful connection with others, and the feeling of being a burden to others (Stellrecht et al., 2006).
Speak slowly, gently, and clearly. Once the client’s suicidal behaviors and feelings are brought under control, the crisis interventions presented earlier in the chapter can be instituted. Suicidal ideation waxes and wanes, so careful observation is critical even after the acute crisis has subsided. Captain (2006) suggests reassessing a client’s suicidal intent every shift, using a 10-point scale and asking the client to “rate your level of suicidal intent on a 0-to-10 scale, with 0 meaning no thoughts of suicide and 10 meaning constant thoughts of suicide” (p. 47). Assessments should be repeated any time changes in behavior are noted and again before discharge.
Crisis Intervention with Psychotic Clients
A psychotic break in which a client is threatening harm to self or to others, is out of touch with reality, or is responding to hallucinations represents a serious mental health crisis. Acutely psychotic and delirious clients have disorganized thinking, reduced insight, and limited personal judgment. The individual is experiencing severe distress and is unable to manage himself or herself. Medication is usually indicated to manage psychotic symptoms.
The florid behavior symptoms associated with psychosis can be frightening for both nurse and client. Nurses should recognize the existence of the client’s feelings and perceptions, even if the logic for their existence is not well understood. Psychotic clients do better in a quiet, softly lighted room, with no shadows, and out of the mainstream. One-to-one supervision usually is required for clients experiencing a psychotic break. Allow the client sufficient space to feel safe, and never try to subdue a client by yourself. Remain calm and positive. An open expression, eye contact, a calm voice, and simple concrete words invite trust. Do not use touch, as it can be misinterpreted.
Crisis management
Disaster and mass trauma situations
A disaster is defined as “a calamitous event of slow or rapid onset that results in large-scale physical destruction of property, social infrastructure, and human life” (Deeny & McFetridge, 2005, p. 432). Recent years have borne witness to more unprecedented natural disasters, terrorism, and barbaric war than the world has seen in many decades. The September 11th terrorist attack on the World Trade Center in 2001, the Oklahoma City bombing, and the devastation of Hurricane Katrina, which demolished a thriving city in a matter of days, stimulated a fresh awareness of the need for community and national planned responses to mass trauma events that can happen anywhere, and at any time, to innocent masses of people. Webb (2004) identifies the components of mass trauma events in Table 21-4.
TABLE 21-4 Assessing Elements of Mass Trauma Events Rights were not granted to include this table in electronic media. Please refer to the printed book. From Webb N: The impact of traumatic stress and loss on children and families (p. 6.). In Webb N, editor: Mass trauma and violence: helping families and children cope, New York, 2004, The Guilford Press. Reprinted by permission. Webb N
Myer and Moore (2006) note, “Crises do not happen in a vacuum, but are shaped by the cultural and social contexts in which they occur” (p. 139). From the perspective of its victims, terrorism is a random event, which reinforces insecurity, creates lingering anxiety, and increases avoidant behaviors around potential risks. The idea of a reciprocal relation between social forces and disaster crisis is supported by the Institute of Medicine (2003).
Planning for disaster management
In the United States, The Federal Emergency Management Agency (FEMA) is responsible for setting forth recommendations related to creating an effective disaster plan (Hendriks & Bassi, (2009). FEMA recommendations provide guidelines for the creation of local disaster planning teams. Community-based governments and businesses, first responders, hospitals, and health providers are expected to be actively involved in community disaster planning. Around the globe, tsunamis in Indonesia, earthquakes occurring in rapid succession in China, Iceland, and South America, the threat of nations developing nuclear weapons, pandemic flu, and severe acute respiratory syndrome (SARS) remind us of a global approach to emergency preparedness.
Strategies for creating and sustaining community-wide emergency preparedness are published by the Joint Commission (2003), which states, “It is no longer sufficient to develop disaster plans and dust them off if a threat appears imminent. Rather, a system of preparedness across communities must be in place everyday” (p. 5). Disaster planning can act as a deterrent to terrorist activity, as well as immediate resource in a disaster situation.
Disaster intervention protocols
Disaster intervention protocols focus on treating injury and acute illness, rather than chronic health conditions (Spurlock, Brown, & Rami, 2009). Crisis intervention responses to mass violence and disaster are quite distinct from treating individual traumas and crisis. Interventions must be embedded in community systems, and must be consistent with societal norms and available resources.
Disaster management requires providing immediate physical and emotional first aid. Instead of initially eliciting details of the experience, Everly and Flynn (2006) stress promotion of adaptive functioning and stabilization as a first response. They use the acronym BICEPS, which stands for brevity, immediacy, contact, expectancy, proximity, and simplicity to describe the type of psychological first aid needed in mass disaster situations.
Noji (2000) identifies four goals to guide disaster management:
• Assess the needs of disaster-affected populations.
• Match available resources to those needs.
• Prevent further adverse health effects; implement disease-control strategies for well-defined problems.
• Evaluate the effectiveness of disaster relief programs and improve contingency plans for various types of future disasters.
Any declared disaster situation affects individuals differently.
Critical incident debriefing
Disasters, deliberate violence, and terrorist attacks are random events producing permanent changes in people’s lives and shaking their perception of being in charge of their lives. Everly and Mitchell (2000) use the term critical incident to describe “an event, which is outside the usual range of experience and challenges one’s ability to cope” (p. 212).
Critical incident debriefing is a type of crisis intervention used to help a group of people who have witnessed or experienced a mass trauma event process its meaning and talk about feelings that otherwise might not surface. The debriefing is designed to help the people directly involved in witnessing or caring for victims and survivors process first the facts and then the feelings associated with a traumatic or critical incident.
The process should allow for free expression of feelings, including guilt, anxiety, and anger. Guided mutual sharing of the crisis experience increases empathy and understanding of its meaning. The debriefing team teaches about the nature of distress reactions and offers helpful hints to mitigate their effects (Dietz, 2009).
The debriefing is conducted as a highly structured group intervention, which is held as soon as possible after the critical incident. The goal of critical incident debriefing is to lessen the symptoms of traumatic stress associated with a sudden crisis or trauma. The debriefing allows the people involved in a traumatic situation to achieve a sense of psychological closure. Although the critical incident will not be forgotten, people are better able to let go of its horror, which increases their potential for a return to normal life for individuals, communities, and organizations. Contact information for the group leader and possible referrals for further intervention should be provided.
Critical Incident Stress Debriefing Process
A specially trained professional generally leads the debriefing. Only those actively involved in the critical incident can attend the debriefing session.
The leader introduces the purpose of the group and assures the participants that everything said in the session will be kept confidential. People are asked to identify who they are and what happened from their perspective, including the role they played in the incident. After preliminary factual data are addressed, the next step is to explore feelings. The leader asks participants to recall the first thing they remember thinking or feeling about the incident. Participants are asked to discuss any stress symptoms they may have related to the incident. The final discussion focuses on the emotional reactions associated with the critical incident. This part of the session is followed by psycho-educational strategies to reduce stress. Any lingering questions are answered, and the leader summarizes the high points of the critical incident debriefing for the group (Rubin, 1990).
Critical incident debriefing is a useful strategy with families witnessing a tragedy involving one of their family members, for children and adolescents dealing with the death of a classmate, mass murders, or environmental disasters. A critical incident stress debriefing offers people an opportunity to externalize a traumatic experience through being able to vent feelings, discuss their role in the situation, develop a realistic sense of the big picture, and receive peer support in putting a crisis event in perspective (Curtis, 1995).
Critical Incident Debriefing for First Responders and Health Care Providers
Critical incidents in health care affect the personnel who respond to them. If there is no opportunity to process the meaning of a critical situation, an involved health care provider can become a psychological casualty. Research indicates that individuals, including health care providers who assist or witness critical incidents, are vulnerable to experiencing “secondary traumatization” similar to that experienced by direct survivors of the incident. Principles of critical incident debriefing can also be applied to strengthen the emotional coping skills of staff working in clinical settings on units with frequent or unexpected loss (Dietz, 2009).
Because of their magnitude, disasters present a more complicated coping process for family survivors and the community at large (Flannery, 1999). Survivors of disaster experience personal crisis response patterns similar to those described earlier in the chapter. In addition, they can experience what Lahad (2000) terms “breaks in continuity.” He suggests that victims, their families, and those secondarily exposed to a disaster are subject to a sudden, serious break in their belief in the continuity of their personal lives that is difficult to ease. The break in continuity occurs in four spheres:
• I don’t understand what is happening (cognitive continuity).
• I don’t know myself (historical continuity).
• I don’t know what to do, how to act here, what it is to be a bereaved person/an injured or wounded person (role continuity).
• Where is everyone? I am so alone. Where are my loved ones? (social continuity).
The experience of trauma from a disaster or terrorist event varies in intensity and impact for survivors. Each survivor brings to the experience a unique personal history, interpersonal strengths, and deficits. Each will interpret the meaning of the crisis differently. Individual, family, and community beliefs about a disaster’s cause and meaning influence each person’s response. Past experience with trauma makes a person more vulnerable to future impairment with traumatic situations (Maguen, Papa, & Litz, 2008). Having limited resources, lack of social support, or mental illness creates additional stress. The level of direct involvement, degree of uncertainty about outcome, nature of the loss, and personal resiliency of the individual and family also affects the impact of the trauma or disaster event, both short and long term. Client needs and individual service delivery requirements will also vary across the entire recovery period.
Another variable in crisis management is culture. Culture plays a role in how a crisis situation is interpreted, and the best means by which people and communities can be helped. Understanding and accepting cultural differences is an important dimension of helping to restore people to their precrisis level of functioning (Dykeman, 2005).
Community response patterns
The Joint Commission (2003) explicitly portrays disaster management and emergency preparedness as a community responsibility. When disaster strikes, the existence and function of the community are significantly impaired, and even in danger of extinction. Initially people are confused and stunned. Emotions vary as the extent of the impact is realized. The closer the person is to the crisis event, the more intense is the impact (Myer & Moore, 2006). The immediate concern is protection of self and those closest to them. The community response to disaster characteristically consists of four phases:
The shock of the disaster pulls people together. Emergency medical teams, neighbors, and friends rally around the survivors, offering emotional support and tangible supplies needed for recovery. The honeymoon phase occurs when the “community pulls together and outside resources are brought in” after an initial search and recovery phase (Bowenkamp, 2000, p. 159). This phase typically lasts up to 6 months after disaster. The focus of intervention is to ensure the public health safety of the victims. Establishing an infrastructure to support the immediate needs of the population related to water, sanitation, food supplies, and insect and rodent control are essential services (Campos-Outcalt, 2006). Sharing the experience of the trauma with others and having tangible evidence of continuing support are crucial components of effective response.
The disillusionment phase usually appears as the initial emergency response starts to subside. The “shared community” feeling starts to leave as people begin to realize the extent of their losses and the limitations of external support. Survivors can experience anger, resentment, and bitterness at the loss of support, particularly if it is sudden and complete. Kaplan, Iancu, and Bodner (2000) suggest that opportunities for psychological debriefing sessions should continue for a period well beyond the initial disaster experience for victims of extreme stress.
The final reconstruction phase occurs when the survivors begin to take the primary responsibility for rebuilding their lives. This period can last for several years after a disaster. Ongoing support is required as survivors learn to cope with new roles and responsibilities, and to develop new alternatives to living a full life after trauma. Although the disaster experience recedes in memory, it is never lost, and the person may never again fully trust in the continuity of life and being in control of one’s destiny. Kaminsky, McCabe, Langlieb, and Everly (2007) describe recovery from the clinical distress, impairment, and dysfunction associated with terrorism and mass disaster as evidenced in the ability to adaptively function psychologically and behaviorally.
Disaster management in health care settings
In 2006, the Joint Commission added new standards for credentialing volunteer health care professionals in declared emergency situations. All hospitals are required to form disaster committees composed of key departments within the hospital, including nursing. That committee is charged with developing disaster plans and implementing practice with them at least twice a year. A rapid credentialing process must be in place. Nurses interested in emergency volunteer activities should become aware of credentialing requirements to ensure their participation as part of a national emergency volunteer system for health professionals.
The Uniform Emergency Volunteer Health Practitioners Act (UEVHPA) provides consistent standards designed to facilitate organized response efforts among volunteer health practitioners in declared emergencies, disaster relief, and public health crisis situations (National Conference of Commissioners on Uniform State Laws, 2006).
Hospital and community disaster planning must be coordinated so that all phases of the disaster cycle are covered. Designated hospital personnel must receive training to carry out triage at the emergency department entrance. Protocols should contain the capability to relocate staff and clients to another facility if necessary, and a plan must be in place detailing mechanisms for equipment resupply. Policies regarding notification, maintenance of accurate records, and establishment of a facility control center are required.
Citizen Responders
Unsolicited responders will play a large role in sudden onset, large scale disasters. Auf der Heide (2006) suggests that emergency plans should anticipate the presence of unsolicited responders and have an infrastructure for coordinating their efforts. Public education related to the citizen role in disaster management is essential.
Citizen Corps Programs, developed by FEMA, is a grassroots crisis intervention strategy that can provide community volunteers with a program to develop emergency preparedness and first-aid skills. The Web site (http://www.citizencorps.gov) provides training and tool kits to help improve the on-site care of disaster victims. It also provides links to information for families interested in developing emergency preparedness around the following issues:
• Providing children and family members with family work and cell phone numbers; name and number of neighbor, friend, or relative; emergency 911, fire, poison control, and police number (these should be posted in a conspicuous place).
• Choosing an out of town contact and instructions on how to make contact.
• Choosing a place to meet with other family members in case of emergency.
• Planning for pets, as they are not allowed in emergency shelters.
Family emergency preparedness plans should be updated annually.
Helping children cope with trauma
Children do not have the same resources when coping with traumatic events as adults do. Preexisting exposure to traumatic events and lack of social support increases vulnerability. It is not unusual for children to demonstrate regressive behaviors as a reaction to crisis. Knapp (2010) suggests that using rituals and memorials for children experiencing loss of peers at school is helpful in mitigating trauma impact. Having a place where children can bring flowers and other mementos commemorating their peer’s death is important.
Children will look for cues from key adults in their lives and tend to mirror their adult caregivers, so it is essential to communicate calm and confidence. More than anything else, children need reassurance that they and the people who are important to them are safe. Encourage the family to maintain regular routines. Parents need to provide children with opportunities both to talk about crisis and to ask questions. Repetitive questions are to be expected. Often they reflect the child’s need for reassurance. Offering factual information helps dispel misperceptions.
Helping older adults cope with trauma
Functional limitations associated with compromised physical mobility, diminished sensory awareness, and preexisting health conditions can create special issues for older clients impacted by a disaster. Older adults have more injury and greater disaster-related deaths than adults in other age groups (Fernandez, Byard, Lin, Benson, & Barbera, 2002). Especially vulnerable are house bound and socially isolated individuals. Other population groups needing extra attention are those who require medical or nursing care, and those receiving services, care, or food from health, social, or volunteer agencies.
Disaster management for older adults needs to be proactive. The following core actions can make a difference in helping older adults weather a disaster event successfully. Proactive planning includes:
• Identify a support network that can be used in an emergency situation. Facilitate connections with social support systems and community support structures. Have this information readily available for use in an emergency situation.
• Older adults with a disability should wear tags or a bracelet to identify their disability. Keeping extra eyeglasses and hearing aid batteries on hand, and identifying any assistive devices is essential.
• Identify the closest special needs evacuation center.
• Develop a written list of all medications, with any special directions, for example, crushing pills, hours of administration, and dietary restrictions.
• Identify physicians and social support contacts, including someone apart from people in the local area who can be contacted.
Other actions, such as ensuring the safety, meeting mobility needs, and medication administration, will need careful attention during the course of actual disaster management. Even the most capable older adult can appear confused and vulnerable in a disaster situation. Reducing anxiety is especially important for the older adult disaster victim. Actions nurses can take include the following:
• Initiate contact and take the older adult to as safe a place as possible.
• Speak calmly and provide concrete information about what is happening, and what you need the older adult to do in simple terms.
• Assess for mobility and provide assistance where needed.
• Older adults may need warmer clothing because of compromised temperature regulation.
Summary
Crisis is defined as an unexpected, sudden turn of events or set of circumstances requiring an immediate human response. People experience a crisis as overwhelming, traumatic, and personally intrusive. It is an unexpected life event challenging a person’s sense of self and his or her place in the world. The most common types of crisis are situational and developmental crises. Most health crises are situational. Crisis can be private involving one person, or public involving large numbers of people. James (2008) describes two additional types of crisis: existential and ecosystem crisis.
Theoretical frameworks guiding crisis intervention include Lindemann’s (1944) model of grieving, derived from his clinical work with survivors of a nightclub fire. Caplan’s (1964) model is based on preventive psychiatry concepts. Aguilera’s nursing model explores the role of balancing factors in defusing the impact of a crisis state. Erikson’s (1982) model of psychosocial development forms the basis for developmental crisis.
Crisis intervention is a time-limited treatment that focuses only on the immediate problem and its resolution. Roberts’ (2005) seven-stage model is used to guide nursing interventions: assessing lethality, establishing rapport, dealing with feelings, defining the problem, exploring alternative options, formulating a plan, and follow-up measures. The goal of crisis intervention is to return the client to his or her precrisis level of functioning.
Mental health emergencies require immediate assessment interventions and close supervision. The most common types are violence, suicide, and a psychotic break. Guidelines for communication with clients experiencing mental health emergencies (e.g., violence and suicide) focus on safety and rapid stabilization of the client’s behavior.
As the world becomes more dynamically unstable, nurses will need to understand the dimensions of disaster management and develop the skills to respond effectively in disaster situations. Disaster management is a special kind of crisis intervention applied to large groups of people. The Joint Commission (2003) requires hospitals to develop and exercise disaster management plans at regular intervals. Critical incident debriefing is a crisis intervention strategy designed to help those closely involved with disasters process critical incidents in health care, thereby reducing the possibility of symptoms occurring.
References
Aguilera, D. Crisis intervention: theory and methodology, ed 7. St Louis: Mosby, 1998.
American Psychiatric Association. Practice guidelines for the assessment and treatment of patients with suicidal behaviors. Arlington, VA: American Psychiatric Association, 2003.
Artean, C., Williams, L. What we learned from the Oklahoma City bombing. Nursing. 1998;28(3):52–55.
Auf der Heide, E. The importance of evidence-based disaster planning. Ann Emerg Med. 2006;47(1):34–49.
Bowenkamp, C. Coordination of mental health and community agencies in disaster. Int J Emerg Ment Health. 2000;2:159–165.
Boyd, M.A. Psychiatric nursing: contemporary practice, ed 4. Philadelphia: Wolters Kluwer Health/Lippincott Williams & Wilkins, 2008.
Bluhm, J. Helping families in crisis hold on. Nursing. 1987;17(10):44–46.
Callahan, I. Crisis theory and crisis intervention in emergencies. In: Kleespies P.M., ed. Emergencies in mental health: evaluation and management. New York: Guilford Press, 1998.
Campos-Outcalt, D. Disaster medical response: maximizing your effectiveness. Fam Pract. 2006;55(2):113–115.
Caplan, G. Principles of preventive psychiatry. New York: Basic Books, 1964.
Caplan, G. Recent developments in crisis intervention and the promotion of support service. J Prim Prev. 1989;10(1):3.
Captain, C. Is your patient a suicide risk? Nursing. 2006;36(8):43–47.
Curtis, J. Elements of critical incident debriefing. Psychol Rep. 1995;77(1):91–96.
Dass-Brailsford, P. Crisis and disaster counseling: lessons learned from Hurricane Katrina and other disasters. Thousand Oaks, CA: Sage Publications, 2010.
Davis, S. De-escalation tips in crisis situations. Rockville, MD: Montgomery County, MD Police Department; 2010.
Davis, S. Field expedient tool to assess dangerousness in self and others. Rockville, MD: Montgomery County, MD Police Department; 2010.
Deeny, P., McFetridge, B. The impact of disaster on culture, self, and identity: increased awareness by health care professionals is needed. Nurs Clin North Am. 2005;40(3):431–444.
Dietz, D. Debriefing to help perinatal nurses cope with a maternal loss. MCN. 2009;34(4):243–248.
Dirkzwager, A., Kerssens, J., Yzermans, C. Health problems in children and adolescents before and after a man-made disaster. J Am Acad Child Adolesc Psychiatry. 2006;45(1):94–103.
Dykeman, B.F. Cultural implications of crisis intervention. J Instr Psychol. 2005;32(1):45–48.
Erikson, E. The life cycle completed. New York: Norton, 1982.
Everly, G. Five principles of crisis intervention: Reducing the risk of premature crisis intervention. Int J Emerg Ment Health. 2000;2(1):1–4.
Everly, G., Flynn, B. Principles and practical procedures for acute first aid training for personnel without mental health experience. Int J Emerg Ment Health. 2006;8(2):93–100.
Everly, G., Mitchell, J. The debriefing “controversy” and crisis intervention: a review of lexical and substantive issues. Int J Emerg Ment Health. 2000;2(4):211–225.
Fernandez, L.S., Byard, D., Lin, C.C., Benson, S., Barbera, J.A. Frail elderly as disaster victims: Emergency management strategies. Prehospital Disaster Med. 2002;17(2):67–74.
Flannery, R. Treating family survivors of mass casualties: a CISM family crisis intervention approach. Int J Emerg Ment Health. 1999;1(4):243–250.
Flannery, R.B., Jr., Everly, G.S., Jr. Crisis intervention: a review. Int J Emerg Ment Health. 2000;2(2):119–125.
Greene, G., Lee, M., Trask, R., Rheinscheld, J. How to work with strengths in crisis intervention: a solution focused approach. In: Roberts A.R., ed. Crisis intervention handbook. New York: Oxford University Press, 2005.
Hendriks, L., Bassi, S. Emergency preparedness from the ground floor up: a local agency perspective. Home Health Care Manag Pract. 2009;21(5):346–352.
Hoff, L. People in crisis: cultural and diversity perspectives, ed 6. New York: Routledge, Taylor & Francis Group, 2009.
Institute of Medicine, Butler, A.S., Panzer, A.M., Goldfrank, L.R. Preparing for the psychological consequences of terrorism: a public health strategy. Washington, DC: National Academies Press, 2003.
Jacobs, D. Screening for mental health: a resource guide for implementing the Joint Commission on Accreditation of Health Care Organizations (CAHO) 2007 patient safety goals on suicide. Wellesley Hills: Screening for Mental Health Inc, 2007.
James, R. Crisis intervention strategies, ed 6. Belmont, CA: Thomson Brooks/Cole, 2008.
Joint Commission. Health care at the crossroads: strategies for creating and sustaining community-wide emergency preparedness systems. Oakbrook Terrace, IL: Joint Commission on Accreditation of Health Care Organizations, 2003.
Kaminsky, M., McCabe, O., Langlieb, A., Everly, G. An evidence-informed model of human resistance, resilience, and recovery: the Johns Hopkins’ outcome-driven paradigm for disaster mental health services. Brief Treat Crisis Interv. 2007;7(1):1–11.
Kaplan, Z., Iancu, I., Bodner, E. A review of psychological debriefing after extreme stress. Psychiatr Serv. 2000;52(6):824–827.
Kavan, M., Guck, T., Barone, E. A practical guide to crisis management. Am Fam Physician. 2006;74(7):1159–1164.
Keely, B. Recognition and prevention of hospital violence. Dimens Crit Care Nurs. 2002;21(6):236–241.
Kleeman, K. Families in crisis due to multiple trauma. Crit Care Nurs Clin North Am. 1989;1(1):25.
Knapp, K. Children and crises. In: Dass-Brailsford P., ed. Crisis and disaster counseling: lessons learned from Hurricane Katrina and other disasters. Thousand Oaks, CA: Sage Publications; 2010:83–97.
Lahad, M., Darkness over the abyss: supervising crisis intervention teams following disaster. [online article]. Traumatology, 2000;6(4). Available online, http://www.fsu.edu/~trauma/v6i4/v6i4a4.html.
Lindemann, E. Symptomatology and management of acute grief. Am J Psychiatry. 1944;101:141–148.
Luck, L., Jackson, D., Usher, K. STAMP: components of observable behaviour that indicate potential for patient violence in emergency departments. J Adv Nurs. 2007;59(1):11–19.
Maguen, S., Papa, A., Litz, B. Coping with the threat of terrorism: a review. Anxiety Stress Coping. 2008;21(1):15–35.
Michalopoulos, H., Micalopoulos, A. Crisis counseling: be prepared to intervene. Nursing. 2009;39(9):47–50.
Myer, R., Conte, C. Assessment for crisis intervention. J Clin Psychol. 2006;62(8):959–970.
Myer, R.A., Moore, H.B. Crisis in context theory: an ecological model. J Couns Dev. 2006;84(spring):139–147.
National Conference of Commissioners on Uniform State Laws. Uniform Emergency Volunteer Health Practioners Act, 2006. Available online http://www.uevhpa.org/DesktopDefault.aspx?tabindex=1&tabid=55. [Accessed February 16, 2010].
Noji, E.K. The public health consequences of disasters. Prehosp Disaster Med. 2000;15(4):21–31.
Perry, J., Jagger, J. Reducing risks from combative patients. Nursing. 2003;33(10):28.
Powley, E. Reclaiming resilience and safety: resilience in the critical period of crisis. Hum Relat. 2009;62(9):1289–1326.
Roberts, A. Crisis intervention handbook: assessment, treatment and research. New York: Oxford University Press, 2005.
Roberts, A., Yeager, K. Pocket guide to crisis intervention. New York: Oxford University Press, 2009.
Roberts, A., Monferrari, I., Yeager, K. Avoiding malpractice lawsuits by following risk assessment and suicide prevention guidelines. Brief Treat Crisis Interv. 2008;8:5–14.
Rubin, J. Critical incident stress debriefing: helping the helpers. J Emerg Nurs. 1990;16(4):255–258.
Spurlock, W., Brown, S., Rami, J. Disaster care: delivering primary health care to hurricane evacuees. Am J Nurs. 2009;109(8):50–53.
Stellrecht, N., Gordon, K., Van Orden, K., et al. Clinical applications of the interpersonal-psychological theory of attempted and completed suicide. J Clin Psychol. 2006;62(2):211–222. [II].
Webb N.B., ed. Mass trauma and violence: helping families and children cope. New York: Guilford Press, 2004.