Communicating for Continuity of Care
At the end of the chapter, the reader will be able to:
1 Describe current challenges in health care delivery creating the need for continuity of care (COC).
2 Define COC and describe its relational, informational, and management dimensions.
3 Discuss the application of relational continuity concepts: client-centered care, professional collaboration, and team communications.
4 Discuss the application of informational continuity concepts related to discharge planning and handoffs.
5 Discuss the application of management COC concepts related to case management and community advocacy.
Modern clinical practice requires new approaches to health care service delivery, with an emphasis on developing cost-saving coordination of health care delivery for individuals with chronic medical and mental disorders. This chapter provides a framework for exploring communication concepts and relationship strategies within and across health care systems. The chapter describes the concept of continuity of care (COC) and identifies its key components: relational, informational, and management continuity (Haggerty et al., 2003). Applications related to each dimension are discussed.
Basic concepts
Continuity of Care COC provides a new model for describing the coordination and connections required across time, multiple clinical settings, and provider/agencies to effectively manage the health care of individuals with chronic conditions in the community (Sparbel & Anderson, 2000). Developing community-based collaborative models of care related to need assessments, referral, and early intervention will be key to providing quality health care, particularly for youths and seniors as budgets tighten (Tractenberg, 2010).
The World Health Organization (WHO) calls for an emphasis on continuous care by skilled and primary care health teams, rather than on episodic hospital care of seriously ill clients to ensure quality care (Thomas, 2009). The Institute of Medicine (IOM, 2001a) identifies continuity of care (COC) as an essential component of quality primary care. At the core of COC is the therapeutic nurse-client relationship. This relationship serves as a critical communication bridge between clients and their health providers in developing and implementing comprehensive care plans.
Current challenges in health care delivery
The nation’s health care delivery system currently faces major challenges for complex interconnected reasons. The need for health care delivery systems organized around an acute, episodic medical model of care no longer suffices as a primary service model. Needed is a redesign of the health care system to include a prominent emphasis on chronic disease self-management (Thorne, 2008).
Clients today are discharged earlier, have complex medication and treatment regimens, and are seen by different health care providers in multiple care settings. Self-management, family involvement, and shared decision making have become an indispensable means of bridging the gap between diminishing financial support for chronic care and multifaceted health care demands that can last for years. To achieve quality health outcomes with chronic conditions, clients and families must have dependable relationships, accurate information, and ongoing collaborative support from coordinated health services.
Managed care is now the dominant form of health care financing in the United States. The goal of this new system of care reimbursement is to administratively lower costs, while providing quality health care delivery (Lein, Collins, Lyles, Hillman, & Smith, 2003). The bulk of health care is increasingly provided in primary care settings, with acute episodic care reserved for short-term hospital stays. People are better informed, more assertive, and more insistent on prompt access and value for their health care dollar (von Bultzingslowen, Eliasson, Sarvimaki, Mattson, & Hjortdah, 2006).
Other factors such as Healthy People 2010 objectives, growing globalization, a sharp increase in migration of people without health insurance to the United States and Canada, and turbulent economic changes call sharp attention to widespread escalating public health issues and health care disparities. Provider shortages in the health care system, notably physicians and nurses, mandate a search for different and more effective, efficient ways of meeting client health care needs across multiple clinical settings.
Continuity of care for chronic conditions
COC is recognized as an essential component of comprehensive care for individuals with chronic health conditions. WHO (2002) defines chronic health conditions as “health problems that require ongoing management over a period of years or decades” (p. 11). Examples include fibromyalgia, cancer, multiple sclerosis, and serious persistent mental disorders. What chronic conditions share in common is a requirement for ongoing health care management.
Kleinman (1988) describes chronic illness from the client perspective:
The undercurrent of chronic illness is like the volcano: it does not go away, It menaces. It erupts. It is out of control…confronting crises is only one part of the total picture. The rest is coming to grips with the mundaneness of worries…Chronic illness also means the loss of confidence in one’s health and normal bodily processes. (pp. 44–45)
Continuity of care
Sparbel and Anderson (2000) define COC as “a series of connected patient-care events both within a health care institution and among multiple settings” (p. 17). Nurses have an important role in implementing COC as a multidimensional concept, which according to Haggerty et al. (2003) is concerned with the following factors:
• Ensuring accessibility to coordinated health care services
• Personalization of care to meet a client’s changing needs across delivery systems
• Informational data sharing of various elements of personal and medical data electronically over time and place, which contribute to appropriate care delivery
• Health services provided in an organized, logical, and timely manner, using a shared management plan
COC is described as a thread binding together episodes of care, and providing linkages across time, service providers and health care settings (Fletcher et al., 1984).
Dimensions of Continuity of Care
COC is an interdependent systems concept, consisting of three interlocking components: relational, informational, and management continuity. Each is dependent on the others (Schultz, 2009). Relational (interpersonal) continuity occurs through relationships with trusted care providers such that discrete health care events are experienced as being coherent and connected. Informational continuity is achieved through accurate record sharing and frequent team communication. Management continuity is accomplished through case management that can be flexibly adjusted to meet changing client needs in the community (Haggerty et al., 2003).
Relational Continuity: Haggerty et al. (2008) define relational continuity as “a therapeutic relationship with a practitioner that spans more than one episode of care and leads, in the practitioner, to a sense of clinical responsibility and an accumulated knowledge of the patient’s personal and medical circumstances” (p. 118). A sustained relationship between health care providers and clients gives clients confidence that their providers know their circumstances well and are able to coordinate care between different providers and specialists.
Respect for client and family values, beliefs, knowledge, cultural background, and preferences are fundamental aspects of the relational continuity required for planning, delivery, and evaluation of comprehensive reliable care, particularly for chronic health conditions. Client participation offers health care providers unique insights into the context of an illness experience.
Providing health care for individuals with complex health care needs can exceed the energy and expertise of any one provider, even when highly talented. Current health care delivery systems emphasize team functioning in which professionals from different disciplines assume treatment responsibility for a common client population, develop common client-centered treatment goals, and function as a unified entity in providing client-centered care.
Professional team collaboration describes a communication process among health professionals required for promoting coordination of services and resolving complex treatment issues. Increasing the level of collaboration among health care professionals has been identified as one of the best strategies to improve the level of continuity in the health care system (San Martin-Rodriguez, D’Amour, & Leduc, 2008).
Informational Continuity: Communication of complete unbiased information is critical to ensuring safe, reliable care continuity (Kohn et al., 2000). Informational continuity refers to data exchanges among providers and provider systems, and between providers and clients related to care. Informational continuity is what “links provider to provider, and health care event to health care event” (Pontin & Lewis, 2008, p. 1199). As the client’s condition changes, alterations are communicated quickly and accurately.
Sources of informational continuity include multidisciplinary team meetings, progress notes, handoff reporting, discharge plans, referral contacts, and client summaries. The SBAR is a new situational briefing format, which provides critical information about changes in a client’s condition and is used in handoff or discharge/transfer of clients (Leonard, Graham, & Bonacum, 2004).
Management Continuity: Nazareth et al. (2008) define management continuity as “the delivery of health care by several providers in a complementary and timely manner through shared management plans that are consistent and flexible” (p. 570). The expectation is that health and complementary delivery services responsive to client needs will be provided to clients and families in a timely coordinated manner over an extended period. Management continuity represents a longitudinal pattern of health care utilization (Saultz & Albedaiwi, 2004), usually coordinated through case management.
Functionality of Continuity of Care
COC describes the communication bridge between discrete illness episodes and coordination of interventions by different providers to address changes in illness status (Mainous & Gill, 1998). When services are effectively coordinated, there is less potential for duplication of services, conflicting assessments, gaps in service, and decreased use of preventable acute care services. COC reduces medication and treatment errors, provides timely follow-up, and eases transitions between care settings for everyone concerned. Clients and families experience greater satisfaction.
Sharing of clinical activities makes for more holistic interventions (San Martin-Rodriguez, D’Amour, & Leduc, 2008). For chronically ill and elderly clients, COC means that they are more likely to have health care providers familiar with their overall history, who can notice subtle changes in the client’s health status (von Bultzingslowen et al., 2006).
Applications
COC approaches are designed to provide a seamless continuum of care for clients through coordinated, acute, and community-based health services and relationships based on client needs and preferences. Multiple research studies have demonstrated improved clinical outcomes, satisfaction with care, and enhanced quality of life related to COC (van Servellen, Fongwa, & Mockus D’Errico, 2006).
Creating relational continuity
Relational stability is the interpersonal aspect of COC. It is a fundamental communication channel used to guarantee well-coordinated health care service delivery, free from errors and tailored to meet the individual client’s health needs. Interdisciplinary collaboration within a health organization and professional communication across health care systems are essential characteristics of professional relationships.
In today’s health care system, a person’s health care is looked on as the joint responsibility of clients, their families, and professional care providers. Although the emphasis with each health care episode may differ depending on the type and setting of care, the client is always the central focus.
Patient (client)-centered care
The IOM (2001a) defines patient (client)-centered care as “providing care that is respectful of and responsive to individual patient preferences, needs, and values, and ensuring that patient values guide all clinical decisions” (p. 40). Client-centered care is designed to recognize subtle differences among clients having the same diagnosis and cultural experiences, and to incorporate this knowledge into the care of the whole individual (Engebretson, Mahoney, & Carlson, 2008; Hasnain-Wynia, 2006).
Client-centered care requires individualizing nursing interventions based on a person’s values, preferences, and beliefs as the basis for customized clinical decisions (Engebretson et al., 2008; Hasnain-Wynia, 2006). Being attuned to cultural cues about beliefs and values, including attitudes about illness, provider relationships, and the nature of healing helps nurses make better sense of the clinical reality of a client’s illness from the client and family perspective.
Client-centered care supports client autonomy and helps people take control of their health care, to whatever extent is possible. Individual need for full disclosure can vary as the client’s condition changes and is affected by cultural norms. Client-centered care respects the amount of information desired by clients and their families, and to whom it should be provided. Attending to the physical and emotional comfort of the client, providing sufficient information with plenty of time for questions, feedback, and time spent on reducing client or family anxiety about new information are significant aspects of patient-centered care. Box 24-1 identifies IOM guiding principles for providing client-centered care.
Building collaborative partnerships with clients
Well-planned, competently executed, client-centered care results in improved practice efficiency and better client outcomes (Epstein, Fiscella, Lesser & Stange, 2010). . Client-centered care emphasizes partnerships between clients and providers, consisting of following factors:
• Mutual respect for the skills and knowledge of client consumers and the health care team
• Accessibility and respectful empathetic responsiveness to client and family needs
• Shared planning and development of mutually agreed-on goals that reflect the client’s needs, beliefs, values, and preferences
• Frequent evaluation, based on a mutual exchange of information, constructive feedback, and negotiation of care strategies that are empowering and practical.
Family-centered care comes into play when the health needs of children are involved. Family-centered care is more complex. Parents may need help with parenting skills both in handling the needs of a chronically ill child and in providing support and direct care. Box 24-2 offers principles of family-centered care.
Shared decision making
A client-centered care views the client and family as equal partners with providers in negotiating treatment decisions and evaluating treatment outcomes (Engebretson et al., 2008; IOM, 2001b). To ensure that care decisions respect client values, needs, and preferences, health care providers need to: (1) observe and listen carefully; and (2) provide clients and families with the education and support they need to make reasoned decisions, and actively participate in their health care. Full disclosure of information is a prerequisite for effective shared decision making. Relevant information includes:
Relational continuity: professional perspectives
Sheehan, Robertson, and Ormond (2007) differentiate between multidisciplinary and interdisciplinary teams. Professionals on multidisciplinary teams “each work within their particular scope of practice and interact formally. Interdisciplinary teams are characterized by greater overlapping of professional roles, formal and informal communication and shared problem solving for the good of the patient” (p. 18).
Although multidisciplinary teams share information with each other, and work in tandem with other disciplines, they function independently, with each being responsible for different care needs. By contrast, an interdisciplinary team develops a collective vision and common language to support a collaborative unified working approach to clinical problems. An interdisciplinary team actually integrates services, using teamwork principles, whereas on a multidisciplinary team, each profession maintains its own silo of expertise without much interaction (Margalit, Thompson, & Visovsky, 2009).
The interdisciplinary team consists of a core group of health professionals (commonly physician, nurse, social worker, pharmacist, and caseworker). Although each discipline has its central role, integrated client-centered care represents the team’s core value. Decision making is nonhierarchal, with every professional being willing and ready to assume responsibility for achieving positive treatment outcomes (Jansen, 2008).
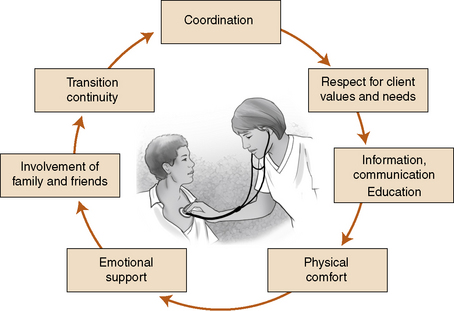
Interdisciplinary team function takes into account the diverse standards and behaviors associated with each clinical discipline, and emphasizes the common mission of working together to resolve complex clinical problems (Clark, Cott, & Drinka, 2007; D’Amour & Oandasan, 2005). Figure 24-1 presents the dimensions of patient centered care.
Each member of the team functions as both an individual and a health care professional representing a distinct discipline. Fundamental to effective participation on an interdisciplinary team is a clear understanding of one’s own discipline, plus a knowledge and mutual respect for each other’s discipline’s roles, professional responsibilities, and expertise (Lidskog, Lofmark, & Ahlstrom, 2007).
Even when core personal and professional values, attitudes, and practices are not at odds with each other, professional training and interpretations of standards can shape how professional values are prioritized (D’Amour & Oandasan, 2005; Hall, 2005). Sparbel and Anderson (2000) identify team role confusion, fueled by professional rivalries, territoriality, and lack of clarification about job responsibilities, as a potential barrier to effective team communication. Exercise 24-1 explores the impact of discovering commonalities in people.
Professional collaboration
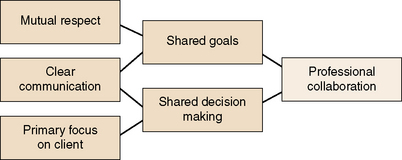
The goal of interprofessional collaboration is to produce “a synthesis of the information such that the outcomes are more than additive” (Muir, 2008, p. 5). Interdisciplinary team collaboration enables practitioners to learn new skills and approaches, and encourages synergistic creativity among professionals. Collaboration decreases fragmentation and duplication of effort and promotes safe quality care (Figure 24-2) presents desired characteristics of professional collaboration.
Team collaboration includes the client as an essential collaborative partner. Within nurse-client relationships, nurses help clients interpret clinical findings, frame important questions about their diagnosis, treatment, or prognosis, and follow through with treatment recommendations.
TeamSTEPPS (Department of Defense, 2009) represents an accepted, evidence-based framework developed jointly by the Agency for Health Care Research and Quality and Department of Defense to guide development and implementation of interdisciplinary team collaboration in health care centers. Competency elements are identified in Box 24-3. Professional collaboration takes place through formally scheduled team meetings, informal huddles, and client comfort rounds.
Team Meetings
Interdisciplinary team collaboration differs from group communication in that team membership, focus of communication, and anticipated outcomes are consistently and solely focused on present moment client needs and solution planning. Team meetings serve the distinct purpose of concentrated discussion about targeted client and family needs, and meeting related treatment goals.
A smoothly run team meeting is one in which the team understands the mission of providing holistic care through defined membership, and where any problem related to client and family care can be worked through to the joint satisfaction of the team and client/family. Wise team leadership and careful attention to member relationships are essential.
The shared goals of client and health care team focus the discussion. Unrelated discussion or focus on routine details or on competing goals are discouraged because they distort or compromise the concentration of the team on key client/family needs and solutions. Time is a precious commodity for busy health care providers, so team meetings begin and end on time. Exercise 24-2 provides an opportunity for students to understand collaboration skills in team decision making.
Huddles
Sometimes an urgent problem arises that cannot wait until the team meets again. Huddles, defined as limited spontaneous or scheduled briefings, allow interdisciplinary team members to meet briefly with each other or with bedside caregivers for the purpose of staying informed, making on-the-spot decisions, and being able to move ahead quickly in rapidly changing health circumstances. Huddles are held more frequently than team meetings, sometimes daily. They typically last no more than 7 to 10 minutes and are convened spontaneously in a convenient location with team members standing rather than sitting close to the site of action (Institute for Healthcare Improvement, 2007).
Sharing Critical information
Leonard et al. (2004) advocate the use of the SBAR format as a succinct way to share critical information with physicians and other team members about sudden changes in a client situation. The statements should contain a concise, convincing statement about the severity of the client’s condition.
Nursing Comfort Rounds
Studies have identified nursing rounds as a way to enhance client-centered care, improve client satisfaction, and enhance client safety (Bourgault et al., 2008; Meade, Bursell, & Ketelsen, 2006). Regular comfort rounds with professional nurses and/or clinical support staff provide opportunities to continuously meet client nonmedical needs and to share information with clients (Castledine, 2002). Common components include assessment of the environment to ensure that equipment is within easy reach of the client, adequate pain management, and attention to personal needs such as repositioning and toileting (Meade et al., 2006).
Role of the hospitalist
A new professional role designed to improve COC in acute care settings is that of the “hospitalist” (Amin & Owen, 2006; Wachter & Goldman, 1996). The hospitalists may be a physician or nurse practitioner employed by the hospital to clinically manage inpatient medical care, with specialty physicians acting as consultants. The hospitalist assumes responsibility for coordinating care, integrating diagnostic test results, making decisions, presenting options to the client and family, and communicating with other professionals who may be or will become involved in the client’s care after discharge. The specific dimensions of the hospitalist role are determined by the care site rather than clinical specialty (Schneller & Epstein, 2006).
Although hospitalists are often the client’s main point of contact throughout the acute hospitalization phase, they may have limited knowledge of the client’s health care patterns before hospitalization. The primary physician may have limited contact with the client during the hospitalization but will be expected to re-engage with the client on discharge.
Nurses have an important communication role with hospitalists. Clients cannot always easily interpret the events related to rapidly changing prognostic changes or treatment options. They are more likely to discuss their concerns regarding particular treatment issues with the nurse during the course of care provision than they are in formal meetings with the health care team. Nurses can and should be proactive in talking informally with physicians about their clients and in contributing data in huddles and team meetings.
Periodically, and or when the client’s condition changes, the hospitalist or entire treatment team may meet with the family to discuss changes, treatment options, and family concerns. Even in the best of circumstances, client/family meetings with the health care team to discuss sensitive health issues such as discontinuing life support or transfer of clients to subacute or community settings with anxious clients and concerned family members can be highly intimidating. Nurses can help clients and families by continuing conversations after the health care team leaves, answering questions and providing support.
Informational continuity
Informational COC allows for an uninterrupted flow of data and clinical impressions between health care providers and agencies, with clients and their families, over time and space. Gaps in informational continuity can occur as a result of misplaced clinical records, inadequate discharge planning or referral data, deficient or delayed authorization for treatment, and lack of understanding by the client of their illness or treatment, or self-management guidelines. Lack of information at time of transfer can result in treatment delays, and can increase the client and/or family’s anxiety unnecessarily. When clients get full information and a consistent message from their health care providers, regardless of where they are in the health care system, they become more relaxed and open to treatment recommendations.
Informational continuity requires sharing health and treatment information and changes with clients and families that are consistent, complete, accurate, value neutral, and delivered in an easily understandable and supportive manner. Notifying the family of changes in the client’s condition or treatment recommendations is an essential part of ensuring informational continuity, particularly if the family is not in close contact with the client.
Handoff care transitions
Communication at transition points in health care takes place in the form of handoffs. Handoffs refer to transfer processes taking place when clients are reassigned to another level of care, for example, from the intensive care unit to a step-down unit, or to a less intensive care facility for continued rehabilitation services. Carr (2008) advises, “Handoffs or care transitions shouldn’t be an abrupt end of care previously provided, but rather considered to be a coordinated changeover for the patient to a new team of involved caregivers” (p. 26). The Joint Commission (2009) mandates timely and accurate transfer of handoff information related to transfer of clients from one unit to another and from one clinical setting to another.
Transitions from one clinical unit to another, and discharge to a different clinical setting provide opportunities for unintentional information gaps (Coleman & Berenson, 2004; Greenwald, Denham, & Jack, 2007). Core functions for transitional sending and receiving teams designed to limit information gaps are presented in Box 24-4.
Documenting transfer information
SBAR is the most commonly used format for communicating pertinent information during handoff transfers and increasingly for shift reports. The format presents a clear, organized picture of a client’s care during a shift or care episode to the different set of health professionals who will be assuming primary responsibility for client care. Mikos (2007) specifies the content information that nurses should include in Box 24-5. Exercise 24-3 provides practice with using the SBAR format.
Discharge planning and referrals
Han, Barnard, and Chapman (2009) use the American Hospital Association (AHA, 1983) definition of discharge planning “as a process of concentration, coordination and technology integration, through the cooperation of healthcare professionals, patients and their families, to ensure that all patients receive continuing care after being discharged” (p. 5).
Discharge planning begins with the client’s admission to the hospital (Birmingham, 2004; Cotera-Perez, 2005). Nurses should educate clients and families about diagnosis and treatment throughout hospitalization, so that by the time the client is discharged, the client and family have a full understanding of the client’s condition as a basis for follow-up care.
Assessment of Postdischarge Needs
Much of the care previously provided in acute care settings for clients has shifted to the home care environment (Cooke, Gemmill, & Grant, 2008). In the community, professional team care will involve interactions separated by both time and space.
Many clients/caregivers will require specific instruction in treatment-related tasks to successfully self-manage health problems at home. Arrangements and/or referrals for essential training needs should be implemented before discharge, if possible. Table 24-2 presents some of the key elements needed to plan for a successful transition from the hospital to the client’s home.
TABLE 24-2
Key Elements in Planning for Successful Transitions
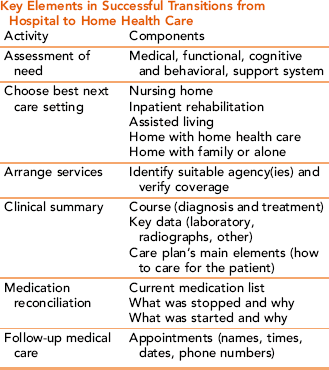
Data from: Boling P: Care transitions and home health care, Clin Geriatri Med 25:135–148, 2009.
Not all clients are discharged back to their home. Clients with complex disability or care needs may need to be discharged to a subacute or transitional skilled nursing facility for extended care. As soon as this is known, the client and the family need to be informed of the need for transfer and what parameters for discharge will be used for each client (Joint Commission, 2009). Recommendations for transfer should be thoroughly discussed with the family and included in the client’s treatment plan. The goal of discharge planning is to provide clients and their families with the level and kind of information they will need to secure their recovery and/or maintain health status during the immediate posthospital period.
Clients may have multiple care transitions as part of their experience after discharge from a hospital setting (Boling, 2009). Frequent communication and careful coordination are keys to ensuring safe, effective care across settings. Successful transitioning involves consideration of the combined needs of the client and family, and the resources of the agency or health care provider to meet those needs. Table 24-1 provides guidelines for helping clients and families.
TABLE 24-1
Collaborative Communication Protocol for Interdisciplinary Team Development
Name: Introduce yourself to other member(s) by name and discipline.
Role: Declare your professional role on the team, and describe it with respect to the target client under discussion.
Issue: Share with other team members your discipline-specific professional ideas regarding the treatment of the target client under discussion.
Feedback: As client issues are discussed, elicit interaction-specific feedback from other team participants in the interaction using prompts such as “Do you have any concerns?” or “Is there something else I should consider?”
Adapted from Zwarenstein M, Reeves S, Russell A, et al: Structuring communication relationships for interpersonal teamwork (SCRIPT): a cluster randomized controlled trial, Trials 8:23–36, 2007.
Clients admitted to emergency departments usually have limited information to prepare them for self-care after discharge. Nurses are responsible for communicating and coordinating postdischarge instructions with clients and families, quickly educating them about the client’s condition and treatment-related tasks, and coordinating care with other health professionals as needed (Han et al., 2009).
Discharge Summary
The discharge summary is the most commonly used format for communicating diagnostic findings, hospital management, and plans for follow-up at the end of a client’s hospitalization (Kripalani et al., 2007). Content mandated for each client’s written discharge summary includes:
• Procedures and treatment provided
• The patient’s condition at discharge
Clients should be encouraged to bring their discharge summary to initial follow-up appointments. The Joint Commission (2009) mandates that discharge summaries be completed within 30 days of hospital discharge.
Nurses are accountable for verbally reviewing discharge summaries with the client and/or caregiver as appropriate, providing written instructions, and completing discharge documentation in the chart. Although the physician is responsible for initiating and signing discharge summaries and orders, nurses play a critical role in the discharge of clients, as identified in Box 24-6.
BOX 24-6 Core Functions for Transitional Sending and Receiving Teams Rights were not granted to include this textbox in electronic media. Please refer to the printed book. From HMO Work Group on Care Management: One patient, many places: managing health care transitions (p. 7), Washington, DC, 2004, AAHP-HIAA Foundation. HMO Work Group on Care Management
Discharge instructions are not the same as discharge orders. Specific written discharge instructions should include a basic follow-up plan identifying diet, activity level, weight monitoring, what to do if symptoms develop or worsen, and the contact numbers of relevant hospital and primary care providers. Written instructions should be simple and concrete—for example, “Call the doctor if you gain more than 2 pounds in 1 week.” A written list of all medications prescribed at discharge, including prescription, over-the-counter medications, and herbals, should be given to the client/caregiver.
Discharge documentation in the client’s chart should include the client’s condition or functional status at time of discharge, followed by a summarization of the treatment and nursing care provided, discharge instructions given to the client/family and the client’s responses. The place to which the client is charged (home, nursing home, rehabilitation center) should be identified. Subheadings help organize and highlight pertinent information for follow-up care (Kripalani et al., 2007). Nurses need to document that the client and/or caregiver was actually given a copy of the discharge instructions.
Management continuity
Management continuity represents a longitudinal approach to the clinical management of chronic disorders in the community. Care is delivered through coordinated referrals, case management, and community supports over a significant period.
The medical home
A new concept in primary care service delivery designed to promote COC is the client/family-centered medical home. The medical home is defined as a community-based delivery process involving a primary care team, led by an identified personal physician for the client. The client’s medical home accepts responsibility for coordinating health care across care settings, and providing accessible, comprehensive primary care services across time for designated clients and families.
The medical home serves as a central point of contact in primary care through which the majority of client health needs are met (Grumbach & Bodenheimer, 2002). Having a primary care home that coordinates care for all aspects of health care including acute and chronic care, preventive care, and palliative care is reassuring to clients and families. Over time, clients learn to depend on the medical home as a first-line treatment resource for all aspects of care. Physicians and other health care providers can provide better quality care because they have knowledge of the client’s lifestyle and can better detect subtle changes in the client’s situation or condition.
Using the medical home care delivery model provides an opportunity to effectively blend relational, informational, and management continuity into a holistic system of care for the client. A qualified provider consistent with the client’s choice takes a clinical leadership role in coordinating care, with other care providers within and external to the medical home, providing skilled services when indicated. Medical homes provide quick access to health care and can facilitate connections to other providers or medical and mental health services when needed.
Case management
Whether one works in the hospital or primary care setting, all nurses should have knowledge of how case management works and how it fits into COC. Carter (2009) states, “Case management is a core component of what is needed to improve health care quality overall, while reducing costs” (p. 166). Knowledge of community resources needed to facilitate health care delivery in primary care settings allows nurse case managers to consistently deliver the right care at the right time to the right client/family.
The Case Management Society of America (2009) defines case management as “a collaborative process of assessment, planning, facilitation and advocacy for options and services to meet an individual’s health needs through communication and available resources to promote quality cost-effective outcomes.” Standards of practice for case management related to quality of care, collaboration, and resource utilization are consistent with National Patient Safety goals developed by the Joint Commission (Amin & Owen, 2006).
With the help of a case manager, clients with serious chronic conditions are able to stay in their homes and function in the community (Ploeg, Hayward, Woodward, & Johnston, 2008). Case managers help individuals and families identify providers and facilities in the community capable of providing an essential continuum of services. For example, the case manager might help the client and/or family locate rehabilitation facilities, make recommendations for placement, serve as a liaison with reimbursement sources, and/or help the family evaluate the care provided at the facility.
The goal of case management strategies is to help clients at their highest possible level in the least restrictive environment. Case management strategies are designed with the following purposes:
• To enhance the client’s quality of life
• To decrease fragmentation and duplication of health delivery processes
• To contain unnecessary health care costs (Gallagher, Truglio-Londrigan, & Levin, 2009)
Populations served by case management
Essentially, clients need a case manager when they are unable to establish or maintain self-management of a chronic health condition in a consistent manner without external support. Included in the population group served by case managers are frail elders and housebound adults or children, clients with minimal brain dysfunction, chronic mental illness, gait or balance problems, individuals with delirium or dementia and/or chronic physical disabilities affecting activities of daily living. Sometimes, the person requiring ongoing case management services is neither elderly nor mentally incapacitated. He or she can be overlooked as a potential recipient of case management services despite significant impairments that interfere with quality of life.
Case management principles and strategies
Case management strategies are designed to coordinate and manage client care across a wide continuum of health care services and community supports. With the help of a case manager, clients with serious chronic conditions are able to stay in their homes and function in the community (Ploeg et al., 2008). Case management frameworks follow the nursing process as a structural framework in service provision. Strategies incorporate COC concepts related to communication, team building, and data sharing with all members of the multidisciplinary care team, including the client and family caregivers.
Case Finding
Case management is a proactive form of care delivery. Case-finding activities, especially in areas of high prevalence, can identify individuals at high risk for potential health problems and provide opportunities for early intervention (Thomas, 2009). Networking and communication with other health professionals involved with the client helps prevent or minimize emergence of full-blown health problems.
Assessment
Comprehensive assessment forms the basis for case management care coordination. In addition to basic health and demographic information, assessment for case management purposes should include the names, addresses, and phone numbers of the client’s health care providers, social service representatives, school or work contacts, if applicable, and health insurance information. Availability of social supports and religious affiliations, previous hospitalizations, and history of treatment, current medications and allergies, advance directives and DNR (do not resuscitate) status, cognitive and mental status, mobility status, and functional assessment of activities of daily living is important case management assessment data. Identifying potential barriers to treatment adherence, including the impact that the client’s diagnosis has on family members and coworkers can be helpful information. Baseline assessment data can be modified as the client’s condition changes.
Treatment Planning
Case management treatment plans are designed to promote treatment compliance and continuity. Case management strategies are customized for each client, based on their needs, values, and preferences. The client/family has final power over decision making and control of a personal recovery process.
Because case management represents a longitudinal treatment management process, the plan will necessarily change over time to reflect changes in the client’s situation and personnel/agency changes.
Implementation
Case managers meet with clients at regularly scheduled intervals. They assess client needs for changes in level of care, monitor client compliance with the plan of care, help clients procure needed supplies and medical equipment, and help clients obtain essential support services. Examples of non-nursing professional assistance clients may need to be linked with include legal aid, Social Security benefits, safe affordable housing, social services, and/or mental health and addiction services.
Effective case managers have a strong understanding of community resources’ strengths and weaknesses, including accessibility, availability, and affordability. They have an understanding of how health care systems work and can navigate the system.
Case managers need to be aware of the client’s needs, values, and preferences, and they need to be able to express these data to the treatment team and agencies involved in the client’s care in a clear, nonjudgmental, manner.
It is not enough to simply provide a referral. Additional follow-up may be necessary to assist clients with scheduling appointments, filling out required forms, getting transportation, or getting finances for participation in referral opportunities. Case managers may need to negotiate on the client’s behalf with insurance companies and equipment suppliers. When single agency resources are insufficient to meet a client’s complex health needs, case managers help clients and families identify and coordinate services with other agencies.
In the process of identifying and coordinating community-based resources, Hawranik and Strain (2007) note, “Nurses, as client advocates and agents of health promotion, can play an important role in modifying the focus of the system and of agency policies to include greater input by caregivers and clients” (p. 168).
Case managers are in a unique position to educate people in the community who work with disabled or chronically ill clients about the social aspects of disability to facilitate understanding and acceptance of the client’s problems. They can be helpful in linking clients and families with faith or social support groups, in initiating contacts for housing or job training, and in coaching clients about seeking social acceptance.
Evaluation
Case management outcomes are described in terms of client satisfaction, clinical outcomes, and cost. Quality improvement variances related to achievement of actual clinical outcomes are analyzed with recommendations for treatment planning, related to observed changes in the client’s situation, health condition, or in health care resources.
Documentation
The case manager is responsible for ensuring that all members of the multidisciplinary team accurately complete written documentation. Documentation from external providers and agencies needs to be included in the client’s case management record, as do variances from the treatment plan, reasons for the variance, and plans for modification in care plans.
Supporting informal family caregivers
COC involves supporting informal family caregivers. As health care delivery moves into the community, living with chronic illness increasingly becomes a home care responsibility, with family members as informal caregivers providing most of the care. Cott, Falter, Gignac, and Badley (2008) describe the home as “a unique clinical setting, different from acute care or institutional environments” (p. 19).
Family caregiving is neither a career choice nor a role for which one can prepare…and the caregiver has no “care map to lead the way,” states Wright, Doherty, and Dumas (2009, p. 209). Exercise 24-5 offers insights into the role of family caregivers from the caregiver perspective. Although many variables cannot be controlled, research findings indicate that caregiver training and support reduces caregiver strain and results in better clinical outcomes for clients (Weinberg, Lusenhop, Gittell, & Kautz, 2007).
Caring for clients with significant disability at home has positive and negative aspects. Being cared for at home offers stronger COC management as home is associated with personal identity, security and relationships with people who genuinely care about the client. Variation exists in a family member’s capacity to be supportive, especially if the caregiver’s health is not optimal, the care is labor intensive and time consuming, or the relationship with the client is conflictual (Weinberg et al., 2007). The need for information and assistance by family caregivers is often unspoken, as demonstrated in this case example.
Case managers and home care nurses can fill in essential information gaps for family caregivers through careful questioning, observation, validation about feelings and observations, and consultation about emerging health issues.
Case management for chronically mentally ill clients
Continuity of care is essential for effectively managing chronically mentally ill clients in the community (Wierdsma, Mulder, deVries, & Sytema, 2009). For clients with chronic mental illness, fulfilling even basic needs for shelter, food, clothing, and transportation can be issues, with the result that many of these clients are homeless and in poor physical health. Individuals with serious emotional and behavioral problems often function at a marginal level because of their symptoms. Many need consistent support to maintain themselves independently in the community. In addition to individualized treatment, COC for mentally ill and dually diagnosed clients includes formal wrap-around support services for mentally ill children and their families and case management for adults and children. Wrap-around services use a strengths based format and involve the family, community, school and service providers of the child’s environment working together as a team with the family to prompt adaptive functioning (Walker & Schutte, 2004). Many of these clients will not avail themselves of the opportunity, even when available.
Case managers provide individual mentoring and coaching, and job training services. They help clients avert crisis relapses that precipitate rehospitalization. Case managers offer strength-based community interventions such as linking clients with counseling and alternative treatment services, social services, and community networks, based on recovery principles of care. Consumer advocacy groups such as the National Alliance for the Mentally Ill (NAMI) provide support and practical advice for clients and families.
Advocacy at the community level
Chinn (2009) challenges nurses as one of the largest professional groups in the health care system to become the leaders, movers, and shakers in bringing about essential and fundamental changes in health care delivery. Sustaining quality health programs and services costs money. Advocacy to influence policy change that promotes availability and adequacy of health services in the public sector becomes urgent as escalating financial constraints narrow availability of community services. The positive policy environment promoted by WHO (2002) and linking community and health organizational efforts to achieve better outcomes for chronic conditions is a useful framework (Figure 24-3) for achieving COC objectives.
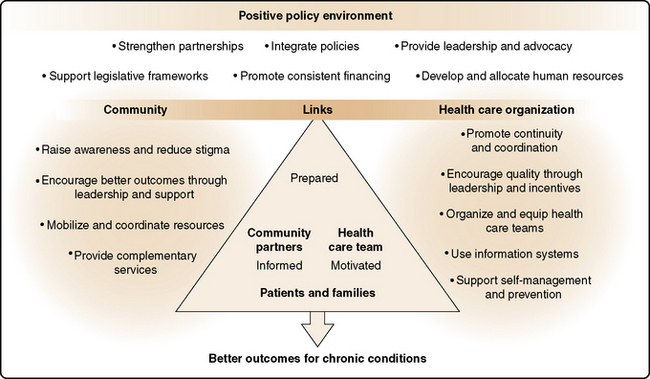
Figure 24-3 Building a positive policy environment for innovative continuity of care. From: World Health Organization. Innovative Care for Chronic Conditions: Building Blocks for Action. Geneva, Switzerland, 2002, p. 65.
Mason, Leavitt, and Chaffee (2007) define health policy as “the choices that a society, segment of society, or organization makes regarding its goals and priorities and the ways it allocates its resources to attain those goals” (p. 3). Advocacy at the system or community level tends to focus on adequate public health service provision, funding for essential health programs, and protecting the rights of vulnerable people to treatment.
Nursing practice in recent years has increasingly recognized political advocacy and involvement at the systems and policy level as a leadership responsibility of the professional nursing role (Francis-Baldesari & Williamson, 2008). Although nurses are on the front lines of the health care system as advocates of individual clients, they sometimes overlook their potential for helping to improve service delivery through advocacy at the community and national level. Clarke and Gottlieb (2008) declare that “keeping silent is no longer an option” (p. 7). Nurses must be willing to join together with other health professionals, their professional organizations, and community commissions and boards to argue for successful resolution of key quality-cost-access issues related to the financing and safe, effective delivery of health care (Spenceley, Reutter, & Allen, 2006).
Nurses can contribute to the development of effective health policy by writing e-mails to policy makers, becoming informed about public issues, sharing impressions with colleagues, testifying at public hearings, conducting and publishing research with health policy implications, and joining professional organizations with advocacy missions (Taft & Nanna, 2008). Concrete suggestions for improving community advocacy are highlighted in Box 24-7.
To be effective, nurses must thoroughly understand the issues on current and proposed legislation, and the formal/informal processes involved in shaping policy and passing legislation. Social networking and interpersonal interaction between providers and policy makers is key to getting research and practice initiatives into policy (Taft & Nanna, 2008). If you testify at a public hearing, you will need to:
• Keep your message simple and easy to understand; that is, What is your key message? Why is it important? What is the solution?
• Provide hard statistical data and support materials for your position. Produce one-page fact sheets.
• If there is time, add one powerful anecdote. Be descriptive, but concise.
• Know your audience; tailor your message and language accordingly.
• Keep within time limits. Memorize key points and practice your testimony. End with restating what you are advocating for.
• Acknowledge controversies and concerns, but do not dwell on them. Exercise 24-6 provides practice with effective advocacy efforts.
Summary
COC is a dynamic, client-centered service delivery process characterized as much by attitude as by actions. It is a multidimensional concept, consisting of relational, informational, and management continuity, and focused on assisting individuals and families with the resources they need to manage chronic illness within and across clinical settings. Conceptualized as the joint responsibility of patient, family, and multidisciplinary health care provider teams, the goal of COC is to ensure a seamless continuum of care for clients, provided through coordinated, community-based health services.
COC in clinical practice means building integrated delivery systems that focus on what really matters to a patient and family, and have the capacity to provide services to meet the patient’s needs.
Relational continuity embraces collaborative relationships and shared decision making between health care providers and clients to whatever extent is possible. Successful outcomes also depend on interdisciplinary collaboration and interprofessional team communication caring for the client, who can be defined as an individual, family, or community in need of care.
Informational COC allows for an uninterrupted flow of data and clinical impressions between health care providers and agencies, with clients and their families, in a care experience that is connected and coherent over time.
Discharge planning and handoff reporting represent important linkages between changes in clinical settings and between nurses at change of shift. The SBAR format for communicating important information offers a standardized comprehensive methodology for transmitting information.
Management continuity is achieved through case management strategies preparation and support of family caregivers in the home, and advocacy to ensure access and adequate funding for high-quality community-based care across health care systems.
References
American Hospital Association. Introduction to discharge planning for hospital. Washington DC: American Hospital Association, 1983.
Amin, A., Owen, M. Productive interdisciplinary team relationships: the hospitalist and the case manager. Lippincott Case Manag. 2006;11(3):160–164.
Birmingham, J. Discharge planning: a collaboration between provider and payer case managers using Medicare’s Condition of Participation. Lippincott Case Manag. 2004;9(3):147–151.
Boling, P. Care transitions and home health care. Clin Geriatr Med. 2009;25:135–148.
Bourgault, A., King, M., Hart, P., et al. Circle of excellence: does regular rounding by nursing associates boost patient satisfaction? Nurs Manag. 2008;39(11):18–24.
Carr, D. On the case: effective care transitions. Nurs Manag. 2008;32(1):25–31.
Carter, J. Finding our place at the discussion table: case management and heath care reform. Prof Case Manag. 2009;14(4):165–166.
Case Management Society of America What is a case manager, 2009. Available online:, http://www.cmsa.org/Home/CMSA/WhatisaCaseManager/tabid/224/Default.aspx. [Accessed August 6, 2009].
Castledine, G. Patient comfort rounds: a new initiative in nursing. Br J Nurs. 2002;11(6):407.
Chinn, P. History in the making. Adv Nurs Sci. 2009;32(1):1.
Clark, P., Cott, C., Drinka, T., et al. Theory and practice in interprofessional ethics: a framework for understanding ethical issues in health care teams. J Interprof Care. 2007;21(6):591–603.
Clarke, S., Gottlieb, L. Editorial: influencing health policy for the imminent health-care crisis: a task for informed citizens, proactive nurses, and committed researchers. Can J Nurs Res. 2008;40(4):5–9.
Coleman, E., Berenson, R. Lost in transition: challenges and opportunities for improving the quality of transitional care. Ann Intern Med. 2004;140:533–536.
Cooke, L., Gemmill, R., Grant, M., et al. Advance practice nurses core competencies: a framework for developing and testing an advanced practice nurse discharge intervention. Clin Nurse Spec. 2008;22(5):218–225.
Cotera-Perez, O. Discharge planning in acute care and long-term facilities. J Legal Med. 2005;26(1):85–94.
Cott, C., Falter, L., Gignac, M., et al. Helping networks in community home care for the elderly: types of team. Can J Nurs Res. 2008;40(1):18–37.
D’Amour, D., Oandasan, I. Interprofessionality as the field of interprofessional practice and interprofessional education: an emerging concept. J Interprof Care. 2005;19(Suppl 1):8–20.
Department of Defense (DoD) Patient Safety Program, in collaboration with the Agency for Healthcare Research and Quality (AHRQ), The TeamSTEPPS™ Teamwork System, 2009. Available online:, http://dodpatientsafety.usuhs.mil/index.php?name=News&file=article&sid=31. [Accessed August 13,].
Engebretson, J., Mahoney, J., Carlson, E., et al. Cultural competence in the era of evidence based practice. J Prof Nurs. 2008;24:172–178.
Epstein, R., Fiscella, K., Lesser, C.S., et al. Why the nation needs a policy push on patient-centered health care. Health Aff (Millwood). 2010;29(8):1489–1495.
Fletcher, R.H., O’Malley, M.S., Fletcher, S.W., et al. Measuring continuity and coordination of medical care in a system involving multiple providers. Med Care. 1984;22:403–411.
Francis-Baldesari, C., Williamson, D. Integration of nursing education, practice and research through community partnerships. Adv Nurs Sci. 2008;31(4):E1–E10.
Gallagher, L., Truglio-Londrigan, M., Levin, R., et al. Partnership for healthy living: an action research project. Nurse Res. 2009;16(2):7–29.
Greenwald, J.L., Denham, C.R., Jack, B.W., et al. The hospital discharge: a review of high risk care transition with highlights of a reengineered discharge process. J Patient Saf. 2007;3(2):97–106.
Grumbach, K., Bodenheimer, T. A primary care home for Americans: putting the house in order. J Am Med Assoc. 2002;288(7):889–893.
Haggerty, J.L., Reid, R.J., Freeman, G.K., et al. Continuity of care: a multidisciplinary review. Br Med J. 2003;327:1219–1221.
Haggerty, J.L., Pineault, R., Beaulieu, M., et al. Practice features associated with patient reported accessibility, continuity, and coordination of primary health care. Ann Fam Med. 2008;6(2):116–123.
Hall, P. Interprofessional teamwork: professional cultures as barriers. J Interprof Care. 2005;19(Suppl 1):188–196.
Han, C.Y., Barnard, A., Chapman, H., et al. Emergency department nurses’ understanding and experiences of implementing discharge planning. J Adv Nurs. 2009;65(6):1283–1292.
Hasnain-Wynia, R. Is evidence-based medicine patient-centered, and is patient-centered care evidence-based? Health Serv Res. 2006;41:1–8.
Hawranik, P., Strain, L. Giving voice to informal caregivers of older adults. Can J Nurs Res. 2007;39(1):156–172.
Institute for Healthcare Improvement, Use regular huddles and staff meetings to plan production and to optimize team communication, 2007. Available online:, http://www.ihi.org/IHI/Topics/OfficePractices/Access/Changes/IndividualChanges/UseRegularHuddlesandStaffMeetingstoPlanProductionandtoOptimizeTeamCommunication.htm. [Accessed April 30,].
Institute of Medicine (U.S.). Committee on Quality of Health Care in America Crossing the quality chasm: a new health system for the 21st century, Washington, DC, National Academies Press, 2001. Available online:, http://www.nap.edu.proxy-hs.researchport.umd.edu/books/0309072808/html.
Institute of Medicine. Envisioning the National Health Care Quality Report. Washington, DC: National Academies Press, 2001.
Jansen, L. Collaborative and interdisciplinary health care teams: ready or not? J Prof Nurs. 2008;24:218–227.
Joint Commission. 2010 Portable comprehensive accreditation manual for hospitals (CAMH): The official handbook. Oakbrook Terrace, IL: Joint Commission on Accreditation of Healthcare Organizations, 2009.
Kleinman, A. The illness narratives: suffering, healing, and the human condition. New York, NY: Basic Books, 1988.
Kohn L.T., et al, eds. To err is human: building a safer health system. National Academies Press: Washington, DC, 2000. Available online:, http://www.nap.edu.proxy-hs.researchport.umd.edu/books/0309068371/html.
Kripalani, S., LeFevre, F., Phillips, C., et al. Deficits in communication and information transfer between hospital-based and primary care physicians: implications for patient safety and continuity of care. J Am Med Assoc. 2007;297(8):831–841.
Lein, C., Collins, C., Lyles, J., et al. Building research relationships with managed care organizations: issues and strategies. Fam Syst Health. 2003;21(2):205–214.
Leonard, M., Graham, S., Bonacum, D., et al. The human factor: the critical importance of effective teamwork and communication in providing safe care. Qual Saf Health Care. 2004;13(Suppl 1):i85–i90.
Lidskog, M., Lofmark, A., Ahlstrom, G., et al. Interprofessional education on a training ward for older people: students conceptions of nurses, occupational therapists and social workers. J Interprof Care. 2007;21(4):387–399.
Mainous, A.G., Gill, J.M. The importance of continuity of care in the likelihood of future hospitalization: is site of care equivalent to a primary clinician? Am J Public Health. 1998;88:1539–1541.
Margalit, R., Thompson, S., Visovsky, C., et al. From professional silos to interprofessional education: campuswide focus on quality of care. Qual Manag Health Care. 2009;18(3):165–173.
Mason D.J., Leavitt J.K., Chaffee M.W., eds. Policy & politics in nursing and health care, ed 5, St. Louis, MO: Elsevier, 2007.
Meade, C., Bursell, A., Ketelsen, L., et al. Effects of nursing rounds on patients call light use, satisfaction, and safety. Am J Nurs. 2006;106(9):58–70.
Mikos, K. Monitoring handoffs for standardization. 2008 Guide to Patient Safety Technology regulatory compliance. Nurs Manag. 2007:16–20.
Muir, J.C. Team, diversity and building communities. J Palliat Med. 2008;11(1):5–7.
Nazareth, I., Jones, L., Irving, A., et al. Perceived concepts of care in people with colorectal and breast cancer—a qualitative case study analysis. Eur J Cancer Care. 2008;17:569–577.
Ploeg, J., Hayward, L., Woodward, C., et al. A case study of a Canadian homelessness intervention programme for elderly people. Health Soc Care Community. 2008;16(6):593–605.
Pontin, D., Lewis, M. Maintaining the continuity of care in community children’s nursing caseloads in a service for children with life-limiting, life-threatening or chronic health conditions: a qualitative analysis. J Clin Nurs. 2008;18:1199–1206.
San Martin-Rodriguez, L., D’Amour, D., Leduc, N., et al. Outcomes of interprofessional collaboration of hospitalized cancer patient. Cancer Nurs. 2008;31(2):E18–E27.
Saultz, J., Albedaiwi, W. Interpersonal continuity of care and patient satisfaction: a critical review. Ann Fam Med. 2004;2(5):445–451.
Schneller, E., Epstein, K. The hospitalist movement in the United States; agency and common agency issues. Health Care Manag Rev. 2006;31(4):308–316.
Schultz, K. Strategies to enhance teaching about continuity of care. Can Fam Physician. 2009;56:666–668.
Sheehan, D., Robertson, L., Ormond, T., et al. Comparison of language used and pattern of communication in interprofessional and multidisciplinary teams. J Interprof Care. 2007;21(1):17–30.
Sparbel, K., Anderson, M.A. Integrated literature review of continuity of care: part 1, conceptual issues. J Nurs Sch. 2000;32(1):17–24.
Spenceley, S., Reutter, L., Allen, M., et al. The road less traveled; nursing advocacy at the policy level. Policy Polit Nurs Pract. 2006;7(3):180–194.
Taft, S., Nanna, K. What are the sources of health policy that influence nursing practice. Policy Polit Nurs Pract. 2008;9(4):274–287.
Thomas, D. Case management for chronic conditions. Nurs Manag. 2009;15(10):22–27.
Thorne, S. Chronic disease management: what is the concept? Can J Nurs Res. 2008;40(3):7–14.
Tractenberg, D. Montgomery County Mental Health Advisory Committee Presentation, 2010. [County Council Member, Montgomery County Member, Rockville, MD, January 7].
van Servellen, G., Fongwa, M., Mockus D’Errico, E., et al. Continuity of care and quality care outcomes for people experiencing chronic conditions: a literature review. Nurs Health Sci. 2006;8:185–195.
Von Bultzingslowen, I., Eliasson, G., Sarvimaki, A., et al. Patients’ views on interpersonal continuity based on four core foundations. Fam Pract. 2006;23(2):210–219.
Wachter, R.M., Goldman, L. The emerging role of “hospitalists” in the American health care system. N Engl J Med. 1996;335:514–517.
Weinberg, D., Lusenhop, R.W., Gittell, J., et al. Coordination between formal providers and informal caregivers. Health Care Manag Rev. 2007;32(2):140–149.
Wierdsma, A., Mulder, C., de Vries, S., et al. Reconstructing continuity of care in mental health services: a multilevel conceptual framework. J Health Serv Res Policy. 2009;14:52–57.
World Health Organization. Innovative care for chronic conditions: building blocks for action. Geneva, Switzerland: Author, 2002.
Wright, J., Doherty, M., Dumas, L., et al. Caregiver burden: three voices-three realities. Nurs Clin North Am. 2009;44:209–221.
Zwarenstein, M., Reeves, S., Russell, A., et al. Structuring communication relationships for interpersonal teamwork (SCRIPT): a cluster randomized controlled trial. Trials. 2007;8:23–36.