5 Patient involvement in health professional education
Cooperative enquiry (also known as collaborative inquiry) Research ‘with’ rather than ‘on’ people, which emphasises that all active participants are fully involved in research decisions as co-researchers.
Continuous professional development (CPD) The continuing education of fully trained and accredited practitioners.
Expert patient A person with a chronic disease who has the confidence, skills, information, and knowledge to play a central role in the management of his/her health concern and to teach others.
Identity construction Social processes in the training of medical and other health professions students whereby they develop a coherent image of self that distinguishes them from other professionals and lay persons.
Kirkpatrick levels A commonly used framework for the evaluation of educational programmes comprising four levels: Reaction, Learning, Behaviour, and Results.
Senior mentor Older adults in the community who provide medical students with long-term mentorship related to ageing and geriatrics.
Social accountability Defined by the World Health Organisation as the obligation of medical schools ‘to direct their education, research, and service activities towards addressing the priority health concerns of the community, region, and/or nation they have a mandate to serve’.
Outline
Patients have always been the ‘clinical material’ for learning medicine, but the role of the patient as teacher has more recently been developed beyond a teaching aid towards more formalised and active participation in the educational process. Many and diverse initiatives have been described in government pronouncements and scholarly activity in the field, including reviews of patient involvement in medical education (Jha et al, 2009; Morgan and Jones, 2009; Wykurz and Kelly, 2002), nurse education (Repper and Breeze, 2007; Warne and McAndrew, 2005), mental health training (Livingston and Cooper, 2004), and social work (Cairney et al, 2006). There has also been an international conference (Farrell et al, 2006).
This chapter explores why that change has occurred and what the benefits and outcomes of active patient involvement are. We identify the factors that need to be considered when involving patients in education and provide examples to illustrate a range of approaches to patient involvement that are being tried in different health professional programmes in different countries, focusing particularly on government policy directives, social accountability, and the role of expert patients. Finally, we identify future directions for educational development and research in this field. The chapter starts by clarifying two major sources of controversy and confusion for anyone who wishes to gain an understanding of the topic: terminology and language, and the spectrum of possible involvement.
Terminology and language
We use the term ‘patient’, for the sake of brevity, to include people with health problems (service users, clients, consumers, survivors, etc.), their care givers (including carers, parents, and families), and healthy people (community members, citizens, lay people, well women, etc.). We have chosen to use the term ‘patient’ as our umbrella term because it is the most commonly recognised word, though the choice is a controversial one. ‘Patients’ are associated with passivity and many people do not like to be labelled in that way. It also defines the person as being ill; in the context of health professions education, there are many healthy people who contribute important experiences, such as parents of children with disabilities, seniors, refugees, and people from different ethnic groups. The term ‘lay’ may be more inclusive but, when contrasted with its opposite – ‘professional’ – it dismisses the expertise of non-professionals, defines them by what they are not (i.e. professionals), and, in our experience, is universally unpopular, even among people who cannot agree on any other term.
The most commonly accepted term in the United Kingdom is ‘user’ or more specifically ‘service user’, especially in professions other than medicine. However, a health practitioner in North America is more likely to connect the term with illicit drug use. There are even those in the United Kingdom who consider the term ‘service user’ as passive and not inclusive of people who cannot or do not access services. It also follows that the counterpart to a service user is a ‘service provider’, which implies a technical kind of interaction that detracts from the provision of more holistic, relationship-centred care. As many of the service users involved in education in the United Kingdom also have carers who play an important role, the collective term ‘service user and carer’ is frequently used. ‘Carer’ is a less controversial term though it is not familiar in North America, where the term ‘caregiver’ is used.
Other words that appear in the literature include ‘consumer’ or ‘client’, but these have overtones of health care as a market and, although favoured in some countries and professions, these terms are generally not used in medical education. The words people use to think of themselves in relation to the health care system vary according to the type of practitioner they are consulting, their condition, and the stage of their illness. Some people who have battled against cancer or mental illness, for example, prefer to call themselves ‘survivors’. The lack of agreed terminology is important on several levels: strong emotions generated by language and labels can create barriers to communication and partnership; the plethora of terms complicates scholarly activity by making it difficult to search the literature; and it makes writing and talking about the topic cumbersome.
The other source of confusion in the area of terminology is the large number of names used to refer to those patients who are actively involved in health professions education. Patients may be involved as teachers, educators, instructors, teaching associates, professional patients, mentors, or partners. When we reviewed the titles used to describe well women who are trained to teach intimate examinations (pelvic and/or breast), we found a total of 18 different titles used in 41 different papers in the literature. The meanings of terms are not always consistent: at one institution they may be called ‘standardised patients’ because they teach in a standardised way but the same role may be designated ‘teaching associate’ at another institution. This makes good literature search difficult and is one reason why reviews of the literature using similar but not identical inclusion criteria may miss many relevant papers.
Spectrum of involvement
Patient involvement occurs throughout the continuum from undergraduate education (pre-registration), postgraduate or specialist education, continuous professional development (CPD), and in-service training, although the majority of reported initiatives occur in undergraduate courses or in the postgraduate training of mental health professionals (predominantly non-psychiatrists such as nurses and counselling psychologists). Patients can actively contribute to different aspects of the educational process. Direct involvement in curriculum delivery is the commonest role; students may learn from people who come into the classroom to talk about their experiences of, say, living with an addiction, HIV/AIDS, or a disabled child. They may also learn from patient educators, who teach clinical skills. Health professionals at all stages learn informally from patients in clinical settings (see below). Patient organisations may contribute to, or lead, CPD activities on specialised topics such as fetal alcohol syndrome and there may be public members on committees that plan CPD (British Medical Association, 2008). The most comprehensive list of potential roles is provided by Tew et al (2004), who give examples of patient involvement in
The diversity of educational initiatives in which patients are actively involved demands a classification scheme. Without such a framework there is no agreed way in which authors can characterise the role of patients in their initiatives, which makes scholarly communication difficult and comparative evaluation or systematic reviews impossible. It is often difficult to find out from published work exactly what the patient’s role was in the educational programme described, especially the degree to which patients were actively involved and the degree to which they participated in decision making. For example, early patient or community contact in medical school often consists of an attachment to a patient with a chronic illness, a pregnant woman, a family, or a community agency; in some cases the patient, family, or community agency may be explicitly identified as a teacher or mentor, whereas in other cases their role is simply to be interviewed. The expected learning outcomes would be quite different for those two different roles.
There are two useful classification schemes: the Cambridge framework developed by Spencer et al (2000), which describes the attributes of educational settings that shape learner–patient encounters, including Who? (the patient’s culture), How? (a passive vs. an active role), What? (a general vs. a specific problem), and Where? (community vs. hospital); and the Ladder of Involvement described by Tew et al (2004), which identifies five levels of involvement – Level 1: No involvement, Level 2: Limited involvement, Level 3: Growing involvement, Level 4: Collaboration, and Level 5: Partnership. More recently, we combined both of these models into a Spectrum of Involvement tool (Towle et al, 2010). Our proposed taxonomy includes six main attributes:
We recognise that these categories, rather than being discrete entities, overlap, and the taxonomy represents a continuum of involvement.
Why involve patients?
Depending on the health profession, country, and time, there are many reasons why health professional educators choose to involve patients actively. We have chosen three different clusters of reasons to discuss in detail. These clusters are not mutually exclusive but each is rooted in a different discourse (see Chapter 3). It is important to know that the movement to involve patients actively in the education of health professionals is based more on the power of these rationales than on robust evidence of beneficial educational outcomes at the time of writing.
Public and patient involvement in health care: government and professional policy directives
The importance of public and patient involvement in health care is recognised in many countries. Members of the public are frequently consulted about health care services, health policy, and research as part of a growing consumerist model of health care. UK government policy has placed public and individual patients at the centre of health care over the past 20 years. Successive policy documents have emphasised a patient-led National Health Service based on choice, participation, and partnerships. It is within this context that the government has also made clear its expectations that service users will be involved in all publicly funded health and social care research and, more recently, that service users and carers should be involved in the education and training of health professionals.
This policy directive has been taken up by accrediting bodies in the United Kingdom. ‘Skills for Health’, the body that is responsible for the quality assurance of all health professional programmes in the United Kingdom, except medicine, requires evidence of patient involvement in education. The Nursing and Midwifery Council requires universities to involve a service user as a panel member during the approval process for pre-registration nursing programmes. The General Medical Council does not have the same explicit requirements for patient–public involvement, although it requires data on the quality of medical education programmes to include feedback from patients (GMC, 2009).
The most significant activity has been in the field of mental health, originally in mental health nursing, extended more recently to social work, psychiatry, and clinical psychology. The National Service Framework for Mental Health published by the UK Department of Health in 1999 proposed that ‘service users should be involved in planning, providing, and evaluating education and training’ (a recommendation that had been made in relation to mental health nursing in a 1994 Department of Health review). In 2006, the Department of Health stated that higher education institutions should ‘involve service users and carers in every aspect of education including recruitment, curriculum planning, teaching, and student assessment’. In some training programmes such as mental health or social work, practitioners have specific courses on ‘user involvement’ that include users in curriculum development or as teachers.
The ‘user’ discourse raises interesting questions about ideology, articulated mainly in the areas of health and social care, but also in research (Cowden and Singh, 2007). The user movement has given service users a voice in decision making, particularly in the areas of disability and mental health; recognition of the importance of their lived experiences has given them roles as educators, researchers, and consultants. Government policy, however, has framed user involvement within a consumerist model of improving the product through market testing and consumer feedback (manager-led/users as consultants) rather than a user-led, liberational model, where users are empowered to develop new kinds of services, research, or education. Health professionals are urged to consult about the quality of services but find that service users’ views vary between individual patients, patient groups, and patient representatives, and also between those with radical and non-radical views. Under those circumstances, it is difficult to select the ‘right’ patients (Williamson, 2007). These groups bring different knowledge and expertise, so finding representatives from each of them is as relevant to health professions education as to health services.
UK policy directives have resulted in a large number of initiatives such that the United Kingdom leads in institutionalising patient involvement in education. No other country has embedded service user involvement in health and social care so deeply into its policies and structures and, by extension, the education of health professionals.
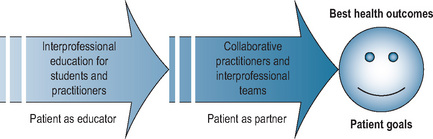
Irrespective of national government policy, however, almost all health professions espouse a version of patient-centred care in their particular good practice model, which involves patients in decision making, with a focus on individual people’s preferences, life circumstances, and experience of illness. There is at least a theoretical link between patient involvement in education, patient involvement in care, and improved health outcomes; Figure 5.1 shows how the model might apply in an interprofessional context (see Chapter 4). Bleakley and Bligh (2008), however, have pointed out that patient-centredness is still typically framed as a set of values and virtues learnt from doctors as role models, reinforced through structured educational input from medical educators, and, paradoxically, not from patients.
Social accountability of higher education institutions: the moral imperative
The World Health Organisation (WHO) has defined the social accountability of medical schools as ‘The obligation to direct their education, research, and service activities towards addressing the priority health concerns of the community, region, and/or nation they have a mandate to serve. The priority health concerns are to be identified jointly by governments, health care organisations, health professionals, and the public’.
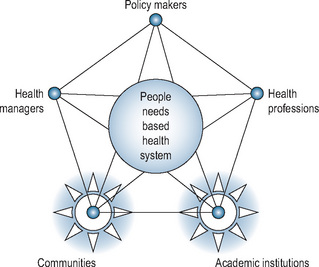
Social accountability is important because good education for health does not necessarily provide a nation with good health; there are many other factors involved such as the career choices of graduates, incentives and rewards for primary health care, and health policy. Translation of good education into good health requires the collaboration of key stakeholder groups. The framework for social accountability developed by the WHO, illustrated by the partnership pentagram (see Figure 5.2), has a central core reflecting a health system that meets human needs. Five partners have to respond to those needs – policy makers, health managers, health professions, communities, and academic institutions – and complex relationships between the stakeholders who serve and are served by the health care system must be managed for health needs to be met.
The Association of Faculties of Medicine of Canada (AFMC), influential in setting the direction for Canadian medical education, has adopted the WHO definition as its mandate for social accountability and the focus for its unifying vision for academic medicine in the country. Central to the AFMC vision was the creation of a ‘Partners Forum’ with representatives of key stakeholder groups, including the public. The concept of community engagement signals recognition by academic institutions of the importance of partnerships with the communities they serve. The Community Campus Partnerships for Health (CCPH), primarily a US organisation originating from a campaign to improve health care for those who need it most, has as its mission the promotion of health (broadly defined) through partnerships between communities and higher educational institutions. Many of the community engagement initiatives in the United States come from the moral imperative to address health disparities, especially by engaging large sectors of the population who do not have access to good health care. One of the major educational activities fostered by CCPH has been community-based service learning. Although active patient or community involvement is not in itself a prerequisite for service learning activities, people in the community play a variety of roles along the spectrum of involvement, from passive recipients of care (the classic provider–patient relationship), to facilitators of reflection seminars, mentors, and assessors of students. The provision of opportunities for service learning has recently been adopted as an accreditation standard for North American medical schools. Other patient involvement initiatives in the United States (e.g. the senior mentor programmes described below) have their origin in the need to improve health care for the underserved (in this case elderly people) through promoting more positive attitudes towards these populations among medical students.
The expert patient: enrichment of education
In the first published review of patients as active teachers in medical education, Wykurz and Kelly (2002) identified 23 studies that demonstrated the diversity of expertise patients brought to their teaching roles. The recognition of patients as experts comes in part from the concept of encounters between professionals and patients as ‘meetings of experts’, first elaborated by Tuckett et al (1985). From that point of view, not only do health professionals bring (biomedical) expertise but also patients bring expertise of their personal and cultural background and their experiences of living with illness or disability. Over the last two decades, educators have tapped into the expertise of patients in order to enrich student education in a variety of ways, providing learning experiences that could not otherwise occur, and broadening curricula from the biomedical model. In some disciplines, the expertise of patients has been used to augment a scarce pool of clinical teachers. Patient–teachers have been shown to create safe learning environments for students to practice clinical skills, especially intimate examinations, and they have been able to provide more in-depth feedback to students than could usually be provided by busy preceptors.
The extent of the expertise patients could offer has not yet been fully explored. At the University of British Columbia, we have worked with patients with mental health problems, arthritis, and epilepsy, and their caregivers, to develop patient-led workshops about a range of diverse topics, including
Outcomes of patient involvement
The diversity of motivations for involving patients predicts an equally diverse range of outcomes. Many reports in the mental health and social work education literature, for example, focus on service users’ and carers’ experiences of interacting with institutions of higher education, the outcomes of interest being more to do with user empowerment than student learning. The literature on patient involvement in general is marked by a lack of clear and measurable outcomes; most studies have been descriptive and few interventions rigorously evaluated. Most descriptions provide insufficient detail about what was done and few use rich, qualitative or mixed methodologies. Experimental studies give inadequate information about the interventions and research designs; initiatives are usually described only once in the literature, soon after implementation (often of a pilot project) along with preliminary evaluation data, usually student satisfaction and patient views. Typically, evaluation of short-term outcomes for a small subset of initiatives is reported (primarily in clinical skills teaching), but few such studies have had rigorous experimental designs.
A review by Morgan and Jones (2009), although limited to studies from the United Kingdom, provides a good summary of the state of the art. Most of the 41 papers they reviewed included some formal evaluation except for those that described patient involvement in curriculum design; in these studies, there were no attempts to demonstrate an impact on students who subsequently took the courses in question. Studies that included an evaluation generally captured the views of students and patients but not of the professional teachers. Using Kirkpatrick’s four-level model of evaluation (Kirkpatrick, 1996), four papers reported evaluation data at Level 2 (changes in measured attitudes, skills, and knowledge), one at Level 3 (change in behaviour), and one at Level 4 (benefit to service users). With respect to Level 1 outcomes (reaction), overall student perceptions of patient involvement were generally positive; concerns that were expressed related largely to interaction with patients who had mental illnesses. Overall benefits for patients were reported, with no negative effects. Morgan and Jones (2009) conclude that ‘despite a limited and weak traditional evidence base for impact on students’ knowledge and practice, both students and service users identify benefits from engagement’.
Approaches to involving patients in education
Several ‘good practice’ guides that provide useful information have been produced in the United Kingdom for education in mental health care (Tew et al, 2004); clinical psychology (British Psychological Society, 2008); and social work (Ager et al, 2005; Levin, 2004). The INVOLVE guides, designed to promote patient involvement in health research, have information relevant to higher education (http://www.invo.org.uk). No such ‘how to’ resources yet exist for medical education but the British Medical Association (2008) has published some useful guidelines, especially on the important topic of ethics, including confidentiality and consent.
Each of these guides organises the key tasks slightly differently but all identify a core set of issues as critical. These include leadership (requires a champion); dedicated funding; recruitment of patients (diversity and representativeness); infrastructure for support, training, and supervision of patients; employment and contracting; payment and expenses; capacity building; and evaluation. They are a good resource for those needing advice about initiating and sustaining involvement. For example, Tew et al (2004) suggest that these activities may be more effectively facilitated by designated support and development workers, as teaching staff are not necessarily the best people to do outreach and capacity building work or to provide support to service users and carers. A network of development workers has been established in the United Kingdom (the Ducie network), which has published guidelines for higher education institutions (Developers of User and Carers in Education, 2009). This liaison role, also referred to as being a ‘culture broker’ or ‘boundary spanner’, is one that many academic institutions have found essential to facilitate partnerships with community-based organisations.
A guide produced by the Social Care Institute for Excellence (Levin, 2004) articulates key practical considerations in ‘preparing for participation’, paraphrased as follows:
Often the words involvement, collaboration, and partnership are used interchangeably. Working in true partnership with people from the community, however, brings challenges for health professional educators: there is a large power imbalance; there may be tensions over decisions (e.g. whose objectives); and there may be barriers to communication. Recognising the difficulty of achieving authentic partnerships between academia and the community, the CCPH has developed a set of partnership principles that have been recognised and applied internationally (see Box 5.1).
Box 5.1 CCPH core principles of good community-campus partnerships (http://www.ccph.info/)
Approaches to some of these issues are illustrated in the following four examples: three diverse initiatives at one institution that engage service users at different levels of involvement; patient educators who teach clinical skills (musculoskeletal examination), using expert knowledge of their own body; programmes developed to meet a national educational need (better geriatrics curriculum) in order to meet a health care need (better care for an underserved population); and how to develop a new educational initiative that involves faculty and students from different health programmes and community organisations, and individual patients, as community educators.
Service user and carer participation in education of mental health practitioners
The University of Southampton School of Nursing and Midwifery, United Kingdom, has tried different ‘socially inclusive’ approaches to engaging service users and, in some cases, carers more fully in the education of mental health practitioners (Lathlean et al, 2006; Simons et al, 2007). The purpose of each project is to develop and evaluate different aspects of ‘good practice’ in which participants are active agents of change in processes of research and education. Each initiative represents movement on a continuum of participation from service users as passive recipients to service users as collaborators and co-researchers, and is grounded in theory.
The first initiative was a service user and carer reference group (i.e. users’ role is collaborative and consultative). In existence for over 5 years, its aim was to share a range of views and knowledge of mental health matters and provide advice to guide the university in the development of its programmes. Challenges included the need to nurture participation, which requires energy, enthusiasm, commitment, and sufficient funding. The benefits were the value of having established members with different contributions to make, including service users, carers, and students. They identified the group as a ‘culture carrier’, that is a shared belief in the value of participation as an essential contributing factor to organisational change towards more user-centred services.
The second was the service user academic initiative: the establishment of a position (‘User Academic’) in the university, modeled on the consumer academic concept from Australia (i.e. user integrated into the academic institution). The holder of the position was a person with experience of mental illness and mental health services, who was employed as a member of an academic team. An evaluation of the development and practice of the position revealed tangible benefits for students and the wider academic community; most importantly, the User Academic provided a powerful role model for students and challenged elitist attitudes by confronting notions of expertise. However, because of mixed expectations of the position and unintended discriminatory behaviour, the role did not become integrated into the team and key sources of support were unavailable.
The third initiative was the participation of mental health service users in the clinical practice decisions of mental health students in training, based on the theories of anti-oppressive practice, contact theory, and moral development. An emancipatory research design, co-operative inquiry, was used to study how service users could be more effectively engaged in students’ clinical decision making (Tee et al, 2005). One of the most significant outcomes was to reveal how detached current concepts and theories of mental health, including the language used, could be from the day-to-day experience of people using services.
Arthritis educators
With the exception of clinical teaching associate programmes (teaching intimate examinations), the arthritis educator programme is unique as a long-lasting programme (the first paper was published in 1982), which has become institutionalised and widespread. It started in the United States as a development of the simulated patient concept but involved ‘real’ patient instructors with arthritis who were trained to teach the musculoskeletal examination through an intensive structured and standardised training programme (Gruppen et al, 1996). It spread through a cascade model to other schools in the United States and to Canada and Australia, thence to several other countries, as well as more recently appearing, apparently independently, in Switzerland and the United Kingdom. Long-term stable funding for the programme has come largely from pharmaceutical companies.
The patients are variously referred to as patient instructors, patient partners, patient educators, and arthritis educators. They are trained by physicians within the biomedical model; there is a strong emphasis on anatomy and the reliable assessment of the performance of the joint examination using a standardised checklist. The autonomy of the patient as educator is limited but patients also teach about psychosocial issues and the experience of living with arthritis in some programmes (Gruppen et al, 1996). The learners are generally medical students in the pre-clinical years, but some programmes teach clinical-level students or postgraduates and in some programmes the arthritis educators teach students from multiple programmes including physical therapy.
Because of differences in programme design and evaluation methods, it is difficult to draw strong conclusions about the outcomes of such programmes. In general, student satisfaction is high, although in comparative studies students tend to prefer being taught by specialists rather than by patients. Some programmes employ arthritis educators because of a shortage of specialists (rheumatologists). Students taught by patients generally have been shown to have examination skills equivalent to those of students taught by specialist physicians. Patient satisfaction is high and no adverse effects of being a patient teacher have been noted.
Senior mentor programmes
Senior mentor programmes (SMPs) have been developed by a number of medical schools in the United States (see e.g. Stewart and Alford, 2006) to meet the need for a better curriculum in geriatrics, including knowledge, skills, and attitudes (to counter ageism).
There are many different models but all have elements in common. Most SMPs are connected with an established ‘doctoring’ course that typically includes practical experience such as learning communication skills, sessions on professionalism (including ethics), and clinical reasoning, as well as contact with individual patients or populations. SMPs use older adults either directly as teachers or as ‘sensitisers’ to particular issues of importance to the medical care of elderly people. The relationship between student and senior is modelled on a learning relationship with mentors as teachers, rather than on a provider–patient relationship model. The programmes are therefore linked to the wider ‘expert patient’ movement in medical education; in this case the mentors’ expertise is in ageing.
The programmes have been integrated into medical school curricula, which recruit seniors who are basically well, living in the community, and without cognitive problems; in this way, students interact with people who are ‘ageing well’ physically and mentally. Seniors are recruited through medical practices or community agencies, but recruitment of a diverse ethnic and socio-economic pool is a challenge.
The relationship that develops between student and mentor is at the heart of the programme and may include social events beyond academic activities. As both students and mentors are placed in new roles, programme staff may need to assist both parties to clarify and redefine their changing roles over time: students’ roles change as they progress through the programme from being a friend to, for example, being asked to conduct a physical examination; mentors may develop health problems during the course of their relationship with students. In the SMPs that span several years, the relationship that develops can be very strong and a closing ceremony of some kind is important.
Community partnerships for interprofessional education
Our initiative at the University of British Columbia, ‘Community Partnerships for Health Professional Education’, aims to create sustainable partnerships with patient organisations that result in community-led educational initiatives for health professional students (Towle et al, 2009). Using a participatory design approach, community members, faculty, and students collaboratively develop, pilot, and evaluate interprofessional workshops led by community educators. Student and faculty collaborators come from medicine, nursing, pharmacy, occupational therapy, physical therapy, social work, human kinetics, and speech–language pathology. Community educators have been recruited through patient organisations, advertisements, and word of mouth.
The direction and evaluation of the project is overseen by an advisory board of students, faculty, and community members (representatives from patient support and advocacy organisations as well as individual patients). The advisory board has defined the mission, vision and goals, membership of the board, evaluation framework for the workshops, and policies for presentation and dissemination of the work. Evaluation methods include pre-workshop survey (student expectations); post-workshop survey (student learning); follow-up interviews, and focus groups with faculty, community educators, and students; and reflective journals maintained by students.
Reported student learning includes
With respect to interprofessional education (IPE), students learnt with each other and about each other by listening to each other’s questions at all workshops. There were specific IPE activities at three workshops so students could learn from and about each other during small breakout groups and through working on a case study together. Although students were keen to learn about interprofessional care, this was not a high priority for the community teachers.
Learning from patients in clinical settings
Although the formal ‘patient as educator’ roles described above are increasing in number, the majority of health professional contacts with patients still occur in clinical settings (hospital wards, clinics, family physician offices), where patients’ main focus is on receiving health care. In those situations, patients may be too ill, disempowered, or focused on health care procedures to be willing or able to take on the additional role of a teacher in any formal way. The dynamics are most often between the student(s) and the clinical teacher, with the patient only peripherally involved. As Bleakley and Bligh (2008) point out, ‘the main focus of the educational process, even where it is ostensibly based “around” the patient, tends to gain meaning and legitimacy only in the interaction between the student and the doctor (as educator)’. They call for a reorientation of the relationship between patient, student, and teacher to enhance collaboration between the student and the patient (for ‘collaborative knowledge production’) with the expert doctor as a resource. The work by Ashley et al (2008) provides some practical ways of achieving this ‘patient-based curriculum’ through a series of recommendations for supervising a medical student in an outpatient clinic or surgery.
The perceptions of patients about their role in student education in the clinical setting are more varied than in the studies in which patients are clearly recruited to be educators. Stockhausen’s (2009) patients were ‘experience brokers’, who mediated and observed teaching and learning to care between nursing students and experienced preceptors, while also becoming participants in learning to care. Ashley et al (2008) found that the dynamics between student and patient were characterised by two themes, identification and participation; patients identified with students and students wanted to participate in the care of patients. McLachlan et al (2009) found that involvement in students’ education was usually described by patients as ‘ordinary’, having little effect on them. There are also negative experiences. Although less commonly reported now, there are still official and anecdotal reports of patients who were uninformed or unwilling participants in the educational process and were unaware that an invasive procedure would be done by a novice student or that students would be performing pelvic examinations while they were anaesthetised for surgery. We have found, through interviews with faculty, health professional students, and patient educators, the following challenges to patient participation in student learning in the clinical setting:
Students
Patients
Working with the same groups, we have developed a set of guidelines for engaging patients as active teachers in the clinical setting (see Box 5.2).
Box 5.2 Guidelines for engaging patients as teachers
Prepare patient for teaching role
Implications for practice
Theory
Very little of the literature about patients’ involvement in education is informed by explanatory theory. Two exceptions are papers by Katz et al (2000) and Rees et al (2007), which take a social science perspective to explore issues on how students learn ‘with’ rather than just ‘about’ patients. Bleakley and Bligh (2008) have proposed a theoretical model of collaborative knowledge production based on theories of text, identity construction, and work-based learning in which the prime locus for knowledge production is the student’s reading of the patient’s condition in collaboration with the patient. These examples provide glimpses of how the active involvement of patients could provide a new educational paradigm in which students, teachers, and patients can create new knowledge and novel solutions to health care problems by learning together.
Research
There is a need for good-quality outcome studies with rigorous experimental designs, especially ones that investigate long-term outcomes. Most initiatives are described only once in the literature, usually at the end of a small-scale pilot or an early implementation phase. There are no studies of long-term outcomes or sustainability. Many initiatives do not last but the reasons why some become embedded within an institution while others fade away are not understood. Towle et al (2010) have identified four research foci – antecedent variables, structures, processes, and outcomes – and given examples of needed enquiry in each category. For example, what are the drivers of patient involvement in health professional education, including external, institutional, faculty, and patient factors? (antecedent variables); what effect does the setting (e.g. patient’s home, classroom, or clinic) have on learning? (structural elements); what are the meanings that involvement has for patients and how do these change? (processes); finally, what factors result in sustainable ‘patient as educator’ programmes and what are the successful models that can be replicated? (outcomes).
Practice
There is a need for coordinated and sustainable programmes of patient involvement. Most initiatives described in the literature are single educational experiences for a specific group of learners. If education is to be patient-centred, we must move from these one-off experiences to coordinated and sustained programmes of development of a patient involvement curriculum and authentic partnerships at an institutional level.
Ager W., Dow J., Ferguson I., et al. Service user and carer involvement in social work education: good practice guidelines. Scottish Institute for Excellence in Social Work Education (now the Institute for Research and Innovation in Social Services, Glasgow, Scotland), 2005.
Ashley P., Rhodes N., Sari-Kouzel H., et al. ‘They’ve all got to learn’. Medical students’ learning from patients in ambulatory (outpatient and general practice) consultations. Med Teach. 2008;31:e24-e31.
Bleakley A., Bligh J. Students learning from patients: let’s get real in medical education. Adv Health Sci Educ. 2008;13:89-107.
Boelen C. Towards unity for health. Geneva: Challenges and Opportunities for Partnership in Health Development, World Health Organization, 2000.
British Medical Association, Medical Education Subcommittee. Role of the patient in medical education. 2008. Available at www.bma.org.uk Accessed November 29, 2009
British Psychological Society Division of Clinical Psychology. Good practice guidelines: service user and carer involvement within clinical psychology training. 2008. Available at www.bps.org.uk Accessed November 29, 2009
Cairney J., Chettle K., Clark M., et al. Theme issue on involvement of service users in social work education. Social Work Educ. 2006;25(4):315-430.
Cowden S., Singh G. The ‘user’: friend, foe or fetish? a critical exploration of user involvement in health and social care. Crit Soc Policy. 2007;27:5-23.
Developers of User and Carer Involvement in Education. Involving service users and carers in education: the development worker role. United Kingdom: Higher Education Academy/Mental Health in Higher Education, 2009. Available at: http://www.mhhe.heacademy.ac.uk/silo/files/ducie-guidelines.pdf Accessed November 29, 2009
Farrell C., Towle A., Godolphin W. Where’s the patient’s voice in health professional education? Vancouver, Canada: Division of Health Care Communication, University of British Columbia, 2006.
General Medical Council. Tomorrow’s doctors. London: GMC, 2009.
Gruppen L.D., Branch V.K., Laing T.J. The use of trained patient educators with rheumatoid arthritis to teach medical students. Arthritis Care Res. 1996;9:302-308.
Jha V., Quinton N.D., Bekker H.L., et al. Strategies and interventions for the involvement of real patients in medical education: a systematic review. Med Educ. 2009;43:10-20.
Katz A.M., Conant J.L., Inui T.S., et al. A council of elders: creating a multi-voiced dialogue in a community of care. Soc Sci Med. 2000;50:851-860.
Kirkpatrick D. Revisiting Kirkpatrick’s four-level model. Train Dev. 1996;50(1):54-59.
Lathlean J., Burgess A., Coldham T., et al. Experiences of service user and carer participation in health care education. Nurse Educ Today. 2006;26:732-737.
Levin E. Involving service users and carers in social work education. Social Care Institute for Excellence, London, UK, 2004. Resource Guide No 2. Available at www.scie.org.uk Accessed November 29, 2009
Livingston G., Cooper C. “User and carer involvement in mental health training. Adv Psychiatr Treat. 2004;10(2):85-92.
McLachlan E., Wenger E., King N., et al. Patients? sense of identity in medical education, Phenomenological analysis, 2009. Poster presentation at Association for Medical Education in Europe (AMEE), Barcelano, Viguera Editors SL. Educacíon Médica, 12. 2009:S132. (suppl 2):
Morgan A., Jones D. Perceptions of service user and carer involvement in healthcare education and impact on students’ knowledge and practice: a literature review. Med Teach. 2009;31:82-95.
Rees C.E., Knight L.V., Wilkinson C.E. “User involvement is a sine qua non, almost, in medical education”: learning with rather than just about health and social care service users. Adv Health Sci Educ. 2007;12:359-390.
Repper J., Breeze J. User and carer involvement in the training and education of health professionals: a review of the literature. Int J Nurs Stud. 2007;44:511-519.
Simons L., Tee S., Lathlean J., et al. A socially inclusive approach to user participation in higher education. J Adv Nurs. 2007;58:246-255.
Spencer J., Blackmore D., Heard S., et al. Patient-oriented learning: a review of the role of the patient in the education of medical students. Med Educ. 2000;34:851-857.
Stewart T., Alford C.L. Older adults in medical education – senior mentor programmes in US medical schools. Gerontol Geriatr Educ. 2006;27:3-10.
Stockhausen L.J. The patient as experience broker in clinical learning. Nurse Educ Pract. 2009;9:184-189.
Tee S., Coldham T. with Student Nurses. Students and service users learning together: co-operative inquiry and its implications for curriculum development. United Kingdom: Mental Health in Higher Education. 2005. UK Case Study. Available at: http://www.mhhe.heacademy.ac.uk/resources/-case-study-14/ Accessed November 29, 2009
Tew J., Gell C., Foster S. Learning from experience. Involving service users and carers in mental health education and training. United Kingdom: Higher Education Academy/National Institute for Mental Health in England/Trent Workforce Development Confederation, 2004.
Towle A., Creak S., Kline C., et al. Community partnerships for interprofessional education, Abstracts of the Canadian Conference on Medical Education. Edmonton, Alberta, Canada, May 2–6, 2009. Med Educ, 43. 2009;suppl 1:11-12.
Towle A., Bainbridge L., Godolphin W., et al. Active patient involvement in the education of health professionals. Med Educ. 2010;44:64-74.
Tuckett D., Boulton M., Olson C., et al. Meetings between experts. An approach to sharing ideas in medical consultations. London, UK: Tavistock Publications Ltd, 1985.
Warne T., McAndrew S. Using patient experience in nurse education. Basingstoke: Palgrave Macmillan, 2005.
Williamson C. How do we find the right patients to consult? Qual Prim Care. 2007;15:195-199.
Wykurz G., Kelly D. Developing the role of patients as teachers: literature review. Br Med J. 2002;325:818-821.
Towle A., Godolphin W. Patient involvement in health professional education: a bibliography 1975–2009. In Division of Health Care Communication. The University of British Columbia; 2009. Available at http://www.chd.ubc.ca/dhcc/node/67 Accessed November 29