CHAPTER 7 Lower limb motion during walking, running and jumping
Most sporting activities involve the movement of the human body over distance. An understanding of the biomechanical factors which affect gait is therefore fundamental to the prevention and management of sports injuries. Abnormal forces placed on the body through alterations in normal running or walking can cause injury. In addition, rehabilitation of lower limb injuries, if it is to be successful, must involve the restoration of correct gait. Failure to do so may impair performance and leave the athlete open to further problems.
Injuries to the lower limb, especially those to the ankle and knee, tend to occur when weight bearing. Typically this is a twist on the fixed foot, or when landing from a jump. Brief analysis of this action will again help to understand injury causality, and to better structure rehabilitation programmes.
Closed and open motion
Motion at a joint is often described anatomically as though it occurred in isolation, yet functionally, isolated joint movements rarely occur. The limbs or trunk may be considered as moveable chains, the links of which are the joints themselves. Movement of one of the joints causes an effect on the other links in the chain, and so other joints respond.
Open chain motion occurs when the proximal bone segment in a limb is fixed but the distal segment remains free. Closed chain motion is the reverse. Both the proximal and distal bone segments are fixed, and movement occurs between the two. When we evaluate a joint within a limb in open chain motion, the movement of the bony segment occurs distal to the joint being studied. Movement within a closed chain will occur both proximally and distally to the joint being studied.
Muscle function is also different in open and closed chain motion. Take, as an example, dorsiflexion of the foot. Open chain dorsiflexion, for example sitting in a chair and pulling the foot upwards, results from concentric action of the anterior tibial muscles. Closed chain dorsiflexion, such as occurs in walking as the bodyweight moves forward over the foot, involves eccentric action of the calf muscles.
Joint movements
Hip joint
The hip joint is the articulation between the head of the femur and the acetabulum. In standing, the femoral head is not completely covered by the acetabulum. This occurs in a position which mimics a quadruped stance, hip flexion to 90°, abduction to 5°, and lateral rotation to 10°. Hip flexion is free, being limited by soft tissue contact, but extension is usually limited to about 20–30°, depending on the amount of anterior pelvic tilt which occurs. Common values for abduction and adduction are 45° each, given a total range of rotation of 90°.
In single leg standing, vertical compression forces of 1.8–3.0 times bodyweight have been recorded at the hip, while in the stance phase of walking, forces between 3.3 and 5.5 times bodyweight have been measured. In running, the forces are higher still. Although the major force on the hip is vertical, anteroposterior forces (AP or ‘shearing’) are still present. At heel-strike and toe off, the AP forces acting on the hip actually exceed bodyweight (Palastanga, Field and Soames, 1998).
Keypoint
In running, compression forces on the hip joint are as much as three times total bodyweight (210 kg in a 70 kg athlete). Shearing forces may exceed total bodyweight.
The hip passes through one flexion/extension movement during the running cycle. The limit of flexion occurs within the middle of the swing phase, and the limit of extension just before the end of the stance phase.
Knee joint
The knee joint articulation is between the condyles of the femur and tibia. The posterior surface of the patella and the patellar surface of the femur is usually considered in the knee complex. The neutral position of the knee is full extension. From this position, approximately 140° of flexion is possible in the average subject. In full extension, no transverse plane motion is possible, but as the knee flexes rotation can occur.
During the last 15° of extension, the femur medially rotates on a fixed tibia, or if the tibia is free it will laterally rotate to bring the bones into close pack formation and lock the knee (the screw home mechanism). Flexion progresses as a combination of rolling and gliding movements of the femoral condyles. At the beginning of flexion, rolling occurs alone, and as flexion increases the amount of gliding increases, until at the end of range, gliding is the only movement present.
Definition
The screw home mechanism is the method by which the knee locks passively into extension. When the foot is on the floor (tibia fixed) the femur medially rotates tightening the knee ligaments and securing the joint.
The medial condyle only rolls for the first 10–15° of flexion, while the lateral condyle continues until 20° flexion, and at the same time the two menisci deform. This range of motion is the amount required during normal gait, and means that the knee is more stable (no gliding movement) during this functional range. Beyond 20° flexion, the knee becomes looser as the part of the femoral condyles now involved in the articulation is smaller. As a result the knee ligaments relax, and a wider range of rotation is available.
During walking, forces between two and four times bodyweight are taken by the knee. Peak forces correspond to hamstring, quadriceps and gastrocnemius contraction, and occur at heel strike and during propulsion. In jumping, forces may approach 24 times bodyweight on the knee (tibiofemoral) joint and 20 times bodyweight on the patellofemoral joint (Palastanga, Field and Soames, 1998). When walking down stairs, the intense eccentric activity in the quadriceps results in joint forces on the patellofemoral joint which are up to six times greater than those seen when walking on a flat surface.
The knee flexes and extends twice during running. At initial contact the knee is extended, and it flexes during mid-stance to absorb shock. As toe-off is reached, the knee extends again to provide propulsion and flexes as part of the swing phase.
Ankle joint
The ankle or talocrural joint consists of the trochlear surface of the talus and the distal ends of the tibia and fibula. The talar trochlea is wider anteriorly, and so plantarflexion is more free than dorsiflexion, average values being 30–50° and 20–30°, respectively. Marked variations occur both between individuals and following injury, and normal foot function can be achieved with as little as 20° of plantarflexion and 10° of dorsiflexion (McPoil and Brocato, 1990).
The ankle is essentially a hinge, externally rotated to between 20 and 25° with the malleoli (Fig. 7.1). In the neutral position, with the foot perpendicular to the lower leg, there is very little frontal or transverse plane motion. With dorsiflexion, abduction of the foot is possible, and during plantarflexion, adduction can occur. In dorsiflexion the broad anterior part of the talus is forced into the narrower mortice between the tibia and fibula. The interosseous and transverse tibiofibular ligaments are stressed, as the bones part slightly, and the joint moves into close pack position.
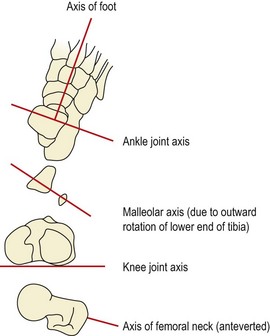
Figure 7.1 Relationship between the ankle, knee and hip joint axes.
From Palastanga, Field and Soames (1998) with permission.
Plantarflexion sees the narrow posterior part of the trochlear surface of the talus moving into the broader tibiofibular mortice. Recoil of the above ligaments causes the malleoli to approximate and maintain contact with the talus.
Keypoint
The trochlea surface of the talus is wider at the front. This wedge shape makes the range of plantarflexion greater than that of dorsiflexion. In addition injury to the talar surface or swelling within the joint is often seen clinically as a marked reduction in dorsiflexion.
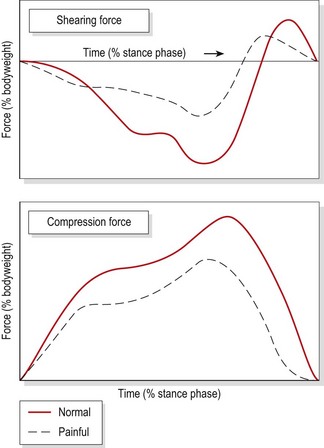
During running, the ankle is dorsiflexed at heel strike, and plantarflexes to bring the forefoot to the ground. Plantarflexion occurs again at push-off, and the foot dorsiflexes throughout the swing phase. As the speed of gait increases, the total range of motion at the ankle decreases, the range reducing by 10% when changing from a cadence of 40 strides/min to one of 60 strides/min. Joint forces at the ankle (Palastanga, Field and Soames, 1998) at heel strike are three times bodyweight for compression and 80% bodyweight for AP shear. At heel lift, muscle force creating the plantarflexion force to lift the body increase compression at the ankle to five times bodyweight (Fig. 7.2). Patients with ankle pain modify their gait pattern to reduce these forces, but in so doing stress other areas of the kinetic chain.
Subtalar joint
The subtalar joint (STJ) lies between the concave undersurface of the talus and the convex posterior portion of the upper surface of the calcaneum. The STJ is said to be in neutral position when the posterior aspect of the heel lies vertical to the supporting surface of the foot, and parallel to the lower one-third of the leg (Subotnick, 1989).
Determining neutral position of the STJ
Neutral position of the STJ is its optimal alignment and this is used as a starting point or baseline to determine foot and leg alignment faults. Neutral STJ position may be obtained in standing, supine lying and prone lying. In standing, the practitioner palpates the head of the talus on the doral aspect of the foot. The athlete then twists the trunk, forcing the tibia to internally and externally rotate. In the neutral position, the head of the navicular bone may be palpated on the medial edge of the foot. The distance between the navicular and the floor should not exceed 1 cm (Mueller, Host and Norton, 1993).
The neutral position is the point at which the head of the talus appears to bulge equally under each palpating finger. In lying (prone or supine), the practitioner grasps the athlete’s foot over the 4/5th metatarsal head and presses the foot into dorsiflexion. Again, the practitioner palpates the head of the talus and swings the foot into inwards and outwards to stop at the point where the talar head seems not to bulge more on one side.
Biomechanics of the STJ
An essential feature of the STJ is its ability to perform triplane motion. This occurs when movement of one joint is in all three body planes, because the joint axis is oblique.
Pronation of the foot is a triplane movement of the calcaneum and foot consisting of calcaneal eversion (frontal plane), abduction (transverse plane) and dorsiflexion (sagittal plane). Supination is an opposing movement of calcaneal inversion, adduction and plantarflexion in the same planes. These are both open chain movements in their pure forms. Functionally, the movements occur in closed chain formation with the foot on the ground. Abduction and adduction cannot occur owing to friction with the floor, and dorsiflexion and plantarflexion will not occur in their pure form as they are no longer free to move. Instead, the talus takes over these movements with supination consisting of calcaneal inversion with abduction and dorsiflexion of the talus, while pronation combines calcaneal eversion with adduction and plantarflexion of the talus (Fig. 7.3).
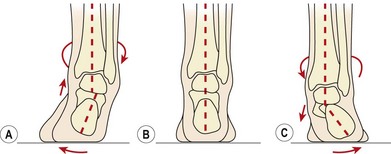
Figure 7.3 Weight-bearing motion of the sub-taloid joint. (A) Supination. (B) Neutral position. (C) Pronation.
From Gould (1990) with permission.
Definition
In the weight-bearing foot, supination (high arched foot) consists of calcaneal inversion with abduction and dorsiflexion of the talus, while pronation (flattened foot) combines calcaneal eversion with adduction and plantarflexion of the talus.
The foot has two important functions during the gait cycle. The first is to act as a mobile adaptor, adjusting to alterations in the ground surface and reducing the shock travelling up to the other lower limb joints. Second, the foot must efficiently transmit force from the muscles of the lower leg to provide propulsion to push off. For this, the foot must change into a rigid lever. These two diametrically opposed functions of mobile adaptor and rigid lever are achieved by changing the bony alignment of the foot joints, and ‘locking’ or ‘unlocking’ the foot.
Mid-tarsal joint
The movement of the STJ alters the alignment of the two components of the mid (transverse) tarsal joint (MTJ). These are laterally the calcaneal cuboid joint, and medially the talocalcaneonavicular joint. The mid-tarsal joint has two axes of motion, one oblique and one longitudinal. The longitudinal axis primarily allows inversion and eversion of the forefoot, while the oblique axis permits adduction/abduction and plantarflexion/dorsiflexion. The direction of the motions at the mid-tarsal joint causes the dorsiflexion force created by weight bearing to lock the forefoot against the rearfoot.
The position of the STJ alters the neutral alignment of the mid-tarsal joint axes (Fig. 7.4B). Supination of the STJ causes the axes to become more oblique (Fig. 7.4C), and less motion can take place. The foot is said to be locked, and acts as a rigid lever ideal for propulsion. Pronation of the STJ causes the mid-tarsal joint axes to become more parallel (Fig. 7.4A), and therefore more mobile. Now the foot is unlocked, and acts as a mobile adaptor capable of accommodating to changes in the ground surface.
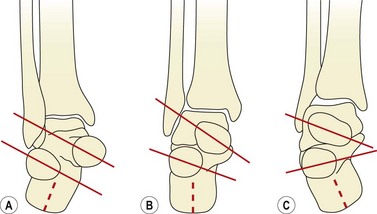
Figure 7.4 Position of mid-tarsal joint axes. (A) Pronation, axes parallel increasing mobility. (B) Neutral. (C) Supination, axes oblique reducing mobility.
From Gould (1990) with permission.
First ray complex
The first ray is a functional unit consisting of the first metatarsal and the first cuneiform. Its axis is at 45° to the sagittal and frontal planes. The joint does have triplane motion, but little abduction and adduction occur functionally. Dorsiflexion of the first ray is accompanied by inversion, and plantarflexion is combined with eversion.
Jumping
A jumping activity usually involves a wind-up period where the body is lowered before the jump is initiated. This period enables the push phase of the jump to last longer and the power for lift off comes from hip and knee extension accompanied by ankle plantarflexion. This leg sequence is reversed to absorb shock as the body lands. The whole jump may be divided into seven phases (Durward, Baer and Rowe, 1999; Fig. 7.5).

In phase 1 the body moves downwards to pre-stretch the extensor muscles of the hip and knee, and the plantarflexors of the ankle. In phase 2 the downward motion of the body decelerates and stops in the lowest position. The negative vertical force of the body dropping is equalled by the positive vertical force of the body coming to a halt in the low position. The two areas are shaded on Figure 7.5. In phase 3 we see the main propulsive action of the body as it accelerates upwards until at phase 4 the body leaves the ground to enter the flight phase. During the flight phase there is no vertical force registered on the force plate because the body is off the ground; there will be some vertical force acting on the body but this will be minimal. Phase 5 sees the body landing with initial contact being made by the foot, and the body and rest of the leg decelerate rapidly. Once the body and leg have flexed to absorb shock, the subject straightens the leg and body to stand upright again (phase 6) and finally comes to a halt (phase 7). In a non-athletic individual, body control is not as skilled, and so additional movements or ‘overshoots’ may appear where the individual tries to regain balance.
The action of flexing or ‘softening’ the legs when landing from a jump greatly affects the forces acting on the body (Fig. 7.6). This occurs especially in ‘drop jumps’ where the body is lowered from a height rather than simply moved upwards in a jumping action. This occurs in plyometrics in sport, and also in daily activities such as stepping down from a kerb or single step. As there is no acceleration phase as with the traditional jump, the body must anticipate the landing surface and prepare accordingly. In a soft landing, flexion of the lower limb attenuates some of the compression forces acting on the body by using the muscles eccentrically as ‘springs’. Where the landing is hard, the time taken to stop is approximately 50% of that of a soft landing (Durward, Baer and Rowe, 1999), so the landing is more abrupt, giving a jolting effect. The combination of shorter time and higher forces in a hard landing makes injury more likely. Athletes performing jumping actions should always be encouraged to use a soft landing ‘going through’ the leg and foot.
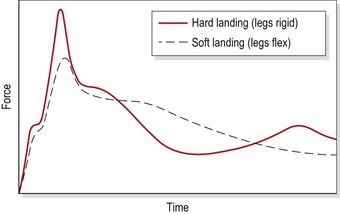
Figure 7.6 Vertical forces on landing from a jump.
Adapted from Durward, Baer and Rowe (1999), with permission.
The gait cycle
The gait cycle can be conveniently divided into two phases. The stance phase occurs when the foot is on the floor, supporting the bodyweight. Closed chain motion occurs in the lower limb, as it decelerates. The swing phase takes place as the foot comes off the ground and open chain motion follows. This time the limb is accelerating.
The foot moves through four positions in three phases during stance. Initially, the heel strikes the ground (contact phase) and as the bodyweight moves forwards, the foot flattens (mid-stance). Forward movement continues and the heel lifts off the ground; finally the toes push off (propulsion) and the leg moves into the swing phase.
At the start of the swing phase the limb is accelerating. In the mid-swing position the speed is constant, and finally the leg decelerates, and is lowered to the ground where heel strike again occurs and the cycle is repeated (Fig. 7.7).
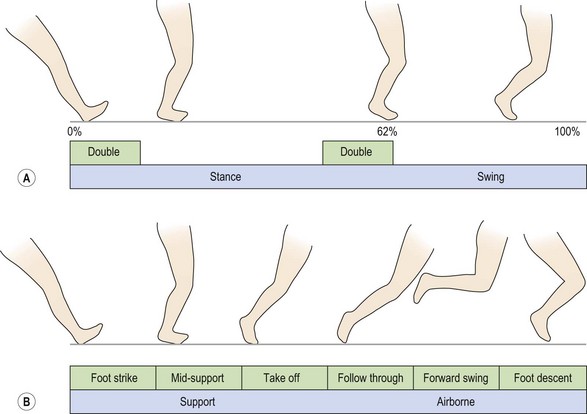
The stance phase in walking is approximately 60% of the total gait cycle, while the swing phase is 40%. Walking at a normal rate of 120 steps/min, the total cycle takes 1 s, so stance occurs for 0.6 s while swing takes only 0.4 s. With running, the movements occur more rapidly, and the stance phase occupies less of the total cycle time. A runner with a pace of 6 min/mile has a total cycle time of only 0.6 s. The stance phase would last for 0.2 s, and so events occurring within this phase are performed three times faster.
During the walking gait cycle, overlap of the stance phases of both legs occurs so that, for a short period, both feet are on the ground at the same time (double leg support). As walking speed increases, the double leg support period reduces. When the stance leg ‘toes-off’ before the swinging leg contacts the ground, double leg support is eliminated and an airborne period is created. Walking has now progressed to running.
Keypoint
In walking both legs remain on the ground for a short period (double leg support). As walking speed increases, double leg support time reduces. When the pace has increased to running, double leg support is eliminated.
Stance phase
During the stance phase, the forces taken by the various areas of the foot will vary from a peak at the heel during the contact phase, to a more gradual and later occurring force curve at the first metatarsophalangeal region at toe-off (Fig. 7.8).

Contact
With the contact phase, the lateral aspect of the calcaneum strikes the ground. The ankle joint is close to its neutral (90°) position, and the subtalar joint is slightly supinated. The hip is flexed to about 30°. The pelvis and the body’s centre of gravity are moving laterally over the weight-bearing leg, producing closed chain adduction of the hip. Total lateral motion of the trunk is 4–5 cm (Whittle, 1996).
The STJ starts to pronate, and the mobility of the mid-tarsal joint is increased. The ankle begins to plantarflex to bring the foot flat onto the ground for mid-stance. Pronation causes the tibia to internally rotate, and this in turn unlocks the knee, allowing it to flex to about 20°, in a movement opposite to the screw home effect. The hip begins to extend and internally rotate and this continues until heel raise.
The anterior tibials contract eccentrically to stop the foot slapping at heel strike, and the posterior tibials decelerate pronation. The quadriceps work eccentrically to allow the knee to bend, and the hamstrings prevent trunk flexion at the hip. Later, the hamstrings work concentrically to extend the hip (closed chain extension). The hamstrings are used in preference to the gluteals here, possibly because they have been prestretched. When the knee bends, the hamstrings can no longer produce hip extension, and the gluteals take over.
The hip abductors work eccentrically to control lateral movement over the supporting leg and then concentrically to pull the bodyweight back again in preparation for the next cycle.
Mid-stance
In mid-stance, the transition of the foot from mobile adaptor to rigid lever occurs. The STJ starts to supinate, reducing mid-tarsal mobility and locking the foot. When hip adduction is completed, closed chain abduction occurs for the rest of the stance phase.
The action of the calf is eccentric to control dorsiflexion and with it forward motion of the body, and the posterior tibials contract concentrically to supinate the foot.
Propulsion
The heel rises with plantarflexion at the ankle and the propulsion phase begins, the knee reaching its point of maximal extension. At toe-off, dorsiflexion again occurs at the ankle to prevent toe drag, and the hip begins to flex. The calf now works concentrically to actively plantarflex the ankle, and the peroneus longus and brevis are eccentric to control supination. The peroneus longus also stabilizes the first ray. The quadriceps work eccentrically to control the knee.
Swing phase
During the swing phase, the maximally supinated STJ moves back to its position of slight supination just before heel strike. The knee continues to flex during the acceleration position of the swing phase, and starts to extend again before heel strike. The hip continues to flex, until it has reached its 30° position to begin the cycle again. The quadriceps continue to contract eccentrically to stop the knee ‘snapping’ back, and the hip flexors are concentric to accelerate the leg forwards. Phasic muscle action during running is summarized in Figure 7.9.
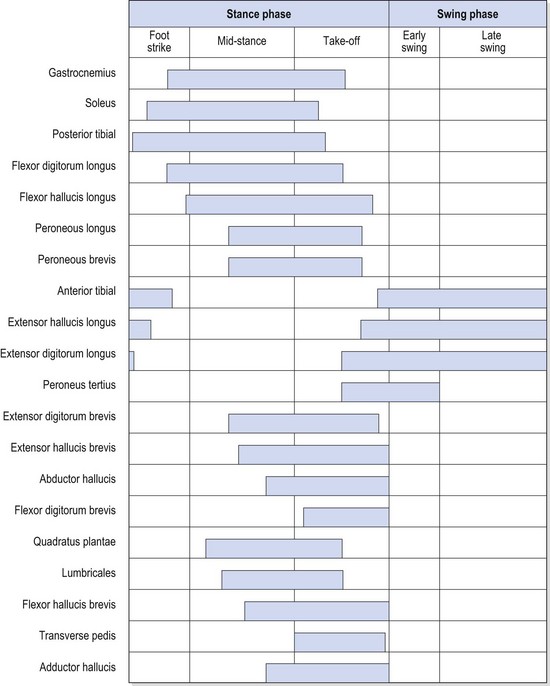
Figure 7.9 Phasic muscular activity during normal ambulation.
From McGlamry (1987), with permission.
Abnormal gait patterns
Several abnormalities of gait are commonly seen in clinical practice, and the reader is referred to Whittle (1996) and Magee (2002) for a more detailed description.
Painful and stiff leg gait
Painful (antalgic) gait and stiff leg (arthrogenic) gait patterns are among the most common walking patterns seen following injury. In the antalgic gait the patient tries to reduce pain by altering his/her walking pattern. The stance (weight-bearing) phase of the affected leg is shortened as the patient tries to take the weight off the leg as quickly as possible. The swing phase of the unaffected leg shortens, the patient attempting to get this leg back on the ground as quickly as possible so that it can again take the weight off the painful side. The overall effect is that the step length on the affected side is reduced. Where the hip is the source of pain, the bodyweight is often shifted over this side to reduce the leverage effect of the hip abductors and so reduce the consequent compression forces on the femoral head.
With an arthrogenic gait, the affected leg is unable to flex during the gait cycle. This may be a result of either knee or hip pathology or simply following immobilization. Four gait changes may occur as a consequence (Table 7.1) Circumduction, hip hiking and high stepping are all modifications of the swing phase. Vaulting is a modification of the stance phase (Whittle, 1996). Circumduction involves swinging the leg out to the side to clear the ground, and is best noticed by viewing the subject from behind. Where weakness of the hip flexors is present, circumduction will move the leg forwards via action of the hip abductors. Hip hitching (hiking) achieves ground clearance by lifting the pelvis on the side of the moving leg (the opposite of the Trendelenburg gait). Often, this pelvic lift is accompanied by excessive pelvic rotation to thrust the leg forwards. High stepping gait sees an increase in both knee and hip flexion to exaggerate the ground clearance. This is especially common in patients with foot drop. Finally, vaulting increases ground clearance by lifting onto the toes of the support leg, and therefore increasing the vertical displacement of the body.
Table 7.1 Changes seen in stiff leg gait patterns
| Fault | Characteristic |
|---|---|
| Circumduction | Swinging the leg out to the side to clear the ground |
| Hip hitching | Lifting the pelvis on the side of the moving leg |
| High stepping | Increase in both knee and hip flexion to exaggerate ground clearance |
| Vaulting | Lifting onto the toes of the support leg |
Trendelenburg gait
One of the most universally recognized faults is the Trendelenburg gait. An excessive lateral flexion of the trunk occurs to reduce forces on the hip joint and hip abductor muscles. During normal standing, the weight of the body is taken evenly on both legs (Fig. 7.10A) and the weight of the legs passes through the ground. As one leg is lifted, the bodyweight and the weight of the opposite leg must be taken by the weight-bearing leg (Fig. 7.10B). If the trunk is laterally flexed towards the weight-bearing leg, the reduction in leverage forces enables the hip to be stabilized by less abductor force, and the resultant compression over the hip joint itself is reduced (Fig. 7.10C). The Trendelenburg gait is typically seen as a result of a painful or abnormal hip joint, weakness of the hip abductor muscles (especially gluteus medius) or unequal leg length.
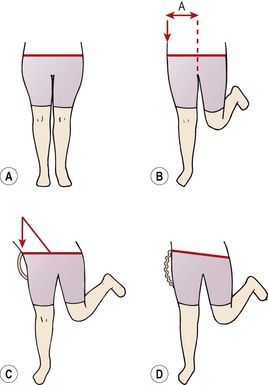
Figure 7.10 Trendelenburg gait. (A) Normal standing. Even weight distribution between both legs. (B) Normal single-leg standing. (C) Trunk lateral flexion eliminating lever arm. (D) Weak hip abductors allow pelvis to dip.
Where weak abductors are present, the Trendelenburg sign may be seen (Fig. 7.10D). As one leg is lifted, the hip abductors of the supporting leg are unable to maintain the neutral position of the pelvis. As a result, the pelvis dips towards the lifted leg. When evaluating a patient with a positive Trendelenburg sign, further information can be obtained by initially observing weight transfer from one leg to the other without lifting the leg to see if the pelvis dips and/or the trunk laterally flexes. In addition endurance of the hip abductor muscles may be assessed using single leg standing. Adequate muscle endurance and control would be indicated by an ability to maintain the horizontal level of the pelvis (no pelvic dip) for 20−30 seconds.
Trunk angulation
Excessive trunk bending in the sagittal plane is normally a result of inadequate muscle control in the knee and hip. During the normal stance phase, the line of force (gravity line) passes behind the knee joint axis, producing a flexion moment (Fig. 7.11A). This must be resisted by the quadriceps to maintain stability of the knee. If the quadriceps contraction is inadequate (either in terms of force generation or timing), the subject flexes the trunk at the hip to move the bodyweight anterior to the knee joint axis, and so eliminate the flexion moment (Fig. 7.11B). Similarly, the line of force during early stance passes in front of the hip joint axis, tending to flex it. This moment is normally resisted by the hip extensors. At heel strike, the hip extensors work to pull the hip back and in so doing propel the body forwards by pushing the pelvis through. Where the hip extensors (especially the gluteus maximus) are weak, the trunk will be thrust back to bring the line of force posterior to the hip joint axis (Fig. 7.11C). The other cause of posterior trunk bending is an increased lordosis due to hip flexor tightness.
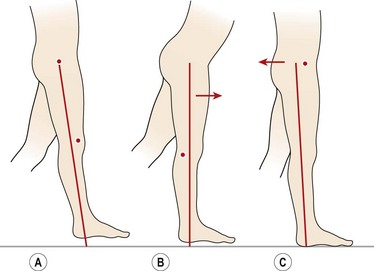
Figure 7.11 Trunk angulation during gait. (A) Normal stance phase. Knee joint axis in front of force line, hip joint axis behind. (B) Flexing the trunk brings the force line anterior to the knee axis. (C) Extending the trunk moves the force line posterior to the hip axis.
Adapted from Whittle (1996), with permission.
Abnormal biomechanics of the foot
Excessive pronation/supination
These conditions occur if the normal pronation and supination periods of the gait cycle are extended, or when there is a change in the angulation of the foot segments. Causes may be extrinsic, such as tight muscles or abnormal lower leg rotation, or intrinsic, as occurs with fixed deformities of the STJ and MTJ.
Severe pronation causes foot flattening. The range of motion at the STJ is increased, making the mid-tarsal joint axes more parallel and unlocking the foot. The foot can then remain pronated and mobile after the stance phase, hence the terms ‘hypermobile’ or ‘weak’ foot.
With excessive supination, the MTJ is locked, the foot is more rigid and the arch higher (cavus). In time the plantar fascia and intrinsic foot muscles become tight, reducing the capacity of the foot to dissipate shock.
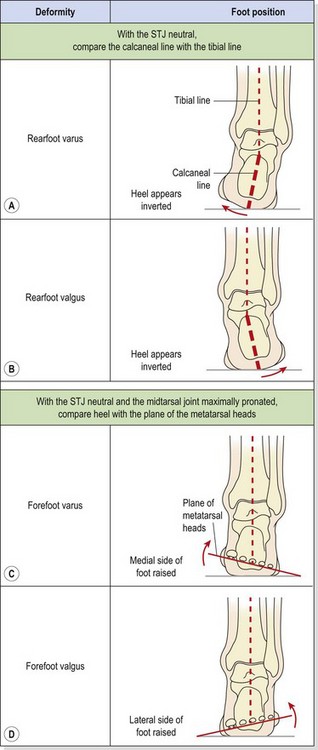
Rearfoot varus
The rearfoot and forefoot can both move outward (valgus) or inward (varus) giving the four alignment faults shown in Table 7.2. The first is rearfoot varus. With this condition, the calcaneus appears inverted when the foot is examined in the neutral position. Left uncompensated the forefoot would invert and leave the medial side of the foot off the ground. To compensate, the STJ pronates excessively on ground contact. This deformity has been associated with an increased number of lateral ankle sprains (Weil, 1979).
Table 7.2 Biomechanical changes in the rearfoot and forefoot
Rearfoot varus is usually a result of developmental abnormality. From the eighth to twelfth fetal week the calcaneum lies at the side of the talus. As the fetus develops, the calcaneum rotates to a more plantar position, so that it lies below the talus. However, the calcaneus may not be completely perpendicular to the ground until the child is 6 years old, and in some cases the rotation is never complete. In addition to the subtalar deformity, the condition is also associated with tibial varum.
Rearfoot valgus
This condition can occur if the calcaneum rotates excessively in its development, or following a Pott’s fracture. The posterior surface of the calcaneum will appear everted, and the foot will hyperpronate, giving a severe flatfoot. The condition is associated with genu valgum (knock knees) and the medial longitudinal arch appears flattened.
Forefoot varus
In this deformity (see Table 7.2) the forefoot is inverted in respect to the rearfoot, when the STJ is in a neutral position. To compensate, and bring the forefoot to the ground, the STJ everts and the entire plantar surface of the foot becomes weight-bearing, flattening the medial longitudinal arch. The head of the talus bulges proximally to the tuberosity of navicular. Plantar calluses are apparent over the second and third metatarsal heads, and an associated hallux valgus deformity may be present.
If the STJ is unable to pronate sufficiently, the entire plantar surface of the foot will be unable to touch the ground. Weight bearing will therefore be lateral, with callus formation this time over the fourth and fifth metatarsal heads.
Abnormal pronation continues into the propulsive phases of the gait cycle, and the foot tries to push off without becoming a rigid lever. This instability causes shearing forces between the metatarsal heads, giving rise to associated pathologies. Interdigital neuroma, postural fatigue, fasciitis, chondromalacia and shin pain have all been described as resultant to this deformity (McPoil and Brocato, 1990).
Forefoot valgus
Here, there is an eversion of the forefoot in relation to the rearfoot, a situation exactly opposite to that above. The medial foot structures are in contact with the ground while the lateral side is suspended. Deformities greater than 6° (McPoil and Brocato, 1990) will require STJ and MTJ compensations. To place the foot flat on the ground, the calcaneus will invert pulling the talus into an abducted-dorsiflexed position. During the contact phase of gait, the foot will pronate more than normal, and remain pronated and therefore mobile into the propulsive phase. Symptoms associated with hypermobility of the metatarsophalangeal and interphalangeal joints occur.
Plantarflexed first ray
This condition is present when the first metatarsal lies below the level of the other metatarsals in neutral position, causing the forefoot to appear slightly everted relative to the rearfoot. When forefoot eversion continues, a forefoot valgus is present.
Various conditions may give rise to this problem. If the first metatarsal phalangeal (MP) joint is rigid (hallux rigidus) the foot is forced rapidly into supination (a supinatory rock) to allow the lateral side of the foot to bear weight. In so doing, the fifth metatarsal head strikes the ground rapidly (Wernick and Langer, 1985). In addition, weakness of the tibialis anterior will allow the peroneus longus to pull the first ray into plantarflexion unopposed. Deformity occurs over time, and is particularly exaggerated in certain neuromuscular diseases.
Biomechanical examination and treatment
Examination of the lower limb may reveal problems with the spine, pelvis, hip or knee. The aim of this section, however, is to deal with the examination of the limb in relation to foot problems, assessment procedures for the other body parts being covered in the sections describing injuries to these areas. Equally, foot examination in isolation is not enough. Forces acting through the kinetic chain, and referral of pain from other structures, make holistic evaluation of lower limb function essential.
Subjective examination and inspection of the lower limb will act as pointers to further assessment, and give clues about any additional tests which may be required.
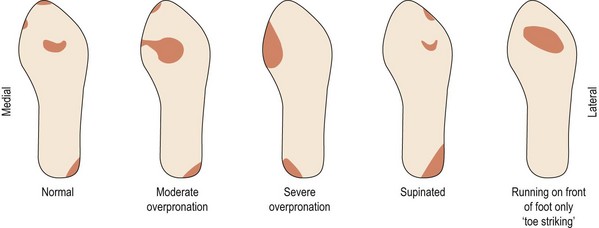
Objective examination is made both with the athlete weight bearing and then non-weight bearing. Positions include standing, sitting, walking and then running. With walking and running, video analysis is often used to slow the motion down and aid in the identification of faults. In each case the examination may be carried out with the athlete in shorts and bare feet, and then while wearing their normal training shoes. The wear pattern of the shoes (Fig. 7.12) is often a useful general guide to the existence of underlying biomechanical faults.
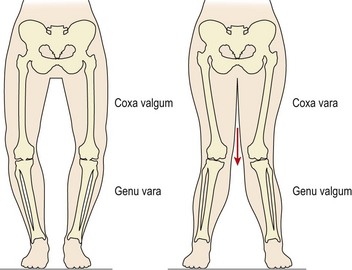
In standing, the alignment of the various body segments is assessed. Starting from the top of the body and working down, viewed from behind, the head and shoulder positions are noted, as is the symmetry of the spine. Shoulder and pelvic levels are assessed. Buttock and knee creases are examined for equal level. Knee position gives a clue to the presence of coxa valga/vara and genu vara/valga (Fig. 7.13).
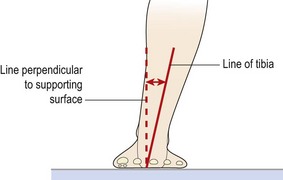
Tibial vara can be measured in standing by comparing the line of the distal third of the leg to a line perpendicular to the supporting surface which passes through the posterior contact point of the calcaneus (Fig. 7.14).
From the front, similar comparisons of shoulder, pelvic, spinal and leg alignments are made. The position of the patella relative to the foot will suggest any tibial torsion. Tibial torsion can be further assessed with the patient in sitting with the knee flexed to 90° over the end of the couch. The examiner places his or her thumbs over the patient’s malleoli and compares an imaginary line connecting these two points with the knee axis.
In supine lying, active and passive range of movement at the knee and hip are measured and any asymmetry or alteration in normal end-feel is noted. Resisted strength is measured and limb girths measured. The distribution of any pain or alteration in sensation is mapped. The appearance of the foot is observed and any skin abnormalities noted. In prone lying, range of movement of the foot is measured and compared to normal values.
Calcaneal inversion and eversion are measured by marking a line bisecting the back of the calcaneus (calcaneal line) and comparing this to a line bisecting the calf and Achilles (tibial line).
Definition
The tibial line joints two points on the midline of the lower third of the tibia. The calcaneal line joints the midpoint of the calcaneus at the insertion of the Achilles with a midpoint 1 cm distal to this point.
Forefoot position is assessed by placing the STJ in its neutral position. A goniometer is then placed over the metatarsal heads, and its line compared to one perpendicular to the line of calcaneal bisection. Alternatively, a forefoot measuring device (FMD) may be used. This has a slit which is placed over the line of calcaneal bisection, the plateau on the front of the FMD is placed over the plantar surface of the foot in line with the met heads, and a value for forefoot–rearfoot alignment read from the scale. Using both goniometry and the FMD, the most common forefoot–rearfoot relationship is one of varus, with average values being 7.5° (Garbalosa, Donatelli and Wooden, 1989).
Significant biomechanical faults of the foot can be managed by using a functional orthotic device.
Orthotics
An orthotic device is usually made after taking a plaster impression of the foot in the neutral position. This may be sent to an orthotic laboratory where a device is fabricated according to the practitioner’s prescription and laboratory assessment of the cast. Alternatively, a number of temporary heat moulded orthotics are available which have the advantage that they are fitted in the functional standing (weight-bearing) position.
The orthotic aims to alter the mechanical functioning of the foot, and so is more than a simple arch support. When worn, the device changes the foot’s alignment to make the lower limb function more normally. There are generally few long-term benefits, and much like with a pair of spectacles, once the orthotic is removed, the body returns to its previous state.
Durward B., Baer G., Rowe P. Functional Human Movement. Oxford: Butterworth-Heinemann; 1999.
Garbalosa J.C., Donatelli R., Wooden M.J. Dysfunction, evaluation and treatment of the foot and ankle. In: Donatelli R., Wooden M.J., editors. Orthopaedic Physical Therapy. London: Churchill Livingstone; 1989:533-553.
Gould J.A. Orthopaedic and Sports Physical Therapy, second ed. St Louis: Mosby; 1990.
McGlamry J.G. Fundamentals of Foot Surgery. Baltimore: Williams and Wilkins; 1987.
McPoil T.G., Brocato R.S. The foot and ankle: biomechanical evaluation and treatment. In: Gould J.A., editor. Orthopaedic and Sports Physical Therapy. second ed. St Louis: Mosby; 1990:293-321.
Magee D.J. Orthopedic Physical Assessment, fourth ed. Philadelphia: W.B. Saunders; 2002.
Mueller M.J., Host J., Norton B. Navicular drop as a composite measure of excessive pronation. Journal of the American Podiatric Medical Association. 1993;83:198-202.
Palastanga N., Field D., Soames R. Anatomy and Human Movement, third ed. Oxford: Butterworth-Heinemann; 1998.
Reid D.C. Sports Injury Assessment and Rehabilitation. London: Churchill Livingstone; 1992.
Subotnick S.I. Sports Medicine of the Lower Extremity. London: Churchill Livingstone; 1989.
Weil L.S. A biomechanical study of lateral ankle sprains in basketball. Journal of the American Podiatry Association. 1979;69:687.
Wernick J., Langer S. A Practical Manual for a Basic Approach to Biomechanics. Stoke-on-Trent: Langer Biomechanics Group; 1985.
Whittle M.W. Gait Analysis, second ed. Oxford: Butterworth-Heinemann; 1996.