12 Thai massage and neuromuscular technique
In his book The Human Machine and Its Forces published in 1937, Dr. Dewanchand Varma says:
We have discovered that the circulation of the nervous currents, slows down occasionally because of the obstruction caused by adhesions; the muscular fibres harden and the nervous currents can no longer pass through them. We have demonstrated effective and positive methods designed to restore nervous equilibrium which promotes the healthy circulation of blood, so that new tissues begin to be built up again
Based in Paris, Dr. Varma practised a form of soft tissue manipulation which he called ‘Pranatherapy’. This was derived from Ayur-veda, the traditional medical system of India, Dr. Varma’s homeland. His system was to become one of the sources of what we now know as neuromuscular technique (NMT).
Stanley Lief, who had trained in America as a chiropractor and naturopath, heard of Dr. Varma’s work and travelled to Paris to receive a series of treatments from him. Lief was so impressed by the results that he persuaded Varma to teach him his system. With the help of his cousin and assistant, Boris Chaitow, Lief further developed and refined the techniques and coined the name ‘neuromuscular technique’ (Chaitow 2003, pp. 32–33).
When I studied NMT in 1995 with Leon Chaitow, Boris Chaitow’s nephew, I was intrigued by the way in which aspects of neuromuscular technique resonated with Thai massage, a system I had already been practising for three years. Around the same period I also discovered the work of Ida Rolf and experienced its practical application in the form of ten sessions of ‘Rolfing’. These two influences began to inform my understanding of Thai massage which, back in the nineties, was taught as a practical work with very little theory.
Thai massage – past and present
In common with Dr. Varma’s ‘Pranatherapy’, Thai massage is said to derive from Indian Ayur-vedic medicine; Jivaka Kumar Bhaccha, a North Indian physician, is generally regarded as the father of Thai medicine. The Foundation of Dr. Shivaga Komarpaj in Chiang Mai preserves his name in its Thai version. The foundation runs the Old Medical Hospital where it has offered short courses in Thai massage since 1962.
Jivaka Kumar Bhaccha was a member of the community (sangha) that gathered around the Buddha 2500 years ago. According to an account in the Vinaya Pitaka, a Theravadin document that records the life of that original sangha, Jivaka’s father was King Bimbisara, a contemporary of the Buddha, and the ruler of the Magadha Empire in North India. Jivaka’s mother was the wife of a merchant who fell for the charms of the king while her unfortunate husband was away on business. Soon after his birth Jivaka was taken by his mother to the king and was raised in the royal household.
As a young man Jivaka realized that medicine was to be his vocation. With his father’s permission he went to study under Atreya, the renowned Rishi physician. Atreya was the personal physician to King Bimbisara’s father, Padma dPal. The years of study bore fruit and Jivaka stood out as the most brilliant student in his class. He quickly developed a reputation as a great physician and his pride grew to match his fame. He is said to have boasted that nobody could cure a somatic disorder, as could he; just as nobody could cure a psychological disorder, as could the Buddha. In time, like many of his contemporaries, Jivaka went to the Buddha to learn the path by which he could free himself from his suffering (Rapgay 1981).
It is generally believed that Jivaka’s name and the medical system he practised came to Thailand with the teachings of the Buddha, although it is not known exactly when that was. Some accounts suggest that Asoka, India’s first Emperor, sent missionaries in the second century BC. Asoka embraced Buddhism in response to the terrible cruelty he saw during the conquest of Kalinga and came to be known as ‘The Prince of Peace’ (Kinder & Hilgemann 1978).
A stone inscription from 1292 AD records the declaration of Rama Khamheng, King of Siam, that Buddhism be recognized as the country’s official religion (Gold 2007, p. 65). Beyond that little more is known. When the Burmese invaded Thailand in 1767 they destroyed the old royal capital of Ayutthia and with it most historical and medical texts.
In 1832 King Rama III gathered what fragments of the medical texts survived and had them carved on stone and set into the walls of Wat Pho, the main Buddhist monastery in Bangkok. These carvings comprise 60 figures and are said to indicate treatment lines and points on the human body along with explanatory notes (Brust 1990, p. 5).
Until the late 1980s Thai massage was little known outside of Thailand. Even within the country the traditional medical system to which the massage belonged was losing favour. In common with many of its Asian neighbours, Thailand was embracing a Western model of industrial and economic development and the modern medical system it brought with it.
Thai massage is now enjoying a new lease of life in Thailand as well as finding its way into massage centres and hotel spas around the world. This revival owes much to the interest shown by Western travellers, some of whom found their way to the traditional massage schools or studied directly with village massage practitioners. Lacking the necessary language skills they learned Thai massage as a practical study with little theory to explain the techniques. Despite, and possibly because of this lack of theory some of these early Western students discovered an affinity with the practice and went on to become teachers themselves.
Between the late 1980s and the present day much has changed in the world of Thai massage. There are now many more schools offering courses in Thailand as well as around the world. There is now an abundance of books on the subject. ‘Thai Reflexology’ and ‘Thai Head Massage’ have emerged as standalone therapies. Even aspects of Thai herbal medicine have entered the mainstream and it is now quite common to see the use of ‘Thai herbal compresses’ in hotel spas. Despite the global reach of Thai massage there has been little development in understanding the medical system to which the massage belongs.
We do know that Thai massage is one of the three branches of traditional Thai medicine; the others being naturopathic medicine and spiritual practices. Traditional Thai medicine is intimately entwined with Theravada Buddhism, the esoteric and monastic branch of Buddhism practised in Southeast Asia and Sri Lanka. In Thailand this traditional medicine is still typically offered under the auspices of the Buddhist monastic community.
Given that Thai massage is but a small part of a Buddhist approach to medicine it is, perhaps, not so surprising that our knowledge is so limited. Buddha taught Jivaka Kumar that the cause of all suffering, whether physical or mental, is the greed, anger and ignorance generated by the unenlightened mind. Although traditional Buddhist medicine includes naturopathic remedies and physical therapy, of far greater importance is the spiritual teaching and practical guidance offered by the lama physicians of the monastic community. Buddhist medicine is taught within the broader context of Buddhist philosophy and medical intervention is similarly prescribed.
Although some Westerners have made the effort to learn the Thai language and explore more deeply Thailand’s culture and religion I am not one of them. For this reason, in this discussion of Thai massage, I will disengage it from its spiritual context and look at it exclusively as a form of bodywork. We will see that in the West, although Thai massage carries with it no more than a fragment of the medical system to which it belongs, in this may lie its strength. Freed from the weight of a substantial theoretical foundation and from the rigour to be expected of a medical system it nevertheless stands its ground as an excellent massage technique. We will seek here to understand why.
Sen, nadi, meridian, myofascial pathway?
There are three main activities involved in the practice of Thai massage:
• the manipulation of treatment lines known as ‘sen’
• the application of passive stretches and postures derived from Hatha Yoga
• the induction of a deep ‘meditation-like’ relaxation in the patient.
The balance of these three activities is quite individual and the massage will vary considerably depending on the massage practitioner’s preferences. Some massage practitioners are more attracted to the yoga aspects of the work and offer quite dynamic massage sessions. Some are drawn more to the stretches, and practise Thai massage with a ‘no pain, no gain’ style similar to that found in sports massage. My own approach to Thai massage focuses mainly on the manipulation of the sen and inducing relaxation. This is the style encouraged by my teachers, both of whom studied at the Old Medical Hospital in Chiang Mai.
The ‘sen’ are the lines documented in the stone carvings of Wat Pho. It is said that these carvings refer to a network of 72 000 lines or channels permeating the body. Ten of these are used for massage. These are known as the ‘ten sen’. In addition to the sen, the stone carvings of Wat Pho also record descriptions of treatment points.
When I first studied Thai massage in 1992, as well as diagrams of the sen, we were given others indicating treatment points on the hands, feet and face. These looked to me like Chinese acupressure and Western reflexology charts. There was little information to explain their use so I disregarded them and concentrated my efforts on the manipulation of the sen.
Asokananda (AKA Harald Brust), with whom I studied advanced Thai massage in 1995, says of treatment points: ‘Thai massage never developed a standardised set of points but therapy always was and is centred around intensive and complete line work’ (Brust 1996, p. 18). If we accept, therefore, to leave aside the idea of treatment points we are left with a simple massage based around the manipulation of treatment lines.
Even though it is said that there are ten main sen used in Thai massage this is actually open to debate. The ten sen are known as: sen sumana, sen ittha, sen pingkhala, sen kalathari, sen sahatsarangsi, sen thawari, sen lawusang, sen ulangka, sen nanthakrawat and sen khitchanna. However, sen lawusang and sen ulangka follow the same path but on the left side and right side of the body. The same goes for sen thawari and sen sahatsarangsi and for sen ittha and sen pingkhala. In all we really only find seven unique pathways.
The story is further confused by the fact that Thai massage only uses aspects of the sen mentioned above and there are many differences of opinion as to where these aspects run. This lack of clarity leads many Western Thai massage practitioners to other systems for the theory to support their practice. These include traditional Chinese medicine, Ayur-vedic medicine and Hatha Yoga, each of which incorporates a system of lines or channels with some similarities to the sen.
Sen and Chinese meridians
Of these traditional systems the best known in the West is traditional Chinese medicine (TCM). TCM is based on a Western anatomical model but with the addition of acupuncture channels and acupuncture points. The channels are used to describe the interconnection of the various functional systems of the body. In TCM however, there are not 7, nor 10 but 14 main channels. There are, in addition, numerous secondary channels. These include connecting channels, muscle channels and cutaneous regions. The connecting channels branch further into minute connecting channels, blood connecting channels and superficial connecting channels (Maciocia 1991). These form an intricate web involved in the distribution of fluids and energies throughout the body. Although there is no specific reference to 72 000 channels in TCM it is quite likely that this web of channels does have something in common with the system of sen referred to in traditional Thai medicine especially when we consider that both systems are thought to originate from around 2500 years ago.
Often, Western writers who liken the sen to acupuncture channels also generalize Thai massage as a form of ‘energy work’ similar to Japanese shiatsu or Chinese acupressure (Mercati 1998, Brust 1990, p. 6, Gold 2007, p. 12). From my own studies in traditional Chinese acupuncture with JR Worsley in the early 1980s I could recognize some similarities between the sen used in Thai massage and the channels used in acupuncture. However this is a perilous comparison. What it reveals are major shortcomings in our knowledge of the sen. In Thai massage there is no sense of a complete system of sen comparable with acupuncture channels and there is no system of diagnosis with which to justify the term ‘energy work’.
Sen and Ayur-vedic nadis
Another common source of information used to explain Thai massage is to be found in India. Here in the homeland of Jivaka Kumar, patron of traditional Thai medicine, a vast historical record exists in the form of the Upanishads and the Vedas. These document the development of the medical and spiritual system that forms the basis of the Hindu and Buddhist religions. The oldest Upanishads, the Brhadaranyaka and the Chandogya, have been dated to the eighth century BC while the Vedas date from 1000 BC (Milne 1995).
Ayur-veda, a naturopathic approach to medicine still practised in India today, dates from the Vedic Period (1800–1000 BC) and is thought to be the source of traditional Thai medicine. The oldest existing encyclopaedic medical work is the Sushruta-Samhita. Although much of this work was completed in the early Christian era, parts of this collection are pre-Buddhist (Feuerstein 1990, p. 88).
Hatha Yoga, the style of yoga practice most familiar in the West, is documented in a series of Upanishads written between the sixth and fourteenth centuries AD. This period saw the birth and development in India of the philosophy of Tantrism, the aim of which was ‘to overcome the dualism between the ultimate Reality (Self) and the conditional reality (ego) by insisting on the continuity between the process of the world and the process of liberation or enlightenment’ (Feuerstein 1990, p. 251).
Although for many Westerners Hatha Yoga represents little more than a system of exercise, for its founders it was the distillation of centuries of research. The result is a psycho spiritual system designed to integrate the spiritual life with the physical reality of the body. Hatha Yoga means ‘yoga of the force’ and its aim is nothing less than ‘the blissful state of ecstatic merging with the Divine’ (Feuerstein 1990, p. 246).
In the Yoga-Upanishads we find reference to ‘nadis’, the Ayur-vedic equivalent of the sen. The renowned, contemporary Hatha Yoga teacher, BKS Iyengar, refers to the nadis as channels ‘through which nervous energy passes’ (Iyengar 1984, p. 117). In common with the Thai system, some of the Yoga-Upanishads refer to 72 000 nadis. Others, however, refer to 350 000. Similarly, some refer to ten important nadis but others refer to fourteen or fifteen (Motoyama 2003, p. 135).
There are other similarities between the Thai sen and the Ayur-vedic nadis. In both systems three channels are considered to be particularly important. In Thai massage they are sen sumana, sen ittha and sen pingkhala. In Ayur-veda they are sushumna-nadi, ida-nadi and pingala-nadi. As well as the similarity of name, sen ittha and ida-nadi are in both systems symbolized by the moon and associated with the feminine quality while sen pingkhala and pingala-nadi are symbolized by the sun and associated with the masculine quality.
Hereafter we discover more differences than similarities. For instance, in the Thai description, sen sumana starts at the navel and ascends inside the throat, terminating at the base of the tongue. Sen ittha and sen pingkhala are described as lines that run either side of sen sumana and then continue down into the legs. In the Yogic tradition these lines are usually depicted as a caduceus; sushumna-nadi forms a central core while ida-nadi and pingala-nadi weave a double helix, intersecting sushumna-nadi at a series of seven centres along the vertical axis of the body. In Sanskrit these centres are called ‘chakras’, meaning wheel or vortex. They are thought to relate to nerve plexuses (Motoyama 2003, pp. 197–198).
According to the Yogic tradition, sushumna-nadi means ‘the current that is most gracious’ (Feuerstein 1990, p. 260). BKS Iyengar calls it the nadi of fire and locates it inside the spinal column. He says it is the main channel for the flow of nervous energy (Iyengar 1984, p. 439). Although there are some variations, most traditional Yogic sources agree that sushumna-nadi begins at the perineum and continues up to a point called ‘Brahman Gate’ at the top of the head (Motoyama 2003, p. 141).
The Yogic tradition goes still deeper, identifying within sushumna-nadi another channel called vajra-nadi and within that yet another called citrini-nadi (Feuerstein 1990, p. 260). According to the Shat-Chakra-Nirupana, written in 1577 by a Bengali guru known as Purananda there is within citrini-nadi yet another called the Brahma-nadi (Motoyama 2003, p. 164).
It soon becomes clear when reviewing Yogic literature that the nadis are part of a complete and complex system involved not only in medicine but also in the development of consciousness. What we know of this system in the West is generally limited to the practice of yoga asanas. According to the Yoga Sutras, compiled some time between the second century BC and the second century AD by Patanjali, the asanas are but one of the eight disciplines of Yogic practice. Hiroshi Motoyama, a Japanese Shinto priest, veteran yoga practitioner and scientist says of this practice:
There are those who may claim that it is too grandiose a wish for us humans to become more than human. But it must be stated that this wish is neither impossible nor too dangerous, as long as the correct practices are performed without error. It should also be added that the guidance of a qualified teacher is essential in case difficulties are encountered along the way
Sen and myofascial pathways
In 1990 Dick Larson, an acupuncturist and Rolfer, wrote a paper discussing the link between the fascial planes used in Rolfing and the channels used in acupuncture. According to Larson, the ancient Chinese were well aware of the significance of connective tissue and its relationship to acupuncture meridians. During the Han Dynasty (206 BC–220 AD) ‘Prince Mang ordered physicians and butchers to perform surgery on live political prisoners to measure their organs and to establish the source and route of blood vessels’ (Larson 1990, p. 25). Larson suggests that the writers of the Qing Dynasty (1644–1912) further clarified this relationship and described a system whereby, ‘the meridians themselves are recognised as flowing through the superficial fascia of the body’, and:
The system of branches which come out from the meridians run through the entire body, just as the superficial fascia does. Thus, when the branches ‘spirally wrap’ the paired organs, they permeate the fascial envelopes that encircle the organs
Larson refers to the earlier work of another Rolfer, Stanley Rosenberg, who in 1986 suggested that:
… the acupuncture meridians are a map of the planes of fascia. By putting my hands on the meridians in certain ways (other than traditional acupressure), I can produce some predictable improvements in structure, easily and with little effort
Ida Rolf had already sensed this connection herself, although she related it to reflexology rather than to acupuncture. In her book ‘Rolfing’, originally published in 1977, she says:
Many people are aware that reflex points can be found on the sole of the foot. When individual visceral organs become congested, pressure on a specific point on the sole elicits pain, sometimes intense in quality … In such reflex situations, fascial planes may be the route of mechanical transmission
Kiiko Matsumoto and Stephen Birch, who were studying the relationship between acupuncture channels and connective tissue in the 1980s, suggest that: ‘Perhaps the fascia, the tissues that cover and line the body and organs, have some special qualities, properties or functions that were recognised by the medical authors of the Han Dynasty’ (Larson 1990, p. 26).
Fascia (and, more generally, connective tissue) does indeed have some special qualities. The first is that it provides a physical means of communication from the outside of the body to the heart of every cell and from the heart of every cell to the heart of every other cell. Each individual cell contains a connective tissue cytoskeleton that provides a framework of support, structure and communication for the various cellular and nuclear elements within. Proteins called integrins reach out from the cytoskeleton, across the cell surface to the surrounding connective tissue matrix. At the outermost layer of the skin, tonofilaments reach in from the epidermis and are attached via hemidesmosomes to the dermal connective tissue. From here, anchoring fibrils link in to the connective tissue matrix (Oschman 2000, pp. 45–47). Thus do we find a route from the massage practitioner’s hands to every cell of the patient’s body.
Another of the special qualities of connective tissue is the presence of collagen fibres within the matrix of ground substance, fibres and cells. Collagen is the ‘longest molecule that has ever been isolated’ and is ‘stronger in tensile strength than steel wire’ (Juhan 2003, p. 72), qualities ideal in its role of providing support and connectivity in the body. Collagen is also hollow, which suits its role in circulation and communication. James Oschman, a researcher into ‘energy medicine’ talks of life energy as ‘bioelectric, biomagnetic, biomechanical, and bioacoustic signals moving through collagen fibres, ground substance, and associated layers of water molecules’ (Larson 1990, p. 25).
Curiously, it has been shown that within the collagen tubule is not only, as we might expect, lymph or ground substance but also cerebrospinal fluid (Juhan 2003, p. 73). This phenomenon provides evidence of an extraordinary communication from the sources of cerebrospinal fluid in the ventricles in the middle of the brain to, potentially, every cell in the body; a point not lost on craniosacral therapists who consider cerebrospinal fluid to be the carrier of the ‘breath of life’.
Fascia is the general name for the dense irregular connective tissue layer surrounding muscles, bones, and joints. It consists mainly of randomly arranged collagen fibres within the ground substance. It provides support and protection and gives structure to the body. Ida Rolf says of it, ‘fascia forms an intricate web coextensive with the body, central to the body, central to its well-being, central to its performance. Clearly fascial tone, fascial span, is a basic contributing factor to bodily well-being’ (Rolf 1989, p. 39).
Fascia consists of three layers: the superficial, the deep and the subserous. The superficial fascia is located directly under the subcutis of the skin. Its functions include the storage of fat and water and it provides passageways for nerves and blood vessels. In some areas of the body, it also houses a layer of skeletal muscle, allowing for movement of the skin.
The deep fascia lies beneath the superficial fascia. It aids muscle movement and, like the superficial fascia, provides passageways for nerves and blood vessels. In some areas of the body, it also provides an attachment site for muscles and acts as a cushioning layer between them.
The subserous fascia lies between the deep fascia and the membranes lining the cavities of the body. There is a potential space between it and the deep fascia that allows for flexibility and movement of the internal organs.
Myofascia extends from the deep fascia as a thin, elastic and dynamic membrane that covers, supports and separates the skeletal muscles. As endomysium it wraps and separates each muscle fibre. As perimysium it wraps each bundle of muscle fibres into a fascicle. As epimysium it wraps each muscle itself. These three varieties of myofascia each contribute collagen fibres to the connective tissue that attaches the muscle either to bone or to other muscles. These attachments may also extend beyond the muscle as tendon or aponeurosis (Tortora & Grabowski 1996, pp. 240–241).
Between adjacent muscles the epimysium provides a protective route for blood vessels, nerves and lymph ducts. The muscles, ideally, act as cushions for these vessels. However, the quality of cushioning depends on the tone of the muscle as well as the dynamism of the myofascial pathways. If the surrounding muscles are hypertonic they will limit the flow of blood and lymphatic fluid through the epimysium and reduce the flow to the surrounding tissue.
This may be exactly the condition Dr Varma describes in the quote at the beginning of this chapter. It is echoed in the words of Andrew Taylor Still (1828–1917) the founder of osteopathy. Still always reminded his students that the physician’s task ‘was to remove with gentleness all perceived mechanical obstructions to the free-flowing rivers of life (blood, lymph, and cerebro-spinal fluid). Nature would then do the rest’ (McPartland & Skinner 2005). Perhaps an ancient appreciation of the significance of myofascia in relation to those rivers of life was what inspired the development of some of the traditional medical systems still available to us today.
Yoshio Manaka, who died in 1989, contributed much to our modern understanding of acupuncture through scientific research. Although he did not specifically refer to the connective tissue he said: ‘While we can offer no clear description of the body’s hardware, we propose that it is better to examine and define the software first’ (Manaka 1995, p. 55). Manaka referred to the ‘X-signal system’, so called because it could not yet be fully explained, even if he considered it to be ‘the biological system that lies at the very heart of acupuncture and moxibustion theory and practice.’ He considered it to be a primitive signalling system, as yet unknown to biologists and impossible to explain with neurophysiology because, ‘it manifests and is manipulated clinically with minute stimuli or influences that cannot be clearly said to affect the nervous system’ (Manaka 1995, p 18). It seems highly likely from what we now know that the connective tissue provides a significant part of the hardware in this signalling system.
Recent research would seem to confirm this. Helene Langevin and colleagues at the University of Vermont College of Medicine used high frequency ultrasound scanning acoustic microscopy to study acupuncture channels and the effects of acupuncture needling. Langevin observes that ‘Acupuncture points and meridians typically are located between muscles or between a muscle and a tendon or bone’ (Langevin 2001, p. 2279). In other words, acupuncture meridians may be myofascial pathways.
In one experiment, Langevin explored a phenomenon discussed for more than 2000 years in acupuncture texts and of great clinical significance to acupuncturists. This phenomenon, known as ‘de qi’ or ‘needle grasp’, is described as a tug on the needle ‘like a fish biting on a fishing line’ (Langevin 2001, p. 2275). Microscopic observation shows that as the acupuncture needle is turned collagen fibres wind around its shaft. Not only does this explain the tug on the needle but it also suggests that acupuncture achieves some of its effects through mechanical influence on the connective tissue matrix. Langevin says that:
The ancient maps of acupuncture points and meridians may essentially be a guide to insert the needle into connective tissue. Spreading of matrix deformation and cell activation along connective tissue planes thus may mediate acupuncture effects remote from the acupuncture needle site
This would certainly fit Manaka’s theory of a signalling system requiring no more than minute stimuli and free from the need for mediation through the nervous system. Hiroshi Motoyama draws similar conclusions in his study of yoga practice and the Ayur-vedic nadis. He says, ‘I consider the nadis to be essentially equivalent to the meridians of Chinese acupuncture; from my research, it appears that these channels are formed of connective tissue and filled with body fluid’ (Motoyama 2003, p. 43).
Perhaps one day we will construct an anatomical model with which to explain exactly how traditional Chinese acupuncture works. Researchers like Matsumoto, Motoyama and Langevin call our attention to the connective tissue matrix as an important part of that model. That matrix might have 72 000 pathways; it might have 350 000 pathways; it might have as many pathways as cells. In the practice of Thai Massage we have only ten sen but if these are myofascial pathways perhaps they are the more significant routes through the connective tissue matrix or, at least, those into which we can most easily press our thumbs. Perhaps we have the beginnings of a way in which to explain the physical benefits of manipulating these lines.
Myofascial sen
In Thai Massage all the schools seem to agree that there are ten main lines, but nobody seems to agree on where they run
If we consider the sen not as lines but as myofascial planes or pathways we can be very clear in our description of where they run because they always relate to muscles and bone and the myofascial channels between them.
As mentioned before, when it comes to the practice of Thai massage we concern ourselves only with fragments of the ten sen. Here they are referred to as treatment lines (Fig. 12.1).

There are only a couple of rules when it comes to manipulating these treatment lines:
This means we are always working to soften and deepen myofascial channels between muscle and muscle and muscle and bone.
Myofascial leg lines
When I first studied Thai massage we were taught five treatment lines on the legs. Nowadays some people teach six, more in keeping with the traditional Chinese meridian model. On the lateral surface of the leg there are two treatment lines, usually referred to as the 1st outside leg line and the 2nd outside leg line (Fig. 12.2).
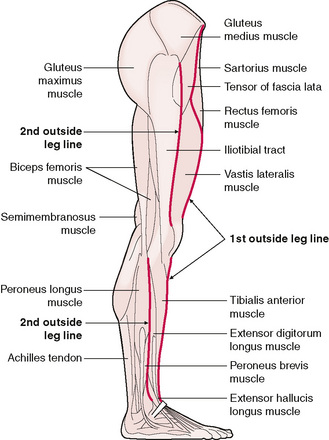
Figure 12.2 Lateral view of the leg showing the path of the 1st outside leg line and the 2nd outside leg line.
The 1st outside leg line begins just above the ankle and follows the lateral edge of the tibia between the bone and the tibialis anterior muscle towards the knee. The technique when working this line is to rest the thumbs on the lateral edge of the tibia and then allow them to drop off the bone into the myofascial channel between the bone and the muscle. Each pass along the line aims to gain a little more softness and depth.
On the upper leg the 1st outside leg line follows the lateral border of the rectus femoris muscle. The line begins at the little dip on the superior, lateral corner of the kneecap and continues up to the anterior superior iliac spine (ASIS).
The 2nd outside leg line begins on the lower leg, just superior to the lateral malleolus and follows the anterior border of the peroneus longus muscle. The aim in working this line is to soften and open the myofascial channel between the peroneus longus muscle and the tibialis anterior muscle. This is achieved by pushing the muscle downwards under the bone. It is tempting to medially rotate the leg to see where the line runs but this is best avoided as the rotation will tighten the fascial web, contrary to the aim of softening it.
Above the knee the 2nd outside leg line follows the anterior border of the iliotibial tract from just above the knee towards the head of the femur. The method of working this line involves pressing the fascial band of the iliotibial tract down and under the femur.
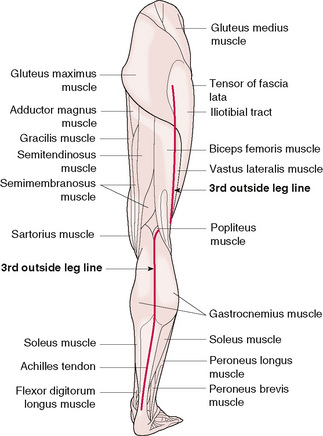
The 3rd outside leg line actually starts at the back of the leg in the centre of the achilles tendon and passes between the two heads of the gastrocnemius muscle into the soft tissue at the back of the knee. Above the knee the 3rd outside leg line follows the lateral border of the biceps femoris muscle from the knee to the hip (Fig. 12.3).
On the medial surface of the leg there are two treatment lines, usually referred to as the 1st inside leg line and the 2nd inside leg line (Fig. 12.4).
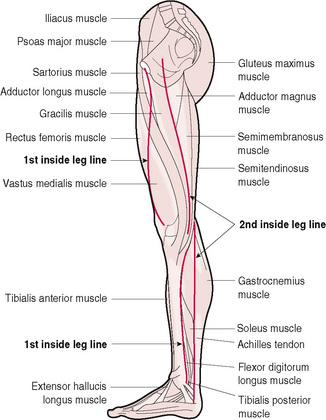
Figure 12.4 Medial view of the leg showing the path of the 1st inside leg line and the 2nd inside leg line.
The 1st inside leg line follows the medial edge of the tibia between the bone and the soleus muscle. The fascial binding associated with this line is often quite tight and extra care is needed to avoid causing pain. Above the knee the line begins at the little dip on the superior, medial corner of the kneecap. From there the 1st inside leg line follows the medial border of the rectus femoris muscle up towards the groin.
The 2nd inside leg line begins at the ankle on the medial border of the achilles tendon and follows the medial border of the gastrocnemius muscle up to the knee. Above the knee the line begins at the posterior border of the sartorius muscle, just above its attachment to the head of the tibia. Moving up towards the groin, the line follows the posterior border of the gracilis muscle.
Myofascial arm lines
Using a myofascial approach to Thai massage we find four treatment lines on the forearms. These prove very useful in working an area that is often poorly attended in other massage systems (Fig. 12.5)
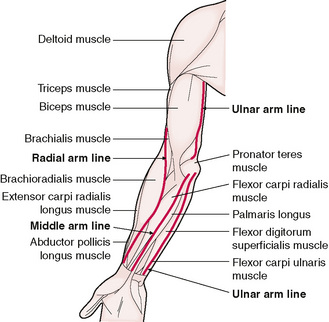
Figure 12.5 Anterior view of the arm showing the path of the radial arm line, the middle arm line and the ulnar arm line.
The middle arm line begins at the wrist, between the tendons of palmaris longus and flexor carpi radialis. The line travels superior to the wrist between the palmaris longus muscle and the flexor carpi radialis muscle to the elbow crease.
The ulnar arm line starts medial to the flexor carpi ulnaris tendon at the crease of the wrist. It follows the myofascial pathway between the flexor carpi ulnaris muscle and the flexor digitorum superficialis muscle. In order to find depth in this myofascial channel it is necessary to bend the flexor digitorum superficialis muscle over the top of the bones of the forearm.
The radial arm line starts at the crease of the wrist on the medial border of the tendon of the brachioradialis muscle and continues up the medial border of the muscle to the elbow crease. This line is manipulated using the thumb which moves the muscle medially in order to find the myofascial channel between the brachioradialis muscle and the flexor carpi radialis muscle.
On the posterior surface of the arm there is only one treatment line to consider (Fig. 12.6).
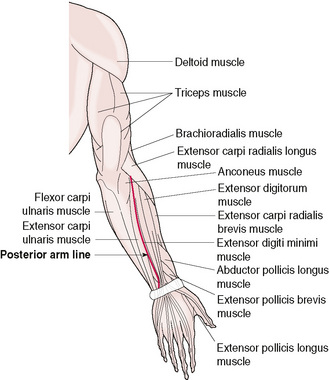
The posterior arm line starts at the centre of the wrist crease, between the heads of the ulna and radius bones. Moving up towards the elbow the line follows the border of the extensor digitorum muscle.
Working all the arm lines involves finding the natural movement of the associated muscles in order to soften and deepen the myofascial channels without pressing against the bones.
Myofascial back lines
In common with all the treatment lines used in Thai massage there are differences in opinion as to where the back lines run. Often they are compared with the bladder meridians used in Chinese acupuncture. Because the arrangement of muscles on the back is so complex and multilayered it is difficult to say exactly which muscles these lines relate to. That said however, in practice the lines are easy to find and use.
There are two medial back lines, one on either side of the spinal column. To locate the lines the thumbs are positioned side by side on the spinous process of a vertebra. They will fall naturally into two channels either side of the spine. Although these channels can be worked from the pelvis to the seventh cervical vertebra it is more practical to stop at the lower edge of the scapulae. In general the channels follow the medial borders of the erector spinae muscles.
There are also two lateral lines on the back. These are located by moving the thumbs laterally from the medial back lines. The thumbs rise up over a ridge of muscle and fall down the other side. In general these lines follow the lateral borders of the erector spinae muscles from the pelvis to the shoulder blades.
These lines are manipulated by walking the palms up the muscle ridge from the pelvis to the lower edge of the scapulae, exchanging the pressure slowly from hand to hand, creating a slight torsion around each vertebra. Once at the scapulae the thumbs take over, following the medial back lines down the spine, vertebra by vertebra until the pelvis. At each vertebra the aim is to engage with the fascia and muscle and push the tissues upwards. It is not unusual to feel or hear a click of release at a vertebra with these movements but it is not specifically the aim of the process. Some people click easily and some do not.
We can also work the lateral back lines while kneeling to the side of our patient. In this case, we engage the lateral back line using the heel of our hand and bend the erector spinae muscle towards the spinal column. Our other hand rests on the pelvis.
Thai massage as myofascial massage
Thai massage is mostly concerned with the manipulation of the sen. The unfolding of this process is really quite simple. It does not matter whether the line is worked from the extremity toward the torso or from the torso toward the extremity. The general technique is to work up and down each line, feeling for any tightness in the tissue. Where there is tightness, the area is worked a little more to soften the tissue and equalize the feel of the entire line. This process is often referred to as ‘clearing energy blocks’. Unlike shiatsu or acupressure there is no method, apart from touch, with which to assess the lines and there is no method of balancing the energy between the sen. The guiding principle is to work to soften all the lines on the limbs and let nature take care of the rest.
There are various ways to work the sen. They are mostly worked with the thumbs or palms. Occasionally they are worked with the knees, elbows or the soles of the feet. Whichever tool is used, the most important thing is the sensitivity of the massage practitioner. The practitioner needs to feel what is happening. When the patient knows that they are being felt they relax, letting go of any fear that they might be hurt or broken.
Usually Thai massage practitioners press into the line to the point where the tissue tightens and resists. They then add a little more pressure. Working with attention on the myofascial pathway requires some modification to this approach. Simply pressing until the tissue resists leaves no room for movement or change in response to the massage practitioner’s input. If the massage practitioner learns to feel the response in the tissue they will often find as they increase the pressure that the connective tissue shows a direction in which it prefers to go. The practitioner follows the direction of the patient’s body.
This way of working requires a very alive attention with each and every move. There is no repetition of a technique. Every technique has to be rediscovered in the moment. This sounds like a slow process but it is not. Learning to work like this takes a little time but soon the sensation of the massage practitioner’s body wakes up.
The massage practitioner feels for the softening of the tissue and connects with the elasticity and inherent movement of the fascia. It may draw their hands up towards the patient’s head or down towards their feet. This natural movement is followed until the first barrier of resistance is met. The practitioner then allows the elasticity of the patient’s body to push their thumbs back out, following the same path in which they came in. This basic movement is never the same. The connective tissue changes with each pass along a myofascial pathway. With each pass the massage practitioner can expect to work a little deeper. Even the direction of movement in the connective tissue may change with the work.
In Thai massage, rhythm is very important. That rhythm is a combination of the practitioner’s action and the response of the patient’s tissues to that action. The rhythm arises in the moment and helps the muscle to soften. Muscle tissue consists of cells and fibres, organized in a connective tissue web, suspended in fluid. Working like this encourages the muscle to change from a more solid to a more relaxed and liquid state. The muscle is expressing a quality called thixotrophy; which describes the way in which a colloidal combination of solid matter suspended in fluid changes state in response to the heat and the quality of the movement administered.
The muscle changes its quality in response to the heat of the practitioner’s contact and the rhythm of their movement. The resulting softening of the ground substance improves the flow of nutrients to the cells and waste from the cells to the lymphatic system (Oschman 2000, p. 171). Rhythmic kneading of the muscle also encourages venous, lymphatic and tissue drainage (Chaitow 2003, p. 174). The softening and loosening of the myofascial pathways further enhances this process by easing and encouraging that flow between adjacent muscles. In addition, this combination can be expected to reduce pressure on the peripheral nerves effectively reducing ‘noise’ flowing through the nervous system.
Thai massage and neuromuscular technique
One of the techniques included under the general heading of Neuromuscular Technique is the ‘c-bend’; recognized as one of the few ways of modifying connective tissue status and lengthening muscle through a process of ‘tension loading’. The technique involves using the thumbs or the heel of the hand to introduce a ‘c-bend’ into the target muscle, until the first barrier of resistance is met. The barrier is engaged until the therapist feels a release in the tissue. This would typically occur between 5 and 30 seconds. Using this technique encourages muscle lengthening without the risk of initiating a stretch reflex. Although the c-bend can be applied as a series of rapid, snapping thrusts with the intention of breaking up rigid tissue, when its aim is to lengthen muscle the process is slower and smoother (Chaitow 2003, pp. 32–33).
The c-bend enlists the help of the muscle spindles and Golgi tendon receptors within the muscles. The muscle spindles detect and adjust the length of the muscle while the Golgi tendon receptors detect how hard the muscle is working (Chaitow 2003, p. 3). Applying a c-bend, signals to the nervous system that the muscle is under load and the nervous system lengthens the muscle to reduce the risk of overload and damage.
In Thai massage, rhythmic manipulation of the sen is a major part of the massage. Using a myofascial approach to the sen, the massage practitioner invariably follows the border of a muscle. As they push into the myofascial pathway they often find themselves applying a c-bend to the muscle. Although in Thai massage it is not usual to hold the c-bend for long, the rhythmic repetition of the movement along the length of the muscle still has the desired effect of lengthening and softening the muscle.
When I studied NMT with Leon Chaitow one of the first attempts we made at applying a c-bend was to the erector spinae muscle. The movement involved using the medial border of the muscle to c-bend it away from the spine. In Thai massage it is more practical to use the lateral border of the erector spinae muscle to apply a c-bend toward the spine. This is the lateral back line. It works just as well. The c-bend is repeated along the length of the spine from the edge of the pelvis to the lower edge of the scapula. One hand works while the other rests (Fig. 12.7).

When manipulating the 1st outside leg line on the upper leg the massage practitioner can use the myofascial pathway to apply a c-bend along the length of the rectus femoris muscle from the corner of the knee to the pelvis. In this case the work usually begins by applying a c-bend using the palm to warm up and soften the muscle before applying a stronger c-bend with both thumbs. The muscle is bent over the top of the femur (Fig. 12.8).

The c-bend can also be applied when working the 2nd outside leg line on the upper leg. This myofascial pathway follows the anterior border of the iliotibial tract. Here the c-bend is applied only using the thumbs. The aim of the movement is to bend the iliotibial tract down and under the femur. This c-bend encourages lengthening of the tensor fascia latae muscle (Fig. 12.9).

The c-bend can similarly be applied to the 3rd outside leg line as well and the 1st and 2nd inside leg lines.
The same technique can be applied to all four treatment lines on the forearm. Here the sen can be felt as myofascial pathways between the muscles of the forearm. For each line the massage practitioner uses the thumb to c-bend the target muscle across the bones of the forearm (Fig. 12.10).

The examples given here are just that; there are many more possibilities and variations. When the sen are felt for as myofascial planes rather than as ‘energy lines’ the entire massage unfolds as a continuous and rhythmic application of c-bends. Although the application of the c-bend in Thai massage does not have the aim of breaking up fibrous tissue nor of holding the muscle for more than a second at its barrier, it does nevertheless have the desired effect of lengthening and softening the muscle. The Thai massage practitioner’s aim is to gain just a little more length and softness muscle by muscle throughout the patient’s body. The accumulated effect is quite profound; undoubtedly more than the sum of the parts.
Conclusion
One of the main sources of modern myofascial techniques is Rolfing. Ida Rolf started teaching her system in the ‘therapeutic’ scene that developed around Fritz Perls, Will Schutz and the Esalen Institute in the mid 1960s. This period at Esalen, in California, saw the birth of a confrontational style of group therapy called ‘encounter’. The Institute also came to be regarded as the centre of the ‘human potential’ movement. Ida Rolf’s system fitted this environment well. Early Rolfing was a fairly confrontational style of bodywork and the ten-session series became a fashionable adjunct to psychotherapy with the belief that it would reach the parts that the ‘talking cure’ could not.
Rolfing is based on the concept of an ‘ideal body’ which, for Ida Rolf, was a body better orientated to gravity. The aim of the Rolfing series was to bring the client closer to this ideal. In my experience of the work in the hands of one of Rolf’s direct students there was little talk and the work was clearly a matter of the therapist ‘knowing’ what was right for my body; a knowing that now takes between six and seven hundred hours of training to acquire. Perhaps, because of this origin, myofascial techniques are generally taught and used within the context of a diagnosis and treatment approach to bodywork; the therapist becomes the expert on the patient’s body.
In comparison, at between 60 and 100 hours, the Thai massage practitioner’s training is quite meagre. And, in the absence of a system of diagnosis on which to base a treatment plan it would seem that the practitioner of Thai massage has little more to offer the patient than attention to the relationship, to the unfolding rhythm of the work and to relaxation. However, if we consider that the massage might actually be a myofascial workout from the feet to the top of the head, we begin to understand just why this humble massage technique is, in practice, fascinating and deeply effective. We may well be improving the flow of blood as it carries oxygen and nutrients to the cells. We may well be assisting the drainage of lymph as it carries toxins away from the cells. We may well be reducing the pressure of muscles and connective tissue bindings leaning against the nerves, thereby reducing the extraneous noise flowing through the nervous system.
Thai Massage Master, Pichet Boonthume, tells his students to work the lines until the limbs become like jelly and everything else will be fine. If those lines are myofascial pathways and, through the rhythmic application of c-bends, they can be used to lengthen the muscles, soften and smooth the connective tissue matrix and enhance the exchange of fluids and information from cell to cell throughout that matrix, we must marvel at the wisdom of the ancients. As modern technology permits us to peek into places where those ancients could only go with their senses we may well find the same thread of perennial wisdom running through NMT and Thai massage as well as a number of other medical systems of similar origin.
Brust H. The Art of Traditional Thai Massage. Bangkok: Editions Duang Kamol, 1990.
Brust H. The Art of Traditional Thai Massage for Advanced Practitioners. Bangkok: Editions Duang Kamol, 1996.
Chaitow L. Modern Neuromuscular Techniques. Edinburgh: Churchill Livingstone, 2003.
Feuerstein G. Yoga, The Technology of Ecstacy. Wellingborough: Crucible, 1990.
Gold R. Thai Massage: A Traditional Medical Technique. St Louis, MO: Mosby Elsevier, 2007.
Iyengar B.K.S. Light on Yoga. London: Unwin, 1984.
Juhan D. Job’s Body: A Handbook for Bodywork. New York: Station Hill Press, 2003.
Kinder H., Hilgemann W. Atlas of World History. Middlesex: Penguin Books, 1978;43.
Langevin H.M., Churchill D.L., Cipolla J. The FASEB. Journal. 15, 2001.
Larson D. The Role of Connective Tissue as the Physical Medium for the Conduction of Healing Energy in Acupuncture and Rolfing. Am J Acupunct. 18(3), 1990.
Maciocia G. The Foundations of Chinese Medicine. Edinburgh: Churchill Livingstone, 1991;152.
Manaka Y. Chasing the Dragon’s Tail. Brookline, MA: Paradigm Publications, 1995.
McPartland J.M., Skinner E. The Biodynamic Model of Osteopathy in the Cranial Field. EXPLORE. 1(1), 2005.
Mercati M. Thai Massage. London: Marshall Publishing, 1998;10.
Milne H. The Heart of Listening. Berkeley, CA: North Atlantic Books, 1995;48.
Motoyama H. Theories of the Chakras. New Delhi: New Age Books, 2003.
Oschman J.L. Energy Medicine. Edinburgh: The Scientific Basis. Churchill Livingstone, 2000.
Rapgay L. Tibetan Medicine, No 3. Dharamsala, India: The Library of Tibetan Works and Archives, 1981;11-14.
Rolf I. Rolfing. Rochester, VT: First Healing Arts Press, 1989.
Tortora G.J., Grabowski S.R. Principles of Anatomy and Physiology. New York: Harper Collins, 1996.