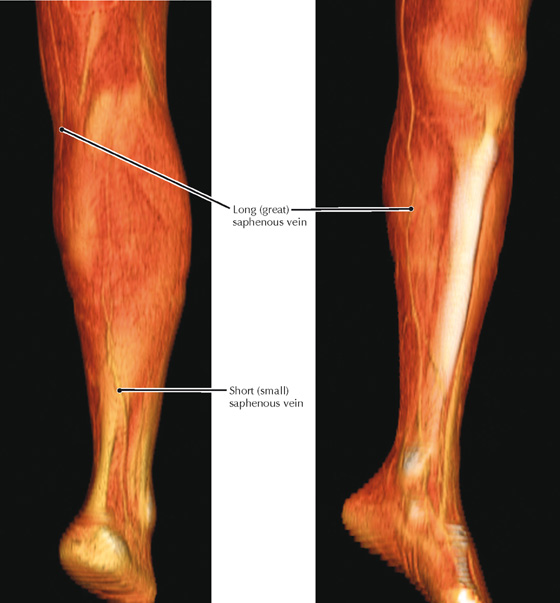
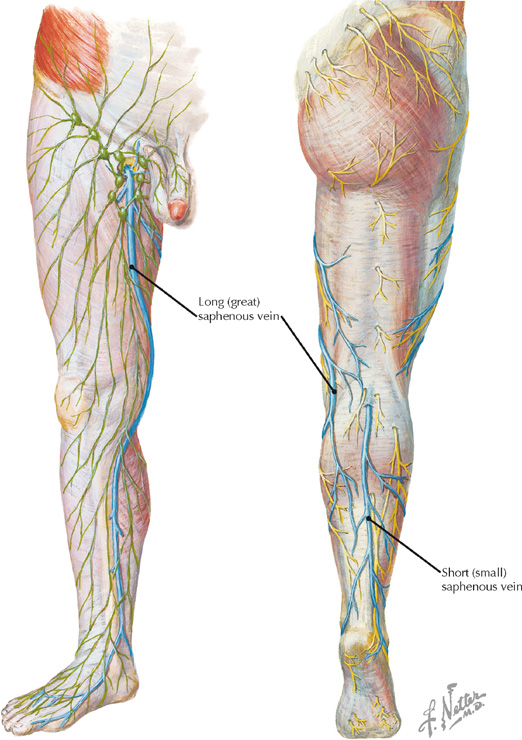
Medial and posterior views of the superficial veins of the lower limb (Atlas of Human Anatomy, 5th edition, Plates 472 and 473)
Volume rendered display, CE CT of the leg
• The small (lesser) saphenous vein enters the popliteal fossa and joins the popliteal vein.
• The great saphenous vein begins at the anterior margin of the medial malleolus, traverses the medial aspect of the popliteal fossa, and wraps around to the anterior thigh to join the femoral vein.
Clinical Note
The superficial veins of the lower limb, including the saphenous veins, drain to deep veins via perforator veins with valves responsible for unidirectional flow to the deep system. When those valves are incompetent (often damaged by phlebitis), increased pressure in the superficial veins results in varicosities.
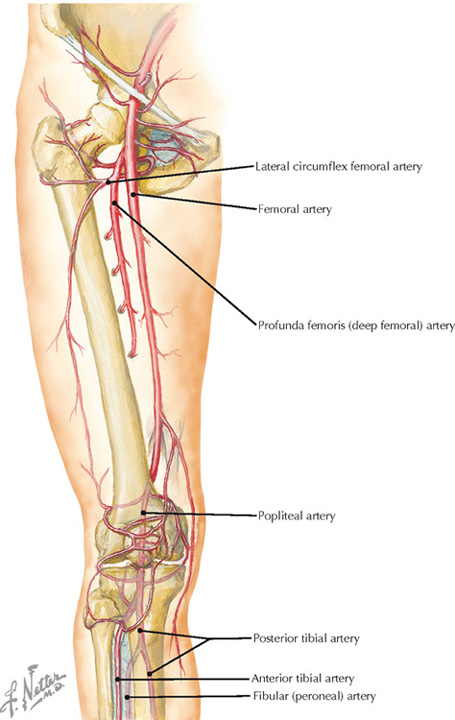
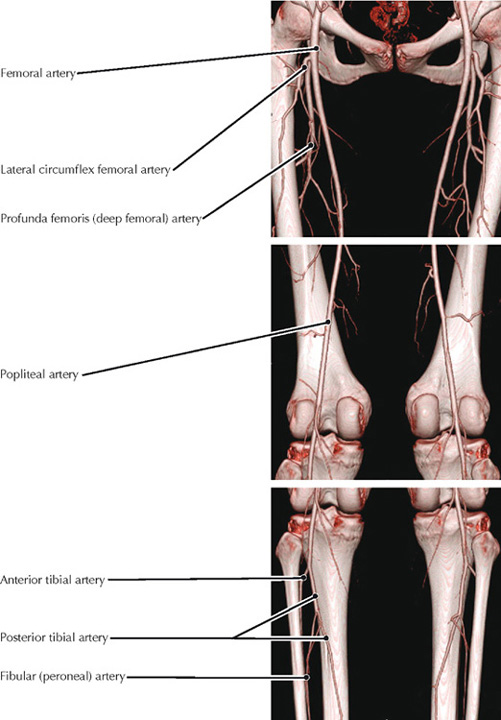
Arteries of the thigh and knee (Atlas of Human Anatomy, 5th edition, Plate 500)
3-D display from CTA of the normal lower limb (From Hiatt MD, Fleischmann D, Hellinger JC, Rubin GD: Angiographic imaging of the lower extremities with multidetector CT. Radiol Clin North Am 43(6):1119-1127, 2005)
• The external iliac artery becomes the femoral artery as it passes posterior to the inguinal ligament.
• The femoral artery becomes the popliteal artery once it traverses the adductor hiatus in the tendon of the adductor magnus muscle.
Clinical Note
Atherosclerosis can cause narrowing of the arteries of the lower limb, producing peripheral vascular disease (PVD). PVD results in claudication (muscle pain with exertion) due to an inability of the vessels to supply sufficient blood to the muscles during activities (e.g., walking).
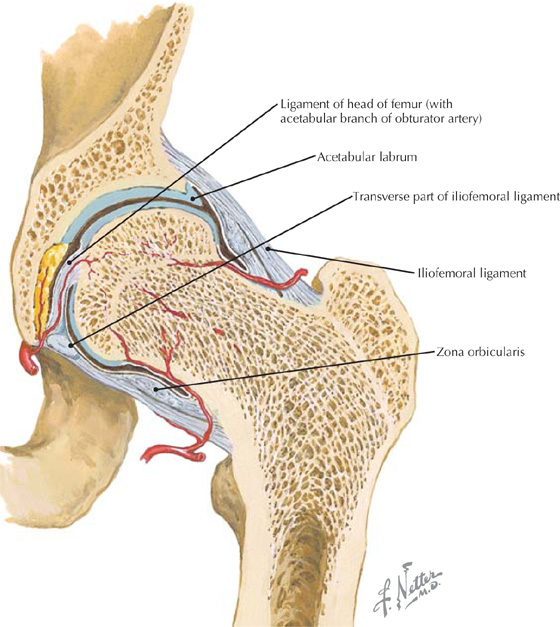
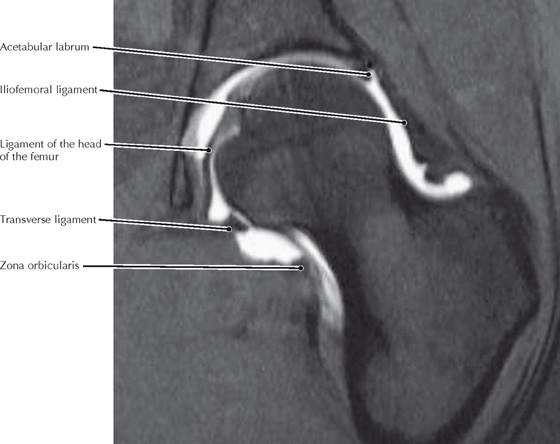
Coronal view of hip joint (Atlas of Human Anatomy, 5th edition, Plate 492)
Coronal FS T1 MR arthrogram of the hip joint (From Chatha DS, Arora R: MR imaging of the normal hip. Magn Reson Imaging Clin N Am 13(4):605-615, 2005)
• The iliofemoral ligament is the strongest ligament of the hip joint. It is a thickening of the hip joint capsule (intrinsic ligament), as are the ischiofemoral and pubofemoral ligaments.
• If there is clinical suspicion of a labral tear, the preferred imaging procedure is an MR arthrogram of the hip.
Clinical Note
The acetabulum, with its labrum, extends more than a hemisphere over the head of the femur, which, along with the strong ligaments from the pelvis to the femur, contributes to a very stable hip joint. Fractures (through the neck of the femur) are more common than hip dislocations.
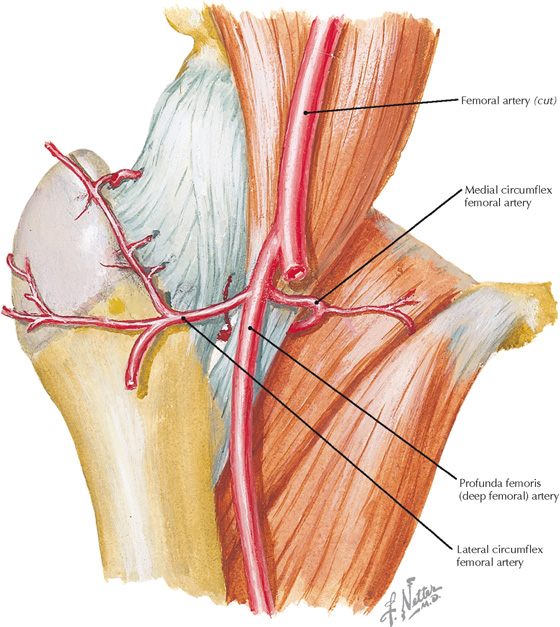
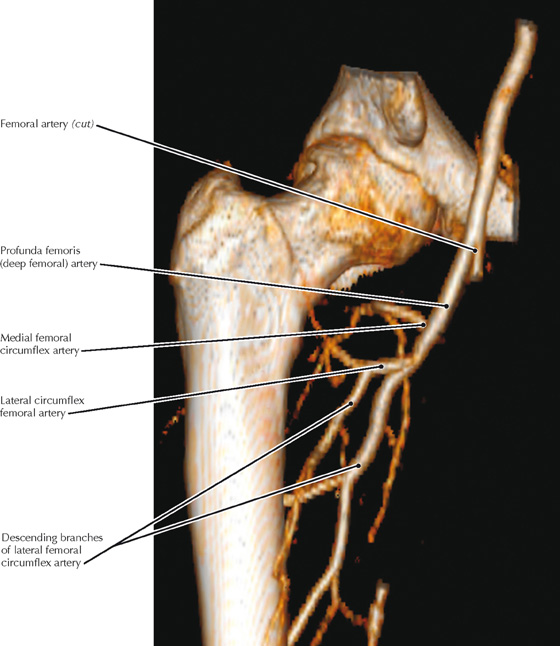
Anterior view of the arterial supply to the head of the femur (Atlas of Human Anatomy, 5th edition, Plate 492)
Volume rendered display, aortofemoral CTA
• A small branch of the obturator artery (acetabular) passes through the ligament of the head of the femur (ligamentum teres) to supply the femoral head, but this branch is usually too small to prevent necrosis if the circumflex arteries are torn.
• In cases of avascular necrosis, the femoral head is removed and a prosthetic hip joint is surgically implanted.
• The profunda femoris artery (deep femoral artery) supplies the muscles of the posterior thigh.
Clinical Note
Most of the blood reaching the head of the femur is supplied by branches of the femoral circumflex arteries (primarily the medial). Because these branches are often compromised in a “fractured hip” (common in elderly women due to osteoporosis), the femoral head subsequently undergoes avascular necrosis.
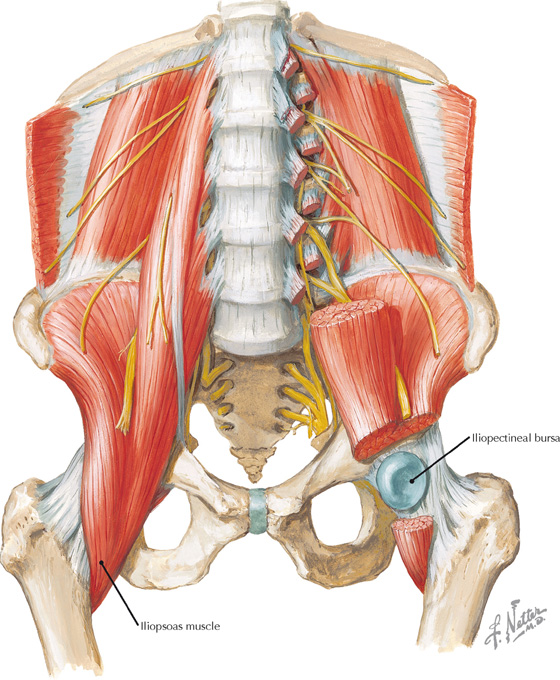
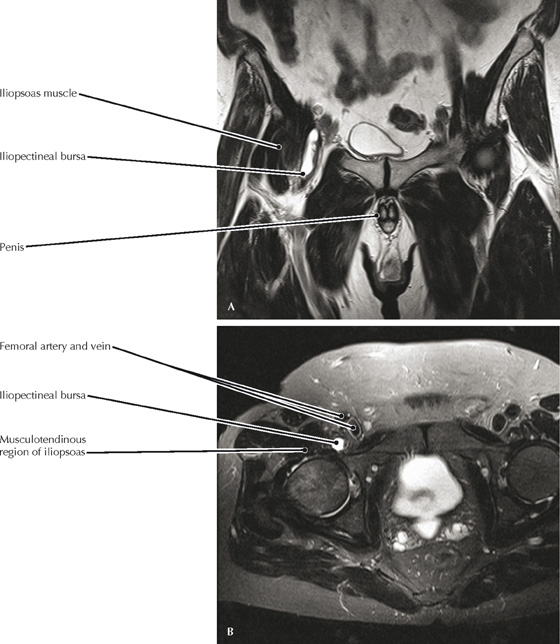
Psoas and iliacus muscles, and iliopectineal bursa (Atlas of Human Anatomy, 5th edition, Plate 484)
(A) Coronal and (B) axial FS T2 MR images of the pelvis
• The iliopectineal bursa allows the iliopsoas muscle/tendon to move freely over the hip joint as it flexes the thigh.
• The iliopsoas tendon (common tendon of iliacus and psoas major muscles) inserts onto the lesser trochanter.
Clinical Note
The iliopectineal (iliopsoas) bursa is the largest bursa in the body and frequently communicates with the hip joint.
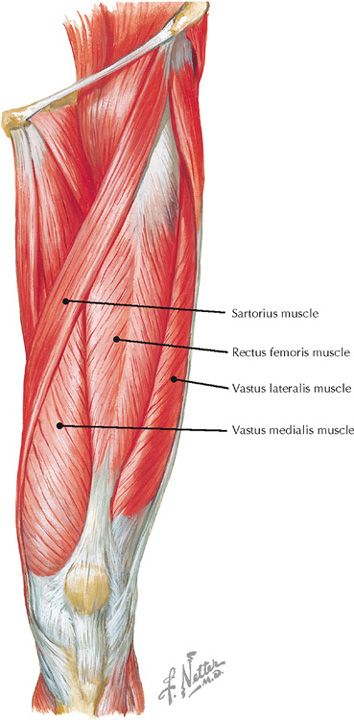
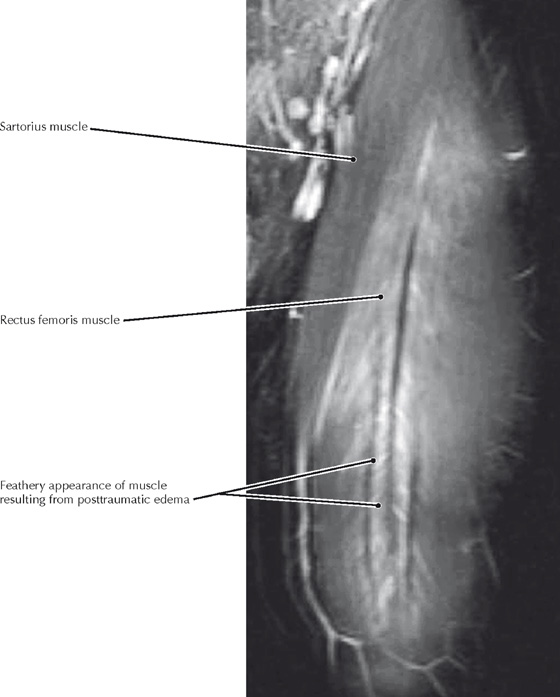
Anterior view of the thigh (Atlas of Human Anatomy, 5th edition, Plate 480)
Coronal MR image of the anterior thigh (From Bordalo-Rodrigues M, Rosenberg ZS: MR imaging of the proximal rectus femoris musculotendinous unit. Magn Reson Imaging Clin N Am 13(4):717-725, 2005)
• Grade 1 muscle injury is a strain of the muscle without architectural disruption. In Grade 2 muscle injury there is more clearly visible disruption of muscle fibers with hemorrhage. Grade 3 muscle injury is characterized by a complete disruption of the muscle.
• All four parts of the quadriceps femoris muscle group are innervated by the femoral nerve, which is composed of the dorsal divisions of the ventral rami of L2-L4 spinal segments.
Clinical Note
The quadriceps femoris muscle group (quadriceps femoris, vastus lateralis, vastus medialis, vastus intermedius) is the only extensor of the knee. The rectus femoris is the only head of the quadriceps group that also crosses the hip joint and is thereby a “biarticular” muscle that can flex the hip.
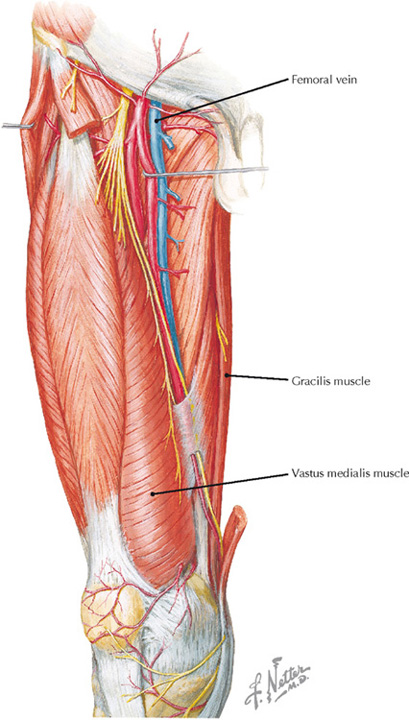
Arteries, nerves, and muscles of the anterior thigh (Atlas of Human Anatomy, 5th edition, Plate 488)
Volume rendered display, low-dose CT scan of the thighs, done shortly after CE CT scan of the chest to rule out pulmonary embolism
• The great saphenous vein has been the vessel of choice for coronary artery grafting for many years, although other vessels (e.g., radial, internal thoracic arteries) are now often used. If the vein is used it must be positioned so that the valves do not impede blood flow.
• Once the popliteal vein passes through the adductor hiatus in the adductor magnus muscle it becomes the femoral vein.
• Clinically suspected thromboembolic disease is usually evaluated by a pulmonary CT angiogram to identify or rule out pulmonary emboli. The scan protocol often includes a low-dose CT scan of the lower limbs, usually done approximately 2 minutes after the IV contrast injection for the pulmonary artery study. This additional scan may demonstrate popliteal and femoral vein thrombi.
Clinical Note
The consistent vascular anatomy and nerve supply of the gracilis muscle, plus its relatively small contribution to thigh adduction, allow this muscle to be used as a wound graft when a long vascular leash is not required. Furthermore, it can also be used to reproduce upper limb, lower limb, or facial muscular function.
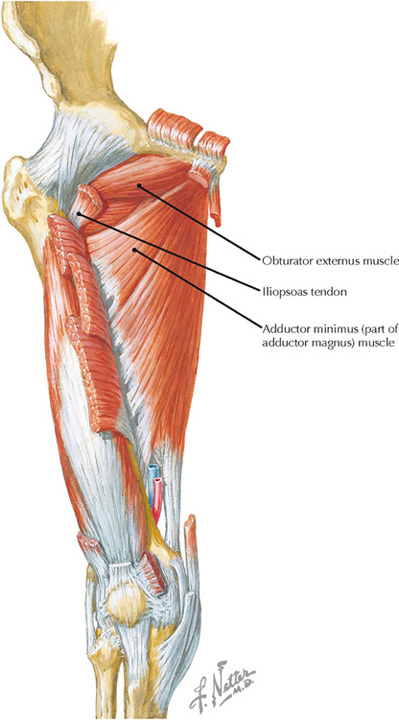
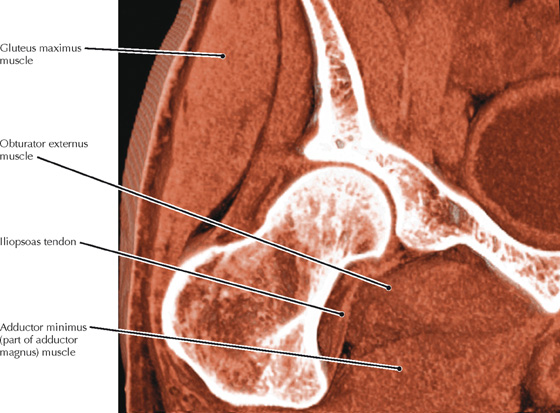
Anterior view of the deep hip muscles (Atlas of Human Anatomy, 5th edition, Plate 481)
Volume rendered display, CT of the pelvis
• The adductor magnus muscle is actually two muscles that are well blended anatomically, but distinct functionally. The superior part is innervated by the obturator nerve and acts with the other adductors in flexing and adducting the femur. The lower part is innervated by the tibial part of the sciatic nerve and acts with the hamstrings as a hip extensor.
• The obturator externus muscle covers the external surface of the obturator membrane and is a strong lateral rotator of the femur.
• A volume rendered display, such as this image, permits visualization of the posterior relationship between the obturator externus muscle and the femoral neck.
Clinical Note
Clicking or snapping hip (coxa saltans) is a symptom complex characterized by an audible “snap” around the hip on specific movements. It is often painless but may become painful or uncomfortable as chronicity develops. One common cause is the iliopsoas tendon snapping over the iliopectineal eminence or femoral head.
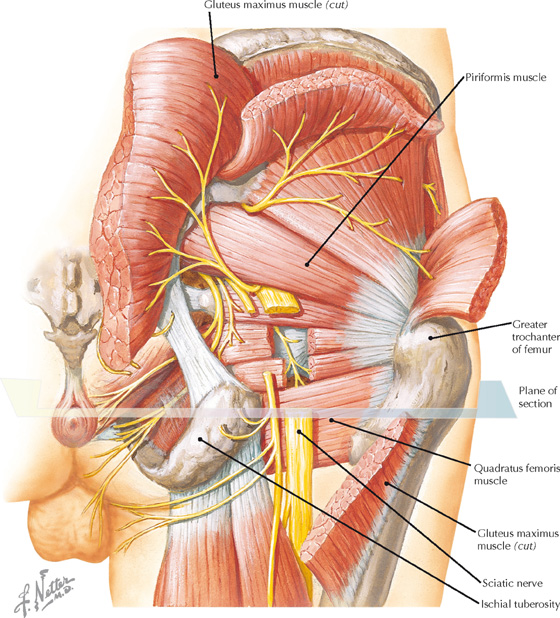
Posterior view of the gluteal region and posterior thigh (Atlas of Human Anatomy, 5th edition, Plate 490)
(A) Coronal T1 MR image of the gluteal region; (B) axial T1 MR image through the gluteal region (A, From Stone JA: MR myelography of the spine and MR peripheral nerve imaging. Magn Reson Imaging Clin N Am 11(4):543-558, 2003)
• The top image is oriented to the long axis of the sciatic nerve as it courses through the greater sciatic foramen; the nerve, which is isointense with muscle, is surrounded by high-signal perineural fat.
• The lower image shows how intragluteal injections placed too far inferiorly and too far medially could injure the sciatic nerve.
Clinical Note
The sciatic nerve can be irritated by tears of the hamstring muscles, producing a type of “sciatica.” The resulting pain can be significant and very disproportionate from what might be expected in a hamstring injury that does not involve the nerve.
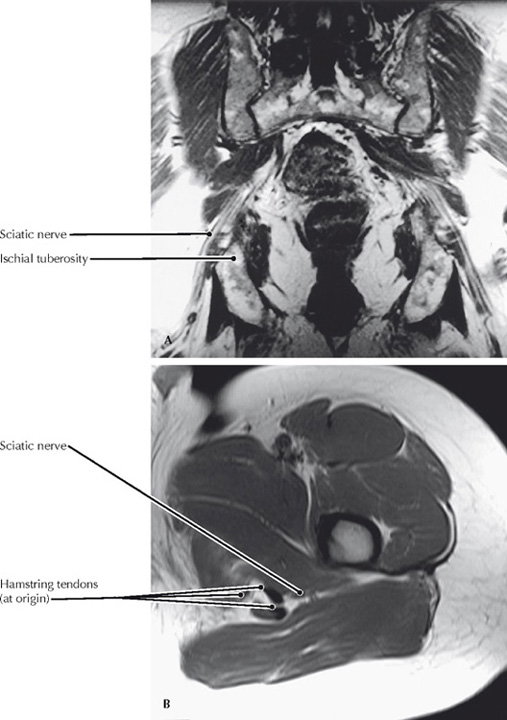
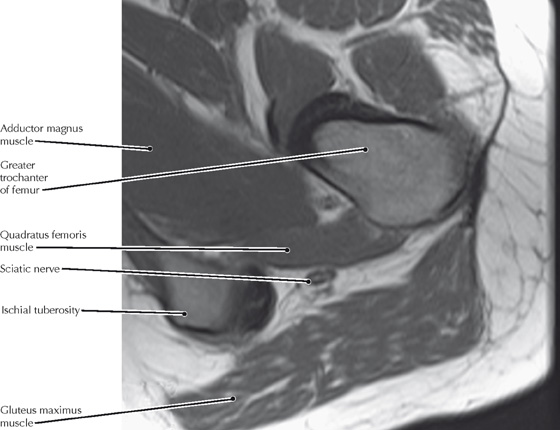
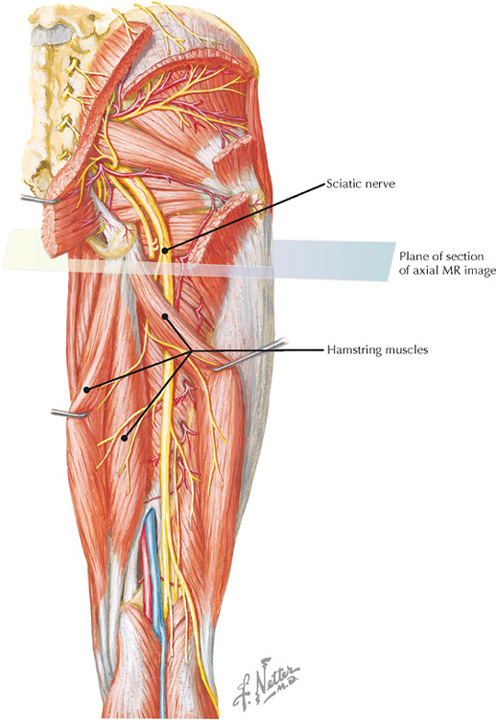
Deep muscles of the posterior thigh (Atlas of Human Anatomy, 5th edition, Plate 491)
Axial T1 MR image, gluteal region
• Although typically the sciatic nerve passes inferior to the piriformis muscle, it may pass through or superior to this muscle.
• The sciatic nerve provides almost all of the motor and sensory innervation of the posterior aspect of the thigh, and the leg and foot.
Clinical Note
The proximity of the sciatic nerve to the ischial tuberosity explains how hamstring tears at their origin on the tuberosity can result in sciatic nerve irritation, with symptoms that mimic sciatica.
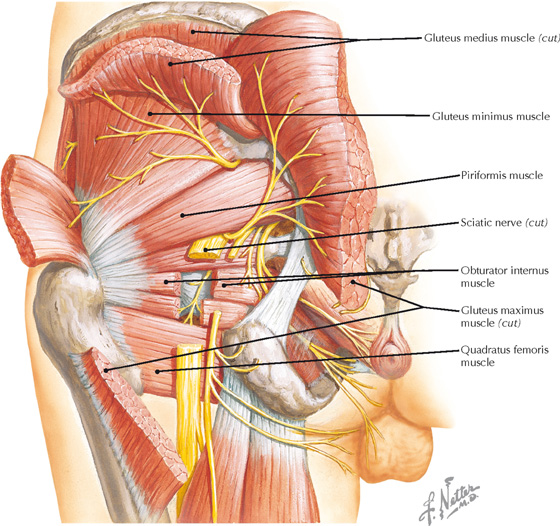
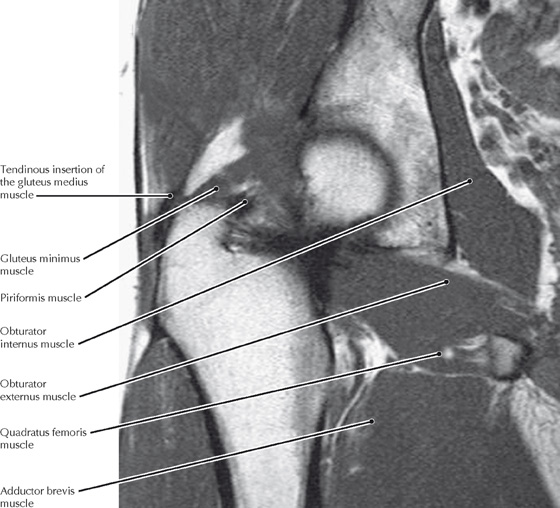
Posterior view of the deep gluteal region (Atlas of Human Anatomy, 5th edition, Plate 491)
Coronal T1 MR image of the posterior gluteal/hip region (From Chatha DS, Arora R: MR imaging of the normal hip. Magn Reson Imaging Clin N Am 13(4):605-615, 2005)
• The gluteus medius and minimus are the primary abductors of the hip and are both innervated by the superior gluteal nerve, which also innervates the tensor fascia latae.
• The quadratus femoris is a lateral rotator of the thigh and is sometimes absent.
Clinical Note
Tears of the gluteus medius and minimus tendons can mimic symptoms of greater trochanteric bursitis of the hip. However, unlike bursitis, tears of these muscles can be treated surgically.
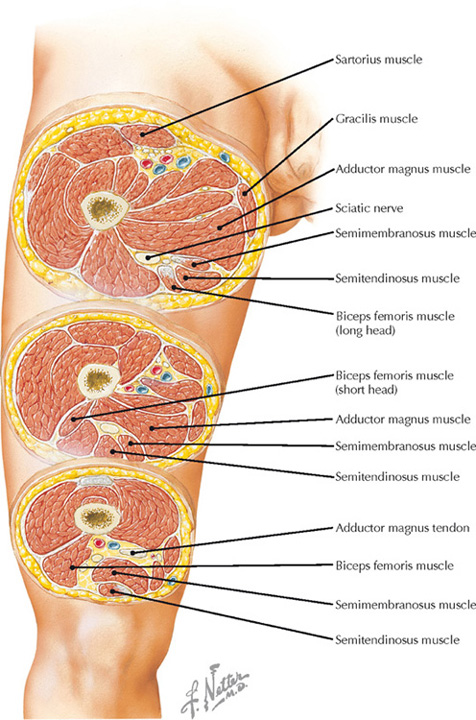
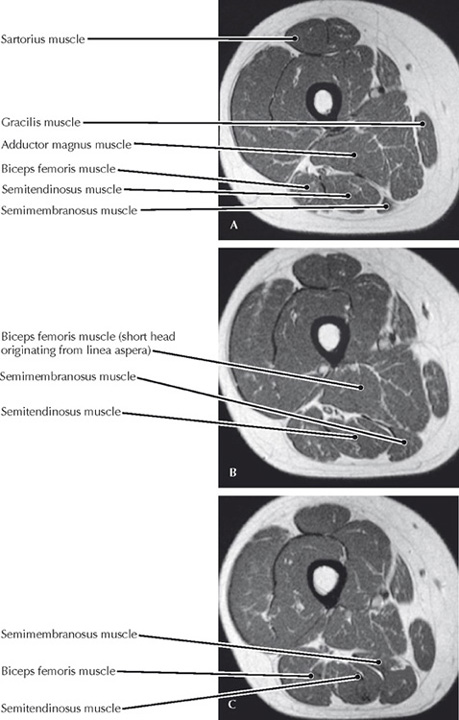
Axial sections through the thigh (Atlas of Human Anatomy, 5th edition, Plate 493)
Axial T1 MR images of the thigh: (A) proximal, (C) distal (From Chatha DS, Arora R: MR imaging of the normal hip. Magn Reson Imaging Clin N Am 13(4):605-615, 2005)
• The hamstring muscles (biceps femoris [long head], semimembranosus, semitendinosus) all originate from the ischial tuberosity, insert into the upper tibia or fibula, extend the thigh and flex the knee, and are innervated by the tibial division of the sciatic nerve.
• The short head of the biceps femoris muscle originates from the linea aspera and inserts with the long head onto the head of the fibula. It is innervated by the common fibular division of the sciatic nerve.
Clinical Note
Hamstring strains (strains of the biceps femoris, semimembranosus, and semitendinosus muscles) are common in patients who participate in running and kicking sports such as baseball, basketball, football, and soccer.
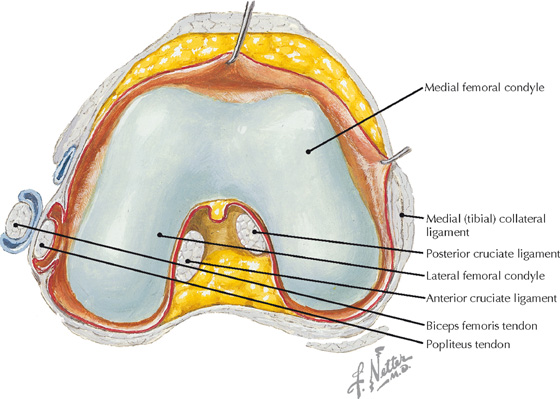
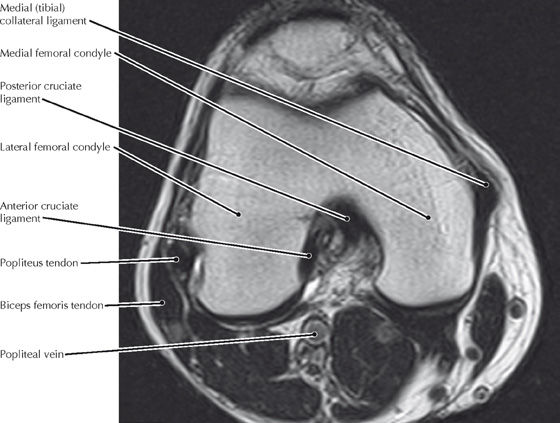
Interior knee joint showing superior aspect of the joint (Atlas of Human Anatomy, 5th edition, Plate 496)
Axial T2 MR image of the knee
• The popliteal vessels may be ruptured in a knee dislocation.
• A tear of the anterior cruciate ligament is often associated with rupture of the medial collateral ligament and tearing of the medial meniscus—the “unhappy triad” (of O’Donoghue).
• The two heads of the gastrocnemius originate on the femoral condyles and therefore flex the knee, as well as plantarflexing the ankle.
Clinical Note
Rupture of a cruciate ligament results in anterior-posterior instability of the knee. An anterior cruciate ligament injury occurs more frequently than a posterior cruciate ligament injury and is often surgically repaired. Excessive anterior movement of the tibia relative to the femur (anterior drawer sign) is indicative of an anterior cruciate ligament tear.
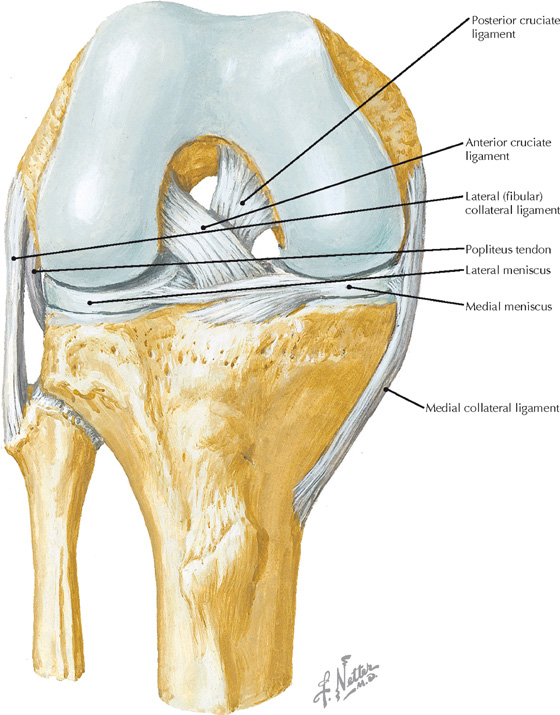
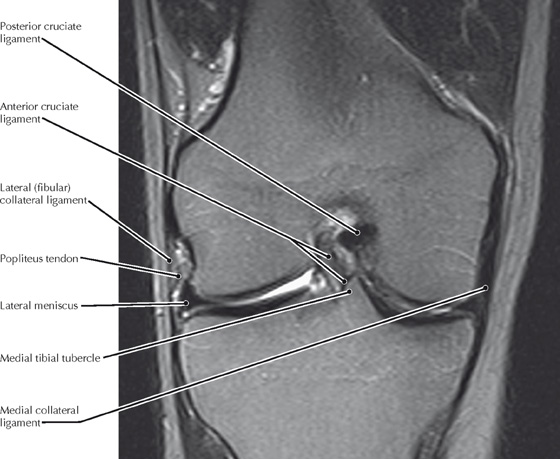
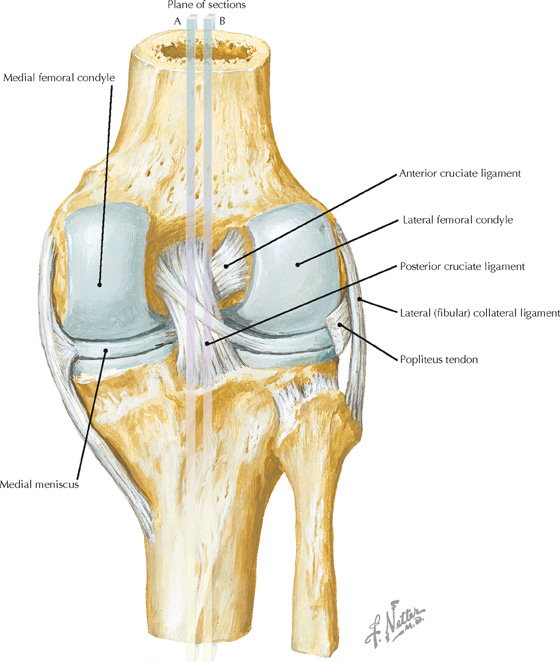
Anterior view of the knee joint showing the cruciate and collateral ligaments, and menisci (Atlas of Human Anatomy, 5th edition, Plate 497)
Coronal T1 MR image of the knee
• Tears of the anterior cruciate ligament usually occur when the knee is twisted while the foot is firmly fixed on the ground.
• The popliteus muscle is very important for providing the rotatory movements that “unlock” the extended knee, allowing it to flex.
• In clinical practice, the tibial tubercles are referred to as the tibial spines.
Clinical Note
The attachment of the medial meniscus to the medial (tibial) collateral ligament explains why tears of both often occur together, whereas this is not the case for the lateral (fibular) collateral ligament and the lateral meniscus.
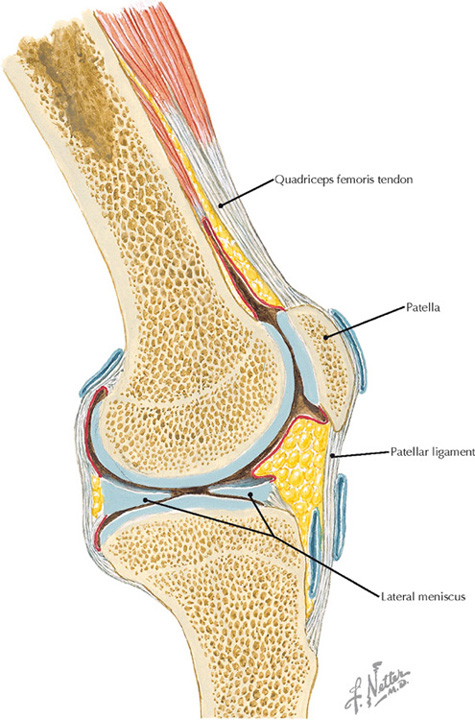
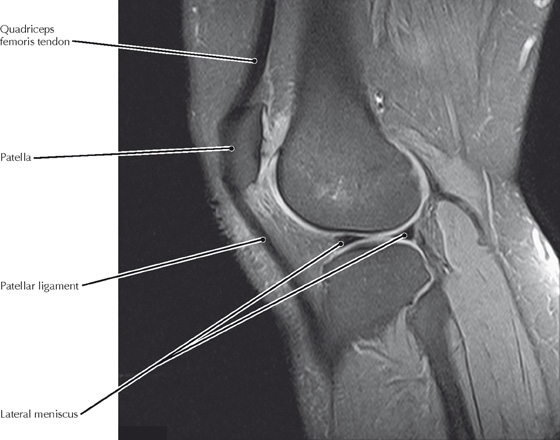
Sagittal view of the lateral knee joint (Atlas of Human Anatomy, 5th edition, Plate 499)
Sagittal fat-suppressed PD MR image of the lateral knee joint
• The medial meniscus is torn much more frequently than the lateral meniscus, primarily because of its attachment to the medial collateral ligament.
• The patellar ligament is really an extension of the tendons of the quadriceps femoris muscles, which act to extend the knee.
Clinical Note
The menisci act as cushions for the joint and are sometimes torn (especially the medial) when the joint is twisted. Patients report pain in the associated knee and a “giving way” of the joint on flexion or extension.
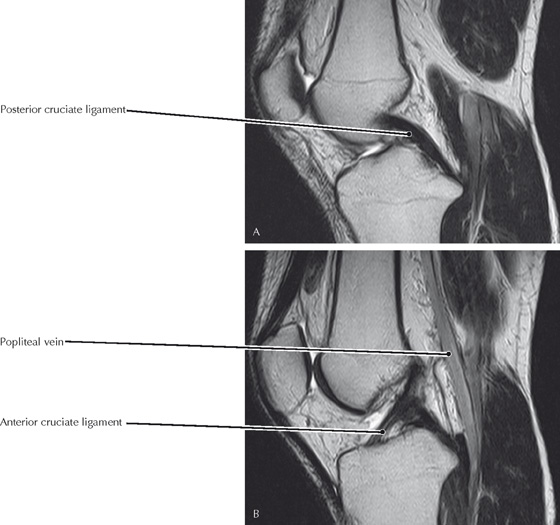
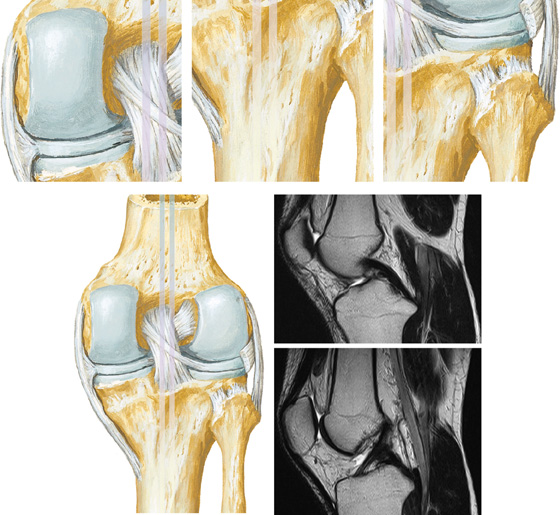
Posterior view of the knee joint showing the cruciate and collateral ligaments, and menisci (Atlas of Human Anatomy, 5th edition, Plate 497)
Sagittal T2 MR images of the knee; B is lateral to A
• Lines A and B on the illustration indicate the sagittal positions of the MR images. However, these images are actually oblique to the sagittal plane in order to maximize the appearance of the ligaments.
• In order to have such oblique images, an MRI technologist must identify the appropriate anatomy on an axial image and then prescribe the appropriate orientation of the sagittal sequences to best show the cruciate ligaments.
• Complete ACL/posterior cruciate ligament (PCL) tears can often be diagnosed clinically, but MRI is used for confirmation and can reveal additional injuries that may not be evident on physical examination.
Clinical Note
A ruptured anterior cruciate ligament (ACL) is often accompanied by a “popping” sensation. Such ruptures occur at a higher frequency in women athletes than in their male counterparts. This may be explained by anatomic differences between men and women (e.g., wider pelvis, smaller intercondylar notch) and by less powerful muscles in women.
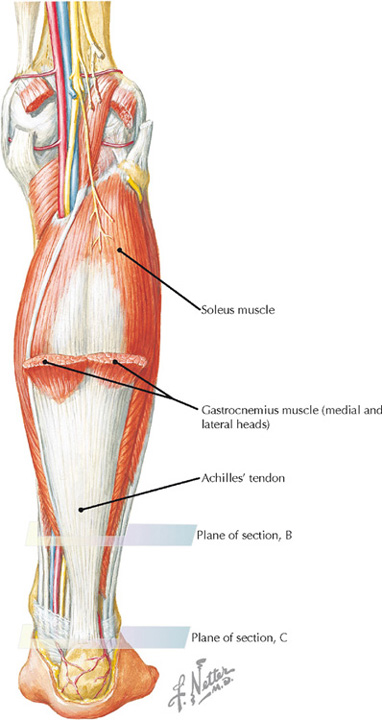
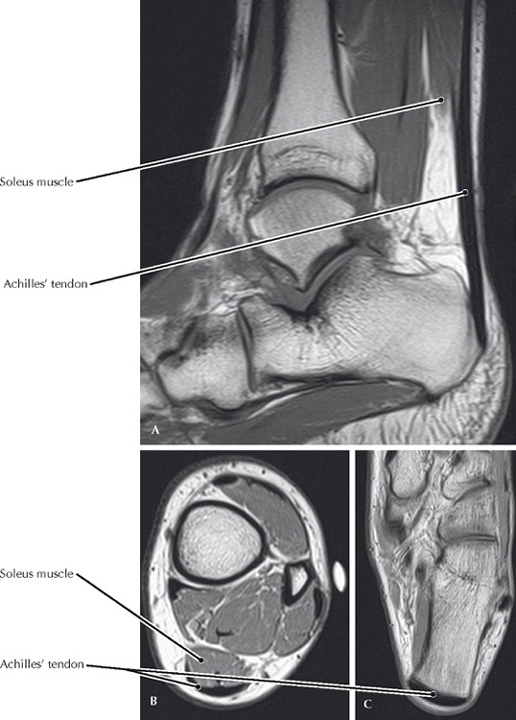
Achilles’ tendon and soleus (Atlas of Human Anatomy, 5th edition, Plate 505)
Sagittal T1 MR image (A) and axial PD MR images (B and C) of the ankle and lower leg
• The gastrocnemius and soleus muscles insert into the calcaneus via the Achilles’ tendon. The primary action of these muscles is to powerfully plantarflex the ankle using the posterior calcaneus as a lever arm. The gastrocnemius fused with the soleus muscle superior to the axial MR images shown here.
• The remaining ankle plantarflexors, such as the tibialis posterior and fibularis (peroneus) longus muscle, are much weaker plantarflexors than the gastrocnemius and soleus muscles because they wind around the malleoli and lack an extended lever arm.
Clinical Note
A ruptured (or torn) Achilles’ tendon may occur when the tendon has been structurally weakened by tendonitis, or when a healthy tendon is subjected to a sudden, unexpected force. When the tendon tears, people often describe feeling a “pop” at the back of the ankle. The injury is accompanied by pain, swelling, and loss of function.
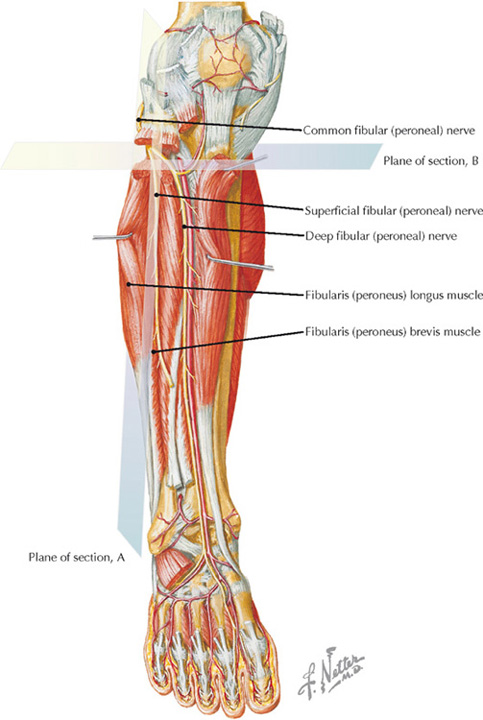
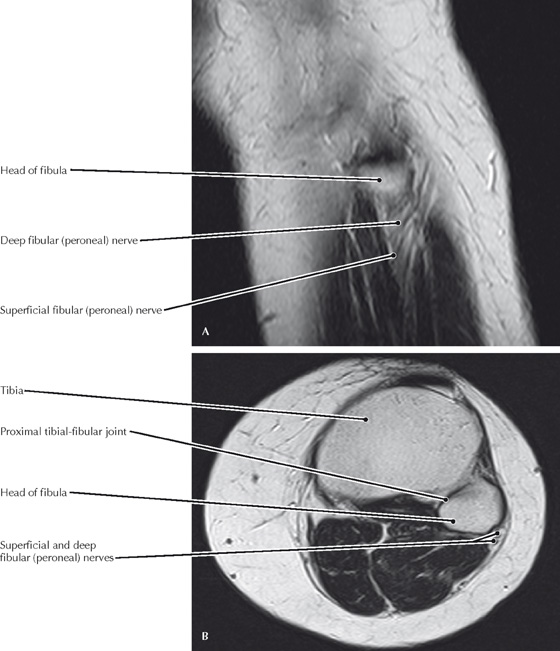
Deep dissection of the anterior leg muscles and nerves (Atlas of Human Anatomy, 5th edition, Plate 508)
Sagittal (A) and axial (B) T2 MR image of the upper leg
• The superficial fibular (peroneal) nerve innervates the fibularis (peroneus) longus and brevis, both of which evert and plantarflex the foot.
• Although very little movement occurs between the tibia and fibula, the superior joint is a plane type of synovial joint.
Clinical Note
As it wraps around the neck of the fibula, the common fibular (peroneal) nerve is vulnerable to injury that results in foot drop because all the dorsiflexors of the foot are innervated by its deep branch.
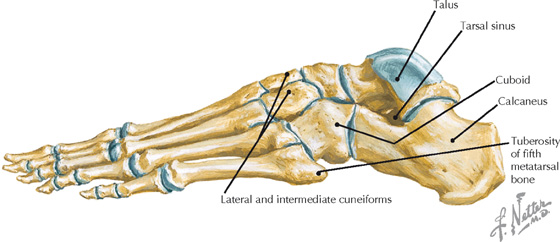
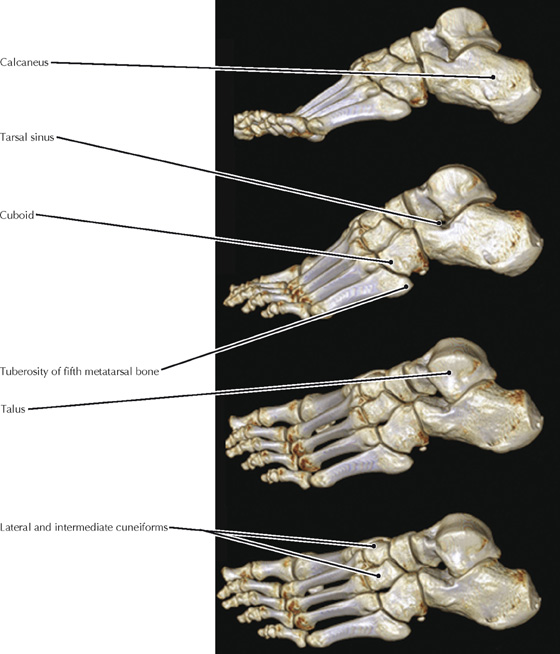
Lateral view of the osteology of the foot (Atlas of Human Anatomy, 5th edition, Plate 512)
Volume rendered CT displays (successive lateral rotations) of the foot
• The tarsal sinus is a cone-shaped region located between the inferior aspect of the neck of the talus and the anterosuperior surface of the calcaneus.
• The tuberosity of the fifth metatarsal may be avulsed during excessive eversion by the fibularis (peroneus) brevis tendon, which attaches there.
Clinical Note
Tarsal sinus syndrome is a painful condition of the tarsal sinus that is associated with a sensation of instability in the hindfoot and that may occur after an inversion injury. It often causes lateral ankle pain.
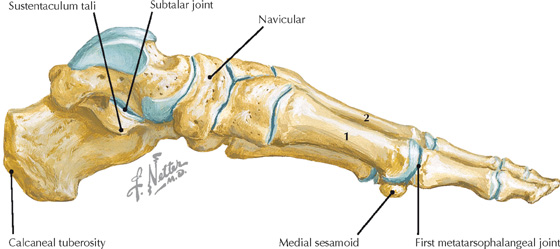
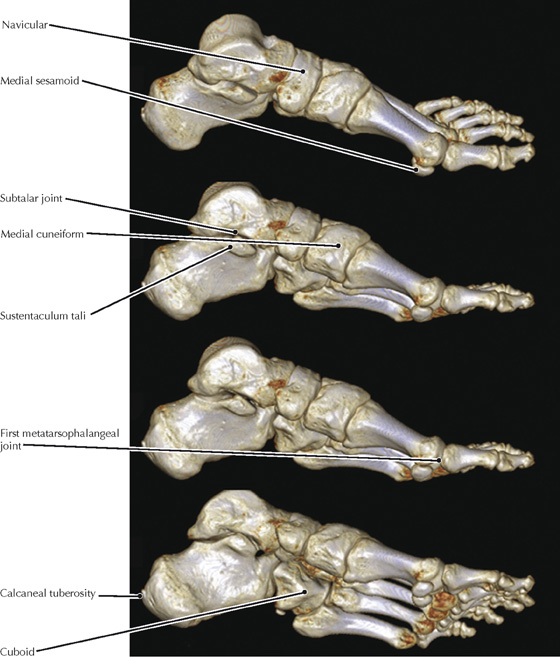
Medial view of the osteology of the foot (Atlas of Human Anatomy, 5th edition, Plate 512)
Volume rendered CT displays (successive medial rotations) of the foot
• Rotating volume rendered displays similar to these can clarify many complex fractures of the hindfoot and midfoot that are otherwise very difficult to comprehend with projectional or cross-sectional images.
• The medial and lateral sesamoid bones are located within the tendons of the flexor hallucis brevis and act to increase the leverage of this muscle.
Clinical Note
Hallux rigidus is a common painful abnormality associated with osteoarthritis at the first metatarsophalangeal joint.
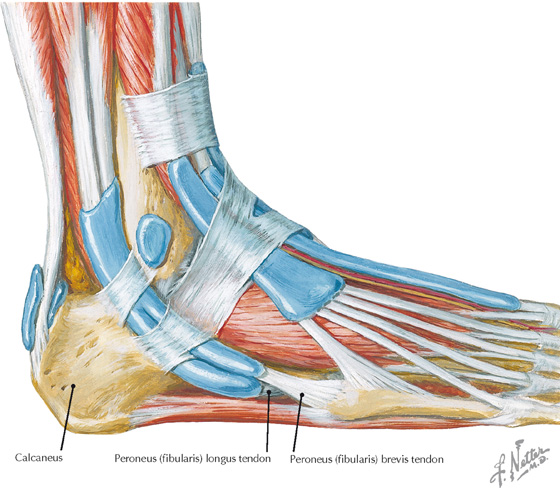
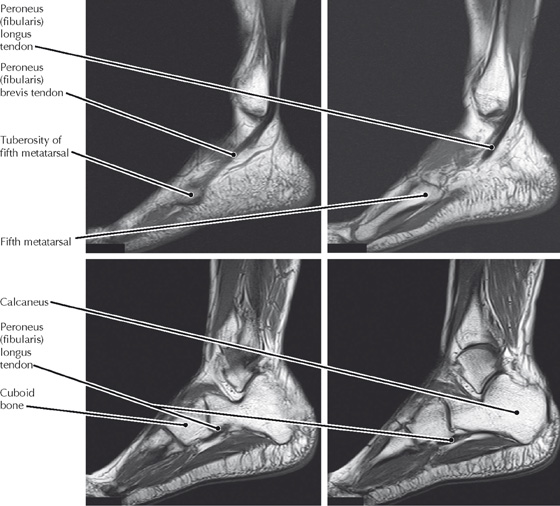
Tendons of the lateral ankle (Atlas of Human Anatomy, 5th edition, Plate 517)
Sagittal T1 MR images of the lateral foot
• The peroneus (fibularis) longus tendon traverses and supports the transverse arch of the foot to insert on the base of the first metatarsal and the medial cuneiform.
• The fibularis (peroneus) brevis tendon inserts on the base of the fifth metatarsal, at the tuberosity.
Clinical Note
Peroneal (fibular) tendon tears (ruptures) are associated with excessive inversion injuries to the ankle joint and cause lateral ankle pain.
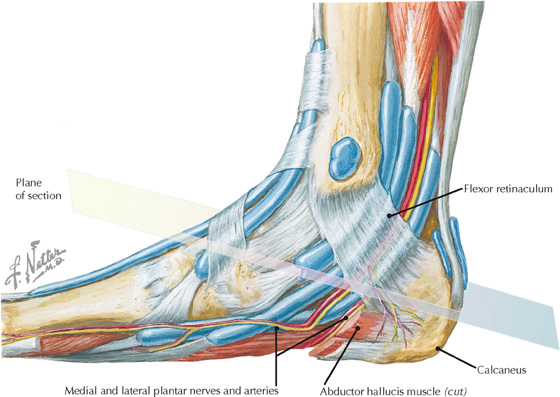
Medial view of the tendons and neurovasculature (tarsal tunnel) at the ankle (Atlas of Human Anatomy, 5th edition, Plate 517)
Oblique T1 MR image through the tarsal tunnel (From Hochman MG, Zilberfarb JL: Nerves in a pinch: Imaging of nerve compression syndromes. Radiol Clin North Am 42(1):221-245, 2004)
• The sustentaculum tali is a projection of the calcaneus that supports the talus along the medial side of the hindfoot.
• Talocalcaneal coalition, which is a fusion of the talus and calcaneus, is a cause of chronic pain and is very difficult to appreciate on plain radiographs.
Clinical Note
As the tibial nerve divides into the medial and lateral plantar nerves, it passes deep to the flexor retinaculum. This area, known as the tarsal tunnel, is a potential site for entrapment of these nerves and the accompanying posterior tibial vessels.
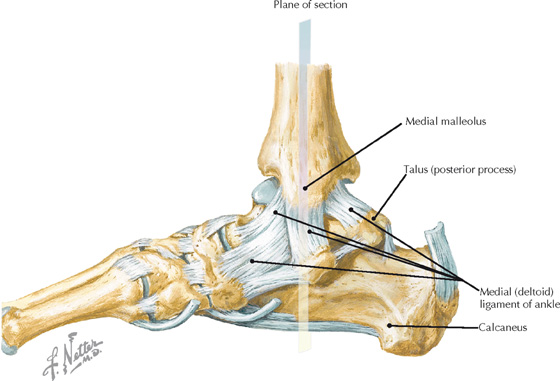
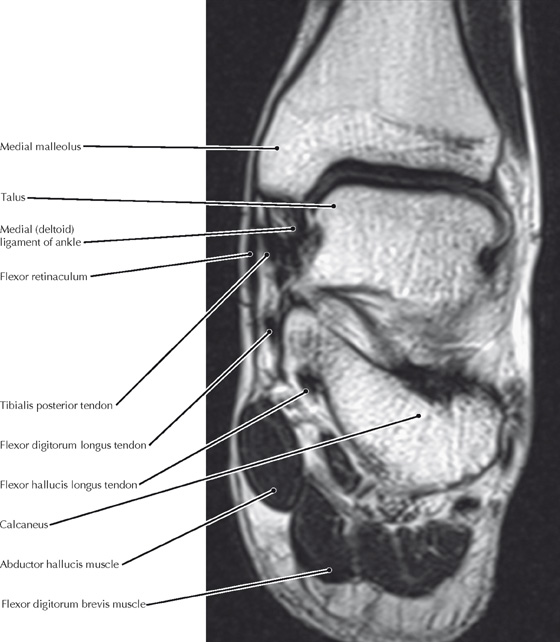
Medial view of the ligaments of the ankle and foot (Atlas of Human Anatomy, 5th edition, Plate 515)
Coronal T1 MR image of the ankle
• The deltoid ligament has four components: anterior and posterior tibiotalar, tibionavicular, and tibiocalcaneal ligaments.
• A more severe injury than the bimalleolar (Pott’s) fracture is a “trimalleolar” fracture involving the posterior lip of the tibia, as well as the distal tibia and lateral malleolus.
• Tendinopathy of the tibialis posterior and flexor hallucis longus is a frequent cause of medial ankle pain.
Clinical Note
Sprains or tears of the deltoid ligament are associated with excessive ankle eversion. A significant eversion injury may result in a bimalleolar (Pott’s) fracture in which the distal fibula and medial malleolus are fractured in addition to the tear in the deltoid ligament.
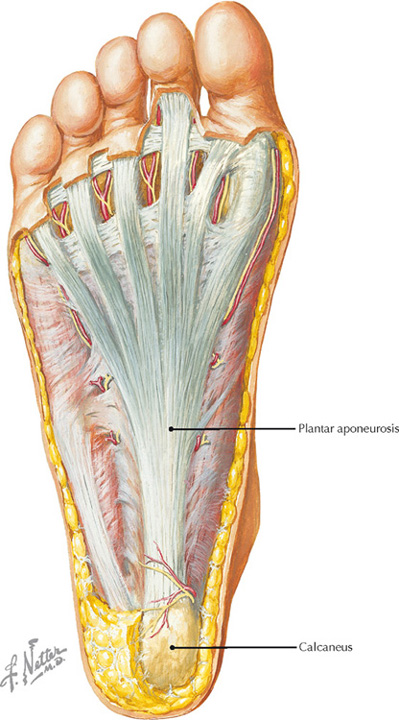
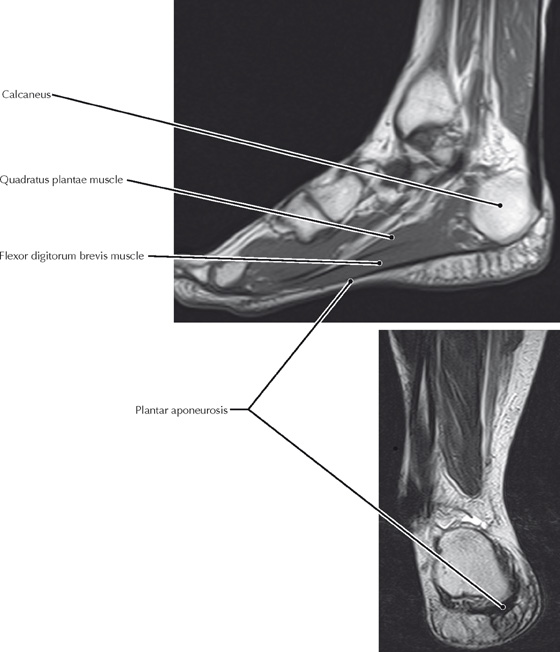
Superficial dissection of the foot showing the plantar aponeurosis (Atlas of Human Anatomy, 5th edition, Plate 520)
Sagittal and coronal T1 MR images of the foot
• A bone spur may develop in association with plantar fasciitis at the junction between the plantar aponeurosis and the calcaneus; this spur may be associated with increased pain during walking.
• The plantar aponeurosis acts as a structural support tie beam, maintaining the integrity of the components of the foot skeleton and especially supporting the longitudinal arch of the foot.
Clinical Note
Inflammation of the plantar aponeurosis at its attachment to the calcaneus results in plantar fasciitis, a painful condition in which the pain is typically felt on the undersurface of the heel. This pain is often the most severe after awakening in the morning.
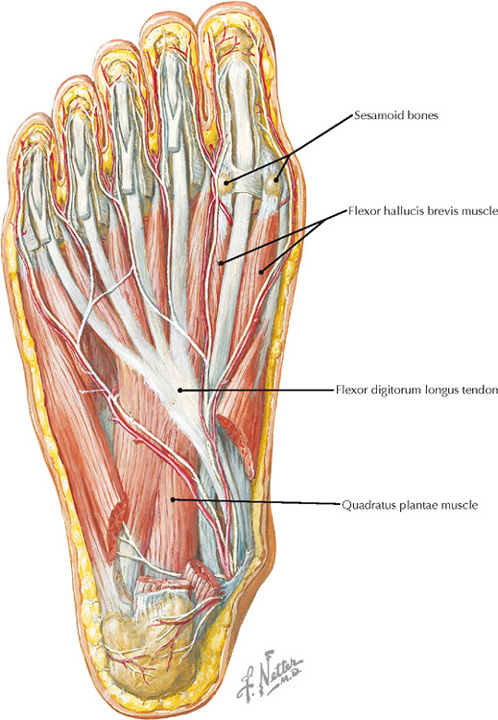
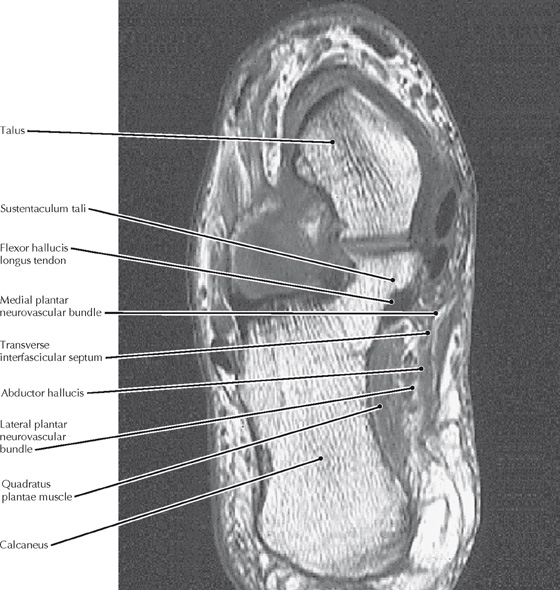
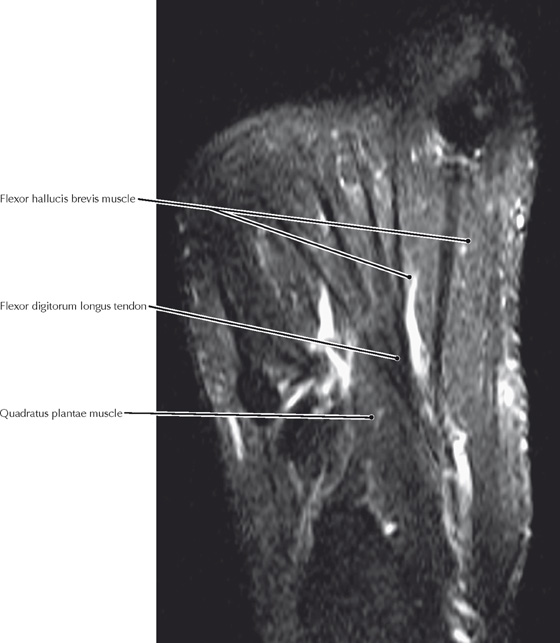
View of the sole of the foot, with the first of four muscle layers removed (Atlas of Human Anatomy, 5th edition, Plate 522)
FS T2 MR image tangent to the plantar surface of the foot
• The flexor digitorum longus tendon corresponds to the flexor digitorum profundus tendon in the upper limb and accordingly inserts into the terminal phalanges of the lateral four digits.
• The quadratus plantae muscle inserts into the tendons of the flexor digitorum longus tendon and aligns the pull of that muscle with the long axis of the foot.
Clinical Note
Hallux valgus is a lateral deviation of the great toe (mnemonic: relate the “L” in valgus to “lateral”) causing inflammation and pain at the first metatarsophalangeal joint. This is called a bunion.