Chapter 235 Cervical Polypectomy
DESCRIPTION
Cervical polypectomy is the removal of cervical or visible endocervical polyps; it is generally a simple, painless office procedure.
REQUIRED EQUIPMENT
TECHNIQUE
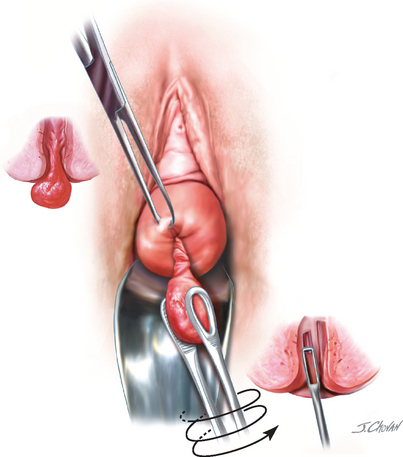
The polyp is first visualized through the use of a standard vaginal speculum. Disinfection with a suitable solution may be performed, although most believe it is not required. The visible portion of the polyp is then grasped, and gentle traction, twisting through several revolutions, or excision accomplishes removal of polyp. If the polyp is thought to arise from high in the endocervical canal, the base may be gently curetted with an endocervical curette. Curettage of the endocervical canal should also be considered to rule out a coexisting hyperplasia or cancer. Although malignancy is rare, all polyps should be submitted for histologic examination. The base of the polyp may be treated with chemical cautery (Monsel solution or silver nitrate), electrocautery, or cryocautery.
FOLLOW-UP
Although the histology of the polyp should be confirmed as benign, malignant degeneration of an endocervical polyp is extremely rare. The reported incidence is less than 1 in 200.
Amesse LS, Taneja A, Broxson E, Pfaff-Amesse T. Protruding giant cervical polyp in a young adolescent with a previous rhabdomyosarcoma. J Pediatr Adolesc Gynecol. 2002;15:271.
Khalil AM, Azar GB, Kaspar HG, et al. Giant cervical polyp. A case report. J Reprod Med. 1996;41:619.
Pradhan S, Chenoy R. Dilatation and curettage in patients with cervical polyps: a retrospective analysis. BJOG. 1995;102:415.