 CHAPTER 127 Oral Cavity
CHAPTER 127 Oral Cavity
The oral cavity is a complex structure including the lips, gums, tongue, teeth, and surrounding structures involved in the functions of chewing and swallowing. The health of oral tissues has a significant impact on the ability to take adequate nourishment and to protect the airway from aspiration. Systemic disorders may have manifestations in the oral cavity that are readily detectable on examination.
EFFECTS OF SYSTEMIC DISEASE ON THE ORAL CAVITY
Medications taken for a variety of conditions may cause oral abnormalities. Drugs with anticholinergic properties diminish saliva production and increase the risk of dental caries and parotitis. Tetracyclines taken before the eruption of the permanent teeth stain the enamel. Excessive fluoride in vitamin preparations or in drinking water can result in mottled teeth. Gingival hypertrophy may be caused by cyclosporine, phenytoin, and calcium channel blockers.
Gastroesophageal reflux (GER) can lead to substantial enamel erosion and caries. Neonatal hyperbilirubinemia can result in discoloration of the deciduous teeth. Renal failure is associated with mottled enamel of the permanent teeth. Congenital syphilis causes marked abnormalities in the shape of teeth, especially incisors and molars. Crohn’s disease is associated with oral ulcers. Abnormal pigmentation of the lips and buccal mucosa is seen with Peutz-Jeghers syndrome and Addison disease. Candidiasis is seen commonly with immunodeficiency disorders and diabetes. Leukemic infiltrates result in gum hyperplasia and bleeding; treatment of neoplastic conditions can cause severe mucositis. Some tumors, including lymphoma, may present as mass lesions of the buccal cavity.
Osteogenesis imperfecta is associated with abnormal dentin and risk of caries. Children with ectodermal dysplasias commonly have malformed or missing teeth. Pierre Robin syndrome is associated with micrognathia and cleft palate. Disorders resulting in facial dysmorphism can have a profound effect on dental occlusion and mandibular function. Examples include mandibulofacial dysostosis, Crouzon syndrome, conditions associated with dwarfism, and others.
DECIDUOUS AND PRIMARY TEETH
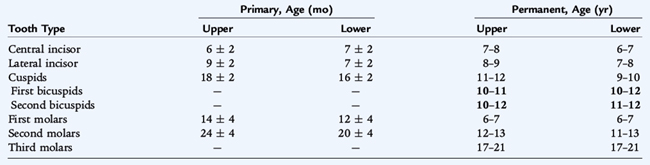
Most infants are born without teeth. Natal teeth are present at birth, are usually supernumerary, and may be poorly attached. No treatment is usually necessary, but removal by a dentist is sometimes needed if they are causing difficulties with feeding or injuries to the tongue. Table 127-1 presents the ages when normal deciduous teeth are acquired. The lower central incisors are the first to erupt, followed by the upper central incisors, lateral incisors, first molars, and bicuspids. Delayed eruption may occur in association with hypopituitarism, hypothyroidism, osteopetrosis, Gaucher disease, Down syndrome, cleidocranial dysplasia, and rickets. Deciduous teeth begin to be replaced by the permanent teeth around age 6 years. The sequence of replacement is similar to that of the appearance of deciduous teeth.
DENTAL CARIES
Etiology
Dental caries, commonly referred to as “cavities,” occur as a result of interactions between the tooth enamel, dietary carbohydrates, and oral flora. There is increased susceptibility if the enamel is abnormal or hypoplastic. Bacteria (Streptococcus mutans) that can adhere to and colonize the teeth, survive at low pH, and produce acids during fermentation of carbohydrates cause dental caries. The diet has a significant role. A classic example is “bottle mouth,” or baby bottle caries. This condition results from allowing an infant to have a bottle in the mouth for prolonged periods, especially during sleep, and with sweet beverages or milk in the bottle. This practice allows bacteria to have continuous substrate for acid production and can result in destruction of multiple teeth, especially the upper incisors. Sticky sweet foods, such as candy, have the same effect.
Epidemiology and Treatment
Risk of caries is associated with lack of dental care and poor socioeconomic status and predictably is greatest in developing countries. Baby bottle caries is seen in 50% to 70% of low-income infants. Treatment of caries involves dental restorative surgery. The carious portion is removed and filled with silver amalgam or plastic. When not properly treated, dental decay results in inflammation and infection of the dental pulp and surrounding alveolar bone, which can lead to abscess and facial space infections.
Prevention
Avoiding inappropriate use of bottles and excessive sweets is a common-sense remedy for baby bottle caries. Oral hygiene offers some protection, but young children (<8 years of age) do not have the ability to brush their own teeth adequately; brushing should be done by the parents. Fluoride supplementation of community water supplies to a concentration of 1 ppm is highly effective in reducing dental caries. Home water supplies, such as from a well, should have the fluoride content tested before prescribing supplements. Excessive supplementation causes fluorosis, a largely cosmetic defect of chalky white marks and brown stains on the teeth. Finally, occlusal sealants applied by a dentist after the eruption of the secondary molars can reduce the cavity rate by about 50%.
CLEFT LIP AND PALATE
Epidemiology
Cleft lip and palate occur separately or together and affect approximately 1 in 700 infants. Clefting is more common in Asians (1:500) and least common in African Americans (1:2500). It occurs with two possible patterns: isolated soft tissue cleft palate or cleft lip with or without associated clefts of the hard palate. Isolated cleft palate is associated with a higher risk of other congenital malformations. The combined cleft lip/palate type has a male predominance.
Etiology
Cleft lip is due to hypoplasia of the mesenchymal tissues with subsequent failure of fusion. There is a strong genetic component; the risk is highest in children with affected first-degree relatives. Monozygotic twins are affected with only 60% concordance, suggesting other nongenomic factors. Environmental factors during gestation also increase risk, including drugs (phenytoin, valproic acid, thalidomide), maternal alcohol and tobacco use, dioxins and other herbicides, and possibly high altitude. Chromosomal and nonchromosomal syndromes are associated with clefting, as are specific genes in some families.
Clinical Manifestations and Treatment
Cleft lip can be unilateral or bilateral and associated with cleft palate and defects of the alveolar ridge and dentition. When present, palatal defects allow direct communication between the nasal and oral cavities, creating problems with speech and feeding. Feeding infants with clefts requires the use of squeeze-bottles, special nipples, nipples with attached shields to seal the palate, or even gastrostomy in severe cases. Surgical closure of the cleft lip is usually done by 3 months of age. Closure of the palate follows, usually before 1 year of age. Cosmetic results are often good but depend on the severity of the defect.
Complications
Speech is nasal as a result of the cleft palate. Surgical treatment is effective, but sometimes does not restore palatal function completely. Speech therapy or occasionally the use of a speech-assisting appliance may help. Frequent episodes of otitis media are common, as are defects of teeth and the alveolar ridge.
THRUSH
Epidemiology
Oropharyngeal Candida albicans infection, or thrush, is common in healthy neonates. The organism may be acquired in the birth canal or from the environment. Persistent infection is common in breastfed infants as a result of colonization or infection of the mother’s nipples. Thrush in healthy, older patients can occur but suggests a possible immunodeficiency, except after recent broad-spectrum antibiotic use or when found in diabetics.
Clinical Manifestations
Thrush is easily visible as white plaques, often with a fuzzy appearance, on oral mucous membranes. When scraped with a tongue depressor, the plaques are difficult to remove, and the underlying mucosa is inflamed and friable. Clinical diagnosis is usually adequate, but may be confirmed by fungal culture or potassium hydroxide smear. Oropharyngeal candidiasis is sometimes painful (especially if associated with esophagitis) and can interfere with feeding.
Treatment
Thrush is treated with topical nystatin or an azole antifungal agent such as fluconazole. When the mother’s nipples are infected and painful, consideration should be given to treating her at the same time. Because thrush is commonly self-limited in newborns, withholding therapy in asymptomatic infants and treating only persistent or severe cases is a reasonable approach.