3 Control of pain and anxiety: selection of and preparation for sedation or anaesthesia
ASSUMED KNOWLEDGE
It is assumed that at this stage you will have at least some knowledge/competencies in the following areas:
If you think that you are not competent in these areas, revise them before reading this chapter or cross-check with relevant texts as you read.
THE PURPOSE OF THIS CHAPTER
It is not possible to cover in detail, in this book, all the issues concerned with control of pain and anxiety in oral surgery. There are, however, other texts which do deal thoroughly with these matters. Nonetheless there are several issues of direct relevance to the practice of oral and maxillofacial surgery, which are worth covering here.
We would not wish pain and anxiety control to appear separate from surgical treatment planning: it is a central issue. This chapter therefore attempts to summarize important points of surgical relevance that should make the treatment less upsetting for both patient and dentist.
PAIN
What pain is
Pain is a defence reaction that tends to be associated with actual or perceived injury. A key feature of pain is that it conditions avoidance. It must be unpleasant to be effective. Not all pain, however, is the same. The distinction between the sharp pain of a needle prick and the ache of overworked muscles is all too obvious and the separation of these two examples into fast, type 1, or acute pain and slow, type 2 or more chronic pain is fairly easy. It is also of considerable therapeutic advantage because the latter responds well to analgesics, but the former does not. However, there are almost as many types or descriptions of pain as there are conditions that cause it. Colicky abdominal pain, the throbbing pain of an abscess and the dull ache of myofascial pain are remarkably different in nature.
Pain may result from a range of stimuli: penetrating injury, pressure, heat, electrical stimulation, inflammation, muscular fatigue, etc. Almost any tissue (excluding dental enamel) may be the source.
This chapter is concerned with pain associated fairly closely with surgery. This includes the pain that would be associated with the surgery if no measures (such as local anaesthesia) were taken to prevent it and the pain so often experienced after surgery, which is more associated with inflammation.
Although we have said that pain is a defence reaction, there is little evidence that it is in any other way beneficial and for that reason we should do all that we can to prevent it during and after any surgery.
It is important to remember that only one individual is in a position to define pain: the patient. Therefore when a patient says that they have pain, they have—it is of no practical benefit to debate with them whether their experience is pressure, movement or whatever! It is wise to remember also that pain requires consciousness to be experienced, and that it is influenced by emotional state, tiredness and anticipation. Local sensitization of the peripheral nerves by inflammatory mediators considerably increases pain experience and can cause difficulty in controlling the pain of patients who have been in pain for several days. This is probably one of the commonest reasons for failure of local anaesthesia in such patients.
How to recognize pain
Your patient will tell you when they are in pain. However, there are some situations where a patient has difficulty in communicating or might not wish to worry you about their pain. Some will even think it is ‘normal’ to experience pain during a surgical procedure.
Pain tends to elicit certain reactions, which can be noted. Bodily movement, tensing of the body, wide opening or screwing shut of the eyes, dilation of the pupils, skin pallor and sweating are all readily recognizable. Noises (ranging from grunts to screams) can be illustrative—and may require immediate action.
ANXIETY
What anxiety is
Anxiety is also a defence reaction, ranging from disquiet, through apprehension and anxiety, to fear and downright terror. Like pain, we must accept that anxiety is a factor that may need to be measured, rather than simply noted as present. Anxiety is the anticipation of an unpleasant event that conditions avoidance.
Some anxiety or fear is clearly advantageous. For example, finding oneself at the edge of a cliff or having misjudged the speed of an oncoming car makes one move swiftly to reduce the danger (many people will also go out of their way to cause anxiety by bungee jumping or fairground rides). But anxiety associated with dental treatment is often unhelpful because it not only causes great suffering but also creates barriers to dental care. It is the dental practitioner’s obligation to aim to minimize their patients’ suffering’and that includes their anxiety.
Some anxiety may even be frankly damaging. For example, in a patient with moderate to severe ischaemic heart disease, the increase in work done by the heart as a result of the fear might not be matched by an increase in coronary blood flow. This can precipitate angina or worse.
Where fear of a particular thing, event or concept is unreasonably excessive it may be described as a phobia. The distinction between what is a somewhat exaggerated concern about dental treatment and what is a true phobia is rather blurred.
How to recognize anxiety
The patient’s description is again of great value, and many people will openly discuss their concerns about dental treatment. However, embarrassment or loss of face can be experienced (particularly amongst men) by admitting to fear, particularly when the patient feels that their fear may be irrational. There is therefore an underreporting of anxiety and considerable variation in the weight that individuals place on their own fear. For this reason it is important that you actively look for and assess the level of anxiety.
Clues can be found in body language: posture and facial expression. Overt signs of sympathetic nervous system activity such as pallor and sweating may be diagnostic. Behaviour such as failing to attend or cancelling appointments, aggressive behaviour or tearful episodes may also be clues. If you need more evidence, the patient’s pulse and blood pressure would show considerable increases.
LOCAL ANAESTHESIA
Why use local anaesthetics?
Local anaesthetics have become the most widely used form of pain relief in dentistry. A variety of techniques and drugs are available and can be varied depending on the patient’s medical and dental history and the pharmacology of the agent.
The drugs are safe to use. Tens of millions of cartridges of local anaesthetics are administered by dentists in the UK each year. The mortality rate associated with dental treatment that does not involve general anaesthesia is about one case per annum and even amongstsuch cases local anaesthesia is rarely regarded as causative of the death. Few drug systems in medicine have such a good safety record.
The drugs are effective. In almost all dental applications it is possible to completely abolish pain during the procedure and, with care, pain on administration of the drug can be kept to an acceptable level.
Reducing pain on administration
The application of lidocaine or benzocaine in the form of a paste, gel or spray to the oral mucosa can result in loss of sensibility to a depth of a few millimetres in a few minutes. This can abolish the pain of needle penetration and, for superficial injections, dramatically reduce the discomfort on injection. This can also have a major impact on the anticipation of pain in those particularly frightened by injections.
The use of topical local anaesthetics does have disadvantages, however. By spreading widely around the mouth they can induce numbness in a much wider area than would otherwise be necessary. Also, they cannot penetrate to the depth at which the inferior alveolar nerve block or greater palatine nerve block injections are given.
For procedures involving the skin topical lidocaine is of no value. However, EMLA cream does penetrate deeply enough to be effective. It should be left on the skin for at least one hour before the procedure. Amethocaine gel can also be effective on skin, and possibly over a time period shorter than that of EMLA, but is more likely to cause skin irritation.
Pain of injection can also be reduced by injecting slowly, distracting the patient and perhaps by stimulating nearby tissues (such as by compressing the cheek between finger and thumb) to activate the central neurological ‘gate mechanism’. Rapid penetration of the mucosa by the needle results in far less discomfort than that experienced on slow pressure. This is made easier in lax tissues by tensing the mucosa before needle penetration.
Extent of anaesthesia required
In preparing for surgical procedures you should plan carefully the area of anaesthesia. If a mucoperiosteal flap is to be raised, the extent of anaesthesia required must include the area at the centre of the surgery, the whole of the distribution of the flap itself and all the areas of mucosa through which a suture needle will eventually pass. Where surgery is to involve more than one quadrant you should consider exactly how much local anaesthetic will be required; for example, if you were attempting to extract three molar teeth in each quadrant in one session, it may not be possible to achieve satisfactory anaesthesia without exceeding the recommended maximum dose.
Failure
Failure to achieve satisfactory pain relief for surgical procedures at the first attempt is not uncommon. Failure may be associated with pain and local inflammation, which result in local neural sensitization (see p. 13). This is a difficult problem in a patient who is particularly anxious about dental treatment and who puts off attending until their pain is unbearable. There may also be a relationship between failure and severe anxiety, which is a common problem in the latter type of patient.
Failure is more common with regional block anaesthesia, probably for anatomical reasons. Although anatomical landmarks provide a guide, no two patients are the same shape and variation should be expected. If you experience repeated failures in regional block anaesthesia you should revise the anatomical guidance in textbooks and consider the accuracy with which you are following recommendations. Rarely, there may be failure due to aberrant innervation. How to manage local anaesthetic failure is described well by Meechan (1999).
NON-PHARMACOLOGICAL CONTROL OF ANXIETY
A great deal can be done to reduce anxiety without medication. Seen from the opposite perspective, there are a number of things that might make things worse: uncertainty, worries about pain, worries about being unable to control the situation. The attitude of the whole dental team to the patient can make a major contribution to the comfort of the patient.
Openness and honesty are very important. You do not need to describe unpleasant things in graphic detail, but advising your patient that he or she will feel pressure and hear noises, but should suffer no pain, is reassuring and still permits alternative outcomes.
Long periods of silence are worrying; try to maintain a flow of conversation. Avoid repeated questions as they prompt the patient into action (this can interfere with treatment) and questions such as ‘Are you all right?’ signal to the patient that you think they might not be. It may be helpful to find a topic of conversation that in some way interests the patient. Distraction by conversation, background music, surgery decor can all contribute to a reduced level of anxiety. It may be helpful to talk through a pleasant scenario for the patient during treatment. They might be asked to imagine that they are on the beach in the sun, it is warm and they are resting on soft sand.
Flexibility in your approach—for instance, at the patient’s request performing only one or two extractions at a time, when several are required—can also give the patient a considerable feeling of control. Timing can also be important. For a new and nervous patient it is better to start treatment with less frightening procedures.
Hypnosis is thought of as a more formal psychological technique, which at its best gives the patient full control over whether they suffer pain or any other adverse effect. However, distraction is probably the most minor form of hypnosis. The depth that can be achieved is dependent upon the patient, the environment, the skill of the dentist and the amount of time and effort employed.
SEDATION
What it is
‘Conscious sedation’ is defined as ‘A technique in which the use of a drug or drugs produces a state of depression of the central nervous system enabling treatment to be carried out, but during which verbal contact with the patient is maintained throughout the period of sedation.’ The drugs and techniques ‘should carry a margin of safety wide enough to render loss of consciousness unlikely.’ In the UK ‘any technique resulting in the loss of consciousness is defined as general anaesthesia’ and thus ‘deep sedation’ is considered in this category (DoH 2003).
It is anticipated with current sedation methods that there will be considerable relief of anxiety as part of the mechanism that ‘enables treatment’. However, unlike general anaesthesia (GA), no currently available sedation technique offers on its own sufficient pain control to permit surgical treatments to be carried out. For that reason a local anaesthetic is also required.
Sedation may be achieved with drugs given by mouth, inhalation or intravenous injection.
It is not possible in this book to review in detail all aspects of sedation for dental purposes and the reader is referred to texts specifically designed for that purpose (e.g. Girdler and Hill 1998, Meechan et al. 1998). However, it is worth considering what is desirable in sedation in order to help select an appropriate technique.
The aim must be to exercise maximum control over the perceived problem (often anxiety) in terms of onset, duration and depth, with a minimum of adverse effects. The latter might include the potential for problems with the cardiovascular or respiratory systems, loss of cooperation by the patient, requirement for venepuncture, the use of a mask, the requirement for altered activities after treatment. Clearly, at present, sedation techniques fall a long way short of being perfectly acceptable and absolutely controllable. For that reason it is usually necessary to tailor the technique chosen to the patient, the treatment to be performed and the particular skills of the team providing the treatment.
Oral, inhalational or intravenous sedation?
Oral sedation
Oral sedation with a drug such as temazepam has the advantages of being safe, highly acceptable to patients and easy to administer. Unfortunately, the effect relies on the patient following instructions, there is a long latent period before the drug takes effect and absorption is unpredictable. Therefore the dose required is unpredictable and, in the interests of safety a lower dose than needed is generally given. Oral sedation can be very successful in the individual who requires relatively little support and in those for whom mask and injections may be unacceptable.
Inhalational sedation
Inhalational sedation commonly uses a mixture of nitrous oxide and oxygen, although much work has been done to develop techniques using other anaesthetic gases. There are great advantages to nitrous oxide sedation. The depth of sedation is controllable, from the deepest to the lightest points, over a period of minutes, because of the rate at which the gas is cleared by respiration. This also means that within 15 minutes of the end of sedation almost all of the sedative effect is gone. With purpose-designed relative analgesia machines the risks due to oversedation can be brought close to zero. finally, nitrous oxide has some analgesic effect, which can contribute to the overall pain relief.
The disadvantages are few. However, the mask limits access to the mouth, and nasal administration requires that the patient breathe through his nose. Some risk is believed to be associated with high concentration of nitrous oxide in the surgery, which means that the environment must be adapted for treatment, such as using active scavenging devices and good ventilation. It may also be that the maximum depth of sedation achievable without the patient becoming disorientated is still not as great as can be achieved by intravenous sedation.
Intravenous sedation
Intravenous sedation is of rapid onset (up to 2 minutes after injection of the drug, e.g. midazolam) and the required dose is usually readily titrated against the patient’s needs. The level of sedation achievable whilst maintaining cooperation and verbal contact is somewhat deeper than can be achieved with inhalational sedation. There is no mask; therefore access is marginally better and there is no requirement for continued nasal breathing. However, the use of intravenous sedation in children is not widely accepted and can be associated with unexpected reactions. Also, recovery from sedation with midazolam usually takes about an hour. During recovery the patient must be accompanied and monitored; this usually requires separate recovery facilities other than the dental chair. Although it is possible to reverse midazolam sedation with the antagonist flumazenil, this is not regarded as ideal routine practice as the latter drug has a shorter half-life.
Advantages
Conscious sedation offers a lower mortality risk than GA, but quantifying that risk for sedation in dentistry is not accurate. The figure is believed to be of the order of one in a million. It also has the distinct advantage, in theory, of maintaining active reflexes to protect the upper airway. The patient is able to cooperate in the treatment. In addition, the patient can be offered the opportunity of reduced levels of sedation for future treatment; this may allow some patients who are terrified of dental treatment to move towards more conventional provision of care. Sedation does not require the presence of an anaesthetist and therefore makes the dental treatment more convenient to arrange.
Preparation of patient
There is some dispute as to whether it is necessary to starve the patient fully, as for GA. It is true that reduction in reflex activity is slight, but sedation can be used very successfully to suppress the gag reflex, to permit dental treatment. Regurgitation of gastric contents seems to be particularly rare with moderate sedation and the risk of aspiration must be seen as very small. Nevertheless, most authorities recommend that the patient avoids a heavy meal before treatment, and a period of full starvation of 2 hours is a reasonable precaution.
In almost all other respects preparation is as for GA. All advice to the patient, detailed discussion and a written record of consent should take place preoperatively. There should be a responsible, fit escort and the patient should avoid demanding activity of the hands or brain for 24 hours (for inhalational sedation it may be reasonable to shorten that period considerably). The procedure should be delayed in the presence of acute medical conditions.
Detailed recommendations on both the preparation of the patient for and discharge of the patient after sedation may be found in the document ‘Conscious sedation in the provision of dental care’ (DoH 2003) as well as in standard textbooks on the subject.
Airway protection
The airway can still be at risk during sedation, partly because the patient is so relaxed and partly because of a reduction in efficiency of reflexes. For this reason some operators place a pack over the back of the tongue for extraction work. There do not appear to be real problems with the reflexes with inhalational sedation.
It is wise to avoid large quantities of water for irrigation and maintain suction throughout the procedure.
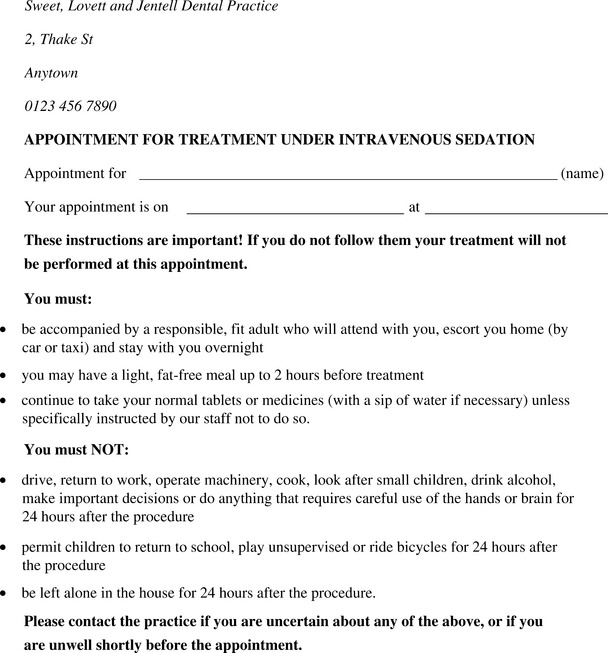
Model instructions to patients
Figure 3.1 is an example of the sort of instructions that may be given to the patient at the time of booking a sedation appointment.
GENERAL ANAESTHESIA
Advantages
General anaesthesia has been used widely for the control of pain in dentistry since the end of the nineteenth century. Indeed, a great deal of the early development of GA was carried out by dentists for dental work, particularly in the UK. By eliminating pain, anxiety and other emotional responses to surgery, the technique has an obvious attraction. It is possible rapidly to render a patient non-responsive, permitting the dentist to concentrate wholly on the surgical task in hand. It can also eliminate muscular activity and reflex responses such as tremors or retching that can make some dental manipulations difficult. And, better still, the patient usually has no recollection of any of the events that have taken place.
Problems
There is however, a down-side to GA: there is a risk of mortality or morbidity with every general anaesthetic given. Patients need to be assessed on an individual basis, taking into account the range of techniques available for behavioural management, pain and anxiety control. GA should be prescribed only when absolutely essential.
The administration of GA requires many additional measures to maximize safety: an anaesthetist must be present; additional equipment is required, measures must be taken to secure integrity of the airway, preparatory measures are needed and patients less fit to undergo the procedure are excluded.
GA deprives the patient of the ability to cooperate and prevents consultation during the procedure. The loss of muscle tone means that action must be taken to keep the mouth open. Additional procedures may also be required to prevent other injury during anaesthesia, such as taping the eyes shut.
An additional point, of some importance, is that, for the patient undergoing treatment under GA because of anxiety, there is no easy mechanism for them to progress towards treatment by a less risky method: they are either awake or asleep.
Indications
There are no absolute indications for the use of general anaesthesia, but there are circumstances in which it is often the preferred approach to control of pain and anxiety:
The referring practitioner has an obligation to discuss alternative methods of control of pain and anxiety with a patient and assure themselves that the patient requires, and is fit for anaesthesia, prior to referral.
Equipment, drugs, competencies
The equipment, the drugs and the techniques of anaesthesia have become progressively more sophisticated over the past century and now require considerable training and expertise to operate to maximum safety. Thus an expert anaesthetist is needed to deliver the anaesthesia, and he or she must be supported by staff specifically trained for the purpose. It is now mandatory in the UK that GA for dental purposes be provided in a hospital setting (GDC 2005).
Fitness
The risk associated with GA is dependent on a number of factors. These must be taken into account if a patient is to benefit from GA. A useful simple measure of fitness for anaesthesia is that recommended by the American Society of Anesthesiologists (ASA 1963) (Table 3.1).
Table 3.1 ASA measures of fitness for anaesthesia
| I | The patient has no organic, physiological, biochemical or psychiatric disturbance. The pathological process for which surgery is to be performed is localized and does not entail a systemic disturbance. Examples: a fit patient with an inguinal hernia, a fibroid uterus in an otherwise healthy woman, a cyst of the jaw. |
| II | Mild to moderate systemic disturbance caused either by the condition to be treated surgically or by other pathophysiological processes. Examples: slightly limiting organic heart disease, diet-controlled diabetes, mild hypertension or anaemia. |
| III | Limitation of lifestyle. Severe systemic disturbance or disease from whatever cause, even though it may not be possible to define the degree of disability with finality. Examples: angina pectoris, healed myocardial infarction, severe diabetes with vascular complications, moderate to severe degrees of pulmonary insufficiency. |
| IV | Severe systemic disorders that are already life threatening, not always correctable by operation. Examples: patients with organic heart disease showing marked signs of cardiac insufficiency, persistent angina, active myocarditis, advanced degrees of pulmonary, hepatic, renal or endocrine insufficiency. |
| V | The moribund patient who has little chance of survival but is submitted to operation in desperation. Examples: the burst abdominal aneurysm with profound circulatory collapse, major cerebral trauma with rapidly increasing intracranial pressure, massive pulmonary embolus. Most of these patients require operation as a resuscitative measure with little, if any, anaesthesia. |
Dental treatment on people in classes IV and V is rarely appropriate and would almost never justify general anaesthesia.
Morbid obesity is a special problem with GA. It can result in hypertension, difficulties in airway management, poor ventilation even in the intubated patient, chest infection, deep venous thrombosis, increased doses of anaesthetic drugs and consequent delayed recovery. In addition, moving the overweight, unconscious person is much more difficult. Obesity may be defined as a body mass index (BMI) exceeding 30 (BMI is calculated as weight (kg) divided by height (m) squared).
Age is not of itself a contraindication to GA, but the very young pose particular anaesthetic problems that may be better dealt with by paediatric anaesthetists in a suitably equipped setting. Elderly people are not only prone to diseases that contraindicate GA but may not tolerate the rigours of GA well, even if fit.
Pregnancy is a contraindication to GA because of risks to the fetus and, in the later stages, risks to the mother associated with the enlarged uterus exerting pressure on the chest and the abdominal veins.
A range of temporary disorders, typified by colds, influenza and sore throats increases risks associated with GA. An individual who is currently undergoing medical investigation, but for whom a diagnosis is not yet available, may also be at risk when undergoing GA. Such risks can usually be avoided by deferring the planned procedure.
Some disorders require a degree of preparation before the GA. For example, a person with type 1 diabetes may require administration of glucose (and insulin) by infusion.
Investigation
There are a number of situations in which a potential medical disorder cannot be evaluated entirely from the patient’s history and for which further investigation would be wise. The examples given here are in no way a complete list of potential investigations, but should serve to indicate the importance of considering medical risk beyond that which the patient alone can describe.
For any patient or situation where the best course of action is uncertain the practitioner should discuss the patient with the anaesthetist who would perform the anaesthetic. On occasion, the anaesthetist may wish to see the patient before making a decision to continue.
Feeding
If there is a significant amount of food within the stomach there is a risk that, during anaesthesia, reflux of gastric contents will occur. As loss of consciousness is associated with loss of cough and swallowing reflexes, there is a concomitant risk of aspiration of gastric contents into the lungs. Gastric contents are extremely damaging to the lining of the respiratory tract and can cause a bronchiolitis, pneumonia and adult respiratory distress syndrome. Solid material could also obstruct part of the airway. The risk of aspiration is believed to increase with increased volume of stomach contents.
It is therefore normal practice to require a patient to refrain from eating or drinking for a period before undergoing GA, commonly for at least 6 hours before GA. That period may be shortened for a small, controlled quantity of clear liquid, particularly in children. The emptying of the stomach is greatly delayed by fatty foods, anxiety or trauma. For hospital inpatients it is possible to control these variables, but that is less easy for outpatients. It is also worth remembering that patients may put greater emphasis on their own comfort than on following what they consider to be arbitrary rules given them by doctors or dentists.
Escort
After an outpatient procedure under GA the patient may be permitted to go home when they are steady on their feet and thinking clearly, but the anaesthetic drugs should be regarded as still influencing their system for at least a few hours. In order to ensure their safety, if they are to go home, they must be accompanied by a responsible and fit adult. They should refrain from driving for 24 hours, and thus the mode of transport must be planned in advance.
Consent
Consent must be obtained before any procedure, but it is doubly important before GA or sedation that the whole procedure is discussed thoroughly because the patient cannot be consulted during the procedure. Also, because GA can be a frightening experience, it is important that consent is obtained away from the environment in which treatment is to take place. Written consent is required.
Recovery and discharge
During the recovery phase following GA, the patient must be monitored continuously by the anaesthetist, or other trained individual who is directly responsible to the anaesthetist. Adequate recovery facilities must be available and the patient should be appropriately protected. The anaesthetist decides when the patient is fit for discharge home, and a check must be made that there is an accompanying responsible adult.
Importance of the mode of anaesthesia to the surgery
The mode of administration and maintenance of anaesthesia is determined by the anaesthetist in consultation with the surgeon.
The placement of a naso-endotracheal tube and having the patient supine gives good access and ample operating time, but intubation is not without its problems (e.g. injury to the nasal mucosa with bleeding into the pharynx). Orotracheal intubation may give better access to the anterior maxilla.
The laryngeal mask (a device that connects an anaesthetic tube to an inflatable mask which seals the airway just above the larynx) works reasonably well for oral surgical procedures. The tube enters the patient through the mouth, inevitably obstructing access to some degree, but the device is associated with less damage to the lining of the nose and larynx than formal intubation and the airway is secure enough to permit most minor oral surgical procedures without difficulty.
There are some situations in which control of the airway must be managed via nasal intubation, notably operation on fractures affecting the jaws or on the temporomandibular joint, where being able to place the teeth in occlusion during operation is essential.
Inpatient or outpatient (day stay)?
For GA where the patient is expected to return home the same day:
In all other circumstances, if a patient is to undergo GA it must be as an inpatient.
WHAT IF NONE OF THESE WILL DO?
Occasionally the practitioner is faced with a patient who is unfit for GA, even on an inpatient basis, but who will not tolerate treatment under local anaesthesia, with or without sedation. It is right in this situation to attempt to balance the risks and potential suffering for each option.
Sometimes there may be advantage in deferring treatment until after a medical event that might be expected to be followed by an improvement in fitness (for instance a woman in the last trimester of pregnancy or a patient about to undergo a coronary artery bypass graft).
Rarely the decision will be made that the risks associated with treatment, which the patient can accept, outweigh the benefits in terms of reduced suffering or potential future suffering. In those circumstances that particular treatment should not be offered: a final decision on such a course of action may be better taken by a hospital specialist.
ANALGESICS
At the beginning of the chapter it was noted that pain may predictably occur during and after a surgical procedure. There are several approaches to postsurgical pain.
Standard local anaesthetics (such as lidocaine with epinephrine) will give pain relief for several hours. It appears that local anaesthetic drugs may reduce the local neural sensitization of surgery and thus reduce pain considerably even after the drug itself has worn off. Longer-acting local anaesthetics such as bupivacaine (with epinephrine) may be used for pain relief after surgical procedures and may give relief for 8 hours or more. However, the numbness associated with these drugs is itself found to be unpleasant by some patients.
Analgesic drugs, such as ibuprofen, paracetamol or opioids are effective against postoperative pain. The author’s first choice is ibuprofen on grounds that it is effective, generally safe, cheap, available over the counter and is a rational choice because of its antiinflammatory effect. However this drug should be avoided in those who have:
Many arguments are raised for and against alter-natives and it can be very confusing for the young practitioner to choose with confidence. Probably more important than details of precisely which drug to choose is that one does actually prescribe or recommend an analgesic! It is also rational to give the analgesic drug early. Particularly antiinflammatory medication is better at preventing pain than stopping it. When analgesia is given before a painful event this may be called ‘preemptive’ analgesia. The choice may also reasonably be affected by the patient’s preference.
Corticosteroids also reduce pain and some surgeons routinely give a drug such as dexamethasone for surgical patients. The drugs reduce swelling simultaneously. There is little evidence of damage caused by use of steroids in this way, but the evidence that steroids add significantly to the benefits of the use of analgesics and local anaesthetics is variable.
American Society of Anesthesiologists. New classification of physical status. Anesthesiology. 1963;24:111.
Cannell H. Evidence for the safety margins of lignocaine local anaesthetics for per-oral use. British Dental Journal. 1996;181:243-249.
Cawson R.A., Curson I., Whittington I. The hazards of dental local anaesthetics. British Dental Journal. 1983;154:253-258.
Coplans M.P., Curson I. Deaths associated with dentistry. British Dental Journal. 1982;153:357-362.
General Dental Council (GDC). Standards for dental professionals. London: GDC, 2005.
Girdler N., Hill C.M. Sedation in dentistry. Oxford, UK: Wright, 1998.
Meechan J.G. How to overcome failed local anaesthesia. British Dental Journal. 1999;186:15-20.
Meechan J.G., Robb N.D., Seymour R.A. Pain and anxiety control for the conscious dental patient. Oxford, UK: Oxford University Press, 1998.
UK Department of Health (DoH). Conscious sedation in the provision of dental care. Report of an expert group on sedation for dentistry. London: DoH, 2003.
SELF-ASSESSMENT
Answers on page 262.