13 Maxillofacial trauma
ASSUMED KNOWLEDGE
It is assumed that at this stage you will have knowledge/competencies in the following areas:
If you think that you are not well equipped in these areas, revise them before reading this chapter or cross-check with texts on those subjects as you read.
INTENDED LEARNING OUTCOMES
At the end of this chapter you should be able to:
INTRODUCTION
Facial injury can occur in isolation or in combination with injuries elsewhere. Regardless of the site of injury, there are local and systemic effects. Trauma causes physical injury to soft or hard tissues and this gives rise to an inflammatory response, resulting in pain, tenderness, swelling and reduced function. Loss of physical integrity at the sites of injury is also common: the skin may be abraded, lacerated or lost and bones and teeth may be stressed to the extent that they fracture or dislocate. Indirect soft-tissue injury is rare, but can occur through traction to the skin due to blunt trauma and tearing at distant sites. Indirect trauma is a more common cause of fracture: for example, a blow to the mandibular symphysis can cause a distant subcondylar fracture.
As well as the inflammatory response and local effects of trauma, systemic effects involving biological and psychological stress reactions occur. Biological stress reactions include release of endogenous catecholamines (the ‘fight, flight and fright reaction’) and associated psychological stress reactions often comprise feelings of shock, fear, an increased sense of vulnerability and sometimes denial (inability or failure to appreciate that the injury has actually occurred). Metabolic changes are similar to those which follow administration of high doses of steroids. Oxygen consumption, carbon dioxide production and protein breakdown increase.
An understanding of the cause of injury is important for several reasons. It helps to focus on the need for injury prevention; it may help identify typical patterns of injury (e.g. the blow to the symphysis associated with a condylar fracture or head injury), and it may raise awareness of the risk of future injuries (for example, in cases of domestic violence). There are many unique features of injuries of the face because it is responsible for the senses of sight, smell, taste and hearing. In addition, eating, drinking, speech and communication through facial expression depend on the integrity of maxillofacial structures. Disruption of the maxillofacial skeleton can hazard the airway.
In those with maxillofacial injuries it is also necessary to consider the possibility that there may be injury to the base of the skull, cranial vault and brain, the cervical spine and the upper aerodigestive tract. Indirect effects on the upper aerodigestive tract may include airway obstruction or partial obstruction because of blood, saliva and fragments of teeth or bones. Airbag injuries may affect the neck and face together. The presence and extent of brain injuries influences the risk of distant effects on the aerodigestive tract where, for example, coma may predispose to the inhalation of fragments of teeth and blood.
There is some evidence that the face acts as a ‘crumple zone’ (in the same way as the front of an automobile absorbs impact which might otherwise be transmitted to the passenger compartment) and therefore has a protective effect in terms of brain injury. Facial injuries and brain injuries are often seen together simply because they share the same anatomical region. Overall, the more serious the facial injury, the more likely is brain injury.
THE CAUSES AND PREVENTION OF MAXILLOFACIAL INJURY
The causes of maxillofacial injury reflect the culture in which it is sustained. The most frequent cause of serious maxillofacial injury in the developed world in the past century has been the motor vehicle, the only exception being epidemics of injury sustained in two world wars. Overall, incidence of maxillofacial injuries has reflected death rates on the roads such that, for example in the UK, incidence reached a peak in the 1960s and the 1970s and has been falling since. Violence has become a more common cause of maxillofacial fracture, on both sides of the Atlantic, since the late 1960s.
The causes of historical increase in road trauma include progressive industrialization and expansion of the motor industry leading to steadily increasing numbers of vehicles, lack of focus on safety during the first 60 years of automobile and motorcycle development and lack of investment in motorways until the 1970s. Determined efforts to reduce risks have led to drink-drive and seat-belt legislation, construction of safer roads and increased safety of the vehicles themselves. Increases in violence have been caused by numerous factors, including low levels of social control of young people in families and in the workplace, unemployment, the development of a drug culture, decline in real alcohol prices and more leisure time. Surveys of maxillofacial injuries in Middle-Eastern countries demonstrate much lower incidence of injury overall and a lower incidence of alcohol-related trauma.
The most effective approach to prevention of maxillofacial injury has been attention to the particular circumstances of injuries in particular environments (secondary prevention). Thus, wearing a cycle helmet has been shown to prevent upper facial injury, gum shields prevent many sports injuries and toughened or plastic glassware reduces the risk of facial injury in assault in licensed premises. Educational interventions, for example in schools, have had much less effect. Preschool education together with early family support (primary prevention) has been shown to reduce later assault as well as other forms of delinquency such as truanting, drug abuse and early pregnancy.
THE MANAGEMENT OF MAXILLOFACIAL TRAUMA
Management of the acutely injured patient
The management of the acutely injured patient in the accident and emergency department depends on organized, well-practised teamwork, under the direction of a team leader. However, whenever a seriously injured, perhaps unconscious patient is encountered, the presence of a cervical spine injury should be assumed until proved not to exist and neck movements should therefore be kept to a minimum. Obvious bleeding should be controlled using pressure, wire ligatures around teeth adjacent to fractures, ligature of vessels (such as the facial artery) and inserting ribbon gauze packs into, for example, intraoral lacerations of the sulci. The airway must be established and maintained by altering posture, by aspiration and, if necessary, by means of endotracheal intubation. Tongue control, by means of oropharyngeal or nasopharyngeal tube airways, may be useful. Where there is total upper airway obstruction, a laryngotomy through the cricothyroid membrane may be necessary. Chest radiography and analysis of blood loss are necessary early in the case of chest emergencies. Ventilation to keep the arterial pO2 above 10 kPa and pCO2 below 5.5 kPa can be achieved by a bag valve mask. To support the circulation, the insertion of the largest possible cannula into an antecubital vein is usually the best option for intravenous infusion.
This focus on Airway, Breathing, Circulation, in this order, together with the assessment of cervical spine integrity, disability and neurological state, comprise the primary survey and resuscitation phases, which are key to life support for trauma patients. This facilitates the logical progression to secondary injury surveys and the definitive care phase.
Practical skills in resuscitation are essential for all clinicians and these can be learnt and maintained only by attending recognized practical courses.
History of injury
Accurate verbatim accounts of injury are important because this medical evidence may be of great relevance to investigations by the police, insurance companies and researchers. Although it is not usually necessary to record the cause of injury in detail, a short summary is always helpful. In relation to assault, for example, this should include the type of weapon, how many assailants were reportedly involved and where precisely the assault took place. For car occupants, seat-belt wearing and position in the car should be recorded. An essential part of the history relates to tetanus prophylaxis: the year of the most recent ‘booster’ should be established and prophylaxis administered if necessary.
Dental surgeons are often asked to see the injured person after their general condition has been stabilized. Occasionally this is not the case, however, and a dental practitioner may be the first to the scene of a serious accident or assault. If injuries are life-threatening, the history should be dispensed with until airway, cervical spine, breathing and circulation have been stabilized.
It is often said that records about alcohol are important, but at the initial consultation it can be extremely difficult without objective measurement to assess its effects. It is a mistake to blame people for their injuries just because they have been drinking. Nevertheless, if alcohol abuse is to be investigated then breath analysis is appropriate for acute intoxication. Pure ethyl alcohol, reflecting its volatile nature, may be smelt on the breath, but almost all alcoholic drinks contain other volatile components (congeners), which make smell alone an unreliable measure of alcohol consumption.
The Glasgow Coma Scale
First described by two Glasgow neuroscientists, the Glasgow Coma Scale (GCS) is an internationally recognized method for measuring coma. It cannot discriminate between causes of coma, such as brain injury or alcohol intoxication, but it provides an excellent means of assessing the need for hospital admission and recovery (Table 13.1).
Table 13.1 The Glasgow Coma Scale
| Score | |
|---|---|
| Eyes open: | |
| Spontaneously | 4 |
| To speech | 3 |
| To pain | 2 |
| Never | 1 |
| Best motor response: | |
| Obeys commands | 6 |
| Localizes pain | 5 |
| Flexion withdrawal | 4 |
| Decerebrate flexion | 3 |
| Decerebrate extension | 2 |
| No response | 1 |
| Best verbal response: | |
| Orientated | 5 |
| Confused | 4 |
| Inappropriate words | 3 |
| Incomprehensible sounds | 2 |
| Silent | 1 |
Scores for the three components can be added together (< 8 is defined as coma; maximum score = 15) or listed separately.
Examination
Very often, by the time a dental practitioner is called to see an injured person, some radiographs have already been obtained. Looking at these before seeing the patient is a mistake. An enormous amount can be missed from focusing first on radiographs. For example, they do not show soft-tissue injuries and superimposition often makes primary diagnosis of mandibular, symphyseal and cranial base fractures difficult or impossible. Much information can be gained simply by observation of the patient. Although dental practitioners will usually not be responsible for managing injuries outside the maxillofacial region, examination should always start with an overall assessment of injuries.
Pay particular attention to signs of bleeding or other discharge from the ears, eyes, nose and mouth. In seriously injured patients there may be leakage of cerebrospinal fluid from the ears or nose. Look for signs of impact, including on the scalp. Abrasions (Fig. 13.1) or haematomas often signal the sites of underlying bone injury. There is often little swelling in the immediate aftermath of injury. However, within 6 hours mandibular angle fractures, for example, are often associated with swelling over the angle (Fig. 13.1) and subcondylar fractures with preauricular swelling.

Always take a systematic approach to the examination of the maxillofacial region. As with occipitomental radiographs, start superiorly and work down the face in a series of arcs to reduce the chances of an injury being missed.
An examination may follow this order:
Having carried out a thorough inspection of the mouth and face, the facial skeleton should be palpated in the same systematic manner, paying particular regard to:
Stand behind and above the patient when assessing facial asymmetry, particularly in relation to suspected zygomatic fractures. In this position place an index finger on the maximum convexity of the zygoma on both sides equidistant from the tip of the nose. Then compare the overlap of the index fingers with the supraorbital ridges.
Mobility of the middle third of the face, such as that brought about by Le Fort I, Le Fort II and Le Fort III pattern fractures (Fig. 13.2) is best assessed by placing the patient’s head securely against a head rest, grasping the upper teeth and alveolus and moving them gently, but purposefully, laterally, superiorly and anteriorly. Simultaneous palpation of the nasal bones has often been advocated but this can give rise to false-positive findings because of the mobility of the scalp and skin in this region. A ‘cracked cup’ sound when the upper teeth are percussed can be diagnostic of a Le Fort pattern fracture.
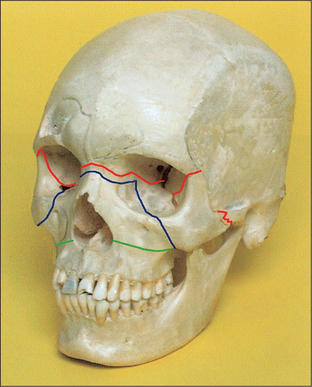
Fig. 13.2 Le Fort fracture lines illustrated on a skull. Green, Le Fort I; blue, Le Fort II; red, Le Fort III.
NB: These extensive mid-face fractures rarely present in classic form. Most involve comminution (fragmentation) and there is frequently a different combination of injuries on the two sides of the face.
A good test for a mandibular fracture is to exert gentle but purposeful backward pressure on the symphysis. The patient will indicate discomfort at the angles or condyles if there are fractures in these regions. If there is symphyseal injury or injury of the overlying skin, then gentle medial pressure on both mandibular angles simultaneously may provide evidence of mandibular fracture in or near the mandibular midline.
Although a comprehensive examination of cranial nerve function is not usually necessary, hearing loss may be investigated by rubbing the thumb and forefinger together 1–2 cm from the patient’s external auditory meatus. Hearing loss may be caused by blood in the external auditory meatus or, exceptionally, may be associated with a cranial base fracture or neurological dysfunction. Whatever the cause, hearing deficit should prompt referral to an otolaryngologist.
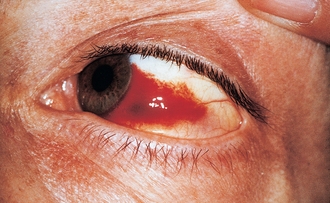
Examination of the orbits and eyes should focus first on visual acuity, diplopia in the various directions of gaze and evidence of bleeding into the surrounding skin, under the conjunctiva (Fig. 13.3), or into either chamber of the eye. Anterior or posterior displacement of the globe gives rise to exophthalmos and enophthalmos respectively and is most important in relation to the diagnosis of retrobulbar haemorrhage (because this condition can give rise to irreversible blindness if left untreated), or a ‘blow-out’ fracture of the orbital floor or medial wall. Examination of the canthi is important for eliminating the possibility of traumatic telecanthus (widening of the distance between the inner canthi due to detachment from sound bone). Corneal abrasions, conjunctival tears and eyelid laceration or loss need to be sought by careful examination of the eyes and charted thoroughly. Diplopia (double vision) is most often caused by haemorrhage or oedema in or adjacent to extraocular muscles, but can be caused by mechanical tethering of muscle attachments or by injuries to the third, fourth or sixth cranial nerves.
Thorough examination of the nose is an aspect of maxillofacial examination often neglected and includes attention to:
Examination of the mouth with a good light, paying attention to the junction of the hard and soft palate (Le Fort pattern fractures cause haematomas here), dental arches and the sulci, is important. The teeth should be charted, noting particularly broken teeth and retained roots, especially those that are very mobile and which may cause airway embarrassment. Gentle but purposeful pressure should be applied to all teeth to detect possible dentoalveolar fractures, a split palate and fractured teeth. Patients with fractures of the mandible between the mental foramen and the mandibular foramen often have reduced levels of sensation in the distribution of the inferior alveolar or lingual nerves and patients with zygomatic fractures often have areas of reduced sensation in the distribution of the infraorbital and anterior superior alveolar nerves. Any such areas of altered sensation should be recorded. Intraoral soft-tissue injuries are usually obvious and some extensive lacerations of the hard and soft palate may be present—for example, if a child has impacted a toy or other object into the mouth during a fall. Sublingual haematomas and tears at the gingival margin can be diagnostic of mandibular fractures (Fig. 13.4).

Examination of jaw function should include measurement in millimetres of maximal comfortable mouth opening from the tips of the central incisors on one side; this should be recorded clearly in the medical records. Abnormalities of jaw function should be sought and recorded: these include deviation on opening, abnormal joint sounds and disrupted occlusion (Fig. 13.5). Temporomandibular joint dislocation is rarely a result of injury but traumatic effusions can give rise to temporary mild posterior open bite. Crucially, anterior open bite can be a feature of Le Fort pattern fractures in which the middle third of the facial skeleton moves backwards and downwards on the cranial base or of bilateral fractures of the mandibular condyles in which the pterygomasseteric sling shortens the ascending rami.

It is important to carry out a thorough examination of the skin of the face, including the pinnae, the scalp and the neck. Areas of numbness or partial numbness should be assessed by means of touch testing, comparing sides and two-point discrimination and recorded. Careful attention needs to be paid to all facial orifices, in particular to discontinuity of eyelids, external nares, the external auditory meati and the vermilion border of the lips. High-quality soft-tissue reconstruction depends on accurate repositioning of the oral mucosa, musculature and skin in these areas.
SPECIAL INVESTIGATIONS
Special investigations should only follow thorough clinical examination: many fractures have been missed by ordering radiographs first. Radiographic examination forms the basis of special investigations of maxillofacial injury and should be specific to the areas of concern. Radiographs should be obtained according to the following categorization:
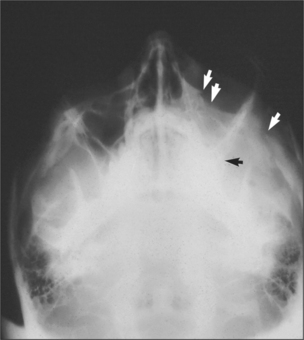
Fig. 13.6 Occipitomental view of fractured zygoma. Arrows indicate fractures at the infraorbital rim, zygomatic arch and zygomatic buttress areas.


Radiographs may be necessary not only to reach a diagnosis but also to inform treatment decisions, for example, about where bone plates should be applied. They also commonly reveal injuries which may not need treatment, for example, undisplaced or minimally displaced fractures, medial blow-out fractures of the orbit and comminution of the mid-face. Radiographs provide much more detailed information on hard-tissue injuries than the clinical examination so they may, for example, show fractures of the roots of teeth and signs of associated soft-tissue abnormality, such as herniation of orbital contents into the maxillary antrum (Figs 13.9, 13.10).
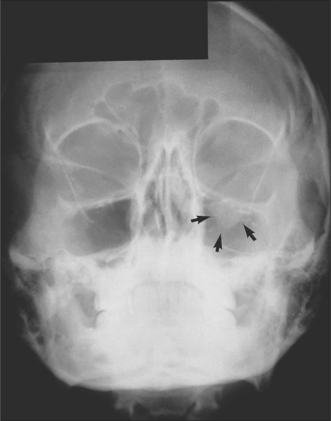
Fig. 13.9 Occipitomental view of a fracture of the left orbital floor. Note the herniated orbital contents, outlined by the arrows.
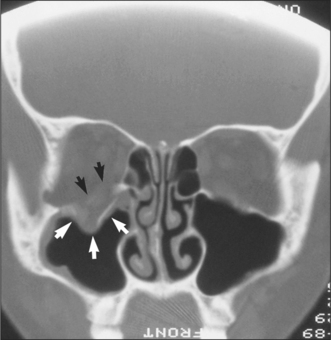
Fig. 13.10 CT scan showing herniation of orbital contents (white arrows) through an orbital floor fracture. The inferior rectus muscle is highlighted with black arrows.
Additional tests may include hearing tests (though these are almost always performed by audiologists or otologists), tests for monocular and binocular single vision such as Hess testing (by orthoptists) and various other ophthalmological tests. The management of patients with multiple maxillofacial injuries relies on teamwork, and it is preferable for specialist ear, eye and neurosurgical tests to be ordered by the relevant specialists so that treatment can be comprehensive and coordinated.
SURGICAL INTERVENTION IN THE MANAGEMENT OF MAXILLOFACIAL INJURY
Many facial injuries require no active treatment and heal spontaneously. Examples include small haematomas, clean abrasions, small lacerations, undisplaced stable fractures and some displaced fractures, such as those of the mandibular condyle where the occlusion is not deranged or where the occlusion settles spontaneously. As with any surgical intervention, a crucial decision is whether operative treatment will benefit the patient. Given there are few randomized controlled trials, and given the recorded clinical experience of generations of oral and maxillofacial surgeons, the management of maxillofacial trauma is more of an art than a science. It is possible to overtreat or undertreat. For example, one may overtreat mandibular condyle fractures if it is not appreciated that many displaced fractures of the neck of the condyle heal spontaneously without complications. Similarly, neglect of grossly displaced condylar fractures can give rise to long-term occlusal derangement.
Indications for surgery and brief descriptions of appropriate operative procedures are set out below.
As in orthopaedics, the principles of treatment are:
Although these principles remain the cornerstone of management of fractures, immobilization is now much less important than it has been historically. This is because research has demonstrated that complications such as long-term jaw stiffness, airway restrictions and psychological problems are greater if the jaws are immobilized (traditionally by wiring them together). Furthermore, the advent of small bone plates provides a method of fixing many fractures precisely and with a degree of stability which makes immobilization unnecessary.
Surgery for fractures of the zygomatic complex
Indications for surgical intervention include:
Trismus often resolves spontaneously because it is often not caused by mechanical interference but by haemorrhage into the masseter or temporalis muscles.
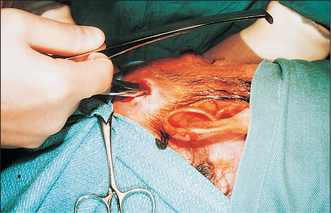
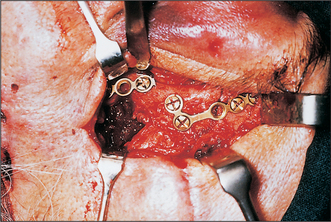
The basis of treatment for zygomatic fractures remains the Gillies’ procedure. This depends upon the anatomical relationship of the temporalis fascia, which is attached to the superior aspect of the zygomatic arch, and the temporalis muscle, which passes beneath the zygomatic arch and body and is attached to the coronoid process and anterior aspect of the ascending ramus. Thus, if an elevator is passed between temporalis fascia and muscle, it can be used to elevate the displaced bone from underneath (Fig. 13.11). Access is achieved by making a 2-cm incision in the temporal scalp, above and in front of the ear and incising through temporalis fascia. If the elevated bone is unstable then it is necessary to stabilize the zygoma with miniplates across the fracture lines in the zygomatic buttress region, the zygomaticofrontal suture (Fig. 13.12) (particularly if the frontal process of the zygoma is displaced medial to the zygomatic process of the frontal bone) and the zygomaticomaxillary region. Surgical approaches to the orbital floor are necessary to retrieve orbital contents from the maxillary antrum and prevent recurrence by the insertion of a graft of either bone or synthetic material. Transconjunctival (with or without lateral canthotomy) and transcutaneous (lower lid or infraorbital) approaches to the orbital floor are in use. The principal objective is limitation of scarring in this most visible and socially important area of the face while gaining sufficient access to the fracture site. Minimizing skin scarring has to be balanced against risks of corneal and subconjunctival injury.
Isolated fractures of the zygomatic arch are much less common than fractures of the zygomatic complex (separation of the entire zygoma) but operative intervention is sometimes necessary because untreated fractures give rise to cosmetic problems or arch/coronoid interference, resulting in restriction of mandibular movement. Again the Gillies’ approach is the basis of treatment. As the zygomatic arch is not a substantial bone, reductions are sometimes unstable and splinting is occasionally necessary. There are a number of ways of doing this—for example, using a Foley catheter inflated under the arch for 48 hours, or using external splinting by means of transcutaneous circumzygomatic sutures.
In extensive or panfacial (multiple fractures of all or most regions of the facial skeleton) trauma, it may be necessary to gain access to craniofacial sutures at a number of sites; in these cases, the coronal scalp flap can be invaluable. In this approach, a coronal scalp incision is made above the hairline, allowing the scalp to be turned down over the face to expose the nasoethmoidal and zygomatic regions. Thus, for example, by such an approach it is possible to reduce a complex nasoethmoidal fracture, repair a cerebrospinal fluid leak and reduce and fix bilateral zygomatic or Le Fort pattern fractures. The basis of the surgical treatment of nasoethmoidal fractures is reduction of the canthal attachment and reduction of the nasal bones. Very often, the medial canthal ligaments are not simply detached from the bone, but rather the ethmoid bone to which they are attached fractures from the rest of the nasoethmoidal skeleton. The basis of treatment is usually the reduction of intercanthal distance to normal by approximating the medial canthal ligaments using a wire suture.
The basis of treatment of fractures of the nasal bones is reduction of each nasal bone and the nasal septum using instruments inserted into the anterior nares. Nasal splinting is often inadequate, particularly with T-plasters, which simply compress haematoma and oedema rather than stabilize the reduced nasal fracture. It is therefore often necessary to provide intranasal splinting using, for example, expansive flexible splints or tulle gras (paraffin wax impreg-nated gauze) to prevent the nasal bones from falling medially. Occasionally, nasal trauma gives rise to bilateral septal haematoma, which should be drained early to avoid necrosis of the cartilaginous septum.
Operative procedures for Le Fort pattern fractures
These fractures are sometimes undisplaced or minimally displaced, resulting in minimal occlusal derangement, which corrects itself with masticatory function during the first week. Indications for operative intervention are asymmetry, displacement, comminution and sustained occlusal derangement. As with almost all fractures of the mid-face, immediate surgical intervention is rarely necessary. Exceptions include haemorrhage and the need to take the patient to the operating theatre for surgery for other injuries. There are many advantages in leaving definitive treatment until 5–7 days have elapsed. These include resolution of soft-tissue swelling that makes operative assessment and access difficult, resolution of any brain injury or other systemic trauma and resolution of any acute intoxication with alcohol or other drugs.
The basis of treatment for these fractures is direct visualization of the fracture sites and fixation with miniplates, paying particular attention to achieving the correct occlusion. Postoperative intermaxillary fixation (IMF) is rarely necessary, although retention of arch bars (metal bars wired to the teeth facilitating wiring the jaws together) (Fig. 13.13) may assist if there are mandibular fractures that have not been fixed directly and for which elastic traction (pulling the teeth into the correct position using elastic bands) may be necessary to settle the occlusion.

Operative procedures in the treatment of fractures of the mandible
Most fractures of the teeth-bearing part of the mandible require operative intervention to restore occlusion and minimize pain due to mobility. Undisplaced fractures, especially in children, may, however, not require operative intervention. Open reduction and fixation with miniplates is the treatment of choice for displaced fractures of the teeth-bearing aspect of the mandible. Miniplates are usually applied intraorally to the external oblique ridge in the case of angle fractures or to the midline in the case of symphyseal fractures. The placement of plates is critical in relation to:
As with the use of implants at other sites, for example in hip replacement, biocompatibility is not as important as it is in dental implantology. Thus, success has been achieved in terms of biointegration with stainless steel, cobalt-chrome alloy and titanium miniplates and screws, the costs of which are generally great. There are numerous types of miniplates currently on the world market and there are clear opportunities for cost savings if a generic rather than a proprietary approach is adopted, as with drugs. Disadvantages of the use of plates include the need for access to the fracture sites and potential for infection and plate mobility leading to plate loss.
Teeth in fracture lines should normally be retained to assist in the accurate reduction of both fractures and the occlusion. They act as spacers and their loss can lead to poor reduction. However, if teeth are fractured, displaced from the socket or terminally diseased in relation to periodontal disease or caries they should be removed.
Fractures of the ascending ramus and condyle of the mandible are almost always of the condylar neck. The most important distinction to be made is between condylar fractures that involve the articular surface and those which do not. Because the occlusion and masticatory function tend to maintain the dimensions of the ascending ramus, operative intervention is normally necessary only when the occlusion does not return to normal within the first 10 days after trauma. All intracapsular fractures should be mobilized immediately and solitary intracapsular fractures are unlikely to affect the occlusion unless there is a traumatic effusion. The majority of subcondylar fractures heal with no long-term occlusal disturbance: the support provided by the occlusion is akin to the weight of the arm, which is normally sufficient to maintain a fractured humerus in a satisfactory position without recourse to surgical intervention. Condylar fractures that may benefit from open reduction and internal fixation are those where:
Fractures of the condyle may be reduced and fixed using miniplates or transfixion screws and the approach may be intraoral or extraoral. Precision at operation is critical because errors may be magnified in the tooth-bearing part of the mandible.
The nature of fixation
Most miniplates provide slight flexibility and are therefore forgiving of minor errors in fixation. Slight movement at the fracture area during the healing period is an advantage because it promotes osteogenesis through the ‘fixator’ effect, first described in orthopaedics, which accelerates healing through periods of slight, controlled, movement of a fracture. Rigid fixation with substantial ‘reconstruction’ plates requires very precise surgical techniques but is more often successful in the presence of infection.
Wire fixation has too much in-built flexibility, leading to deformation in function. Traditional means of immobilizing the jaw with intermaxillary fixation are eyelet wires and arch bars. Both provide wire loops, through or around which tiewires are passed. Arch bars, intraosseous screws or orthodontic brackets may be used if elastic traction is necessary, for example, to maintain the occlusion after bilateral subcondylar fractures. With miniplates, intermaxillary fixation is usually not required, apart from intra-operatively to maintain occlusion while miniplates are applied.
Infection and maxillofacial fractures
Although most maxillofacial fractures are compound into (communicate with) the mouth or paranasal sinuses, the incidence of infection is low in otherwise healthy patients. Bone surgery and grafting increase the chances of infection but this risk can be reduced by giving broad-spectrum antibiotics during the operation, using the intramuscular or intravenous routes and postoperatively using the oral route.
Stabilization of middle-third fractures with antral packs is associated with more infection than other means of stabilization. Small fragments of bone, particularly in the mid-face, rarely become infected.
Gross infections of non-united mandibular fractures usually require sequestrectomy and rigid fixation with reconstruction plates.
Repair of facial lacerations
It is important not to neglect soft-tissue injuries because of too sharp a focus on underlying fractures. These injuries usually comprise abrasions, contusions and lacerations but deep, penetrating injuries and loss of soft tissue may also occur, particularly in firearm wounds. Many of the principles of management have been set out above but, in summary, skin, oral mucosa and intervening musculature should be repaired accurately in layers, especially at the margins of the eyes, nose and lips. Account should be taken of the orientation of the muscles of facial expression. Inaccurate repair of a laceration of the vermilion border can lead to an ugly step defect and the need for scar revision.
Even minor scars can be constant reminders of the original trauma as well as socially embarrassing. Resorbable suture material should be used for the oral mucosa and musculature and it is important that the oral mucosa is allowed to heal before muscle sutures resorb. Continuous sutures are often useful for linear mucosal lacerations and can be useful externally. Accurate repositioning of irregular wounds nearly always necessitates the use of interrupted sutures. Infection rates are lower with mono-filament suture material (like nylon) than with multifilament or braided suture material (like silk).
Tips for soft-tissue repair
Psychological injury
About one-third of adults with maxillofacial skeletal injury and lacerations more than 3 cm long develop post-traumatic stress disorder (PTSD). This may be defined as acute or chronic, depending on the basis of persistence after 6 months. A diagnosis of PTSD requires the presence of flashbacks to the trauma that produced injury, depression, sleep disruption and irritability/hyperarousal (‘jumpiness’). The risk of developing PTSD is increased for patients with a previous history of psychiatric illness, patients who are upset immediately after their injury and people who have been injured in assaults. It has been shown that house surgeons/residents can predict accurately, on the basis of how shocked the patient appears to be initially, who will go on to develop PTSD. The symptoms of PTSD can be reduced by early intervention, for example cognitive-behavioural therapy, for those at risk, who should be referred early to relevant mental health professionals. Liaison psychiatrists are becoming important members of trauma teams. However, non-targeted, blanket mental health interventions, such as ‘critical incident debriefing’, are now known to do more harm than good.
Psychological problems are not limited to PTSD and may include anxiety, fear of further injury or depression. The prevalence of these conditions is very high in people with facial injuries, and dental practitioners need to be alert to them and have routes of referral to appropriate mental health professionals and voluntary agencies such as Victim Support. It is important not to separate the physical effects of trauma from the psychological effects: the two are often interlinked and minor physical symptoms such as lack of ordinary sensation in the lip can trigger the flashbacks of PTSD.
Dental injuries
Thoroughly chart all dental injuries, including those of the enamel/dentine, root fractures and displaced or avulsed teeth. Account for all the major fragments. Minor damage to the enamel usually requires no immediate intervention. Exposed dentine should be dressed to control sensitivity and prevent loss of vitality. Use thermal rather than electrical pulp testers: pulp reactions can be misleading in the acute phase. Monitor pulp vitality closely but remember that non-responding teeth may reflect neurological rather than pulpal injury.
Fractures of the coronal third of the root of a single-rooted tooth usually necessitate extraction. Undisplaced fractures of the middle and apical third of the root may repair without recourse to treatment. Wire loops can be used to temporarily stabilize mobile teeth or a fracture between two teeth. Reimplanted teeth require calcium hydroxide root-filling at 1–2 weeks to prevent later resorption. Avoid splints that involve the gingival margins.
REHABILITATION
Return to normal function and appearance is the goal of all clinical management. In many cases, particularly of panfacial trauma, definitive repair of soft-tissue injuries and fractures is only the first step in rehabilitation. Since miniplates and direct fixation have largely replaced intermaxillary and internal wire fixation, there is great opportunity for early mobilization of the mandible. This reduces the risk of permanent limitation of jaw movement. Many patients with jaw fractures require restorative dentistry as part of their rehabilitation from either family dentists or specialists in restorative dentistry. Lacerations should be reviewed for at least 12 months to assess the need for scar revision, which should not normally be done earlier because scars change in shape, bulk and colour over that time.
Rehabilitation may include the need for the services of an ophthalmic optician to replace spectacles or contact lenses or provide them for the first time if there are permanent effects on vision. Advice from a dietitian may help patients whose nutrition has been compromised through associated injuries of the digestive tract and for those who have postoperative intermaxillary fixation.
In relation to psychosocial rehabilitation it is important to be aware of the level and quality of support at home and to involve the voluntary sector if support is lacking. In many parts of the developed world victim support organizations exist to provide social support, help with practical difficulties (such as those that may follow a robbery), support with police investigations, appearances in court as prose-cution witnesses and help with completing applications for criminal injuries compensation.
Family dental practitioners are responsible for ongoing restorative care, and therefore have opportunities to monitor a patient’s psychological state and refer if there is evidence of depression or more serious psychiatric problems such as PTSD.
Alcohol misuse predisposes to maxillofacial trauma. In both hospital and primary care settings, effective treatments are available. Patients with maxillofacial trauma should be screened for alcohol problems with a standard test, such as AUDIT (Alcohol Use Disorders Identification Test) and appropriate treatment instituted.
MEDICOLEGAL MANAGEMENT
Practitioners who treat patients with facial injury are often asked to provide factual statements about the injuries and treatment and may be called upon as expert or professional witnesses to interpret the causes and effects of such injuries. A medical report should be completed promptly according to soli-citors’ instructions but practitioners should ensure that confidential information about a patient is disclosed only with their written consent. All practitioners who treat patients with maxillofacial injuries should be prepared to give written reports and oral evidence in court. Remember that it is not usually the standard of treatment or the possibility of negligence which is important to the courts, but the causes, nature and effects of injury.
Ali T., Shepherd J.P. The measurement of injury severity. British Journal of Oral and Maxillofacial Surgery. 1994;32:13-18.
American College of Surgeons. Advanced trauma life support (ATLS) course. Chicago, IL: American College of Surgeons, 1998.
Andreason J.O., Andreason F.M., Bakland L.K., Flores M.T. Traumatic dental injuries: a manual. Copenhagen, Denmark: Munksgaard, 1999.
Bisson J.I., Shepherd J.P., Dhutia M. Psychological sequelae of facial trauma. Journal of Trauma. 1997;43:496-500.
Bisson J.I., Shepherd J.P., Joy D., Probert R., Newcombe R.G. Early cognitive-behavioural therapy for post-traumatic stress symptoms after physical injury. British Journal of Psychiatry. 2004;184:63-69.
Brickley M.R., Shepherd J.P. The relationship between alcohol intoxication, injury severity and Glasgow Coma Score. Injury. 1995;26:311-314.
Evans T. R. (ed) (1989) ABC of resuscitation. British Medical Journal, London.
Harrison M.G., Shepherd J.P. The circumstances and scope for prevention of maxillofacial injuries in cyclists. Journal of the Royal College of Surgeons of Edinburgh. 1999;44:82-86.
Omovie E.E., Shepherd J.P. Assessment of repair of facial lacerations. British Journal of Oral and Maxillofacial Surgery. 1997;35:237-240.
Shepherd J.P. Victim services in the NHS: combining treatment with violence prevention. Criminal Behaviour and Mental Health. 2005;15:75-81.
Shepherd J.P., Farrington D.P. Preventing crime and violence. British Medical Journal. 1995;310:271-272.
Shepherd J.P., Qureshi R., Preston M.S., Levers B.G.H. Psychological distress after assaults and accidents. British Medical Journal. 1990;301:849-850.
Ward L., Shepherd J.P., Emond A.M. Relationship between adult victims of assault and children at risk of abuse. British Medical Journal. 1993;306:1101-1102.
Williams J.L., editor. Rowe and Williams’. Maxillofacial injuries, 2nd edn., Edinburgh: Churchill Livingstone, 1994.
SELF-ASSESSMENT
Answers on page 268.