chapter 18 Dysphagia and Other Eating and Nutritional Concerns with Elders
1. Discuss the increased incidence of swallowing, eating, and nutritional problems occurring with elders.
2. Identify the basic anatomical structures related to swallowing and the swallow sequence.
3. Relate the physiological changes and the onset of increased age-related medical conditions with the increased incidence of swallowing problems.
4. Identify intervention strategies and precautions for improving oral intake and nutrition.
5. Discuss the roles of the team members and the importance of teamwork in addressing swallowing and nutritional concerns.
6. Relate ideas for managing different types of feeding problems.
7. Discuss the psychological and ethical concerns that are present when swallowing problems develop.
oral intake, undernourishment, malnutrition, dehydration, institutionalized, nutrition, hydration, bolus, velum, compensations, dysphagia, aspiration pneumonia, positioning, alternative means, contraindicated
Eating is essential for survival, is a basic activity of daily living (ADL), and often a very meaningful area of occupation.1 As the elder population continues to increase, the incidence of swallowing, eating, and nutritional problems is increasing. Death and illness resulting from impaired oral intake are now considered major health problems of elders.2
Most elders have at least one chronic medical condition, and many have multiple conditions. These conditions include arthritis, hypertension, heart disease, hearing impairments, orthopedic impairments, sinusitis, diabetes, and vision impairments. These chronic conditions can influence elders’ abilities to effectively and independently perform ADL, such as eating, self-care, transfers, going outside, and instrumental activities of daily living (IADL), such as meal preparation, shopping, money management, and housework. The need for individuals to receive help increases with age.3 When such help is unavailable, this lack of assistance can lead elders to social isolation and depression, which may lead to decreased oral intake. In addition, many elders often take multiple medications, which may affect oral intake.4 This decrease in oral intake can result in undernourishment, malnutrition, and dehydration.
Among institutionalized elders, the prevalence of undernourishment and malnutrition may be as high as 80%. This high prevalence may be explained by the increased numbers of elders who need assistance with feeding and the lack of sufficient staff to assist them. In nursing homes, government statistics show that 23% of residents are reported to need total feeding assistance and 45% require some feeding assistance. In these settings, it has been reported that a nursing assistant may feed from 5 to 20 individuals an hour, with research showing that it may take up to 40 minutes for a nursing home resident to complete a meal.5
These statistics clearly reflect the growing need for occupational therapy (OT) involvement with elders to help them maintain optimal independence in a home, hospital, or nursing home setting. OT assistance may include training in self-feeding, safe swallowing, positioning, mobility, meal preparation and cleanup, shopping, money management, provision of assistive equipment, and caregiver and nursing instruction. All of these activities are essential for elders to adequately maintain nutrition and hydration.
The Role of the Certified Occupational Therapy Assistant
The certified occupational therapy assistant (COTA) works in partnership with a registered occupational therapist (OTR) to collect data to identify the strengths and weaknesses of elders and establish and implement intervention plans to attain their goals. Ongoing assessment and communication between the COTA and the OTR are necessary for program and goal changes. The COTA is involved in individual and group intervention and in staff and caregiver instruction. Providing quality care is the function of the entire health care team. The amount of involvement of the COTA with elders with swallowing problems depends on the COTA’s level of experience. An entry-level COTA may work on activities that reinforce good nutrition and hydration such as meal preparation, money management, shopping, oral-facial exercises, instruction in assistive devices, and energy conservation during activities. An experienced COTA who has demonstrated competence in this area may participate in videofluoroscopic swallow studies and assist tracheostomized and ventilator-dependent elders with self-feeding and swallowing. It is recommended that the COTA review the article “Specialized Knowledge and Skills in Feeding, Eating, and Swallowing for Occupational Therapy Practice,” developed by the American Occupational Therapy Association.6
Normal Swallow
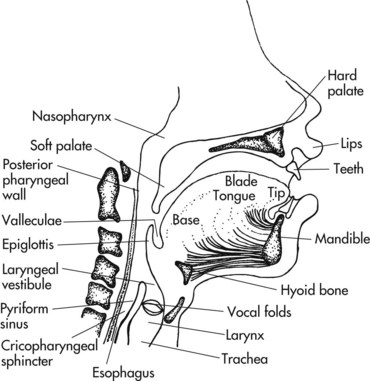
The swallow response requires a rapid interplay between the brain, 6 cranial nerves, 48 pairs of muscles, the salivary glands, and cartilaginous structures (Figure 18-1). The COTA working with elders who have dysphagia must clearly understand the anatomy and physiology of swallowing.7
Four phases of swallowing have been defined: oral preparatory, oral, pharyngeal, and esophageal (Figure 18-2, A to E).8
1. Oral preparatory phase: The oral preparatory phase includes seeing, smelling, reaching for the item, bringing it to the mouth, and putting it in the mouth. Once the item is placed in the mouth, the lips close to maintain a seal, and the tongue and cheek muscles move the bolus (that is, the food or liquid) around the mouth in preparation for swallowing. The base of the tongue and the velum (soft palate) also make a seal to prevent the bolus from entering the pharynx prematurely. Saliva mixes with the bolus to aid in swallowing. Taste, temperature, and texture receptors of the tongue also play a part in preparing for the action of swallowing.
2. Oral phase: The oral phase occurs once the bolus is prepared and formed by the tongue. The bolus is then propelled by the tongue to the back of the mouth and over the base of the tongue.
3. Pharyngeal phase: The pharyngeal phase occurs when the bolus passes over the base of the tongue and enters the pharynx. At this time, the soft palate elevates to seal the entrance to the nose, the hyoid bone and larynx elevate upward and anteriorly, the vocal folds close, the epiglottis tilts downward, and the cricopharyngeal sphincter opens to allow the bolus to enter the esophagus.
4. Esophageal phase: The esophageal phase occurs when the bolus passes into the esophagus and is propelled to the stomach.
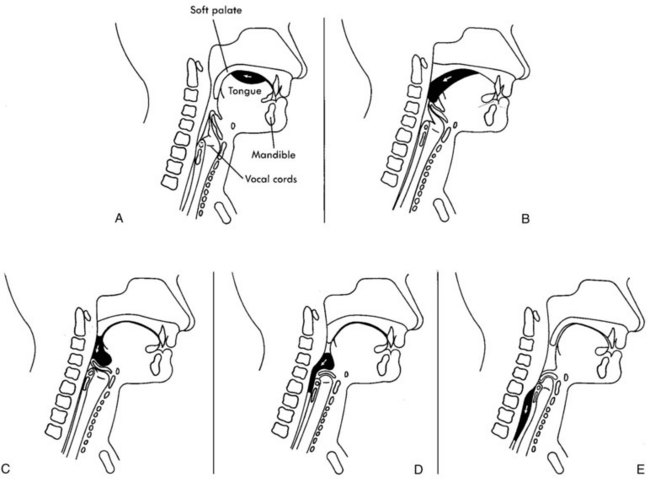
FIGURE 18-2 Lateral view of bolus propulsion during the swallow. A, Oral preparation of the bolus and voluntary initiation of the swallow by the oral tongue. B, Bolus moves from oral cavity to pharynx, pharyngeal swallow is triggered. C, Bolus enters the valleculae and the airway is protected. D, The tongue base retracts to the anteriorly moving pharyngeal wall. E, Bolus enters the cervical esophagus and cricopharyngeal area.
(From Logeman, G. [1998]. Evaluation and Treatment of Swallowing Disorders, 2nd ed. Austin, TX: Pro-Ed.)
Changes of Swallowing Structures
When individuals eat and swallow, the oral and pharyngeal structures adapt easily to different liquid and food consistencies and to the texture, temperature, and volume of the bolus. These structures also adapt to the different positions that the head and body may assume while swallowing. As individuals age, changes in these swallowing structures occur naturally.2 Individuals develop compensations to these changes spontaneously and often unknowingly. These compensations allow them to eat safely and efficiently, such as with smaller bites, longer chewing time, and softer food.8 However, if individuals also develop a medical or neurological disorder, these compensations may no longer be effective and may result in increased swallowing problems (Table 18-1).9,10 In addition to understanding the physical changes that occur, COTAs must be aware of the psychological effect of swallowing problems on individuals who can no longer eat as they once did. COTAs should acknowledge elders’ and caregivers’ feelings about certain types of liquids or favorite foods being eliminated from their daily diet.
Table 18-1 Age-Related Swallowing Changes
| Swallowing phase | Healthy elder | Frail elder |
|---|---|---|
| Oral preparatory | Vision may be declining. Sense of smell and taste decrease and may result in decreased intake. Elder may be missing teeth and need to wear full or partial dentures and require more time to chew food. |
Cognitive impairment (poor memory and decreased attention may exaggerate the influence of normal aging changes). Isolation and depression result in decreased food intake and weight loss. Decreased endurance may interfere with chewing and result in slow eating and low intake. Missing teeth and poor-fitting dentures may result in slow eating and poor intake. |
| Oral | Tongue and lip muscles atrophy, and elder may take smaller bites and require softer food. Elder may require longer time to form bolus in mouth. |
Decreased strength in lips and tongue and jaw muscles may result in drooling, decreased chewing, and problems moving the bolus in the mouth. |
| Pharyngeal | Phase becomes mildly prolonged. Muscle tone decreases and may delay clearing of food residuals. Bolus moves more slowly through the pharynx. Upward movement of hyoid and larynx becomes delayed. Epiglottis may become smaller and move more slowly. Cricopharyngeal sphincter remains open for shorter time. |
Time of passage of bolus increases. Structures move more slowly and may put elder at greater risk for aspiration. |
| Esophageal | Decreased strength of muscles results in increased time for passage of bolus to stomach. | Increased time needed for bolus to reach stomach. Food contents may reflux from stomach and reenter esophagus and pharynx. |
Adapted from Cherney, L. (2004). Clinical Management of Dysphagia for Adults and Children, 2nd ed. Rockville, MD: Aspen.
Etiology of Dysphagia
Dysphagia is the inability to swallow. This condition is often seen in elders and may have a variety of causes. These causes may be neurological (for example, from a cerebrovascular accident, brain tumor, or head injury), neuromuscular (for example, from Parkinson’s disease, multiple sclerosis, or amyotrophic lateral sclerosis), dementia (such as with Alzheimer’s disease), multi-infarct structural (for example, from cancer), and systemic (for example, from diabetes, rheumatoid arthritis, and scleroderma). Dysphagia may also result from prolonged illnesses or from the side effects of medications. If swallowing problems are not identified, they can result in aspiration pneumonia, malnutrition, dehydration, and death.8,11
Intervention Strategies
Elders achieve a sense of empowerment, control, and motivation when they are successful at self-feeding and swallowing. To achieve this success, COTAs should implement individually planned interventions to resolve swallowing problems and promote functional self-feeding. The COTA must first establish a therapeutic relationship with the elder. This will enhance the interventions affecting empowerment and quality of life during mealtime. Intervention of swallowing disorders entails focusing attention on every aspect of the mealtime experience, including preparation, the dining environment, positioning of the elder, assistive devices, direct intervention, dietary concerns, precautions, and caregiver training (Box 18-1).
BOX 18-1 Preparation Checklist for Dysphagia and Self-Feeding Interventions

Environmental Concerns
In American society, people usually eat three meals each day, or about 1,092 meals each year, excluding snacks. Eating is a vital part of social participation1 and greatly adds to the quality of an individual’s life. To promote an enjoyable dining experience, pleasant surroundings and personal comfort should be provided to elders during meals. Aesthetics of the dining area should include tablecloths, centerpieces, flowers, and cleanliness. If elders are institutionalized, food items should be taken off serving trays and put directly on the table to help establish a homelike atmosphere. Deficits in visual acuity, light sensitivity, and color perception are common in elders. Poor lighting can greatly exaggerate these problems; therefore, insufficient light and glare should be avoided. Natural light without glare or soft, diffused overhead lighting is best. A quiet, calm environment excludes television but may allow for age-appropriate dining music. Television may be distracting and detract from social interaction. Compatible table mates in small groups around a table can add to a positive dining experience (Figure 18-3). COTAs and other service providers should maintain a therapeutic attitude by allowing elders plenty of time to eat a meal. Lengthy waiting periods before being served may decrease the elder’s interest in food and may increase fatigue. The table height should be between 28 and 30 inches to accommodate both regular chairs and wheelchairs. The distance between the table surface and an elder’s mouth should be between 10 and 15 inches.12 Adopting these suggested environmental factors can help provide a pleasurable experience during mealtime and possibly assist elders to increase their food and fluid intake.

Positioning Techniques
COTAs must have knowledge of proper positioning techniques with elders who have dysphagia. Proper positioning is important for effective and safe swallowing, correcting mechanical problems with swallowing, and increasing dining pleasure. The trachea, or airway, is next to the esophagus, which is the food pipe. Safe positioning can prevent food from entering the trachea, avoiding aspiration. Proper positioning of elders also increases alertness, normalizes muscle tone, provides comfort, and helps with digestion, while allowing dynamic movement for self-feeding.
The preferred seating position for mealtime is sitting in a dining room chair with armrests rather than sitting in a wheelchair. A wheelchair, however, is preferable to a geriatric chair, which is preferable to sitting up in bed. COTAs should transfer an elder to a regular chair if the elder can possibly sit in one. If optimal posture cannot be obtained in a regular chair, use of a wheelchair may be necessary (Figure 18-4). The elder’s head, neck, trunk, and hips should be aligned. First, the pelvis should be positioned in neutral with a slight anterior tilt. The elder should have an erect posture and sit symmetrically with weight distributed equally on each hip. Second, the elder’s head should be positioned in midline with the chin slightly tucked. Both upper extremities should be fully supported on a table or lap tray of appropriate height. Finally, the lower extremities should be in a weight-bearing position. Hips and knees should be flexed 80 to 90 degrees, with ankles in neutral position under the knees and the feet flat on the floor. If the feet do not reach the floor, a stool or wheelchair footrest should be used to provide a secure base of support.

FIGURE 18-4 This gentleman is correctly positioned in his wheelchair for self-feeding. This position promotes dynamic trunk movement.
(From Community Hospital of Los Gatos, CA, 1996.)
If feeding in bed is essential, elders should be as close to the headboard as possible before the head of the bed is elevated to 45 degrees or more (Figure 18-5). A pillow may be placed behind the elder’s back to increase upright trunk posture and hip flexion. To prevent elders from sliding down in the bed, the knees should be flexed and supported from underneath with pillows if necessary.12 As with sitting in a chair, elders should be upright and aligned symmetrically for optimal safety while eating and drinking.

FIGURE 18-5 This gentleman is correctly positioned in bed for self-feeding.
(From Community Hospital of Los Gatos, CA, 1996.)
Positioning devices are often required to aid elders in maintaining a straight midline for a dynamic, upright posture. Padded solid back and solid seat inserts provide better postural support that offsets the slinging seats and backs of wheelchairs. Lumbar and thoracic support can facilitate increased scapulohumeral control for self-feeding. Elders with low muscular tone may benefit from high-back wheelchairs. Wedges, lateral and forward trunk supports, headrests, pelvic belts, pillows, and towel rolls are often used to obtain proper positioning. Seating systems must be designed to correct or to accommodate postural problems while preventing skin erosion, maintaining comfort, promoting self-feeding, and providing the right position for safe swallowing.
Many variables affect elders’ positioning. If an elder is sitting in a kyphotic posture, the COTA should have the elder lean back slightly so the chin is parallel to the floor. Special considerations are also needed for elders with scoliosis, depending on the curvature of the spine. Elders with a hemiplegic arm should have the arm placed on the table. The arm/hand should be incorporated as a gross stabilizer during meals. Those elders who have recently had a lower extremity amputation may also have special positioning needs. COTAs also must consider poor sitting tolerance. Elders with back pain or low endurance need to complete their meal within the time limitations of their upright tolerance. The lower extremities may need to be elevated when sitting up in a chair if edema is present, which often occurs as a result of congestive heart failure. Hearing and visual deficits should also be considered when positioning elders to increase their awareness of their surroundings and to maximize social interaction. The COTA is responsible for following through with the OTR’s instructions for positioning while considering the elder’s individual needs.
Assistive Devices
An abundance of options for assistive devices is available to assist elders in maintaining independence in self-feeding and safe swallowing. Some devices are prefabricated, whereas others are designed by the creative minds of the COTAs. A hole punched in the plastic lid of a cup can hold a straw and will prevent spilling for elders who have tremors or ataxia. Built-up handles can be used for joint protection or a weak grasp. A universal cuff is available for elders who have no grasp. A swivel spoon or a long-handled spoon is available to assist elders with limited range of motion. Nonslip mats or plates with suction cups can keep items from sliding on the table. Plate guards and plates with lips prevent food from spilling off of the plate. Cutout cups and straws can reduce the need for the elder to tilt the head back while drinking, thus protecting against aspiration while swallowing. Straws and cups with spouted lids can also limit the amount of each sip and are helpful for elders with severe dementia who have a sucking reflex only. Small rubber-coated spoons can help control bite size and prevent elders from hurting themselves when biting down on utensils. Rocker knives can be used for one-handed cutting. Mobile arm supports can provide stabilization and assist in hand-to-mouth movement.
Assistive devices should be issued if elders experience a decrease in function. However, elders should be encouraged toward further independence rather than to continue using assistive devices. Before assistive equipment is issued, the COTA should consult with the OTR regarding his or her recommendations.
Direct Intervention
Various feeding strategies may be used to help elders with dysphagia to feed themselves and to swallow safely. To ensure that mealtime is a pleasurable experience, the COTA should avoid making parental comments or giving parental cues (for example, use the word napkin rather than bib). A method of communication must be established with nonverbal elders so they can indicate when they are ready for another bite or drink. All team members, including family and other caregivers, should use this method consistently. Examples may be a nodding of the head or raising a finger. In addition, the COTA should sit next to the elders rather than standing over them during meals.
As noted in the preparation checklist in Box 18-1, oral exercises, sensory stimulation, and tone facilitation or reduction techniques are often needed before eating. Slow, deep pressure on facial and jaw muscles in the opposite direction to the pull of increased muscle tone may help reduce it.13 Tongue and facial exercises can increase strength and tone for bolus manipulation. Sensory stimulation may include brushing teeth and icing the cheeks and tongue to increase oral tone and sensation. Brushing teeth also stimulates the salivary glands and helps elders with dry mouths manipulate the bolus easier. After using these necessary strategies, elders are ready to begin eating.
These and many other general strategies help elders with eating and should be enacted before food enters the mouth. Hand-over-hand guiding can provide tactile cueing while bringing food to the mouth and is especially helpful for elders with perceptual difficulties. Proximal upper extremity stabilization techniques can compensate for tremors, ataxia, and weakness. To help with weakness, elders may also use the opposite hand to assist in the movement of the dominant hand when bringing food to the mouth. The “clock method” is helpful for blind elders or for those with other visual deficits to orient them to the position of the plate, cup, eating utensils, and food in front of them. Items should be positioned consistently for this method to be most effective. Elders who are impulsive may require cues for both bite size and pacing of bites. Elders can be guided or instructed to put the eating utensil down between bites to pace the amount of food entering the mouth. Presenting elders with one food item at a time may also be helpful. Large food items should be cut into bite-sized portions. Using a spoon for liquids is often helpful. COTAs should coordinate eating with breathing for elders on ventilators or for those with other breathing difficulties. Energy conservation may also be indicated, including limiting conversation during mealtime. For elders with low endurance, alternating food textures during the meal, ordering foods that are easy to chew, and/or having six small meals available during the day may be helpful.
Several strategies may be helpful to use with elders who have severe dementia. Frequent small feedings and finger foods are useful for elders with low attention spans or who pace constantly and cannot sit still long enough to complete a meal. Decreasing environmental stimulation, maintaining consistency in feeding helpers, and reducing verbal communication during the meal may help decrease distractions and permit elders with dementia to focus longer on eating. When such elders refuse a particular food item, a helpful strategy is to place that food item on a plate of a different color, reheat it, and serve it again. With this particular elder population, COTAs should be careful that elders do not eat nonedible items placed on the table such as plants and napkins. Removing the knife from the place setting of such elders may also be necessary for safety.14
Several interventions may be used during the oral phase. Tongue sweeps prevent oral pocketing of food. Alternating solids and liquids helps clean the mouth and remove any food residue in the mouth, but may be contraindicated when dysphagia is present. Food should be placed in the center of the tongue. Varying food temperatures with each bite may promote a safer swallow by stimulating the mouth and increasing awareness of the bolus. Occasionally, elders with hypertonicity need food to remain at a consistent temperature to avoid increasing muscle tone. Asking elders to increase the number of times they chew a bite of food helps break down the bolus and reduce the pace of eating. Elders may need to be cued to close the lips to prevent spillage. The oral cavity should be checked for any residue after each meal. Dentures must fit well and should be thoroughly cleaned after each meal to prevent ulcers from developing in the mouth, to prevent chipping of the dentures from hardened food, and prevent risk for aspiration from food residue under the dentures.15
Problems during the pharyngeal phase of swallowing may require many intervention strategies. Elders should be given sufficient time to swallow between bites. COTAs should learn to observe and palpate swallowing and be able to recognize delays in the swallow response. These skills help in the ongoing assessment of elders. Individuals with hemiplegia may benefit from turning the head toward the hemiplegic side or tilting the head toward the non-hemiplegic side to protect the airway while swallowing.16 Elders should be checked for voice clarity after a swallow to make sure that there is no food or liquid residual on the vocal folds.17 Coughing or clearing the throat followed by a dry swallow may help eliminate a wet-sounding voice after a swallow. Multiple swallows after each bite may also be encouraged. The COTA should work closely with the OTR when feeding elders with tracheostomies. If approved by the physician, the tracheostomy may or may not be plugged, and the cuff can be deflated during feeding to increase air pressure for a stronger swallow.
Several advanced techniques, including the supraglottic swallow, Valsalva maneuver, and Mendelsohn maneuver, may be required, for which close instruction and supervision from the OTR is essential.8 Advanced training is necessary for the implementation of these strategies, and the COTA should demonstrate competency in their application because they are not entry-level skills. Because of the wide range of individual dysphagia problems, the strategies presented here can be modified as necessary. When interventions are planned and carried out with the elder’s quality of life in mind, as well as his or her safety while swallowing, the elder’s motivation for food intake and sense of empowerment will prevail.
Dietary Concerns
Research into the nutritional needs of elders has increased as the elderly population grows.17-19 COTAs should understand elders’ nutritional requirements. Elders often prefer to eat softer, sweeter, and easy-to-prepare foods, and also often drink less fluids. These habits may result in the elder becoming undernourished or malnourished. If elders become ill and are institutionalized, undernourishment or malnutrition can lead to other health problems and delay recovery.
Physiological changes occur slowly over time in all body systems as people age. These changes are influenced by past nutritional habits, life events, illnesses, genetic traits, and socioeconomic factors.20 Sensory changes may include a decline in sight and peripheral vision, hearing, smell, and taste.21 Although the losses are neither total nor rapid, they can affect nutritional intake and health status. For example, loss of visual acuity may lead to less activity or a fear of cooking, especially using a stove. Inability to read food prices, nutrition labels, or recipes may affect grocery shopping, food preparation, and eating. Loss of hearing may lead to less eating out or not asking questions of the waiter or store clerk. Finally, changes in smell and taste are more obvious. If food does not taste appetizing or smell appealing, elders may not want to eat it. If they must cut back on salt, sugar, or fat, they may tend not to eat.22
Many structural changes may also take place as people age, particularly loss of lean body mass. Muscle loss may include skeletal and smooth muscle mass that can affect the function of organs, particularly the heart. This may result in reduced cardiac capacity. Because about 72% of total body water is in lean muscle tissue, loss of total body mass also means loss of hydration.23 Other organs often affected include the kidneys, lungs, and liver, which may result in the body’s lowered ability to generate new protein tissue or in slowing the immune system’s ability to produce antibodies.24 The most significant result of the loss of lean body mass may be the decrease in basal energy metabolism because of the decline in total protein tissue. As protein tissue declines, calories are more likely to become body fat if a person’s level of activity also decreases.25 Finally, women tend to lose bone mass at an accelerated rate after menopause. Severe osteoporosis is debilitating and serious because of the risk of falls and fractures. Vertebral compression as a result of loss of hydration and/or fractures can change chest configuration which, in turn, can affect breathing, intestinal distension, and internal organ displacement.26
Nutrition can be a factor in all of the changes noted above. However, the slowing of the normal action of the digestive tract plus general physiological changes have the most direct effect on nutrition. Digestive secretions diminish markedly, although enzymes remain adequate. Adequate dietary fiber will maintain regular bowel function and not interfere with the digestion and absorption of nutrients, as may occur with laxative use or abuse.26 The challenge for the elderly is to meet the same nutrient needs as when they were younger, yet consume fewer calories. Choosing nutrient dense foods (high in nutrients in relation to their calories), reducing overall fat content of the diet, emphasizing complex carbohydrates, enhancing dietary fiber intake, assuring adequate liquid intake, and consuming a variety of food remain a priority for elders.22 It may be important for the elder to be referred to a dietitian to obtain information about optimal nutrition and hydration that does not interfere with medications.
Diet modifications are frequently needed for elders with dysphagia. These modifications may include different consistencies of liquids (for example, thin-like water, semi-thick-like nectar, and thick-like honey) and different methods of preparing solid foods (for example, pureed, minced, chopped, and soft).8 If oral intake is limited or impossible, elders with dysphagia may receive nutrition and hydration through alternative means (such as a nasogastric tube, a gastrostomy, a jejunostomy, or parenteral nutrition). The entire treatment team is responsible for monitoring intake and ensuring that elders consume the appropriate amounts of protein, fiber, vitamins, minerals, and fluids.2,12 Misinterpretations regarding intake may occur when intake is being monitored if food sources are not also recorded together with calories consumed.
Food preferences, food allergies, and any diet restrictions resulting from medical conditions such as diabetes and congestive heart failure should be considered when food and liquid selections are being made with elders and their families. Cultural issues regarding food must also be considered when planning for an elder’s care. Increased discussion has occurred regarding the ethical and legal issues associated with permitting elders to consume unsafe liquid or solid food consistencies or imposing alternative means for feeding. Ultimately, the physician is responsible for finalizing a decision regarding this issue with elders and their families. This issue, however, requires much input from the team regarding the benefits, risks, alternatives, and prognoses. If the decision is made to allow elders to consume unsafe food items, discontinuation of OT intervention is recommended.27,28
Precautions
When working with elders with feeding and swallowing problems, COTAs should consider many factors concerning the safety of oral intake. Some of these factors include level of alertness, orientation and cognitive status, positioning, general endurance, and the ability to self-feed. The presence of a delayed swallow, food pocketing, effortful chewing, coughing, choking, a runny nose, and a wet-sounding voice indicates swallowing difficulties with the food or liquid being consumed. The COTA should either discontinue the troublesome food or liquid or modify it to a safer consistency. The OTR should be informed of this as soon as possible so that the elder can be further evaluated.
Other indicators of swallowing and nutritional problems may include an increased temperature, lung congestion, and poor intake. Increased temperature and lung congestion may be a sign that the elder has aspirated food or liquid and that pneumonia is developing. Poor intake may indicate an inability to swallow rather than a poor appetite. All personnel working with elders with possible swallowing problems must be aware of these indications and be trained in how to assist someone who is choking and in cardiopulmonary resuscitation in the event that an elder chokes.
Many elders receive medications for various conditions. Medications must be taken with the correct liquid or semisolid consistency. More than 1 oz (30 ml) liquid should be taken after each pill to ensure adequate transport to the stomach. Elders should be sitting up and should be prevented from reclining for 20 minutes after a meal or after taking medication to ensure the safe passage of the food or pill to the stomach. Pills should be taken as specified by the physician. COTAs should consult with the physician or pharmacist to check whether the pills can be halved or crushed because some pills work through time release and crushing them may result in too much medication being absorbed at once. Nursing staff should be present while the medications are taken to ensure that swallowing has actually occurred.
Many elders are at greater risk for aspiration when using straws and taking serial swallows with liquids. The OTR should alert the COTA if an elder is safe to drink fluids in these ways. Many elders who are impulsive require close supervision to prevent overfilling the mouth or eating too fast, activities that may result in choking. The COTA should gain extensive knowledge and experience with the swallowing process before attempting to work with elders who have tracheostomies or are on ventilators. Again, service competency in this should be established with the OTR before the COTA implements any intervention.
Nursing/Caregiver Instruction
COTAs have a vital role in training caregivers to assist elders with self-feeding and dysphagia management. Caregivers may include spouses, partners, family members, friends, hired attendants, and other health care workers such as nurses and nurse’s aides. COTAs must consider the caregiver’s culture and lifestyle when making decisions about the most beneficial type of teaching technique to use. Some individuals learn best through observing the COTA. Others may learn best by doing it themselves under the direction of the COTA, and others may perform best with verbal instruction. Written information and instructions should be provided to elders and caregivers whenever possible. In general, all of these techniques should be used with each caregiver to assure the best follow-through. COTAs must be aware of their verbal tone when teaching the caregiver, taking care not to sound condescending.
The education of caregivers must include training in many aspects of self-feeding and swallowing. First, caregivers should understand the feeding strengths and weaknesses of elders. The need for quality time during the meal and for presentation of a positive attitude to promote elder motivation and independence should be stressed. Thorough instruction should be given on proper body mechanics required by caregivers when assisting elders with feeding. Additional instruction should be provided regarding safe positioning, environmental concerns, use and care of assistive equipment, specific intervention techniques, appropriate verbal and nonverbal cueing, dietary modifications, and signs of possible food or liquid aspiration. Caregivers may take some time to develop good observation and problem-solving skills. Caregivers must understand the importance of communicating any problems or changes in an elder’s status to the appropriate team member. Caregivers should also be familiar with choking prevention maneuvers and emergency suctioning procedures. Problem solving together with caregivers is useful when dealing with elders who have difficult feeding behaviors. COTAs may share with caregivers their anecdotal successful experiences in cueing and obtaining desirable behaviors and eliminating undesirable ones with a particular elder.
An integral part of caregiver training is monitoring the food and fluid intake of elders, together with considering nutritional value and maintaining a modified diet. Family and friends may occasionally present a problem by not complying with the dietary restrictions of their loved one. The possible negative consequences of not following through with the prescribed feeding program should be stressed. COTAs should work with dietitians and caregivers in helping families plan meals. COTAs may also ask the caregivers of institutionalized elders to bring a meal from home and modify it with the assistance of a COTA.
Instructing caregivers on the swallowing and self-feeding protocols set up for elders helps COTAs promote continuity and quality of care. Caregivers should be integrated as soon as possible in the intervention and care of elders. Training several family members and nursing staff helps spread the responsibility of assisting elders during the meal. As with any intervention given to elders, all training of caregivers should be thoroughly documented. By fulfilling these principles, the COTA abides by the Code of Ethics developed by the AOTA.29
Ideas for Managing a Feeding Program
Residents of skilled nursing facilities who are fed in their rooms are frequently positioned poorly, spend most of their day in bed, are often rushed, and often cannot finish their meals. Consequently, their intake, nutrition, and body weight decrease.18,19 A well organized facility-wide feeding program helps get elders out of bed, changes their environment, provides social stimulation, ensures good nutrition and hydration, and increases safety. This type of program also helps maximize their functional abilities and enhances the quality of the mealtime for institutionalized elders. Although many feeding program formats designed for a variety of settings are available, the following is a generic program that requires adjustments to fit the needs of particular elders and particular facilities.
An interdisciplinary approach is the most beneficial in a feeding program. Usually the elder, the OTR, COTA, speech and language pathologist, dietitian, kitchen staff, physician, nursing staff, and family are involved. The physical therapist may also be included to assist with positioning, and the respiratory therapist may be included to assist with issues of pulmonary hygiene or coordination of tracheostomy or ventilator equipment. Elders with self-feeding and dysphagia difficulties are evaluated and referred to a dining group by the OTR or the speech and language pathologist, or both. These elders then are placed in one of several groups organized by the amount of assistance they require. The ratio of elders to COTAs varies depending on the needs of the group. COTAs should always have a group size that can be safely managed. A written protocol should exist that includes information on the purpose of the program and the format, staffing, size, and site of the group. There also should be criteria for referral to, continuation in, and discharge from the program. Timelines, goals, and responsibilities of the COTA or other leader should be made explicit, and documentation and equipment protocols should be explained. There should also be an established system to maintain communication with the entire team to ensure a successful program.
The feeding program should address all meals. In some settings, COTAs are unable to be present at each meal. In other settings, a COTA may not be needed to assist higher-level groups that require minimal assistance or supervision. In these situations, nursing aides, restorative aides, family members, and volunteers may be best used. However, before volunteers are used in this capacity, the guidelines from regulatory agencies should be consulted. For all individuals to perform effectively and safely, they must receive formal training on leading groups, on therapeutic interventions, and on safety.
Case Study
Eric is a 68-year-old, right-hand dominant man who experienced a left cerebrovascular accident and now has right hemiplegia. He has impaired movement and sensation on the right side. In addition, he has apraxia, aphasia, right hemianopsia, and right neglect. One week after his stroke, Eric was transferred to a skilled nursing facility’s rehabilitation unit.
A dysphagia evaluation and videofluoroscopy were done and the following observations were noted: decreased muscle tone with impaired movement and sensation of the face, tongue, and soft palate on the right side, resulting in facial droop, poor lip seal, minimal drooling and food spillage, slurred speech, and a nasal quality to his speech. The videofluoroscopy revealed impaired oral control of the bolus and spillage of food and liquid into the pharynx before the swallow was initiated. Initiation of the swallow was delayed up to 5 seconds. Residual pooling was observed in the valleculae and pyriform sinuses after the swallow. Spontaneous clearing of the throat with additional swallows was impaired. Eric required verbal cueing to initiate clearing swallows. Aspiration into the trachea was observed while Eric swallowed thin and semi-thick liquids by spoon and thick liquids by cup and a mixed consistency bolus (liquid and solid combination, such as soup). Eric did cough spontaneously when aspiration occurred. He had difficulty chewing dry, hard solids and did better with moist, soft solids and semisolids, although oral pocketing and spillage from the mouth was observed with these consistencies. When Eric used the compensation method of turning his head to the right, decreased pooling in the right valleculae and pyriform sinus resulted.
Therapeutic recommendations included one-on-one assistance at meals for self-feeding and a modified diet of thick liquids by spoon. Semisolids and minced, soft solids with no mixed consistencies also were recommended. Further suggestions were to provide verbal and tactile cues for Eric to turn his head to the right side during the initial swallow and to follow up the initial swallow with two dry swallows. In addition, Eric’s caloric and fluid intake were to be closely monitored.
Before the meal, the COTA reviewed the chart for any recent orders and nursing and therapy progress notes to understand how the elder’s day had gone thus far. The COTA arranged to meet Eric’s family in the dining room for them to observe this meal. When Eric arrived in the dining room, the COTA observed that he was not sitting erect in his wheelchair and that he needed to be repositioned. When Eric was sitting erect, the COTA brought him to the table, locked the wheelchair, positioned Eric’s feet on the floor, and placed his hemiplegic arm forward on the table.
Before the meal the COTA directed Eric through several oral-facial exercises. Icing also was used to increase tone and sensation in his right cheek and throat. The COTA iced the outside of Eric’s mouth with ice wrapped in a washcloth and then iced the inside of his cheeks and tongue with a cold metal spoon that was dipped in a cup of ice. Icing also would be done on the cheek, the anterior part of the neck, and inside his mouth on the right side during the meal.
When the tray with Eric’s meal arrived, the COTA checked to ensure that the consistencies of both solids and liquids were correct. The liquid on the tray was semi-thick, therefore the COTA thickened it with a thickening agent. No other modifications were needed. A plate guard was put on the plate to prevent food from spilling.
Because Eric requires assistance with tray setup and self-feeding, the COTA guided Eric’s left hand (non-hemiplegic) using the hand-over-hand method to remove the container lids, butter the bread, cut the food with the rocker knife, and bring the food to his mouth. When Eric was able to integrate the movement and its rhythm and was able to feed himself independently, the COTA stopped providing hand-over-hand guiding. However, when Eric moved too quickly and took too large a bite, the COTA resumed the guiding. When Eric drooled, the COTA guided him to wipe his face with a napkin. With each bite the COTA directed Eric to double swallow and felt Eric’s throat for the swallow. The COTA asked Eric to speak occasionally to check his vocal quality, and when it was wet-sounding, the COTA asked Eric to clear his throat. Whenever Eric was unable to clear his throat, the COTA asked him to dry swallow. Finally, the COTA periodically checked Eric’s mouth for food pocketing and directed him to clear residuals in his right cheek by using his tongue or left index finger.
After the meal, the COTA guided Eric to use a toothette to clean his oral cavity of the food residue. The COTA instructed Eric to remain upright for at least 20 more minutes. A nurse then arrived with medications, which were crushed and mixed with the thick liquid and given to Eric with a spoon. After he swallowed the medication, Eric was given additional thick liquid by spoon to ensure that the medication passed to the stomach.
The COTA then asked the family if they had any questions and provided them with additional instructions. Finally, the COTA documented what and how much Eric ate; the level of assistance that was required; how long it took to complete the meal; the presence of any coughing, wet-sounding voice, or choking; and the food consistency given to him when these events occurred. In addition, the COTA documented all instructions given to the family.
As Eric progressed during meals, he needed less and less hand-over-hand guiding and verbal instruction from the COTA. The COTA began supervising family members as they assisted Eric with meals. Eric progressed to a group dining situation, and when Eric seemed to have a little problem with a wet-sounding voice, food pocketing, follow-through with compensatory techniques, duration of the meal, caloric intake, and spiking temperatures, the COTA requested that the OTR reevaluate him. A follow-up videofluoroscopy was done to rule out aspiration of thin liquids and mixed consistencies, and it showed that Eric had improved but still had impaired oral control of the bolus and pooling in the pharynx. However, Eric now clears this pooling spontaneously, no aspiration is noted, and these items were added to his diet.
Because Eric can now set up his tray with minimal assistance, cut the food with a rocker knife, bring the food to his mouth, eat slowly, and check for pocketing independently, he no longer requires OT supervision at meals.
1. What is the definition of dysphagia?
2. What are the four phases of swallowing?
3. What are the three liquid consistencies?
4. Name four signs that may indicate the presence of swallowing problems.
5. Name three common changes that occur during the phases of swallowing as an individual ages.
6. Identify at least two psychological issues that may have an effect on oral intake.
7. Explain why the COTA should be concerned about nutritional balance and amount of oral intake.
8. Why is the dining environment important for nutritional intake?
9. What should the COTA do if an elder coughs continuously during a meal?
10. Describe how an individual’s body should ideally be positioned during a meal.
1 American Occupational Therapy Association. Occupational therapy practice framework: Domain and process, 2nd ed. American Journal of Occupational Therapy. 2008;62(6):625-683.
2 Ney D., Weiss J., Kind A., Robbins J. Senescent swallowing: Impact, strategies, and interventions. Nutrition in Clinical Practice. 2009;24(3):395-413.
3 Administration on Aging. A Profile of Older Americans: 2008. Washington, DC: U.S. Department of Health and Human Services; 2008.
4 Hays N., Roberts S. The anorexia of aging in humans. Physiology & Behavior. 2006;88(3):257-266.
5 Schnelle J., Bertrand R., Hurd D., White A., Squires D., Feuerberg M., et al. The importance of standardized observations to evaluate nutritional care quality in the survey process. Journal of the American Medical Directors Association. 2009;10(8):568-574.
6 American Occupational Therapy Association. Specialized knowledge and skills in feeding, eating, and swallowing for occupational therapy practice. American Journal of Occupational Therapy. 2007;61:686-700.
7 McFarland D. Netter’s Atlas of Anatomy for Speech, Swallowing, and Hearing. St. Louis, MO: Mosby; 2008.
8 Murray T., Carrau R. Clinical Management of Swallowing Disorders. San Diego, CA: Plural; 2006.
9 Cherney L. Clinical Management of Dysphagia for Adults and Children. Rockville, MD: Aspen; 1994.
10 Cook I. Oropharyngeal dysphagia. Gastroenterology Clinics of North America. 2009;38(3):411-431.
11 Puisieux F., D’andrea C., Baconnier P., Bui-Dinh D., Castaings-Pelet S., Crestani B., et al. Swallowing disorders, pneumonia and respiratory tract infectious disease in the elderly. Revue Des Maladies Respiratoires. 2009;26(6):587-605.
12 Dewing J. Prioritising mealtime care, patient choice, and nutritional assessment were important for older in-patients’ mealtime experiences. Evidence-Based Nursing. 2009;12(1):30.
13 Hägg M., Anniko M. Lip muscle training in stroke patients with dysphagia. Acta Oto-Laryngologica. 2008;128(9):1027-1033.
14 Amella E., Grant A., Mulloy C. Eating behavior in persons with moderate to late-stage dementia: Assessment and interventions. Journal of the American Psychiatric Nurses Association. 2008;13(6):360-367.
15 Haidary A., Leider J., Silbergleit R. Unsuspected swallowing of a partial denture. American Journal of Neuroradiology. 2007;28(9):1734-1735.
16 Singh S., Hamdy S. Dysphagia in stroke patients. Postgraduate Medical Journal. 2006;82(968):383-391.
17 Foley N., Martin R., Salter K., Teasell R. A review of the relationship between dysphagia and malnutrition following stroke. Journal of Rehabilitation Medicine. 2009;41(9):707-713.
18 Walton K., Williams P., Bracks J., Zhang Q., Pond L., Smoothy R., et al. A volunteer feeding assistance program can improve dietary intakes of elderly patients—a pilot study. Appetite. 2008;51(2):244-248.
19 Wright L., Cotter D., Hickson M. The effectiveness of targeted feeding assistance to improve the nutritional intake of elderly dysphagic patients in hospital. Journal of Human Nutrition and Dietetics. 2008;21(6):555-562.
20 Thomas D. Nutritional requirements in older adults. In: Morley J., Thomas D., editors. Geriatric Nutrition. Boca Raton, FL: CRC Press; 2007:103-122.
21 Schiffman S. Sensory impairment: Taste and smell impairment in aging. In: Bales C., Ritchie C., editors. Handbook of Clinical Nutrition and Aging. 2nd ed. New York: Humana Press; 2009:77-98.
22 Chernoff R. Geriatric Nutrition: The Health Professional’s Handbook, 3rd ed. Sudbury, MA: Jones & Bartlett; 2006.
23 Thomas D., Morley J. Water metabolism. In: Morley J., Thomas D., editors. Geriatric Nutrition. Boca Raton, FL: CRC Press; 2007:131-136.
24 Morley J. The role of nutrition in the prevention of age-related diseases. In: Morley J., Thomas D., editors. Geriatric Nutrition. Boca Raton, FL: CRC Press; 2007:29-44.
25 Drozdowski L., Iordache C., Woudstra T., Thompson A. Lipid absorption in aging. In: Watson R., editor. Handbook of Nutrition and the Aged. 4th ed. Boca Raton, FL: CRC Press; 2009:113-148.
26 Omran L., Aneed W. Nutrition and gastrointestinal function. In: Morley J., Thomas D., editors. Geriatric Nutrition. Boca Raton, FL: CRC Press; 2007:451-468.
27 Groher M.E. Ethical dilemmas in providing nutrition. Dysphagia. 1990;5:102-109.
28 Vesey S., Leslie P., Exley C. A pilot study exploring the factors that influence the decision to have PEG feeding in patients with progressive conditions. Dysphagia. 2008;23(3):310-316.
29 American Occupational Therapy Association. Occupational Therapy Code of Ethics. American Journal of Occupational Therapy. 2005;59:639-642.