1. AAA Foundation for Traffic Safety, Beverly Foundation. Transportation alternatives for seniors: high cost problems low cost solutions. Available at http://www.seniordrivers.org/STPs/whitepaper6.cfm.
1a. ADA Law. Americans With Disabilities Act of 1990. Available at www.adaportal.org/adadoc-Law/ADA_Statute_TOC.aspx.
2. ADA. Accessibility guidelines for transportation vehicles. Available at http://www.access-board.gov/transit/html/vguide.htm#AP.
3. Adler, C. Wheelchairs and seat cushions: a comprehensive guide for evaluation and ordering. San Jose, Calif: Santa Clara Valley Medical Center, Occupational Therapy Department; 1987.
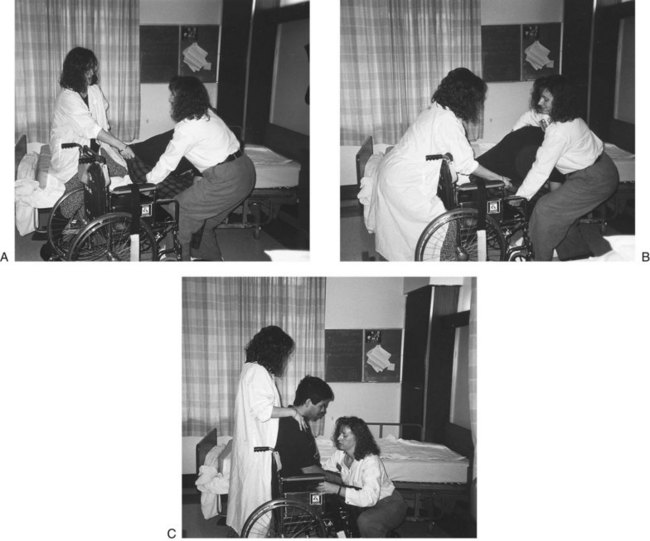
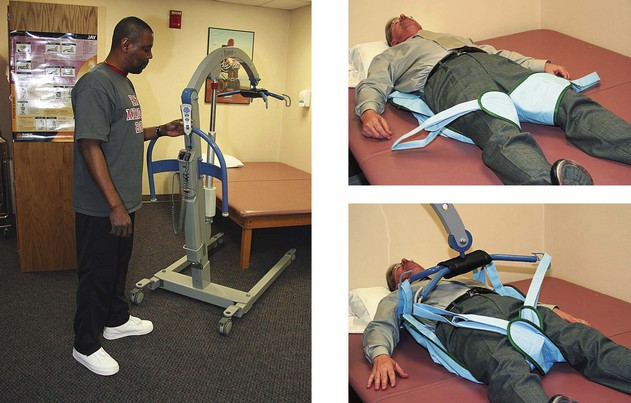
4. Adler, C, Musik, D, Tipton-Burton, M. Body mechanics and transfers: multidisciplinary cross training manual. San Jose, Calif: Santa Clara Valley Medical Center; 1994.
5. Alexander, H. On the road: are we prepared to keep older drivers safe? Physical Disabilities Special Interest Quarterly. 2010;33:23.
6. American Association of Retired Persons, Graduated driver licensing creating mobility choices. Pub. No. D15109, Washington, DC, AARP, 1993.
7. American Medical Association. Physician’s guide to assessing and counseling older drivers. Chicago: American Medical Association; 2003.
8. American Occupational Therapy Association. AOTA’s centennial vision and executive summary. Am J Occup Ther. 2007;61:613.
9. American Occupational Therapy Association. Board and specialty certification. http://www.aota.org/Practitioners/ProfDev/Certification.aspx, 2010. [Available at].
10. American Occupational Therapy Association, Commission on Continuing Competence and Professional Development (CCCPD). Available at http://www.aota.org/members/area16/index.asp.
11. American Occupational Therapy Association. Driving and transportation alternative for older adults (fact sheet). Bethesda, Md: AOTA; 2003.
12. American Occupational Therapy Association. Guidelines for supervision, roles, and responsibilities during the delivery of occupational therapy services. http://www.aota.org/Practitioners/Resources/Otas/Supervision/36202.aspx, 2009. [Available at].
13. American Occupational Therapy Association. Occupational therapy practice framework: domain and process. Am J Occup Ther. 2002;56:609.
14. American Occupational Therapy Association. Older driver: for professionals. Available at http://www.aota.org/Olser-Driver/Profesionals.aspx.
15. American Occupational Therapy Association. Statement: driving and community mobility. http://www.aota.org/Practitioners/Official/Statements/41093.aspx, 2010. [Available at].
16. American Public Transit Association. Funding the needs of an aging population. Available at http://www.apta.com/resources/reportsandpublications/Documents/TCRP_J11_Funding_Transit_Needs_of_Aging_Population.pdf.
17. American Public Transportation Association. Public transportation takes us there. Available at http://www.publictransportation.org/takesusthere/docs/facts_at_a_glance.pdf.
18. American Public Transportation Association. Transit ridership report first quarter 2004. Available at http://www.apta.com/research/stats/ridership/riderep/documents/04q1cvr.pdf.
19. American Society on Aging. Drive well toolkit and training program. Available at http://www.asaging.org/asav2/drivewell/toolkit.cfm.
20. American Society on Aging. Driving transitions education program: tools, scripts, and practice exercises. Available at http://www.asaging.org/asav2/drivewell/driving_transitions.cfm.
21. Amini, D, Mortera, M, Gulick, K, et al. The centennial vision and physical disabilities practice. Physical Disabilities Special Interest Quarterly. 2008;31:1.
22. Arbesman, M, Pellerito, JM. Evidence based perspective on the effect of automobile related modifications on the driving ability, performance, and safety of older adults. Am J Occup Ther. 2008;62:173.
23. Arilotta, C. Performance in areas of occupation: the impact of the environment. Physical Disabilities Special Interest Quarterly. 2003;26:1.
24. Association of Driver Rehabilitation Specialists (ADED). ADED documents and resources, CD-ROM. Ruston, La: ADED; 2004.
25. Association for Driver Rehabilitation Specialists (ADED). Best Practices for the delivery of driver rehabilitation services. Available at: from http://www.driver-ed.org/Files/public/ADED_Best_Practices_2009.Edition.
26. Association for Driver Rehabilitation Specialists (ADED). Certification. Available at http://www.driver-ed.org/i4a/pages/index.cfm?pageid=120.
27. Association for Driver Rehabilitation Specialists (ADED). Disabilities and driving fact sheets. Available at http://www.driver-ed.org/i4a/pages/index.cfm?pageid=329.
28. Association for Driver Rehabilitation Specialists (ADED). History. Available at http://www.driver-ed.org/i4a/pages/index.cfm?pageid=119.
29. Babirad, J. Driver evaluation and vehicle modification. In: Olson D, DeRuyter F, eds. Clinician’s guide to assistive technology. St Louis: Mosby, 2002.
30. Baker, P. Driver rehabilitation: assessing the older driver. OT Practice. May 28, 2007:10.
31. Ball, K, Owsley, C. The useful field of view test: a new technique for evaluating age-related declines in visual function. J Am Optom Assoc. 1992;63:71.
32. Berlly M, Lillie SM: Long term disability: the physical and functional impact on driving. Presented at: ADED Annual Conference, 2000, San Jose, Calif.
33. Berres, S. Keeping kids safe: passenger restraint systems. OT Practice. October 20, 2003:13.
34. Beverly Foundation. About us. Available at http://www.seniordrivers.org/STPs/about_us.cfm.
35. Beverly Foundation. Community effectiveness in safeguarding at-risk senior drivers, interim report. Pasadena, Calif: Beverly Foundation; February 1998.
36. Beverly Foundation. STPs in America, fact sheet. Available at http://www.beverlyfoundation.org/media/factsheet/factsheet.vol.1.no.3.STPs.America.pdf.
37. Blanc C: Seating and positioning behind the wheel: special considerations when driving a vehicle from a wheelchair. Presented at: ADED Annual Conference, 1995, Dearborn, Mich.
38. Bohr, PC. Critical review and analysis of the impact of the physical infrastructure on the driving ability, performance, and safety of older adults. Am J Occup Ther. 2008;62:159.
39. Bouska, MJ, Gallaway, M. Primary visual deficits in adults with brain damage: management in occupational therapy. Occup Ther Pract. 1991;3:1.
40. Brachtesende, A. Ready to go? OT Practice. October 6, 2003:14.
41. Brain Injury Association of America. Driving after brain injury: issues, obstacles, and possibilities. Available at http://www.biausa.org/elements/pdfs/awareness/driving_booklet.pdf.
42. Breske, S. The drive for independence. Adv Rehabil. 1994;8:10.
43. Bromley, I. Tetraplegia and paraplegia: a guide for physiotherapists, ed 3. London, United Kingdom: Churchill Livingstone; 1985.
44. CarFit. Helping mature drivers find their safest fit. Available at http://www.car-fit.org.
45. Centers for Disease Control and Prevention. Healthy aging: improving and extending quality of life among older Americans: at a glance 2010. Available at http://www.cdc.gov/chronicdisease/resources/publications/AAG/aging.htm.
46. Centers for Disease Control and Prevention. Injury prevention and control: traumatic brain injury. Available at http://www.cdc.gov/traumaticbraininjury.
46a. CarFit. Frequently asked questions. Available at http://www.car-fit.org/carfit/FAQ.
47. Centers for Disease Control and Prevention/National Center for Health Statistics (2007-2008). Available at www.cdc.gov/nchs.
48. Cesari, M. Prevalence and risk factors for falling in an older community-dwelling population. J Gerontol. 2002;57:722.
49. Christopher and Dana Reeve Foundation Paralysis Resource Center. Prevalence of paralysis. Available at http://www.christopherreeve.org/site/c.mtKZKgMWKwG/b.5184255/k.6D74/Prevalence_of_Paralysis.htm.
50. Clark, F. AOTA’s centennial vision: what it is, why it’s right. Available at http://www.aota.org/News/Centennial/Backgrounnd/36563.aspx.
51. Classen, S. From the desk of the guest editor: special issue on older driver safety and community mobility. Am J Occup Ther. 2010;64:211.
52. Classen, S, Levy, C, McCarthy, D, et al. Traumatic brain injury and driving assessment: an evidence-based literature review. Am J Occup Ther. 2009;63:580.
53. Classen, S, Shectman, K, Awadzi, KD, et al. Traffic violations versus driving errors of older adults informing clinical practice. Am J Occup Ther. 2010;64:233.
54. Classen, S, Winter, SM, Velozo, CA, et al. Item development and validity testing for a self and proxy report: the safe driving behavior measure. Am J Occup Ther. 2010;64:296.
55. Classen, S, Winter, S, Lopez, EDS. Metasynthesis of qualitative studies on older adult driver safety and mobility. Occup Ther J Res. 2009;29:24.
56. Conference on Driver Competency Assessment: Summary of proceedings, CAL-DMV-RSS-91-132, Sacramento, Calif, 1993, State of California Department of Motor Vehicles, Program and Policy Administration, Research and Development Section.
57. Consortium for Spinal Cord Medicine. Outcomes following traumatic spinal cord injury: clinical practice guidelines for health-care professionals. Available at http://www.pva.org/site/DocServer/OUT.pdf?docID=686.
58. Cook, AM, Hussey, SM. Assistive technologies: principles and practice. St Louis, Mo: Mosby; 1995.
59. Davis, ES. Defining OT roles in driving. OT Practice. January 13, 2004:15.
60. Dickerson, AE, Molnar, LJ, Eby, DW, et al. Transportation and aging: a research agenda for advancing safe mobility. Gerontologist. 2007;47:578.
61. Disability Rights Education and Defense Fund (funded by the Federal Transit Administration). Topic guides on ADA transportation: origin to destination service in ADA paratransit: door to door service is required when necessary. Available at http://www.dredf.org?ADAtg/O-D.shtml.
62. Driving Systems Incorporated. The Scott driving system. Available at http://www.drivingsystems.com/ScottSystem.html.
63. Easter Seals Project Action. Accessible community transportation in our nation. Available at http://projectaction.easterseals.com/site/PageServer?pagename=ESPA_homepage.
64. Easter Seals Project Action. Determining ADA paratransit eligibility: an approach, guidance, and training materials. Available at http://projectaction.easterseals.com/site/DocServer/04ELIG1.pdf?docID=4703.
65. Easter Seals Project Action. Introduction to travel training. Available at http://projectaction.easterseals.com/site/PageServer?pagename-ESPA_travel_training_intro_course_brochure.
66. Eberhard J: A national perspective on older adult transportation: safe mobility for life. Presented at: Older Adults and Transportation: The New Millennium Regional Forum, Los Angeles, Calif, July 22, 1999.
67. Eisenhandler, SA. The asphalt identikit: old age and the driver’s license. Int J Aging Hum Dev. 1990;30:1.
68. Electronic Mobility Controls. J series. Available at http://www.emc-digi.com/explore.cfm/aevitgasbrakesteer/100002.
69. Elgin, J, McGwin, G, Wood, JM, et al. Evaluation of on-road driving in people with hemianopia and quadrantanopia. Am J Occup Ther. 2010;64:268.
70. Federal Interagency Forum on Aging-Related Statistics. Number of older Americans. Available at http://www.aoa.gov/agingstatsdotnet/Main_Site/Data/2008_Documents/population.aspx.
71. Federal Transit Administration. Access for persons with disabilities. Available at http://www.fta.dot.gov/transit_data_info/transit_info_for/riders_with_disabilities/1631_4918_ENG_HTML.htm.
72. Federal Transit Administration. Highlights of the Federal Transit Administration’s impact on public transportation in the United States. Available at http://www.fta.dot.gov/documents/FtaImpactBookz.pdf.
73. Federal Transit Administration. National transit database glossary. Available at http://www.ntdprogram.gov/ntdprogram/Glossary.htm.
74. Fisk, GD, Owsley, C, Pulley, LV. Driving after stroke: driving exposure, advice, and evaluations. Arch Phys Med Rehabil. 1997;78:1338.
75. Florida Department of Transportation Research Center. Project #BD549-44: impact of more rigorous ADA paratransit eligibility on riders with disabilities. Available at www.nctr.usf.edu/pdf/77721.pdf.
76. Freeman, E, West, S, Munoz, B. Driving status and adjusted risk of long term care entry in older adults. Gerontologist. 2004;44:479.
77. Fuhrman, SI, Buning, ME, Karg, P. Wheelchair transportation: ensuring safe community mobility. OT Practice. October 6, 2008:10.
78. Glantz, C, Curry, M. Professional development and certification: what’s in it for me? OT Practice. April 14, 2008:21.
79. Glass, TA, de Leon, CM, Marottoli, RA, Berkman, LF. Population-based study of social and productive activities as predictors of survival among elderly Americans. Br Med J. 1999;319:478.
80. Golden, M, Kilb, L, Mayerson, A. Explanation of the contents of the Americans With Disabilities Act of 1990. Washington, DC: Disability Rights Education and Defense Fund; 1990.
81. Green, L. Keys to starting a driver rehabilitation program. OT Practice. October 6, 2003:18.
82. Howard Hughes Medical Institute. FDR and polio: public life, private pain. Available at http://www.hhmi.org/biointeractive/disease/polio/polio2.html.
83. Hunt, LA, Arbesman, M. Evidence-based and occupational perspective of effective interventions for older clients that remediate or support improved driving performance. Am J Occup Ther. 2008;62:136.
84. Insurance Institute for Highway Safety. Fatality facts 2008: older people. Available at http://www.iihs.org/research/fatality_facts_2008/olderpeople.html.
85. Insurance Institute for Highway Safety. Question and answers: older people. Available at http://www.iihs.org/research/qanda/older_people.html.
86. Janke, MK. Age related disabilities that may impair drivers and their assessment. Sacramento, Calif: State of California, Department of Motor Vehicles; 1994.
87. Johannson, C, Top 10 emerging practice areas to watch for in the new millennium. OT Practice January 13, 2000. Available at, www.aotalorg/Practitioners/PracticeAreas/Emerging/36247.aspx.
88. Kalina, T. Starting a driver rehabilitation program. Work. 1997;8:229.
89. Kaplan, W. The occupation of driving: legal and ethical issues. Physical Disabilities Special Interest Quarterly. 1999;22:1.
90. Kartje, P. Approaching evaluating, and counseling the older driver for successful community mobility. OT Practice. October 23, 2006:11.
91. Kelley-Moore, A, Schumacher, JG, Kahana, E, Kahana, B. When do older adults become “disabled”? Social and health antecedents of perceived disability in a panel study of the oldest old. J Health Soc Behav. 2006;47:126.
92. Korner-Bitensky, N, Bitensky, J, Sofer, S, et al. Driving evaluation practices of clinicians in the United States and Canada. Am J Occup Ther. 2006;60:428.
93. Lamb, SE, Ferrucci, L, Volapto, S, et al. Risk factors for falling in home-dwelling older women with stroke. The Women’s Health and Aging Study. Stroke. 2003;34:494.
94. Latson, LF. Overview of disabled drivers’ evaluation process. Physical Disabilities Special Interest Quarterly. 10, December 1987.
95. Lohman, H, Gabriel, L, Furlong, B. The bridge from ethics to public policy: implications for occupational therapy practitioners. Am J Occup Ther. 2004;58:109.
96. Lysack, CL, Neufeld, S, Mast, BT, et al. After rehabilitation: an 18-month follow-up of elderly inner-city women. Am J Occup Ther. 2003;57:298.
97. Macciocchi, S, Seel, RT, Thompson, N, et al. Spinal cord injury and co-occurring traumatic brain injury: assessment and incidence. Arch Phys Med Rehabil. 2008;89:1350.
98. Mahoney, JE. Use of an ambulation assistive device predicts functional decline associated with hospitalization. J Gerontol. 1999;54:83.
99. Mallon, K, Wood, JM. Occupational therapy assessment of open-road driving performance: validity of directed and self-directed navigational instructional components. Am J Occup Ther. 2004;58:279.
100. National Council on Disability. Workforce infrastructure in support of people with disabilities: matching human resources to service needs, January 20, 2010. Available at http://www.ncd.gov/newsroom/publications/2010/NCDWorkforce508.pdf.
101. National Highway Traffic Safety Administration: Air bags and on-off switches: information for an informed decision, Pub. No. DOT HS 808 629, Washington, DC, 1999, U.S. Department of Transportation.
102. National Highway Traffic Safety Administration. Driver rehabilitation: a growing niche. OT Practice. May 10, 2004:13.
103. National Highway Traffic Safety Administration. Older driver safety plan. Available at http://www.nhtsa.gov/people/injury/olddrive/OlderDriverSafeyPlan.pdf.
104. National Highway Traffic Safety Administration. Supplemental questions and answers regarding air bags. Available at http://www.nhtsa.dot.gov/people/injury/airbags/supplbag.qa.html.
105. National Highway Traffic Safety Administration. Tools, scripts, and practice exercises. Available at http://www.nhtsa.gov/DOT/NHTSA/Traffic%20Injury%20Control/Articles/Associated%20Files/811152.pdf.
106. National Highway Traffic Safety Administration. What you need to know about airbags. Available at http://www.nhtsa.gov/people/injury/airbags/airbags03/airbags1.html.
107. National Highway Traffic Safety Administration, U.S. Department of Transportation, USA.gov. Airbag FAQs. Available at http://www.safercar.gov/portal/site/safercar/menuitem.13dd5c887c7e1358fefe0a2f35a67789/?vgnextoid=2d4be66aeee35110VgnVCM1000002fd17898RCRD.
108. National Mobility Equipment Dealers Association, Association for Driver Rehabilitation Specialists (ADED). Model practices for driver rehabilitation for individuals with disabilities. Tampa, Fla: The Association; 2002.
109. National Spinal Cord Injury Statistical Center. Facts and figures at a glance. Available at https://www.nscisc.uab.edu/public_content/pdf/Facts%20and%20Figures%20at%20a%20Glance%202010.pdf.
110. National Spinal Cord Injury Association. More about spinal cord injury. Available at http://www.spinalcord.org/html/factsheets/spinstat.php.
111. Odenheimer GL: Cognitive dysfunction and driving abilities. Presented at: Annual Meeting of the American Geriatric Society, May 18, 1990, Atlanta, Ga.
112. Odenheimer, GL, Beaudet, M, Jette, AM, et al. Performance based driving evaluation of the elderly driver: safety, reliability, and validity. Gerontol Med Sci. 1994;49:153.
113. Owen, MM, Stressel, DI. Motor-free visual perception test as a screening tool for driver evaluation and rehabilitation readiness. Physical Disabilities Special Interest Quarterly. 1999;22:3.
114. Owsley, C, Ball, K, McGwin, G, Jr., et al. Visual processing impairment and risk of motor vehicle crash among older adults. JAMA. 1998;279:1083.
115. Pardessus, V. Benefits of home visits for falls and autonomy in the elderly. Am J Phys Med Rehabil. 2002;81:247.
116. Park, S, Fisher, AG, Velozo, CA. Using the assessment of motor and process skills to compare occupational performance between clinic and home settings. Am J Occup Ther. 1994;48:697.
117. Pellerito, JM, Davis, ES. Screening driving and community mobility status: a critical link to participation and productive living. OT Practice. March 21, 2005:9.
118. Pelli, E. Visual field requirements in the U.S.A. Available at http://www.eri.harvard.edu/faculty/peli/papers/viv9.pdf.
119. Perr, A, Barnicle, K. Van lifts: the ups and downs and ins and outs. Team Rehab Report. 1993;4:49.
120. Pezenik, D, Itoh, M, Lee, M. Wheelchair prescription. In: Ruskin AP, ed. Current therapy in physiatry. Philadelphia, Pa: WB Saunders, 1984.
121. Pierce, S. The occupational therapist’s roadmap to safety for seniors. Gerontol Special Interest Q. 2003;26:1.
122. Pierce, S. Starting down the road to establishing a driver evaluation program. OT Practice. June 13, 2005:10.
123. Poole, D, Chaudry, F, Jay, WM. Stroke and driving. Top Stroke Rehabil. 2008;15:37.
124. Public Broadcasting System. Freedom: a history of us. Available at http://www.pbs.org/wnet/historyofus/web12/segment3b.html.
125. Ragland, DR, Satariano, WA, MacLeod, KE. Driving cessation and increased depressive symptoms. J Geront A Biol Sci Med Sci. 2005;60a:399.
126. Rapport, LJ, Hanks, RA, Bryer, RC. Barriers to driving and community integration after traumatic brain injury. J Head Trauma Rehabil. 2006;21:34.
127. Rehabilitation Engineering Research Center on Wheelchair Transportation Safety. The WC19 information resource: crash-tested wheelchairs and seating systems. Available at http://rercwts.org/WC19.html.
128. Rehabilitation Engineering Research Center on Wheelchair Transportation Safety. Wheelchairs and seating systems successfully crash tested with 4-point strap-type securement as of August 18, 2010. Available at http://www.rercwts.org/RERC_WTS2_KT/RERC_WTS2_KT_Stand/RERC_WTS2_19_Chart.html.
129. RideSafe: Information to help you travel more safely in motor vehicles while seated in your wheelchair. Available at http://www.travelsafer.org/step1.shtml.
130. Rosenbloom, S. Mobility of the elderly: good news and bad news. In: Conference proceedings: transportation in an aging society: a decade of experience. Washington, DC: Transportation Research Board; 1999:3.
131. SeniorDrivers.Org. Measuring your driving skills/needs. Available at http://www.seniordrivers.org/home/#assessment.
132. Santa Clara Valley Medical Center, Physical Therapy Department. Lifting and moving techniques. San Jose, Calif: Santa Clara Valley Medical Center; 1985.
133. Schaafsma, JD, Giladi, N, Balash, Y, et al. Gait dynamics in Parkinson’s disease: relationship to Parkinsonian features, falls and response to levodopa. J Neurol Sci. 2003;212:47.
134. Shaheen, S, Rodier, C, Mineta Transportation Institute. Video transit training for older travelers: a case study of the Rossmoor senior adult community, California. Available at http://76.12.4.2491/artman/uploads/1/MTI-06-04.pdf, 2007.
135. Sheffield, FSF. Open your eyes to driving. OT Practice. October 3, 2005:10.
136. Shutrump, SE, Manary, M, Buning, ME. Safe transportation for students who use wheelchairs on the school bus. OT Practice. August 25, 2008:8.
137. State of California Department of Rehabilitation, Mobility Evaluation Program: Interpretive guidelines for vehicle modification participants, Downey, 1998.
138. State of California Department of Rehabilitation, Mobility Evaluation Program: Statement of assurances for providers of driver evaluation services, Downey, 1990.
139. Stav, W. Differentiating yourself in the market as a specialist. OT Practice. July 14, 2008:21.
140. Stav, WB. Review of the evidence related to older adult community mobility and driver licensure policies. Am J Occup Ther. 2008;62:149.
141. Stav, WB, Lieberman, D. From the desk of the editor. Am J Occup Ther. 2008;62:127.
142. Stroke, SA. Driving after stroke: fact sheet G. Available at (Supporting People After Stroke) http://stroke.org.au/pdf/Drivingafterstroke.pdf.
143. Strzelecki, MV. Driving the profession. OT Practice. March 31, 2008:9.
144. CAL-DMV-RSS-91-132. Summary of proceedings of the Conference on Driver Competency Assessment, Sacramento, Calif, State of California Department of Motor Vehicles, Program and Policy Administration, Research and Development Section, 1993.
145. Taylor H, Harris L: N.O.D. survey of Americans with disabilities: the new competitive advantage: expanding the participation of people with disabilities in the American work force. Reprinted from Business Week, May 20, 1994, Washington, DC, National Organization on Disability.
146. Traumatic Brain Injury Model System Consumer Information. Driving after traumatic brain injury. Available at www.tbi.pmr.vcu.edu/FactSheets/Driving.pdf.
147. U.S. Department of Justice, Civil Rights Division, Disability Rights Section. A guide to disability rights laws. Available at http://www.ada.gov/cguide.htm#anchor62335.
148. U.S. Department of Transportation. Americans With Disabilities Act (ADA) paratransit eligibility manual. DOT-T-93-17. Available at http://ntl.bts.gov/DOCS/ada.html.






 Threaded Case Study
Threaded Case Study


 Ethical Considerations
Ethical Considerations