4 The patient journey within medical placements
Introduction
It is important to think about your practice learning pathways and how these can truly reflect the journey your patients are taking. Health care is changing rapidly and it is essential that you are knowledgeable and competent at the point of registration to care for a patient wherever they are within their healthcare journey. Practice learning opportunities should, where possible, reflect local and national care delivery approaches including care pathways (Nursing and Midwifery Council (NMC) 2010a). This might mean that while you are on placement you could move between the community, social care, voluntary sector, non-NHS sector and acute hospital to follow a patient though their journey. Or it could be for you to gain an understanding of the healthcare journey that some of your patients might experience.
This chapter aims to provide you with some examples of patient journeys and how these can translate into practice learning. It will also provide you with an introduction to the key documents you should be familiar with and how they may impact on your practice and the practice of those around you. It will look at clinical policies and guidelines as well as professional guidelines, such as those produced by the NMC, that you should be adhering to as a student nurse.
The broad nature of medical learning pathways and their journey through the healthcare system
Some of your practice learning pathways will be 4 weeks, with others being up to 12 weeks or longer. It is important that you discuss your placement needs and expectations with your mentor. Your mentor will be used to assessing students within their area and will be able to discuss the possible practice learning pathway placements that you may wish to negotiate. The welcome pack and information on your university Website will also help to prepare you for what to expect from this placement. Most mentors have established effective working relationships with other members of the multidisciplinary team across the patient journey and some may have planned your experience to ensure that your placement learning truly reflects the experience of the patient journey. There are many learning opportunities and experiences of the patient pathway that you may wish to negotiate with your mentor.
Stroke unit
A patient who has suffered a stroke will come into contact with a number of the multidisciplinary team. The patient will spend some time in the acute phase of their condition and then some time rehabilitating. Personnel involved in their care might include a psychologist, speech and language therapist, physiotherapist, occupational therapist and doctors. There may also be voluntary groups for carers and patients that you could explore and spend time with. Table 4.1 provides an example of a typical week in the life of a patient following a stroke that you might experience on an 8-week placement.
Table 4.1 Example of an 8-week placement: the patient experience and interprofessional working (negotiated with the mentor)
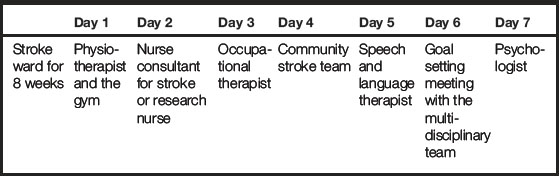
The learning opportunities within this 8-week placement are vast and really allow you to gain knowledge and understanding of the patient journey and experience. The bespoke 1-day placements with the the psychologist, etc., may already be arranged for you by your mentor or there may be an expectation that you, as an adult learner, will arrange these bespoke days. However, you can discuss this with your mentor during your initial meeting. To meet your learning outcomes in such a placement, you would need to negotiate and discuss with your mentor how you could evidence what you have learnt within all of your experiences, and when you would meet up for your midpoint and endpoint meetings to discuss your learning. The teams work closely together and there will be space within your record of achievement/practice curriculum documentation to allow for comments from other nurses and healthcare professionals to document what you have achieved and experienced within your 1-day and 8-week placements (NMC 2010a).

Acute medical admissions unit
You could also be placed on an acute medical admissions unit which would look very different from a stroke unit, however the same principles might apply. Your patient may come in from the accident and emergency (A&E) department and you may find it helpful to spend some time there to understand how the department works and what your patient might have experienced. Your patients may be transferred to other departments and it will be helpful to discuss this with your mentor to determine where else you might need to spend some of your placement time. Some patients may be discharged home with a care package and others may go to a general medical ward or high-dependency unit. Other members of the multidisciplinary team will be involved and, again, you can find this out from your mentor. Table 4.2 gives an example of acute medical admissions unit placement opportunities.

Virtual ward
You may find that your placement base is on a virtual ward. The term ‘virtual ward’ may mean nothing to you and you may worry that you may be disadvantaged or undertaking simulated practice when other members of your cohorts appear to be in more technical or acute placements.
Virtual wards were discussed in Chapter 2 but here is a brief outline. Virtual wards provide support in the community for people with complex medical and social needs. People are cared for by a team of staff as they would be in hospital, however there is no physical building. The virtual ward aims to provide multidisciplinary case management, to prevent admission to secondary care (acute hospital wards) and to enhance the communication for all those involved in the care. The patient is at the centre of the care. There are different models for virtual wards with some being nurse led and others GP led. The patients that you will care for during your virtual ward placement will still require nursing care and interprofessional team working, which will be coordinated by a community matron. There will be liaison with the acute hospital and some teams will work across the acute and community journey of the patients.
For a 4-week learning pathway on a virtual ward, the weeks might be set out as in Table 4.3. For every practice learning pathway you will be provided with a mentor and, as can be seen in Table 4.3, there could be a variety of nurses who might be assigned as your mentor. It could be the community matron, the district nurse or one of the more specialist nurses.
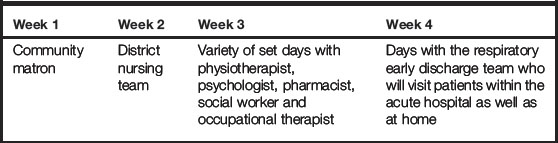
During this placement your mentor can directly or indirectly supervise you (NMC 2008a) and how this will occur will be negotiated during your inital meeting. Within the virtual ward, teams of healthcare professionals will work closely together and a team approach may be taken to ensure that your mentor has all the evidence required to assess you. You should ensure, when you are working with another healthcare professional, that what you have experienced and achieved are documented. Other members of the healthcare team that you spend time with should have been suitably prepared to ensure they are familiar with your learning needs and their role in contributing to your assessment (NMC 2010a).
6-week medical investigations ward placement
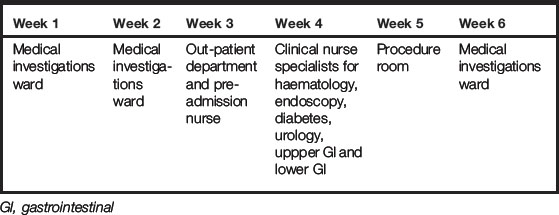
The medical investigations ward may also be called the medical day care unit and provides care for patients who require medical treatment/investigations on a day stay basis who will then be discharged home once their care is complete. Care is often provided on a day case basis and there are now more medical day care units within NHS and non-NHS hospitals.
As a student, after discussion with other students, you may consider that you feel disappointed about not going somewhere more acute and may feel disadvantaged. Do not worry – medical day care is a fabulous experience and you will be able to follow the patient journey from pre-admission to discharge. You will be able to experience the care of the patient pre-procedure, peri-procedure and post-procedure for a number of conditions. Medical day care is often multifaceted with several specialties running alongside each other. It may also be part of the journey for patients who are admitted to acute medical admissions, high-dependency and general wards. You may have the opportunity to follow them back to their ward base and be able to understand their journey. Other patients will be admitted from nursing homes, intermediate care and out-patient departments. Table 4.4 shows an example of how a 6-week placement could look in medical day care.
12-week placement on a general medical ward
Of course, placements can be longer, and a 12–14 week placement is not uncommon within any year of your programme regardless of your field of practice. Longer placements can be really useful in allowing your learning to become much deeper and sustained. Table 4.5 shows an example of a 12-week placement. In this example, you could spend 6 weeks on a general medical ward and then spend 1 or 2 weeks within the specialist clinic environment linked to that ward or spend time with a variety of clincial nurse specialists that your patient may encounter during their journey.
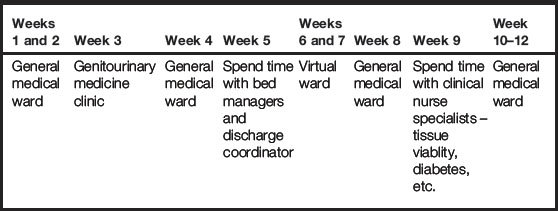
Spending some time with the discharge coordinator can be eye opening and you may begin to understand how vital early discharge planning is and the impact on the patient, carers and organisation if this does not run smoothly. If you can spend some time within a community area that your patients are commonly discharged to, you will be begin to broaden your understanding of the patient journey outside of acute hospital admission. It will help you to understand what information the practitioners require to look after your patient within the community and highlight the resources available there.
The above practice placement pathways are just examples, but hopefully have allowed you to think about the possible learning opportunities when placed on a medical ward, day care or virtual ward.
Some mentors may use the hub and spoke model of placing students, where the placement is considered the hub and all the spokes relate to who the patient might come into contact with and where during their stay in your placement. The spokes also represent learning opportunities and possible experiences that you as a student could benefit from. The examples given in Figures 4.1 and 4.2 look at some hub and spoke models for respiratory and HIV wards.
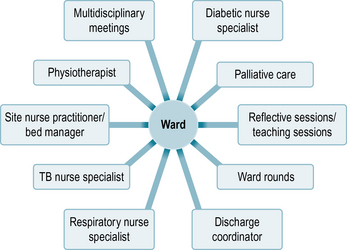
Fig 4.1 Hub and spoke model in practice if you are placed on a medical ward specialising in respiratory medicine
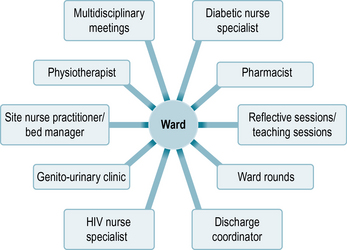
Fig 4.2 Hub and spoke model in practice if you are placed on a medical ward where patients with HIV/AIDS are cared for

When you speak with your patients, try to find out about their journey so far. How long have they been unwell, who have they seen so far and what phase of their journey are they in?
For example, a patient may be admitted to the ward with liver failure due to excess alcohol intake/addiction. So far, the patient may have encountered the following throughout the health journey:
• Drug and alccohol dependency clinic.
• Doctors including the GP, A&E doctors, consultant physicians in the out-patient department and ward departments and a psychiatrist within the drug and alcohol dependency clinic and in an acute ward stay.
This patient has spent time in clinics, wards, day care units and more acute departments.
Keeping up with the changing healthcare service
As you move through your training you will no doubt learn or hear about the seemingly constant changes in the structure, organisation and management of the healthcare system in which you are working. These changes in structure, organisation and management impact on the patient journey as they will affect the commissioning and procurement of resources for patients. Such changes are often not felt directly by staff on the frontline but they have an indirect influence on care through the formation of policy and guidance.
You may feel far removed from the policy makers and politicians who set the guidance, standards and benchmarks by which we provide care services. You may even feel that they have little or no relevance to your day-to-day life as a student nurse. But the reality is that all the care you will observe or take part in is related to a guideline, policy, standard or benchmark that has been set either locally, based on national guidance, or directly by a governing body such as the Department of Health, Care Quality Commission or Nursing and Midwifery Council.
You may find it helpful to look up the following Websites which outline the ‘High Impact Actions’ for nursing and the Commissioning for Quality and Innovation targets:
http://www.institute.nhs.uk/building_capability/general/aims (accessed July 2011).
http://www.miltonkeynes.nhs.uk/assets/_managed/editor/file/QMK/Quality%20improvements/Monitoring/UsingtheCQUINframework_1.pdf (accessed July 2011).
http://www.cqc.org.uk (accessed July 2011).
One of the competencies from the NMC leadership management and team working (NMC 2010a) incorporates the need the nurses to be able to manage the care of their patients:
across their health care journey recognising when to communicate with and refer to other professionals to deliver positive outcomes and smooth effective transition between services and, where possible, to secure their preferred place of care.
One aspect of demonstrating leadership as a nurse requires you to be politically astute and aware of the culture and context of the healthcare system that you work in.
The following Website can help you understand the journey of the NHS since 1948 and has a couple of informative videos:
http://www.nhs.uk/NHSEngland/theNHS/NHShistory (accessed July 2011).
Now look at the BBC Website to see the latest news regarding the NHS and consider how the new White Paper (Department of Health (DH) 2010a) could affect patients’ journeys in the future:
http://www.bbc.co.uk/search/nhs (accessed July 2011).
This is considered one of the most radical changes to health care since 1948. How does it affect the organisations that you are placed in?
Once you have looked at these Websites, you will understand that there may be other providers such as private health firms and social enterprises that may be involved with the patient journey and this could affect who you are communicating with and referring patients to. What is important is that you recognise that changes in the structure, organisation and management of the healthcare system will continue to occur throughout your career which you need to be aware of if you are going to lead, manage and work within teams as a nurse for the benefit of your patients.
Understanding some of the key policy documents related to your placement area will give you an insight into the culture and context of the organisation and why certain things are done in a certain way, why staff monitor or regularly audit aspects of their care and the pressures that staff are working under.
Local policy and guidance
Each care institution will have its own set of policies and guidance that staff must adhere to. These will range from operational issues, such as management of a major incident or a uniform policy, to health and safety policies and clinical guidelines. These policies or guidelines are usually produced by the department/clinician responsible or specialist in that area. They aim to translate national policy, legal frameworks and evidence-based practice into a usable document that will apply specifically to the area you are working in. It is important that you are aware of these local policies and guidelines as you will be expected to adhere to them while you are working in that area (see Box 4.1).
What to look for
 Think of policies that apply specifically to you – uniform, health and safety, fire, moving and handling.
Think of policies that apply specifically to you – uniform, health and safety, fire, moving and handling.
Think of policies or guidelines that may be associated with the clinical area you are working in – infection control, wound management, slips, trips and falls.
Think of clinical procedures that are common in the clinical area – insertion of a nasogastric tube, care of a chest drain.
National guidance and policy
Government departments, such as the Department of Health, regularly produce policies and guidance which aim to ensure that care services provided are of an equal standard across the country. As their guidance and policy are required to reach a wide range of care providers, they can often be very broad and may require a more specific local version to be created in individual institutions.
Having an understanding of current national policy and guidance around health care is essential for nurses. It provides the background to understanding why we practise health care in the way we do, what the constraints on that care are and what the government and the public feel should be care priorities. In the UK, the public is increasingly being consulted on priorities in care and this is subsequently being reflected in policy (see Box 4.2).
Box 4.2 Where to find national policies and guidance in the UK
http://www.dh.gov.uk – this is the Department of Health Website which contains all policies and guidance issued by the Department of Health, health service circulars and the Chief Nursing Officer bulletin which also contains useful information about new policy and guidance.
http://www.nice.org.uk/ – the National Institute for Health and Clinical Excellence is an independent organisation that produces clinical guidelines based on best available evidence.
http://www.institute.nhs.uk – the NHS Institute for Innovation and Improvement supports the NHS by promoting tools and news ways of working that improve care and the patient experience.
You will no doubt hear nursing staff, particularly ward managers and matrons, talking about auditing aspects of the care they are providing. This is often the method trusts will use to monitor standards of care and ensure that they are meeting the guidance, targets and benchmarks set by government policy. Some of these audit results have to be reported directly to the Health Protection Agency, for example infection control rates of MRSA and Clostridium difficile (see http://www.hpa.org.uk/infections (accessed July 2011)).
As there is a plethora of policy and guidance nationally, it is difficult to know where to start and how to determine which is the most useful for you to be aware of. To begin with, it is good to be aware of any policies that are specifically aimed at nursing care as these are the ones that are most likely to impact on your day-to-day practice (see Box 4.3).
Box 4.3 Examples of nursing policy in the UK
Essence of Care (DH 2010b)
Essence of Care is a set of benchmarks and a toolkit aimed at helping nurses get the ‘basics of care’ right. The benchmarks include: continence; communication; personal and oral hygiene; food and nutrition; pressure ulcers; privacy and dignity; record keeping; principles of self-care; safety of clients with mental health needs; and promoting the healthcare environment.
High Impact Actions for Nursing and Midwifery (Institute for Innovation and Improvement 2009)
This document contains eight high-impact actions that have the potential to improve quality, the patient experience and reduce cost in the NHS. They are to be driven by nurses and midwives. The eight high-impact actions concern: pressure ulcers; falls; nutrition; promoting normal birth; end of life care; reducing sickness absence in the NHS; improved discharge; and urinary tract infections.
The next set of policies or guidelines you might like to look for should be based on any national priorities in care (see Box 4.4). These are often issues that are very topical so if you are unsure what they may be, think back to any recent media stories that have made newspaper headlines or aspects of health care that have been discussed on television news programmes, for example dignity issues and infection control issues. Also ask your colleagues, mentor and tutors what they think the priorities in health care are at the moment and then try searching with these terms on the DH Website or other healthcare Websites.
Box 4.4 Examples of policy based on care priorities in the UK
Dignity in Care (DH 2010c)
This is a set of resources including best practice frameworks, guidance and toolkits to help organisations drive up dignity in care and can be found at: http://www.dignityincare.org.uk/ (accessed July 2011).
Saving Lives (DH 2007)
This is a toolkit for organisations to help implement the Code of Practice for Prevention and Control of Healthcare-Associated Infections which is a legal requirement for trusts. It includes care bundles and guidance to direct the care of: central and peripheral venous catheters; renal catheters; urinary catheters; reducing surgical site infections; ventilated patients; MRSA; Clostridium difficile; antimicrobial prescribing; and blood cultures.
Finally you may want to look at policies or guidelines that specifically target the clinical area you are working in (see Box 4.5). You could do this by searching healthcare Websites, such as those of the DH or National Institute for Health and Clinical Excellence (NICE), with the specialty you are working in (e.g. cardiac care, respiratory) or speak to the nurses working in your area, especially senior nurses and specialist nurses. They should be able to direct you to the most current and appropriate policies and guidelines for the clinical area. Governing bodies such as the NMC and trade unions such as the Royal College of Nursing (RCN) also often produce guidance in caring for specific groups of patients so a search of their Websites will be useful. (See the list of Websites at the end of the chapter.)
Box 4.5 Examples of specifically targeted policies/guidance in the UK
National service frameworks (NSFs)
These frameworks set out standards of care and treatment in a number of specialties and aim to ensure that, wherever patients receive care for these conditions, the service and care they receive is equitable and based on best practice. There are NSFs for older people, long-term conditions, renal, mental health, coronary heart disease, stroke, diabetes, primary care and children and maternity services. Progress towards achieving these standards is measured regularly and then standards are reviewed as necessary. They can be accessed via the DH Website.
NICE guidelines
These guidelines often target the treatment and care of a specific condition (e.g. urinary incontinence, back pain) or they may focus on the more general services needed for a particular condition (e.g. dementia). These guidelines are evidence-based and reflect cost-effectiveness of the treatments recommended. Again, they are to ensure that individuals receive the same diagnostic care and treatment wherever they receive services.
Professional guidance
As a student nurse, you are bound by some extent to the same codes of conduct and practice that registered nurses will be. Developing a working understanding of how these apply to you now will help as you progress through your training and stand you in good stead when you become a registered nurse. The Website of your governing body, the NMC in the UK, will be the best place to start. Look specifically for any guidance that applies to student nurses but also read those that concern general standards of professional behaviour and areas of care that you may be involved in such as documentation and administration of drugs (see Box 4.6).
Box 4.6 Nursing and Midwifery Council guidance in the UK
Standards for medicines management (2008b).
Guidance on professional conduct for nursing and midwifery students (2009a).
Record keeping: guidance for nurses and midwives (2009b).
Good health and good character: guidance for students, nurses and midwives (2010b).
Translating policy to practice
As you read the policies and guidance that are applicable to you and the clinical area you are placed in, in some cases it will be obvious how you can apply them to your practice. In other cases, you may be left feeling none the wiser
Consider your patient's journey
Identify a suitable patient with your mentor and then undertake the following.
Speak with one of your patients on your placement and ask them about their experiences of health care and what that healthcare journey has been like for them. Consider the following points:
1. Where are they in their journey – pre-admission, acute admission, rehabilitation, discharge, follow up, etc.?
2. How do they feel about their care?
3. Can they identify the healthcare professional involved in their care?
4. Who do they feel is leading their care?
5. What is their understanding of their goals for care and treatment?
6. Do they feel that all the professionals involved in their care communicate effectively with them?
7. When looking at patient documentation, electronically and written, are the goals of the patient's care clear?
9. What research has influenced the care they have received?
10. What national and local policies and practice guidelines have influenced their journey?
about what is expected of you or even if it applies to your practice at all. The checklist in Box 4.7 may help you to summarise what you have read and begin to see how it could influence your practice and that of those around you.
Who wrote the policy and who was it aimed at?
Is the policy a legal requirement, mandatory, statutory or contractual requirement – does it have to be done?
Is the policy or guidance based on referenced evidence-based care?
What benefits would this policy have for you and/or your patients?
Break the policy down into manageable parts, e.g. one standard or quality measure at a time.
Do nurses have a part to play in achieving each standard or quality measure? Think about nurses in other clinical areas and the community too.
What is it that nurses need to do to ensure this is achieved? Could you play a part in this?
Look to see if this is happening in your clinical area. If so, ask your mentor about it, get involved in an audit or monitoring of standards of care.
Summary
This chapter has encouraged you to think about your practice learning pathways and how these can truly reflect the journey your patients are taking. It has given you some examples of patient journeys and how these can translate into practice learning. You have been prompted to think about constant changes in the structure, organisation and management of the healthcare system in which you are working, to understand the impact on the patient experience and the need for you to keep up to date.
Department of Health. Saving lives: reducing infection, delivering clean and safe care. London: DH; 2007. Online. Available at http://www.dh.gov.uk/en/Publicationsandstatistics/Publications/PublicationsPolicyAndGuidance/DH_124265 (accessed July 2011)
Department of Health. Equity and excellence. Liberating the NHS. London: DH; 2010. Online. Available at http://www.dh.gov.uk/en/Publicationsandstatistics/Publications/PublicationsPolicyAndGuidance/DH_117353 (accessed July 2011)
Department of Health. Essence of care. London: DH; 2010. Online. Available at http://www.dh.gov.uk/en/Publicationsandstatistics/Publications/PublicationsPolicyAndGuidance/DH_119969 (accessed July 2011)
Department of Health. Dignity in care. London: DH; 2010. Online. Available at http://www.dhcarenetworks.org.uk/dignityincare/ (accessed July 2011)
Institute for Innovation and Improvement. High impact actions for nursing and midwifery. Online. Available at http://www.institute.nhs.uk/building_capability/general/aims/, 2009. (accessed July 2011)
Nursing and Midwifery Council. The code: standards of conduct, performance and ethics for nurses and midwives. London: NMC; 2008.
Nursing and Midwifery Council. Standards for medicines management. London: NMC; 2008.
Nursing and Midwifery Council. Guidance on professional conduct for nursing and midwifery students. London: NMC; 2009.
Nursing and Midwifery Council. Record keeping: guidance for nurses and midwives. London: NMC; 2009.
Nursing and Midwifery Council. Standards for pre-registration nursing education. London: NMC; 2010.
Nursing and Midwifery Council. Good health and good character: guidance for students, nurses and midwives, 2010.
Best C., Hitchings H. Day case gastrostomy placement for patients in the community. British Journal of Community Nursing. 2010;15(6):272–278.
Department of Health. The national service framework for long-term conditions. London: DH; 2005.
Department of Health. Saving lives: reducing infection, delivering clean and safe care. London: DH; 2007. Online. Available at http://www.dh.gov.uk/en/Publicationsandstatistics/Publications/PublicationsPolicyAndGuidance/DH_078134
Department of Health. Ready to go? Planning the discharge and the transfer of patients from hospital and intermediate care. London: DH; 2010.
Glasper A. Can high-impact nursing actions result in enhanced patient care? British Journal of Nursing. 2010;5(6):1056–1057.
Kempshall N. The care of patients with complex long-term conditions. British Journal of Community Nursing. 2010;15(4):181–187.
Levett-Jones T., Bourgeois S. The clinical placement. A nursing survival guide, 2nd ed. Edinburgh: Baillière Tindall; 2009.
Lawlor P. Referring patients with complex problems to community matrons. Primary Health Care. 2009;19(1):122–124.
Mellor S. Managing dysphagia in practice. Journal of Community Nursing. 2009;23(8):10–13.
O'Leary K., Thompson J., Landler M. Patterns of nurse–physician communication and agreement on the plan of care. Quality and Safety in Healthcare. 2010;19(3):195–199.
Shirley M.R. Nursing practice models for acute and critical care: an overview of care delivery models. Critical Care Nursing Clinics of North America. 2008;20(44):365–373.
Snoddon J. Case management of long-term conditions: principles and practice for nurses. Oxford: Wiley–Blackwell; 2010.
Institute for Innovation and Improvement: http://www.institute.nhs.uk.
National Institute for Health and Clinical Excellence: http://www.nice.org.uk.
Royal College of Nursing: http://www.rcn.org.uk
http://www.nmc-uk.org/Students/Good-health-and-good-character-Guidance-for-students-nurses-and-midwives/.
http://www.nmc-uk.org/Students/Guidance-for-students/.
http://www.nmc-uk.org/Documents/Guidance/NMCandYou-September-2010.PDF.