6 Assessment of risk and the medical patient
• To understand why risk assessments are important for medical patients
• To identify the risk assessments undertaken in the placement learning pathways throughout the patient journey
• To begin to understand the nursing actions taken when a risk is identified to ensure patient safety
• To understand the term ‘vulnerable adult’ and be able to identify patients who are vulnerable
• To understand safeguarding adult procedures and the use of the Mental Capacity Act in your placement area
• To understand what constitutes abuse
• To understand the needs of a patient with learning disabilities in your placement area
Introduction
Life is full of risks and we are constantly making risk assessments for ourselves without realising it. Each time you get into a car to drive, you are unconsciously making an assessment of risk: is it safe to drive to my destination, do I have the skills and knowledge to drive, will I be tired, is the weather good, do I have an alternative way of getting to my destination? Making these sorts of risk assessments for ourselves becomes a part of life that we rarely spend any time thinking about.
Patients with a medical health problem may be at risk in a number of ways, such as the risk of developing a pressure ulcer, of falling, of abuse. Part of your role as the nurse caring for a medical patient is to assess their risk and plan their care accordingly. These risks will apply in any setting the medical patient is in, so risk assessment will be an essential skill to learn wherever your placement learning experience may be.
Within your curriculum you will have a number of competencies and/or learning outcomes around risk assessment and safeguarding. This chapter aims to help you identify the essential knowledge and skills required to meet these learning outcomes and be able to identify opportunities within your medical placement to do this. The Essential Skills Clusters (Nursing and Midwifery Council (NMC) 2010a) include competencies around risk assessment and safeguarding vulnerable adults, organisational aspects of care, infection prevention and control and nutrition and fluid management.
The NMC (2010b) Domain ‘Professional Values’ is relevant to risk assessment and safeguarding. For example, the competencies include the following:
• You must understand and apply current laws relating to the care of adults and, where appropriate, children and young people. This includes safeguarding vulnerable individuals, including during end of life care.
• You must practise in a holistic, non-judgemental, caring and sensitive manner that supports social inclusion and recognises and respects diversity and the beliefs, rights and wishes of individuals of all ages, groups and communities. Where necessary, you must challenge inequality, discrimination or exclusion from access to care.
• You must support and promote the health, wellbeing, comfort, dignity and rights of individuals, groups, communities and populations whose lives are affected by transition, disability, mental capacity, ill health, distress, disease, ageing or death. You must understand how these can affect the care and health promotion of people from different communities.
There are also aspects of the domain ‘nursing practice and decision making’ that apply to risk assessment and safeguarding. For example, the competencies include the following:
• You must work closely with individuals, groups and carers, using a range of skills to carry out comprehensive, systematic and holistic assessments. These must take into account current and previous physical, social, cultural, psychological, spiritual, genetic and environmental factors that may be relevant to the individual and their families.
• You must know the limitations and known hazards in the use of a range of technical nursing skills, activities, interventions, treatments, medical devices and equipment. This must include safe application and evaluation of the outcome in a variety of care settings, including complex, technical, diverse environments, to provide effective person-centred care for people of all ages and backgrounds. Interventions will include safe medicines management, wound management, pain relief and infection prevention and control. You must report any concerns through appropriate channels and modify the plan of care to maintain safe practice.
• You must know when a person of any age is at risk and in a vulnerable situation in any environment and in need of extra support and protection. You must also act to safeguard them against abuse of any kind.
What is risk assessment?
Risk assessments are a way of identifying potential problems your patient may have so that actions can be put into place to prevent these risks occurring. For example, if you identify that your patient is at risk of falls, you can put into place a plan of care to reduce their risk of falling.

Speak to your mentor and find out which risk assessments are carried out within your placement learning experience on a regular basis. If you can get copies of these, it is a good idea to take them away with you and familiarise yourself with them.
Were you surprised at the number of risk assessments that are carried out?
Now find out when and how often these assessments are carried out. Are they carried out on all patients or are there criteria to decide who gets the risk assessment? If so, find out what these criteria are.
It is also worth asking whether the risk assessment is locally driven or a nationally driven assessment. For example, is it linked to national best practice guidelines such as those developed by the National Institute for Health and Clinical Excellence: http://www.nice.org.uk/ (accessed July 2011)?
Most of the risk assessments you will have found will be standardised instruments that have been locally or nationally validated. The validity (that it measures what it sets out to measure) and reliability (that it consistently measures what it sets out to measure) of a tool is important as it helps you to know that the results of the risk assessment can be relied upon.
If you are not sure whether the risk assessment tools you are using on your medical placement have been validated, try searching for the tool on the Internet.
Enter the name of the tool into a search engine and see if any author names or articles are in the results. These should be articles published in peer review journals that describe how the tool was developed and how it was validated.
If you cannot find the tool you are using, speak to your mentor as it may be a locally developed tool which has been validated locally and not published.
Examples of risk assessment tools
The following are examples of the kind of risk assessments you may find and some of the validated tools that are in use:
• Falls risk assessment, e.g. Morse (1997), STRATiFY (Oliver et al 1998).
• Bed rail assessment, e.g. National Patient Safety Agency (NPSA; 2007a) tools.
• Pressure ulcer risk assessment, e.g. Waterlow (2005), Norton et al (1962).
• Malnutrition risk assessment, e.g. Malnutrition Universal Screening Tool (British Association for Parenteral and Enteral Nutrition (BAPEN) 2008).
• Infection control, e.g. Visual Infusion Phlebitis score (Jackson 1998) to detect signs of phlebitis.
• Early warning scores to detect patient deterioration, e.g. Modified Early Warning score (Stenhouse et al 1999).
Different risk assessment tools will apply at different stages of your patients’ journey. Some of them will be common across all stages of the journey (Box 6.1).
Box 6.1 Examples of risk assessment across the patient journey
Some risk assessments are tied to statutes, for example manual handling. You should have received training in moving and handling patients before you commenced your clinical placement, and some of you may have found that you were not able to commence your placement until this was completed. Check with your university to find out their requirements and provision of manual handling training.
How are risk assessment tools developed?
The assessments are often based on evidence-based factors that contribute towards a certain risk. These factors are then given a numerical value which will give a total value at the end of the assessment and this helps you to decide the level of risk your patient is at.
It is important that you understand why certain factors put some people at an increased risk. Spending some time looking at a tool and working out how risk factors are determined is a useful exercise. Look at the Waterlow score (Waterlow 2005) in Figure 6.1 for assessing risk of developing pressure ulcers. Think about each category of risk and why such factors contribute to the development of pressure ulcers – you will need to think back to anatomy and physiology. Table 6.1 describes what each of the categories for risk within the Waterlow score mean.
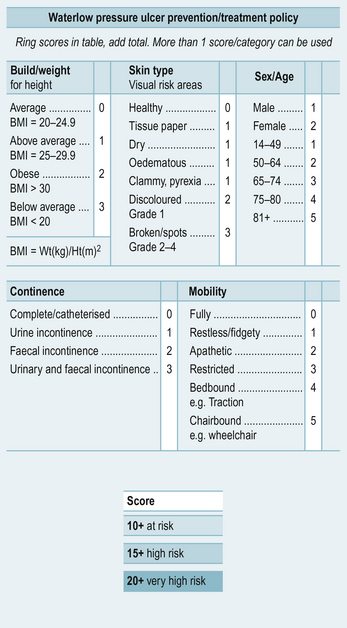
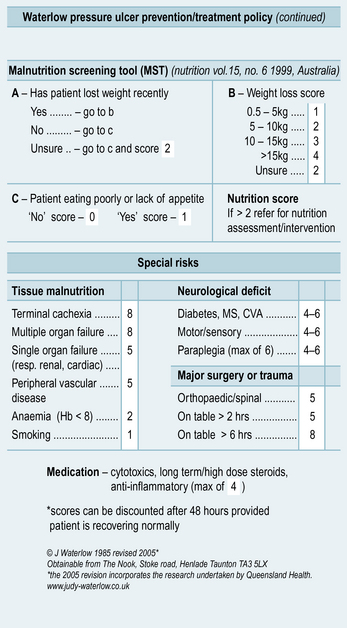
Table 6.1 The categories for risk within the Waterlow score
| Risk factor | How it contributes to pressure ulcer development |
|---|---|
| Build/weight for height | Being overweight restricts your mobility and consequently your ability to relieve the pressure on parts of your body when sitting or lying down. Being underweight reduces the subcutaneous fat that protects your bony prominences from increased pressure |
| Skin type | If skin is dry it is much more likely to crack and damage easily. Tissue paper skin is thin and more easily damaged. Skin that is stretched over oedematous areas is also thinner and more easily damaged. Oedema will also reduce the blood supply to the skin surface. Discoloration is a sign that damage has already occurred. Skin that is clammy or damp is more susceptible to friction and shearing forces |
| Sex/age | Skin loses its elasticity as it ages and a reduction in blood supply to the skin surface means that it will take longer to heal |
| Continence | Wet and soiled skin from incontinence can become easily excoriated, increasing risk of skin breakdown. It also makes the skin more susceptible to friction and shearing forces |
| Mobility | The less able a person is to move, the less able they are to relieve pressure when sitting or lying down |
| Tissue malnutrition | There are many conditions that contribute to a reduced perfusion and blood flow to tissues and reduced overall mobility of the patient. These will all increase the risk of skin breakdown and delay healing |
| Neurological deficit | A condition that results in a sensory deficit will mean the person is unable to fully feel pressure or pain and therefore will not change position to reduce pressure |
| Major surgery or trauma | The prolonged period of immobility associated with major surgery or trauma increases the risk of pressure damage |
| Medication | Medication that reduces the body's own inflammatory response will affect the skin's ability to heal |
| Nutrition | Being underweight, having significant weight loss and a poor appetite all contribute to an increased risk of acute illness and immobility and a reduced ability of the skin to heal |
But risk assessment is not just about completing a risk assessment form. You must know what actions to take depending on the results of the assessment. Many widely used forms will have guidance about how to interpret the results and the actions you need to take, but these may not always be obvious if you have not used the tools before. Again, ask your mentor about this and do some reading around the tool to help you understand its significance to your patient.
It is also important to know the limitation of the risk assessment you are carrying out. You must always use you clinical judgement as well as the risk assessment. If the tool is telling you there is no need for concern, but your clinical judgement is telling you otherwise, then always follow your judgement and take whatever action is necessary to safeguard your patient.
The popularity of risk assessment tools also changes and new evidence may show that some well used tools are not as useful as they have been. Examples of this are falls risk assessment tools. Recent evidence has shown that they are not absolutely necessary in the prevention of falls for patients in hospital and that an assessment of modified risk factors should always be carried out with or without a numerical risk assessment (NPSA 2007b).

Mrs Kalra is a 73-year-old lady who lives locally with her family who are her main carers and are very supportive. Over the last 10 days they have found it increasingly difficult to manage her daily needs. She has become weaker, is not eating and drinking so well and her mobility has decreased. She has also had some urinary incontinence on occasions. Mrs Kalra has a past medical history of osteoarthritis in her hips, which she takes regular analgesia for, and she has Alzheimer's disease. Her ability to speak English has reduced as her Alzheimer's disease has progressed. She now speaks mainly in her first language, Gujarati.
Her family called the community matron who, after assessing her, feels she should be admitted to the local intermediate care unit for intravenous fluids. She has also developed a grade 2 pressure ulcer on her sacrum as a result of her reduced mobility in the last few days.
Imagine you are the nurse admitting Mrs Kalra at the intermediate care unit. Which risk assessments would you carry out and why?
Using the Roper, Logan and Tierney (2000) model of activities of daily living (introduced in Ch. 1), identify which activities Mrs Kalra will require assistance to meet. Construct a care plan detailing the nursing actions you would take to meet each of these activities of daily living.
(See page 104 for answers.)
You may have considered that Mrs Kalra(see case history 6.1) would need a nutritional risk assessment as she is not eating and drinking well at present. As her mobility is reduced, she would require a manual handling risk assessment to determine the safest way for staff to help her mobilise, reducing the risk of injury both to Mrs Kalra and nursing staff. She may also be at risk of falls due to her confusion, dehydration and poor mobility so a falls risk assessment would be necessary. She already has a grade 2 pressure ulcer and her reduced mobility and oral intake will put her at risk of developing further pressure ulcers, so a pressure ulcer risk assessment would be required to help guide your management of her pressure ulcer risk. She is about to commence intravenous fluids, so her intravenous cannula site would require regular assessment for early detection of phlebitis or other complications.
One major consideration in your assessment and management of the risks that Mrs Kalra may face is her limited ability to understand and speak English. You will need to consider the best way to communicate with Mrs Kalra. Initially this may be with the help of a bilingual advocate or a member of her family, but on a daily basis you may need to rely heavily on visual prompts and cues. You will also need to get detailed information from her family about her usual routine, likes and dislikes as this is an important aspect of delivering person-centred care for a person with dementia.
Use this opportunity to improve your knowledge about caring for people with dementia in a hospital/intermediate care setting. The following two articles by Dewing describe some of the challenges of caring for people with dementia in an acute setting and an intermediate care setting along with suggestions about how nursing care for such patients can be improved.
The Alzheimer's Society has produced a document ‘This is me’ aimed at gaining as much information as possible about a person with dementia to ensure the care they receive is person centred. It can be accessed at:
Protecting from harm – safeguarding adults
Some risks, as described in the first part of this chapter, are known risks that we can assess and have strategies in place to prevent. Some of the other risks that make your patients vulnerable are not as obvious but can have devastating consequences.
All patients may be vulnerable despite their age, diagnosis or social situation. The experience of being unwell and adapting to a care environment for any patient is often very frightening. This, coupled with the fact that a power balance exists between health professionals and patients, means that some patients are reluctant to question the decisions made by health professionals and are even less likely to complain or raise concerns if the care they are receiving is below standard, especially if they are dependent on the health professionals caring for them to maintain their wellbeing, for example washing and dressing, toileting, helping with eating and drinking and pain control.
A vulnerable adult is defined as someone over the age of 18:
who is or may be in need of community care services by reason of mental or other disability, age or illness; and who is or may be unable to take care of him or herself, or unable to protect him or herself against significant harm or exploitation.
It is an important role of the nurse and everybody working in a healthcare environment to be aware of the kinds of abuse that patients may be suffering, or are vulnerable to, and to act in order to safeguard that person.
The NMC (2010c) states that ‘Safeguarding is part of everyday nursing and midwifery practice in whatever setting it takes place’ and that ‘you should have the skills to confidently recognise and effectively manage situations where you suspect a person in your care is at risk of harm, abuse or neglect, including poor practice’.
As a student nurse, you may feel uneasy and not so confident about raising concerns over possible abuse of vulnerable adults. If the abuse has taken place outside of the care environment you are placed in, for example in the person's own home or care home, then each local authority will have a procedure in place to report the concern.
Find out what the safeguarding adult procedures are in your placement area. Is there a policy you should be aware of? Is there a lead person to contact if you have concerns? Talk to your mentor about the support available and how you would go about raising an alert if you felt it was necessary.
Make yourself familiar with the national guidance as well – No Secrets: Guidance on Developing and Implementing Multi-agency Policies and Procedures to Protect Vulnerable Adults from Abuse – available to download from the Department of Health Website (search for ‘No Secrets’):
http://www.dh.gov.uk (accessed July 2011).
If you are concerned that practice within your placement area is poor and may constitute abuse, it is also essential that you raise your concerns appropriately. The NMC provides guidance for this in Raising and Escalating Concerns (NMC 2010d) and, specifically for students, states that you should:
– inform your mentor, tutor or lecturer immediately if you believe that you, a colleague or anyone else may be putting someone at risk of harm
– seek help immediately from an appropriately qualified professional if someone for whom you are providing care has suffered harm for any reason
– seek help from your mentor, tutor or lecturer if people indicate that they are unhappy about their care or treatment.
Go to the NMC Website and look at the safeguarding resources there:
http://www.nmc-uk.org/Nurses-and-midwives/safeguarding/ (accessed July 2011).
Watch the three short films showing safeguarding vulnerable adults from different perspectives:
 The first concerns an older man living in a care home and shows how his dignity is compromised and his needs neglected as they get him ready for breakfast.
The first concerns an older man living in a care home and shows how his dignity is compromised and his needs neglected as they get him ready for breakfast.
The second concerns a young woman attending an antenatal clinic with her husband. The midwife identifies bruising on the woman's arms but is unsure of how to deal with this as the lady does not speak English and her husband answers all questions for her.
The third concerns a young woman with a learning disability in hospital who is clearly distressed when her mother comes to visit. The mother speaks to the nurse about her concerns but is not listened to.
Spend some time reflecting on how you would respond if you were the nurse caring for these patients.
Types of abuse
There are seven broad categories of abuse:
1. Physical, e.g. slapping, kicking, punching, restraint and inappropriate use of medication (for example, to sedate a person).
2. Psychological, e.g. emotional abuse, threats of harm or abandonment, humiliation, blaming, intimidation, coercion, isolation, verbal abuse, controlling, deprivation of contact.
3. Sexual abuse, e.g. rape, sexual assault, sexual acts that have not been consented to or where the person could not consent or was pressured into consenting.
4. Financial abuse, e.g. fraud, exploitation, theft, misuse of or pressure in connection to property, benefits or possessions.
5. Neglect and acts of omission, e.g. ignoring medical or health needs, withholding adequate food, drink, medication, heating, etc., failing to provide access to health and social care services.
6. Discriminatory abuse, e.g. racism, sexism, ageism, based on disability, other forms of harassment or slurs.
7. Institutional abuse, e.g. abuse that occurs in prisons, hospitals, schools, care homes, such as restrictive routines, inappropriate, or a lack of, policy and procedures, poor management.
Abuse can occur in any setting. It may occur in the patient's own home or a day centre or other facility that they visit. It may also occur in a hospital or long-term care setting. The perpetrator of abuse can also be anyone – it may be a relative, a friend or a carer, or it could be a health professional in hospital. Therefore, you need not only to be aware of signs of abuse that could have happened before the patient was admitted, but also be alert to any situations that may arise while they in are hospital, in particular acts of omission or neglect. Examples of this type of abuse in a healthcare setting could be prescribed medications not being given, assistance not being provided in a dignified way to wash and dress, not addressing toileting needs, assistance not being given to eat and drink.
Looking at the seven types of abuse above, what signs might you look out for that would indicate abuse was taking place?
Look at the following Website from Action on Elder Abuse for some information about the signs of abuse:
http://www.elderabuse.org.uk/About%20Abuse/What_is_abuse%20define.htm (accessed July 2011).
Talk to your mentor about vulnerable adults they have looked after. How did they identify issues of abuse and how did they deal with it? Think especially about how you talk to the patient you suspect is being abused. This is a difficult topic to discuss and needs to be addressed sensitively. Your mentor may have experience of this or will know who the best person to contact is in these situations.
Mr Gray is a 56-year-old man admitted to your medical ward with dehydration. He is malnourished and cachexic. He has a history of alcohol abuse and a psychiatric history of schizophrenia. He lives alone in a one-bedroom flat.
1. Would you call Mr Gray a vulnerable adult? If so, why? What are your initial concerns about Mr Gray?While you are assessing Mr Gray and asking him about how he manages his activities of daily living, he tells you that he gives his bank card to a friend who withdraws money from his account and does his food shopping for him. He also tells you that his friend sleeps in the only bedroom of the flat and that he sleeps on the sofa in the living room.
2. Would you be concerned that he is at risk of abuse? If so, what kind of abuse? What would you do with this information?The trust lead for safeguarding adults comes to see Mr Gray and carries out a Mental Capacity Act assessment to see if he has the capacity to decide whether or not his friend should have access to his money. He finds that Mr Gray does have capacity. He is also able to contact the friend, who tells the safeguarding lead that he does do the shopping for Mr Gray and that he cooks and leaves food for Mr Gray to eat but he often doesn't eat it.
3. If Mr Gray is to be discharged, what actions do you think would be necessary to safeguard him at home?In this case you would initially be concerned that Mr Gray is being financially abused and neglected by his friend who has control over his money and his ability to get food. But as the case is looked into further, Mr Gray has the capacity to decide who has his money and buys him food and also whether or not he eats it. He is clearly a vulnerable adult though, and a referral to social services to provide him with some support at home, if he is willing to accept this, would be important.
The Mental Capacity Act
The Mental Capacity Act 2005 (DH 2005) (an Act of Parliament in the UK) provides a legal framework for acting or making decisions on the behalf of those who lack the capacity to make the decision themselves. It provides clear guidance on how to assess capacity, document it and make decisions that are in the best interests of the person concerned. As a nurse, you are likely to be involved in helping to assess the capacity of patients with regard to some of the decisions they need to make, therefore it is important that you make yourself familiar with the Act and how to apply it in your practice. The NMC Code (2008) states that:
You must be aware of the legislation regarding mental capacity, ensuring that people who lack capacity remain at the centre of decision making and are fully safeguarded.
You may find the following Website useful, as it not only explains what the Mental Capacity Act is but includes guidance and tools on assessing mental capacity:
http://www.amcat.org.uk/ (accessed July 2011).
Caring for the patient with learning disabilities
Recently in the UK there has been considerable concern about the care that people with learning disabilities receive when they are admitted to hospital with acute medical problems. The number of people with learning disabilities is set to increase over the next decade (to see the latest statistics and information regarding adults with learning disabilities in the UK, go to http://www.learningdisabilities.org.uk). This means that you are very likely to have patients who also have a learning disability on a medical placement.
Two high-profile reports identified the problems adults with learning disabilities face when they are admitted to hospital and these included not receiving acceptable standards of basic care and, in some instances, people being denied health care and treatment because they had a learning disability. You can access both of these reports online:
• Death by Indifference – published by MENCAP (2007): http://www.mencap.org.uk/node/5863 (accessed July 2011).
• Six Lives – a report of the Parliamentary and Health Service Ombudsman (2009): http://www.ombudsman.org.uk (accessed July 2011).
Your placement organisation is likely to have a local policy or strategy about caring for people with learning disabilities and may have access to an acute liaison nurse, who will be a learning disability nurse, or team based in the hospital to provide support to people with learning disabilities, their carers and staff when they are admitted to hospital. Ask your mentor about what is available in your organisation and how to access support if you need it.
There are some basic principles of care that will help you to support a patient with learning disabilities during you medical placement:
• Find out as much as you can about the person – some of this information will come from the patient, but you will need to talk to their carer or relatives to get more information.
• Find out about their usual routine at home – what they like to eat or drink, what helps them relax, what makes them anxious, etc.
• See if they have a hospital passport – an individualised document that contains all the important information you need to know about the person you are caring for.
• Always tell the person what you are doing and why.
• Think about your communication style and adjust it to meet the needs of the person you are caring for.
• Pay particular attention to ensuring that the person is eating and drinking well and having their toileting and personal care needs met.
• The person may also have a Health Action Plan – a plan detailing the actions, services and support the person needs to maintain their health. It is an individualised document and will have been produced in conjunction with the person. For more information on Health Action Plans, see Health Action Planning and Health Facilitation for People with Learning Disabilities: good practice guidance: http://www.dh.gov.uk (accessed July 2011).
• Always seek specialist advice if you are not sure – your mentor will know who to contact and how.
The following guidance from the Royal College of Nursing (RCN) will also help to increase your knowledge and confidence in caring for a person with learning disabilities:
Louise is a 36-year-old woman with severe learning disabilities. She has very little verbal communication and is only able to make sounds to express how she feels. She lives in a community home with three other people with learning disabilities and they receive 24-hour care from trained carers. She has a past medical history of epilepsy and has been admitted via the accident and emergency department to the medical admissions unit following a seizure.
1. Would you call Louise a vulnerable adult? If so, why? Do you have any initial concerns about Louise?When you are helping to wash and change Louise she is very resistant and screams continually. You stop what you are doing and wait for her mother to visit. She is calmer when her mother is present and it is easier to help her wash and dress. But she still screams every time you touch her left arm. Over the next couple of days, significant bruising appears on her left arm and an X-ray confirms that she has fractured her humerus. Louise's mother is very concerned as she was not informed by the carers at her home that Louise had fallen or had any kind of accident.
2. Are you concerned that she is at risk of abuse? If so, what kind of abuse? What would you do with this information?The lead for safeguarding adults raises a safeguarding alert about her care at home and this is subsequently investigated by an independent person. The findings of the investigation were that one of the other people with learning disabilities who shares the home with Louise had pushed her over which had resulted in the fracture, and a review of their care needs took place.Louise is a vulnerable adult and, although there were no initial concerns about her care at home, an unexplained injury should always be investigated. You would have been right to suspect she might have been being physically abused. It is important in a situation like this that an alert is raised by the trust and that it is investigated independently. Louise would stay in hospital or move to another place of safety while this takes place, not return to her home, until the investigation and any subsequent action to reduce her risk of being abused has taken place.
Summary
Assessment of risk and safeguarding adults are important aspects of a nurse's role. They will not only guide and inform the care you give, in the case of risk assessments, but will also ensure the safety and wellbeing of your patients, alerting you to their changing healthcare needs. This chapter aims to equip you with the basic knowledge you need to identify when and which risk assessments are necessary and how they consequently help to form a plan of care. As you become more experienced, risk assessment will become a natural part of your day-to-day nursing care, whichever setting you are working in. The risk assessment skills you develop throughout your medical placement will be useful to you in many different clinical settings.
Safeguarding vulnerable adults is often a difficult aspect of caring for patients with medical needs, but as you progress through your training you will develop confidence in identifying and acting upon situations where a patient may be at risk of abuse or being abused. Until you feel confident about this, do not be afraid to raise a concern even if you are not sure about it. Speak to your mentor or any of the registered nurses you are working with. They would rather you raise a concern that turns out to be nothing than ignore some information that may be crucial to the safety of your patient.
British Association for Parenteral and Enteral Nutrition. Malnutrition Universal Screening Tool. Redditch: BAPEN; 2008. Online. Available at http://www.bapen.org.uk/must_itself.html (accessed July 2011)
Department of Health. No secrets: guidance on developing and implementing multi-agency policies and procedures to protect vulnerable adults from abuse. London: Department of Health & Home Office; 2000.
Department of Health. The Mental Capacity Act. London: Office of the Public Guardian; 2005.
Jackson A. Infection control: a battle in vein infusion phlebitis. Nursing Times. 1998;94(4):68–71.
Morse J.M. Preventing patient falls, first ed. Thousand Oaks, California: Sage; 1997.
Nursing and Midwifery Council. The code: standards of conduct, performance and ethics for nurses and midwives. London: NMC; 2008.
Nursing and Midwifery Council. Essential skills clusters. London: NMC; 2010.
Nursing and Midwifery Council. Standards for pre-registration nursing education. London: NMC; 2010.
Nursing and Midwifery Council. Safeguarding adults. London: NMC; 2010. Online. Available at http://www.nmc-uk.org/Nurses-and-midwives/safeguarding/ (accessed July 2011)
Nursing and Midwifery Council. Raising and escalating concerns. Guidance for nurses and midwives. London: NMC; 2010.
National Patient Safety Agency. Resources for reviewing or developing a bed rail policy. London: NPSA; 2007.
National Patient Safety Agency. Slips, trips and falls in hospital: the third report from the patient safety observatory. London: NPSA; 2007.
Norton D., McLaren R., Exton-Smith A.N. An investigation of geriatric nursing problems in hospital. London: National Corporation for the Care of Old People; 1962.
Oliver D., Britton M., Seed P., et al. A 6 point risk score predicted which elderly patients would fall in hospital. British Medical Journal. 1998;315:1049–1053.
Roper N., Logan W., Tierney A. The Roper–Logan–Tierney model of nursing. Edinburgh: Churchill Livingstone; 2000.
Stenhouse C., Coates S., Tivey M., et al. Prospective evaluation of a modified Early Warning Score to aid earlier detection of patients developing critical illness on a general surgical ward. British Journal of Anaesthesia. 1999;84:663.
Waterlow J. Pressure ulcer risk assessment and prevention, 2005. Online. Available at http://www.judy-waterlow.co.uk/index.htm
Brooker C., Waugh A. Foundations of nursing practice. Edinburgh: Mosby; 2007.
Fyson R. Independence and learning disabilities: why we must also recognise vulnerability. Journal of Integrated Care. 2009;17(1):3–8.
Gates B. Learning disabilities: toward inclusion, 4th ed. Edinburgh: Churchill Livingstone; 2004.
Hewitt D. Not just in the Mental Capacity Act: using the law to protect vulnerable adults. Journal of Adult Protection. 2009;11(2):25–31.
Kydd A., Duff T., Raymond Duffy F.J. Care and wellbeing of older people. Devon: Reflect Press; 2009.
Morgan A. Review of safeguarding practice points towards a new culture of transparency. Nursing Older People. 2010;22(1):6–7.
The Alzheimer's Society Website has a section dedicated to researchers and professionals which contains many excellent resources including the brain tour, an interactive video describing how the different types of dementia affect the brain: http://www.alzheimers.org.uk (accessed July 2011)
MENCAP, a leading learning disability charity, has a section for professionals with good resources to read and video clips to watch http://www.mencap.org.uk/ (accessed July 2011) this website contains information on assessing mental capacity including tools to use: http://www.amcat.org.uk/ (last accessed 16.05.11.)
European Pressure Ulcer Advisory Panel http://www.epuap.org (accessed July 2011)
Answer
Case history 6.1
Mrs Kalra may need assistance with the following activities of living:
The following are examples of care plans you may have considered for Mrs Kalra:
Problem: Mrs Kalra has limited English which makes it difficult for her to communicate her needs and to fully understand the goals for her treatment. Her ability to communicate may also be affected by her Alzheimer's disease.
Goal: To ensure that Mrs Kalra is able to communicate her needs and understand her treatment as far as possible.
| Nursing action | Rationale |
|---|---|
| Ensure a bilingual advocate is available at the first assessment and as frequently as possible afterwards | To establish a baseline of what Mrs Kalra is able to understand about her reason for admission, problems and treatment plan To enable Mrs K to discuss her condition confidentially and to ensure that she is fully informed |
| Spend time finding out as much as possible about how Mrs Kalra usually communicates and complete a document such as ‘This is Me’ (www.alzheimers.org.uk), e.g. how she asks for the toilet, a drink, something to eat, how she expresses herself when in pain, upset, angry | To ensure that the care provided to Mrs Kalra is person centred and that staff are able to communicate with her and understand her needs |
| Ask the family to translate basic words, e.g. drink, pain, I need the toilet, if Mrs Kalra would understand these | To enhance communication |
| Allow a family member to stay with Mrs Kalra to reduce her anxiety if they wish to do so | To reduce Mrs Kalra's anxiety levels |
| Use non-verbal communication to enhance understanding, e.g. pointing to things, gestures | To promote and enhance communication |
| Ensure time is spent attempting to communicate with Mrs Kalra while her other care needs are being met, e.g. when helping her to wash and dress, at mealtimes, when giving medication | To enable staff to build a rapport with Mrs Kalra which will make understanding her needs and communicating with her much easier |
| Introduce yourself to Mrs Kalra each time you see her and be prepared to repeat information as many times as necessary | To compensate for Mrs Kalra's memory problems |
Problem: Mrs Kalra is not eating or drinking adequately due to her condition.
Goal: For Mrs Kalra to have adequate fluid and dietary intake.
| Nursing action | Rationale |
|---|---|
| Ensure a malnutrition risk assessment is undertaken in the first 24 hours | To determine Mrs Kalra's nutritional status |
| Maintain strict food and fluid balance monitoring With the help of an advocate, inform Mrs Kalra about this and provide Mrs Kalra with rationale Inform the nurse in charge or doctor if Mrs Kalra's diet or fluid intake are below the normal limits |
To ensure that Mrs Kalra receives adequate fluids and nutrition To prevent complications of dehydration To ensure that there is effective communication within the multidisciplinary team |
| Find out what kinds of foods Mrs Kalra would eat at home and what time she would usually eat Discuss with dietician/kitchen about providing such foods |
To provide food and drink which is familiar to Mrs Kalra at familiar times to encourage her oral intake |
| Encourage Mrs Kalra to drink nutritional supplements in a flavour she likes | High-calorie/high-protein supplements aid recovery and wound healing |
| Monitor and document Mrs Kalra's observations of her vital signs, including weight | To detect any deterioration/improvement |
| Administer intravenous therapy as prescribed and ensure that the cannula site is inspected regularly for signs of phlebitis | To reduce the risk of cannula-associated infection/complications |
Problem: Mrs Kalra has a pressure ulcer.
Goal: To heal the wound and to prevent infection.
| Nursing action | Rationale |
|---|---|
| Assess the wound every time it is dressed – size, depth, width and length Document deterioration/improvement on the wound assessment and review chart |
To assess deterioration or improvement |
| If wound shows any signs of infection – redness, increased pain, heat, swelling, increased exudates, odour – send wound swab for culture and sensitivity | To detect infection |
| Aseptically dress the wound with a hydrocolloid dressing | To prevent infection |
| Consider analgesia prior to dressing changes | To keep Mrs Kalra as comfortable as possible |
| Weekly Waterlow score | To determine risk |
| Provide pressure redistribution mattress and cushion | To promote comfort, healing and prevent deterioration |
| Encourage Mrs Kalra to mobilise – refer to physiotherapist (see mobility care plan) | See mobility care plan |
| Ensure Mrs Kalra has a high-protein diet (see eating and drinking care plan) | A high-protein diet will enhance wound healing |
| Liaise with the tissue viability/wound nurse specialist | For specialist advice and best practice |
Problem: Mrs Kalra has pain in her hips and from the wound site.
| Nursing action | Rationale |
|---|---|
| Using a pain assessment tool that is appropriate for a non-English speaking patient and also a person with dementia, assess severity of Mrs Kalra's pain Observe for behavioural changes and non-verbal cues that might indicate she is in pain |
To determine the type, intensity and site of the pain using a tool that Mrs Kalra can understand if possible |
| Administer prescribed analgesia | To reduce the pain |
| Reassess pain to determine the effectiveness of the analgesia | To assess the effectiveness of the analgesia given |
| Inform the doctor if Mrs Kalra's pain relief is inadequate, referring to the analgesic ladder | For analgesia to be increased promptly |
| Assist Mrs Kalra to manage her pain by careful positioning and other non-pharmacological techniques | To increase comfort and reduce pain using culturally appropriate pain relief methods to complement the analgesia |
| Consider timing the analgesia for wound dressings and physiotherapy | To ensure full benefit of physiotherapy and to ensure comfort during therapy and wound dressings |
Problem: Mrs Kalra has reduced mobility due to weakness and pain.
Goal: To maximise Mrs Kalra's mobility.
| Nursing action | Rationale |
|---|---|
| Refer to the physiotherapist and liaise to ensure that Mrs Kalra mobilises safely | For full assessment of mobility problems and provision of walking aids if necessary |
| Using a bilingual advocate and other communication strategies identified, explain why it is important to mobilise and encourage her to do so as often as she can, e.g. to the toilet | To increase likelihood of Mrs Kalra wanting to mobilise and reduce the chances of her losing the ability to walk |
| Administer analgesia prior to physiotherapy | To control pain and maximise ability to walk |
| Complete a falls risk assessment | To address any modifiable risk factors that may contribute to falling |
| Minimise friction on movement | To reduce the risk of skin breakdown |
| Ensure that Mrs Kalra does not sit out of bed for more than an hour at a time to prevent further pressure damage | To reduce the risk of further pressure damage |
Problem: Mrs Kalra has recently become incontinent of urine.
Goal: To keep Mrs Kalra clean and dry, maintain her dignity and to determine cause.
| Nursing action | Rationale |
|---|---|
| Obtain mid-stream specimen of urine for ward-based urinalysis and to send to the lab for culture and sensitivity | To determine if infection is present and to determine antibiotic sensitivity |
| If possible, using a bilingual advocate, ask Mrs Kalra about her urinary symptoms Alternatively, her family may be able to provide information |
Ongoing treatment and investigation of incontinence will depend on type of incontinence |
| Complete a bladder diary and a fluid chart for a minimum of 3 days to establish her pattern of incontinence | To assist in creating a regular toileting regime to help maintain continence and ensure adequate fluid intake |
| Ensure her bed is placed close to the toilet and her walking aid and call bell are at hand | To enable Mrs Kalra to use the toilet in the bathroom in a timely manner |
| Offer assistance and prompting to use the toilet at regular intervals, according to the bladder diary Mrs Kalra may need to be shown where the toilet is on a regular basis as a result of her memory problems |
To provide a reminder to Mrs Kalra to use the toilet and an opportunity for her to establish a regular voiding routine |
| Provide an incontinence pad and fixation pants if necessary | For her dignity to be maintained |
| Help Mrs Kalra to maintain her hygiene needs | To ensure Mrs Kalra is comfortable, for her dignity to be maintained and reduce risk of skin breakdown |