Chapter 2 The user patient journey
KEY POINTS
INTRODUCTION
Society as a whole has little understanding of Musculoskeletal Conditions (MSC) and the consequences to the individual. This can have a significant ‘knock on’ effect to the individual with joint disease particularly, as MSC may cause individuals to stop working, contributing to high levels of claims for incapacity benefit, depression and poor self esteem (Department of Health 2006). People with MSC are the second highest group claiming incapacity benefit (which, for new claimants since October 2008, is now termed Employment and Support Allowance).
For individuals with MSC (e.g. osteoarthritis, rheumatoid arthritis and back pain) the consequences of their disease, both to the individual and society, are immense (Department of Health 2006). Many individuals fail to seek medical advice despite having significant pain and disability, believing there is “nothing that can be done”. This presents challenges when encouraging people to seek medical care as they may be dissuaded by public opinion and have little encouragement from family and friends to do so (Department of Health, 2006, Oliver 2007). Recent patient surveys have identified poor knowledge and support for those with MSC in the workplace and limited educational or financial incentives for support in these areas (The National Rheumatoid Arthritis Society 2004, 2006, 2007).
This chapter will briefly outline an example of patient journeys from a mapping project exploring patient experiences in rheumatoid arthritis (RA), discuss some of the issues related to these and the challenges individuals face in negotiating their healthcare needs.
THE USER-PATIENT JOURNEY – MAPPING PROJECT
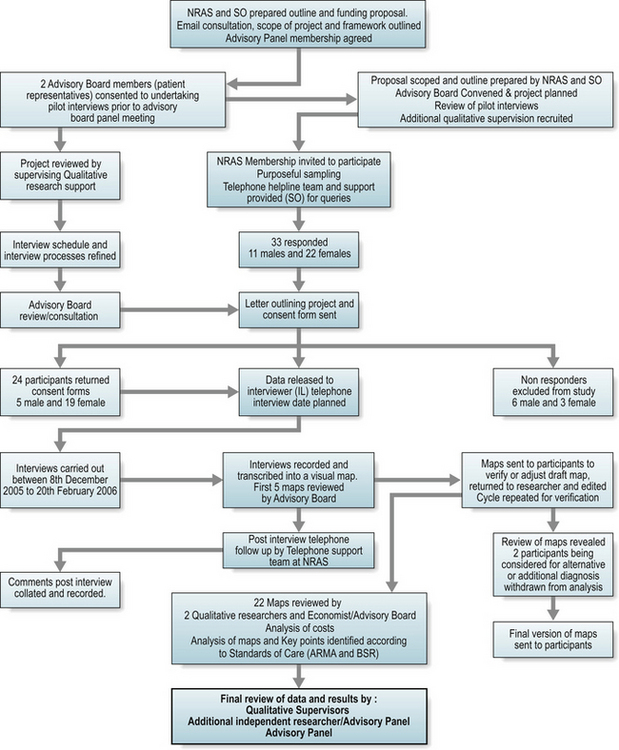
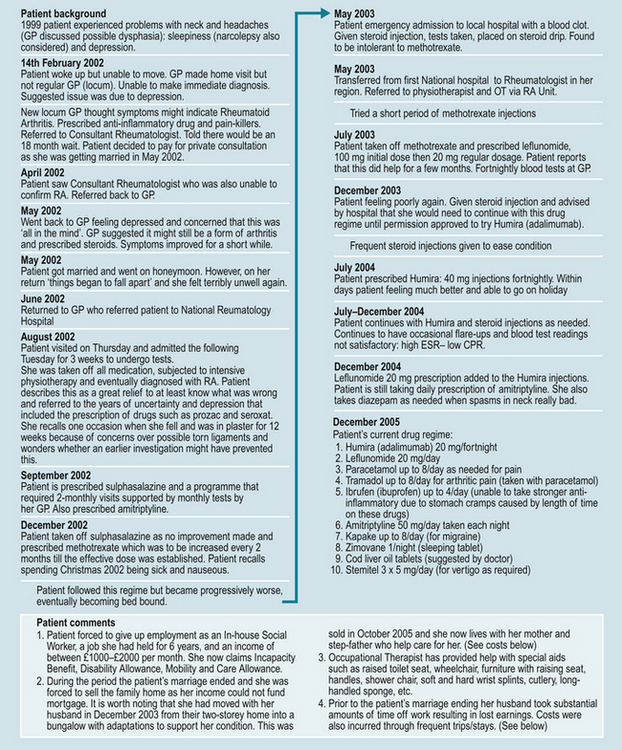
A mapping project explored the journeys of patients with early sero-positive RA. Participants were grouped into three disease duration categories ( < 1 year; 1–2 years; and > 2–3.5 years from diagnosis). The mapping project used qualitative and process mapping principles used in industry but increasingly applied to healthcare settings. Twenty-two individual patient pathways were mapped retrospectively to explore the user-patient journey and attribute direct and indirect costs to variances in care (Fig. 2.1). An example of one participant map is shown in Figure 2.2. Wide variances in many aspects of care were identified, including access to specialist services, adherence to National Institute of Clinical Excellence (NICE) guidance, support to stay in work and importantly, regular, patient-focussed support to enable active self management (such as telephone advice line services).
The mapping project demonstrated that indirect costs to the individual were high and borne silently (e.g. job losses). Seven of the 22 participants took early retirement or lost jobs directly due to the RA within the study period (Oliver & Bosworth 2006). These findings are borne out in other observational and quantitative research (Bone and Joint Decade 2005, Hulsemann et al 2005, Woolf et al 2003, 2004).
An additional burden is the time spent waiting to be seen by a consultant. For conditions, such as RA, early referral is essential to improve long-term outcomes. Yet, in the mapping project seven of the 11 participants seen rapidly, i.e. within 12 weeks of symptom onset, were seen as a result of private referral. The evidence collated from the mapping project is supported by other patient stories, such as those on seen on www.healthtalkonline.org, which is a registered charity describing a range of MSCs and individuals’ experiences. There are many patient stories outlined according to disease duration.
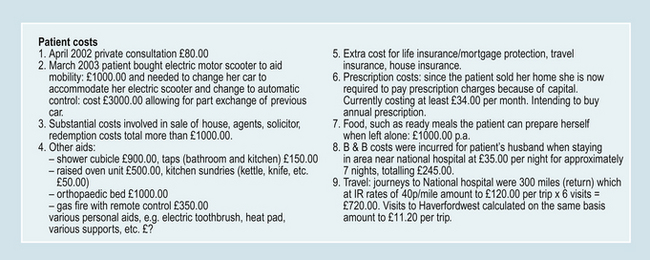
One UK study identified average annual direct costs of RA to be £3980 (Cooper et al 2002). Higher costs were associated with those who were either younger, had longer disease duration or more severe disease. A younger group is more likely to be in full-time employment and thus, additional costs relate to loss of work, extended sick leave or reduction in work hours (Merkesdal et al 2005). For example, over a three year period, delays in referral or receiving a definitive diagnosis or treatment for this group identified significant costs. Personal costs for three individuals in this project averaged £1990.27. Some of the variances in treatment costs are outlined in Table 2.1.
Table 2.1 Variances in treatment and personal costs
| BIOLOGIC PARTICIPANTS | TOTAL COST TO HEALTH PROVIDER | TOTAL COST TO PATIENT |
|---|---|---|
| Patient number (disease duration). | ||
| 002 (2–3.6 yrs) | £30,836.21 | £3675.47 |
| 005 (1–2 yrs) | £1941.03 | £2150.70 |
| 007 ( < 1 yr) | £2071.78 | £3135.42 |
| 010 (2–3.6 yrs) | £21,738.55 | £11,097.00 |
| 016 (2–3.6yrs) | £24,084.21 | £8382.33 |
| 023 (2–3.6yrs) | £10,975.30 | £413.00 |
| Grand Total | £91,647.08 | £28,853.92 |
| DMARD PARTICIPANTS* | TOTAL COST TO HEALTH PROVIDER | TOTAL COST TO PATIENT |
|---|---|---|
| Patient number(disease duration). | ||
| 004 ( < 1 yr) | £304.10 | £514.00 |
| 007 ( < 1 yr) | £2071.78 | £31135.42 |
| 009 (2–3.6 yrs) | £3346.32 | £444.94 |
| 011 ( < 1 yr) | £1218.56 | £11.00 |
| 018 (2–3.6 yrs) | £727.60 | £348.50 |
| 019 (1–2 yrs) | £10,034.56 | £2937.60 |
| Grand Total | £17,702.92 | £7391.46 |
(time from diagnosis)
* DMARD = Disease Modifying Anti-Rheumatic Drug
Receiving a diagnosis of a long-term condition, such as RA, is a significant life event. The social and psychological impact to the individual varies (Fitzpatrick et al 1988, Oliver & Ryan 2004). Initially, this may be because those receiving the diagnosis are unaware or unable to accept the diagnosis or that they have their own specific health beliefs or coping strategies that have an impact on their perceptions of the diagnosis and the underlying symptoms they are experiencing. Importantly however, evidence suggests that the spectrum of patient need, routes to treatment, advice and support vary dramatically (Bone and Joint Decade 2005). Indeed the various patient journeys can, as a result, be confusing and complex to map (Fig. 2.3).
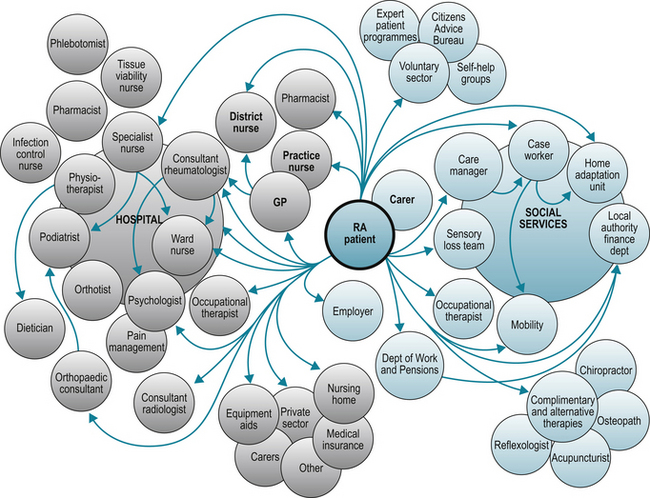
One participant (005) stated “At first the GP very helpful but I was not diagnosed at this time. The second GP good but not particularly clued up on RA and saw this as an old age disease and had no knowledge of medications being prescribed. My current GP has a specialist interest in RA which is wonderful”. For the individual, their knowledge and understanding of their condition develops over time. In some circumstances knowledge is gained from interactions with healthcare professionals (Oliver 2004). For others, the general illness experiences learnt through times of exacerbations or temporary remission, form their views and abilities on personal self management strategies (Corben & Rosen, 2005, Department of Health 2001, 2005). The reality is that people with long-term conditions manage much of their care themselves at home with their families and interact with their healthcare team for a few hours per year (Department of Health 2005) (Fig. 2.4).
Some individuals resolved their problems and needs themselves particularly if they were adequately informed of the benefits of the multi-professional team. One participant (009) had to “push hard” for access to a physiotherapist when she wanted advice on walking aids. The same participant asked for splints but ultimately had to purchase them herself. When the issue was raised with the consultant they were advised that the purchased splints “seemed to be doing the trick”.
Negotiating healthcare services and accessing the support, information and treatment required can be a challenge. These challenges may be as a result of their point of contact when they receive a diagnosis in a busy clinic environment that is alien to them. This experience is filled with many complex, and sometimes intimidating processes, that are a mystery to those lacking knowledge of healthcare systems. Over time, for most, these experiences should become less intimidating and the threats and challenges of the condition more readily understood and managed.
Participant (024) stated that he “had nothing but praise for the way he has been looked after by all the health professionals and the health service”. One participant (021) has subsequently moved from her first hospital but had a less satisfactory experience. The first time she was aware of her diagnosis was when the consultant took her to the RA nurse. As he handed the file to the nurse he told the nurse that the patient had RA. This was the first time it was mentioned.
There are numerous factors that affect the individual’s ability to comprehend, retain or accept the information that is provided at the time of diagnosis (Hill 2006). In addition, there are complex issues that affect the initial consultation and information giving process. Some of these include knowledge of the disease prior to seeking a diagnosis, the level of stress and pain experienced at the time of diagnosis, prior health issues, manner of communication at the time of diagnosis, personal health beliefs and the individual’s coping styles.
One participant (017) outlined how they were bombarded with information about the condition, drugs, physiotherapy etc as part of a drug trial..… “but very little of this contained advice on what she would experience or how to manage the pain on a day to day basis other than with the use of painkillers”.
Education and information giving are not a one stop package but an ongoing part of care. Newly diagnosed individuals may not fully recognise this need in the early phases of the disease (Luqmani et al 2006). The variations in individual needs continue throughout their illness pathway and healthcare professionals (HCPs) need to be continually mindful of opportunities to provide information giving, education and support as and when the individual appears responsive, or requests additional information. HCPs should focus not only on the medical aspects of care but also the social and psychological consequences of disease (Arthritis & Musculoskeletal Alliance 2004, Luqmani et al 2006).
HCPs aim to encourage and support the individual from the first point of contact throughout their healthcare journey, and encourage them to know they are entitled to be an active participant in their treatment choices. At the same time, HCPs need to be mindful of those who are unable or do not wish to make informed decisions about their care. In the changing healthcare system these individuals will need to be considered and appropriate ‘safety nets’ be in place to ensure they still receive the optimum in care.
FROM NEWLY DIAGNOSED TO ACHIEVING MASTERY IN EMPOWERMENT
It can be seen from the mapping projects that individuals retrospectively understood more about their care and what they should have received. However, the consequences of not having the appropriate management at the right time were significant to the individual. Patient empowerment is high on the healthcare agenda and this should enable individuals to be more informed about their care.
The question is, ‘what is empowerment and how do individuals achieve mastery?’ Empowerment is defined as: ‘To give ability to; enable or permit’. This definition outlines the need to enable or permit patients to take control and this means HCPs must play a key role in providing the help to develop strategies and the right level of support at the right time to facilitate ‘empowerment’. If the individual develops effective self-management strategies, their abilities and self-efficacy can be negatively affected if principles fail to be endorsed in the healthcare setting.
The natural course of the disease is variable and an individual’s disease path varies dependent upon the actual disease and severity, as well as contributing factors such as:
Each of the above aspects can present at different times in the individual’s journey. HCPs need to be aware of and ready to provide the appropriate support and guidance that can enable the individual to work their way through these challenges or changes that present. For the individual, recognising their ability to overcome some of these challenges can build their self-esteem and perceptions of self-efficacy.
The relationship between patients and HCPs builds over time and illness experiences, yet the first and specific challenge in the early days of this therapeutic relationship is at the time of diagnosis (Oliver & Ryan 2004). HCPs are aware of the importance of information giving and have to consider issues related to informed consent to treatment. Some individuals will wish to have all the information they can to aid their ability to understand and cope with their newly acquired diagnosis, whilst others need time to adjust and come to terms with the diagnosis or may simply fail to accept the initial diagnosis.
The HCP’s expertise is in rapidly assessing the individual and their specific needs at first point of contact and defining how best to support them. However, it still has to be accepted that treatment will need to be started early in the disease process if optimal patient outcomes are to be achieved and this can be particularly difficult for patients who have always had a strong antipathy to taking drugs.
Individuals with RA are likely to have a wide spectrum of needs and meet a wide range of practitioners throughout the life of their disease. They will receive different aspects of care across a wide range of healthcare settings (Fig. 2.3). Yet it is clear that currently, knowledge is poor about how best to provide support and appropriate care for those with RA outside the specialist field of practice (Frank & Chamberlain 2001, Memel & Kirwan 1999, Woolf et al 2003). Individuals who have become adept at negotiating their healthcare needs in specialist services can experience barriers and frustrations when they are perhaps more informed about the management of their disease than for example, their own GP.
Individuals first presenting with joint symptoms in primary care receive widely disparate levels of advice and support. Some receive optimum care and are rapidly referred to specialist services for a diagnosis. Others experience a delay of several months before gaining the same level of management (Oliver & Bosworth 2006, Sanders et al 2004). The mapping project demonstrated that 16 out of the 22 participants received treatment with a disease modifying drug (e.g. methotrexate) within 6 months of first presentation. For those eligible for a biologic therapy (e.g. anti-TNFα inhibitors – adalimumab, etanercept or infliximab), half experienced delays before accessing treatment (ranging from 2–10 months).
Over time, many individuals manage on a day to day basis in their community with the support of their families and local services. Individuals learn to manage their pain and cope with the disability. Individuals who use emotion-focussed coping strategies may end up in a spiral of repeated visits to their doctor and ‘learned helplessness’ (Ryan et al 2003). The aim of management should be to encourage positive coping styles and self management principles and, hopefully, prevent individuals developing negative health beliefs or coping styles.
GUIDELINES AND STANDARDS
HCPs and patients need a clear framework for practice that will inform and guide them on acceptable standards of care for those with musculoskeletal conditions. Some guidelines have been written with a very strong patient focus under the auspices of patient and professional organisations (Arthritis and Musculoskeletal Alliance 2004, Luqmani et al 2006) and health organisations (National Institute of Clinical Excellence, 2009). Guidelines and standards should encourage individuals with a MSC to develop strategies that can enhance self management and enable them to cascade their own knowledge and expertise of their disease to others. However, such standards and guidelines alone do not ensure equity of access. If we are to encourage individuals to be active participants in their healthcare we need to ensure that information and advice is available at all points of access to health care (Department of Health 2006, Hammond & Badcock 2002). The Arthritis and Musculoskeletal Alliance (ARMA) standards of care provide a reference point for all those providing care, in all healthcare settings and also enable the individual to know what they should expect as they negotiate their complex journey through healthcare.
Patient organisations and volunteer networks can also be a powerful and effective resource in supporting traditional healthcare support. Examples of effective projects include those run by the National Rheumatoid Arthritis Society Volunteer Network and the Arthritis Care self management courses.
CONTINUITY OF CARE
Community care is often the first port of call for most individuals when they are ill. Individuals with a chronic disease may experience various ‘health crises’. The problem for them is that many of these crises are not perceived as life threatening and in the current pace of healthcare, individuals with a chronic disease can feel very isolated. Community practitioners at all points in the patient’s journey must take responsibility to ensure that they are informed about how to access care for the individual whatever their condition. The ARMA standards of care provide a clear framework for practice not only for the practitioners but also, most importantly, provide information and a rationale for individuals about the care they should be able to expect to receive. At times, there are also unique problems in gaining access to care, as identified by this patient with RA: “My nurse specialist is fantastic and I know I can rely on her to help me but her ever increasing workload means that it is becoming more difficult to get an appointment” (a quote from a patient who participated in a survey exploring implementation of ARMA Standards of Care).
Most individuals will have some experience of being cared for by a nurse or practitioner. These memories may relate to a time as an inpatient receiving day to day care by ward nurses or in outpatient clinics discussing issues such as how to manage pain or receiving information about new medications with a specialist nurse. Experience may equally come from assessment of physical ability by a physiotherapist or discussing the need for splints with an occupational therapist to the on-going care provided by the community teams visiting individuals’ own homes. Perceptions and memories of prior aspects of care can alter over time and subsequent illness experiences along the healthcare journey. Such memories are important factors when individuals’ are trying to evaluate current experiences or make sense of what to expect in their care and access to services.
Evidence has demonstrated the importance of providing guidance and support to enable individuals with a chronic disease to be informed about their disease, treatments and ultimately how to have an active role in their disease management (Hill & Bird 2003, Homer 2005). People presenting with joint pain are frequently unaware of the standards they should expect, leaving them vulnerable to sub-optimal care.
CONCLUSION – THE USER PATIENT JOURNEY
In this chapter it has only been possible to outline a few key issues in relation to the NRAS mapping project and the importance of the support that individuals need from their HCPs. Understanding the individual’s experience of negotiating their pathways through healthcare has recently become an area of intense interest. This is partly due to national and international initiatives to improve service delivery based upon understanding and improving patient flows through the system, using manufacturing principles (often referred to as lean thinking). This has two objectives, firstly to put the patient at the centre of thinking and planning, and secondly, to explore hierarchical and traditional boundaries that prevent high quality care being delivered, which in many cases increase costs and potential bottlenecks (The National Health Service Modernisation Agency 2005).
The process of mapping pathways can also help to identify new ways of delivering services, in particular service redesign. The variances in costs in patient journeys through healthcare are increasingly being scrutinised. Some costs were identified in the mapping project, providing a ‘snapshot’ of not only health care costs but also, importantly, to the individual. Such individual and societal costs are higher than the costs to healthcare.
IMPROVING THE PATIENT JOURNEY
Musculoskeletal care should no longer be considered a second class specialism in healthcare provision. The consequences to the individual and to society are too high. The ARMA standards of care provide a tool for those with arthritis and health care providers to work with others and ensure they have the expertise to treat, guide and support patients appropriately, recognising the central role the patient has a right to play in their own care. In recent years the role of the nurse and allied healthcare professionals has been recognised as pivotal to providing comprehensive healthcare support to individuals.
In this age of patient choice, risk management and informed decision-making, there are opportunities and threats to the therapeutic relationship that individuals with musculoskeletal conditions should have with their HCPs. Although these principles may be admirable and desirable concepts, the mapping project demonstrates that it can be difficult for individuals to make informed choices through their healthcare journey, particularly for those newly diagnosed who have inadequate knowledge to make choices and limited opportunity to negotiate their healthcare needs.
HCPs and individuals with musculoskeletal conditions need to work together to ensure that patient needs are recognised and high standards of care implemented nationally so that individuals receive the care they deserve.
ACKNOWLEDGEMENT
The authors would also like to thank the Parkinson’s Society in Cornwall and Sue Thomas, Nurse Advisor at the Royal College of Nurses. Their work and shared experiences from a mapping project informed the NRAS project. The authors also wish to recognise and thank the full NRAS mapping project advisory board for their advice and support in overseeing the project.
 Consider the potential personal cost implication of having RA (these are often called indirect costs). Include personal costs such as work, adaptations/aids, and mobility issues as well as other factors. Compare your calculations against a research paper discussing indirect costs. Consider social and psychological aspects of adjusting to a chronic disease (such as rheumatoid arthritis). List ten possible factors that might affect audits or surveys evaluating patient experiences and satisfaction with care. Evidence has demonstrated the importance of providing guidance and support to enable individuals with a chronic disease to be informed about their disease, treatments and ultimately how to have an active role in their disease management (Hill & Bird 2003, Homer 2005). People presenting with joint pain are frequently unaware of the standards they should expect, leaving them vulnerable to sub-optimal care.
Consider the potential personal cost implication of having RA (these are often called indirect costs). Include personal costs such as work, adaptations/aids, and mobility issues as well as other factors. Compare your calculations against a research paper discussing indirect costs. Consider social and psychological aspects of adjusting to a chronic disease (such as rheumatoid arthritis). List ten possible factors that might affect audits or surveys evaluating patient experiences and satisfaction with care. Evidence has demonstrated the importance of providing guidance and support to enable individuals with a chronic disease to be informed about their disease, treatments and ultimately how to have an active role in their disease management (Hill & Bird 2003, Homer 2005). People presenting with joint pain are frequently unaware of the standards they should expect, leaving them vulnerable to sub-optimal care.The National Rheumatoid Arthritis Society:
Patient organisation and site for full evidence on mapping project
The British Health Professionals in Rheumatology
HCP organisation resources, guidelines, bursaries
http://www.rheumatology.org.uk
The Arthritis Research Campaign
Patient information leaflets & HCP resources
The NHS Institute for Innovation & Improvement
The Health Talk Online Website
References and further reading
Arthritis and Musculoskeletal Alliance. Standards of Care for Inflammatory Arthritis, Back Pain and Osteaoarthritis. London: Arthritis and Musculoskeletal Alliance; 2004.
Bone and Joint Decade. European Bone and Joint Health Strategies Project. European Action Towards Better Musculoskeletal Health: A Public Health Strategy to Reduce the Burden of Musculoskeletal Conditions. Sweden: Bone and Joint Decade; 2005.
Cooper N.J., Mugford M., Symmons D.P.M., et al. Total costs and predictors of costs in individuals with early inflammatory polyarthritis; A community-based prospective study. Rheumatology. 2002;41:767-774.
Corben S., Rosen R. Self Management for Long-Term Conditions; Patients’ Perspective on the Way Ahead. London: Kings Fund, 2005.
Department of Health. The Expert Patient: A New Approach to Chronic Disease Management for the 21st Century. London: Department of Health; 2001.
Department of Health. Supporting People With Long-Term Conditions: Liberating the Talents of Nurses Who Care for People With Long-Term Conditions. London: Department of Health; 2005.
Department of Health. The Musculoskeletal Services Framework. A Joint Responsibility; Doing it Differently. London: Department of Health; 2006.
Fitzpatrick R., Newman S., Lamb R., Shipley M. Social relationships and psychological well being in RA. Soc. Sci. Med.. 1988;27:399-403.
Frank A.O., Chamberlain M.A. Keeping our patients at work; implications for the management of those with rheumatoid arthritis and musculoskeletal conditions. Rheumatology. 2001;40:1201-1205.
Hammond A., Badcock L. Improving education about arthritis; Identifying the educational needs of people with chronic inflammatory arthritis. Rheumatology. 2002;41(Suppl. 87):216.
Hill J. Rheumatology Nursing; a Creative Approach, second ed. Chichester: John Wiley & Sons; 2006. pp. 151–172
Hill J., Bird H. Outcomes for patients with RA: a rheumatology nurse practitioner clinic compared to standard outpatient care. Musculoskeletal Care. 2003;1(1):5-20.
Homer D. Addressing psychological and social issues of rheumatoid arthritis within the consultation: a case report. Musculoskeletal Care. 2005;3(1):54-59.
Hulsemann J.L., Mittendorf T., Merkesdal S., et al. Direct costs related to rheumatoid arthritis; the patient perspective. Ann. Rheum. Dis.. 2005;64:1456-1461.
Luqmani R., Hennell S., Estrach C., et al. British Society for Rheumatology and British Health professionals in Rheumatology Guidelines for the management of Rheumatoid Arthritis (the first two years). Rheumatology. 2006;45:1167-1169.
Merkesdal S., Ruof J., Huelsemann J.L., et al. Indirect cost assessment in patients with rheumatoid arthritis; comparison of data from the health economic patient questionnaire HEQ RA and Insurance claims data. Arthritis Rheum.. 2005;53(2):234-240.
National Institute of Clinical Excellence (2009) CG79:RHEUMATOID ARTHRITIS National clinical guideline for management and treatment in adults. http://guidance.nice.org.uk/CG79/Guidance/pdf/English
Memel D., Kirwan J.R. General practitioners’ knowledge of functional and social factors in patients with rheumatoid arthritis. Health Soc. Care Comm.. 1999;7(6):387-393.
Oliver S., Ryan S. Effective pain management for patients with arthritis. Nurs. Stand.. 2004;18(50):43-52.
Oliver S. Social and psychological issues in rheumatoid arthritis. Primary Health Care. 2004;14(4):25-28.
Oliver S., Bosworth A. On behalf of the national rheumatoid arthritis mapping project group. Mapping the patient’s journey in rheumatoid arthritis the health and social costs. Ann. Rheum. Dis.. 2006;65(Suppl. II):597.
Oliver S. Best practice in the treatment of patients with rheumatoid arthritis. Nurs. Stand.. 2007;21(42):47-56.
Ryan S., Hassell A., Dawes P., Kendall S. Perceptions of control in patients with rheumatoid arthritis. Nurs. Times. 2003;99(13):36-38.
Sanders C., Donovan J.L., Dieppe P.A. Unmet need for joint replacement; a qualitative investigation of barriers to treatment among individuals with severe pain and disability of the hip and knee. Rheumatology. 2004;43(3):353-357.
The National Health Service Modernisation Agency. Improvement Leaders Guide; Matching Capacity and Demand; Process and System Thinking. London: Department of Health; 2005.
The National Rheumatoid Arthritis Society. Beyond the Pain: The Social and Psychological Impact of RA. Berkshire: National Rheumatoid Arthritis Society; 2004.
The National Rheumatoid Arthritis Society. Meeting the Standards of Care for Inflammatory Arthritis. A National Pilot Survey of Nras Members on the Arma Standards of Care for Inflammatory Arthritis. Berkshire: The National Rheumatoid Arthritis Society; 2006.
The National Rheumatoid Arthritis Society. I Want to Work….’ The National Rheumatoid Arthritis Patient Survey. Berkshire: National Rheumatoid Arthritis Society; 2007.
Woolf A.D., Zeidler H., Haglund U., et aland on behalf of the Arthritis Action Group. Musculoskeletal pain in Europe: its impact and a comparison of population and medical perceptions of treatment in eight European countries. Ann. Rheum. Dis.. 2004;63:342-347.