Chapter 12 Orthotics of the hand
KEY POINTS
 There is no evidence to indicate that static orthoses can prevent deformity from occurring nor correct established deformity
There is no evidence to indicate that static orthoses can prevent deformity from occurring nor correct established deformityINTRODUCTION
Static hand orthotics have been used in rheumatology for many years (Rotstein, 1965). They are recommended for helping individuals manage their arthritis (Scottish Intercollegiate Guidelines Network 2002) and are a popular, commonly used intervention (Henderson & McMillan 2002).
Hand orthotics are used in rheumatology:
PRINCIPLES OF ACTION
RESTING THE JOINT AND PAIN REDUCTION
During periods of acute synovitis, resting affected joints in a biomechanically sound position may reduce joint friction and temperature. At a cellular level this may contribute to a reduction in the pro-inflammatory chemical environment within the joint (Hendiani et al 2003).
CORRECTLY POSITION JOINTS, MINIMISE CONTRACTURES AND DEFORMITIES AND INCREASE JOINT STABILITY
Static orthoses aim to support structures within the wrist and hand that are vulnerable. The radio-carpal, carpometacarpal joint (CMJ), metacarpophalangeal (MCPJ) and proximal interphalangeal (PIPJ) joints and the thumb web space are key anatomical areas for consideration when splinting. Where inflammation causes the potential for muscle imbalance, for example in swan neck and boutonnière deformities, orthotics apply a counterbalance force to prevent or correct extensor tendons slipping across normal joint fulcrums.
IMPROVE HAND FUNCTION
By adding support to proximal joints, applying counterbalanced force to deforming joints and improving biomechanical advantage splints have the potential to improve hand function (Prosser & Conolly 2003). In particular improving support to the wrist can improve grip strength and gross hand function (Nordenskiöld 1990).
Hand orthotics have some biological and biomechanical rationale for their use and action, however, evidence to support and clarify the clinical effectiveness of orthotics in rheumatology is still emerging (Adams et al 2005). This evidence is considered below in regard to five types of orthotics.
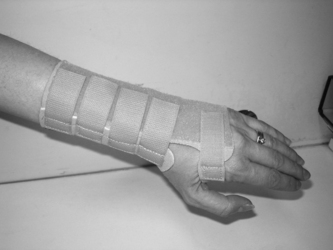
THE WRIST EXTENSION ORTHOSIS
Wrist extension orthoses may be custom-made using either thermoplastic or neoprene material or commercially manufactured from a soft or reinforced fabric with a possible addition of a volar metal support (Fig. 12.1). They may be prescribed to limit wrist circumduction and decrease torque during heavy tasks involving the wrist (Cordery & Rocchi 1998). They may also be used to increase the mobility of the arthritic hand. Wrist extension orthoses can stabilise the wrist in a functionally effective position (10-15 degrees of extension), and facilitate the action of the extrinsic finger flexors to improve handgrip strength (Stern et al 1996). Wrist orthoses provide support to the carpals and wrist joint and several designs of commercial wrist splints have been shown to significantly reduce the electrical activity of the wrist extensors during lifting tasks in people without RA (Stegink- Jansen et al 1997). This may serve to reduce potentially deforming forces on the wrist and carpals.
When worn these orthosis can provide immediate pain relief and significantly reduce pain on functional use of the hand (Haskett et al 2004, Kjeken et al 1995, Nordenskiöld, 1990, Pagnotta et al 2005). Kjeken et al’s (1995) randomised controlled trial analysed splint wear versus non-splint wear over 6 months (n = 69). There was no difference by group on pain, joint swelling, grip or hand motion. However, the control group (n = 33) without splints showed statistically significant improvement in wrist range of motion that was not evident in the splinted group. Both Kjeken et al (1995) and Sharma et al (1991) comment that these wrist orthoses can reduce wrist movement when worn over a number of months and the effects of this should be considered on provision.
In small-scale studies, elastic wrist orthoses have been shown to improve power grip strength for individuals with moderate to severe RA (Backman & Deitz 1988, Haskett et al 2004, Nordenskiöld 1990). However, they have been reported in a small sample (n = 36) to transiently reduce grip strength when first worn and to offer no improvement in grip strength (Stern et al 1996). Although both commercially available and custom made splints have contributed towards improvements in pain and grip strength after four weeks wear in the most able male patients elastic orthoses can hinder maximum grip strength (Sharma et al 1991).
Studies examining hand function have shown that these orthoses are particularly task specific, i.e. they may be able to assist one particular hand skill but reduce another (Pagnotta et al 1998, Stern et al 1996). Functional grip strength has been seen to increase significantly by up to 29% in a woman with RA when these orthoses were worn (Nordenskiöld 1990) yet dexterity, fine finger movement and speed of hand activity have not (Backman & Deitz 1988, Stern et al 1994, 1996).
In summary, wrist extension orthosis have been seen to increase handgrip strength, hand function and provided immediate hand pain relief in some patients. However, they may also contribute to a less dextrous and less mobile hand. There is little evidence to demonstrate the long-term effectiveness of these splints and the quality of evidence available to indicate the clinical effectiveness of these splints is weak (Egan et al 2003).
METACARPAL ULNAR DEVIATION ORTHOSES
These may be small palm-based orthoses or have the additional support of a wrist and forearm component. They may be used early in the rheumatoid disease process to limit the physical factors predisposing the MCPJs to ulnar deviation. By providing a medial force to the proximal phalanges, these orthotics can realign the metacarpals and phalanges during use to improve functional ability of the hand and to prevent further MCPJ ulnar drift and volar subluxation (Adams et al 2005). Therapeutic exercise MCP splints have also been designed to provide exercise options for extrinsic hand extensors and flexors and combat intrinsic plus deformities in the rheumatoid hand (Wijdenes et al 2003).
There is limited evidence for the clinical effectiveness of metacarpal ulnar deviation (MUD) orthoses. In a small repeated measures six months study patients (n = 26) rated them as highly acceptable and satisfactory (Rennie 1996). When worn they realigned the MCPJs and maintained that alignment during functional use of the hand and significantly improved ulnar drift in middle, ring and little finger. They also significantly improved three-point pinch grip strength but did not significantly improve scores on the Sollerman test of hand function (Sollerman 1984), reduce visual analogue pain levels nor improve gross power grip strength. There was no evidence to suggest that they had any long-term effect on correcting MCP joint alignment nor delayed the progression of ulnar deviation.
STATIC RESTING ORTHOSES
This orthosis aims to decrease localised pain and inflammation by resting the joint in a correct anatomical position, provide volar support for the carpus and proximal phalangeals to prevent subluxation realigning drifting MCP joints by providing an ulnar border to the orthosis and restricting carpal movement (Biese 2002). The rationale that correct joint positioning at rest can influence joint integrity has been challenged. Adams et al (2005) argue that the forces contributing towards joint deformity are present when the hand is used functionally thus correct positioning at rest is unlikely to address or correct these (Fig. 12.2).

It is the most commonly used orthosis for treating people with RA and the most frequently used to relieve wrist and hand pain (Henderson & McMillan 2002). These splints do not permit wrist or hand joint movement and are recommended to be worn whilst resting and/or during the night. There have been a few controlled studies examining clinical effectiveness.
Malcus Johnson et al’s (1992) small, 18-month follow-up study of seven people with RA identified that the orthoses reduced nocturnal but not day time pain and MCPJ ulnar deviation continued unabated with splint use. Callinan and Mathiowetz’s (1996) investigation (n = 39) demonstrated that for two types of resting orthosis (soft fabric and hard thermoplastic), there were significant reductions in overall pain levels when these orthoses were worn at night for a month. Hand function and morning stiffness were no different over time when wearing the splint. The majority of the study sample preferred the soft splints.
Janssen et al’s (1990), 12-month, randomized, controlled trial of 29 patients reported a statistically significant reduction in hand joint swelling and a decrease in pain and tenderness scores when these splints were worn. There were improvements in grip strength but not hand function. These findings are difficult to interpret when changes in disease activity nor baseline values of outcomes were considered in the analysis.
Adams et al (2008) randomised controlled trial recruited (n = 116) controlled for baseline outcome value as well as disease activity at baseline in analysis. There were no significant differences in handgrip strength, self-report hand function using the Michigan Hand Outcomes questionnaire and MCPJ ulnar deviation by groups over 12 months follow-up. There was some evidence to indicate that early morning stiffness increased with splint wear (Adams et al 2006).
There is little evidence from longitudinal fully powered studies to indicate that these splints can impact on hand function and deformity, there is some evidence to suggest that hand pain may be improved.
FINGER SWAN NECK ORTHOSES
These small finger based splints apply a three-point force around the PIPJ to prevent PIPJ hyperextension and subsequent distal interphalangeal joint (DIPJ) flexion present in swan necking of the fingers. They are small functional orthoses that permit full PIP joint flexion but prevent hyperextension. They aim to decrease digital pain, correct or prevent swan necking in the digits and improve hand function (Zijlstra et al 2002).
These splints can be custom made using thermoplastic material or silver. Silver custom made options (Fig. 12.3) are more costly but have been reported as more durable than the thermoplastic alternatives, they are also more popular gaining higher adherence levels than thermoplastic alternatives (Macleod & Adams 2002, Macleod et al 2003).

There have only been three reported studies of clinical effectiveness. Ter Schegget and Knipping (2000) demonstrated in a crossover study of 18 individuals there was pain relief when worn but this did not reach statistically significant levels. There were significant improvements in digital stability and DIPJ extension. Zijlstra et al’s (2002) small longitudinal study of 15 people with RA (using 48 ring orthoses) over a 12 month period demonstrated that these orthoses improved functional dexterity levels to statistically significant levels. These results were confirmed by their later study (Zijlstra et al 2004). Conversely, they were seen to have no effect on self-reported hand function, grip strength or hand pain (Zijlstra et al 2002, 2004).
THUMB SPLINTS
In CMCJ basal joint osteoarthrtis thumb splints are used for relief of thumb pain, weakness, contracture and improvement of function (Wajon & Ada 2005). Thumb splints may immobilise just the CMCJ: short opponens type (Fig. 12.4) or combine CMCJ with distal radio carpal joint immobilisation: long type (Fig. 12.5).


There have been no published studies that have compared splinting to no splint intervention. Studies that have examined both short and long type of splints in one study have reported no difference between the outcome of the splints. Weiss et al’s, (2000) short, 2-week cross-over study, examined 26 hands using short and long splints. They reported that both types of splint appear to reduce subluxation of the first CMCJ. Pinch strength was not improved over 2 weeks of splinting, however patients reported anecdotally that they gained some pain relief on wear. Short splints were preferred to long. Soft neoprene splints are preferred to rigid thermoplastic splints and patients prefer the soft splints for daily and long-term use. The beneficial effects have been seen to be amplified with the soft type of thumb splint (Weiss et al 2004).
Patients report preference for soft splints (Buurke et al 1999). In their cross-over study ten female patients were recruited and wore three types of manufactured splints (supple elastic, elastic and semi rigid material), over a period of 12 weeks. There was no difference in pain and pinch scores between the orthoses.
Wajon and Ada’s (2005) randomised trial (n = 40) compared a short opponens type splint and a pinch exercise regime with a thumb strap splint and an abduction exercise regime over a 6 week period. Comparison of change scores over the 6 week follow-up assessments by a blinded assessor demonstrated no difference in outcome by groups for reported pain at rest, pinch grip strength and levels of hand function.
Swigart et al’s retrospective study (1999) examined the effects of thumb splinting on 130 thumbs with varying stages of CMCJ osteoarthritis (OA). Some patients received surgical intervention but patients were excluded if they had been treated with exercise or steroid injections. Long thumb splints were reviewed after a maximum of 4 weeks wear. In milder forms of OA, 76% of patients benefited from some symptomatic improvement and in more severe cases of OA, 54% benefited. These benefits were maintained over 6 months.
Evidence that static thumb splinting may delay or prevent the need for surgical intervention has also been supported by Berggren et al’s seven year follow-up study (Berggren et al 2001). The provision of occupational therapy including aids and equipment, joint protection advice and thumb splinting reduced the number of individuals requiring thumb joint surgery by 65% over a 7 year period (Berggren et al 2001).
Static thumb orthoses have been reported as being effective in long-term relief of OA symptoms when used alongside a single corticosteroid injection (Day et al 2004). A single corticosteroid injection combined with 3 weeks static splinting produced long-term relief from the symptoms of OA in stage I OA (n = 30 thumbs). Although individuals with later stage OA (stage IV) reported less benefit, 40% of participants received symptomatic improvement that was considered sufficient and sustained irrespective of their stage.
CONCLUSION
Static orthoses continue to be enthusiastically endorsed by therapists (Henderson & McMillan 2002). During an era when drug developments continue to assist with more effective control of disease activity and synovitis, continued research is needed into the most appropriate types of orthosis to recommend. The challenge is to provide objective evidence as to whether the continued use of orthoses is indicated for people with arthritis and if so which designs are the most effective and at which stage of the disease process.
Scottish Intercollegiate Guidelines Network (SIGN): Management of early rheumatoid arthritis guidelines: http://www.sign.ac.uk/guidelines/fulltext/48/index.html/
Cochrane database: http://www.cochrane.org/index.htm/
National library for health: http://www.library.nhs.uk/ Default.aspx/
British association of hand therapists: http://www.handtherapy. co.uk/
College of Occupational Therapists Specialist Section: Rheumatology http://www.cot.org.uk/specialist/rheumatology/membership.php/
American Society of Hand Therapists http://www.asht. org/
References and further reading
Adams J., Hammond A., Burridge J., Cooper C. Static orthoses in the prevention of hand dysfunction in rheumatoid arthritis: A review of the literature. Musculoskeletal Care. 2005;3:85-101.
Adams J., Burridge J., Hammond A., et al. The clinical effectiveness of static resting splints in early rheumatoid arthritis: a randomised controlled trial. Rheumatology. 2008;45:1548-1553.
Adams J., Burridge J., Hammond A., et al. The potential side-effects of static resting splints in early rheumatoid arthritis. Ann. Rheum. Dis.. 2006;65:657. (abstract)
Backman C., Deitz J. Static wrist splint: its effect on hand function in three women with rheumatoid arthritis. Arthritis Care Res.. 1988;1:151-160.
Berggren M., Joost-Davidsson A., Lindstrand J., et al. Reduction in the need for operation after conservative treatment of osteoarthritis of the first carpometacarpal joint: a seven year prospective study. Scand. J. Plast. Reconstr. Surg. Hand Surgery. 2001;35:415-417.
Biese J. Therapist’s evaluation and conservative management of rheumatoid arthritis in the hand and wrist. In Mackin E.J., Callahan A.D., Skirven T.M., Schneider L.H., Osterman A.L., editors: Rehabilitation of the Hand and Upper Extremity, 5th ed., St Louis pp 1569–1582: Mosby, 2002.
Buurke J., Grady J., De Vires J., Baten C. Usability of thenar eminence orthoses: report of a comparative study. Clin. Rehabil.. 1999;13:288-294.
Callinan N.J., Mathiowetz V. Soft versus hard resting splints in rheumatoid arthritis:pain relief, preference and compliance. Am. J. Occup. Ther.. 1996;50:347-352.
Cordery J., Rocchi M. Joint protection and fatigue management. Melvin J., Jensen G., editors. Rheumatologic Rehabilitation vol 1 Assessment and Management. . Bethesda:American Occupational Therapy Association. 1998.
Day C., Gelberman R., Patel A., et al. Basal joint osteoarthritis of the thumb: a prospective trial of steroid injection and splinting. J. Hand Surg.. 2004;29A:247-251.
Egan M., Brosseau L., Farmer M., et al. Splints/orthoses in the treatment of rheumatoid arthritis. Cochrane Dat. System. Rev.. 1, 2003. CD004018
Feinberg J., Brandt K.D. Use of resting splints by patients with rheumatoid arthritis. Am. J. Occup. Ther.. 1981;35:173-178.
Hammond A. The use of self-management strategies by people with rheumatoid arthritis. Clin. Rehabil.. 1998;12:81-87.
Haskett S., Backman C., Porter B., et al. A crossover trial of custom-made and commercially available wrist splints in adults with inflammatory arthritis. Arthritis Care Res.. 2004;51:792-799.
Henderson S., McMillan I. Pain and function: occupational therapists use of orthotics in rheumatoid arthritis. Br. J. Occup. Ther.. 2002;65:165-171.
Hendiani J.A., Westlund K.N., Lawand N., et al. Mechanical sensation and pain thresholds in patients with chronic arthropathies. J. Pain. 2003;4:203-211.
Janssen M., Phiferons J., Van de Velde E., Dijkmans B. The prevention of hand deformities with resting splints in rheumatoid arthritis patients. A randomised single blind one year follow-up study. Arthritis Rheum.. 1990;33:123.
Kjeken I., Moller G., Kvien T. Use of commercially produced elastic wrist orthoses in chronic arthritis. Arthritis Care Res.. 1995;8:108-113.
Macleod C., Adams J. Improving patient adherence to swan neck ring splints. Rheumatology. 2002;41:89.
Macleod C., Adams J., Cox N., France J. Ringing the change. Occup. Ther. News. 2003;11:37.
Malcus Johnson P., Sandkvist G., Eberhardt K., et al. The Usefulness of Nocturnal Resting splints in the Treatment of Ulnar deviation of the Rheumatoid Hand. Clin. Rheumatol.. 1992;11:72-75.
McClure P., Blackburn L., Dusold C. The use of splints in the treatment of joint stiffness. Biologic rationale and an algorithm for making clinical decisions. Phys. Ther.. 1994;74:1101-1107.
Nordenskiöld U. Reduction in pain and increase in grip force for women with rheumatoid arthritis. Arthritis Care Res.. 1990;3:158-162.
Ouellette E. The rheumatoid hand: orthotics as preventative. Semin. Arthritis Rheum.. 1991;21:65-72.
Pagnotta A., Baron M., Korner-Bitensky N. The effect of static wrist orthosis on hand function in individuals with rheumatoid arthritis. J. Rheumatol.. 1998;25:879-885.
Pagnotta A., Korner-Bitensky N., Mazer B., et al. Static wrist splint use in the performance of daily activities by individuals with rheumatoid arthritis. J. Rheumatol.. 2005;32:2136-2143.
Prosser R., Conolly W.B. Rehabilitation of the Upper Limb. Edinburgh: Butterworth Heinemann, 2003.
Rennie H.J. Evaluation of the effectiveness of a metacarpophalangeal ulnar deviation orthosis. J. Hand Ther.. 1996;9:371-377.
Rotstein J. Use of splints in conservative management of acutely inflamed joints in rheumatoid arthritis. Arch. Phys. Med. Rehab.. 1965;46:198-199.
Scottish Intercollegiate Guidelines Network. 2002. Management of early arthritis Section 5 The role of the multidisciplinary team.
Sharma S., Immonite V., Schumacher H.R. Relationship of wrist splint to wrist pain and grip strength in rheumatoid arthritis (RA) patients. Arthritis Care Res.. 1991;4(3):S25(c3).
Sollerman C. Assessment of Grip Function: Evaluation of a New Test Method. Sweden: Medical Innovation Technology (MITAB) Sjobo; 1984.
Stegink-Jansen C., Olson S., Hasson S. The effect of use of a wrist orthosis during functional activities on surface electromyography of the wrist extensors in normal subjects. J. Hand Ther.. 1997;10:283-289.
Stern E.B., Sines B., Teague T.R. Commercial wrist extensor orthoses. Hand function, comfort and interference across five styles. J. Hand Ther.. 1994;7:237-244.
Stern E.B., Ytterberg S.R., Krug H.E., et al. Immediate and short term effects of three commercial wrist extensor orthoses on grip strength and function in patients with rheumatoid arthritis. Arthritis Care Res.. 1996;9:42-50.
Swigart C., Eaton R., Glickel S., Johnson C. Splinting in treatment of arthritis of the first carpometacarpal joint. J. Hand Surg.. 1999;24A:86-91.
Ter Schegget M., Knipping A. A study comparing use and effects of custom-made versus prefabricated splints for swan neck deformity in patients with rheumatoid arthritis. Br. J. Occup. Ther.. 2000;59:101-107.
Wajon A., Ada L. No difference between two splint and exercise regimens for people with osteoarthritis of the thumb: a randomised controlled trial. Aust. J. Physiother.. 2005;51:245-249.
Weiss S., La Stayo P., Mills A., Bramlet D. Prospective analysis of splinting the first carpometacarpal joint: an objective, subjective, and radiographic assessment. J. Hand Ther.. 2000;13:218-226.
Weiss S., La Stayo P., Mills A., Bramlet D. Splinting the degenerative basal joint:custom-made or prefabricated neoprene? J. Hand Ther.. 2004;17:401-406.
Wijdenes P., Formsma S., Leysma M., Van der Sluis C. The MCP stabilisation splint: a new method to treat the intrinsic plus phenomenon in patients with rheumatoid arthritis. Ann. Rheum. Dis.. 2003;62:547.
Zijlstra T., Heijnsdijk-Rouwenhorst L., Rasker J. The effect of silver ring splints (SRS) on hand function in patients with rheumatoid arthritis (RA). Ann. Rheum. Dis.. 2002;61:210.
Zijlstra T., Heijnsdijk-Rouwenhorst L., Rasker J. Silver Ring Splints improve dexterity in patients with rheumatoid arthritis. Arthritis Care Res.. 2004;51:947-951.