Chapter 13 Podiatry, biomechanics and the rheumatology foot
KEY POINTS
FOOT INVOLVEMENT IN THE RHEUMATIC DISEASES
This chapter describes the involvement of the foot in rheumatic diseases using examples of commonly presenting features. It outlines the biomechanics of the foot and how disruption of normal function can occur in rheumatic disease. The role of the podiatrist is described in relation to routine and extended scope practice in the management of foot health in patients with rheumatic conditions. Further information on specific rheumatic conditions can be seen in the chapters following.
INFLAMMATORY JOINT DISEASE
Rheumatoid arthritis
Small joint inflammation in the hands and feet is the hallmark of early rheumatoid arthritis (RA). Metatarsophalangeal (MTP) joint synovitis can be detected using magnetic resonance imaging (MRI) in 97% of patients (Boutry et al 2003). The MTP joints are involved early: MRI can detect bone oedema and synovitis even when the finger joints are normal (Ostendorf et al 2004). Erosive changes also occur early in these joints, and their grade of destruction is high (Belt et al 1998). Cardinal signs and symptoms are pain and stiffness which is worse in the early morning and after periods of standing and walking. Pain under the MTP joints is likened to ‘walking on pebbles, glass or stones’. The feet can throb and burn and stiffness is a persistent background feature. The forefoot can rapidly widen with ‘daylight sign’ between the toes related to MTP synovitis, and joint capsule and periarticular ligament damage (Fig. 13.1). Patients report that normal footwear becomes tight, uncomfortable and difficult to wear. On examination the metatarsal squeeze test (gripping the MTP joints and compressing them together) may be positive and one or more MTP joints swollen and tender on palpation.
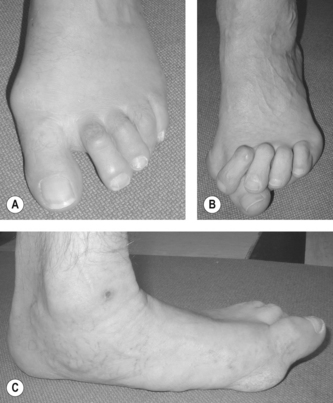
Figure 13.1 (A) Typical forefoot changes in the early stages of rheumatoid arthritis. (B) The forefoot of a patient with advanced, long-standing RA; and (C) pes planovalgus in RA.
Early involvement in the peritalar region affects the tenosynovium of tibialis posterior in around 60% of patients (using MRI) and the midtarsal, subtalar and ankle joints in around 25% of patients (Bourty et al 2003, Fleming et al 1976). Pain and stiffness are common and subtle but clinically important changes in function can be detected within 2 years from onset (Turner et al 2006). Mild-to-moderate pes planovalgus (flat footedness) can be found. However, this tends to be passively correctable. In contrast to the MTP joints, ankle and subtalar joint erosions and destruction occur infrequently and in the later stages (> 15 years). True bony ankylosis is rare (Belt et al 2001).
In established RA the prevalence of foot symptoms is over 90% (Michelson et al 1994). Synovial pannus and joint erosions weaken intra-articular and peri-articular structures, whilst joint effusion distorts the capsule. Therefore under normal weightbearing loads progressive and severe deformities can develop. In the forefoot, fibular drift of the toes mimics ulnar deviation of the finger joints and if severe the subluxed or dislocated toes can over- or under-ride adjacent toes. Hallux valgus, tailors bunion and hammer, claw or mallet toe deformity can rapidly develop (Briggs 2003). Bursitis between or under the metatarsal heads is common and can be detected using MRI in around 60% of cases (Boutry et al 2003). Morton’s interdigital neuroma may also be more prevalent in RA patients (Awerbuch et al 1982). Painful callosities can develop over the dorsum of prominent toe joints, medially on a hallux valgus joint or around the plantar metatarsal heads (Korda & Balint 2004).
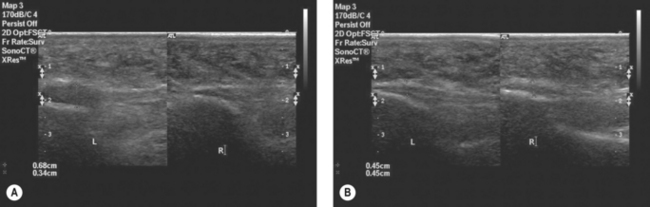
Persistent disease in the peritalar region leads to the development of pes planovalgus and in severe cases the medial longitudinal arch may be completely collapsed (Turner et al 2008a). Pes planovalgus is associated with tendinopathy of tibialis posterior (Bouysset et al 2003, Jernberg et al 1999). Clinically the tendon may be swollen and inflamed medially at the ankle region (Woodburn et al 2002). MRI or ultrasound (US) imaging reveals tendon enlargement, tenosynovitis, tendinopathy, and intra-substance splits, however true rupture occurs in less than 5% of cases (Lehtinen et al 1996, Premkumar et al 2002). Pain and swelling in the posterior heel region may be associated with retrocalcaneal bursitis, Achilles enthesopathy and posterior calcaneal erosions (Falsetti et al 2003). Enthesopathy of the plantar fascia, or more rarely a plantar nodule, may lead to plantar heel pain.
Extra-articular manifestations such as peripheral arterial disease (nail fold infarcts, cutaneous vasculitis and digital gangrene), neuropathy, ulceration and subcutaneous nodules affect some patients with RA. Foot ulceration and infection are major clinical red flags, especially in patients treated with biologic therapies, glucocorticosteroids and some disease modifying antirheumatic drugs (DMARDs). Ulceration occurs most commonly over the dorsal aspect of hammer toes, over the metatarsal heads and the medial bunion with hallux valgus deformity. The overall prevalence of ulceration in people with RA is 9.7% (Firth et al 2008a) and common risk factors include deformity, elevated skin contact pressures, loss of protective sensation, peripheral vascular disease, active disease and steroid use (Firth et al 2008b). The risk of serious infection involving the skin is recognised in RA patients receiving anti-TNF therapy, and a number of case series have described infection associated with skin ulceration (Otter et al 2005) and spontaneous onychocryptosis (in-growing toenail) (Davys et al 2006a).
Seronegative spondlyoarthropathies
The seronegative spondyloarthropathies (SpAs) share a number of common clinical features, of which asymmetric oligoarthritis, peripheral small joint arthritis, enthesopathy, and dactylitis affect the feet. Peripheral enthesitis (characterised by inflammation at sites of tendon, ligament and joint capsule into bone) is regarded to be a hallmark feature of SpAs and may be associated with enthesophyte formation (bony proliferation). Inflammation may occur at any entheses, however, enthesitis at the heel is reported to be the most frequent and occurs at the attachment of the Achilles tendon (AT) and plantar fascia to the calcaneus (Olivieri et al 1992). In routine clinical practice enthesitis is diagnosed based on patient symptoms and clinical examination to determine tenderness on palpation. However, clinical examination underestimates the presence of enthesitis and detection is improved when imaging techniques such as MRI and high resolution US are used (Balint et al 2002, D’Agostino et al 2003, Galluzzo et al 2000).
Management of SpAs relies on DMARD and biologic drug therapy targeting the underlying disease mechanisms. However, ultrasonographic data suggest that despite intensive pharmacological management enthesitis in the foot is detectable in a high proportion of patients (approximately 60-80% of patients) and is poorly correlated with systemic parameters of disease activity (Borman et al 2006, D’Agostino et al 2003, Genc et al 2005). Biomechanical factors, including foot function, may contribute to the development of enthesopathies (Benjamin & McGonagle 2001) and may help explain the discordance between disease activity parameters and enthesitis. It has been suggested poor alignment of the rearfoot and control of foot pronation, may make the enthesis at the heel more vulnerable to injury however, data are currently lacking to support this theory.
Forefoot deformity and nail pathologies are especially common in patients with PsA. A recent survey found 95% of patients had some deformity in the forefoot (Hyslop et al 2008). PsA will often present initially in the interphalangeal (IP) joints of the toes and then the MTP joints. Usually both IP joints in the toe are affected providing the characteristic clinical presentation dactylitis or ‘sausage toe’. Inflammation at the IP and MTP joints can cause stretching and damage to the joint capsules and collateral ligaments leading to the typical toe joint deformities of RA. Inflammation can also lead to the formation of joint erosions, however, unlike in RA these tend to occur in the juxtaarticular region (adjacent to the articular surface). The course and progression of radiological damage can vary in patients with PsA, and a number of common features in the foot have been identified (Fig 13.2). These include the characteristic pencil in cup deformity (Gold et al 1988), the so called ivory shaft (increased bone density in the shaft of the phalanx), resorption of the distal phalanx, resulting in a characteristic pointed toe pulp (Moll 1987).
JUVENILE IDIOPATHIC ARTHRITIS
Foot problems such as synovitis, limited range of motion, malalignment and deformity have been reported in over 90% of children with juvenile idiopathic arthritis (JIA), generally increasing in severity with age, disease duration and in those with polyarticular disease (Spraul & Koenning 1994). Foot pain, deformity and impaired function are persistent problems even in those children optimally managed on DMARD and biologic therapy (Hendry et al 2008). Synovitis in the ankle and rearfoot joint occurs in approximately one-third of patients across all disease subtypes and is associated with limited ankle range of motion, pronated rearfoot and midfoot joints, and weakness of the ankle dorsiflexors/plantarflexors (Brostrom et al 2002, Spraul & Koenning 1994). Pes planovalgus is twice as common as varus heel alignment (pes cavus foot type) in these children (Mavidrou et al 1991).
Synovitis, effusion, erosive changes and deformity at affected MTP joints are observed in about one-fifth of JIA children and hallux valgus is common (Ferrari 1998). Deformities such as splaying of the forefoot; hammer, claw, and mallet toe deformity and MTP joint subluxation can rapidly develop. Leg length discrepancy, deformity and proximal joint malalignment resulting from growth disturbances can also impact on foot structure and function. Other problems such as Achilles tendinopathy, retrocalcaneal bursitis, tenosynovitis and plantar fasciitis occur in association with specific disease sub-types.
Disabling foot pain in JIA is associated with abnormalities in gait, either as a direct consequence of joint damage or as compensation to underlying impairments (Brostrom et al 2002, Hendry et al 2008, Witemeyer et al 1981). Typically these include reduced walking speed, increased double-limb support time, and step asymmetry. Gait can also be cautious and guarded with reduced heel-strike and push-off force (Brostrom et al 2002).
OSTEOARTHRITIS
The commonest sites for osteoarthritis in the foot are the 1st MTP joint (hallux rigidus), the ankle joint and the tarsometatarsal joints. Hallux rigidus is found in approximately 5% of adults above the age of 50 (Shereff & Baumhauer 1998) and is associated with trauma, metabolic and congenital disorders. The condition is often bilateral and affects more women than men. Patients may complain that the joint is stiff and painful and made worse by walking. Examination reveals a dorsal exostosis which is palpable and tender along the MTP joint line. Dorsiflexion motion is limited and painful. Radiographs reveal loss of joint space, dorsal osteophytes, subchondral bone sclerosis and cysts.
Primary osteoarthritis of the ankle joint occurs in less than 10% of all cases and over 70% are post-traumatic (Saltzman et al 2005, Valderrabano et al 2008). The lower rate of primary disease in comparison to the hip and knee is attributed to anatomic, biomechanical, and cartilage properties which protect the joint from degenerative changes (Huch et al 1997). Trauma is usually associated with malleolar fractures and ankle ligament lesions. The ankle is stiff and painful with mild-moderate effusion. Pain can be elicited on specific movements such as dorsiflexion/inversion and crepitus can be felt. Range of motion will be limited, the joint unstable and gait adapted to achieve relief. Bony enlargement, malalignment and/or deformity, can progressively develop (Fig. 13.3). Malalignment is distributed in favour of varus across all etiologies (55% varus, 37% neutral, 8% valgus) (Valderrabano et al 2008). Joint space narrowing, osteophtye formation, subchondral bone sclerosis, and cyst formation are typical radiographic features as well as varus malalignment, anterior protrusion of the talus and flattening of the tibial plafond (articular surface of the distal end of the tibia).

CONNECTIVE TISSUE DISEASES
Foot involvement is prevalent but often overlooked in the two most common connective tissue diseases; scleroderma and systemic lupus erythematosus (SLE). The feet are involved less frequently and later than the hands in scleroderma but nevertheless 90% prevalence has been reported (La Montagna et al 2002). Radiological changes in the joints in these patients include juxtaarticular demineralisation, distal phalange resorption, joint space narrowing, and extraarticular calcification. Radiological foot abnormalities have been reported in 26% of patients (Allali et al 2007). Approximately 90% of patients suffer from Raynaud’s syndrome which can lead to pain in the feet and digital ulceration, scarring and in some cases gangrene and amputation (La Montagna et al 2002, Sari-Kouzel et al 2001).
Localised thickening and tightening of the skin of the toes (sclerodactyly) and flexion contractures have been reported in 6% of cases (La Montagna et al 2002) and are associated with atrophy of the underlying soft tissues. Subcutaneous calcinosis occurs infrequently (6%) but can be extremely painful and disabling if it occurs on a weight bearing area of the foot. Whilst problems in the feet occur less frequently than those in the hand they can be a major source of morbidity and disability in patients with scleroderma.
Non-erosive arthritic manifestations (Jaccoud’s type arthropathy) involving the foot and ankle have been reported in patients with SLE. Common foot deformities found in these patients are hallux valgus, subluxation and fibular deviation of the MTP joints, and widening of the forefoot (Mizutani & Quismorio 1984, Reilly et al 1990). Erosive changes are rare in this group; however, hook like erosions caused by pressure erosion beneath the distorted joint capsules in the deformed joints may appear and have been reported at the metatarsal heads. Accelerated atheroma is a well recognised complication of SLE and abnormal ankle brachial pressure indices have been reported in almost 40% of patients (Theodoridou et al 2003). However, it rarely leads to critical peripheral ischaemia and gangrene is a relatively uncommon finding (Jeffrey et al 2008). Raynaud’s syndrome occurs in approximately 30% of cases (Bhatt et al 2007).
CRYSTAL JOINT DISEASE
Sudden onset of pain, swelling, erythema and limited movement in the foot or ankle is characteristic of acute gout. The 1st MTP joint is most commonly involved, although acute gouty arthritis can involve the dorsum of the foot or ankle. Diagnosis of gout is established when monosodium urate (MSU) crystals are found in joint aspirate. Tophi are chalky white deposits of MSU that are large enough to be seen on radiographs and may occur at virtually any site but commonly occur in the joints of the hand and foot (Harris et al 1999). The rate of tophi formation correlates with duration and severity of hyperuricaemia (Gutman 1973). Intra-articular tophi are associated with the formation of bone erosions. However in contrast to RA, these are ill defined with overhanging edges and are not associated with osteopenia (Dalbeth et al 2007). Compared with RA, joint space narrowing occurs late in the disease or joint space widening may also occur in advanced disease (Dalbeth et al 2007). Moreover there is a strong relationship between bone erosion and the presence of intraosseous tophus. This suggests that tophus infiltration into bone as the dominant mechanism for development of bone erosion and joint damage in gout (Dalbeth et al 2008).
Pseudogout is much less common than gout and usually presents with a less severe clinical picture. It is characterised by deposition of calcium pyrophosphate dehydrate (CPPD) crystals in the joint or periarticular tissues which produces an acute inflammatory synovitis. Whilst the disorder is more common in the knee, hip, shoulder and wrist, it can also affect the 1st MTP joint and ankle.
HYPERMOBILITY
Hypermobility (excessive mobility) can occur at a single joint or can be widespread throughout the body. There are several conditions associated with hypermobility, including Ehlers-Danlos disease, Marfan syndrome, osteogenesis imperfecta and benign joint hypermobility syndrome (BJHMS) which is the most common and will be the focus of this section. BJHMS has been defined as generalised joint laxity and hyperextensibility of the skin in the absence of any systemic disease. The pattern and course of musculoskeletal problems can vary considerably in patients with BJHMS from intermittent problems in a single joint to persistent widespread involvement of joints and soft tissues. A high proportion of patients with BJHMS have intermittent joint and soft tissue pain, joint effusions, dislocations, and they also have a tendency to bruise and scar easily.
Patients with BJHMS have poorer proprioceptive feedback and muscle strength, although this can be improved with proprioceptive exercises (Hall et al 1995, Sahin et al 2008a, Sahin et al 2008b). The proprioceptive system plays a critical role in maintenance of joint stability, including body position and movement of joints. Therefore deficits in proprioceptive function can make joints and soft tissues more vulnerable to minor traumas and may allow acceleration of degenerative joint conditions (Hall et al 1995). Hypermobility at the ankle and foot has been reported in a high proportion of patients. In the foot it is common for patients with BJHMS to report ankle instability and recurrent ankle inversion sprains (Finsterbush et al 1982). Other common features include joint instability, pes planovalgus deformity, subluxation of the MTP joints and hallux valgus (Fig. 13.4). In a review of a 100 consecutive patients, the most frequent complaint (48% of cases) was pain in the feet and calf associated with pes planovalgus deformity. Both general and local hypermobility at the 1st MTP joint have been linked with hallux valgus deformity (Carl et al 1988, Myerson & Badekas 2000).
BIOMECHANICS OF THE FOOT AND ANKLE
FUNCTION OF THE FOOT AND ANKLE IN HEALTH
Normal foot function is required for efficient ambulation and is related to three events: shock absorption, weight-bearing stability and progression (Perry 1992). Subtalar joint eversion, with internal tibial rotation and midtarsal dorsiflexion are the shock absorbing mechanisms that lessen the impact at initial foot-to-ground contact (∼1.2-1.4 × body weight). This occurs during the first (heel) rocker when the body vector (centre-of-pressure) is located in the heel, behind the ankle to generate a plantarflexion moment. This causes rapid foot placement on the ground through ankle joint plantarflexion. Pre-tibial muscle activity (tibialis anterior and extensor hallucis and digitorum longus) controls the rate of plantarflexion until forefoot contact is made. Simultaneously, eversion at the subtalar joint, coupled with internal leg rotation serve to further absorb shock during this initial phase of gait. Tibialis anterior absorbs some of the shock during the heel rocker period as subtalar eversion is decelerated. Tibialis posterior initiates activity in the middle of this phase and serves as a reserve muscle force to control subtalar eversion. It also contributes to dynamic support of the midtarsal joint which dorsiflexes immediately following forefoot contact at the onset of midstance (Woodburn et al 2005). This movement also contributes to shock absorption and is further supported by the long flexor muscles of the leg and the intrinsic plantar foot muscles.
During the midstance period, the body moves forward across a plantargrade foot increasing the loading on the forefoot. The centre-of-pressure moves forward anterior to the ankle joint and a plantarflexion moment starts to develop. Weightbearing stability is established by synergistic ankle, subtalar and midtarsal joint motion aided by tightening of the plantar fascia (a ligament band extending from the calcaneus to the bases of the proximal phalanges). The tibia externally rotates and advances forward to dorsiflex the ankle joint and subtalar eversion reverses to inversion movement. This is the second ankle functional rocker. In combination these actions raise the talar head, dynamically lock the midtarsal joint and stabilise the medial and lateral columns of the foot. The third functional rocker is the forefoot rocker which characterises forward progression of the body. In the foot the centre-of-pressure reaches the metatarsal heads and terminates between the first and second metatarsal heads. The medial side of the foot is stabilised by plantarflexion of the first metatarsal by action of the peroneus longus. Dorsiflexion occurs through the MTP joints and the heel lifts from ground contact. The gastrocnemius and soleus calf muscles first act to control the rate of tibial advancement and then through concentric activity plantarflex the ankle joint. The foot pivots about the MTP joints and the body advances.
DISRUPTED FOOT AND ANKLE FUNCTION IN THE RHEUMATIC DISEASES
Across the rheumatic disorders pathological disease processes serve to disrupt the shock absorption, weight-bearing stability and progression functions of the foot and ankle. The clinical consequences are impairments such as pain, joint stiffness, and deformity which lead to degraded and adapted changes in gait. As a universal response to pain, independent of specific rheumatic diseases, patients adapt gait by slowing walking speed, reducing the step length, and increasing the period of double-limb support (Turner et al 2008a, 2008b, Woodburn et al 2004). In RA for example, in both early and established disease, the heel rocker can be absent as the foot is placed flat to the ground (Turner et al 2006, 2008a). The tibia is vertical with the centre-of-pressure located close to the ankle joint axis and the initial contact angle of the foot is parallel to the floor. This pattern occurs secondary to MTP disease and weak muscle action (e.g. gastrocnemius-soleus) and serves to reduce the rate of limb loading, and the joint and soft-tissue reaction forces. These actions lessen pain and protect joints vulnerable to progressive inflammatory damage (Turner et al 2008a).
In other diseases it may also be beneficial to reduce walking speed and shorten step length at initial heel contact to control symptoms. In the spondlyoarthropathies, these adapted changes may lessen the tensile and compressive forces on the Achilles tendon, plantar fascia and tibialis posterior; the classic and functional enthesis sites. Primary osteoarthritis of the ankle and or subtalar joints is rare but in post-traumatic secondary cases the large forces experienced during initial loading may serve to concentrate focal stresses on the articular surfaces when the geometry has changed as a result of instability or realignment. Malalignment and pain are associated so gait adaptation may beneficially improve symptoms and reduce stress on cartilage lesions.
Inflammatory joint disease most commonly disrupts the ankle rocker during the mid-stance period of gait when the weightbearing stability is required the most (Turner et al 2008a). Synovitis in the ankle, subtalar and midtarsal joints and tenosynovitis of tibialis posterior leads to stretching of the joint capsule and supporting ligaments, as well as attenuation (longitudinal tears or more rarely tendon rupture) (Woodburn et al 2005). Detailed gait studies have characterised the associated changes in joint motion and forces as well as plantar stresses and centre-of-pressure pathways (Turner et al 2008a, 2008b, Woodburn et al 2004). Excessive and prolonged subtalar eversion and ankle dorsiflexion occur, along with collapse of the medial weightbearing column. This is a highly unstable foot, which progresses to pes planovalgus. Reduced ankle plantarflexion moment and power both reflect the accompanying slow walking speed as well as gastrocnemius-soleus muscle weakness (Turner et al 2008a, 2008b). Keenan et al (1991) used electromyography to show that in patients with RA and pes planovalgus, tibialis posterior has elevated and prolonged activity in an attempt to stabilise the subtalar and midtarsal joints, even though the muscle is weak (Keenan et al 1991). The centre-of-pressure is directed more medially in the foot and focal stresses can appear on the medial mid-foot indicating column collapse (Turner et al 2008b).
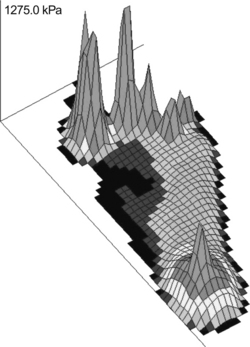
Any of the rheumatic diseases associated with acute pain or swelling at the MTP joints (e.g. acute gout or synovitis) will normally disrupt the forefoot rocker during progression (Semple et al 2007). In RA for example, forward progression of the centre-of-pressure is delayed in the heel and mid-foot and rapidly advances through the forefoot as patients convert to a hip-pulling strategy. The adapted gait serves to minimise the time and magnitude of loading at painful joints (Semple et al 2007). In chronic disease, advanced deformity, joint stiffness, and pain are all associated with elevated areas of peak plantar pressure, irrespective of the underlying disease. Changes in joint motion and kinetics (forces) can also be detected during progression. In RA and PsA for example, motion analysis reveals reduced ankle plantarflexion in terminal stance, reduction in vertical and anterior/posterior ground reaction forces, and reduced peak ankle joint power (Turner et al 2008a, 2008b). Advancement of the tibia is slow and the foot is lifted from the ground further emphasising the loss of forefoot rocker. In severe forefoot disease, plantar callosities, bursa and ulceration are closely associated with localised sites of high pressure. Overall, the appearance is of a slow, shuffling style gait, with guarding and deliberate and cautious placement of the foot.
PODIATRY
OVERVIEW
Podiatry is a branch of the allied health professions dealing with the assessment, diagnosis and treatment of foot and ankle problems. Practitioners in specialist or extended scope roles are expertly placed to assess, advise and treat patients with the rheumatic diseases. Podiatry care is one of the most frequently requested service among RA patients (Martin & Griffith 2006) yet service provision throughout the UK is low (Redmond et al 2006). Encouragingly, the evidence base is growing for podiatry treatments (Brouwer et al 2005, Farrow et al 2005, Murley et al 2008).
BASIC FOOT HYGIENE, SELF-MANAGEMENT AND ADVICE
In patients with RA and foot problems, approximately half are unable to manage their own feet due to problems with reach and grip strength (Semple et al 2008). Podiatrists can assist patients and their family or carers to help them maintain good standards of personal foot hygiene. This can involve assistance with reaching the feet and using equipment such as nail-clippers and files. Self-management has benefits such as improved foot health outcomes, reduced demand on podiatry services, and develops self-monitoring for those with a history of problems such as ulceration and infection.
A small amount of well designed and validated patient information is available and focuses on causes and treatment of common problems as well as advice on self-management and footwear (e.g. ‘Feet, footwear and arthritis’, Arthritis Research Campaign patient information leaflet). Deformed toes, which cause pressure and thickening on the toenails may require periodic reduction using nail burrs to ease discomfort. Plantar or dorsal corns or callus require regular debridement and whilst effective, pain relief is short and the problem may rapidly recur within a few weeks (Davys et al 2005, Woodburn et al 2000). Surgical correction of underlying deformities is advised when callosities are persistent, or where skin tissue viability is poor and lesions have ulcerated. Given the high prevalence of dermatophytosis (superficial fungal infection or tinea) (Bicer et al 2003), advice on treatment for tinea pedis (athlete’s foot) and onychomycosis (fungal infection of the nail) should be directed to the rheumatologist or GP.
FOOT ORTHOTICS
Foot orthotics are indicated in patients with rheumatic diseases to provide:
(after Kavlak et al 2003)
Across the rheumatic diseases complex foot problems are treated with customised orthoses to provide personalised fit and function (Fig. 13.5). Indeed, moderate-to-good levels of evidence suggest that in RA for instance, good outcome (pain reduction and increased function) can be achieved by customised functional orthoses, especially in early disease (Gossec, et al 2006, Woodburn et al 2002) and when combined with extra-depth shoes (Farrow et al 2005).

Figure 13.5 Customised foot orthotic for a patient with inflammatory joint disease. The orthosis has polypropylene middle shell to stabilise the subtalar and talonavicular joints and a cushioning top surface to protect painful MTP joints
Customised orthoses comprise both cushioning, stability and correction elements. The basic orthotic shell will vary by stiffness according to the materials used and their thickness. For example, carbon graphite devices are thin and provide rigid functional control so are suitable for the early stages of inflammatory arthritis (Woodburn et al 2002). These devices are manufactured to plaster models, or digital scans which capture the optimal foot pose in neutral alignments at the ankle, rearfoot and forefoot. Medial/lateral correction (for flexible eversion/inversion deformity) is created by heel and/or forefoot posts (or wedges), which are built externally or intrinsically into the shell. A top layer of cushioning material is added to reduce sheer and compressive stresses, which offload painful joints or plantar pressure lesions (Woodburn et al 2002). In pursuit of pain relief many patients with rheumatic foot conditions purchase off-the-shelf insoles and orthoses. Despite lacking robust data, many of these products do offer varying levels of symptom relief.
Total contact orthoses are custom-made to plaster or impression moulded casts of the feet and are indicated for moderate-to-severe deformity when joints are stiff and when secondary problems such as pressure lesions or ulceration exist. During manufacture, semi-rigid and cushioning materials are combined and shaped to closely fit the plantar foot geometry. This provides moderate stabilisation combined with maximum surface contact to cushion and support prominent and deformed joints. They are used in conjunction with extra-depth footwear. In ulcerated feet, devices such as the DH Off-Loading Walker™ (Ossur, Manchester, UK) and the Aircast SP Walker™ (DJO Incorporated, CA, USA) are used to off-load the ulcerated lesions. These lightweight walking braces permit near normal ambulation and provide total contact fit through mechanisms such as adjustable air cells. They also provide space to incorporate ulcer/wound dressings and/or insole systems to off-load the target ulcer site. Other walking braces such as the AirLift™ PTTD Brace (DJO Incorporated, CA, USA) can also be used for severe tendon and soft-tissue disease to mechanically off-load vulnerable tissues, and are also indicated during episodes of acute inflammation, e.g. tibialis posterior tendinopathy in RA or Achilles tendinopathy in psoriatic arthritis.
Podiatrists are also involved in providing insoles and orthotics to treat osteoarthritis of the knee. Laterally wedged insoles reduce the knee adduction moment in medial compartment knee OA and offer short term pain relief (Hinman et al 2008, Kuroyanagi et al 2007). Longer term symptomatic effects are unclear, although nonsteroidal anti-inflammatory drug use may be reduced (Brouwer et al 2005, Gélis et al 2005, Pham et al 2004). Similarly, a medial-wedged insole, when combined with an ankle support, can achieve pain relief and provide functional improvement of valgus knee OA (Rodrigues et al 2008).
FOOTWEAR
Specialist footwear can be used to relieve pain, protect joints, and improve function in any of the rheumatic diseases (Chalmers et al 2000, Fransen & Edmonds 1997, Shakoor et al 2008). However, challenges exist to balance comfort and fit with style and design, especially for women. Indeed Williams concluded in a recent study of extra-depth shoe use in RA patients, ‘Footwear replaces something that is normally worn and is part of an individual’s body image. It has much more of a negative impact on the female patients’ emotions and activities than previously acknowledged and this influences their behaviour with it’ (Williams et al 2007a). This is often ignored as many clinicians do not have the time or necessary experience to properly advise patients. Ultimately this leads to poor treatment adherence and outcome (Williams & Meacher 2001).
Fully personalised orthopaedic shoes are the skilled domain of the orthotist and the appliance/footwear technician. They are indicated for patients with the severest and most complex foot deformities. Extra-depth footwear is used much more extensively these days as design, functionality and patient choice continue to improve. These shoes are either provided straight ‘off-the-shelf’ or assembled from modular sections which permit variation in width and depth of the toe box, and allow personalised modifications such as outer sole (e.g. rocker sole) and heel modifications (e.g. medial flare) to improve function, as well as adaptations such as Velcro fastenings, which are particularly helpful to those with hand disease (Helliwell et al 2007). These shoes are particularly useful in inflammatory joint disease when patients are unable to fit suitable retail shoes due to disabling foot pain and deformity. In RA there is evidence that extra-depth shoes are effective for pain relief and to improve function, particularly when combined with customised orthoses (Chalmers et al 2000, Fransen & Edmonds 1997, Williams et al 2007b). Overall satisfaction is raised when patients are involved in the design, supply and monitoring processes throughout treatment (Williams et al 2007b). Elsewhere, novel footwear concepts are being developed and tested to reduce knee joint loads (Shakoor et al 2008).
GAIT TRAINING, EXERCISE, AND MUSCLE STRENGTHENING
Muscle strengthening, proprioception training and gait re-education are undertaken in conjunction with orthotic, footwear and anti-inflammatory treatments. Since general aerobic condition might be poor and proximal limb involvement highly prevalent, rehabilitation (gait training, muscle and proprioception training and appliance/equipment supply) is routinely undertaken in a coordinated programme, working alongside other members of the multidisciplinary team.
TISSUE VIABILITY AND WOUND CARE
Foot ulceration can occur in patients with RA, connective tissue and crystal joint diseases (Firth et al 2008a, Jeffrey et al 2008, Kumar & Gow 2002). The management of foot wounds and prevention of infection, especially in those patients receiving biologic therapies, remains a key challenge (Davyset al 2006b). The podiatrist firstly has a key role to initiate preventative measures. This primarily involves joint protection to remove focal pressure from vulnerable sites using customised orthoses, braces or footwear. In those cases where ulcers develop, vascular assessment techniques and appropriate referral, wound care management/debridement, pain relief and orthoses and braces to facilitate off-loading are the cornerstones of practice.
Management of foot ulceration can be challenging for patients with rheumatic diseases. Systemic drug therapies may increase the risk of infection, delay wound healing, and may mask the classic signs of infection. Wounds may often extend down to the underlying bone and in the presence of joint erosions and deformities detection of osteomyelitis can be difficult. Severe foot deformity may make debridement and dressing of wounds challenging, furthermore, it may limit the choice of dressing which can be applied (many may be too bulky and uncomfortable for patients). The newer biologic therapies are increasingly used to suppress inflammation in patients with rheumatic diseases; however, these drugs are powerful immunosuppressants and are associated with an increased risk of infection of skin/soft tissues (Otter et al 2005). Foot ulceration is a contraindication to treatment with any biologic agent as the risk of rapidly progressing infection is too great, therefore the treatment must be suspended. In these instances, ulcers need to be healed quickly so the patient can recommence drug therapy and strategies put in place to prevent recurrence.
EXTENDED SCOPE PRACTICE: INTRA-ARTICULAR AND LESIONAL INJECTIONS AND FOOT SURGERY
Podiatrists are trained in local anaesthesia at an undergraduate level and can perform regional anaesthesia of the foot or ankle to facilitate a number of treatments (usually surgery) and may use injections of local anaesthetics diagnostically. A number of AHPs including podiatrists can now access specialist training programs to undertake intra-articular (IA) or soft tissue (ST) injections as an adjunct to their practice and they can deliver injection therapy under a Patient Group Direction. Both IA and ST injections of corticosteroids can be an extremely effective method to reduce pain, inflammation, swelling and increase function at joints without exposing patients to the usual side effects associated with systemic drug therapy. However, a number of both local and systemic adverse effects have been identified including infection, bleeding, post injection flare, subcutaneous tissue atrophy/skin depigmentation, tendon rupture, nerve damage and delayed soft tissue healing (Saunders & Longworth 2006). Common sites for IA injection include the ankle, subtalar, talonavicular, MTP and IP joints. ST injections of the plantar fascia, retrocalcaneal bursa, interdigital neuroma/bursitis and the tendons of tibialis posterior and peroneal muscles also respond well. The effectiveness of IA or ST injection depends on the accuracy of placement.
The complex anatomy of the foot (particularly in the rearfoot) makes it hard to determine precisely which structures are involved from clinical examination alone and use of ultrasound (US) has been shown to influence sites selected for injection and positively influence short-term efficacy of injection (D’Agostino et al 2005). The use of US to guide injections is likely to occur more frequently as the technology becomes cheaper and more accessible and more clinicians are appropriately trained in the technique (Fig. 13.6). It has been shown that with appropriate training and mentorship, podiatrists, can provide adequate sonographic images and reliably report features such as erosions, synovitis and bursitis with excellent levels of agreement when compared to expert radiologists (Bowen et al 2008). Therefore it is anticipated that US will become part of extended scope practice for podiatrists working in advanced/consultant practitioner roles. Podiatrists routinely monitor response to rehabilitation therapies and when indicated (non-response, deteriorating foot health, and complications such as ulceration or infection) surgical opinion should be sought.
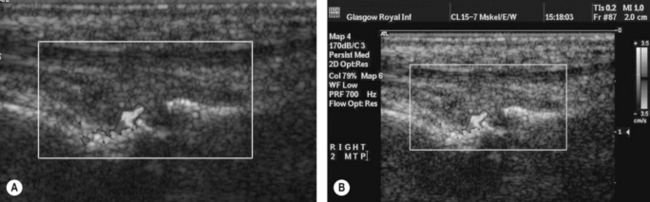
Figure 13.6 (A) Intra-articular corticosteroid injection into the 2nd MTP joint in an RA patient and (B) with high resolution ultrasound proven synovitis.
In 2008, there were approximately 150 surgically trained podiatrists and some may be undertaking forefoot reconstruction procedures in patients with rheumatic foot conditions. In more complex cases involving rearfoot and ankle conditions, techniques such as arthrodesis and joint replacement largely remain the remit of orthopaedics.
 Review the ARMA Standards of Care 13-18 for people with musculoskeletal foot health problems. Identify key assessments that you would undertake in a patient with inflammatory arthritis. http://www.arma.uk.net/pdfs/musculoskeletalfoothealthproblems.pdf. Accessed February 2009.
Review the ARMA Standards of Care 13-18 for people with musculoskeletal foot health problems. Identify key assessments that you would undertake in a patient with inflammatory arthritis. http://www.arma.uk.net/pdfs/musculoskeletalfoothealthproblems.pdf. Accessed February 2009.Scottish Intercollegiate Guidelines Network (SIGN). 2000. Management of Early Rheumatoid Arthritis. A National Clinical Guidelines. SIGN publication No. 48, December http://www.sign.ac.uk/guidelines/fulltext/48/index.html/ accessed February 2009
ARMA Standards of Care for people with musculoskeletal foot health problems. Podiatry Rheumatic Care Association, 2008 http://www.arma.uk.net/pdfs/musculoskeletalfoothealthproblems.pdf/ accessed February 2009.
References and further reading
Allali F., Tahiri L., Senjari A., et al. Erosive arthropathy in systemic sclerosis. BMC Public Health. 2007;7:260.
Awerbuch M.S., Shephard E., Vernon-Roberts B. Morton’s metatarsalgia due to intermetatarsophalangeal bursitis as an early manifestation of rheumatoid arthritis. Clin. Orthop. Relat. Res.. 1982;167:214-221.
Balint P.V., Kane D., McInnes I.B., et al. Ultrasonography of entheseal insertions in the lower limb in spondyloarthropathy. Ann. Rheum. Dis.. 2002;61:905-910.
Belt E.A., Kaarela K., Lehto M.U. Destruction and arthroplasties of the metatarsophalangeal joints in seropositive rheumatoid arthritis. A 20-year follow-up study. Scand. J. Rheumatol.. 1998;27:194-196.
Belt E.A., Kaarela K., Mäenpää H., et al. Relationship of ankle joint involvement with subtalar destruction in patients with rheumatoid arthritis. A 20-year follow-up study. Joint Bone Spine. 2001;68:154-157.
Benjamin M., McGonagle D. The anatomical basis for disease localisation in seronegative spondylarthropathy at entheses and related sites. J. Anat.. 2001;199:503-526.
Bhatt S.P., Handa R., Gulati G.S., et al. Peripheral vascular disease in systemic lupus erythematosus. Lupus. 2007;16:720-723.
Bicer A., Tursen U., Cimen O.B., et al. Prevalence of dermatophytosis in patients with rheumatoid arthritis. Rheumatol. Int.. 2003;23:37-40.
Borman P., Koparal S., Babaoglu S., et al. Ultrasound detection of entheseal insertions in the foot of patients with spondyloarthropathy. Clin. Rheumatol.. 2006;25:373-377.
Boutry N., Lardé A., Lapègue F., et al. Magnetic resonance imaging appearance of the hands and feet in patients with early rheumatoid arthritis. J. Rheumatol.. 2003;30:671-679.
Bouysset M., Tebib J., Tavernier T., et al. Posterior tibial tendon and subtalar joint complex in rheumatoid arthritis: magnetic resonance imaging study. J. Rheumatol.. 2003;30:1951-1954.
Bowen C.J., Dewbury K., Sampson M., et al. Musculoskeletal ultrasound imaging of the plantar forefoot in patients with rheumatoid arthritis: inter-observer agreement between a podiatrist and a radiologist. J. Foot Ankle Res.. 2008;1:5.
Briggs P.J. Controversies and perils. Reconstruction of the rheumatoid forefoot. The Stainsby operation. Tech. Orthop.. 2003;18:303-310.
Brostrom E., Haglun-Akerlind Y., Hagelbers S., et al. Gait in children with juvenile chronic arthritis. J. Rheumatol.. 2002;31:317-323.
Brouwer, R.W., Jakma, T.S., Verhagen, A.P., et al., 2005. Braces and orthoses for treating osteoarthritis of the knee. Cochrane Database Syst. Rev. 25 CD004020.
Carl A., Ross S., Evanski P., et al. Hypermobility in hallux valgus. Foot Ankle. 1988;8:264-270.
Chalmers A.C., Busby C., Goyert J., et al. Metatarsalgia and rheumatoid arthritis: a randomised single-blind, sequential trial comparing 2 types of foot orthoses and supportive shoes. J. Rheumatol.. 2000;27:1643-1647.
D’Agostino M.A., Said-Nahal R., Hacquard-Bouder C., et al. Assessment of peripheral enthesitis in the spondylarthropathies by ultrasonography combined with power Doppler. Arthritis Rheum.. 2003;48:523-533.
D’Agostino M.A., Ayral X., Baron G., et al. Impact of Ultrasound Imaging on Local Corticosteroid Injections of Symptomatic Ankle, Hind-, and Mid-Foot in Chronic Inflammatory Diseases. Arthritis Rheum.. 2005;53:284-292.
Dalbeth N., Clarke B., McQueen F., et al. Validation of a radiographic damage index in chronic gout. Arthritis Rheum.. 2007;57:1067-1073.
Dalbeth, N., Clark, B., Gregory, K., et al., August 15, 2008. Mechanisms of bone erosion in gout; a quantitative analysis using plain radiography and computed tomography. Ann. Rheum. Dis. Epub ahead of print.
Davys H.J., Turner D.E., Helliwell P.S., et al. Debridement of plantar callosities in rheumatoid arthritis: a randomized controlled trial. Rheumatology. 2005;44:207-210.
Davys H.J., Woodburn J., Bingham S.J., et al. Onychocryptosis (ingrowing toe nail) in patients with rheumatoid arthritis on biological therapies. Rheumatology. 2006;45(Suppl. 1):i171.
Davys H., Turner D.E., Helliwell P.S., et al. Foot ulceration in patients with rheumatic diseases. Ann. Rheum. Dis.. 2006;65(Suppl. II):669.
Falsetti P., Frediani B., Fioravanti A., et al. Sonographic study of calcaneal entheses in erosive osteoarthritis, nodal osteoarthritis, rheumatoid arthritis and psoriatic arthritis. Scand. J. Rheumatol.. 2003;32:229-234.
Ferrari J. A review of the foot deformities seen in juvenile chronic arthritis. The Foot. 1998;8:193-196.
Farrow S.J., Kingsley G.H., Scott D.L. Interventions for foot disease in rheumatoid arthritis: a systematic review. Arthritis Rheum.. 2005;53:593-602.
Finsterbush A., Pogrund H. The hypermobility syndrome. Musculoskeletal complaints in 100 consecutive cases of generalized joint hypermobility. Clin. Orthop. Relat. Res.. 1982;168:124-127.
Firth J., Hale C., Helliwell P., et al. The prevalence of foot ulceration in patients with rheumatoid arthritis. Arthritis Rheum.. 2008;59:200-205.
Firth J., Helliwell P., Hale C., et al. The predictors of foot ulceration in patients with rheumatoid arthritis: a preliminary investigation. Clin. Rheumatol.. 2008;27:1423-1428.
Fleming A., Crown J.M., Corbett M. Incidence of joint involvement in early rheumatoid arthritis. Rheumatol. Rehabil.. 1976;15:92-96.
Fransen M., Edmonds J. Off-the-shelf orthopedic footwear for people with rheumatoid arthritis. Arthrit. Care Res.. 1997;10:250-256.
Galluzzo E., Lischi D.M., Taglione E., et al. Sonographic analysis of the ankle in patients with psoriatic arthritis. Scand. J. Rheumatol.. 2000;29:52-55.
Gélis A., Coudeyre E., Aboukrat P., et al. Feet insoles and knee osteoarthritis: evaluation of biomechanical and clinical effects from a literature review. Annales de Réadaptation et de Médecine Physique. 2005;48:682-689.
Genc H., Cakit B.D., Tuncbilek I., et al. Ultrasonographic evaluation of tendons and enthesal sites in rheumatoid arthritis: comparison with ankylosing spondylitis and healthy subjects. Clin. Rheumatol.. 2005;24:272-277.
Gold R.H., Bassett L.W., Seeger L.L. The other arthritides. Roentgenologic features of osteoarthritis, ankylosing arthritis, psoriatic arthritis, Reiter’s disease, multicentric reticulohistiocytosis, and progressive systemic sclerosis. Radiol. Clin. N. Am.. 1988;26:1195-1212.
Gossec L., Pavy S., Pharm T., et al. Non-pharmacological treatments in early rheumatoid arthritis: clinical practice guidelines based on published evidence and expert opinion. Joint Bone Spine. 2006;73:396-402.
Gutman A.B. The past four decades of progress in the knowledge with gout, with assessment of the present status. Arthritis Rheum.. 1973;16:431-445.
Hall M.G., Ferrell W.R., Sturrock R.D., et al. The effect of the hypermobility syndrome on knee joint proprioception. Brit. J. Rheumatol.. 1995;34:121-125.
Harris M.D., Seigel L.B., Alloway J.A. Gout hyperuricemia. Am. Fam. Physician. 1999;59:925-934.
Helliwell P.S., Woodburn J., Redmond A.C., et al. The Foot and Ankle in Rheumatoid Arthritis. A Comprehensive Guide. London: Elsevier Limited; 2007.
Hendry, G.J., Gardner-Medwin, J.G., Watt, G.F., et al., July 10, 2008. A survey of foot problems in Juvenile Idiopathic Arthritis. Musculoskeletal Care [Epub ahead of print].
Hinman R.S., Payne C., Metcalf B.R., et al. Lateral wedges in knee osteoarthritis: what are their immediate clinical and biomechanical effects and can these predict a three-month clinical outcome? Arthritis Rheum.. 2008;59:408-415.
Huch K., Kuettner K.E., Dieppe P. Osteoarthritis in ankle and knee joints. Semin. Arthritis Rheu.. 1997;26:667-674.
Hyslop E., Turner D.E., McInnes I.B., et al. An outpatient survey of foot problems in psoriatic arthritis. Ann. Rheum. Dis.. 2008;67(Suppl. II):527.
Jeffrey R.C., Narshi C.B., Isenberg D.A. Prevalence, serological features, response to treatment and outcome of critical ischaemia in a cohort of lupus patients. Rheumatology. 2008;47:1379-1383.
Jernberg E.T., Simkin P., Kravette M., et al. The posterior tibial tendon and the tarsal sinus in rheumatoid flat foot: magnetic resonance imaging of 40 feet. J. Rheumatol.. 1999;26:289-293.
Kavlak Y., Uygur F., Korkmaz C., et al. Outcome of orthoses intervention in the rheumatoid foot. Foot Ankle Int.. 2003;24:494-499.
Keenan M.A., Peabody T.D., Gronley J.K., et al. Valgus deformities of the feet and characteristics of gait in patients who have rheumatoid arthritis. J. Bone Joint Surg. Am.. 1991;73:237-247.
Korda J., Balint G.P. When to consult the podiatrist. Bailliéres Best Pract. Res. Clin. Rheumatol.. 2004;18:587-611.
Kumar S., Gow P. A survey of indications, results and complications of surgery for tophaceous gout. N. Z. Med. J.. 2002;115:U109.
Kuroyanagi Y., Nagura T., Matsumoto H., et al. The lateral wedged insole with subtalar strapping significantly reduces dynamic knee load in the medial compartment gait analysis on patients with medial knee osteoarthritis. Osteoarthritis and Cartilage. 2007;15:932-936.
La Montagna G., Baruffot A., Tirri R., et al. Foot involvement in Systemic Sclerosis: A longitudinal study of 100 patients. Semin. Arthritis Rheu.. 2002;31:248-255.
Lehtinen A., Paimela L., Kreula J., et al. Painful ankle region in rheumatoid arthritis. Analysis of soft-tissue changes with ultrasonography and MR imaging. Acta Radiologica. 1996;37:572-577.
Martin L.J., Griffith S.M. High disease activity scores predict the need for additional health services in patients over 60 with rheumatoid arthritis. Musculoskeletal Care. 2006;4:1-11.
Mavidrou A., Klenerman L., Swann M., et al. Conservative management of the hindfoot in juvenile chronic arthritis. The Foot. 1991;1:139-143.
Michelson J., Easley M., Wigley F.M., et al. Foot and ankle problems in rheumatoid arthritis. Foot Ankle Int.. 1994;15:608-613.
Mizutani W., Quismorio F.P. Lupus foot: deforming arthropathy of the feet in systemic lupus erythematosus. J. Rheumatol.. 1984;11:80-82.
Moll J.M.H. Seronegative arthropathies in the foot. Baillière’s Clin. Rheumatol.. 1987;1:289-314.
Murley, G.S., Landorf, K.B., Menz, H.B., et al., October 13, 2008. Effect of foot posture, foot orthoses and footwear on lower limb muscle activity during walking and running: A systematic review. Gait Posture [Epub ahead of print].
Myerson M.S., Badekas A. Hypermobility of the first ray. Foot Ankle Clin.. 2000;5:469-484.
Olivieri I., Foto M., Ruju G.P., et al. Low frequence of axial involvement in Caucasian pediatric patients with seronegative enthesopathy and arthropathy syndrome after 5 years of disease. J. Rheumatol.. 1992;19:469-475.
Ostendorf B., Scherer A., Mödder U., et al. Diagnostic value of magnetic resonance imaging of the forefeet in early rheumatoid arthritis when findings on imaging of the metacarpophalangeal joints of the hands remain normal. Arthritis Rheum.. 2004;50:2094-2102.
Otter S., Robinson C., Berry H. Rheumatoid arthritis, foot infection and tumour necrosis factor alpha inhibition-a case history. The Foot. 2005;15:117-119.
Perry J. Gait analysis. Normal and pathological function. NJ. USA: Slack Incorporated; 1992.
Pham T., Maillefert J.F., Hudry C., et al. Laterally elevated wedged insoles in the treatment of medial knee osteoarthritis. A two-year prospective randomized controlled study. Osteoarth. Cartilage. 2004;12:46-55.
Premkumar A., Perry M.B., Dwyer A.J., et al. Sonography and MR imaging of posterior tibial tendinopathy. AJR Am. J. Roentgenol.. 2002;178:223-232.
Redmond A.C., Waxman R., Helliwell P.S. Provision of foot health services in rheumatology. Rheumatology. 2006;45:571-576.
Reilly P.A., Evison G., McHugh N.J., et al. Arthropathy of hands and feet in systemic lupus erythematosus. J. Rheumatol.. 1990;17:777-784.
Rodrigues P.T., Ferreira A.F., Pereira R.M., et al. Effectiveness of medial-wedge insole treatment for valgus knee osteoarthritis. Arthritis Rheum.. 2008;59:603-608.
Sahin N., Baskent A., Cakmak A., et al. Evaluation of knee proprioception and effects on proprioception exercise in patients with benign joint hypermobility syndrome. Rheumatol. Int.. 2008;28:995-1000.
Sahin N., Baskent A., Ugurlu H., et al. Isokinetic evaluation of knee extensor/flexor muscle strength in patients with hypermobility syndrome. Rheumatol. Int.. 2008;28:643-648.
Saltzman C.L., Salamon M.L., Blanchard G.M., et al. Epidemiology of ankle arthritis. Iowa Orthop. J.. 2005;25:44-46.
Sari-Kouzel H., Hutchinson C.E., Middleton A., et al. Foot problems in patients with systemic sclerosis. Rheumatology. 2001;40:410-413.
Saunders S., Longworth S. Injection techniques in orthopaedics and sports medicine. A practical manual for doctors and physiotherapists, third ed. Edinburgh: Elsevier; 2006. p7
Semple R., Turner D.E., Helliwell P.S., Woodburn J. Regionalised centre of pressure analysis in patients with rheumatoid arthritis. Clin. Biomech. (Bristol, Avon). 2007;22:127-129.
Semple, R., Newcombe, L.W., Finlayson, G.L., et al., September 17 2008. The FOOTSTEP self-management foot care programme: Are rheumatoid arthritis patients physically able to participate? Musculoskeletal Care [Epub ahead of print].
Shakoor N., Lidtke R.H., Sengupta M., et al. Effects of specialized footwear on joint loads in osteoarthritis of the knee. Arthritis Rheum.. 2008;59:1214-1220.
Shereff M.J., Baumhauer J.F. Hallux rigidus and osteoarthrosis of the first metatarsophalangeal joint. J. Bone Joint Surg. Am.. 1998;80:898-908.
Spraul G., Koenning G. A descriptive study of foot problems in children with juvenile rheumatoid arthritis (JRA). Arthrit. Care Res.. 1994;7:144-150.
Theodoridou A., Bento L., D’Cruz D.P., et al. Prevalence and associations of an abnormal ankle-brachial index in systemic lupus erythematosus: a pilot study. Ann. Rheum. Dis.. 2003;62:1199-1203.
Turner D.E., Helliwell P.S., Emery P., et al. The impact of rheumatoid arthritis on foot function in the early stages of disease: a clinical case series. BMC Musculoskelet. Disord.. 2006;7:102.
Turner D.E., Helliwell P.S., Siegel K.L., et al. Biomechanics of the foot in rheumatoid arthritis: identifying abnormal function and the factors associated with localised disease ‘impact’. Clin. Biomech. (Bristol, Avon). 2008;23:93-100.
Turner D.E., Woodburn J. Characterising the clinical and biomechanical features of severely deformed feet in rheumatoid arthritis. Gait Posture. 2008;28:574-580.
Valderrabano, V., Horisberger, M., Russell, I., et al., October 2, 2008. Etiology of ankle osteoarthritis. Clin. Orthop. Relat. Res. [Epub ahead of print].
Williams A., Meacher K. Shoes in the cupboard: the fate of prescribed footwear? Prosthet. Orthot. Int.. 2001;25:53-59.
Williams A.E., Nester C.J., Ravey M.I. Rheumatoid arthritis patients’ experiences of wearing therapeutic footwear – a qualitative investigation. BMC Musculoskelet. Disord.. 2007;8:104.
Williams A.E., Rome K., Nester C.J. A clinical trial of specialist footwear for patients with rheumatoid arthritis. Rheumatology. 2007;46:302-307.
Witemeyer S., Ansell B.M., Ashburn A., et al. Gait analysis: a pilot study- a possible mode of assessment of lower limb function in juvenile chronic arthritis. Rheumatol. Rehabil.. 1981;20:31-37.
Woodburn J., Barker S., Helliwell P.S. A randomized controlled trial of foot orthoses in rheumatoid arthritis. J. Rheumatol.. 2002;29:1377-1383.
Woodburn J., Stableford Z., Helliwell P.S. Preliminary investigation of debridement of plantar callosities in rheumatoid arthritis. Rheumatology. 2000;39:652-654.
Woodburn J., Nelson K.M., Siegel K.L., et al. Multisegment foot motion during gait: proof of concept in rheumatoid arthritis. J. Rheumatol.. 2004;31:1918-1927.
Woodburn J., Cornwall M.W., Soames R.W., et al. Selectively attenuating soft tissues close to sites of inflammation in the peritalar region of patients with rheumatoid arthritis leads to development of pes planovalgus. J. Rheumatol.. 2005;32:268-274.