INTRODUCTION
The initial, most important step in achieving a satisfactory consultation and management of any dermatological condition is to obtain a thorough history. Taking short cuts in this step can lead to a misdiagnosis, affect the welfare of the animal, and add a lot of unnecessary expense and dissatisfaction for the owner.
The history should be obtained in a logical fashion, with the view of building up a picture of the condition and a list of differential diagnoses, while examining the patient. This book shows how to work up a case in this manner.
With computerized records in most practices, the age at onset, breed and sex of the individual animal should be readily available. This information provides some useful clues when formulating a list of differential diagnosis.
Age at onset:
•
Parasitic problems such as pediculosis, otoacariasis, cheyletiellosis and demodectic mange are more commonly seen in puppies and adolescent animals.
•
Genodermatoses can become progressive and, in some cases, are more apparent with age. They are usually established by 3 years of age.
•
Of the allergies, atopic dermatitis has an age of onset of more than 6 months and below 3 years, and flea allergic dermatitis is more common in animals older than 5 years of age.
•
Hormonal problems tend to manifest after the age of 6 years.
•
Neoplastic conditions generally occur in older animals.
Breed predispositions:
•
Demodicosis in Staffordshire bull terriers, Scottish terriers.
•
Atopic dermatitis in Labradors, West Highland terrier and other terrier breeds, German shepherd dogs, whereas flea allergic dermatitis can occur in any breed.
•
Dermatophytosis is more prevalent in Persian cats.
•
Dilute coat colour in certain breeds, i.e. blue coat in Dobermanns may be responsible for colour dilution alopecia.
Sex: Note whether the individual is entire or neutered. This is of particular interest when dealing with skin conditions associated with sex-hormone imbalance. There are few other skin conditions where sexual predispositions are recognized.
HISTORY TAKING
History taking is divided into those enquiries that relate specifically to the skin’s condition and those about the general history and management of the animal. In general practice, because time is limited, you could combine some of the questioning with the examination of the animal. If the condition is recurrent, much of the history will already be available on records and will just need confirmation from the owner.
Specific history – key questions:
•
Is the condition seasonal or non-seasonal?
•
If non-seasonal is it continuous and progressive or is it intermittent?
•
Is the condition pruritic or non-pruritic? This should include licking, biting, scratching or rubbing. If pruritic, we need to know whether initially non-pruritic and subsequently changed or has always been pruritic.
•
Distribution of the lesions now, and initially, and how they have progressed?
•
Is there a smell associated with the condition?
•
Are there any in-contact animals in the house or casual contacts and if so are they affected?
•
Are any people in the house affected?
•
Did the condition start following a visit to the grooming parlour, or to boarding kennels?
•
Are there any fleas on any of the pets in the house?
Non-specific history: You should include questions relating to the animal’s general health and management, and you may need to ask more specific questions as you build up a picture of the condition.
General health – key questions:
•
Is the appetite affected and, if so, has it increased or decreased?
•
Has there been any change in water intake?
•
Has the exercise tolerance changed?
•
Is there any cough, sneezing or breathing difficulty?
•
Have there been signs associated with gastroenteric disorders?
•
Are sexual behaviours or oestrus cycle affected?
•
Is the animal on any medication for any other conditions, i.e. cardiac, arthritic?
Management – key questions:
•
Diet, including titbits, should be noted.
•
Is the animal kennelled or kept indoors, and if so where does it spend most of its time? For example, those sleeping in bedrooms would have higher exposure to house dust mites.
•
Is the dog a pet or used to work?
•
Is the cat kept indoors and/or outdoors and if outdoors is it a hunter?
•
What sort of bedding is used?
•
Is the house carpeted or not?
•
Is the condition worsened after contact with certain things? For example, grass or after a walk.
•
Topical and systemic treatments used and response.
•
Travel history, ectoparasitic, endoparasitic and vaccination status.
CLINICAL EXAMINATION
For the clinical examination, it is good practice to establish a routine to include both a general physical and a specific dermatological examination.
General physical examination: All organ systems should be examined in a methodical manner. Certain abnormalities may be indicative of certain diseases:
•
Bradycardia may be suggestive of hypothyroidism.
•
Oral lesions may be consistent with autoimmune, immune-mediated or neoplastic conditions.
•
Conjunctivitis or epiphora may suggest an allergic aetiology.
•
Muscle atrophy is suggestive of either spontaneous or iatrogenic hyperadrenocorticism.
•
Abdominal palpation may reveal a mass or other abnormality.
Dermatological examination: The examination involves a detailed inspection of the skin based on visual inspection and palpation followed by specific procedures such as coat brushings, skin scrapings, etc. (see Chapter 2). You are looking for different indicators from the different parts of the skin:
•
Mucous membranes – petechiae, ulceration, vesicles, bulla, erosions, hypopigmentation.
•
Coat condition – lustreless, greasy, matted, scaly, dry and brittle or alopecic.
•
Elasticity of the skin – loss of elasticity is associated with hyperadrenocorticism.
•
Skin surface – examine for lesions on the entire skin surface, not just the obviously visible area. Distinguish between primary and secondary lesions and note the distribution (focal or multifocal; symmetrical or asymmetrical). The lesions may be present singly or grouped, or in annular, linear, polycyclic, arciform or serpiginous configurations. In some animals, the coat may need to be clipped to appreciate the lesions.
Primary lesions:
•
Macule – flat, circumscribed area of discoloration of 1 cm or less.
•
Papule – solid, raised palpable mass of 1 cm diameter or less (
Fig. 1.1).
•
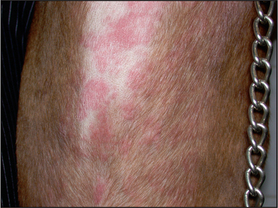
Plaque – solid, raised elevation of more than 1 cm diameter (
Fig. 1.2).
•
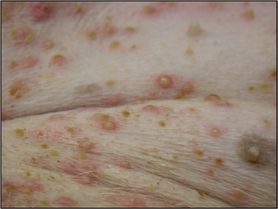
Pustule – pus-filled, raised circumscribed lesion of 1 cm or less (
Fig. 1.3).
•
Vesicle – serum-filled, raised circumscribed lesion of 1 cm or less (
Fig. 1.4).
•
Bulla – serum-filled, raised circumscribed lesion of more than 1 cm.
•
Cyst – cavity which is lined with membranous lining and is filled with fluid or semi-solid material.
•
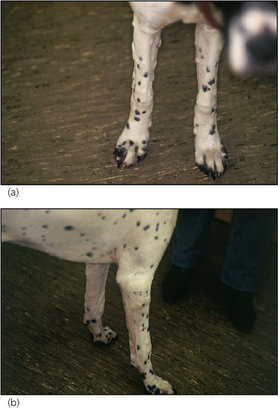
Nodule – solid, raised palpable mass of more than 1 cm (
Fig. 1.5).
•
Tumour – large palpable mass.
•
Wheal – oedematous, raised circumscribed lesion which blanches on diascopy (
Fig. 1.6).
•
Alopecia – loss of hair (this can be primary or secondary, i.e. self-induced).
Secondary lesions:
•
Erythema – increased redness to the skin.
•
Scale – superficial visible accumulation of loose corneocytes on the surface of the epidermis.
•
Epidermal collarette – circular arrangement of scale with a central area of hyperpigmentation (
Fig. 1.7).
•
Crust – results from accumulation of dried cells and exudate (e.g. serum, blood, pus) on the skin surface (
Fig. 1.8).
•
Erosion – loss of the superficial epidermis without the loss of the basal layer (
Fig. 1.9).
•
Ulceration – loss or the epidermis resulting in exposure of the dermis (
Fig. 1.10).
•
Fissure – a split or crack into the epidermis and dermis due to either trauma or disease.
•
Scar – abnormal fibrous tissue which replaces damaged dermal and subcutaneous tissue.
•
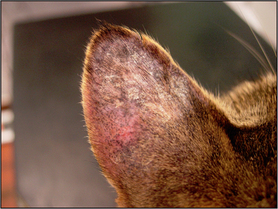
Lichenification – thickening of the skin resulting in exaggeration of the skin markings due to chronic inflammation (
Fig. 1.11).
•
Hyperpigmentation – darkening of the skin due to increased pigment in the epidermis and sometimes the dermis (
Fig. 1.11).
•
Hypopigmentation – reduction or loss of pigment in the epidermis.
•
Comedone – dilated hair follicle blocked with sebum and other cellular debris (
Fig. 1.12).
•
Follicular cast – accumulation of keratin and sebum on the hair shaft and/or the hair bulb (
Fig. 2.9).
Although all of the above are normally considered as secondary lesions, erythema, scale, crusts, comedones, follicular casts, hypopigmentation and hyperpigmentation may, in some skin conditions, be regarded as primary lesions.
It is good practice to examine the animal using a set procedure so that no part of the skin goes unchecked.
Unless the diagnosis is immediately obvious, which in the majority of cases it isn’t, the next step is to list all the conditions consistent with the signalment, history and examinations – the ‘differential diagnosis’ – and then eliminate them by appropriate testing and therapeutic trials, to come to a definitive diagnosis. These tests and trials are discussed in Chapter 2.