4 Sarcoptic mange
INTRODUCTION
Sarcoptic mange (also referred to as scabies) is a highly contagious, intensely pruritic and potentially zoonotic skin condition, due to an infestation of the skin by a sarcoptid mite Sarcoptes scabiei var. canis. The presenting signs of pruritus – papules, crusting, scaling, erythema and self-induced alopecia – are often confused with other dermatological conditions, such as staphylococcal pyoderma, allergic skin diseases or other ectoparasitic diseases.
CASE HISTORY
All dogs present with a history of intense pruritus, which in most cases fail to respond to increasing doses of glucocorticoids. The onset of pruritus tends to be sudden and severe, and the animal is usually presented shortly after onset, unless the individual has been intermittently treated with ectoparasiticidal products. A history of indirect contact with foxes is usually noted, especially in urban and suburban areas of the UK. Sarcoptic mange is contagious and of zoonotic importance, and evidence of contagion and zoonosis may come to light during the history taking.
The history in this case was as follows:
CLINICAL EXAMINATION
The clinical signs can range from subtle lesions with marked pruritus to severe lesions. The primary lesions include erythematous and/or crusted papules, and secondary lesions include crusts, lichenification, scaling and hyperpigmentation. Initial lesion distribution tends to be on the ear margins, elbows, sternum and the hocks. If untreated the lesions can become widespread and often affect the demeanour of the dog, as in this case.
The physical and dermatological examination revealed:



CASE WORK-UP
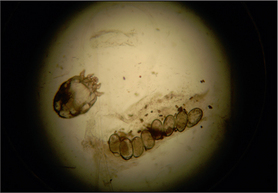
The demonstration of a mite, eggs or faecal pellets on deep skin scrapes confirms the diagnosis but this test is only positive in around 50% of cases of canine scabies despite examination of scrapings from multiple sites. In those cases where mites are not seen, but the history and clinical signs are suggestive of infestation, a serological test to demonstrate the presence of anti-Sarcoptes IgG may further support the diagnosis. This test is reported to have sensitivity ranging between 83% and 92%, and specificity ranging between 89.5% and 92%.
The following tests were performed:
Flea allergic dermatitis remained a possible concurrent problem, given the distribution of the lesions. If the response to treatment for the sarcoptic mange and staphylococcal pyoderma were partial, one would need to either do further tests or monitor response to ongoing aggressive flea control.
Investigations into thyroid function were deferred, as the dog had been treated with prednisolone, which would affect the results. The test was performed after 8 weeks and was found to be within normal limits. The diagnoses of pemphigus foliaceus, sebaceous adenitis and cutaneous epitheliotropic lymphoma would be confirmed or ruled out by histopathological analysis of multiple skin biopsies but the first step was to treat the scabies. In this case, because of the complete response to the treatment, it was not necessary to subject the dog to further investigations.
DIAGNOSIS
A diagnosis of sarcoptic mange and secondary staphylococcal pyoderma was made based on the results of the skin scrapes and cytology.
PROGNOSIS
The prognosis is usually excellent for this condition provided there are no sources for re-infestations.
AETIOPATHOGENESIS OF SARCOPTIC MANGE
Sarcoptid mites belong to the family Sarcoptidae and are small (200–400 μm) and globose in shape. The mites mate in a moulting pocket on the surface of the skin and the fertilized female then burrows through the stratum corneum, laying eggs in a tunnel behind her. The eggs hatch into larvae and then nymphs, which burrow back to the surface of the skin to feed, or remain in a moulting pocket until they are mature. The life cycle of the mite is 17–21 days. Mites tend initially to infest sparsely haired areas such as the elbow, hock, convex aspects of the pinnae and the ventrum.
The sarcoptid mite is a source of multiple antigens to which the host is exposed as it feeds, burrows and defecates. Exposure to the antigens induces humoral and cell-mediated immune responses. Even though spontaneous resolution is reported, most infected dogs go on to develop intense pruritus and lesions, caused by the burrowing of the mite in the epidermis and to a hypersensitivity reaction.
EPIDEMIOLOGY
The condition has a worldwide distribution, can occur at any time of the year, tends to be continuous and worsens over time. Even though the mite is an obligate parasite, it can survive, depending on the environmental temperature and humidity, off the host for up to 19 days. The incidence depends on contact with infected animals, fomites such as grooming implements, infected kennels (especially rescue kennels) and, in the UK, indirect contact with foxes would also appear to be a problem.
There is no age, breed or sex predisposition. Although infestation usually starts on lesser haired areas, it can become generalized and affect large areas of the body.
The infestation can spread to other dogs and in-contact humans. When exposed to an infested dog, people can develop a papular rash in areas of contact, such as the arms and the trunk, within 24 hours. These lesions tend to regress spontaneously once the affected animals are treated.
TREATMENT OPTIONS
Currently amitraz, moxidectin and selamectin are the only licensed preparations for sarcoptic mange in the UK. Moxidectin and selamectin are applied topically to the skin, through which they are absorbed. Most clinicians now favour these agents because of the ease of application and to avoid clipping the patient. The key to successful resolution is the concurrent treatment of both the in-contact animals and the environment.
Amitraz: Amitraz is licensed as a topical sponge-on preparation, applied every 7 days for 2–6 weeks. It exerts its effect by inhibiting monoamine oxidase. Clipping long-haired animals is advised prior to application of the product. It is contraindicated in chihuahuas at any age, in puppies less than 12 weeks of age and in nursing bitches. The product is toxic to fish and the manufacturer’s guidelines should be followed. The side-effects of amitraz are transient sedation, lethargy, slow shallow breathing and bradycardia. These symptoms usually last for 24 hours, but if they persist, they can be reversed by the α2-adrenoreceptor antagonist atipamezole at the dose of 0.2 mg/kg, or the dog can be washed with a mild soap. Amitraz should not be handled by diabetic owners, as it could cause transient hyperglycaemia.
Moxidectin: Moxidectin is a second-generation systemic macrocylic lactone with broad-spectrum antiparasitic activity. It interacts with γ-aminobutyric acid (GABA) and the glutamate-gated chloride channels at the postsynaptic junctions, allowing an influx of chloride ions resulting in flaccid paralysis and death of the parasite. Moxidectin (2.5%) combined with imidacloprid is available as a spot-on preparation for the treatment of sarcoptic mange in puppies and dogs over 7 weeks of age. After topical application, moxidectin is absorbed percutaneously and reaches maximum plasma concentration after 4–9 days. The recommended dose is 2.5 mg/kg of moxidectin to be applied twice 4 weeks apart. Moxidectin is tolerated by collies and collie crosses; however, accidental ingestion in sensitive dogs can cause vomiting, salivation and transient neurological signs, such as ataxia, tremors, dilated pupils and nystagmus. Moxidectin is also reported to be toxic to aquatic organisms and therefore it should not be allowed to enter water.
Selamectin: Selamectin, a novel avermectin, is another safe broad-spectrum topical antiparasitic drug licensed for sarcoptic mange. It is easy to apply and is recommended for use at 6–12 mg/kg twice 30 days apart. Some dermatologists recommend applying the product three times at 14-day intervals. This advice is based on anecdotal reports of an improved response. However, even though the margin of safety is good, the owners should be warned of the extra-label use.
Milbemycin oxime: Three doses of milbemycin oxime given orally at 2 mg/kg every 7 days has been reported to have a variable efficacy ranging from 71% to 100%. It is available as a heartworm preparation in some countries and is not licensed for sarcoptic mange. It is expensive but can be used as a much safer alternative to ivermectin in ivermectin-sensitive dogs.
Ivermectin: Ivermectin given orally at 0.2–0.4 mg/kg three times 7 days apart, or injected subcutaneously twice 14 days apart, is effective against the mite. However, it is not licensed and is potentially toxic in ivermectin-sensitive breeds such as collies, collie crosses and other sheepdogs. The adverse effects include ataxia, tremors, dilated pupils, nystagmus, salivation, depression, coma and death.
Environmental treatment
The sarcoptic mite is able to survive in the environment, which can be a source of re-infestation. Because the dogs are intensely pruritic and scratch a lot, they often leave scale, crusts and hairs containing mites in the environment. Thorough vacuuming and the application of an acaricidal preparation are recommended as part of the treatment.
Treatment in this case
In this case the sarcoptic mange was treated with moxidectin combined with imidacloprid three times, 2 weeks apart (Figs 4.5 and 4.6) The staphylococcal pyoderma resolved with 6 weeks of cefalexin (20 mg/kg). The environment was treated with a permethrin spray. There was complete response to the treatment and all the hair had regrown within 8 weeks (Fig. 4.7).



Most dogs with chronic sarcoptic mange require an Elizabethan collar to prevent self-trauma. If the animal has been admitted into the surgery and kennelled whilst investigations are carried out, nurses must remember to clean the kennel thoroughly using an environmental ectoparasiticide spray before the kennel is used again. Clippers etc. and any potentially infected surfaces must also be thoroughly cleaned. Potentially infected dogs should be kept away from other animals in the waiting room.
The prevalence of the disease varies with areas and therefore local knowledge of the area is useful. History of recent contact with foxes or rolling in fox faeces should alert the clinician. Often, individuals show a pinnal scratch reflex. In some cases the lesions may be subtle, especially if the individual has been regularly bathed or is being intermittently treated with flea preparations, which include miticidal drugs.
To increase the chance of demonstrating the mite on skin scraping, choose an untraumatized area with heavy scaling or crusted papules (usually the ear pinna or the elbow) to scrape. Scrape a wide area and collect all the material onto the slide. Allowing the slide to warm by the microscope light often activates the mite, making it easier to find. Placing a coverslip on the sample provides an even surface and makes it easier to see. Scan the entire slide under a ×4 or ×10 objective. Always treat all the in-contact dogs at the same time.