Chapter 36 Consequences of digital imaging in radiography
Chapter contents
36.1 Aim
The aim of this chapter is to introduce the reader to the principal consequences of digital imaging in radiography.
36.2 Image processing
The analogue image produced on a film is not capable of further processing. The digital image, however, is capable of undergoing a number of processes which aid image interpretation. These will now be discussed.
36.2.1 Data clipping
The X-ray pattern which hits the imaging plate covers a wide range of exposures. Processing all this data into an image would produce an image of very low contrast which would make image interpretation difficult. For this reason, an algorithm is applied to the image depending on the area of the body selected by the radiographer when inputting the patient data. This algorithm discards data which are not of clinical interest to the examination and so increases the contrast of the image produced. The effect of this ‘data clipping’ is shown in Figure 36.1.
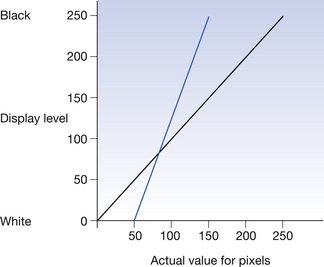
Figure 36.1 Graph to show the effect of ‘data clipping’ on the contrast. The contrast is represented by the gradient of the coloured line. The black line shows the image as it would be displayed without data clipping. The blue line shows the data as displayed if only pixels with a value between 50 and 150 are used to produce the image. Note the increase in gradient compared to the blue line.
36.2.2 Plate sensitivity
Once the system has clipped the data to data of clinical interest, it then has to correct the image for overall exposure. This is possible because of the linear response of the imaging plates to exposure. This is done by applying a formula which defines the average exposure within the clinically useful range. This is given a different name by different manufacturers – S number (Fuji), Exposure index (Kodak), LogM (Agfa), etc. Thus, if the plate has been overexposed, an image can be produced which has the correct density range displayed on the monitor. The principles behind this are illustrated in Figure 36.2.
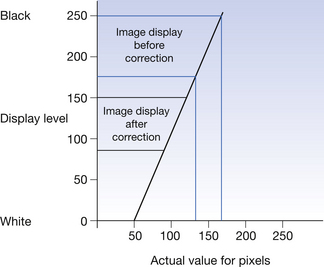
Figure 36.2 Graph to show the effect of altering the plate sensitivity. The original image (shown by the blue lines) has been overexposed and so would produce an image towards the black end of the display range. The corrected image is more in the centre of the display range and so is easier to interpret.
36.2.3 Edge enhancement
It is possible to enhance the edges of structures displayed on the digital image. This sometimes makes it easier to see subtle structures like hairline fractures or small catheters in the mediastinum.
36.2.4 Magnification
Because of the digital nature of the image, it is possible to magnify either the whole image or a part of the image.
36.2.5 Image annotation
With the appropriate software, it is possible to annotate the image. This can be a useful tool either to point out structures or to add anatomical data for teaching purposes.
36.2.6 Image stitching
Because of the size limitation of the digital imaging plates (usually about 50 cm×50 cm), it is impossible to image the whole of the spine as a single image – this may be useful in the imaging of scoliosis. It is, however, possible to take a number of images with the patient in the same position and then to use the software to ‘stitch’ the images together to produce a composite image. Similar techniques are utilized in lower limb measurement and also for display of the blood supply to the lower limb.
36.3 Image storage and retrieval
Because of the digital nature of the image data, there are a number of possibilities for image storage and retrieval. In most cases, the image is stored as part of a picture archival and communication system (PACS) which will be discussed in more detail in the next section of the chapter. This presents a number of possibilities and challenges in terms of the storage and retrieval of this data.
36.3.1 Patient demographics
In order that the correct images are stored and retrieved from the correct files, it is crucially important that the correct patient demographic data are entered into the system. Different systems require different inputs and these can usually be entered from barcode readers or other input devices. In many cases, an important identifier is the patient’s NHS number which is a unique identification number given, centrally, to each NHS patient. The same precise data must be entered for the patient each time he/she is examined – e.g. if on one occasion the patient is identified as ‘John Smith’ and on the next occasion he is identified as ‘John S. Smith’, then the system will treat these as two separate patients and will allocate separate files.
36.3.2 Sign on and password
The security of data in the store is important both in terms of patient confidentiality and to prevent unauthorized altering of the data. For this reason, most systems require the operator to sign on to the system (usually from a card with a magnetic strip) and to enter an appropriate password. This password may have an expiry date on it. When the person is identified by the signing on signature and password, the system will then give access only to appropriate data.
36.3.3 Bedside image retrieval
There are some situations where it is useful to review images of a patient at that patient’s bedside. An example of this may be in the intensive therapy unit (ITU). By having the appropriate monitor and connections systems, it is possible for staff to review images and reports at the bedside. This can be very helpful when images are used to monitor the efficacy of a specific therapy.
36.3.4 Case conferences and teleconferences
When the image is recalled from the image store, it is possible to display this image on a number of monitors simultaneously. This means that a patient may be discussed in a case conference where the staff involved may not be in the same location or even in the same hospital. This facility is especially useful where the possibility of transferring a patient from one hospital to another is being discussed.
36.3.5 Teleradiology
Because the digital image can be transmitted from one site to another by any secure link then it is possible for images produced in one location to be reported by a radiologist or a radiographer in another location. This facility is extremely useful where the geographical spread of hospitals is great or when a second opinion is required outwith normal working hours.
36.4 Picture archiving and communications systems (PACS)
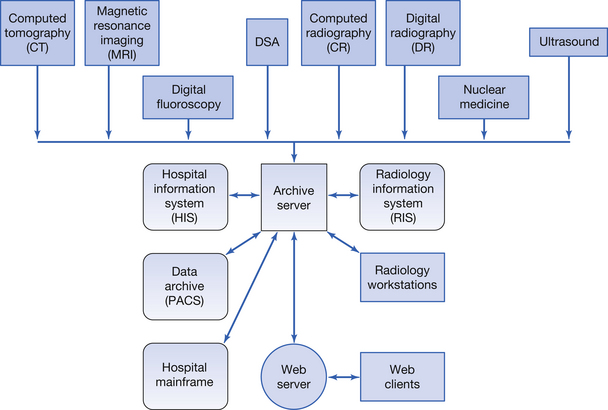
Figure 36.3 shows the structure of a typical PACS system. The system is centred around the archive server. Various imaging modalities (or input modules), e.g. digital radiographic (DR), can input data to this server. This image can then be acquired by a radiology workstation where the image appearances are reported. The image and the report are then returned to the archive server. Information from the hospital information system (HIS) can be acquired via the archive server – this could be information required for the image report, e.g. the patient’s blood pressure. Similarly, information is available through the archive server from the radiology information system (RIS) – this could be something like a list of any other radiological examinations booked for this patient. Data from the archive server can be sent to remote locations, e.g. peripheral hospitals, via the web server. After an appropriate time, data are transferred from the archive server to the data archive for-long term storage. Because the various components of a PACS must be able to ‘speak to each other’ then it is important that they comply with Digital Imaging and Communications in Medicine (DICOM) compatibility. This means that, for example, the RIS may be from a different manufacture to the HIS but both systems are still able to communicate.
36.5 Digital imaging and communication in medicine (DICOM)
DICOM is a global information technology standard which allows network communication between the various components of a PACS. The DICOM standard covers the handling, storage and transmission of medical information. The DICOM statements were originally written by the National Electrical Manufacturers Association (NEMA) in 1985 and these statements have been modified since then. NEMA still holds the copyright for the DICOM statements. All manufacturers of digital medical imaging equipment boast DICOM compatibility but the statements must be read carefully to determine the extent of the compatibility. If the DICOM standard is properly applied, then scanners, servers, workstations, printers and network hardware from different manufacturers can be incorporated into a PACS.
In this chapter, you should have learnt the following:
• The possibilities for image processing presented because of digital imaging (see Sect. 36.2).
• Methods of Image Storage and Retrieval (see Sect. 36.3).
• The basis of a PACS and its purpose in Radiology (see Sect. 36.4)
• The importance of DICOM compatibility for components of a PACS (see Sect. 36.5).
Further reading
There are many sites on the Internet where the manufacturers of digital equipment give information on their specific technologies. In addition, you may find the following useful.
Carter C.E., Veale B.L. Digital Radiography and PACS. Missouri: Mosby Elsevier, 2008.
Siegel E.L., Kolodner R.M. Filmless Radiology. New York: Springer, 1999.