Chapter 17 Dysfunctional breathing
INTRODUCTION
To breathe is the bedrock of our mortal life. It is the activity on which our physiological and our psychological being depends. Most of the time we are unaware of breathing, yet as soon as something physical or psychological causes it to change, it immediately impinges on our conscious sense of well-being and causes a range of sensations from discomfort, through dyspnoea, to fear of death. This chapter looks in detail at some aspects of overbreathing, or hyperventilation and the reordering of this disordered pattern. It will also consider more briefly the re-education of disordered breathing patterns in asthma and emphysema and in relation to musculoskeletal dysfunction.
The term ‘dysfunctional breathing’ is, in itself, confusing. One would expect it to mean that a particular breathing pattern does not fulfil its function, yet it appears to be used as a synonym for hyperventilation. In a review Morgan (2002) remarks on ‘this new term’, that:
‘Dysfunctional breathing is therefore just the latest imprecise description of a behaviour and symptom-complex which remains unexplained … definition of dysfunctional breathing and methods for identifying it require careful validation’
Since the previous edition of this book, the term dysfunctional breathing has become more popular. Papers relating to dysfunctional breathing in asthma and chronic obstructive pulmonary disease (COPD) have been published and the work relating to hyperventilation has become more varied. A deeper understanding of how musculoskeletal dysfunction can restrict the normal free pattern of breathing is resulting in new approaches to treatment.
However, there is still no clear understanding of the relationships between the psychological, anatomical, physiological, pathological and behavioural variables as they appear to affect the central breathing pattern generator and/or disrupt the physical movements of breathing in differing ways.
CONTROL OF BREATHING
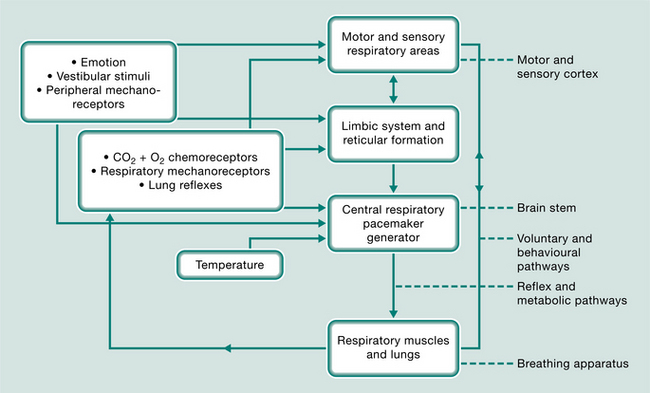
The respiratory system is the only autonomic function that can be controlled voluntarily. This complex system (Fig. 17.1) is self-sustaining and is centred on the respiratory-pacemaker-generator in the brain stem. It is moderated by oxygen and carbon dioxide chemoreceptors, lung tissue reflexes, mechanoreceptors in the ventilatory and the peripheral muscles and joints, emotion, temperature and vestibular influences. This sensory feedback may be filtered through, and integrated by, the reticular formation and limbic autonomic system or be transmitted directly to the breathing centre. Voluntary and behavioural stimuli from the cerebral cortex also feed back to the breathing centre and can influence the respiratory muscles directly by bypassing or overriding the reflex pathways. The cerebral cortex is also responsible for perceiving dyspnoea. Adaptation of any of the components of these motor or sensory pathways or centres of respiration could influence or concentrate disordered responses, breathing patterns and carbon dioxide levels. This results, in time, in what appears to be a resetting of the respiratory centre’s triggering mechanisms and the formation of new conditioned patterns of breathing.
Why are some people more prone to respond to physiological, psychological or environmental stimuli with grossly altered breathing patterns? Clark & Cochrane (1970), considering patients with chronic bronchitis and emphysema, concluded that the sensitivity of the respiratory centres is personality linked and related to mood-state and disposition. Papp et al (1993) discuss the theory of an inherently unstable autonomic nervous system and a hypersensitive respiratory control system. Cowley & Roy-Byrne (1987) suggest that this underlying biological and often inherited vulnerability, leading to a hypersensitive central nervous ‘alarm system’, may be triggered inappropriately, causing a premature ‘fight or flight’ response.
HYPERVENTILATION
Hyperventilation may be acute, it may coexist with organic disease or may occur in a chronic idiopathic form. In the past few years, together with ongoing research into the relationships between hyperventilation and panic disorders, researchers and practitioners have noted strong relationships between hyperventilation and vestibular and musculoskeletal disorders. These findings have now influenced some treatment programmes and investigative procedures.
Acute hyperventilation
Acute hyperventilation or breathing in excess of metabolic requirements results in a lowering of alveolar partial pressure of carbon dioxide PACO2), arterial partial pressure of carbon dioxide PaCO2) and a respiratory alkalosis. It is a normal response to pain or psychological or emotional states such as stress, anxiety, anger or fright. It may result in self-regulatory paraesthesia, dizziness, palpitation and, in extreme circumstances, tetany.
Chronic hyperventilation
The chronic fluctuating disorder of chronic hyperventilation or idiopathic hyperventilation is difficult to define. It has been characterized as:
‘… sustained arterial and alveolar hypocapnia [commonly to levels below 30 mmHg] with no discernable aetiology’
‘… a physiological response to abnormally increased respiratory “drive” which can be caused by a wide range of organic, psychiatric and physiological disorders or a combination of these’
Clinically it can be recognized by the spontaneous occurrence of multiple and alarming symptoms.
In 1937 Kerr et al described a group of patients who, in addition to their anxious tensional state, presented with:
‘… a variety of symptoms referable to many structures in the body; and in whom hyperventilation precipitates and maintains a state of hyperirritability’
In the table of their laboratory work they coined the term ‘hyperventilation syndrome’ (Kerr et al 1937). A syndrome is, by definition, identified by its combination of symptoms and is therefore not able to be contained within a single diagnostic measurement. The difficulty regarding the understanding of the various mechanisms producing the symptoms, of finding a definitive form of diagnostic test and agreeing a more appropriate name for this disorder, is still creating some discussion in the literature, as views change regarding the possible causes and effects (Gardner 2000, Hornsveld et al 1996, Howell 1997, Malmberg et al 2000, Troosters et al 1999). Howell (1997) and Tweeddale et al (1994) considered that ‘behavioural breathlessness’ may be a more appropriate term, but as many patients do not experience breathlessness as their main symptom (if at all) Howell considered at the time, that there was nothing to be gained by changing the name.
Although anxiety was a component in Kerr’s original description of hyperventilation syndrome, anxiety is not always present. Also, there may not always be a hyperventilation component in anxiety. With no universally agreed term for this subtle form of chronically disturbed breathing, the terms hyperventilation syndrome (HVS), idiopathic symptomatic hyperventilation (IH) and behavioural breathlessness continue to be used.
HYPERVENTILATION SYNDROME
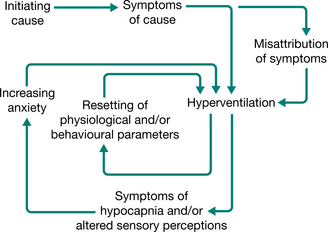
The diagnosis was not uncommon in the past (Baker 1934, Wood 1941) but in the present technological era, hyperventilation in its various chronic recurrent forms often tends to go unrecognized and the diverse symptoms are labelled as functional. Even though it has been shown that severe chronic hyperventilation with profound hypocapnia can be present in the absence of psychiatric, respiratory or other organic abnormalities (Bass & Gardner 1985), patients may attend a succession of clinics, presenting with increasingly disturbing symptoms and yet receive little help. The new anxiety aroused by the situation increases the hyperventilation–anxiety spiral, which may already be in operation. The spiral may be perpetuated by physiological and/or psychological causes, setting up conditioned reflexes of new and incorrect habitual patterns of breathing and a resetting, or loss of fine tuning, of the respiratory centre’s trigger mechanisms (Fig. 17.2).
Hyperventilation is today likely to be recognized more often in association with panic disorders or phobic states because of its causal, consequential or perpetuating relationships (Cowley & Roy-Byrne 1987). Patients presenting with panic disorder or anxiety (van den Hout et al 1992) or anxiety and evidence of depression (Jack et al 2003) have been shown to have lower resting levels of carbon dioxide than normal. Some may demonstrate a greater than normal sensitivity of the basilar artery’s response to hypocarbia (Ball & Shekhar 1997).
Hyperventilation has been shown to be prevalent in patients with vestibular dysfunction. This could be caused by the anxiety of the condition, but for some patients neither the hyperventilation nor the vestibular dysfunction provokes anxiety (Humphriss et al 2004). Ongoing work demonstrates a relationship between the vestibular and respiratory pathways in the brain stem, the contribution of the vestibular system to respiratory muscle activity and cardiovascular control during changes of posture and movement, and posture instability following hyperventilation (Yates & Bronstein 2005, Yates & Miller 1998, Yates et al 2002). Stress, acute pain and chronic pain may often result in hyperventilation producing hypocapnia (Terekhin & Forster 2006).
SIGNS AND SYMPTOMS
The vast array of commonly reported signs and symptoms can be loosely grouped as they affect different systems (Table 17.1). Timmons (1994) suggests that it would be useful to have a comprehensive validated list of symptoms, in order to hasten history taking and to facilitate comparisons of therapeutic trials. Few, if any, studies have looked at the association of symptoms with age, sex, personality traits and causal factors.
Table 17.1 Commonly reported signs and symptoms
| System | Signs and symptoms |
|---|---|
| Cardiovascular | |
| Gastrointestinal | |
| General | |
| Musculoskeletal | |
| Neurological | |
| Respiratory | |
| Psychological/psychiatric |
Some patients present with a constant resting level of hypocapnia and others present with resting levels of carbon dioxide within the normal range. Both groups feel generally unwell and experience ‘attacks’ featuring a galaxy of symptoms, which appear to occur sometimes with no apparent reason. Further hypocapnia may or may not be recorded at these times. In some patients the symptoms seem to precede the event of hypocapnia rather than be a consequence (Hornsveld et al 1996). If symptoms in some patients are not generated by hypocapnia, we must ask what other mechanisms could be the cause. Could the symptoms be a direct consequence of the disordered movements of overbreathing and their abnormal feedback? And if so, which sensory, motor or behavioural mechanisms could be involved?
Hypocapnia induces vascular constriction, resulting in decreased blood flow, and as a response to the Bohr effect there is also inhibition of transfer of oxygen from haemoglobin in the circulating blood to the tissue cells. Hypocapnic vasoconstriction is probably the cause of the characteristic range of cerebral, peripheral and cardiac symptoms. As the cerebral symptoms of hypoglycaemia are similar to those of hypocapnia, the cerebral effects of hyperventilation are highlighted at times of low blood sugar and it has been suggested that hyperventilation increases circulating histamine, which may be the cause of the high incidence of allergies reported (Lum 1994). Fluctuations in PaCO2 can have a destabilizing effect on the autonomic system resulting in a sympathetic dominance (Freeman & Nixon 1985). The patients are often in a state of arousal. It has been shown that the mean urinary excretion of adrenaline in a group of persons who hyperventilate was three times as high as in a group of normals (Folgering et al 1983). Mogyoros et al (1997) suggest that hyperventilation has a selective action on nerve conduction, which is greater on sensory than motor fibres. This may explain why hyperventilation induces paraesthesia before fasciculation.
Altered patterns of breathing can cause musculo-skeletal dysfunction. The combination of habitual overuse, ischaemia and increased sympathetic drive increases myofascial tone via smooth muscle cell contraction and leads to the evolution of active myofascial trigger points (Chaitow 2002). Pain thresholds are also reduced. Patients with dysfunctional breathing may describe a history of neck and/or thoracic pain and stiffness, headaches, low back pain and temporomandibular joint dysfunction. Orofacial pain is also associated with this patient group (Hruska 1997).
The diaphragm has a place in postural control and spinal stability, such that control of intra-abdominal pressure occurs through coordinated activity of the diaphragm, pelvic floor and transversus abdominis muscles (Hodges & Gandevia 2000, Hodges et al 1997). Dysfunction in this stabilizing mechanism has been implicated in recurrent low back pain. Postural activity in the diaphragm (and transversus abdominis) was shown to be reduced or absent after only 60 seconds of experimentally induced hypercapnia, suggesting that stability of the spine may be compromised in some respiratory disease or dysfunction (Hodges et al 2001). It is hypothesized that such a compromise may lead to increased potential for injury to spinal structures and reduced postural control (Hodges et al 2001); however, further research is indicated. Disorders of breathing (and continence) have been shown to have a higher association with low back pain than obesity and physical activity (Smith et al 2006).
Alternatively, acute or chronic musculoskeletal disorders may precipitate breathing dysfunction due to pain, postural compensations, and structural and functional changes in the fascial, neural, muscular and skeletal systems. The typical flexed posture of a person in pain impedes normal respiratory function. Musculo-skeletal dysfunction such as thoracic spine hypomobility, rib immobility, and short overactive accessory respiratory muscles can directly cause dysfunctional breathing patterns to develop (Chaitow 2002).
The relationship between chronic fatigue syndrome (CFS) and hypocapnia is questioned and Naschitz et al (2006) suggest that unrecognized hypocapnia is common in CFS. Interestingly, patients with CFS also frequently experience chronic musculoskeletal pain (Nijs et al 2006). Patients with hypermobility syndrome commonly present with dysfunctional breathing patterns and chronic pain. Hypermobility syndrome may have an effect on ventilation because of abnormally compliant lungs, disordered lung receptors, hypermobility of the thoracovertebral joints and/or pain. Hypermobility syndrome has been shown to be associated with fibromyalgia (Ofluoglu et al 2006) and CFS (Nijs et al 2006). Could dysfunctional breathing be the common link between these three conditions?
CAUSES OF HYPERVENTILATION
The many circumstances that may stimulate a hyperventilatory response (Box 17.1) may or may not become a chronic disorder. Other than HVS being the primary cause of the patient’s symptoms, we have seen that it is not uncommon for chronic hyperventilation to coexist with other conditions and to be a sustaining factor within the complex interaction of a number of physiological, organic and psychological disorders (Gardner 1994). Before embarking on a treatment programme, it is necessary to ensure that the patient has been suitably investigated in order to diagnose any underlying treatable disease or disorder and to recognize any other possible coexisting factors. Where pain is believed to be a causative or contributing factor, appropriate management strategies should be investigated.
DIAGNOSTIC TESTS
There are no generally accepted measurable diagnostic criteria and it is probably not possible to devise a satisfactory or conclusive diagnostic test for HVS because of the multifactorial effects and complex systemic inter- actions. Various tests have been described but time has shown that none should be used alone. Each test can be useful when used with other information.
The voluntary hyperventilation provocation test (HVPT)
The hyperventilation provocation test (HVPT) (Hardonk & Beumer 1979) records end-tidal PACO2 and all symptoms provoked during and after the test. Using end-tidal PACO2 recordings, the patient is requested to hyperventilate for 3 minutes. If the PACO2 falls by at least 1.33 kPa (10 mmHg) and the level of recovery is less than two-thirds of the former resting level after 3 minutes, the result is recorded as a positive diag- nosis of a hyperventilation syndrome. Nevertheless, as about a quarter of ‘normals’ also show this phenomenon, a lowering of PACO2 and slow recovery is not in itself diagnostic. Immediately after the completion of the recordings the patient is asked to compare any symptoms provoked during the test with recognized complaints. When two or more major symptoms are reproduced, the HVPT is considered positive. Generally, tingling of fingers and dizziness are not included because these symptoms occur in ‘normal’ subjects. However, some patients report that some provoked symptoms are only ‘similar’ but not the ‘same’. Sometimes provoked symptoms are new experiences and not related to the patient’s complaints. Others may be helped by recognizing that altered breathing can precipitate their symptoms. Caution should be exercised on using this test if the patient complains of cardiac symptoms or pseudoangina. As yet this test has not been standardized.
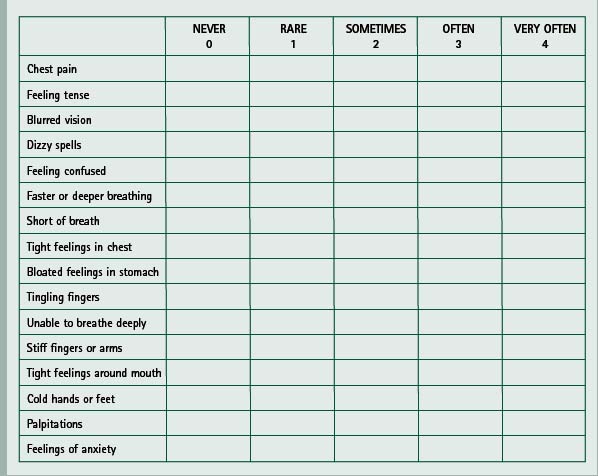
The Nijmegen questionnaire
This was first drawn up as a list of 16 complaints chosen by a team of specialists from different disciplines, from 45 clinically relevant symptoms related to hyperventilation syndromes (van Doorn et al 1982). The complaints fall into three categories or dimensions, corresponding with the classic triad of breathing disruption, paraesthesiae and central nervous system effects. The list does not include fatigue or behavioural disturbances. Patients score on a five-point scale from 0–4 (0 = never, 1 = rare, 2 = sometimes, 3 = often, 4 = very often) against each of the 16 listed symptoms and a score over 23 is recognized as positive (Box 17.2). The efficacy of the questionnaire was investigated by comparing patients who hyperventilate with persons who do not. It showed a high ability to differentiate between the two groups (van Dixhoorn & Duivenvoorden 1985) and, although not conclusive, it was recognized that the questionnaire was suitable to be used as a screening instrument in diagnosing HVS when used with additional information. A correlation has been shown between positively rated Nijmegen questionnaire results (score of 24 or more) and positive HVPT results (recognition of at least two major symptoms) (Vansteenkiste et al 1991).
Humphriss et al (2004) found that, despite some limitations, the Nijmegen questionnaire is a quick and easy to administer assessment tool to detect HVS in patients seen for vestibular assessment. It is important to diagnose the condition in vestibular disease as it has been suggested that hyperventilation disrupts vestibular compensation and increases postural sway. Conventional vestibular rehabilitation may be only suboptimally successful until a normal breathing pattern has been re-established. The questionnaire has been used to diagnose HVS in some patients complaining of nasal congestion and subsequent breathing re-education has been successful in correcting the nasal congestion without further surgery (Bartley 2005).
The questionnaire can be useful for physiotherapists to record symptoms and, if used at regular intervals, to record the changing status in relation to treatment. A final score at discharge could be used as a semi-objective outcome measure.
The ‘think test’
The ‘think test’ (Nixon & Freeman 1988) provides a patient-specific stimulation, which can have an advantage over unspecific challenges in testing for episodic hypocapnia or a change in the breathing pattern. The patient is invited to close the eyes and then to recall the emotions and sensations surrounding certain situations that have caused distress or provoked symptoms. A change in the breathing pattern and/or a fall in PaCO2 greater than 1.33 kPa (10 mmHg) is considered to be significant.
Ambulatory monitoring of transcutaneous carbon dioxide
The transcutaneous sensor is attached to the patient who is instructed how to press the ‘event button’ and in the use of a diary. The ‘event button’ marks the recording tape and the diary entry records:
Prolonged monitoring may produce helpful data (Hibbert & Pilsbury 1988).
Patients with recurrent laryngeal nerve palsy can become fatigued during prolonged phonation, due to excessive breath loss while trying to maintain sufficient subglottal pressure for speech. Transcutaneous carbon dioxide (PTcCO2) recordings have shown significant decreases in PaCO2 in these patients. Education of the disrupted pattern and control of the expiratory phase during vocalization has produced improvement in PaCO2 levels on PTcCO2 and a decrease in symptoms (Miyazaki et al 1999).
Breath-holding time
This is a semi-objective measure that generally shows a direct relationship between the maximum breath-holding time (BHT) and the resting PaCO2 (short breath-holding time is usually associated with a low or unstable resting PaCO2). Breath-holding time tends to increase as the breathing pattern becomes more regular and stable. The patient is given a description of the method and then asked to take a normal breath in, followed by a normal breath out and to hold the breath in the resting phase until it becomes too uncomfortable to hold any longer. This breath-holding time is recorded. Some ask for the breath-hold after a full inspiration and a full expiration. Whichever method is used, it is essential to use a similar process and a similar posture each time. Standardization of the procedure would be helpful. The average BHT is suggested to be approximately 30 seconds (Bradley 2002). The patient will hope to increase the BHT if it is low but it is not helpful to know the norm at this time, as it may cause a forced hold time, which could be damaging to the process. If breath-holding time is recorded at regular intervals it could be used as a semi-objective outcome measure.
PATTERNS OF BREATHING
Quiet normal breathing patterns at approximately 8–14 breaths per minute at rest involve three phases:
During inspiration, the active descent of the diaphragm is reflected as a gentle forward swelling of the abdomen and there may be minimal movement outwards of the lower ribs. On natural passive expiration the abdomen and lower chest return to the resting position. During exercise, the minimal lower thoracic movement increases and as exercise increases so does the thoracic involvement. Rate, volume and place of movement change with posture, motion, exercise, varying stimuli, disease or dysfunction. The act of inspiration naturally draws air in through the nose where it is warmed, filtered, moistened and the flow controlled before entering the airways. Air that is drawn in through the mouth bypasses this conditioning.
Breathing patterns, related to the chronic hyper- ventilation syndromes or idiopathic symptomatic hyperventilation, vary widely from gross upper thoracic movement with sternocleidomastoid and accessory muscle involvement at a rate as high as 50 breaths/min to a near-normal rate and volume and minimal upper thoracic movement. The degree of lower thoracic movement and abdominal movement also varies from almost nil to normal.
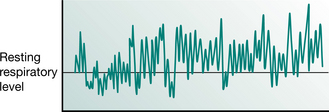
The respiratory rate and volume may be extremely irregular (Fig. 17.3) and the pattern interspersed with sighs, sniffs and yawns. At the other extreme, once habitual hypocapnia has been established, it may require only an occasional deep sigh to maintain the new low levels of carbon dioxide and the general breathing pattern may appear normal.
The breathing patterns vary with each patient and within the daily experience of each patient. The only constant feature in HVS is that the patient’s breathing appears to respond inappropriately to the changing metabolic and emotional requirements of daily living and that symptoms generally vary throughout the day for no apparent reason. Often there are ‘good days’ and ‘bad days’. There does not seem to be a strict correlation between the abnormality of the breathing pattern, the depression of PaCO2 and the severity and type of symptoms.
REFERRAL FOR PHYSIOTHERAPY
There appear to be various groups of patients with symptoms related to overbreathing. Patients presenting for physiotherapy tend to fall into four main groups:
OVERVIEW
Re-education of the breathing pattern for all groups will follow similar lines, involving a conscious control of nose breathing, place of movement, rate, volume and regularity of the breathing cycle. If the PaCO2 is low or labile, the programme will be devised to help to raise and stabilize the resting level. If low PaCO2 is not an issue, attention will remain with making the pattern slow and regular and in correcting the place of movement. A predominantly relaxed, passive abdominal movement (reflecting the movement of the diaphragm) is preferred and movement directed away from the upper thorax and shoulder girdle. This abdominal pattern of movement may in turn help to induce physical and mental relaxation. Relaxation is often aided by a regular, slow pattern of breathing. It may be necessary with some patients to teach and practise a suitable relaxation technique before, during or after the breathing control. The long-term goal is to re-establish a more normal, slower and personally acceptable pattern of movement that decreases ventilation sufficiently to raise the resting PaCO2 by a small measure.
In the short term, until the new pattern of breathing becomes the natural, constant, unconscious, spontaneous method of breathing, the patient is likely to continue to experience episodes of symptoms. Some symptoms may be provoked if the patient ‘tries too hard’ and, by overcompensating in one component of the new pattern, increases ventilation rather than decreases it. Early warning of these phenomena must be built into the sessions. Other symptoms may be related to certain recognizable situations, stresses or exercise, precipitating disordered breathing before the patient has mastered control of the new pattern. The patient needs to know of these frustrating possibilities and pitfalls and be taught to take ‘first aid’ measures of controlled breath-holding or rebreathing expired carbon dioxide from a bag or cupped hands. In time, with reassurance and perseverance, it should be possible to control the new way of breathing and ward off any episodes of falling carbon dioxide levels, or inappropriate breathing by identifying the provoking situations and practising precautionary measures.
Initially treatment sessions usually take approximately 1 hour. Outpatients should attend weekly at first. As the patient progresses the sessions become less frequent. Some patients who have been diagnosed early and who have no underlying pathology may need only 2 or 3 sessions; others, with organic disorders, will need more time and those with background psychological history may need 12 or 14 sessions spaced out over 12 or 18 months. At the time of discharge it is important for the patient to know that it is possible to keep in touch and to have a telephone number to call in an emergency for advice or review if necessary. Inpatients will probably be treated daily at first. Sessions will be given less frequently as soon as possible, to allow the patient to take more responsibility and to practise alone.
TREATMENT
Assessment
The assessment should include:
History
The patient may have been referred for treatment with a breathing problem related to an organic cause. If not, it is helpful to ask open-ended questions to elicit when the patient first became aware of problems and the response to them. The giving of the history and the description of the symptoms may trigger unpredictable responses from the patient which could slow up the process, yet help to bond an understanding relationship between patient and physiotherapist when handled sensitively (it is always helpful to have a box of tissues to hand). The first awareness of a problem may have been an acute ‘attack’, for instance driving home on the motorway on a Friday night after a stressful week and experiencing dizziness, tingling in the limbs and central chest pain. The response to this could be that of believing it to be a heart attack. This would be very understandable, especially if a member of the family had recently died of coronary disease. The anxiety would stimulate the respiratory rate further and the symptoms would increase, possibly to the point of admission to the nearest accident and emergency department. Misrepresentation of the symptoms of an acute short-term episode of stress may cause a single natural response to be transformed into a pattern of inappropriate responses thereafter.
Signs and symptoms may not present so dramatically. Commonly symptoms may be traced back to a history of glandular fever, a long viral illness or low-grade fever, bereavement, failed expectations, change of lifestyle or job or house, family breakdown, frightening experience, fear of inability to perform to targets and fear of failure or prolonged emotional pressures, conflicts or abuse. A definitive trigger point may not be found and the first experience of the disorder may be related to an array of stimuli or events that happened together or in close succession. History of musculoskeletal pain, previous injuries or accidents, past surgical history and generalized feelings of muscular tenderness, tension and stiffness should be recorded as any of these may be the underlying cause.
Family history. Any similar symptoms, allergy, anxiety, hypermobility syndrome, cardiac or respiratory disease experienced by other members of the family should be elicited. Not uncommonly, the habit of overbreathing can be traced back to family illness patterns or relationships.
Childhood history. History of premature birth; oxygen therapy or artificial ventilation immediately after birth are incidents which are increasingly reported. It is also helpful to record childhood general health, including any tonsil or adenoid problems, physical ability, exercise tolerance, allergy and some idea of the quality of the relationships at school and at home.
Signs and symptoms
There may be difficulty in describing the symptoms, as many of them are not usually within one’s everyday experience. The symptoms generally occur when the brain is trying to function in a hypoxic condition or the patient is trying to respond to an abnormal situation, thus causing difficulty in perception, retention and recall of phenomena. A full list of symptoms, including any allergies, should be recorded, listed and numbered in relation to severity, occurrence and concern. The degree to which a symptom is incapacitating could rate 0–10 on a disability scale and the degree to which a symptom is fear provoking could rate 0–10 on a distress scale, while the frequency of occurrence of the symptom could also be rated 0–10. These records will give a guide to progress and ultimately could give a semi-objective outcome measure.
Assessment of personality
A detailed analysis of the personality is neither possible nor necessary in this setting. However, a simple assessment may be made by noticing the posture, facial expression, demeanour of the hands, manner in which the history is given and the patient’s emotional responses and reactions to the situations related in the history. One patient may be overtly obsessive and perfectionist and obviously reacting against the uncertainties of life, while another may be superficially tranquil, masking the underlying burden of troubles and emotions that are being carried. These may come spilling out at any time during the treatment sessions when the patient begins to feel safe.
Physical examination
It is wise to complete a physical examination; however, it may not always be necessary if pertinent information is given in the referral. When examination is deemed necessary and with the patient’s chest unclothed, note should be made of:
 the shape and posture of the chest and shoulder girdle, and abdominal and accessory muscle tone. Observe for pectus excavatum, asymmetries and any physical deformity
the shape and posture of the chest and shoulder girdle, and abdominal and accessory muscle tone. Observe for pectus excavatum, asymmetries and any physical deformityGenerally the pattern of breathing can be assessed with the patient dressed. The place of movement, size, regularity and rate of breathing should be recorded and whether the patient breathes through the nose or mouth. The physiotherapist should have a watch with a second hand available to record the breathing rate per minute. It will be helpful to make a record of the number of breaths per minute at each visit and ultimately this record can be used as an outcome measure. The patient should not be informed at this stage that the rate is being recorded nor of the rate per minute, as the re-education of the pattern will take place at the level of the individual breath or phase of breath. A knowledge of the greater timescale, in the early stages, can be damaging as the patient may try to take fewer breaths per minute without regard to the size of the breath.
Treatment plan
The overall plan should be discussed with the patient. The transfer of oxygen and carbon dioxide should be described in lay terms and related to the patient’s manner of moving air. Once patients are able to connect their symptoms to the manner of breathing and not to some life-threatening disease, they are usually only too delighted to make a firm commitment to learn more about the manner of breathing and its control and to take responsibility for the home treatment programme. They happily recognize that it is possible to help themselves and to gain a degree of mastery over symptoms and the environment.
Treatment is not a matter of learning ‘breathing exercises’, but of learning how to feel, alter and control the manner of breathing. The treatment plan in the short term (to control symptoms) and in the long term (spontaneously to maintain a corrected pattern of breathing) should be described and agreed. Agreement should also be sought to look constructively at the activities of the day and to try to identify possible factors influencing the onset of symptoms. A fitness programme may be discussed at this stage, but it should not be introduced until later in the plan when there is some semblance of breathing control.
Breathing awareness education
Probably the most comfortable position for learning about breathing is lying with suitable support. Most people with chronic hyperventilation do not have respiratory disease and therefore can lie flat without distress. The suggested position is supported with one or two pillows under the head and under the knees. The knee pillow(s) help to prevent tension in the abdominal muscles and thus enables a natural passive abdominal movement during the respiratory cycle. In lying, the abdominal contents move up somewhat into the thorax and during inspiration act as a stimulating natural resistance to the descent of the diaphragm. For patients who find that this position is uncomfortable or if it precipitates breathlessness or a feeling of vulnerability, another position should be found. Relaxed sitting with adequate support is usually acceptable to most people.
The first step of breathing awareness is to help to bring the breathing pattern into the consciousness by beginning to concentrate on the feeling of the body movements in relation to the flow of air while breathing. Sensory input and body awareness are increased if the patient rests both hands on the abdomen. Some prefer to place the dominant hand on the abdomen and the other on the upper chest, better to distinguish the place of movement. This position may be helpful at certain times during re-education to confirm the movement pattern. These possible positions are personal preference, but proprioceptive input may be more positive for retraining if both hands are rested on the abdomen. The physiotherapist lightly covers them with her hands. This light contact helps to bond the physiotherapist–patient relationship and allows the physiotherapist to feel, as well as observe, the movements related to the breathing cycle.
Again, a simple description of respiration should be given to help the patient observe sensations and movements relating to the flow of air in and out and to the chest, diaphragmatic and abdominal movements. The patient is helped to ‘internalize’ these descriptions of airflow and body movement by using the imagination. If the patient is a mouth breather, time should be spent describing the purpose of breathing through the nose and practising nose breathing. Tuition and discussion should continue in this position until the physiotherapist is satisfied that the patient has grasped a basic and simple anatomical and physiological understanding. Generally the patient will become more relaxed as the interaction distracts from excess self-awareness.
Having had the breathing described, the patient is asked to close the eyes and try to feel and sense what is happening to the body with regard to the breathing. It may be necessary for the physiotherapist to relate what is happening.
Care must be taken not to direct the pattern but merely to describe. For example:
‘You are now breathing in … and now you are breathing out’
‘You are breathing in and your abdomen is swelling … and now your abdomen is falling back to rest’
At this early stage, the patient is learning to establish the relationships between air movement and the associated body movement and to recognize that as the air moves ‘in’ the body moves ‘out’ to accommodate the air and vice versa. By this stage a feeling of discomfort may be experienced and an explanation must be given relating to the subconscious, reflex and automatic nature of breathing. When the act of breathing is brought into the consciousness – as it has to be for re-education – there will be some discomfort, which has to be recognized, accepted and yet, at the same time, disregarded. It is within this forum that changes can voluntarily take place. The patient is then asked to focus on the ‘in breath’ and notice when and how it starts and finishes. This ‘quiet attentiveness’ is then transferred to the ‘out breath’ and note taken of the beginning and end of this phase. Particular attention should be given to the end of the phase to recognize when the breath gently stops. The spontaneous rest point is identified as the natural rest point in the breathing cycle and the patient is helped to feel it as a place of relaxation, a place of balance, not a place of tension. It may be helpful to practise general relaxation into this place of ‘no movement’. Most patients can accept this experience and begin to recognize it as a welcome rest.
In order to recognize the full breathing capacity it is helpful to ask the patient to hold the breath at the upper point of the tidal volume and then to request a continuation of inspiration until full inflation is achieved. In this way it is possible to experience the inspiratory capacity. Similarly, the expiratory reserve can be experienced by breath-holding at the bottom of the tidal volume and then exhaling entirely by using all the expiratory muscles. Having practised these two manoeuvres, the patient will also realize that the relaxed tidal volume is relatively easy compared with the muscle work needed above and below the tidal flows. Patients may be able to use this information to perceive a change in their breathing pattern before symptoms occur. The learned corrective steps could then be made before full-blown symptoms take hold.
Breathing pattern re-education
The initial education and breathing awareness training is followed by re-education of any components that have been identified as being disordered. Any change, especially in volume or rate, must be balanced to attain a decrease in minute volume. The components are:
The new breathing cycle may be of two or three phases, depending on the patient’s body preference at the time. The two-phase cycle consists of a gentle inspiration followed by a slower expiration and hopefully, in time, progress to a more normal three-phase cycle. In a three-phase cycle the natural rest point at the end of expiration is inserted and/or extended. A gentle inspiration is followed by an easy (passive) expiration, which naturally changes into the rest period, which is comfortably extended until the next inspiration is gently initiated. Practice will help to lengthen this rest, but care has to be taken not to extend it to the point where a gasping inspiration is stimulated.
Method
By this stage the patient and physiotherapist should be aware of the volume and flow rate of each breath and the rhythm of the breathing pattern. The physiotherapist will describe these components and clarify with the patient what changes need to be made to decrease the minute volume and to regularize the pattern. Breathing is a very personal activity, and the new pattern should not be imposed by another from the outside. The changes should be made by the patient from within, guided carefully by the physiotherapist. They work together experimenting with changing certain aspects until a pattern evolves which fulfils the physiological requirements and which harmonizes with the patient’s inner knowledge of well-being. The new pattern will be remade with the least possible interference.
As many patients who hyperventilate have a predominantly thoracic movement, this needs to be changed to a gentle passive movement of the abdominal wall. In general, most patients manage to recognize what is needed to change from a thoracic ‘in and up’ pattern to an abdominal ‘in and down’ pattern. However, some patients find it extremely difficult to obtain any abdominal movement and it may be necessary to spend several treatment sessions using different word combinations and images until a more relaxed abdominal movement is achieved. Should this not be the case then incorporation of manual therapy techniques, such as myofascial release techniques and mobilization, may be indicated. Large or forced breaths must be discouraged. Any increase in ventilation will increase or precipitate symptoms.
Some therapists like to place a heavy book or sandbag on the abdomen to give resistance and direction to the inspiratory movement. The weight is inanimate and therefore will need to be controlled during expiration; thus expiration cannot be a relaxed, passive, natural movement but rather the abdominal muscles will be called into an unnatural state of extrinsic work in order to control the expiratory phase, thus compromising the work of re-education. It is not physiological to pursue this practice. If resistance to inspiration is required to help centre the new movement of the abdomen, manual resistance given by the physiotherapist can be graded and be flexible according to need. It is not wise for the patient to give manual resistance as this would recruit shoulder girdle muscles. The weight of both hands is usually sufficient but the use of a pillow over the abdomen on which the forearms are rested is often useful and comfortable.
Special care also needs to be taken in order not to increase the volume if the flow is slowed, nor to increase the flow rate if the volume is decreased. A new pattern is introduced by gradual and patient work. It will be very individual. Guidance should be given breath-by-breath and phase-by-phase, relating which movement is good and which incorrect, and thus reinforcing correct patterns of volume, movement and rest, which will of course be smaller and slower and more regular.
This decrease in body movement and ventilation may cause the patient an uncomfortable sensation akin to suffocation. This sensation is probably due to altered responses from the stretch reflexes in muscles, joints and lung tissue and from any rise in PaCO2. The patient is helped to understand and accept this sensation of unease or discomfort, which will in time subside.
It is necessary to experience this sensation at a minimal level while practising the corrected pattern. It should be perceptible but acceptable. Changes should not be so great that they create an unacceptably strong sensation, as the new pattern would not be physiologically and psychologically sustainable and would stimulate a sense of anxiety. By maintaining the controlled pattern for as long as possible, the respiratory centres will be reprogrammed to trigger inspiration at a higher level of carbon dioxide and the reflexes involved in the new movement pattern will be reinforced. (The reprogramming is similar to that which occurs in patients with ventilatory insufficiency in COPD. An imperceptible increase in PaCO2 over a period of time appears to condition the respiratory centre to accept higher levels before triggering inspiration and any altered patterns of movement become habitual.)
If the desire to breathe becomes too great to contain, simple swallowing may ease the discomfort. If this is not sufficient, a slow, controlled deep breath may be taken. To compensate for moving this large volume of air, a longer period of time must be used. It is helpful to hold the breath after expiration, if it is possible, for a count of five or six (3–4 seconds) or as long as is acceptable without stimulating an inspiratory gasp. In normal subjects the PaCO2 drops as the result of a deep breath and takes 3–4 minutes to return to normal if no compensatory measures are taken. Patients need to learn of this phenomenon and to use the knowledge positively by compensating for deep breathing or sighing by breath-holding (preferably at the point of expiration) for a count of five or six. It is helpful to practise this slow deep breath, with a breath-hold on expiration, during treatment sessions.
Once a pattern has been found that fulfils the change criteria and suits the patient, it needs to be reinforced in the patient’s mind. Some are able to recognize the pattern without external help; others find it difficult to recognize the timescale required. The correction in time may be helped by the physiotherapist guiding, by counting monotonously, the time span of the phases of each breath. The possibilities are many and individual. They may vary from in out and in out and … to a slower more natural pattern of in and out two three and rest and in and out two three … (Fig. 17.4). The use of a recording machine, to capture the timing of the pattern during a treatment session, may help the patient to practise more effectively at home. The chosen new pattern may be the ideal to control the symptoms and enable the patient to feel better. However, it is sometimes necessary to move forward more slowly and, having achieved a very small step, to make further corrective changes until a curative pattern can be accepted.
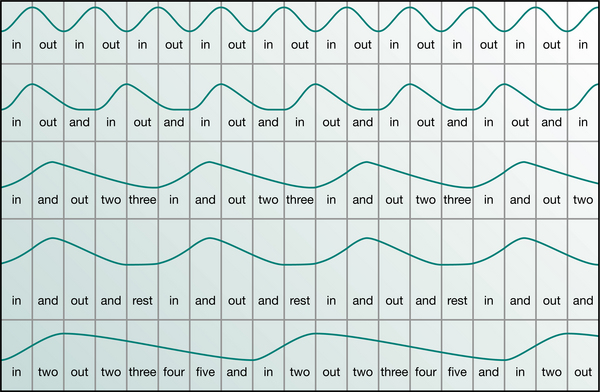
Figure 17.4 Some suggested breathing patterns demonstrating a regular small tidal volume with various flow rates and rest periods.
The patient will need to learn control of the breathing pattern in sitting, standing, walking and during and after exercise. Evidence to support this practice is offered by Malmberg et al (2000), who reported that when changing body posture from supine to standing, patients with HVS increase their pulmonary ventilation in excess of metabolic needs greater than healthy controls. The work of Yates (1998) and his colleagues has shown an important relationship between vestibular stimulation and respiratory control. It may be necessary to practise changing positions and exercising during treatment sessions. Natural breathlessness will occur on exercise and should be recognized and accepted as normal. Some patients may feel better on exercise, as the body’s metabolic needs rise to equilibrate with the respiratory physiology. Others may overbreathe on exercise; this will be recognized by an increase in, or occurrence of, symptoms. Appropriate control measures will need to be introduced and practised. If the natural breathlessness does not subside within an acceptable time span after exercise (by the time the pulse rate is back to normal), control may be gained by changing one component of the breathing cycle at a time. First slow the rate, then decrease the volume, then slow the rate, etc., until control is achieved.
Compensatory procedures
The patient must become aware that the old habits of irregular large breaths, frequent sighs, yawns and sniffs, and also coughing and laughing, are likely to precipitate symptoms and will need to be compensated. An easy first aid measure is to respond immediately with a compensatory breath-hold followed by a normal size breath. It is useful to form a habit of intermittent breath-holding during the day. The hold should not be anticipated by a deep breath; rather, the breathing cycle should be stopped anywhere in the cycle for a count of 2 or 3 or a longer time such as does not provoke a large following inspiration. It can also be practised and linked to simple everyday activities (like walking through a doorway) until it becomes a conditioned reflex. The hypothesis of this manoeuvre is to help lessen the risk of carbon dioxide falling to symptomatic levels.
Planned rebreathing
It has been recorded that paper bag rebreathing may carry the hazard of hypoxia (Callaham 1989). However, poorly programmed rebreathing in acute hyperventilators who may have undiagnosed cardiac or respiratory conditions should not rule out the careful, controlled use of rebreathing therapy for chronic hyperventilators. There is a small group of people who cannot control the breathing pattern when it is most needed. There may be many reasons for this. One possibility is that the low PaCO2 and associated cerebral vasoconstriction have an effect on memory programming and recall. If the PaCO2 can be raised by rebreathing, the patient becomes clearer-headed and can then remember the breathing control programme.
At times of acute distress or inability to control the disordered breathing, a bag (25 cm × 30 cm minimum) may be used as a rebreathing apparatus. The bag must be shaken out so that it is full of room air. The open end of the bag is placed loosely over the nose and mouth, allowing some free passage of air between face and bag. The patient should breathe freely within the bag. Rebreathing of the expired gases takes place, thus raising the PaCO2. After approximately 6–8 breaths, the bag should be removed from the face and shaken out to refill it with fresh room air. The procedure should continue with regular shaking of the bag until the acute presenting symptoms subside or until the patient is capable of controlling the breathing pattern effectively. For safety reasons the rebreathing bag must only be used in the sitting or standing position and never in lying. Should the patient lose consciousness, the bag would fall away from the face and not remain in situ, with the risk of asphyxia. Cupped hands held over the nose and mouth form another suitable and less obvious rebreathing procedure.
Rebreathing only raises the PaCO2 during the procedure and, if the breathing pattern is not changed, the PaCO2 would fall back when rebreathing ceased. The purpose of the procedure is to raise the carbon dioxide sufficiently to calm the patient and to enable conscious correction of the breathing pattern to take place.
An ordinary oxygen mask with large holes, as used for inhalation therapy, may be used for patients who are unable to control the breathing sufficiently at certain times or who, as a result of hyperventilation, are housebound and unable to do household and personal routines. The facemask may be worn for the duration of the task. The PaCO2 is artificially raised by the rebreathing function of the mask. The vent holes are left open so that room air can be drawn in to maintain sufficient oxygen concentration.
A facemask may be the short-term therapy of choice for patients who are terminally ill and hyperventilate with anxiety.
It is unwise to use bags or masks too freely, as some patients can become dependent on the aid and never learn to reorder the breathing cycle. They should only be used when the patient’s personality and situation are understood and when all other avenues have been investigated.
Speech
Many patients report that speaking and singing provoke symptoms. Normal conversational speech occurs at the upper end of expiratory tidal flows and there is a delicate interplay between breathing and speaking. Complex coordination of the respiratory muscles is required to produce the necessary subglottal pressures and the intricate manipulations needed to produce and maintain sound.
Speech requires longer controlled expirations and shorter, faster inspirations than resting breathing. These inspirations need to be taken at suitable points in the sentence in order to maintain fluency and intelligibility. Often the old pattern of speech is very fast, as the patient tries to say as much as possible on one breath, before snatching at the next. The aim to amend this habit is to articulate each word more slowly, to say fewer words on each breath and to try not to move down into the expiratory reserve volume. The new pattern of breathing required to incorporate these needs has to be found and carried out. It is usually helpful if the physiotherapist works with the patient, while the patient practises reading aloud and listening carefully to the new pattern of speech. This process helps to re-educate the breathing control and the sensory feedback loop.
Home programme
Therapy is directed towards re-educating the breathing pattern, not to breathing exercises. Practice sessions should be as many and for as long as possible. By using a practical approach, an acceptable programme must be worked out by the physiotherapist and the patient. At first it may only be possible to practise for 5 minutes a day, but three or four sessions of 20–30 minutes each is obviously more beneficial. Many patients find that as they change their lifestyle, more time can be made available for breathing control and relaxation sessions.
It is good to start the day with a period of conscious control of breathing. It is suggested that 10–15 minutes is spent in practice before rising in the morning. When travelling by bus or train, conscious breathing control and relaxation is time well spent, even if one is standing in a crowd. Car drivers can use their time constructively while waiting at traffic lights. Coffee, lunch and tea breaks could afford a few minutes of practice. Some people prefer to remember to practise breathing control for a few minutes each hour, on the hour, during the day. Fifteen or 20 minutes should be put aside when returning home from work or shopping, to relax and practise breathing control. It is worth spending this time after a working day to allow the body to equilibrate. The evening can be more enjoyable when not fighting symptoms. The last period of practice can be done having retired to bed using the favourite sleeping position.
Compensatory breath-holding, intermittent breath-holding and general physical and mental relaxation should become part of the normal day. People who have experienced HVS are probably always at risk, even after the presenting episode has been resolved. It would be judicious always to remember to practise breathing control before aggravating situations such as flying, travelling to a high altitude, heat, hot baths and periods of prolonged excitement, stress or risk.
Exercise and fitness programmes
As a result of the disordered breathing pattern, many patients have been unable to exercise and have become unfit, thus compounding the problem. Guidance in a slowly graded exercise scheme forms an important part of management. It may need to start with very simple movements in lying, such as arm raises, heel slides or knee fallouts at low repetitions. The progression must be carefully graded into more functional positions such as sitting and standing and activities such as walking. Swimming is another excellent form of exercise, which encompasses general movement synchronized with breathing. Most importantly, the physiotherapist should guide the patient to find an activity that is enjoyable and may be fitted easily into the daily routine. It should start with very short sessions of only a few minutes, interspersed with rest breaks as needed. Sessions can be gradually built up toward 20–30 minutes with close monitoring of symptoms. Realistic short-term goals should be set, such as walking an extra bus stop, or swimming one length of the pool at a time. The exercise programme should be clearly prescribed, monitored and gradually progressed by a physiotherapist. To err on the slow side is preferable to advancing too quickly as impatience for progress may cause decline rather than improvement. Rehabilitative styles of Pilates or stability training, both performed with a physiotherapist on an individualized basis, can offer a safe and gentle approach to exercise. Breathing control, stability, balance, spinal mobility, postural alignment and body awareness can all be improved with this method. There is variation in the way Pilates is taught and the physiotherapist should review the teacher’s qualifications and experience before referring patients. It is not appropriate to refer these patients to Pilates sessions or group classes until they have worked individually with a physiotherapist and can independently control their breathing with movement. Work within a group should never be competitive. Each person should be following an individual programme. These group sessions must be monitored carefully to ensure that they are not used for ‘swapping symptoms’. With careful guidance they can help to give confidence and enhance the patient’s ability to return to a more active life.
Discharge
At discharge the outcome could be measured by:
Those who habitually hyperventilate are often gifted and interesting people and are generally highly motivated and compliant with treatment. A high proportion of people with dysfunctional breathing are helped by a systematic, individual treatment programme and by an intelligent and sympathetic approach to the syndrome. The condition is a challenging one for the physiotherapist and the improvement is pleasing.
Breathing is a very complex system that is affected by many stimuli and appears to have effects other than the exchange of gases (van Dixhoorn 1996). Some patients’ symptoms may be attributed to various dysfunctional aspects within the inherent mechanisms of the afferent and efferent responses of the breathing system, other than the variable or low levels of PaCO2. Many phenomena are not yet understood and there are many areas inviting research. Work is currently in progress in a few centres, which should offer a greater understanding of the physiological sensitivities and complexities and the interplay of feedback loops in the breathing system in relation to individual responses to life events.
DYSFUNCTIONAL BREATHING IN ASTHMA AND COPD
Breathing pattern modulation
Based on the understanding that the pattern of breathing and the central control mechanisms can be changed (Grossman et al 1985), a programme of breathing pattern re-education should be a positive part of the total care management plan. The knowledge of the underlying causes of the breathing problem, the capacity to recognize the onset of acute problems and the ability to alter the method of breathing appropriately would not only decrease the anxiety that the patient experiences but also make a positive input to the actual process of ventilation.
HYPERVENTILATION AND ASTHMA
The relationship between hyperventilation and asthma is ambiguous. Papers regarding ‘dysfunctional breathing and asthma’ relate to overbreathing or a hyperventilatory component and not to the typical disrupted pattern of ‘gasping in’ and ‘squeezing out’ of acute asthma. Hyperventilation does appear to be one factor in acute asthma, either in cause or effect. Panic or anxiety could exacerbate the symptoms of asthma by their propensity to stimulate hyperventilation. Hammo & Weinberger (1999) have shown that chest discomfort and dyspnoea, in some children, precipitated by exercise are associated with hypocapnia from hyperventilation rather than a true exercise-induced asthma. They suggest that an atypical history in the form of late onset, the absence of other symptoms of asthma, the absence of response to inhaled β2-agonist and a competitive personality should alert physicians to this alternative diagnosis of ‘exercise-induced hyperventilation’ rather than misdiagnose asthma.
Osborne et al (2000) have demonstrated that decreased airflow in a group of patients diagnosed with asthma was related to a low PaCO2 and end-tidal PCO2 in association with hyper-responsive airways, rather than to airway obstruction or mucosal inflammation. In some people with ‘mild asthma’, hypocapnia may be responsible for the increase in smooth muscle contractility rather than true asthma. These patients would benefit by learning breathing control, which includes the rest periods and breath-holds as described above.
Regulation of the breathing pattern with regard to true asthma should be taught ideally when the patient is in good health and would incorporate the techniques already described, when deemed appropriate. Finding a basic pattern together would give confidence and reduce the risk of panic. Control of air through the nose helps to regulate the pace, keeps the flow as laminar as possible and prevents any unnecessary irritation of the airways as when cold, fast moving air is drawn in through the mouth. Encouragement is given to move the air as smoothly as possible and to raise the respiratory level of each breath by not breathing out to the end and by starting inspiration a little sooner in the cycle. This should help to prevent excessive compression of the airways and allow a freer flow of air. Learning to cope with an acute attack would include changing the pattern of inspiration from the upper chest and shoulder girdle to the diaphragm. This would be encouraged by appropriate resistance, given by the physiotherapist’s hands, to encourage a gentle swelling of the abdominal wall. A relaxed passive expiration is the norm, but during a period of extreme airways obstruction a degree of abdominal contraction will probably be necessary and it should be taught to be controlled rather than forced, and not extended too far towards full expiration. Greater control of this new pattern and some confidence to ward off attacks can be gained by practising changing back and forth between thoracic ‘in and up’ breathing and diaphragmatic ‘in and down’ breathing (Innocenti 1974). Free exercise and posture awareness will help to prevent the possibility of deformity in children.
Clinically relevant improvements in quality of life scores have been seen in patients who have received breathing retraining (Thomas et al 2003).
Kellet & Mullan (2002) comment that techniques regarding control of flow rate, tidal volume, cadence, place of movement and the three-phase cycle described here have similarities with those described by Buteyko. They suggest that physiotherapists are ideally placed to develop and research these techniques and if they are shown to be of value it may herald the dawn of a new era in the management of asthma.
The Buteyko breathing technique is spreading in Australia, New Zealand and United Kingdom. The technique is based on the theory that hyperventilation is a major cause of asthma and the technique of ‘reducing the depth and frequency of respiration’ and of breath-holding is taught, together with other input. It seems to be based on a similar understanding of the need to upregulate the PaCO2 levels. The regimen appears to be a fixed formula, which is imposed on everyone in the group. The training occurs over 7 days; each session lasts 60–90 minutes and consists
‘… of exercises in which subjects reduced the depth and frequency of respiration. Breath-holding exercises measured the impact of this training and gauged progress. Participants were encouraged to practise these exercises several times a day.’
‘People experiencing difficulty with the technique were given extra breathing classes’
DYSFUNCTIONAL BREATHING IN EMPHYSEMA
Correspondence (Connolly 2003) on ‘dysfunctional breathing in COPD’ appears to relate to a general feeling of breathlessness. This may be so, but no comment is made regarding the different forms of breathing patterns that evolve due to the specific pathological changes effected in emphysema and chronic bronchitis. The typical pattern in emphysema is one of a prolonged ‘push-out’ expiration, frequently with pursed lips and a further tightening of the abdominal muscles, followed by a quick gasping inspiration.
There is little change in the volume of the emphysematous areas during the ventilatory cycle. They appear to act as space-occupying lesions. Prolonged expiration, therefore, does not produce significant emptying of the emphysematous spaces; rather, it compresses the normal lung tissue and the unsupported airways. Pursed lip breathing tries to keep the airways open longer by increasing the intraluminal pressure; this it does, but the work of breathing is increased and not much more air is moved.
Therefore more space and less expiratory pressure is required to prevent the early closure of the unsupported airways and to allow the unaffected lung tissue to participate more effectively in the ventilation. Airflow is freer and less expensive of energy, when the expiratory pattern with muscle contraction (with or without pursed lips) is reversed to an inspiratory pattern with a slightly raised resting respiratory level.
Re-education can take place in the sitting position and after attention has been drawn towards the upper chest expiratory pattern, it is then directed towards an abdominal inspiratory pattern. Appropriate manual resistance is given by the physiotherapist’s hands on the abdomen throughout inspiration, to stimulate diaphragmatic descent. The resistance is gradually released as expiration takes over. This should not be prolonged; rather, the next inspiration is begun a little sooner than previously, thus raising the resting respiratory level a few cubic centimetres (Fig. 17.5) (Innocenti 1966). Care must be taken to ensure that the breathing rate is not slowed, such that the patient becomes more breathless. A comfortable pace and level of flow should be found to improve ventilation and comfort. Although these procedures have been reported as beneficial and practised for many years, there has been no formal research to replicate the original laboratory findings of improved air flows and reduced intrathoracic pressures (Innocenti 1966), and to test objectively the subjective reports of improved exercise tolerance, well-being and activities of daily living.
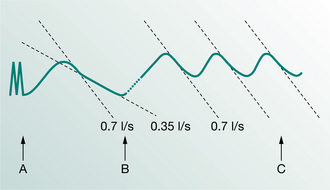
Figure 17.5 Tracing showing the effect of raising the resting respiratory level by approximately 300 cc. Note the velocity of airflow remains higher for a greater part of expiration (taken from the tracing of a severely disabled patient). (A–B), old pattern level; (B–C), new pattern level (from Innocenti 1966).
MUSCULOSKELETAL INTERVENTION
Dysfunctional breathing inevitably induces both structural and functional changes in the musculoskeletal system (Chaitow 2002). These changes, in turn, affect breathing function, thus perpetuating a chronic cycle. Where there is evidence of musculoskeletal compromise in this patient group and treatment includes breathing techniques only, it may be difficult for a patient to revert to, and maintain, a normal breathing pattern. Despite effective respiratory intervention, the patient may be unable to master the diaphragmatic pattern of breathing. This may be due to over-riding dominance in the accessory muscles of respiration, thoracic hypomobility, excessive activity in the rectus and oblique abdominals which restricts free descent of the diaphragm, costovertebral dysfunction or increased myofascial tone. Alternatively, the patient may be able to master the breathing pattern in a relaxed supported position, but it may not become functionally integrated and their symptoms persist. In clinical practice, when the musculoskeletal and postural dysfunction is addressed, which may include manual release techniques for the diaphragm in order to enhance its contraction and relaxation functions, the patient is often seen to revert more easily to the lower chest, diaphragmatic pattern of breathing. However, there is as yet little evidence to support this clinical finding.
The effects of dysfunctional breathing on the musculoskeletal system, and the importance of breathing retraining in musculoskeletal physiotherapy, are becoming more widely recognized. Re-education of the diaphragmatic pattern of breathing in a supported neutral spine position is the first stage in stability training for low back pain (Richardson et al 2004). Clinically, physiotherapists specializing in musculoskeletal work see a high incidence of postural-based musculoskeletal dysfunction in patients who spend prolonged periods driving, sitting at a desk or working on computers, particularly if the seating arrangements are not ergonomically sound. Invariably exacerbation of their symptoms is associated with an increase in work or family demands, poor sleep, stress and insufficient ‘time-out’. A stressful meeting, phone call or commute can be enough to aggravate their symptoms. The patient may present to physiotherapy complaining of widespread (or localized) aches, pains and stiffness with or without a mechanical pattern. Often the symptoms are worse at the end of the day, and may fluctuate depending on factors such as stress, emotion and fatigue. In this group of patients there is very commonly an associated breathing dysfunction which, when addressed, can significantly contribute to their recovery and management of symptoms. When the breathing dysfunction is not addressed, the physiological consequences of hyperventilation (ischaemia, fatigue and pain, increased sympathetic arousal, spasm and reduced pain thresholds) will continue to drive the musculoskeletal complaint. As such, the patient may only derive temporary benefit from treatment or the problem may recur. A joint management approach may be required in this patient group for optimal outcome.
Posture
Normal breathing function relies upon correct postural alignment. The classic postural set described by Janda (1983) as the ‘upper-crossed syndrome’ with a forward head posture, thoracic kyphosis and anterior shift of the pelvis with reduced abdominal and gluteal tone can, over time, lead to breathing dysfunction, chronic musculoskeletal complaints and a cyclic link between the two. Poor postural habits are known to contribute to myofascial dysfunction (Edwards 2005). Assessment of posture and early education regarding the importance of correct alignment for the optimal functioning of the respiratory and musculoskeletal systems are integral parts of the rehabilitation process in this patient group. The patient should be in a relaxed state for postural re-education. Diaphragmatic breathing in a supported supine position, and appropriate manual therapy techniques should be applied before postural retraining in order to bring the body into an optimal state to accept the aligned posture. Re-education should occur in both sitting and standing. The patient should be encouraged to become aware of their individual postural habits and how these affect their respiratory function and musculoskeletal system. The patient should be taught to correct their alignment independently and this may take several sessions. Often in an enthusiastic attempt to achieve ‘good posture’ patients may overcorrect and extend excessively through the thoracolumbar junction. This is not favourable, can reinforce an upper chest-breathing pattern, and will ultimately lead to further musculo-skeletal problems. We are aiming to normalize posture and movement, not overcorrect it. Any habit takes conscious retraining to change, and posture is no exception. At first the aligned posture will feel unnatural to the patient; however, over time, this will become their new norm. The patient should be encouraged to accept this change.
Assessment
It is useful to evaluate the musculoskeletal system as to whether it is the primary cause of, or consequential to, the breathing dysfunction. Referral to a musculoskeletal physiotherapist may be appropriate. A suggested guideline is as follows:
Management
Treatment clearly depends on assessment findings. Manual techniques such as mobilization, muscle energy techniques (MET), proprioceptive neuromuscular facilitation (PNF), trigger point release and myofascial release can help to normalize joint, fascial and muscular restrictions. There are several books which describe these techniques in detail, including Cantu & Grodin (2000), Chaitow (2001), Chaitow et al (2002) and Maitland et al (2005), listed in ‘Further reading’. A great number of techniques may be applied to each individual and their effectiveness needs to be assessed within and between treatment sessions. Outcome measures may include measurement of rib expansion, range of movement, observation of breath pattern and ease of postural alignment.
In conjunction, specific movement retraining may be necessary to improve stability with smooth execution and efficiency of movement. For example, a common habit is to fix or grip unnecessarily through the upper trapezius in activities of daily living (ADLs). This type of movement habit will encourage overactivity in the accessory respiratory muscles and reinforce the dysfunctional breathing pattern. This is just one example of a myriad of movement impairments with which the patient may present. A functional motor control approach whereby normal patterns of movement are facilitated from a well-aligned stable base is suggested. Specific stabilization training may be indicated in this group and the reader is referred to Richardson et al (2004).
CONCLUSION
It is clear that a close relationship exists between the respiratory and musculoskeletal systems. Dysfunction in one can lead directly to dysfunction in the other. In order to restore efficient functioning of each system, a holistic and coordinated approach is required. Patience and perseverance of physiotherapist and patient are necessary for the long-term re-education of the breathing pattern. Each patient’s respiratory system is unique and each physiotherapist will learn new nuances of breathing patterns and new ways of helping to re-educate the system from each patient. The treatment programmes can never be exactly the same, nor should they be imposed rigidly. Each patient needs to be guided to find a personal corrected breathing arrangement, which suits and fulfils the basic physiological principles. The chosen pattern should eventually become the new, unconscious, habitual method of breathing. When pathological conditions are involved an important aspect of training is to control acute exacerbations as best as possible. Likewise, efficient move ment and postural alignment will become recognized as the norm and be integrated into everyday activities, thus helping to break the negative cycle between musculoskeletal and respiratory dysfunction. It is in the experience of many physiotherapists that patients can, and do, change the way they use their bodies and learn how to change their pattern of breathing and how to control it in moments of crisis. Reports of improvements are common. With increasing numbers of people reporting breathing difficulties, it is essential that research is undertaken to ascertain the merits of these procedures.
Patients are currently prescribed drugs, even though the breathing disorder may not have any associated pathology and the risk is that they may become established as the treatment of choice. Those who hyperventilate could be maintained indefinitely on addictive tranquillizers or inappropriate antidepressants (Timmons 1994) and long-term pain medications. In cases where symptoms can be minimized by controlling the breathing pattern and by addressing any related musculo-skeletal dysfunction, drug therapy should be decreased to enable patients to attain their full recovery potential.
The effects of re-education of the breathing pattern and the place of musculoskeletal interventions in this group of patients merit further study and the field is wide open for physiotherapists to research.
Baker DM. Sighing respiration as a symptom. Lancet. 1934;1:174-177.
Ball S, Shekhar A. Basilar artery response to hyperventilation in panic disorder. American Journal of Psychiatry. 1997;154(11):1603-1604.
Bartley J. Nasal congestion and hyperventilation syndrome. American Journal of Rhinology. 2005;19(6):607-611.
Bass C, Gardner WN. Respiratory and psychiatric abnormalities in chronic symptomatic hyperventilation. British Medical Journal. 1985;290:1387-1390.
Bowler SD, Green A, Mitchell CA. Buteyko breathing techniques in asthma: a blinded randomized controlled trial. Alternative Medicine. 1998;169:575-578.
Bradley D. Patterns of breathing dysfunction in hyperventilation syndrome and breathing pattern disorders. In: Chaitow L, Bradley D, Gilbert C, editors. Multidisciplinary approaches to breathing pattern disorders. Edinburgh: Churchill Livingstone; 2002:51.
Callaham M. Hypoxic hazards of traditional paper bag rebreathing in hyperventilating patients. American Emergency Medicine. 1989;18(b):622-628.
Chaitow L. Biomechanical influences on breathing. In: Chaitow L, Bradley D, Gilbert C, editors. Multidisciplinary approaches to breathing pattern disorders. Edinburgh: Churchill Livingstone; 2002:83.
Clark TJH, Cochrane GN. Effect of personality on alveolar ventilation in patients with chronic airways obstruction. British Medical Journal. 1970;1:273-275.
Connolly CK. Dysfunctional breathing in COPD. Thorax. 2003;58:460-461.
Cowley DS, Roy-Byrne PP. Hyperventilation and panic disorder. American Journal of Medicine. 1987;83:929-937.
Edwards J. The importance of postural habits in perpetuating myofascial trigger point pain. Acupuncture Medical Journal. 2005;23(2):77-82.
Folgering H, Ruttern H, Rouman Y. Beta-blockade in the hyperventilation syndrome. A retrospective assessment of symptoms and complaints. Respiration. 1983;44(1):19-25.
Freeman LJ, Nixon PGF. Chest pain and the hyperventilation syndrome: some etiological considerations. Postgraduate Medical Journal. 1985;61:957-961.
Gardner WN. Diagnosis and organic causes of symptomatic hyperventilation. In: Timmons BH, Ley R, editors. Behavioural and psychological approaches to breathing disorders. New York: Plenum Press; 1994:99-112.
Gardner W. Orthostatic increase of respiratory gas exchange in hyperventilation syndrome. Thorax. 2000;55:257-259.
Gardner WN, Bass C. Hyperventilation in clinical practice. British Journal of Hospital Medicine. 1989;41(1):73-81.
Glyn C, Lloyd JW, Folkard S. Ventilatory responses to intractable pain. Pain. 1981;11(2):201-211.
Grossman P, De Swart JCG, Defares PB. A controlled study of a breathing therapy for treatment of hyperventilation syndrome. Journal of Psychosomatic Research. 1985;29(1):49-58.
Hammo AH, Weinberger MM. Exercise-induced hyperventilation: a pseudoasthma syndrome. Annals of Allergy, Asthma and Immunology. 1999;82(6):574-578.
Hardonk HJ, Beumer HM. Hyperventilation syndrome. In: Vinken PJ, Bruyn GW, editors. The handbook of clinical neurology. Amsterdam: North Holland; 1979:309-360.
Hibbert G, Pilsbury D. Hyperventilation in panic attacks. Ambulant monitoring of transcutaneous carbon dioxide. British Journal of Psychiatry. 1988;153:76-80.
Hodges PW, Butler JE, McKenzie DK, Gandevia SC. Contraction of the human diaphragm during rapid postural adjustments. Journal of Physiology. 1997;505(Pt 2):539-548.
Hodges PW, Gandevia SC. Activation of the human diaphragm in a repetitive postural task. Journal of Physiology. 2000;522(Pt 1):165-175.
Hodges PW, Heijnen I, Gandevia SC. Postural activity in the diaphragm is reduced in humans when respiratory demand increases. Journal of Physiology. 2001;537(Pt 3):999-1008.
Hornsveld HK, Garssen B, Fiedeldij Dop MJC, Van Spiegel PI, De Haes JCJM. Double blind placebo-controlled study of the hyperventilation provocation test and the validity of the hyperventilation syndrome. Lancet. 1996;348:154-158.
Howell JBL. The hyperventilation syndrome: a syndrome under threat? Thorax. 1997;52(3):S30-s34.
Hruska RJJr. Influences of dysfunctional respiratory mechanics on oro-facial pain. Dental Clinics of North America. 1997;41(2):211-227.
Humphriss RL, Baguley DM, Anderson G, Wagstaff S. Hyperventilation in the vestibular clinic: use of the Nijmegen questionnaire. Clinical Otolaryngology and Allied Sciences. 2004;29(3):232-237.
Innocenti DM. Breathing exercises in the treatment of emphysema. Physiotherapy. 1966;52(12):437-441.
Innocenti DM. Physiotherapy in the management of acute asthma. Nursing Mirror July. 1974;12:77-79.
Jack S, Rossiter HB, Warburton CJ, Whipp BJ. Behavioural influences and psychological indices of ventilatory control in subjects with idiopathic hyperventilation. Behaviour Modification. 2003;27(5):637-652.
Janda V. Muscle function testing. London: Butterworths, 1983.
Kellet C, Mullan J. Breathing control techniques in the management of asthma. Physiotherapy. 2002;88(12):751-758.
Kerr WJ, Dalton JW, Gliebe PA. Some physical phenomena associated with the anxiety states and their relation to hyperventilation. Annals of Internal Medicine. 1937;11:961-992.
Lum LC. Hyperventilation syndromes: physiological considerations in clinical management. In: Timmons BH, Ley R, editors. Behavioural and psychological approaches to breathing disorders. New York: Plenum Press; 1994:113-123.
Malmberg LP, Tamminen K, Sovijarvi ARA. Orthostatic increase of respiratory gas exchange in hyperventilation syndrome. Thorax. 2000;55:295-301.
Miyazaki H, Yamashita H, Masuda T, Yamamoto T, Komiyama S. Transcutaneous PCO2 monitoring in the evaluation of hyperventilation of patients with recurrent nerve paralysis. European Archives of Otorhinolaryngology. 1999;256(1):S47-S50.
Mogyoros I, Kiernan MC, Burke D, Bostock H. Excitability changes in human sensory and motor axons during hyperventilation and ischaemia. Brain. 1997;120(Pt 2):317-325.
Morgan MDL. Dysfunctional breathing in asthma: is it common, identifiable and correctable? Thorax. 2002;57(Suppl 11):ii31-II35.
Naschitz JE, Mussafia-Preselac R, Koalev Y, et al. Patterns of hypocapnia on tilt in patients with fibromyalgia, chronic fatigue syndrome, non-specific dizziness and neurally mediated syncope. American Journal of Medical Science. 2006;331(6):295-303.
Nijs J, Meeus M, De Meirleir K. Chronic musculoskeletal pain in chronic fatigue syndrome: recent developments and therapeutic implications. Manual Therapy. 2006;11(3):187-191.
Nixon PGF, Freeman LJ. The ‘think test’: a further technique to elicit hyperventilation. Journal of the Royal Society of Medicine. 1988;81:277-279.
Ofluoglu D, Gunduz OH, Kul-Panza E, Guven Z. Hypermobility in women with fibromyalgia syndrome. Clinical Rheumatology. 2006;25(3):291-293.
Osborne CA, O’Connor BJ, Lewis A, Kanabar V, Gardner WN. Hyperventilation and asymptomatic chronic asthma. Thorax. 2000;55:1016-1022.
Papp LA, Klein DF, Gorman JM. Carbon dioxide hypersensitivity, and panic disorder. American Journal of Psychiatry. 1993;150(8):1149-1157.
Pilsbury D, Hibbert GA. An ambulatory system for long term continuous monitoring of transcutaneous PCO2. Clinical Respiratory Physiology. 1987;23:9-13.
Richardson C, Hodges P, Hides J. Therapeutic exercise for lumbopelvic stabilisation. Edinburgh: Churchill Livingstone, 2004;185-219.
Smith MD, Russell A, Hodges PW. Disorders of breathing and continence have a stronger association with low back pain than obesity and physical activity. Australian Journal of Physiotherapy. 2006;52(1):11-16.
Terekhin P, Forster C. Hypocapnia-related changes in pain-induced brain activation as measured by functional MRI. Neuroscience Letters. 2006;400(1-2):110-114.
Thomas M, McKinley RK, Freeman E, et al. Breathing retraining for dysfunctional breathing in asthma: a randomised controlled trial. Thorax. 2003;58:110-115.
Timmons BH. Breathing-related issues in therapy. In: Timmons BH, Ley R, editors. Behavioral and psychological approaches to breathing disorders. New York: Plenum Press; 1994:261-292.
Tweedale PM, Rowbottom I, McHardy GJR. Breathing retraining: effect on anxiety and depression scores in behavioural breathlessness. Journal of Psychosomatic Research. 1994;38(1):11-21.
Troosters T, Verstraete A, Ramon K, et al. Physical performance of patients with numerous psychosomatic complaints suggestive of hyperventilation. European Respiratory Journal. 1999;14:1314-1319.
van den Hout MA, Hoekstra R, Arntz A, et al. Hyperventilation is not diagnostically specific to panic patients. Psychosomatic Medicine. 1992;54(2):182-191.
van Dixhoorn J, 1996 Hyperventilation and dysfunctional breathing. A presentation at the Third Annual Meeting of the International Society for the Advancement of Respiratory Psychophysiology (ISARP), University of Nijmegen
van Dixhoorn J, Duivenvoorden HJ. Efficacy of Nijmegen questionnaire in recognition of the hyperventilation syndrome. Journal of Psychosomatic Research. 1985;29(2):199-206.
van Doorn P, Colla P, Folgering H. Control of end-tidal PCO2 in the hyperventilation syndrome: effects of biofeedback and breathing instructions compared. Bulletin Europeen de Physiopathologie Respiratoire. 1982;18:829-836.
Vansteenkiste J, Rochette M, Demedts M. Diagnostic tests of hyperventilation syndrome. European Respiratory Journal. 1991;4:393-399.
Wood P. Da Costa’s syndrome (or effort syndrome). British Medical Journal. 1941;1:767-772., 805-811, 845-851
Yates BJ, Bronstein AM. The effects of vestibular system lesions on autonomic regulation: observations, mechanisms and clinical implications. Journal of Vestibular Research.. 2005;15(3):119-129.
Yates BJ, Miller AD. Physiological evidence that the vestibular system participates in autonomic and respiratory control. Journal of Vestibular Research. 1998;8(1):17-25.
Yates BJ, Billig I, Cotter LA, Mori RL, Card JP. Role of the vestibular system in regulating respiratory muscle activity during movement. Clinical and Experimental Pharmacology and Physiology. 2002;29(5):112-117.
Cantu RI, Grodin AJ. Myofascial manipulation. USA: Aspen Publishers Inc., 2000.
Chaitow L. Muscle energy techniques, 2nd edn., Edinburgh: Churchill Livingstone, 2001.
Chaitow L, Bradley D, Gilbert C. Multidisciplinary approaches to breathing pattern disorders. Edinburgh: Churchill Livingstone, 2002.
Lum LC. The syndrome of chronic hyperventilation. In: Hill O, editor. Modern trends in psychosomatic medicine. London: Butterworths; 1976:196-230.
Maitland G, Henglefeld E, Banks K, English K. Maitland’s vertebral manipulation, 7th edn., Edinburgh: Butterworth-Heinemann Ltd, 2005.
Timmons BH, Ley R. Behavioral and psychological approaches to breathing disorders. New York: Plenum Press, 1994.