8 Vertebral Column
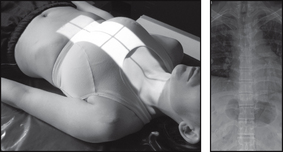
CERVICAL SPINE
Centring Point: To the sternal notch – then angle the central ray cranially to the thyroid cartilage. Central ray approximately 15° cranially
Points to consider
Technique
 Remember to set the exposure before positioning
Remember to set the exposure before positioning
Remember to remove jewelry that is in the field of interest and dentures/orthodontic appliances where possible
AP C1–C3 – adjust patient so that occipital bone and lower edge of upper incisors are superimposed
 AP C1–C3 – patient may overextend the head when opening the mouth
AP C1–C3 – patient may overextend the head when opening the mouth
AP – mental region of mandible should be superimposed over the occiput

AP C1–C3
CERVICAL SPINE

Points to consider
Technique

Radiological assessment
Anterior displacement over 3.5 mm – ligaments torn
Vertebral bodies C3–T1 should be the same size – a disparity of 2 mm may be due to a compression #
Check all seven vertebrae are seen on the radiograph
Oblique – demonstrates intervertebral foramina closest to the film (right anterior oblique – right foramina; left anterior oblique – left foramina)
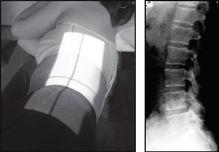
Lateral
• Patient in the erect position with the shoulder against the cassette
• Median sagittal plane parallel to the cassette
• Patient’s shoulders should be relaxed and arms are placed down and slightly behind the trunk
• Feet are separated to aid stability
• Patient’s chin is raised and extended slightly forwards so that the mandible does not obscure the spine
Anterior obliques – both sides for comparison
CERVICOTHORACIC


THORACIC SPINE

Points to consider
Technique

Radiological assessment
AP – abnormal soft tissue enlargement around the spine is a positive indication of trauma or infection
Check all pedicles are present and intact
Vertebral bodies should be the same height – anteriorly and posteriorly
Lateral – upper spine difficult to visualise due to shoulders. A swimmer’s projection may be required – CT is better
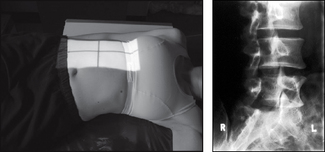
LUMBAR SPINE
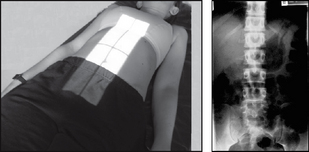
Centring Point: 8–10 cm anterior to the third lumbar spinous process at the level of the lower costal margin
Points to consider
Technique
AP – reduce lumbar lordosis – flex knees and support where indicated
AP – ensure sacroiliac joints included on the radiograph
AP and lateral – exposure on arrested expiration – diaphragm should be above L1 – or try breathing technique to blur bowel shadows
Lateral – non-opaque pad under the waist may assist in bringing the spine parallel to the table top
Use gonad shield – but take care not to obscure the area of interest

Radiological assessment
AP – distance between pedicles gradually widens from L1 to L5
AP – must inspect the transverse processes for #
Check soft tissue changes – may indicate underlying pathology – renal stones mimic skeletal back pain
Lateral – vertebral bodies should be same height anteriorly and posteriorly
Any loss of height or wedging suggests a possible compression #
AP
LUMBAR SPINE
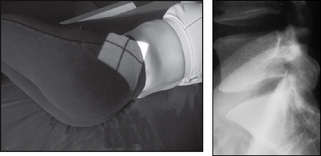
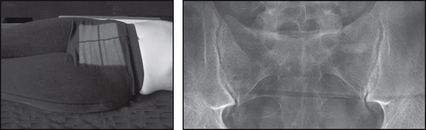
Projection: LUMBOSACRAL JUNCTION (L5–S1)
Centring Point: 8 cm anterior to the fifth lumbar spinous process
Points to consider
Technique

Radiological assessment
Disc space at L5–S1 – usually smaller than at L4–L5
Joint space must be visualised open
Obliques – suspected spondylolisthesis – a defect in pars articularis – look for a collar around the Scottie dog’s neck!
Obliques – will demonstrate superior and inferior articular processes and the zygopophyseal joints of the side nearest the cassette
SACRUM
Centring Point: Midline 5 cm above superior border of symphysis pubis. Cranial – central ray: 10° male, 20° female