3 Types of surgical nursing opportunities and clinical placements
Surgical nursing placements
For many of you, a surgical nursing placement will be one of many placements you will experience in your programme of study, depending of course on the learning outcomes to be achieved as well as the specific requirements of your field of practice. In the main, placements where you are assessed in relation to the NMC Standards must be a minimum of 4 continuous weeks, but you may have shorter experiences in a surgical environment as part of a ‘hub and spoke’ approach to learning. Other terms used by the NMC (NMC 2010) are ‘placement learning pathways’, ‘placement learning opportunities’ and ‘insight days’, all focused on offering students opportunities to develop their skills and enhance their knowledge of ‘understanding and supporting the patient journey’ (NMC 2010:40).
The length of time in a placement will be determined initially by your curriculum requirements. Discussion with your mentor about what you can realistically achieve in terms of clinical skills and patient care experience will ensure you meet the required learning outcomes and competences for that placement (see Ch. 4 for a discussion of placement learning opportunities).

Imagine you have been told that your next placement is a surgical nursing one and you have no prior experience of visiting one nor have you worked on one as a healthcare assistant.
What do you imagine the environment will look like that is different to a medical nursing placement? Consider the explanations offered in Chapters 1 and 2 regarding the nature of surgical nursing and section on Description of a Surgical ward for further discussion of what a surgical ward may look like.
In the main, placements identified as ‘surgical’ are normally named or relate to various aspects of medical care or anatomy and physiology/systems of the body. Each one is a specialty with specific nursing-related care, but each involves the same perioperative process. Here are some examples:
Consider all these types of surgery and find out what ‘body systems’ they are associated with. Use a nursing dictionary to help you identify the kind of surgery that normally takes place in your placement.
You will have discovered the following:
• Orthopaedic surgery involves surgery of the musculoskeletal system.
• Ear, nose and throat surgery involves surgery of the ear, nose and throat, including the larynx.
• Gynaecology surgery involves surgery of the female reproductive system.
• Vascular surgery involves surgery of the arteries and veins.
• Abdominal surgery involves surgery of abdominal organs such as liver, bowel, stomach, gall bladder.
• Renal and urinary tract surgery involves surgery of the kidney and related organs and systems.
• Neurological surgery involves surgery of the brain and spinal cord.
• Ophthalmic surgery involves surgery of the eye and related structures.
• Thoracic/chest surgery involves surgery of the respiratory organs.
• Breast surgery involves surgery of the breast – male and female.
• Cardiac surgery involves surgery of the heart.
• Plastic surgery involves reconstructive surgery in varied parts of the body.
You may be undertaking a placement that is simply identified as a general surgical ward, and here you may meet patients undergoing a range of surgical interventions. It is up to you to be knowledgable about general and specific surgery, as well as anatomy and physiology. (We explore why it is important to revise anatomy and physiology prior to your placement throughout the book, but especially in Section 3.)
Further reading related to surgical placements can be found at the end of Chapter 4.
Description of a surgical ward
It is important to remember that each hospital and its layout varies. All we can consider here is a basic idea of what a surgical ward might look like and the kind of equipment and activities you are likely to encounter.
A surgical ward is usually a very busy environment, with patients being taken back and forth to theatre by nurses, theatre attendants and other relevant personnel. (Other linked placements are described in Section 2: for example, the operating theatre.)
Consider what you imagine a surgical ward might look like. Have a look at some photos on the Internet or in books to compare current images and past images.
If you have been a patient or visitor on a surgical ward, is your first impression of the placement the same as you recall?
When you go to the placement for the first time, note the layout of the ward and what makes it identifiable as a surgical placement as opposed to an outpatient placement. What kinds of objects and activities make it identifiable as such?
Read Holland's (1993) article, which describes an ethnographic study carried out on a surgical ward, for a description of what she calls ‘cultural artefacts’ and specific practices she observed which clearly identified it as a surgical ward. Specific language used in communication between nurses was also an indicator. (See Box 3.1 for some of her observations.)
Box 3.1 Data from an ethnographic description of a nursing cultural scene
Description of the ward
The patients who were part of this particular cultural scene were allowed in on the basis that they had a medically diagnosed, specific, disordered body function which required surgical intervention. The nature of their treatment gave the ward its name (i.e. a surgical ward), thus differentiating it from others within the hospital.
For instance, domain analysis of ‘kinds of surgical intervention’ – right inguinal hernia repair, mid-thigh amputation, appendicectomy, draining of rectal abscess, transurethral prostatectomy.
Description by one nurse of what would make them take someone's temperature or not
Um well, the charts, really I know I shouldn't say that but I go to the charts…If someone is pre-op, it should be morning and evening…post-op should be 4-hourly for signs of infection and until the wound heals sufficiently…If they look like they've got a temperature or feel hot, take it in-between times, if they were chesty or look like they've got a urine infection…(Mary)
(From Holland 1993)
Some students, however, are not happy about where they are to undertake their placement, complaining that they won't learning anything there. This is often an issue of perception, perhaps influenced through personal experience or that of a relative.

Consider the following example from a student at the beginning of their second year of study.
‘I am going to a day surgery ward. What am I going to learn there? I want to be caring for patients who have big operations and lots going on. It's going to be really repetitive and boring.’
We [KH and Student] discussed generally the kinds of experience he could have and he was advised to set very clear learning goals with regards to the patient journey.
On his return from placement, he said he had had a brilliant time and had learned loads of things! Among these, he had experienced meeting a patient, going with him to theatre, staying with him during surgery, staying with him in the recovery room and being there for him when he woke up in a strange environment and then taking him back to the ward and caring for him until he was discharged home from hospital that evening.
It had not been possible for the student to follow up the patient after his discharge home, but this is one aspect of care that can be negotiated with your mentor. It may be possible to visit patients in their home/community setting through liaising with the health centre/district nurse who may be in charge of their care.

Consider how your placement experience might help you to attain the NMC competences. For those of you who are expected to meet the NMC 2004 Standards and Competencies, the wording of those identified here will be similar – please note, however, that there are now field-specific competencies to achieve. See Box 3.2 for an example for adult students undertaking the adult nursing pathway.
Box 3.2 Domain: Nursing Practice and Decision Making (NMC 2010)
Generic Standard for Competence
Graduate nurses must practise in a compassionate, respectful way, maintaining the dignity and wellbeing of all concerned. Decision making must be person-focused, and through a process of critical analysis leading to a range of technical skills and nursing interventions from basic to highly complex. They must practise in a safe and confident manner, in various care settings, understanding how the environment and location of care delivery can have an impact on health and outcomes. All practice must be based on current evidence and up-to-date technology.
Competencies
1. All nurses must work closely with individuals, groups and carers, using a range of skills to carry out comprehensive, systematic and holistic assessments. These must take into account current and previous physical, social, cultural, psychological, spiritual, genetic and environmental factors that may be relevant to the individuals and their families.
2. All nurses must listen, recognise and respond to an individual's physical, social and psychological needs. They must then plan, deliver and evaluate technically safe, competent, person-centred care that addresses all their daily activities, in partnership with people and their carers, families and other professionals.
Placement learning opportunities and pathways in surgical nursing placements
The NMC (2010) guidance stresses the importance of placement learning in the community and hospital in order to gain a holistic understanding of patients' journeys through health and social care services as well as the competencies to be able to work on registration in either environment. As a student whose main placement is on a surgical ward, how then can you gain experience in the community?
Consider the following pathway options which include various learning opportunities and experiences.
Mapping of potential surgical placement learning pathways
Example for a 10-week placement: the patient journey (pre-planned pathway)
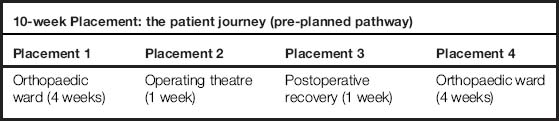
In this option, you can see that as a ‘pre-planned’ pathway, the student experience has been mapped out for a hospital placement with a clearly defined journey. Some of you will already have experienced this kind of planned surgical experience.
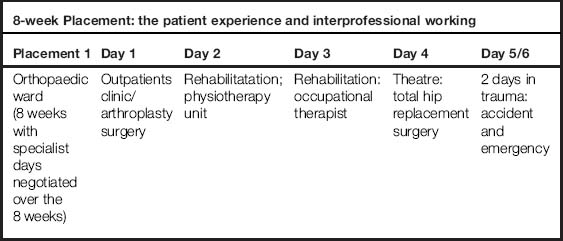
Example for an 8-week placement: the patient experience and interprofessional working (learning outcomes negotiated with mentor and personal tutor)
In this option, however, there are still experiences which enable the student to gain an understanding of what a patient's surgical journey may be like, but this pattern is a negotiated learning experience which many of you know as a ‘hub and spoke’ model, or a ‘base and insight learning days’ approach. In this kind of experience, the interprofessional aspects can be much more clearly defined and if you have to gain this experience to meet specific learning outcomes on interprofessional working in practice, then this negotiated learning would be beneficial. It is important to remember that in any kind of placement learning pathway, negotiating learning outcomes around interprofessional working is an essential part of achieving your NMC competences to practice.
Example for a 14-week placement: an integrated hospital/community plan: the patient experience and journey (a pre-planned allocation pathway)
This option is a pre-planned and allocated one, usually by the placement learning unit at university, in collaboration with practice colleagues such as practice education facilitators.
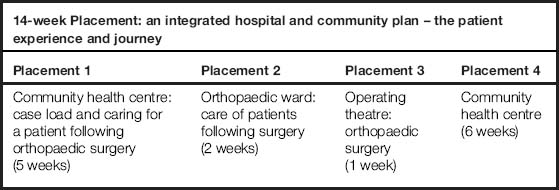
This is the kind of placement that a student may undertake in the final year of their programme of study, when they would be assessed as fit for practice by their sign off mentor. Importantly, however, there is the option and opportunity within their allocated case load to gain leadership and management competencies as well as those of communication and interpersonal skills, nursing practice and decision making and professional values, but including a ‘surgical’ patient journey.
Imagine you have an 8-week allocation to a surgical placement, a ward that specialises in cardiothoracic surgery. What kind of surgery would patients experience on this ward?
Plan a learning experience you would like to gain during the 8 weeks, taking account of all resources available. You will find many of these in Chapter 4 regarding university and placement information, and throughout the book with regards to possible learning outcomes and surgical interventions. Use these and any others discussed with your personal tutor to negotiate learning with your named mentor and the practice team.
Note: the NMC has stated that 4 weeks is the minimum number of weeks for a student to be assessed in a clinical placement with regards to their competences. All of these placement options reflect this.
Summary
As well as focusing learning to prepare yourself for specific surgical nursing placements, there is a need to focus on general expectations in relation to what you are expected to achieve by your university as well as the specific programme of study you are undertaking. Chapter 4 considers these in more detail.
Holland C.K. An ethnographic study of nursing culture as an exploration for determining the existence of a system of ritual. Journal of Advanced Nursing. 1993;18:1461–1470.
Nursing and Midwifery Council. Standards for pre-registration nursing education. London: NMC; 2010. Online. Available at: http://standards.nmc-uk.org/PreRegNursing/statutory/background/Pages/introduction.aspx (accessed September 2011)
Callaghan A. Student nurses' perceptions of learning in a perioperative placement. Journal of Advanced Nursing. 2010;67(4):854–864.
Callaghan P. Rethinking clinical placements for mental health nursing students. Mental Health Practice. 2007;10(5):18–20.
Hughes S. Evaluating operating theatre experience. Journal of Perioperative Practice. 2006;16(6):290–298.
Sampson H. Introducing student nurses to operating department nursing. Journal of Perioperative Practice. 2006;16(2):87–94.
RCN website for student nurses and clinical placement experiences with a range of other resources for student nurses: http://nursingstandard.rcnpublishing.co.uk/students/clinical-placements/placement-advice/picking-the-right-placement/student-nurses-should-vary-their-placements (accessed December 2011).