19 Rabbit dacryocystitis
PRESENTING SIGNS
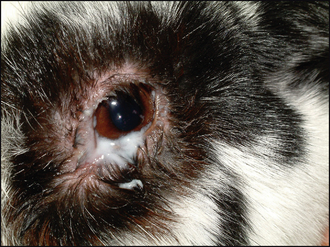
Dacryocystitis, inflammation of the nasolacrimal system, is frequently encountered in rabbits and can be a frustrating condition to manage. Since the aetiology and prognosis are different from dogs (and cats) the condition is being discussed separately. Most rabbits present with unilateral disease but on occasion it can be bilateral. The owners bring the rabbit along because the eye has a nasty discharge. This is usually a thick, whitish, sticky material and can be copious. The medial canthal fur is typically wet and matted and sometimes the rabbit is unable to open the eye as the discharge sticks the lids closed. Sometimes the animal will also show evidence of dental disease, with excessive drooling, anorexia with weight loss and grooming problems (leading to caking of the faeces and so on).
CASE HISTORY
The condition is normally quite gradual in onset – the owners might have been aware that the eye was a bit wet or mucky for several days, or that the rabbit had been off its food for example. There is not normally any specific history suggesting a primary infectious agent (such as the introduction of a new rabbit to the environment). The condition may have occurred previously and if this is the case the owner is more likely to present the rabbit earlier in the course of the disease.
CLINICAL EXAMINATION
Ophthalmic examination will confirm the presence of a copious mucopurulent discharge centred around the medial canthus (Figure 19.1). Samples should be taken for bacterial culture and sensitivity (although samples from nasolacrimal flushings will be more representative – see below). The discharge can then be gently removed, including from the ventral fornix, with damp gauze swabs to facilitate examination. Conjunctival hyperaemia is normally present, often more severe at the medial canthus. Gently pressing the area will result in pus appearing from the single ventral nasolacrimal punctum. The cornea should be evaluated and fluorescein dye used – some patients will have ventromedial corneal ulceration present (presumably related to excoriation by the discharge). Intraocular contents are normally unremarkable although a mild reflex uveitis can be present.
General clinical examination should pay particular attention to the teeth. Overgrowth of both incisor and molar teeth can be the primary problem, as can generalized hyperparathyroidism due to imbalance in the calcium metabolism – often diet related and resulting in poor skull calcification. The rabbit’s bodily condition should also be assessed.
CASE WORK-UP
The most important diagnostic test, which is also an important part of treatment, is to perform a nasolacrimal flush in exactly the same way as in dogs. Most rabbits tolerate this conscious (Figure 19.2). This will differentiate dacryocystitis from a solely conjunctival disease and samples can be obtained for bacterial culture and sensitivity. Once the discharge has been bathed away, including pressing at the medial canthus a couple of times and removing the extra discharge thus produced, topical anaesthetic is instilled into the conjunctival sac. The ventral punctum is cannulated (rabbits do not have an upper punctum) and sterile saline is gently injected. It is likely that initially there will be marked resistance and backflow of purulent discharge around the cannula. However, with repeated gentle attempts hopefully the discharge will be loosened and milky fluid will drip from the ipsilateral nasal punctum. Further flushing and treatment is described below.
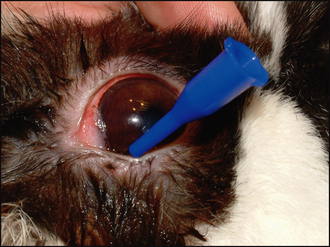
Figure 19.2 Nasolacrimal cannula in place in the sole ventral punctum prior to flushing (the discharge has been bathed away to facilitate localization of the punctum).
In addition to flushing the nasolacrimal duct, careful dental examination is required, with skull radiography if indicated. The prognosis will vary depending on whether dental disease is also present and hence the importance of a complete oral examination.
Frequent bathing of the accumulated discharge will be required and it is important to prevent matting of fur around the medial canthus. Thus clipping the fur in the area and the application of a protectant ointment such as soft petroleum jelly (Vaseline) can be useful – but it is important to ensure that this does not get in the eye. An ophthalmic formulation of soft white paraffin would be more suitable if this is a concern. General husbandry should be checked – for example, sawdust would not make suitable bedding as it could stick to the discharge and the eye, exacerbating the condition. Shredded paper might be more appropriate until the rabbit has recovered.
Topical and sometimes systemic medication will be prescribed. Drop formulations are normally preferred since they will not allow further clogging in the area and will enter the nasolacrimal duct more readily. Some owners find drops more difficult to apply in rabbits due to the lateral placement of their eyes and nurses should show owners the easiest way to medicate their pet.
EPIDEMIOLOGY
The development of dacryocystitis is multifactorial. The pathogens involved are typically opportunists – Escherichia coli, Neisseria and Streptococcus spp. and Pasteurella multocida. The last is frequently cited, and can be a primary pathogen in the rabbit, but in clinical practice is not the most frequent isolate as is often quoted. Mixed infections are common. Normally individual rabbits are affected – it is not usually a contagious disease. Any age and breed can be affected, although it is uncommon in very young animals. Dwarf breeds seem to be particularly susceptible – probably due to their brachycephalic conformation.
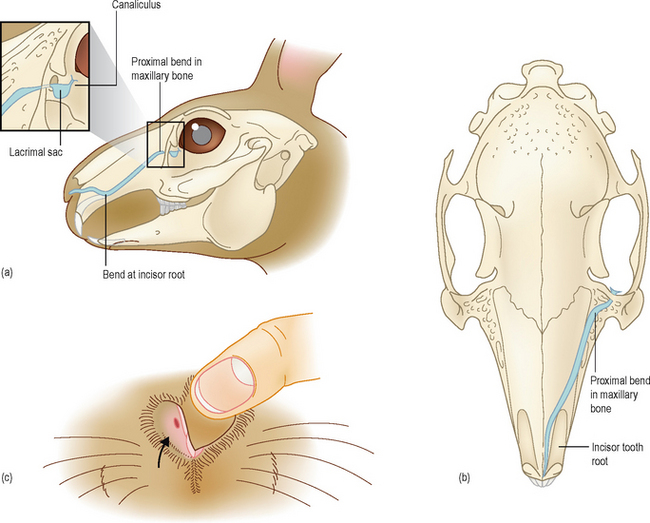
Reduced tear drainage is necessary to allow a build-up of stagnant tears within the duct, which then becomes infected. Extension from a bacterial conjunctivitis is also possible, but less likely, and foreign bodies such as seeds and grass awns can also trigger dacryocystitis. The long, twisted nature of the nasolacrimal duct and its changes in diameter (see below) contribute to the frequency of infections. Additionally, the close association with the teeth roots (molar and incisor) and the presence of open tooth roots in rabbits are predisposing factors.
ANATOMY AND PHYSIOLOGY REFRESHER
An understanding of the anatomy of the nasolacrimal duct and its close relationship with the orbit and tooth roots (molar and incisors) is important in relation to oculodental disease. The rabbit has just one nasolacrimal punctum, situated ventromedially, and the nasolacrimal duct has a convoluted path through the lacrimal and maxillary bones. In addition to the tortuous route, the duct suddenly changes diameter several times and can easily become obstructed in its narrow sections. The duct passes close to the tooth roots of both molars and incisors and subsequently becomes involved with disease processes in the tooth roots (Figure 19.3).
TREATMENT OPTIONS – MEDICAL
Repeated nasolacrimal flushing and appropriate antibacterial medication is the mainstay for the treatment of dacryocystitis in rabbits. How to perform the nasolacrimal flush is described above in the section on case work-up. Normally this can be done in the conscious rabbit with the use of topical anaesthesia; however, if particularly painful, then sedation should be used. Sometimes it is not possible to flush initially. Several gentle attempts are made and if these do not result in any discharge appearing from the ipsilateral nostril, it is best to abandon attempts and treat symptomatically for 48 hours before trying again. A broad spectrum systemic antibiotic such as enrofloxacin and topical gentamicin or ofloxacin is advised. All being well, a second attempt at flushing will be more rewarding. Sterile saline should be used to flush initially and once patency has been established some authors advise a final flush with an antibiotic such as enrofloxacin. However, the pH of injectable forms can be inappropriate, causing stinging, and a 2% (1 : 50 dilution) solution of povidone–iodine might be more suitable. Always ensure that it is the solution and not the detergent formulation that is used. Catheterization of the duct, using fine nylon suture material, is very difficult due to the complicated anatomy and the risk of iatrogenic damage is high. As such it is not recommended.
After successful flushing, the patient is treated with topical and systemic medication for 1–2 weeks and the nasolacrimal duct should be flushed again every few days. Once there is no further discharge it is sensible to repeat a final flush 2–3 weeks later.
In some cases it is not possible to establish drainage at all. This is due to either inspissated pus completely blocking the duct or stenosis at one of the narrow or twisted regions. Dacryocystorhinography can be performed to locate the area of the blockage which might correspond to tooth root problems. Addressing the dental disease, and the rabbit’s diet, might prove beneficial in such cases.
TREATMENT OPTIONS – SURGICAL
Surgery is rarely performed for cases of dacryocystitis. Dental extractions might occasionally be required. If permanently blocked, it is theoretically possible to create another drainage route into the nasal chambers (dacryocystorhinotomy) or mouth (dacryocystobuccostomy) but these procedures are rarely performed in dogs and cats let alone rabbits.
PROGNOSIS
The prognosis for cases of dacryocystitis in rabbits is poor, even if there is no underlying dental disease, but guarded if the latter is present. For simple cases, repeated flushing with antibiotic cover can be curative. However, many cases can be recurrent and pose a frustrating challenge to manage successfully. Some rabbits require life-long flushing on a monthly basis to keep the condition at bay, but an outright cure is not possible. Long-term antibiosis can also be considered. Realizing that this is an oculodental disease, and addressing feeding and other general management issues, can be beneficial.