33 Canine uveitis
PRESENTING SIGNS
Dogs are normally presented with a sudden onset painful eye, often with colour change, and sometimes with reduced vision. The pain is manifested by the patient holding the affected eye closed with increased lacrimation and photophobia. The dog might shy away from attention to this side of its face, or may be seen rubbing the eye. Owners will often also comment that the dog is depressed. The condition can be either unilateral or bilateral. Any age of dog can be affected and there is no particular breed predisposition which is a reflection of the wide variety of causes for uveitis in dogs.
CASE HISTORY
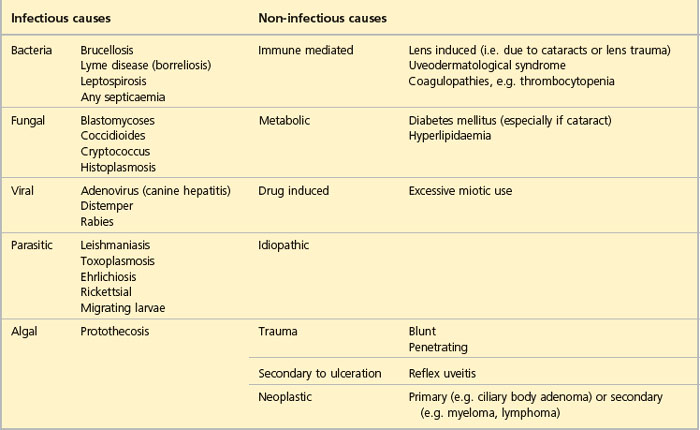
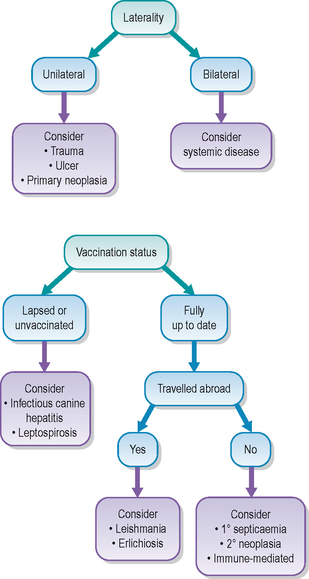
Since there are so many potential causes for uveitis the history can be variable. A few common examples are the dog returning from a walk with a sore eye, which might suggest a traumatic uveitis (due to blunt or penetrating injury). A recently vaccinated puppy might present with a ‘blue’ eye – which despite being a vaccine reaction to the canine adenovirus 1 vaccine is surprisingly often unilateral not bilateral. Thankfully this condition is not commonly encountered with modern vaccines. A history of recent travel abroad, especially to the Mediterranean, might alert one to possible Leishmania infection. The patient might have suffered from mammary carcinoma a few months previously which could be relevant to the ocular symptoms. Thus it is very important in all cases of uveitis to take a detailed history. This can point us in the right direction regarding further diagnostic tests and will help to rule out certain causes of uveitis immediately.
CLINICAL EXAMINATION
General clinical examination can be normal but may show abnormalities. For bilateral cases of uveitis an underlying systemic problem is possible and should be considered. Such patients might be pyrexic, have a lymphadenopathy, foci of pain or an abdominal mass. Unilateral cases might be traumatic, and careful evaluation for evidence of injury (e.g. bite wounds around the face, severe bruising, etc.) might be noted.
The typical ophthalmic signs of uveitis are episcleral congestion with conjunctival hyperaemia, corneal oedema, miosis and increased lacrimation (see Table 33.1). Pain is normally present such that the examination might be resented. The ocular discharge is usually serous. Vision might be reduced, especially if there is posterior segment involvement. Aqueous flare is often present, sometimes along with frank hypopyon or hyphaema. The iris will be dull and swollen, with rubeosis iridis, although this is quite difficult to appreciate in dogs with dark irides as most do have; however, it is readily noted in blue-eyed dogs. Redness might also be present around the limbus encroaching on the cornea – ciliary flush – or inflammation of the deep episcleral vessels with growth into the cornea (Figure 33.1).
Table 33.1 Ophthalmic signs of canine uveitis
| Acute signs | Chronic signs and complications |
|---|---|
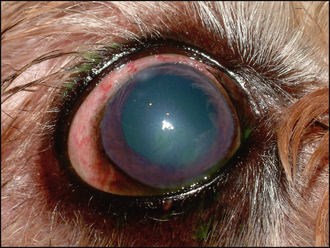
Figure 33.1 Acute anterior uveitis in a Shih Tsu. The pupil has been dilated with atropine but note the episcleral congestion, corneal oedema, out-of-focus appearance to the iris due to aqueous flare and faint fluorescein uptake (ventrally). The dense white spot at 12 o’clock close to the limbus was the site of a traumatic perforation which caused the inflammation. Intraocular pressure was 8 mmHg.
Fluorescein testing should be performed. Usually this will be negative, unless a traumatic incident has occurred or the patient has traumatized the eye secondarily. Measurement of intraocular pressure (IOP) is important and normally readings will be low – commonly 6–10 mmHg. Evaluation of the posterior segment might not be possible. Indirect ophthalmoscopy is likely to be more rewarding than using a direct ophthalmoscope. Mydriasis will assist with fundus examination, but many cases of uveitis will be slow to dilate with tropicamide such that several drops need to be applied over 30–40 minutes before adequate dilation is achieved. Vitreal haze (hyalitis) might be noted along with retinal detachment or areas of active chorioretinitis. These will be seen as dull grey areas within the fundus. Perivascular oedema might be noted as a result of leaky blood vessels. The optic disc is usually normal on examination.
CASE WORK-UP
If the cause for the uveitis is identified on clinical examination – a deep corneal ulcer or head trauma for example – then specific work-up for the uveitis is not always required. Unfortunately, the inciting agent is elusive in most cases and extensive investigation can be required to identify the underlying cause. If the cornea or anterior segment is too opaque to allow direct visualization, then ocular ultrasonography should be considered. In unilateral cases this could well outline a uveal tumour for example, or perhaps demonstrate a posterior scleral rupture following blunt trauma.
It is the bilateral cases that can be the most challenging to diagnose. Clearly a systemic problem is likely and routine blood screening with haematology and biochemistry profiles are a minimal baseline. These might highlight an infectious aetiology such that more specific diagnostic tests are indicated or suggest a blood dyscrasia or neoplastic process. Generalized septicaemia such as associated with pyometra can cause uveitis. Therefore, the basic screen might suggest that clotting profiles are indicated, or perhaps Toxoplasma, Ehrlichia, Leishmania or Borrelia titres. Mycotic causes for uveitis are rare in the UK but should be considered in immunocompromised patients or those that have travelled through endemic areas. Migrating parasite larvae, such as Toxocara canis, Angiostrongylus vasorum and, less commonly, Dirofilaria immitis, can all trigger an acute uveitis. Faecal examination can be diagnostic in such cases. Some possible causes of uveitis are listed in Table 33.2.
If the uveitis is severe but no cause can be identified, then referral for aqueocentesis or vitreocentesis can be considered while the eye(s) is/are still potentially sighted. By the time a secondary glaucoma has developed the prognosis for saving vision is very poor, and enucleation can be considered both on humane grounds but also as a diagnostic aid. Clearly this is a last resort!
Abdominal ultrasonography is sometimes useful as part of the uveitis work-up – especially if neoplasia is suspected. Most cases of bilateral uveitis which are associated with neoplasia are secondary – lymphoma, myeloma or mammary carcinoma for example.
If all diagnostic tests are negative, then one assumes a diagnosis of idiopathic or immune-mediated uveitis. Symptomatic treatment is started, but further tests might be warranted if the patient does not respond as expected or develops other clinical signs.
Most cases of acute uveitis are painful and so appropriate analgesia should be considered. Nurses will be well placed to evaluate the degree of discomfort. Attempts at rubbing the eye(s) should be discouraged. The treatment for uveitis usually involves both topical and systemic medication which nurses can administer, as well as ensuring that owners are competent to continue the treatment regimen at home. Some patients with uveitis might be contagious – canine adenovirus for example. The risks of zoonotic infections such as Leishmania should not be overlooked and appropriate barrier nursing undertaken.
EPIDEMIOLOGY
Many cases of uveitis occur on an individual basis, but occasional outbreaks of infectious disease in which uveitis is part of the clinical picture do occur in dogs. Thus, unvaccinated patients could be seen with canine adenovirus or leptospirosis, both of which can have ocular signs in addition to the systemic problems. Younger dogs are more likely to suffer from traumatic causes while neoplasia is clearly more frequent in older patients. There are some breed predispositions – for example, Japanese Akitas are predisposed to uveodermatological syndrome, an immune-mediated disease where ocular and dermatological melanocytes are targeted and destroyed with severe localized inflammation.
Whatever the cause, be it exogenous or endogenous, the ocular inflammation develops following breakdown of the blood–ocular barrier. Chemical mediators (such as prostaglandins) result in a leaky barrier, often within the iris endothelium (but also in the choriocapillaris in cases of posterior uveitis), and both proteins and cells (red and/or white blood cells) pass between the gaps into the anterior chamber. Aqueous flare, hypopyon, hyphaema and keratic precipitates are all visible results of the breakdown of the blood–ocular barrier. Miosis occurs via a prostaglandin-mediated iris sphincter muscle spasm and this is particularly painful. The lowered IOP mentioned above results from reduced aqueous production.
If the inflammatory response is mild and localized, healing will occur with minimal scarring. However, small lesions in the eye can result in severe impairment of function – unlike in many other body organs where scarring can be incidental. Thus profound and uncontrolled inflammation can have catastrophic effects on vision. Chronic and recurrent uveitis occur frequently following acute episodes, although the detailed immunological actions resulting in this are complicated and poorly understood (and their discussion is beyond the scope of this text). However, the uveal tract does act rather like an accessory lymph node which is certainly important in recurrent immunological responses.
TREATMENT OPTIONS – MEDICAL
Uveitis is usually treated medically. Prompt therapy is required to prevent the potentially devastating sequelae of uveitis which are discussed in the section on prognosis. A combination of therapies, both topical and systemic, is normally required and treatment will be divided into specific elimination of the inciting cause, if known, together with symptomatic therapy. Clearly the specific therapy can be variable – particular antibiotics such as clindamycin for toxoplasmosis, or tetracyclines for ehrlichiosis. Otherwise a broad spectrum agent with good ocular absorption such as cefalexin can be chosen. Other specific treatment could be anthelmintics if migrating parasite larvae are identified or antifungal drugs in the rare cases of systemic fungal disease. It is sensible to use systemic antibiotics if the cause is uncertain but systemic steroids are required – the immunosuppression could allow an unidentified bacterial infection to proliferate and cause severe generalized septicaemia.
In severe cases of uveitis, systemic steroids, usually prednisolone at 1–2 mg/kg, will be required. Clearly the potential side effects of these high doses need to be considered, particularly if long-term medication is required – for immune-mediated causes for example. Some patients might even require systemic immuno-suppressant drugs such as azathioprine or ciclosporin. Careful management in liaison with both ophthalmologists and internal medicine or oncology practitioners is sensible in such cases. If systemic steroids are contraindicated (e.g. in patients with diabetes mellitus), then systemic NSAIDs should be used instead, but they are not usually as effective at reducing the inflammation.
Thankfully many cases of uveitis are not so severe and do not require systemic medication, apart perhaps from a few days of systemic NSAIDs for pain relief. Topical therapy is centred on the use of anti-inflammatory agents and usually atropine. Topical antibiotics are not usually necessary unless an ulcer or intraocular infection is suspected. Topical steroids are preferred over topical NSAIDs although the latter might be indicated instead if ulceration is present, or as well as topical steroids in very severe cases. The choice of topical steroid is important – agents that are potent and have good intraocular penetration are required. Thus 1% prednisolone acetate and 0.1% dexamethasone are preferred over betamethasone sodium phosphate which has little intraocular activity. The frequency of application will clearly depend upon the severity of the uveitis, as will the duration of treatment. Mild cases might require just twice daily dosing for a week, while severe cases will require six to eight times daily initially, reducing as the condition improves, but many weeks of treatment are often required to prevent relapses. Clearly the underlying cause will affect the long-term outcome as well – immune-mediated causes will require life-long treatment. Occasionally subconjunctival steroids can be injected but they are not a substitute for topical therapy. Methylprednisolone acetate is the most commonly used – 4–10 mg in the bulbar conjunctiva.
Topical NSAIDs are used if corneal ulceration is present (and thus topical glucocorticoids are contraindicated) and in severe cases in conjunction with steroids where their combined effects are additive. The most frequently used topical agents are flurbiprofen and ketorolac trometamol, usually two to four times daily.
Topical atropine is an important agent to use in dogs with uveitis. This parasympatholytic drug is both mydriatic and cycloplegic. By dilating the pupil synechia formation should be reduced, and paralysing the ciliary body muscle relieves the pain associated with spasm of this muscle. There is also a non-specific stabilization of the blood–aqueous barrier. Care should be exercised if secondary glaucoma is a risk – in severe cases of uveitis where posterior synechiae are already present, and in breeds which suffer from primary goniodysgenesis such as springer spaniels and flat coated retrievers for example. Atropine will lower aqueous tear production so its use must be cautious in patients with low Schirmer tear test readings. These should be checked at each re-examination if borderline. Treatment is to effect, i.e. frequently enough to maintain a dilated pupil. This might be just once daily in mild cases, or three to four times in more severely affected animals. Atropine can last a long time in non-inflamed eyes. Therefore do not be surprised if the pupil is still slightly dilated a week after stopping treatment when the eye is quiet.
TREATMENT OPTIONS – SURGICAL
Surgery is only required in a very few specific cases of uveitis. Clearly, if a pyometra is present, an ovariohysterectomy is required along with systemic antibiotics, topical corticosteroids and atropine. If an aberrant parasite larva is present in the anterior chamber this might need surgical removal prior to treating with anthelmintics – the dead larva can cause a very severe inflammatory reaction with disastrous consequences for the eye and so removing it while still alive and following this with appropriate treatment is usually advised. Referral should be considered in such cases.
Most cases of uveitis which are secondary to intraocular neoplasia are not amenable to surgery but a few can be – these are discussed in the section on intraocular neoplasia. If the uveitis has resulted in secondary glaucoma, then enucleation might be advised. Clearly histopathology is important in such cases.
PROGNOSIS
As with the causes and treatment regimens for uveitis in dogs, the prognosis is also extremely variable. A simple case which is secondary to corneal damage – ulcer or foreign body – will resolve fully with no scarring, no relapse and normal vision. At the other end of the spectrum, a panuveitis with retinal detachment due to multiple myeloma will not just be blinding, but life threatening. The chronic sequelae of uveitis include posterior synechia, cataract formation, secondary glaucoma and phthisis bulbi, all of which can be blinding and some of which can require enucleation. Long-term treatment is frequently required in immune-mediated cases – chronic usage of topical steroids can predispose to corneal ulceration and owners must be made aware of this and asked to stop the drops should any signs of ulceration – a wet, painful eye for example – develop. Systemic steroids should be reduced to the lowest possible dosage regime.
The dog was presented as an emergency. She had been completely fine the previous day, but on waking she appeared blind, both eyes were very cloudy and she held them closed and tried to shy away from the owner. She did not eat her breakfast. No previous ocular or systemic problems were reported. She had not travelled abroad and had completed her full vaccinations 3½ months previously.
CLINICAL SIGNS
Both eyes were similarly affected. Vision was absent but dazzle responses were present. Severe corneal oedema was present bilaterally, along with marked episcleral congestion and miosis (Figure 33.3). No corneal ulceration was present. Intraocular pressures were 6 mmHg bilaterally. Fundus examination was not possible. The dog was clinically depressed and pyrexic (39.5°C) although no other systemic abnormalities were detected.
WORK-UP
Blood was taken for routine haematology and biochemistry but surprisingly no abnormalities were detected. Ocular ultrasonography showed debris in the anterior chamber, no lens abnormalities and no evidence of vitreal disease or retinal detachment. It was decided to treat the dog symptomatically initially and, depending on her response to treatment, to consider further laboratory investigation.
TREATMENT
The dog was started on prednisolone acetate drops hourly for 6 hours then every 2 hours plus atropine drops hourly for three doses then three times daily. Carprofen was given by injection together with intravenous cefalexin (although the bloods did not show any evidence of bacterial infection it was possible that the anterior chambers were infected and it was considered that the antibiotic would do no harm!).
OUTCOME
Twenty-four hours later the dog was dramatically improved. Vision was good from both eyes, the corneal oedema was clearing and the pupils were well dilated. Intraocular pressures were 12 mmHg in the right eye and 14 mmHg in the left. Fundus examination by indirect ophthalmoscopy revealed no problems. Rectal temperature was back to normal and the dog was bright and eating. The dog was sent home on six times daily prednisolone acetate, twice daily atropine drops and oral cefalexin and carprofen at standard doses. Five days later, only minimal conjunctival hyperaemia remained and treatment was reduced to Pred Forte only, four times daily. This was continued for 2 weeks then reduced to twice daily for another week before stopping. No relapses occurred and the dog did not develop any other symptoms whatsoever.
This is a slightly unusual case in that the eyes were very severely inflamed yet no abnormality was present on initial blood screening and she made a dramatic recovery such that further investigation was not justified. Bilateral trauma is unlikely to cause such symmetrical changes. The pyrexia could have been pain related, but a viral aetiology was also possible.
The dog presented with painful, cloudy eyes. The owner had noticed that they had been a bit red for a few days prior to suddenly deteriorating. Vision was reportedly OK but the dog was lethargic with a reduced appetite. No previous ocular or systemic problems were reported. She was fully vaccinated and had not travelled outside the UK.
CLINICAL SIGNS
Ophthalmic examination was bilaterally similar. Menace responses were present. Pupils were slightly miotic and slow to constrict further on stimulation with bright light. Some episcleral congestion was noted together with slight corneal oedema. No corneal ulceration was present. The eyes were very hazy in appearance due to marked aqueous flare which had a slightly reddish tinge. Fundus examination was not possible – some vitreal haze was also present. Intraocular pressures were 10 mmHg bilaterally. General clinical examination revealed that the dog was depressed but in good condition. Several petechial haemorrhages were noted along the gum margins and some bruising was present on the ventral abdomen. There was no history of recent treatment with any systemic medication.
WORK-UP
A systemic problem was suspected. Blood was taken for haematology, biochemistry and clotting profiles. These showed a severe thrombocytopenia with 8000 platelets/μl and a moderate regenerative anaemia. Prothrombin time and activated partial thromboplastin times were normal. Biochemistry was unremarkable. Urinalysis showed mild proteinuria but no haematuria. An anti-platelet antibody test was performed and was positive and so bone marrow aspirates for direct immunofluorescence tests were not considered necessary. Survey chest and abdominal radiography was unremarkable with no evidence of neoplasia. The diagnosis was immune-mediated thrombocytopaenia.
TREATMENT
Topical treatment was started with prednisolone acetate drops six times daily and atropine drops three times daily initially. Oral prednisolone at 2 mg/kg was started.
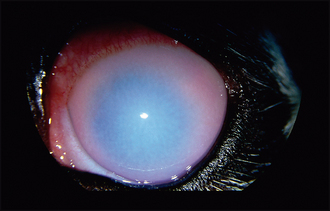
OUTCOME
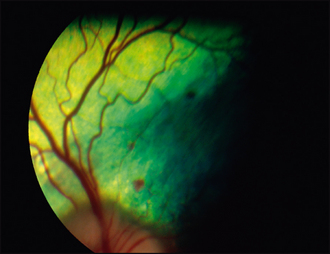
A week later the eyes were improving well. The hyph-aema had cleared well although a small area of vitreal haemorrhage was noted (Figure 33.4). Fundus examination revealed several pinpoint retinal haemorrhages (Figure 33.5). Clinically the dog remained lethargic and was polydipsic, polyuric and polyphagic from the steroids. Topical treatment was reduced to twice daily prednisolone acetate for a month and once daily atropine for a week. The systemic steroids were reduced to 1 mg/kg/day. Her platelet count at this stage had increased to 15 000/μl. The eyes fully resolved, although the retinal haemorrhages took several weeks to reduce.
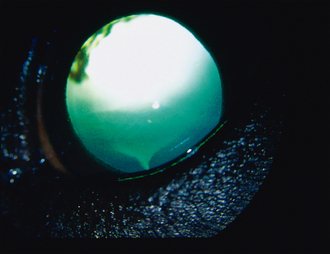
Figure 33.4 One week after starting treatment. The pupil is dilated from atropine use. Note the area of haemorrhage from 9–11 o’clock. This is in the anterior vitreous and will have come from the ciliary body.
The dog’s general health improved slightly but then she became acutely lame on her right hind, with a painful swollen hock joint. A spontaneous haemorrhage was suspected. This resolved, and 2 months later the dog was bright and comfortable with no ocular changes (apart from the resolving retinal haemorrhages). Platelet counts returned to the normal range. She was maintained on oral prednisolone 0.5 mg/kg/48 hours for a further 2 months.
This case illustrates that what might appear to be a purely ocular problem should always be fully investigated since a serous systemic aetiology might be present.