Chapter 9 Therapeutic Use of Self
a model of the intentional relationship
Introduction
A recent survey of practising occupational therapists within the United States revealed that more than 80% of therapists consider therapeutic use of self to be the most important variable in successful therapy outcomes (Taylor et al in press). In a similar study in the UK 83% of respondents placed a significant amount of importance upon therapeutic use of self and 72% felt it is a key determinant of therapy (Forsyth et al submitted). At the same time, fewer than half of US therapists and just half of UK therapists felt they were adequately trained in this area upon graduation. Additionally, about two-thirds of both cohorts of therapists felt that there was sufficient knowledge about use of self in occupational therapy (Forsyth et al submitted, Taylor et al in press).
These therapists’ perceptions of the importance of therapeutic use of self are supported by other research studies; a growing number of which indicate that the client–therapist relationship is a key determinant of whether occupational therapy has been successful or not (Ayres-Rosa and Hasselkus 1996, Cole and McLean 2003). In this chapter, we provide an overview of the historical foundations and literature on use of self within the field of occupational therapy. This is followed by a rationale for the introduction of a new conceptual model of use of self and an explanation of the research that has been conducted thus far to support the development of this model. The model and its four components and functions are then described. Ultimately, a case example is presented that illustrates a clinician’s use of this model in a practice situation.
Historical overview
The topic of therapeutic use of self has been addressed throughout occupational therapy’s history. Recommendations about how therapists should interact with clients have changed as our thinking about practice has evolved over time. An historical account has identified three distinct eras in occupational therapy (Kielhofner 2004). Each of these eras offers a unique perspective and emphasis on the role of the client–therapist relationship in the therapy process.
The earliest occupational era reflected ideals embraced by the field’s founders (Kielhofner 2004). Initial descriptions of therapeutic use of self came from Europe in the late 1700s during the time of moral treatment (Bockoven 1971, Bing 1981). Moral treatment emphasised the facilitation of self-determination through engagement in everyday activities such as arts and crafts, sports and other pursuits. When more formalised approaches to occupational therapy emerged in the early 1900s, the humanistic approaches of moral treatment were emphasised. Supporters of moral treatment argued that all activity prescriptions should be based on an in-depth understanding of the patient’s personality, preferences and interests (Bing 1981). Consideration and kindness were put forward as essential interpersonal values. During this era, the therapeutic relationship was viewed as existing solely as a means for encouraging the client to engage in occupation. In creating this relationship, the therapist’s role was to serve as an:
In the mid-20th century, the early occupational era was replaced by a more analytical era labelled the era of inner mechanisms (Kielhofner 2004). In this era, concern for addressing a client’s underlying impairment became the focus. Rooted in the medical establishment, the role of the occupational therapist during this era was to understand the nuances of and correct internal failures of body and mind. The client–therapist relationship was viewed as the central mechanism for change and understanding of this relationship was largely based on principles borrowed from literature influenced by the psychoanalytic perspective. Often, the relationship was viewed as a means by which to understand a client’s unconscious motives, desires and behaviour toward others and toward occupations. Within the relationship, the therapist’s role was to:
Within mental health settings, which then comprised a significant amount of occupational therapy practice, it was common to expect that the client would achieve catharsis by acting out unconscious motives and desires within the therapeutic relationship. The therapist then assisted the client in achieving insight into any issues that were viewed to be at the core of the client’s pathological feelings and behaviours. By the 1970s, some believed that occupation had lost its place as the key dynamic of therapy (Yerxa 1967, Shannon 1977, Schwartz 2003, Kielhofner 2007).
In the latter part of the 20th century a new, contemporary era was born, which returned the field to its initial focus on occupation. This era was labelled the return to occupation (Kielhofner 2004). In part, this new era represented a reaction to what was perceived as an over-emphasis on the role of the therapeutic relationship during the era of inner mechanisms. In this contemporary era, the strong focus on the therapeutic relationship has been set aside in favour of a renewed emphasis on occupational engagement as the true mechanism for change and positive outcomes in occupational therapy (Yerxa 1967, Kielhofner and Burke 1977, Shannon 1977, Schwartz 2003). Similar to the early occupational era, the role of the relationship in the contemporary era is more uni-dimensional in its focus, which is strictly to facilitate the client’s engagement in occupation. The therapist’s role is to use a variety of interpersonal strategies to make occupations appealing.
Within this contemporary era, there have been three central movements with which the client–therapist relationship has been associated:
Collaborative and client-centred approaches (e.g. Mosey 1970, Townsend 2003, Duncan 2006) have focused on re-adjusting power imbalances within the therapeutic relationship and on facilitating client control over decision-making and problem-solving. Generally, these approaches emphasise open communication, orientation toward the client’s perspective, recognition of the client’s strengths, shared goals and priorities, and a collaborative partnership. There has also been an emphasis on therapist self-awareness. Therapists are encouraged to recognise, control and correct non-therapeutic reactions, incorporate their own life experiences into an understanding of their client’s perspectives, and to draw upon their personal reactions to clients to guide their clinical reasoning.
In conjunction with collaborative and client-centred approaches, the contemporary era has also been characterised by an emphasis on empathy and caring within the therapeutic relationship. This can be summarised as an emphasis on the emotional exchange that occurs between client and therapist, on goal-directed activity, and on activities that promote personal growth (Baum 1980, Gilfoyle 1980, King 1980, Yerxa 1980, Devereaux 1984, Peloquin (1989a, 1989b, 1990, 1993, 1995, 2002, 2003). Caring was put forth as a much-needed value and it was defined as follows (Baum 1980, Gilfoyle 1980, King 1980, Yerxa 1980, Devereaux 1984):
More recently, empathy has been written about extensively and defined as a communication of partnership:
Peloquin (1989b, 1990, 1993) emphasised the roles of art, literature, imagination and self-reflection. She further argued that the fundamental characteristics required to develop one’s therapeutic use of self are well conveyed through reading literature and viewing and doing art (Peloquin 1989b). She believed that providing therapists with both fictional and non-fictional poems and stories that illustrate empathy and the depersonalising consequences of neglectful attitudes and failed communication could be a powerful motivator for the development of caring (Peloquin 1990, 1993, 1995).
Clinical reasoning and narrative approaches comprise the final general category of contemporary scholarship that includes the client–therapist relationship as a focal point (Rogers 1983, Crepeau 1991, Mattingly 1991, 1994, Clark 1993, Schell and Cervero 1993, Fleming 1994, Mattingly and Fleming 1994, Kielhofner 1997, Jonsson et al 2001, Lyons and Crepeau 2001, Schwartzberg 2002, Schell 2003, Schwartz 2003). These approaches emphasise the role of therapist understanding and reflection about the unique way in which clients think about and summarise key events in their lives (Kielhofner 2004). Clinical reasoning approaches incorporate thinking about the relationship as a component of one’s overall approach to making sense of assessment findings and developing a treatment plan (Mattingly and Fleming 1994). This element has been referred to as interactive reasoning (Mattingly and Fleming 1994) and it has been described as an ‘underground practice’ in occupational therapy (Fleming 1991) because relatively little is known about the mechanisms that underlie it. One exception involves work by Mattingly and Gillette (1991), which resulted in six relationship-building strategies pertinent to clinical reasoning. These included:
Narrative approaches (e.g., narrative reasoning) were developed in tandem with clinical reasoning approaches (Mattingly 1994, Kielhofner 1997). Narrative approaches seek to organise and make sense of information from clients by encouraging them to present information about themselves through storytelling, poetry or metaphor. Thinking in story form is thought to allow both the client and the therapist to discover the meaning of the impairment experience according to the client’s unique perspective. Therapeutic approaches are then focused toward reconstructing more hopeful narratives to re-shape one’s life story.
Rationale for a model of use of self
We have seen that occupational therapy’s view of the therapeutic relationship has changed and developed throughout history. Early perspectives of the field’s first era emphasised the centrality of occupation and the therapist’s role in promoting occupational engagement. The second era redefined the therapeutic relationship as a psychodynamic process that, according to some perspectives, replaced occupation as the central dynamic of therapy. With some exception (e.g., Blair and Daniels 2006) this idea was, in large part, rejected in favour of the contemporary, renewed focus on occupation.
During our contemporary era of heightened occupational focus, the three major themes related to the therapeutic relationship described in the prior section have been introduced: (1) collaborative and client-centred approaches; (2) an emphasis on caring and empathy; and (3) clinical reasoning and use of narrative. These are important themes that offer broad and useful principles related to the therapeutic use of self.
Despite the fact that these approaches coexist with the field’s returned emphasis on occupational engagement, they do not directly address the question of how therapeutic use of self can be used specifically to promote both occupational engagement and positive therapy outcomes. Their relationship to an occupationally focused practice is assumed, but not made explicit.
In addition, some implicitly assume that, when therapists achieve a reflective, appreciative, and emotionally connected state with clients, a positive therapeutic process will simply emerge. This assumption is a large one that appears to be contradicted in the experience of most practising therapists. Despite the existence of a fairly extensive contemporary literature on collaboration, client-centred practice, caring, empathy, clinical reasoning and narrative, the vast majority of practising therapists that we surveyed, believe occupational therapy does not have sufficient knowledge to support the therapeutic use of self (Forsyth et al submitted, Taylor et al in press). Their perspectives suggest that something is still missing.
To date, there has been no effort to integrate all of the contemporary interpersonal approaches in occupational therapy into a coherent explanation of the therapeutic relationship. Moreover, beyond broad principles, there are few details about how the therapeutic relationship should be approached and managed in light of the central focus on the client’s engagement in occupation. Consequently, there is still a lack of clarity regarding the exact definition, use and relevance of therapeutic use of self in occupational therapy.
These observations were the impetus for developing the conceptual practice model presented in this chapter, the Intentional Relationship Model. The model was developed in an attempt to clarify and provide more detailed guidance of how to enact the therapeutic use of self in occupational therapy. Therapeutic use of self involves a highly personal, individualised and subjective decision-making process. For some therapists, the process is driven by emotional reactions to clients and a perceived reliance on an innate or nurtured intuitive capacity. Others perceive the process as largely rational and grounded in the disciplined application of a set of interpersonal guidelines. Irrespective of such viewpoints, therapeutic use of self is, in large part, a product of the extent to which one possesses a knowledge base and interpersonal skills that can be applied thoughtfully to common interpersonal events in practice. Accordingly, therapeutic use of self is an occupational therapy skill that must be developed, reinforced, monitored and refined.
The Intentional Relationship Model explains therapeutic use of self and its relationship with occupational engagement. Additionally, it provides a means of mapping, interpreting and responding to the unique and everyday interpersonal events of therapy by incorporating a variety of perspectives, skills and approaches. The model provides educators, supervisors, students, clinicians with a common vocabulary with which to discuss and describe the interpersonal phenomena that have an ongoing impact on everyday practice.
The Intentional Relationship Model
The Intentional Relationship Model is an empirically based model that was developed over a 3-year period. In part, its concepts were based on practitioner responses to a large-scale (n = 1000, response rate 64%) nationwide survey of occupational therapists’ knowledge, attitudes and interpersonal behaviours related to use of self (Taylor et al in press). In addition, 12 occupational therapy practitioners from various regions of the world were observed and interviewed using a semi-structured interview measure developed by the first author. In each region, these therapists were nominated by their local peers as having exceptional talent in terms of their ability to form successful therapeutic relationships with a wide range of clients. They also participated in an initial introductory interview with the first author to determine their suitability for participation in the formal interview and observation. The insights that emerged from the observation of these expert therapists were critical to the development of this model. The second author is one of the therapists who was selected and studied for her expertise and her approach to the therapeutic use of self will be used later in this chapter to illustrate some aspects of this model.
Many of the concepts for the intentional relationship model have their origins in theory underlying psychotherapy practice models. However, the intentional relationship model recognises a fundamental difference between occupational therapy and traditional psychotherapy. Figure 9.1 portrays the traditional psychotherapy process. In psychotherapy, interpersonal relating between client and therapist is the central focus. The verbal communication between client and therapist is lengthy, intense, highly complex, nuanced and derived from detailed conceptual models of how psychological change is intended to occur. Interpersonal communication is typically the only activity that occurs during psychotherapy.

In occupational therapy the client–therapist relationship does not and should not pretend to emulate the intensity, duration and complexity of a traditional psychotherapy relationship.
By contrast, the central focus of occupational therapy is occupational engagement. A diagram of the unique role that the therapeutic relationship plays in occupational therapy is presented in Figure 9.2.
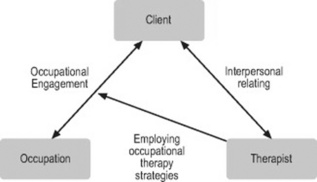
Figure 9.2 The unique relationship between client, therapist and occupation in occupational therapy (fix arrows)
As it shows the occupational therapist employs a number of therapeutic strategies, usually rooted in existing models of practice, to facilitate the client’s engagement in occupation. Depending on the occupational needs, capacities and diagnosis of the client, any number of occupational therapy practice models might be employed alone or in combination to promote occupational engagement. However this main task of promoting occupational engagement through employing the specific methods and strategies of occupational therapy does not exist in isolation of a larger process of relating that occurs between client and therapist.
The intentional relationship model explains the relationship between client and therapist that is part of the overall process of occupational therapy. Accordingly, the intentional relationship model is intended to complement existing occupational therapy conceptual practice models rather than replace any single model. It explains the detailed and overarching aspects of the client–therapist relationship, an important aspect of occupational therapy not addressed extensively by other conceptual practice models. Figure 9.3 shows how the intentional relationship is designed to supplement the use of other occupational therapy conceptual practice models.
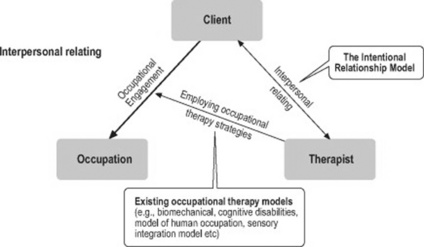
Figure 9.3 The intentional relationship model as a complement to existing occupational therapy models
As shown, the intentional relationship model should complement the usual concepts and strategies of occupational therapy that are directly aimed at facilitating occupational engagement. The model’s utility for occupational therapy lies in addressing the otherwise unarticulated aspects of the interpersonal relationship that occur during the therapy process and that influences both occupational engagement and therapy outcomes. The next section defines the elements of this model and provides an explanation of how the elements interact to optimise the circumstances for a successful client–therapist relationship in occupational therapy.
To reiterate, the intentional relationship model is not a free-standing model of practice for occupational therapy. If a therapist only utilised this model, the essential work of occupational therapy would not occur. The model was designed to fill a gap in our practical knowledge about how to manage the interpersonal aspects of therapy – particularly the more challenging ones. This model should complement the field’s existing methods and models by making the process of establishing a successful relationship with clients easier, clearer and more straightforward.
Elements of the Intentional Relationship Model
This chapter provides only a basic overview of the Intentional Relationship Model (IRM). Those who are interested in a more thorough treatment should consult The Intentional Relationship: Therapeutic Use of Self in Occupational therapy (Taylor 2008). The IRM views the therapeutic relationship as being comprised of four central elements:
A summary diagram of the model is presented in Figure 9.4.
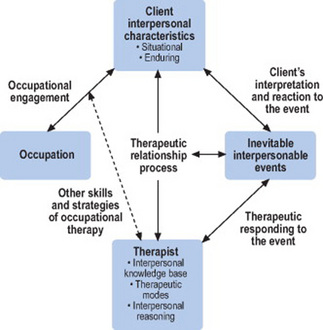
The model explains the requirements for a functional client–therapist relationship and it incorporates guidelines for responding to common interpersonal events that frequently occur in therapy. In the following section, the relevant aspects of each element of the model and their relationships with one another are described.
The client
According to the IRM, the client is the focal point. It is the therapist’s responsibility to work to develop a positive relationship with the client and to respond appropriately when interpersonal events occur. In order to develop this relationship and respond appropriately to the client, a therapist must work to understand the client from an interpersonal perspective. This involves getting to know the client’s interpersonal characteristics. According to IRM, a client’s interpersonal characteristics can be understood according to two dimensions:
Situational characteristics are interpersonal characteristics that are inconsistent with how a client typically and consistently behaves when interacting with others. Instead, they reflect a client’s acute emotional reaction to a specific situation. Typically, a client’s situational characteristics attract our attention when he or she is encountering a situation that is somehow painful, frustrating or stressful. For most of us, stressful situations result in some negative emotional state that makes it temporarily difficult for us to engage in occupations as planned. Thus, a client’s situational characteristics are likely to surface when they interfere with the client’s ability to engage in the activities of therapy as planned.
A client’s situational characteristics are most likely to reveal themselves in therapy when the client is facing a situation where some immediate aspect of the impairment and/or the environment is experienced as stressful. Impairments, particularly when they are new or when there is a medical crisis or exacerbation in severity that disrupts one’s usual relationship with the environment, often cause people to experience stress. Therapists are encouraged to assume, on some level, that a client’s impairment situation and/or the client’s interaction with an unaccommodating or difficult environment will cause the client to be more vulnerable to experiencing a variety of emotional reactions, many of which may be perceived as negative or at least atypical for that individual. For example, feelings of loss are common among newly disabled individuals and they may manifest in terms of sadness, irritability, anxiety, insecurity or anger. A therapist’s interpersonal behaviour, if perceived as insensitive, judgemental or uncaring, may also serve as a source of stress and cause the client to interact in a manner that is generally inconsistent with his or her personality. It is important for newer therapists to recognise that these and other acute emotional reactions are normative. In fact they are givens in many health-care situations. They bear no reflection on the client’s character or personality. However, they do have the potential to play out within the therapy relationship, and the way in which a therapist chooses to respond to them is often vital to the future of that relationship.
By contrast, enduring characteristics are more stable and consistent aspects of the client’s interpersonal behaviour. They are not necessarily related to the situation of acquiring an impairment or to the environment’s reaction or lack of accommodation to that impairment. Instead, they comprise an interpersonal profile that is idiosyncratic to the client. Enduring interpersonal characteristics include such things as a client’s preferred style of communicating, capacity for trust, need for control, general orientation to relating and usual way of responding to change, challenge or frustration.
Because they coexist in each client, situational and enduring characteristics are mutually informative. Behaviour that reflects one’s acute emotional reaction to a stressful event may temporarily attenuate, alter or intensify one’s interpersonal behaviour in what are usually more stable categories. For example, a client that normally responds to a challenging situation adaptively may become irritated when the therapist recommends a more challenging activity if, earlier in that day, the client underwent a painful biopsy and then discovered that she did not have the funds to pay for transportation after leaving the physician’s office. The rationale for distinguishing the two categories of interpersonal characteristics is to help inform therapists’ understanding of the client in stressful and non-stressful situations so that therapeutic responses can be appropriately tailored and modulated.
The interpersonal events of therapy
An interpersonal event is a naturally occurring communication, reaction, process, task or general circumstance that occurs during therapy and that has the potential to detract from or strengthen the therapeutic relationship. In therapy, these events may be precipitated by the following kinds of circumstances:
These, of course, are only a few of the myriad of possible interpersonal events that occur in the course of occupational therapy.
When interpersonal events of therapy occur, their interpretation by the client is a product of the client’s unique set of interpersonal characteristics. Sometimes the event may have a significant effect upon the client and other times a client will be unaffected or minimally affected. When such events occur, what is important is that the therapist be aware that the event has occurred and take responsibility for responding appropriately.
Interpersonal events are part of the constant give and take that occurs in a therapy process. They are distinguished from other events or processes in that they are charged with the potential for an emotional response either when they occur or later upon reflection. Consequently, if they are ignored or responded to less than optimally, these events can threaten both the therapeutic relationship and the client’s occupational engagement. When optimally responded to, these events can provide opportunities for positive client learning or change and for solidifying the therapeutic relationship. Because they are unavoidable in any therapeutic interaction, one of the primary tasks of a therapist practising according to the IRM is to respond to these inevitable events in a way that leads to repair and strengthening of the therapeutic relationship.
The therapist
Within the IRM, the therapist is responsible for making every reasonable effort to make the relationship work. Specifically, the therapist is responsible for bringing three main interpersonal capacities into the relationship:
This section provides a brief description of each of these interpersonal capacities. The first capacity involves development and application of a wide-ranging fount of knowledge about how to manage the various aspects of one’s relationships with other people. The therapist’s interpersonal skill base is comprised of a continuum of skills that are judiciously applied by the therapist to build a functional working relationship with the client. The perspective of the model is that, depending on the unique experiences, knowledge and innate capacities of the therapist, some of these skills will come more naturally while others will require significant effort and practice to develop.
These interpersonal skills are summarised in terms of nine categories:
The first category, therapeutic communication, involves activities such as verbal and nonverbal communication skills, therapeutic listening, assertiveness, providing clients with direction and feedback, and seeking and responding to client feedback. Interviewing skills is another skill set that involves being watchful and intentional about the way in which one approaches the process of asking a client questions. Socratic questioning is a specific approach to questioning born out of cognitive psychology (e.g., Beck 1995). It involves asking questions in a way that guides the respondent to think more broadly or differently. Establishing relationships with clients includes rapport building, matching one’s therapeutic style to the interpersonal demands of the client, managing a client’s strong emotion, judicious use of touch, and cultural competence.
Because many clients have caregivers, family members or other individuals with whom they have regular contact, understanding and working with families, social systems and groups is an essential aspect of occupational therapy practice. It includes using guiding principles of IRM, in combination with prominent systems theories, to gain the collaboration of partners, parents, other family and friends to serve the goals of therapy. It also involves understanding the structure, process and interpersonal dynamics of group therapy.
Another fundamental skill involves knowing how to work collaboratively with supervisors, employers and other professionals. It involves knowing how to communicate with other professionals about clients both in the presence and in the absence of those clients. Additionally, it requires understanding the power dynamics and value systems that underlie supervisor/student and employer/employee relationships. Understanding and managing clients’ difficult behaviour is another category of necessary interpersonal skills required in many practice situations. It involves knowing how to respond effectively to behaviours that involve manipulation, excessive dependency, symptom focusing, resistance, emotional disengagement, denial, difficulty with rapport and trust, and hostility. Responding effectively will help limit the extent to which this behaviour disrupts the goal and process of therapy.
Knowing how to resolve conflicts and empathic breaks (or rifts in understanding between client and therapist) is another fundamental skill set that can salvage a failing relationship or repair minor threats to an otherwise functional relationship. Professional behaviour and ethics encompasses knowledge of how one’s own values are consistent or inconsistent with the occupational therapy core values, ethical behaviour and decision making, behavioural self-awareness around clients, being reliable and dependable, upholding confidentiality, and setting and managing professional boundaries. Therapist self care incorporates knowing and managing one’s own emotional reactions to clients and being accountable to those reactions, a general capacity for self-reflection, an ability to manage one’s personal life and seek support when necessary, and the capacity to maintain perspective regarding client outcomes. More information about all of these skills, which comprise a therapist’s interpersonal skill base, is provided in Taylor (2008).
The second interpersonal capacity that a therapist brings to the client–therapist relationship is her or his primary therapeutic mode or modes. A therapeutic mode is a specific way of relating to a client. The IRM identifies six therapeutic modes:
A brief definition of each mode and an example of how the second author used the mode in practice is provided in Table 9.1.
Table 9.1 The six therapeutic modes in practice
| Mode | Definition | Example |
|---|---|---|
| Advocating | Ensuring that the client’s rights are enforced and resources are secured. May require the therapist to serve as a mediator, facilitator, negotiator, enforcer, or other type of advocate with external persons and agencies | Lobbying to secure adequate resources for the provision of ongoing support and environmental adaptation. This enabled a man with learning disabilities to participate safely in self care and domestic activities within his own home environment |
| Collaborating | Expecting the client to be an active and equal participant in therapy. Ensuring choice, freedom, and autonomy to the greatest extent possible | Setting recovery oriented occupational goals with a man who had been through an inpatient detoxification program for alcohol misuse. The service user reported that the structured routine for healthy activity choices coupled with feedback to the therapist helped to build him a sense of personal responsibility for achieving the goals |
| Empathising | Ongoing striving to understand the client’s thoughts, feelings, and behaviours while suspending any judgement. Ensuring that the client verifies and experiences the therapist’s understanding as truthful and validating | Taking care to fully appreciate the occupational requests and sensitivities of a woman experiencing psychotic symptoms. This approach enabled her to reclaim her values of being a vegan and being very environmentally conscious throughout her therapeutic recovery experience |
| Encouraging | Seizing the opportunity to instill hope in a client. Celebrating a client’s thinking or behaviour through positive reinforcement. Conveying an attitude of joyfulness, playfulness and confidence | Spontaneously responding to a woman attending an occupational therapy group session who, inspired by some background music started to dance. Therapeutic connection was enhanced by this small gesture to join with her joy of the activity |
| Instructing | Carefully structuring therapy activities and being explicit with clients about the plan, sequence, and events of therapy. Providing clear instruction and feedback about performance. Setting limits on a client’s requests or behaviour | Enabling a withdrawn woman with little belief in her own abilities to undertake self care activities. This was achieved by talking the woman through the task, all the while reinforcing verbally the support available with the task if required |
| Problem-solving | Facilitating pragmatic thinking and solving dilemmas by outlining choices, posing strategic questions, and providing opportunities for comparative or analytical thinking | Allowing a young man with Aspergers syndrome to undertake the activities of value to him that also supported his well-being. This involved analysing options and negotiating with his family, who were concerned about his extraordinary choices of some occupations and his neglect of others |
Therapists naturally use therapeutic modes that are consistent with their fundamental personality characteristics. For example, a therapist who tends to be more of a listener than a talker and believes in the importance of understanding another person’s perspective before making a suggestion would likely use empathising as a primary therapeutic mode in therapy. Therapists vary widely in terms of the range and flexibility with which they use modes in relating to clients. Some therapists relate to clients in one or two primary ways, while others draw upon multiple therapeutic modes depending upon the interpersonal characteristics of the client and the situation, or inevitable interpersonal events, at hand. One of the goals in using the intentional relationship model is to become increasingly comfortable utilising any of the six modes flexibly and interchangeably depending upon the client’s needs. A therapeutic mode or set of modes define the therapist’s general interpersonal style when interacting with a client. Therapists able to utilise all six of the modes flexibly and comfortably and to match those modes to the client and the situation are described as having a multi-modal interpersonal style.
According to the IRM, a therapist’s choice and application of a particular therapeutic mode or set of modes should depend largely on the enduring interpersonal characteristics of the client. In addition, certain events or interpersonal events in therapy may call for a mode shift. A mode shift is a conscious change in one’s way of relating to a client. Mode shifts are frequently required in response to interpersonal events in therapy. For example, if a client perceives a therapist’s attempts at problem-solving to be insensitive or off the mark, a therapist would be wise to switch from the problem-solving mode to an empathising mode so that she can get a better understanding of the client’s reaction and the root of the dilemma. An interpersonal reasoning process, described in the following paragraph, can be utilised to guide the therapist in deciding when a mode shift might be required and determining which alternative mode to select. Because the interpersonal aspects of occupational therapy practice are complex and require a therapist to possess a highly adaptive therapeutic personality, the IRM recommends that therapists learn to draw upon all six of the therapeutic modes in a flexible manner according to the different interpersonal needs of each client and the unique demands of each clinical situation.
The third therapist interpersonal competency involves the capacity to engage in an interpersonal reasoning process when an interpersonal dilemma presents itself in therapy. Interpersonal reasoning is a step-wise process by which a therapist decides what to say, do or express in reaction to the occurrence of an interpersonal dilemma in therapy. It includes developing a mental vigilance toward the interpersonal aspects of therapy in anticipation that a dilemma might occur, and a means of reviewing and evaluating options for responding. The six steps of interpersonal reasoning include:
An extensive description and discussion of these steps can be found in Taylor (2008).
The desired occupation
Occupational therapy is unique in that the crux of the therapy process is the client’s occupational engagement. The final component of the IRM is the desired occupation. The desired occupation is the task or activity that the therapist and the client have selected for therapy. These desired occupations may include a wide range of tasks and activities such as dressing oneself, driving, shopping, gross motor play, participating in a goal setting group, completing a craft activity or engaging in a simulated or modified work task. The selection of the occupation and support for occupational engagement will be primarily informed by other occupational therapy conceptual practice models such as the biomechanical model, the sensory integration model, or the model of human occupation (Kielhofner 2004)
The primary function of the IRM is to enable the therapist to manage the interpersonal dynamic between the client and the therapist that also occurs as part of the therapy process. This interpersonal dynamic influences the occupational engagement and also serves as an arena in which the emotional reactions that stem from or influence occupational engagement can be positively managed. Thus, according to the model the therapeutic relationship functions both as:
Relationships within the model
According to the IRM, the client and therapist relationship can be viewed at two different levels or scales:
The therapeutic relationship is a socially defined and personally interpreted interactive process between the client and therapist. It is socially defined in that the therapist and the client are engaged in an interaction within publicly understood roles. The therapist is recognised as bringing a certain kind of expertise, ethical guidelines and values into a relationship. The client is recognised as a person receiving service in order to address a particular need. The relationship is understood to exist for the sole purpose of achieving an improvement in the client’s situation. These parameters are given and provide an important definition of the relationship. Therapist and client are in a particular relationship that can be differentiated from other kinds of relationships such as friendships. At the same time, this relationship has a personal side. The client and therapist are human beings who encounter each other with the same potential range of thoughts and emotions that occur when any two people interact.
Consequently, the therapist’s responsibility is to ensure that:
Sustaining the therapeutic relationship is an ongoing task that does not focus solely on interpersonal events. The everyday therapeutic relationship process that occurs outside of any specific interpersonal events is the macro dimension of the interpersonal process of therapy.
Responding to the immediate events that occur during therapy is the micro dimension. Responding to these interpersonal events of therapy requires that therapists detect the occurrence of an event, read the client’s reaction to the event, and decide upon an appropriate way to address the event with the client.
Both the micro and macro scales of therapeutic interaction play a critical role in the overall process of occupational therapy. Moreover, they are interrelated. That is, the nature of the therapeutic relationship will have an influence on how the client interprets and how the therapist responds to interpersonal events and, in turn, interpersonal events and their resolution will either enhance or detract from the therapeutic relationship.
In some cases, the two scales of interaction are difficult to differentiate. For example, some therapy relationships only last for one or two sessions. In these cases, a therapist must work to respond to a client and to interpersonal events with much more vigilance and self-control because a more stable underlying therapeutic relationship does not yet exist. Moreover, the interpersonal events and their resolution during the therapy sessions will be the major determinants of the therapeutic relationship.
However, in most cases, therapy continues over a period of weeks or months, allowing for the development of some kind of predictable pattern or usual way of interacting within the therapeutic relationship. That therapeutic relationship will infuse and be shaped by interpersonal events that occur in the moment-by-moment therapy process. It will also be influenced by characteristics and behaviours that the client and therapist bring to the relationship, as well as by the circumstances surrounding the relationship. These circumstances include such factors as the nature and unfolding of the client’s impairment and the context (e.g., school, rehabilitation setting, home, work) in which therapy takes place.
It is the therapist’s responsibility to manage and continually strive to fortify the therapeutic relationship and to seek optimal resolutions to interpersonal events in therapy. The stability and success of a therapeutic relationship cannot be assumed. Rather, it begins early in treatment with attempts by the therapist to build rapport, followed by other efforts to develop a relationship that meets the client’s immediate interpersonal needs and is appropriate in terms of the circumstances of therapy and the demands of the treatment setting. Recognising and sustaining a successful therapeutic relationship might include such things as:
These are only a few examples of myriad factors that might contribute to a successful therapeutic relationship. It is the responsibility of the therapist to be vigilant to explore, identify and sustain those factors that contribute to a relationship that supports positive therapy outcomes.
This is not to say that the client will not make positive contributions to the therapeutic relationship. In most instances, clients will bring important or essential characteristics and behaviours into the therapeutic relationship. However, the fundamental difference is that it is the therapist who must assume the ultimate responsibility for assuring that the relationship is positive. By assuming this responsibility the therapist creates a space in the relationship wherein a client can be vulnerable, distressed, frustrated or angry without fearing that the relationship will be ruptured. Moreover, this does not mean that the therapist assumes an expert or authoritative stance in the relationship. Rather, it means that the therapist must assume responsibility for the caring within the relationship.
The enduring aspects of the therapeutic relationship are systematically built and fortified as a result of naturally occurring variables in relationship (similar personality styles or interpersonal chemistry or other optimal circumstances and timing) and as a result of the therapist’s consistent efforts to build the relationship in the face of the inevitable interpersonal events and challenges that occur. If the therapist’s efforts to build a relationship are successful and the client is not particularly sensitive, untrusting or otherwise vulnerable, the therapeutic relationship becomes stronger over time and is more likely to withstand interpersonal events that would otherwise challenge or strain the relationship.
For any number of reasons, however, the therapeutic relationship may not develop adequately enough to endure threats caused by the interpersonal events that routinely emerge during therapy. Signs that there is difficulty within the therapeutic relationship may include, but are not limited to:
There are a number of potential reasons why difficulty may emerge within the therapeutic relationship. For example, a client may bring a particular interpersonal history into the treatment relationship that makes it difficult for the therapist to establish rapport in ways that usually work. Conversely, the client may be mistrustful of the therapist because of the circumstances under which he is being seen. For example, a client may have been mandated by an insurance company to receive an evaluation for work potential and the client perceives that the therapist has tremendous power to influence his life (i.e., whether he continues to receive disability support). Alternatively, a therapist may have a negative reaction to a client because the client reminds the therapist of someone with whom the therapist has had a difficult relationship in the past. General sources of difficulty within the relationship may include, but are not limited to:
These and other kinds of obstacles to a more stable enduring relationship with a client are only intensified by inevitable interpersonal events. Examples of events that are likely to further stress an already-vulnerable therapy relationship include such things as a therapist’s unanticipated absence for a period of time, a common misunderstanding that occurs between client and therapist, a comment or question that is perceived by the client as insensitive or inappropriate, or an unexpected personal crisis that causes the client to regress or temporarily relinquish treatment goals. While these are normal and inevitable examples of difficult aspects of therapy, the way in which the therapist responds to them is a powerful mediator of the final outcome.
Irrespective of the extent to which the therapeutic relationship process is stable and strong, the process of therapeutic responding to interpersonal events is essential to good therapy. If a therapist does not respond adequately to interpersonal events or challenges to the relationship, the process of occupational engagement may suffer and the therapeutic relationship process will quickly erode.
Thus, for the duration of the therapy process, the therapist must engage in a process of interpersonal reasoning. Interpersonal reasoning is the process by which a therapist consciously and reflectively monitors both the therapeutic relationship and the interpersonal events of therapy in order to decide upon and enact appropriate interpersonal strategies. The six steps of this process were presented earlier in this chapter. A full description of the steps of interpersonal reasoning and examples of its application in practice are provided in Taylor (2008).
Case example
In the following section, a case example of how aspects of the IRM can be used in practice is provided by the second author, a practising occupational therapist for the Gloucestershire Partnership National Health Service Trust in Gloucestershire, England, United Kingdom. Jane has been practising for 20 years and her primary areas of expertise include inpatient and community interventions for adults with severe mental illness and for adults with learning disabilities. Jane also uses the model of human occupation (Kielhofner 2007) to underpin the formulation of her client’s abilities and challenges with regard to their engagement in occupations.
Jane’s interpersonal challenge: Resolving power struggles with Cecile
Cecile is a woman in her 40s who is divorced and lives alone. In the past, Cecile worked in a department store but was fired from her job, which she describes as one of many significant losses in her life. Cecile was referred for occupational therapy during a stay at an inpatient psychiatric unit. Her diagnosis has been difficult to determine, but Cecile has a long history of depression and anxiety with features of both borderline and narcissistic personality disorder.
Before she was referred to occupational therapy, Cecile had been using the psychiatric inpatient unit repeatedly during the previous 3 years. Cecile’s behaviour was also characterised by a tendency to lose favour with her health-care workers. She often made strong and repeated demands for support and assistance but then became dismissive of any attempts to meet these demands. At times she has been known to become rejecting or subtly hostile towards care workers. Her non-verbal messages matched her verbal communication conveying that she was defensive, hopeless or angry. She often twisted facts about her care and distorted or ignored attempts at support from family, friends and caregivers. Her communication was redundant with statements like, ‘I can not carry on like this’ or ‘You are not helping me’ or ‘This is not making me better’. In therapy, Cecile lacked curiosity and explored new environments only hesitantly. Though she was a highly capable person, she did not take pride in any current achievement nor seek out challenges. She was reluctant to show preferences, engage with others, complete activity, sustain focus or show that any activity was significant to her. This was particularly true when she was aware that staff were observing her, but were not prompting, instructing or encouraging her. Because of her attitude and behaviours, many health-care workers have become weary of providing support and some have refused to work with her.
The interpersonal response
Quickly I realized that issues of power were dominating our interactions and I began to specifically look for interpersonal events that presented power dilemmas. At once Cecile would say something that indicated a desire to change (e.g., ‘I want to be myself again’) and shortly thereafter she would tell me my approach was not working. Because this dynamic occurred repeatedly despite my many efforts to change my approach or incorporate her feedback, I interpreted this pattern’s true meaning as ‘I can say your intervention is not making me better and therefore I am powerful over you – even though I tell you that I want to change’. This played out in other ways. For example, we once shared a joke when visiting a local café and Cecile smiled. Because she rarely smiled, I pointed out that I enjoyed seeing her smile. She immediately returned to a mask-like expression. On another occasion I was gently questioning Cecile about her interests and achievements and she quickly became tearful and insisted we stop the conversation.
One of the central tasks of our work together involved understanding this power dynamic as an indication of Cecile’s high need for control, which is one of her more consistent and enduring interpersonal characteristics. Knowing this, I then had to work with this dynamic to maximise Cecile’s feelings of control so that she could develop other aspects of volition. On some occasions, this meant occasionally giving in to the dynamic and sometimes becoming vulnerable in her eyes. For example, I might use some self-disclosure about how her behaviour affects me. I did this with the hope of stimulating her self-reflection about our conversation and raising her awareness of how her use of power in this way affects other people.
On other occasions, I have worked with the power dynamic by standing my ground and providing a rationale for why my approach might assist her. I often validate Cecile’s desire for me to see that she is deeply troubled, but I also remind her that if and when she is ready to build strength I will be there to assist her. On some occasions, we have also agreed to take short, planned breaks from our work together. The reason for these breaks is to give her space from the therapy process, to allow her time to reflect upon the responsibility that she holds within the therapy relationship, and to enable me to reform with ideas and energy to maintain the relationship. Aside from working with the power dynamic in these ways, an overarching aspect of my approach has been to not take any of Cecile’s behaviours or comments personally.
The outcome
Cecile was discharged after an 8-month stay in the hospital. A structured and sophisticated support network was designed and implemented including regular occupational therapy appointments. Activities were set up and undertaken with the aim of engaging Cecile in making choices, taking control over her activities, regaining interest in past activities, and formulating a pattern within her occupations. Cecile’s motivation for doing did not develop any further than what she needed to maintain independent functioning. Importantly, however, it was maintained at the same level and now after many months since her last hospitalisation Cecile has not yet felt the need to return to the hospital.
Jane is a very circumspect therapist who has mastered the delicate art of walking on eggshells without breaking them. Her judgement about what people need, particularly when they are feeling vulnerable or threatened, is very precise and a quality that any therapist would admire. The story above illustrates that Jane’s level of sophistication in managing more difficult interpersonal issues within therapeutic relationships is highly developed. She utilised interpersonal reasoning to recognise inevitable power dilemmas within the relationship and she responded to them appropriately by shifting between the empathising and instructing modes to achieve a balance between acceptance-oriented strategies and change-oriented approaches. She was careful to select and time these modes carefully to accommodate Cecile’s high need for control within the relationship in a way that allowed her to feel more empowered without feeling the need to dominate or manipulate the relationship.
Summary
In occupational therapy, therapeutic use of self is a fundamental aspect of practice that has significant implications in terms of the course and ultimate outcomes of therapy. In this chapter, we learned that initiating and maintaining a relationship that supports occupational engagement is a complex and dynamic process that must be intentional in order to be maximally responsive to a client’s developing interpersonal needs in therapy. The chapter began with a historical overview of prior conceptualisations and approaches to therapeutic use of self throughout the history of our field. A rationale for the need for a conceptual model of practice that uniquely addresses the interpersonal aspects of occupational therapy and does not interfere with other models and approaches to practice was provided. A model that responds to that need, the IRM was presented. The primary components of the model and their relationships were described. A successful therapeutic relationship was defined according to the model’s principles. Finally, a case example was provided by the second author to illustrate application of specific aspects of the model in a practice situation.
American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders – Text Revision IV. American Psychiatric Association, 2000.
Ayres-Rosa S, Hasselkus BR. Connecting with patients: The personal experience of professional helping. The Occupational Therapy Journal of Research. 1996;16:245-260.
Baum CM. Occupational therapists put care in the health system. American Journal of Occupational Therapy. 1980;34:505-516.
Beck J. Cognitive therapy: Basics and beyond. New York: Guilford Press, 1995.
Bing RK. Eleanor Clark Slagle lectureship 1981 Occupational therapy revisited: A paraphrastic journey. American Journal of Occupational Therapy. 1981;35:499-518.
Blair SEE, Daniels MA. An Introduction to the Psychodynamic Frame of Reference. In: Duncan EAS, editor. 2006 Foundations for Practice in Occupational Therapy. Edinburgh: Elsevier, 2006.
Bockoven JS. Occupational therapy – a historical perspective: Legacy of moral treatment – 1800s to 1910. American Journal of Occupational Therapy. 1971;25:223-225.
Clark F. Occupation embedded in a real life: Interweaving occupational science and occupational therapy, 1993 Eleanor Clarke Slagle lecture. American Journal of Occupational Therapy. 1993;47:1067-1078.
Cole B, McLean V. Therapeutic relationships re-defined. Occupational Therapy in Mental Health. 2003;19(2):33-56.
Crepeau EB. Achieving intersubjective understanding: Examples from an occupational therapy treatment session. American Journal of Occupational Therapy. 1991;45:1016-1025.
Devereaux EB. Occupational therapy’s challenge: The caring relationship. American Journal of Occupational Therapy. 1984;38(12):791-798.
Duncan EAS, editor. Foundations for Practice in Occupational Therapy, 4th Ed, Edinburgh: Churchill Livingstone, 2006.
Fleming MH. The therapist with the three-track mind. American Journal of Occupational Therapy. 1991;45(11):1007-1014.
Forsyth K, Sommerfield G, Taylor RR, submitted. A survey of use of self among therapists in the United Kingdom
Gilfoyle EM. Caring: A philosophy for practice. American Journal of Occupational Therapy. 1980;34(8):517-521.
Jonsson H, Josephsson S, Kielhofner G. Narratives and experience in an occupational transition: a longitudinal study of the retirement process. American Journal of Occupational Therapy. 2001;55(4):424-432.
Kielhofner G. Conceptual foundations of occupational therapy, 2nd edn. Philadelphia, PA: FA Davis; 1997.
Kielhofner G. The Model of Human Occupation, Theory and Application, 4th edn. Maryland: Lippincott, Williams and Wilkins. 2007.
Kielhofner G. Conceptual Foundations of Occupational Therapy, 3rd edn. Philadelphia, PA: FA Davis. 2004.
King LJ. Creative caring. American Journal of Occupational Therapy. 1980;34(3):522-528.
Lyons KD, Crepeau EB. The clinical reasoning of an occupational therapy assistant. American Journal of Occupational Therapy. 2001;55(5):577-581.
Mattingly C. The narrative nature of clinical reasoning. American Journal of Occupational Therapy. 1991;45(11):998-1005.
Mattingly C. The narrative nature of clinical reasoning. In: Mattingly C, Fleming MH, editors. Clinical Reasoning: Forms of inquiry in a therapeutic practice. Philadelphia, PA: Davis; 1994:239-269.
Mattingly C, Fleming MH. Clinical Reasoning: Forms of inquiry in a therapeutic practice. Philadelphia, PA: Davis, 1994;178-196.
Mattingly C, Gillette N. Anthropology, occupational therapy, and action research. The American Journal of Occupational Therapy. 1991;45(11):972-978.
Mosey AC. Three Frames of Reference for Mental Health. Slack. NJ: Thorofare, 1970.
Peloquin SM. Moral treatment: Contexts considered. American Journal of Occupational Therapy. 1989;43(8):537-544.
Peloquin SM. Sustaining the art of practice in occupational therapy. American Journal of Occupational Therapy. 1989;43(4):219-226.
Peloquin SM. The patient–therapist relationship in occupational therapy: Understanding visions and images. American Journal of Occupational Therapy. 1990;44(1):13-21.
Peloquin SM. The depersonalization of patients: A profile gleaned from narratives. American Journal of Occupational Therapy. 1993;47(9):830-837.
Peloquin SM. The fullness of empathy: Reflections and illustrations. American Journal of Occupational Therapy. 1995;49(1):24-31.
Peloquin SM. Reclaiming the vision of reaching for heart as well as hands. American Journal of Occupational Therapy. 2002;56(5):517-526.
Peloquin SM. The therapeutic relationship: Manifestations and challenges in occupational therapy. In: Crepeau EB, Cohn ES, Boyt Schell BA, editors. Willard & Spackman’s Occupational Therapy. Tenth Edition. Philadelphia, PA: Lippincott, Williams & Wilkins; 2003:157-170.
Rogers JC. Clinical reasoning: The ethics, science, and art. 1983 Eleanor Clarke Slagle lecture. American Journal of Occupational Therapy. 1983;37(9):601-616.
Schell BA. Clinical reasoning: The basis of practice. In: Crepeau EB, Cohn ES, Boyt Schell BA, editors. Willard & Spackman’s Occupational Therapy. Tenth Edition. Philadelphia, PA: Lippincott, Williams & Wilkins; 2003:131-152.
Schell BA, Cervero RM. Clinical reasoning in occupational therapy: An integrative review. American Journal of Occupational Therapy. 1993;47(7):605-610.
Schwartz KB. The history of occupational therapy. In: Crepeau EB, Cohn ES, Boyt Schell BA, editors. Willard & Spackman’s Occupational Therapy. Tenth Edition. Philadelphia, PA: Lippincott, Williams & Wilkins; 2003:5-13.
Schwartzberg SL. Interactive reasoning in the process of occupational therapy. Upper Saddle River, NJ: Pearson Education, 2002.
Shannon PD. The derailment of occupational therapy. American Journal of Occupational Therapy. 1977;31:229-234.
Sommerfield G, Forsyth K, Taylor RR. Therapeutic Use of Self within Paediatric Practice. Manuscript submitted for publication, 2007.
Taylor RR. The Intentional Relationship: Occupational Therapy and Use of Self. Philadelphia: FA Davis, 2008.
Townsend E. Reflections on power and justice in enabling occupation. Revve Canadienne D’Ergotherapie. 2003;70:74-87.
Yerxa EJ. Authentic occupational therapy [Eleanor Clarke Stagle Lecture]. American. Journal of Occupational Therapy. 1967;21:1-9.
Yerxa EJ. Occupational therapy’s role in creating a future climate of caring. American Journal of Occupational Therapy. 1980;34(8):529-679.