Chapter 22 Clinical Supervision Skills
Overview
In this chapter, clinical supervision will be defined, and the elements of clinical supervision elucidated. What clinical supervision is not will be briefly mentioned, as will the differences between supervision and mentoring. The perceived benefits of clinical supervision for occupational therapists, the organisation and the clients will then be described. While there are many models of supervision, the model this author has successfully implemented as part of a multidisciplinary collaboration in a mental health setting will be presented. The evidence in support of clinical supervision will be outlined. Skills, procedures and guidelines for enhancing clinical supervision will then be described. Examples of clinical supervision in action will be presented throughout the chapter.
Historical context
Within occupational therapy, considerable attention has been given to the clinical supervision of students undertaking clinical placements (see, for example, Strong et al 1996, Hummell 1997). The other area of practice where clinical supervision has traditionally been available has been in mental health, where workers of many disciplines have sought supervision (see Spence et al 2001). More recently, supervision for new graduate occupational therapists (Jacobs 1994) and occupational therapists working in isolated, rural and remote locations has become prominent. For example, Lee and Mackenzie (2003), identified that the availability of support/supervision was the most common factor assisting in the transition of new graduates starting work in a rural setting. Cusick and her colleagues (2004) examined priorities and problems for new graduate occupational therapists entering acute care hospitals. The need for quality supervision was highlighted as critical for assisting these new graduate occupational therapists to function in the acute care clinical role, and to assist with staff retention.
Professional associations worldwide have developed standards and position papers about supervision and mentoring. For example, in 2000, OT Australia Inc published its national policy on mentoring and supervision, in tandem with its personal accreditation scheme. The policy identified the need for new graduate occupational therapists and therapists newly arrived in Australia to gain a minimum of 20 accreditation points from the ‘receiving mentoring or supervision’ category during the cycle of accreditation. Practitioners with more than 2 years of experience were not mandated supervision/mentoring, but could still gain accreditation points.
In this chapter, the contention is made that the benefits of clinical supervision are to be had in all areas of practice, and for occupational therapists of all levels of clinical experience. Of course, one size does not fit all. New graduates will need more frequent and possibly directive supervision than occupational therapists with many years experience working in a particular area. Occupational therapists moving from one practice area to another may also require more frequent supervision. Experienced practitioners also have much to gain from supervision.
As we reflect on our experiences as occupational therapists, it will be clear that supervision, when and where it occurs, does not just happen. For occupational therapists working within mental health facilities, there is a rich tradition of supervision, both within the work setting and privately. Supervision denotes a considered, planned, and resource-intense interaction, usually between two people, over a period of time. It can be considered as having a set of functions, core tasks and processes. As Rich (1993) commented, supervision is characterised by ‘the development of a supportive supervisory climate and a base of staff professional skills and values, enacted through a cycle of observation and discussion, and directed towards the delivery of quality client services in accordance with organisational and professional values’ (p. 172).
It should also be clear that supervision is different to mentoring, although some supervisors provide the encouragement and professional development support that we might typically expect to receive from a mentor. They provide this support and encouragement in addition to other roles and functions they perform as supervisor.
Supervision
Supervision has been defined as a ‘working alliance between two or more professional members where the intention of the interaction is to enhance the knowledge, skills and attitudes of at least one staff member’ (Spence et al 2001: 136). Spence et al (2001: 136) asserted that the main aim of supervision was ‘to optimise the service provided to clients, in line with the goals, expectations, and ethical and professional standards of the organisation and profession concerned (Proctor 1994; Rich 1993)’. Within supervision, clinical practice issues, administrative/organisational issues and personal support issues are worked on (Spence et al 2001).
What supervision is not …
It is important to understand that supervision is not therapy (Jones 1998, Yegdich 1999, MacDonald 2002). The goals of supervision and therapy are different, as is the focus of the interaction (Yegdich 1999). In supervision, the focus is upon the supervisee’s work with their patients, while the focus of therapy would be the well-being of, in this case, the supervisee (Yegdich 1999). Keeping the clients centre-most is critical for supervision. For example, it is not appropriate for supervision to become a time where the supervisor helps the supervisee with his personal problems. In circumstances where the supervisor ascertains that the supervisee has personal problems which are impacting upon their ability to perform his work, the supervisor should advise the supervisee to seek professional help for their problems. Where such facilities exist, the supervisor may also recommend the supervisee attends the organisation’s occupational health department for assessment and support.
Supervision is not a time for the supervisor to dazzle the supervisee with their brilliance, or unload their own issues. The focus must be on the supervisee and her work. Supervision is not a time for a general chat about life. Nor should it become a conversation where either party complains about the professional practices of other staff.
Having a clear supervision agreement and basing supervision upon a model of practice helps ensure focus upon the real business of supervision.
Differences between mentoring and supervision
The example that comes easily to mind of a mentoring relationship is one of a more experienced occupational therapist (or other more senior health professional) providing general career guidance, emotional support and staff development for a more junior occupational therapist. Reflecting on my own career, I was fortunate to find life-long mentors through both my early involvement with the occupational therapy professional association, my university academic mentors who continued to be significant in my professional life long beyond my graduation ceremony, and my clinical practice environments. These women and men were dedicated and selfless in the mentoring relationship. Rather than dealing with specific clinical cases as should occur in supervision, they assisted me to see the generality of practice, the thematic issues in practice, the burning questions for myself and the profession, and the key issues for scholarly practice. At a time when few of my peers were embarking upon post-graduate studies, they nurtured and supported my dreams and visions, and challenged me to dig deeper to achieve more, more for me as an individual therapist, and in so doing, more for the profession and for my patients.
How did these mentoring relationships differ from clinical supervision? In a number of ways:
Several agencies (see, for example, The University of Queensland http://www.uq.edu.au/hupp/index.html?page=25415&pid=25173, accessed 24/04/2006) make a clear distinction between performance management and mentoring, with the key element being that mentoring is a private, non-reporting relationship. Mentoring is something which is entered into on a voluntary basis, on both the part of the mentee and the mentor. Supervision, on the other hand, is not an optional matter; it is a requirement of many workplaces.
Benefits of supervision
Strong et al (2003) in their study of supervision practices for occupational therapists, psychologists, social workers and speech pathologists (hereafter referred to as allied health professionals) working within a large mental health service, found that allied health professionals perceived five main benefits from supervision. First and foremost was the view that supervision provided important professional development and support for workers. Such support was seen as affirming and greatly valued by participants. Furthermore, the provision of such support was seen as a useful way of enhancing job satisfaction and reducing job burnout.
The second perceived benefit found in the study (Strong et al 2003) was that supervision provided an important means of ensuring the competence of allied health professionals, and hence assisted with the provision of best practice for clients. This quality assurance function was seen as working through the provision of feedback and direction to supervisees on their practice with particular clients. The delivery of evidence-based outcomes to clients was highlighted as an important benefit of such quality assurance.
Third, the allied health professionals saw supervision as helping them learn about the organisational culture and practices of a workplace. Supervision was also seen to assist in the preservation of disciplinary identity, especially given the interdisciplinary nature of much of the work. Finally, allied health professionals saw that supervision was beneficial because it assisted them to learn new skills and further develop their clinical reasoning.
Using a similar methodology of focus group interviews with school guidance counsellors in a large education service, McMahon and Patton (2000) found that supervision was perceived as providing support to individual counsellors, as reducing professional isolation, as providing opportunities for debriefing, as assisting in accountability, providing professional skill development, and helping induct new counsellors into the profession. Thus it seems the benefits of supervision are similar, regardless of professional grouping.
Vignette 22.1 provides an example of how supervision can assist a newly graduated occupational therapist in her work.
Vignette 22.1 Supervision with a new graduate
Let me give you an example of how supervision might help a new graduate occupational therapist to enhance her outcomes with the children and families she is currently working with. Lets call the therapist Lisa. Lisa is in the first 6 months of her first job, in a Child and Youth facility. Her caseload includes a number of children aged between 712 who are school avoidant, and falling behind in their schoolwork. One of her clients is 9-year-old Jane, who comes to therapy with her mother Nina. Lisa dreads these therapy sessions: each time, Jane and her mother end up shouting at each other, before Jane storms out of the room and wont come back. This has happened three times now, and Lisa knows shes not made any progress. But she doesnt know what to do.
Lisa brings this case to her monthly supervision session. Her supervisor asks her what her goals for therapy are. Who is she providing therapy for? Lisa thinks shes trying to help Jane to improve her performance at school and to help her get on better with her Mum. That is why she has been seeing them together. As she talks it through with her supervisor, Lisa sees how she can better structure the therapy sessions, so she works alone with Jane on her performance skills. She also schedules time to meet with the Mum, to explain the things shes doing with Jane, and to reinforce the Mums efforts to support Jane.
At the next supervision, the supervisor asks Lisa how her client Jane has been getting on. And Lisa is able to report about the gains that Jane has been making. She's glad she raised it in supervision last month. She almost hadnt mentioned it, as she was feeling she was such a hopeless therapist, and she didn't want her supervisor to know how bad she was.
Lisa's initial hesitancy to expose her ignorance to her supervisor is not an uncommon feeling. Many clinicians have expressed vulnerability in supervision where the supervisor has line management authority. However, because she and her supervisor had developed a supervision agreement, and she understood that the supervision was not a punitive thing, she had the confidence to raise the issue.
Skills and procedures for effective supervision
Good supervision does not occur by osmosis. It requires a positive attitude and commitment on the part of the organisation, the supervisor and the supervisee. Along with such commitment, there are requisite resource implications, especially relating to time and training. Having a clear model of supervision in the organisation, and a written policy, is very, very important.
There are a number of concrete ways that individual occupational therapists can enhance existing supervisory relationships or, in the absence of a supervisory relationship, establish beneficial working alliances in the workplace. The best first step is in developing a supervision agreement (or contract) with your supervisor. It is also useful to have an agenda for each supervision session; this time is precious, so aim to maximise it. It can be useful to have some understanding about your preferred learning style, and that of your supervisee (Kolb 1984). A variety of methods for learning in supervision can be used, including self-review, chart review, audio-tape or video-tape review, or real-time observation, and role play methods. These are things you can discuss in your introductory session, when you are drawing up your supervision agreement. The best, most effective supervision is not confined to verbal learning.
It is recognised that supervision can be adapted to meet different needs and contexts. Things which should be considered include the level of experience of the supervisee, the nature of the work tasks, the resources available to support supervision, the size of the staff, and the location of the workplace. Supervision may be individual, or peer-based. It may involve face-to-face sessions, audio/visual, teleconferencing sessions or email contact.
The supervisor needs to be clear on their role as a supervisor, and ideally to have received training in supervision.
A model for supervision and the role of the supervisor
Having a model for supervision can assist both the supervisee and supervisor to gain clarity about the supervision process. It assists all to have a clear understanding about the purpose, content, and rights and responsibilities of all parties. Concurrent with an acceptable model of supervision, there needs to be a policy that resources and supports this use of staff time to promote positive outcomes for the patients or clients and the ongoing professional development of the staff.
A model of supervision should be built on a belief that supervision is a desirable and valued activity that enhances the quality of clinical practice, improves client outcomes and supports staff who may be working in difficult circumstances.
The model which we have used in our supervision work in a large mental health workforce is called the ‘flexible working alliance approach’ to supervision (Kavanagh et al 2004); see Figure 22.1. The model has a triad of participants: supervisor, patient/client and the supervisee, and a triangle of supervisor functions. These functions are:
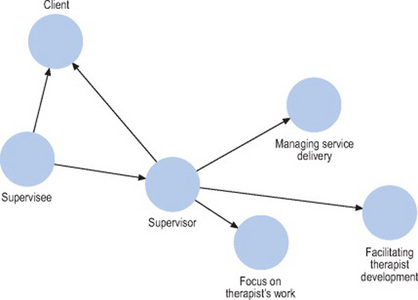
Figure 22.1 A model of supervision, highlighting the importance of the client, the supervisee and the supervisor, in addition to the supervisor’s responsibilities in managing service delivery, focusing on the therapist’s work and facilitating the therapist’s professional development
The supervisor needs to be mindful of the focus upon the needs of the client, the needs of the supervisee, and the needs of the organisation. For example, if the supervisor focuses exclusively on only a few pieces of the supervisee’s work, she may neglect to ensure that the needs of all clients are being met and an assessment of the worker’s professional development needs may be inaccurate. The model highlights how different aspects of the work are linked and may be in tension with each other. This tension may manifest itself as conflict, for example asking an under-prepared therapist to take on tasks because of a high demand for services.
The triadic nature of the model illustrates that supervision involves an interaction between functions, tasks and outcomes. In any supervision session choices are made about what to focus on (Hawkins and Shohet 1989). Effective supervision requires that all functions and all participants are eventually attended to, though at any one time the supervisor will need to focus on one or two functions or participants.
A supervisor will need to adapt her personal responses, and the use of other resources, depending on:
Supervisors need to have the following core skills:
Supervision agreement
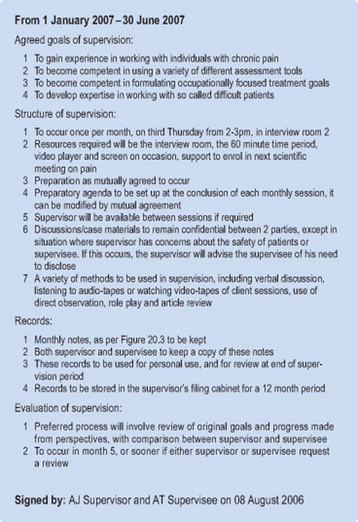
It is very helpful for the supervisee and supervisor to develop and use a supervision agreement (or contract) (see Figure 22.2 for an example). First and foremost, the agreement will identify the goals of the supervisory relationship. This should involve making a detailed list of the knowledge and skills that the supervisee and supervisor would like the supervisee to develop in the supervision sessions.
It will be useful for this list to be reviewed regularly, and renegotiated as the needs and skills of the supervisee change over time. In developing this list, it can be useful for the supervisee and supervisor to independently write a list, and then compare lists to arrive at a set of mutually agreed goals. If at this time, it appears that there are some skills required which the supervisor does not herself/himself hold, then the mechanisms and resources for gaining these skills should be identified.
The structure of supervision should then be documented. Matters such as the frequency of supervision, time available and location need to be explicitly stated, for example, supervision will occur on the third Friday of the month in office X from 2–3 pm. The sorts of notes that will be made of the sessions, and who has access to those records will be identified. A set of sample supervision session notes are contained in Figure 22.3.
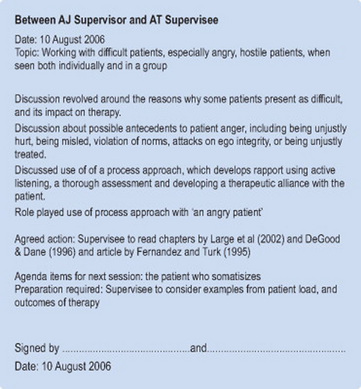
The format of the supervision sessions will also be documented. For example, case notes will be reviewed, training videos and role-plays will be used, in addition to verbal discussion of cases. Acceptable reasons for non-attendance at supervision will be discussed and agreed upon. (Note: being too busy with clinical work is generally, but not always, a non-defensible reason for cancelling supervision.) The mutual obligations of both supervisor and supervisee should be discussed and documented. These include matters around confidentiality, especially when the supervisor is the line manager for the supervisee. Also, the level of preparation required for supervision sessions by both supervisor and supervisee should be indicated. Establishing the use of agendas can also be a useful part of this agreement. The agenda planning can be included as part of the notes of supervision, as illustrated in Figure 22.3. The supervision agreement should indicate when and how the supervision will be reviewed.
There are times when a therapist’s supervisor is also the line manager of a service. This can place pressure on both the supervisee, who may think ‘but I can’t let him know I am having difficulty with my therapy with clients, or I might be put on performance review’, and the supervisor, who may be juggling demands to increase caseload and client outcomes versus supporting a new member of the team find his feet with his clinical cases. This is definitely a case where developing clear expectations and boundaries for supervision and building them into a supervision contract can be so useful.
It should be stated that many points in the supervision agreement will not be open to negotiation (Hughes and Pengally 1997). This is not a contract between equals. However, it is important for building the trust in the relationship that the supervisee’s views are carefully considered in formulating the supervision agreement.
The supervision agreement which will be developed needs to be based on relevant policies that exist in the organisation, including policies on the aims and functions of supervision, resources to carry out supervision, including time, space, absence of interruptions, the status of records of supervision, provision for situations where the supervisory relationship breaks down, rights and responsibilities of supervisor and supervisee, confidentiality and its limits, and evaluation and reviewing supervision and the role of supervision in staff appraisal.
Situations that may arise in supervision
Some supervisory relationships proceed without a hitch, and the agreed goals of assisting the supervisee to become a more competent practitioner are realised. In other cases, situations may arise in supervision which challenge either the supervisor or the supervisee. For example, the situation might arise where the supervisor notices that the supervisee is very defensive, and resists participating in the supervision, right from the first session when they met to draw up a supervision agreement. The supervisee attends his supervision sessions, but seems to be responding only on a superficial level. In this case, the supervisor needs to consider whether the supervision relationship is contributing to the supervisee defensiveness, and if so, attempt to build a greater level of support and trust. The supervisor would highlight this issue, and indicate how it was hampering effective supervision. In one case where a supervisee was upset that the supervisor had been promoted to a position for which the supervisee had also applied, it was necessary to obtain a different supervisor, as the deep-seated resentment limited any progress.
In another case, the supervisor became aware that the supervisee was engaging in unethical practice. She was able to discuss this problem with the supervisee, and review both the professional and organisational ethical guidelines for practice. Sometimes, the correct ethical stance is not directly clear to therapists. As a young graduate I worked with patients with brain tumours, and their families, over extended periods of time. In one instance, I became close to one patient who came for weekly therapy almost up until the time of her death. I wanted very much to attend her funeral to pay my respects to her and her family. Unfortunately, I did not have a supervisor to discuss this issue with. Supervision was not an accepted part of the landscape in my work environment at this time. I decided not to go to her funeral, as I worried it was unethical to do so. I did not want to get personally involved, and misconstrued attending a funeral with getting personally involved. With hindsight, my decision would have been different. I certainly did not do anything unethical. However my interpretation on my code of ethics was not totally sensible at that time.
Another situation that might arise is where the supervisor and the supervisee have different theoretical orientations. For example, an occupational therapist may have begun work in a pain management unit, where the prevailing theoretical orientation is the cognitive-behavioural approach. His supervisor is a strong advocate of cognitive-behavioural-based therapy, while he has a much more humanistic, client-centred approach. Rather than argue over which approach is better, in supervision the pair agreed to respect both approaches after the supervisor reframed the questions to consider what was in the particular patient’s best interest.
Supervision training
As may have been gleaned from earlier sections, the skills for effective supervision do not just appear by serendipity. This has been both our experience (see Spence et al 2001, Strong et al 2003, Kavanagh et al 2004), and that of other workers (see Hancox et al 2004). Ideally, both supervisors and supervisees can be trained, so that both have the skills and attitudes to make supervision work best for them and their patients. MacDonald (2002) has suggested the importance of adult learning principles in supervision training. Training programmes have been developed by multiple authors, and for multiple purposes. For example, Kavanagh et al (2004) developed a 2-day supervision training programme for allied health professionals, nurses and medical staff working in a state-wide mental health service. Hodgins et al (2005) developed a model of supervision to be provided to rural general practitioners working with clients with mental health problems. Jones (1998) developed a seminar to prepare nurses for clinical supervision, while Hancox and her colleagues (2004) developed a clinical supervision training programme for nurses working in the mental health service in one Australian state.
Evidence in support of supervision
In 2001, as part of a supervision project with allied health professionals in a large mental health service, Spence and her colleagues observed that there was minimal evidence in support of supervision, despite a plethora of literature and a general agreement among practitioners that supervision was of value. ‘It is not clear whether supervision actually produces a change in clinical behaviour, nor whether it produces benefits in terms of client outcome’ (Spence et al 2001: 135). Other researchers concur with the paucity of empirical evidence on the impact of supervision (Holloway and Neufeldt 1995, Freitas 2002).
Several authors have observed the difficulties in evaluating the effectiveness and impact of supervision (Freitas 2002, Worrall et al 2006). Issues such as lack of comparison groups, the lack of random assignment of supervisors and supervisees to experimental groups, small sample sizes, and drop-out rates have all been observed in the research literature (Ellis et al 1996, Spence et al 2001). Furthermore, attempting to determine the impact of supervision on client outcomes raises issues with client confidentiality and confounding life events that may have a bearing upon outcomes.
It is proposed that the effectiveness of supervision can be best considered through the lens of the tripartite model of supervision illustrated in Figure 22.1. Using this model, one can ask ‘what is the impact of the supervision on?’:
Key findings from available studies will be considered from these different viewpoints.
Supervisee studies
McMahon and Patton (2000) utilised a focus group methodology to ascertain the value of clinical supervision for school guidance officers in a large education authority. A randomly selected group of 51 guidance officers reported that supervision assisted them to develop their skills, for personal development, to debrief, to counteract the effects of geographical and/or professional isolation, to assist in induction of new staff members and to help with accountability. These findings were similar to those by Strong et al (2003) reported earlier in this chapter.
Teasdale et al (2001) surveyed 211 nurses about the impact of clinical supervision, using both written questionnaires and qualitative comments on critical incidents. Results compared supervised and non-supervised nurses. It was found that supervised nurses felt part of a more supportive organisation, coped better at work, and felt that they had better access to support than non-supervised nurses. These findings were particularly notable in more junior nurses.
In a state-wide mental health service study of 272 allied health staff, using a Supervision Attitude Scale, Kavanagh et al (2004) found that staff perceived the benefits of the supervision in terms of managing their own stress levels and in debriefing, rather than a specific improvement in their own skills.
Studies by Christie et al (1985) of occupational therapy students, and Kadushen (1974) of social work supervisees, found that inexperienced practitioners preferred the supervisor to observe their practice, to provide skills training and to be available to assist them when and if they had difficulties.
Organisation studies
Kavanagh et al (2004) examined the perceptions of service directors regarding the benefits of a state-wide supervision training programme for allied health professionals. Seventy-eight percent of the Directors of all community mental health centres in Brisbane reported a positive impact of the project on the clinical effectiveness of their staff, while 64% reported a positive impact on staff morale. ‘Directors reported that they perceived that the quality and standard of allied health practice had improved’ (Kavanagh et al 2004: 18).
Client studies
As noted by Spence et al (2001: 144), ‘there has been very little research to determine whether supervision is actually effective as a method of enhancing the best practice of clinicians and of maximizing client outcomes.’ Some researchers have reported that clients are more likely to attend therapy sessions more often with therapists who have been receiving more frequent supervision (see, for example, Burgoyne et al 1976, Steinhelber et al 1984). While this does not indicate better client outcomes, it is suggestive of some positive impact of supervision upon the clients. Clearly, more work is needed in this difficult area.
Conclusions
While the research evidence is still not in about the benefits of clinical supervision, there are many indications that the provision of clinical supervision can have benefits for the individual therapist, the organisation and most importantly, the clients. It is recommended that occupational therapists’ embrace the concept of supervision, across all areas of practice. Training in the provision of supervision is helpful, as good supervision does not just happen. Practical strategies such as developing a supervision agreement, and using agendas for supervision, should be used. Using a variety of learning methods in supervision is also strongly recommended.
Acknowledgements
I thank my colleagues, Prof David Kavanagh, Prof Jill Wilson, Prof Susan Spence, and Prof Linda Worrall, with whom I have spent many hours learning about supervision. Most of the ideas raised in this chapter were learned and/or crystallised with these good colleagues and friends over the past decade. I acknowledge the financial support of Queensland Health which enabled us to develop and evaluate a supervision training programme for the mental health services in Queensland Australia. Queensland Health is the copyright holder of all the reports delivered on the outcomes of this project. Some findings from the studies are referred to in this chapter.
Burgoyne RW, Santini S, Kline F, et al. Who gets supervised? An extension of patient selection inequity. American Journal of Psychiatry. 1976;133:1313-1315.
Christie BA, Joyce PC, Moeller PL. Fieldwork experience: I. impact on practice preference. American Journal of Occupational Therapy. 1985;39:671-674.
Cusick A, McIntosh D, Santiago L. New graduate therapists in acute care hospitals: priorities, problems and strategies for departmental action. Australian Occupational Therapy Journal. 2004;51:174-184.
deGood DE, Dane JR. The psychologist as a pain consultant in outpatient, inpatient and workplace settings. In: Gatchel RJ, Turk DC, editors. Psychological approaches to pain management. A practitioner’s handbook. London: Guilford Press; 1996:403-437.
Ellis MV, Ladany N. Inferences concerning supervisees and clients in clinical supervision: an integrative review. In: Watkins CEJr., editor. Handbook of psychotherapy supervision. New York: Wiley; 1997:447-507.
Ellis MV, Ladany N, Krengel M, et al. Clinical supervision research from 1981 to 1993: a methodological critique. Journal of Counselling Psychology. 1996;43:35-50.
Fernandez E, Turk DC. The scope and significance of anger in the experience of chronic pain. Pain. 1995;61:165-175.
Freitas GJ. The impact of psychotherapy supervision on client outcome: a critical examination of two decades of research. Psychotherapy: Theory, Research, Practice, Training. 2002;39:354-367.
Hancox K, Lynch L, Happell B, et al. An evaluation of an educational program for clinical supervision. International Journal of Mental Health Nursing. 2004;13:198-203.
Hawkins P, Shohet R. Supervision in the helping professions:an individual, group and organisational approach. Philadelphia, PA: Open University Press, 1989.
Hodgins G, Judd F, Kyrios M, et al. A model of supervision in mental health for general practitioners. Australasian Psychiatry. 2005;13:185-189.
Holloway EL, Neufeldt SA. supervision: its contributions to treatment efficacy. Journal of Consulting and Clinical Psychology. 1995;63:207-213.
Hughes L, Pengelly P. Staff supervision in a turbulent environment: managing process and task in front-line services. London: Jessica Kingsley Publishers, 1997.
Hummell J. Effective fieldwork supervision: OT student perspectives. Australian Occupational Therapy Journal. 1997;44:147-157.
Jacobs J. Clinical supervision. An international issue. American Journal of Occupational Therapy. 1994;57:488-499.
Jones A. Getting going with clinical supervision: an introductory seminar. Journal of Advanced Nursing. 1998;27:500-506.
Kadushin A. Supervisor–supervisee: a survey. Social Work. 1974;19:288-297.
Kavanagh D, Wilson J, Worrall L, et al. A research evaluation of professional supervision and mentoring of health professionals in the mental health service. Brisbane, Australia: A collaboration between the University of Queensland and Queensland Health, 2004;7-14. Reports
Kolb DA. Experiential learning: experience as a source of learning and development. Englewood Cliffs, NJ: Prentice Hall, 1984.
Large RG, New F, Strong J, et al. Chronic pain and psychiatric problems. In: Strong J, Unruh AM, Wright A, et al, editors. Pain textbook for therapists. Edinburgh: Churchill Livingstone, 2002.
Lee S, MacKenzie L. Starting out in rural New South Wales: the experiences of new graduate occupational therapists. Australian Journal of Rural Health. 2003;11:36-43.
MacDonald J. Clinical supervision: a review of underlying conceptual developments. Australian and New Zealand Journal of Psychiatry. 2002;36:92-98.
McMahon M, Patton W. Conversations on clinical supervision; benefits perceived by school counsellors. British Journal of Guidance & Counselling. 2000;28:339-352.
OT Australia Inc. mentoring/supervision policy paper. 2000. Available http://www.uq.edu.au/hupp/index.html?page=25415&pid=25173, 2000.
Proctor B. Supervision: competence, confidence, accountability. British Journal of Guidance & Counselling. 1994;22:309-318.
Rich P. The form, function and content of supervision: an integrated model. The Clinical Supervisor. 1993;11:137-178.
Spence SH, Wilson J, Kavanagh D, et al. Clinical supervision in four mental health professions: a review of the evidence. Behaviour Change. 2001;18:135-155.
Steinhelber J, Patterson V, Cliffe K, et al. An investigation of some relationships between psychotherapy supervision and patient change. Journal of Clinical Psychology. 1984;40:1346-1353.
Strong J, O’Reilly M, Elliot Schmidt R, et al. Clinical supervisors’ training for rural occupational therapists. In A University of Queensland and Rural Health Support. Australia: Education and training (RHSET) funded project; 1996.
Strong J, Wilson J, Kavanagh D, et al. Supervision practice within a large allied mental health workforce: exploring the phenomenon. The Clinical Supervisor. 2003;22:191-210.
Teasdale K, Brocklehurst N, Thom N. Clinical supervision and support for nurses; an evaluation study. Journal of Advanced Nursing. 2001;33:216-224.
Worrall L, Wilson J, Kavanagh D, et al. Reported effects of supervision on clinical practice – an initial descriptive study. Clinical Supervisor, 2006. revision submitted
Yegdich T. Lost in the crucible of supportive clinical supervision: clinical supervision is not therapy. Journal of Advanced Nursing. 1999;29:1265-1275.