Chapter 8 Traditional plant medicines as a source of new drugs
DEFINITION
The scientific study of traditional plant medicines can be considered as a major part of ethnopharmacology, a term that was only introduced in 1967 but which describes an approach to the discovery of single biologically active molecules that has been used ever since the first compounds were isolated from plant material. Ethnopharmacology can be defined as the scientific study of materials used by ethnic and cultural groups as ‘medicines’; in most instances, this is synonymous with the study of traditional medicines. These are usually the flowering plants, and so in most cases ethnopharmacology can be considered as a branch of ethnobotany: the study of the uses of plants by ethnic groups. However, it should be noted that some cultures, e.g. traditional Chinese medicine (TCM), also make use of animal and mineral matter, and so ethnopharmacology would also encompass the study of these.
Some discussion has taken place concerning the boundaries of what is meant by ‘ethnic’. Some would include all ethnically based systems outside Western scientific medicine but the balance of opinion probably rests on a more restrictive definition, which includes only those bodies of knowledge that are restricted to a group that has lived in a locality for a long period of time but that does not have a sophisticated theoretical framework, formal education and a documented written history. This more rigid definition excludes the medical systems that have developed over thousands of years in cultures based in China and the Indian subcontinent, and emphasizes small ethnic groups where there is a threat of the rapid loss of knowledge due to globalization, loss of habitat migration and other factors that might lead to loss of cultural distinctiveness.
Some ethnographers would distinguish between folklore and ethnopharmacology, claiming that the former is common knowledge in the population as a whole, largely concerning remedies for minor conditions, based on relatively innocuous material. Ethnopharmacology is more concerned with the knowledge of a few specialists who are regarded by the society as able to correctly diagnose and treat disease states, generally using more potent products. In many situations, these specialists are also linked with the religious practices of the society.
It should also be noted that the discovery of new drugs might derive from a wider use of plants than for strictly medical purposes alone. Thus materials used as poisons, in pest control, in agriculture, as cosmetics, in fermentation processes and for religious purposes might also yield active substances that can be exploited as leads for drug development. It can thus be seen that ethnopharmacology is a very interdisciplinary subject and any thorough investigation will probably need the input of a variety of specialists, such as anthropologists, botanists, chemists and pharmacologists.
HISTORICAL DIMENSION
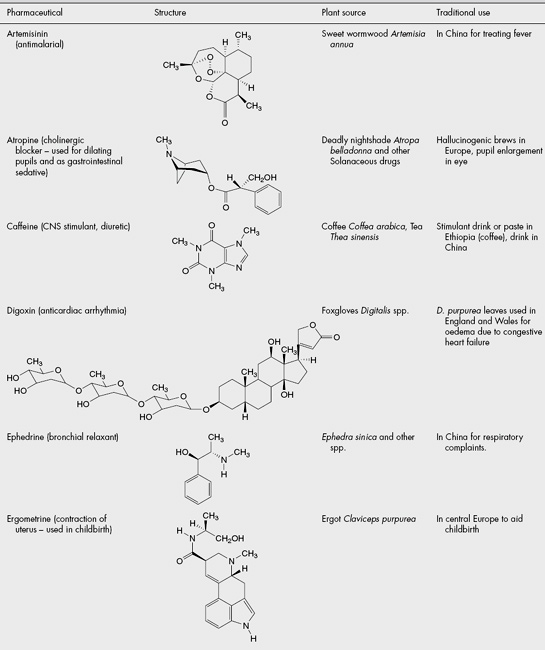
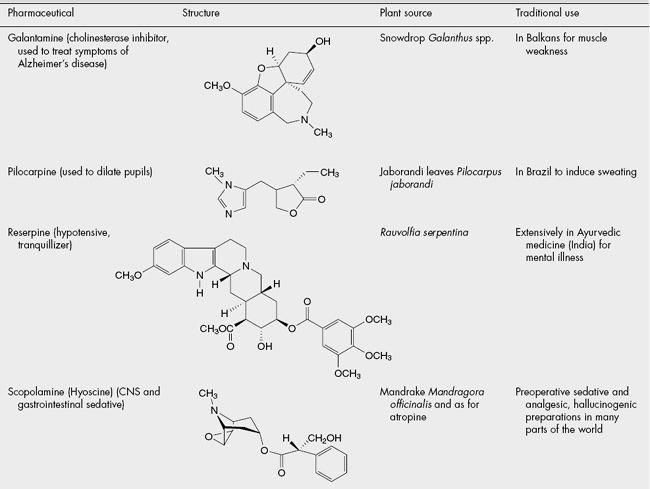
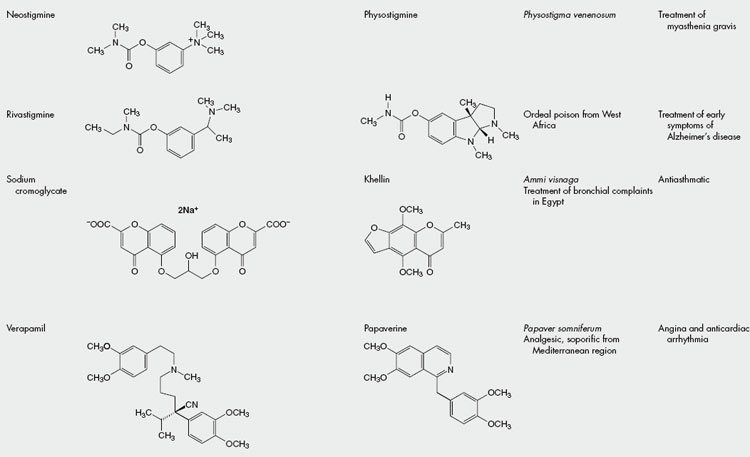
The isolation of some of the opium alkaloids in the early nineteenth century was a key event in the development of modern pharmacy. It showed that isolated compounds had much the same activity as the existing ethnopharmacological material and so paved the way for current orthodox Western medicine, which uses pure compounds for treatment. Since then, a vast amount of money has been spent on the synthesis of novel compounds but also on the isolation of molecules from natural sources and their development into medicines. The contribution of traditional plant medicines to this process has been significant and some notable examples are shown in Table 8.1.
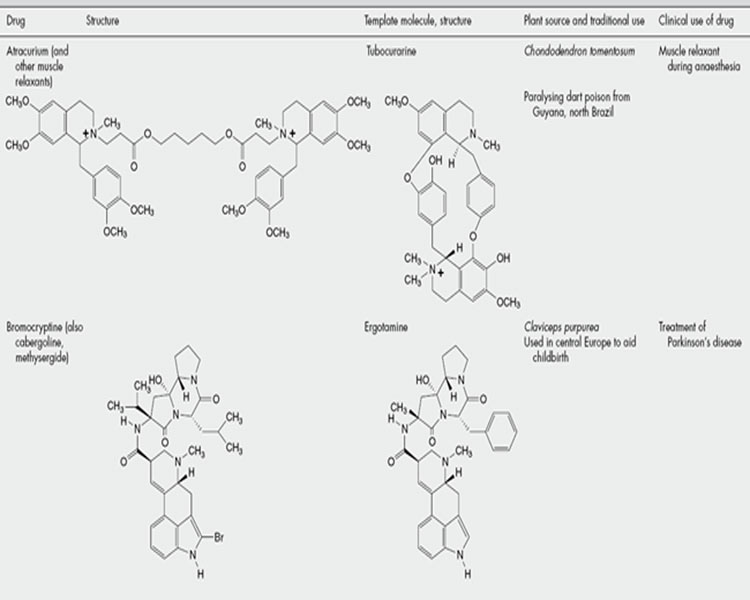
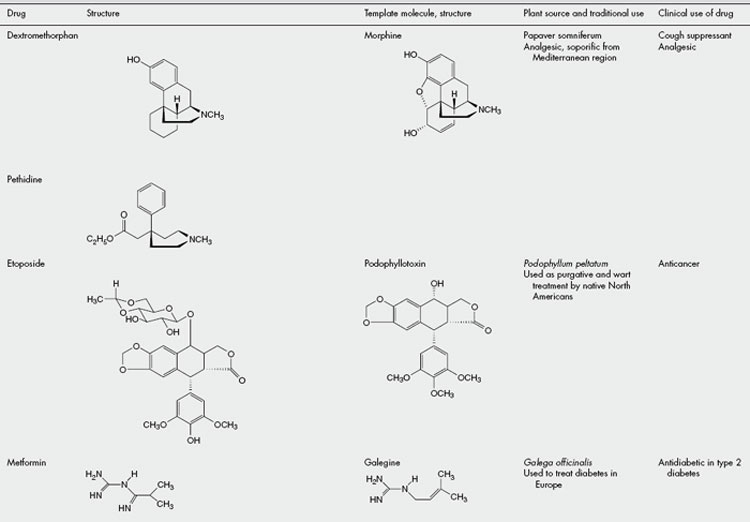
It should also be remembered that the active molecules isolated from traditional medicinal plants might not only provide valuable drugs butare also valuable as ‘lead molecules’, which might be modified chemically or serve as a template for the design of synthetic molecules incorporating the pharmacophore responsible for the activity. Examples of drugs having this origin are shown in Table 8.2.
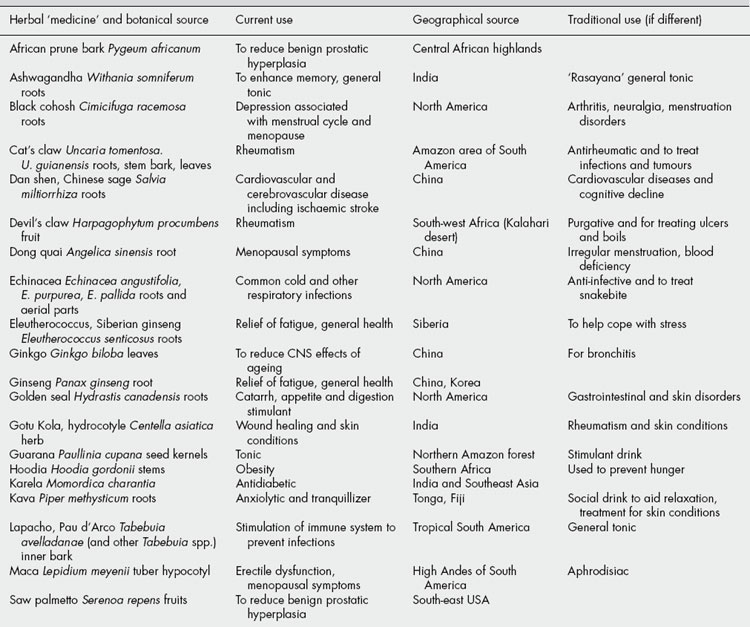
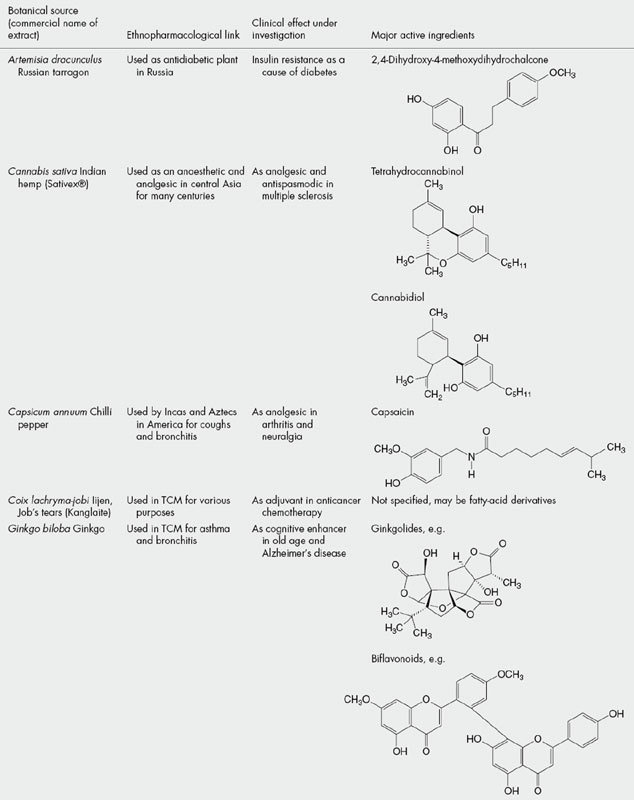
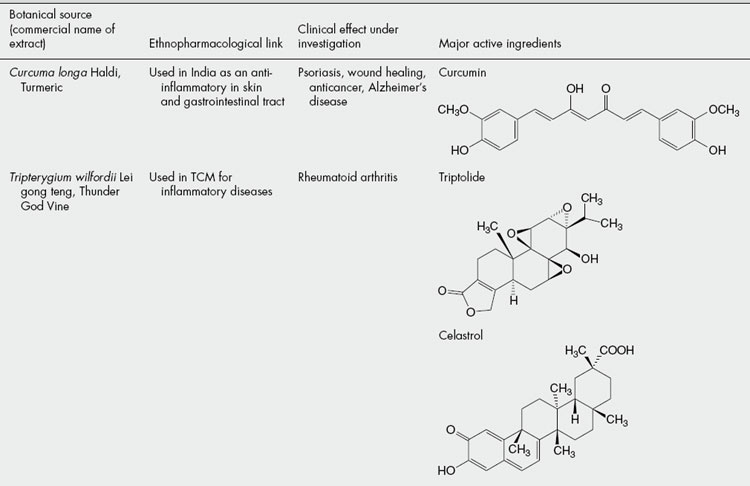
Although the term ‘drug discovery’ is generally used to refer to the isolation of molecules with activity, it should also be remembered that there is increasing interest and recognition that a ‘drug treatment’ might consist of a mixture of compounds. This has always been the case for plant extracts (and most other natural substances), which contain several ‘active ingredients’. It should be noted that such extracts, usually based on a reputed traditional use somewhere in the world, are being introduced and increasingly used as a complementary therapeutic approach in the West. A selection of common ones, together with their ethnopharmacological roots, is shown in Table 8.3.
Scientific interest in ethnopharmacology has increased over the last few years and this is reflected in the formation of the International Society for Ethnopharmacology in 1990 and the European Society for Ethnopharmacology at about the same time. Both of these groups hold regular meetings. Several scientific journals also publish papers on this topic, notably the Journal of Ethnopharmacology, founded in 1979. The 100th volume of this journal, published in 2005, contains many useful ‘state of the art’ reviews on various aspects of ethnopharmacology.
This scientific interest is reflected by wider Western society, with its fascination with a much wider range of aspects of other cultures (e.g. dress, music, food, philosophy, as well as medicines) and this has been catalysed by large population migrations to the West and the relative ease of exposure to exotic cultures, which has been facilitated by large-scale international travel.
Although primarily concerned with human aspects, there has been a recent upsurge of interest in veterinary ethnopharmacology, i.e. methods and materials used to treat animals, particularly those important to the local economy as providers of food, transport and fibres. Other expansions from a strict definition of ethnopharmacology as being the study of medical practices include aspects of plants and other materials used in the diet, those used for ritualistic purposes, for poisons of various types, as cosmetics and as adjuncts to social gatherings. The increasingly blurred distinction between food and medicine, which has become a notable feature in ‘Western’ society, is a situation that has always been the case in other medical systems, such as Ayurveda and TCM, and it is now widely recognized that particular plants comprise part of the regular diet as much as for health maintenance as fortheir macronutritional properties. Attention has also been focused on the ways in which the role of a substance can change through time or as it is transferred from one culture to another. Thus, coffee was thought of as primarily medicinal when it was first introduced into northwest Europe in the seventeenth century, but quite rapidly became a beverage. It is also of interest that cultural restraints might minimize abuse of a substance in its indigenous context but that, when these restraints are removed as the plant begins to be used in another part of the world or society, it becomes a problem to that society. An example of this situation is seen with the abuse of kava-kava in Australia by aboriginal peoples, who do not have the framework of ritualistic use of these roots in the Pacific islands of Fiji and Tonga, where it originates.
Several recent surveys have shown that using ethnopharmacology as a basis of selecting species for screening results in a significant increase in the ‘hit rate’ for the discovery of novel active compounds compared with random collection of samples. It should be noted that several ‘classical’ drugs stated to have derived from ethnopharmacological investigations, e.g. several shown in Table 8.1, arise from plants known as poisons rather than those with a more ‘gentle’ action, which comprise the bulk of many herbal medicine species. The latter group often relies on a mixture of compounds with a mixture of activities, where synergism and polyvalence might be occurring, and where the isolation of one ‘active constituent’ is much less likely.
With a very large number of living organisms still awaiting scientific investigation (about 90% of the estimated 250,000 species of flowering plants, probably the most studied part of the biosphere), ethnopharmacology appears to offer a reasonable selective strategy to be considered in deciding which organisms to study. An interesting overview of some ethnopharmacologically based molecules and the problems involved in their gaining regulatory status was published recently (T. W. Corson and C. M. Crews, Cell, 2007, 130: 769–774).
THE PROCESS OF MODERN DRUG DISCOVERY USING ETHNOPHARMACOLOGY
The discovery process is composed of several stages. The first stage must be the reported use of a naturally occurring material for some purpose that can be related to a medical use. Consideration of the cultural practices associated with the material is important in deciding possible bases of the reputed activity. If there is an indication of a genuine effect, then the material needs to be identified and characterized according to scientific nomenclature. It can then be collected for experimental studies, usually comprising tests for relevant biological activity linked with isolation and determination of the structure of any chemicals present that might be responsible. The ‘active’ compounds are usually discovered by several cycles of fractionation of the extract linked with testing for the activity of each fraction, until pure compounds are isolated from the active fractions, a process known as bioassay-guided fractionation. These compounds, once their activity is proven and their molecular structure ascertained, serve as the leads for the development of clinically useful products. These various stages are discussed in detail below.
INFORMATION SOURCES
The most reliable type of information arises from in-depth studies carried out by field workers, living in the particular community of a particular ethnic group, on the use of the local plants and other materials. This usually comprises frequent communication with the local population, preferably in their own language. In should be noted, however, that an extensive knowledge of traditional medicines might reside with only a few people and a focus on this group would yield greater results. However, many such people are often reluctant to give away knowledge, which is regarded as ‘protected’ in some way, and this is exacerbated by concern that such knowledge could be exploited by drug companies, with little or no return to the original possessors of this knowledge.
Although the in-depth approach is most valuable, the fact is that most of the drugs that have been developed have arisen from less rigorous observations as a by-product of conquest or colonization. Thus, the more enlightened members of the Spanish conquistadores of Central and South America noted the practices of the various native American groups; and members of the British and French colonial administrations, together with non-governmental groups such as Christian missionaries, catalogued the uses of plants in Africa.
Most of these observations cannot now be checked in any way at first-hand, because the authors are long dead, but their records, books and other documents have been left as sources of information. This also applies to cultures that have left some type of written record, so that information on materials used in medicine in ancient Egypt, Babylonia, India and China is available. A recent paper (E. J. Buenz et al., Trends in Pharmacological Sciences, 2004 25: 494–498) describes some recent advances in electronic scanning of ancient texts that make information retrieval much easier, although the difficulties of linguistics and identifying the plants mentioned are not minimized as obstacles in such research.
Before such knowledge can be investigated scientifically, the information provided will often need clarification and translation into scientific terms. Of particular importance is the correct identification of the species used, which can be very difficult due to a lack of, or poor quality, illustrations as well as language difficulties. However, data on the part used, time of collection, methods of preparation, formulation and application are also necessary as they all affect the nature and amount of any biologically active compounds. Any restrictions on use due to time of year may be important, as they can indicate low levels (leading to inefficacy) or high levels (with concomitant risk of toxicity) of active compounds. Similarly, any types of individual excluded from treatment might indicate groups at risk due to age, gender or occupation.
Definition of the disease state in Western medical terms might also not be easy if the information is derived from a culture in which concepts of disease cause and symptoms are very different. In many records, the condition treated is described by a symptom that might be due to a number of disease states, e.g. a headache might be due to stress, tiredness, migraine attack or a brain tumour. Conversely, a particular disease state might be characterized by a number of symptoms, all of which have to be addressed when searching for possible leads to treating that illness. Thus, as an example, when searching an inventory of plants with a view to selecting those used for diabetes, those used for treating excess urination, weakness and ulcers should be considered, especially if diabetes is not recognized as a distinct illness diagnosed by sweet-tasting urine. Unfortunately, these factors are often ignored in current research, when a statement that ‘plant species X is used to treat illness Y by people living in Z’ is considered to provide adequate ethnopharmacological information. Such vague statements do not take into account all the possible sources of variation of biological activity that must be considered before any investigation proceeds.
SCIENTIFIC INVESTIGATION
Extraction
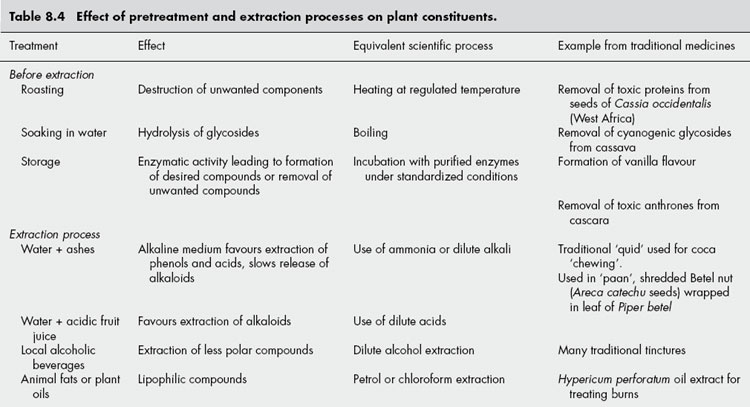
The extract used for testing should approximate as closely as possible that obtained by the traditional process used. Much research that has been published on the chemistry and activity of medicinal species is not very relevant to the traditional uses because it has concentrated on extracts made with non-polar solvents, such as ether or chloroform, whereas polar solvents are most commonly used. In many cases these will be simple extractions with hot water but a variety of other solvents can be used, as well as various additives or treatment of the material before use (see Table 8.4). In most instances, however, it is likely that fairly polar compounds will be extracted, although the solubility of less polar substances might be elevated considerably due to solubilizing compounds, e.g. saponins, also being present. Thus, an aqueous extract of the antimalarial plant, Artemisia annua, contains appreciable levels of the major antimalarial sesquiterpene artemisinin, which on its own has very low solubility in water.
Tests for activity
In most instances of modern drug discovery carried out by industrial and academic research groups, a particular bioassay, or series of in-vitro bioassays, designed on the basis of the biochemistry or molecular biology of the disease, is used to test extracts. In these situations, ethnopharmacology has little relevance to the tests used except that it provides a number of screening samples selected on the basis of their traditional use for the disease in question. However, this approach is valuable in selecting plants for further investigation from a list of those with a local reputation of treating serious diseases and this has been applied in screening programmes to detect antimalarial, antituberculosis and antidiabetic activity. These are not necessarily aimed at providing new lead compounds for ‘conventional’ drugs but have the goal of providing a scientific basis for the more effective use of extracts and mixtures. The Global Initiative for Traditional Systems (GIFTS)of Health is one example. It arose from academia and cooperates with the Tropical Disease Research programme of the World Health Organization (WHO) in finding new antimalarials in a collaborative network of research, government and community organizations named RITAM, the Research Initiative on Traditional Antimalarial Methods.
In spite of the common use of in-vitro bioassays, ethnopharmacological research can adopt a different approach when a particular biological effect of the traditional medicine or poison has been noted but the causes are not known. This is often the case when historical data are consulted and ailments are described in terms of their symptoms rather than underlying causes (see above). The biological effect might be essentially toxicological, e.g. use of poisoned arrows, and so it is important to seek to ascertain the basis of the toxic effect.
The best type of test to verify a reputed activity (and any toxicity) is a well-designed clinical trial, but this does not lend itself to bioassay-guided fractionation! It has been argued that long-term use of a material in traditional medicine is a good indicator of therapeutic efficacy but many are cautious about making such claims, preferring the suggestion that a long history of use is more an indicator of lack of obvious toxicity. In-vivo animal models of disease states are the next-best approach but expense and ethical considerations preclude this type of experiment in many countries, particularly for a fractionation process.
Most test systems for biological activity therefore utilize in-vitro systems using animal tissue, cultured cells, cloned receptors or enzyme systems. Many tests have been developed in recent years, and these offer the opportunity to carry out large numbers of tests using small amounts of material in a short time and are, therefore, well-suited to bioassay-guided fractionation. To be of most value, the range of tests chosen should be closely related to the possible underlying causes of the disease, e.g. tests for the efficacy of a preparation for an inflammatory disease such as arthritis should encompass key mechanisms associated with the formation of the various mediators involved, such as the lipoxygenases and cyclooxygenases involved in eicosanoid synthesis, histamine antagonists, secondary messenger systems such as the cytokine NFκB, as well as more general oxidation processes involving free radical damage. The advantages and disadvantages of in-vitro testing have been summarized in a paper presented at a recent meeting of the International Society for Ethnopharmacology (Houghton et al., J. Ethnopharmacol., 2007 110: 391–400).
It should be noted that biological testing for the traditional use might reveal a different, but nevertheless interesting, activity. Such was the case in the discovery of the anticancer compounds from Catharanthus roseus, a plant originally investigated because of its reputation in Jamaica as a treatment for diabetes. Deaths of animals treated with the extract were traced to dramatic reductions in leucocyte count, and it was from this that the application to treatment of leukaemic cancers was made.
Chemical examination
Chemical examination should be linked with tests for biological activity and it is probably only a happy accident of history that the many alkaloidal drugs were developed from traditional medicines, without the need for bioassay-guided fractionation, because the alkaloids were present in fairly high amounts and they were relatively easy to obtain in a purified state. For many other traditional medicines, where activity is not due to alkaloids, it has been much more difficult to separate the actives from all the other compounds. Chemotaxonomic considerations can often provide a reasoned guess to the nature of the active components and thus a short cut to their isolation. Thus, insecticidal or anti-inflammatory activity noted in a member of the Asteraceae could be ascribed to the sesquiterpene lactones that are present in many members of this family.
The presence of common classes of naturally occurring compounds can be screened by the use of appropriate chromogenic reagents after separation using thin-layer chromatography or by more sophisticated techniques, such as gas chromatography or liquid chromatography linked with mass spectrometry. These techniques are also valuable in dereplication, the process by which known active compounds present in the extract are detected, and so time is not wasted in a long bioassay-guided process that culminates in the ‘discovery’ of a well-known compound.
SOME MODERN EXAMPLES OF DRUG DISCOVERY BASED ON THE ETHNOPHARMACOLOGICAL APPROACH
SINGLE COMPOUNDS
Although the list of existing drugs introduced as a result of ethnopharmacological leads is impressive, some newer interesting examples of compounds arising from this approach have appeared in recent years, including galantamine and artemisinin (see Table 8.1). Others, which have attracted considerable research interest, are described below.
Prostratin
An ethnobotanical survey of Samoa carried out by the American Paul Cox in the late 1980s revealed the traditional use of a hot-water infusion of the stem wood of Homalanthus nutans for the viral disease yellow fever. Work carried out in conjunction with the National Cancer Institute in USA resulted in the isolation of a phorbol named prostratin, which was found to be effective against the killing of human host cells by HIV. Prostratin appeared to stimulate protein kinase C, which was a novel mode of action for an anti-HIV drug. Although extensive trials were commenced, prostratin has since been dropped from the anti-HIV drug development programme due to some toxic effects.
Flavopiridol
The bark of the Indian tree Dysoxylum malabaricum (Meliaceae) was traditionally used to treat arthritis and investigations into the related D. binectariferum provided rohitukine, a chromone alkaloid that exhibited anti-inflammatory activity in laboratory animals. Studies into the mechanism of action found that it was different from many other natural anti-inflammatory compounds in that it inhibited tyrosine kinase. A series of analogous compounds was developed to optimize the effect and the flavonoid derivative flavopiridol was shown to have superior activity. As numerous oncogenes encode for the production of protein with such kinase activity, inhibition might decrease tumour growth and this was found to be the case with flavopiridol, which is now in advanced stages of clinical testing as an anticancer agent.
Huperzine A
A tea from Huperzia serrata, a club moss, was a traditional drink for elderly people in several areas of China. Over the last twenty years, huperzine A, an alkaloid with cholinesterase inhibitory properties, has been isolated and shown to have significant beneficial effects on memory in patients. As memory appears to be impaired in patients with low levels of acetylcholine (ACh) in the brain, inhibition of the enzyme that degrades ACh will have the net effect of raising ACh levels and thereby improving memory. Huperzine A is in clinical use in China for treatment of elderly patients showing loss of memory and clinical trials in other countries are being planned.
PURIFIED AND STANDARDIZED EXTRACTS
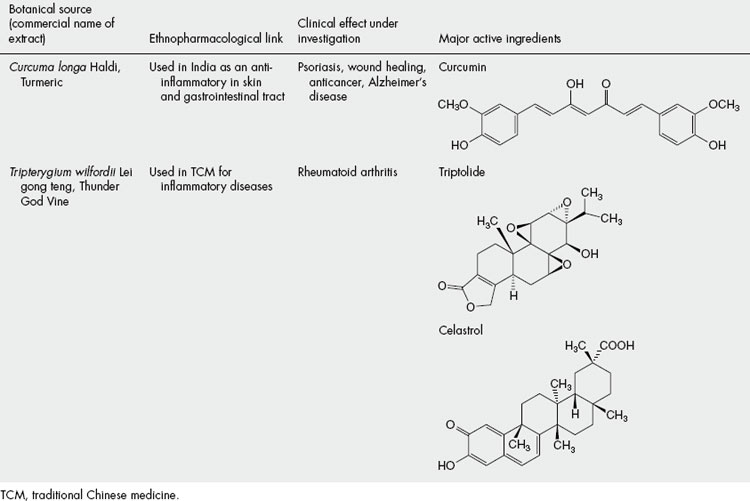
There has been a renaissance of interest in using mixtures of compounds rather than single chemical entities in orthodox therapy (see Schmidt et al., Nature Chemical Biology, 2007 3: 360–366); this has always been the approach in herbal systems of medicine. The acceptance of such products is still in its infancy as regards Western regulatory procedures but is at an advanced stage in some of the emerging economies such as India and China. Even in Western countries such as USA and UK, funds are being released by government agencies, non-profit-making funding organizations and industry for clinical trials of characterized and standardized extracts, practically all of them having an ethnopharmacological basis and many are from Asia. Some of the interesting products being investigated are listed in Table 8.5 but it should be noted that, in some cases, the compounds thought to be most active are also being investigated for use as single chemical drugs or as lead compounds for development of the same.
THE VALUE OF THE ETHNOPHARMACOLOGICAL APPROACH
EFFICACY AND SAFETY
The argument most often used to support the ethnopharmacological approach to drug discovery is the fact that a plant material has been used for generations in a particular culture. Lack of technological sophistication is not synonymous with a lack of appreciation of efficacy or safety and so it is likely that there would be no serious adverse effects associated with the regular use of the material. In many cases it has been shown that potential harm is minimized through a selected method of preparation of the material, by its administration being restricted to trained personnel (most commonly the ‘medicine men (or women)’ of the community), or by its being used in special ways, particularly by the addition of other materials that might decrease the toxicity by countering unwanted pharmacological effects or by altering the bioavailability or metabolism of the material. The addition of alkaline ash to coca leaves in the traditional method of ‘chewing’ them is a good example of this. The high pH favours the less water-soluble form of cocaine, so affecting its release into the saliva and uptake into the bloodstream, and possibly reducing the addictive potential.
ECONOMIC AND SOCIOPOLITICAL CONSIDERATIONS
Although not closely related to the process of ‘drug discovery’ by the industrially developed countries, the scientific validation of a local remedy from a developing country can encourage its use and introduction into therapy in its original habitat, or its growth and adoption as therapy in areas with similar growing conditions. Cultivation and production of extracts from such plants might be a substitute for more expensive Western drugs and medicines, especially in countries where healthcare resources are stretched.
A notable example of this is Plantas do Nordeste, a collaboration between the Royal Botanic Gardens Kew, UK, and a consortium of scientists and agriculturists in the impoverished region of north-eastern Brazil. The project has evaluated some of the local medicinal plants and promoted the cultivation of them across the region as an aspect of healthcare, together with the training of personnel in their use.
The possible validation of their traditional remedies by the scientific ethnopharmacological approach is also valuable in helping small ethnic groups retain or recover their sense of identity and value, especially when threatened by globalization and cultural imperialism by more politically or commercially powerful groups.
PROBLEMS WITH THE ETHNOPHARMACOLOGICAL APPROACH
RELIABILITY OF INFORMATION
Some of the difficulties of obtaining accurate and reliable information have been discussed above. It should also be noted that the use of a plant might not be due to rational observation or experimental evidence, but instead be based on a subjective consideration. Probably the most notorious example of an irrational approach is the ‘doctrine of signatures’ whereby some sensory aspect of the plant was thought to indicate its medicinal usefulness, e.g. a plant with yellow juice might be considered for treating jaundice, one with heart-shaped leaves for cardiac complaints, etc. Although, in some cases, relevant activity has been found for plants identified in this way, these are usually the exceptions rather than the rule.
BIOLOGICAL VARIATION
On a scientific level, the chief concerns are the difficulty of knowing the chemical composition of a plant or its extract due to its complexity and also due to the variation caused by genetic or environmental factors. This complicates elucidation of the active compounds and also makes the activity of different batches less reliable. Indigenous knowledge often has subtle ways of distinguishing ‘best’ plant species or varieties and only thorough investigation will uncover the criteria used.
LOSS OF SPECIES
It is estimated that 25% of the flowering plant species of the world might become extinct within the first 25 years of the twenty-first century. Climate change, increasing population making demands on land and resources, as well as commercial exploitation of the environment all play a part in this and result in a loss of habitats. It is not unusual to record the presence of an interesting species in one locality only to return a few months later to find that the whole area has been cleared for some commercial activity. Although many ethnic groups in all parts of the world are affected, and most have a rich fund of knowledge about the medicinal uses of local organisms, it is probably those small groups in the centres of biodiversity, especially tropical rainforests, who are most vulnerable to irretrievable loss of species. Although the imminent extinction or increasing rarity of species are often promoted as a loss of potential new drugs for the developed world, it should be remembered that the local inhabitants could lose many of their basic affordable or available medicines.
In light of this, many medicinally important species have been subjected to some form of cultivation and, in several places, gardens of medicinal plants, formerly collected from the wild, are now being cultivated to provide local healers with species that they formerly collected from the wild.
LOSS OF KNOWLEDGE
The current opportunity to exploit ethnopharmacology might not last long. Whereas much concern has been quite rightly expressed over the disappearance of the world’s biodiversity and habitats, less attention has been paid to the threat to the immense wealth of knowledge about the medicinal uses of the local flora that exists amongst threatened ethnic groups. The irretrievable loss of large amounts of this knowledge is possible, due not only to the extinction of plant species due to climate change, urban expansion and destruction of habitat, but also to the breakdown in traditional societal structures of the transmission of such knowledge. The threat is especially acute in cultures in which information is oral rather than written, and is exacerbated by urban drift, particularly of young people, neglect of local materials, adoption of Western globalized products and health structures, and by war, famine and other causes of migration and consequent disruption of traditional society.
THE NEED FOR DEREPLICATION
Extracts from plants can show an interesting activity and, conventionally, this is followed by laborious, prolonged, bioassay-guided fractionation to isolate the compounds responsible. However, such considerable effort might result in the isolation of known compounds, or the activity might be found to be due to substances, such as polyphenols, which have a general inhibitory activity on many enzymes. This problem might be overcome by the use of dereplication procedures, whereby suspected known active compound types are removed by fractionation and purification procedures. Alternatively, active extracts and fractions can be examined by techniques, such as chromatography linked to mass spectrometry, which can afford substantial amounts of information about each component and data from the peaks obtained can be screened against a data library of known compounds.
INTELLECTUAL PROPERTY RIGHTS (IPR) ISSUES
The commercial aspects of the ethnopharmacological approach have aroused much controversy in recent years with regard to the intellectual property rights of the groups having the knowledge. Several international agreements, particularly the Rio Declaration and Convention of Biological Diversity (CBD) of 1992, have concentrated on sharing with the source countries the benefits and profits that might arise from the development of new drugs based on ethnopharmacological leads. The effect that such measures might have on their patent rights and returns from investment have been considered closely by pharmaceutical companies and some have decided not to take the risks involved. Some other companies, however, have been willing to sign agreements aimed at sharing profits directly or making substantial payments to countries in exchange for access to their flora for testing purposes.
CONCLUSION
The study of plants used in traditional medicine has received new impetus with the introduction of a wide variety of small-scale bioassay methods and improved methods for fractionation, isolation and characterization of compounds. In some cases, individual compounds responsible for the reputed activity have been isolated and used as lead molecules. However, it is also apparent that, in many cases, the observed effects seen in patients or animals are due to a mixture of constituents, perhaps each contributing a different biological effect to the overall activity. Thus it is likely that not only will traditional medicines continue to provide new molecules for drug discovery, but that they might also form the basis for the wider acceptance of crude extracts, in a standardized form, as another type of medicine in orthodox practice.
Balick MJ, Cox PA. Plants, people and culture: the science of ethnobotany. London: Freeman, 1997.
Chadwick DJ, Marsh J, editors. Ethnobotany and the search for new drugs. Ciba Foundation Symposium 185. Chichester, UK: Wiley, 1994.
Heinrich M, Barnes J, Gibbons S, Williamson EM. Traditional systems of herbal medicine. In: Fundamentals of pharmacognosy and phytotherapy. Edinburgh: Churchill Livingstone; 2004:169-183.
Journal of Ethnopharmacology. Perspectives of ethnopharmacology. 2005;100:1-2. issues
Lewis WH. Ethnobotany in new drug discovery – a review. Economic Botany. 2003;57:126-134.
Phillipson JD, Anderson LA. Ethnopharmacology and Western medicine. Journal of Ethnopharmacology. 1989;25:61.
Pieroni A, Price LL. Eating and healing: traditional food as medicine. Binghamtown, NY: Haworth Medical Press, 2006.
Prendergast HDV, Etkin NL, Harris Houghton PJ. Plants for food and medicine. Kew, UK: Royal Botanic Gardens, 1998.
Proceedings of the First International Congress of Ethnopharmacology, Strasbourg 1990. Journal of Ethnopharmacology. 1992;32:1-235
Proceedings of the Second International Congress of Ethnopharmacology, Uppsala 1992. Journal of Ethnopharmacology. 1993;38:89-225.