Chapter 32 The plant nutraceuticals
A number of plant nutraceuticals are common food constituents, and extracts of many others are used as nutraceuticals.
There are a number of definitions of nutraceuticals, but the first and most straightforward is that coined by De Felice, of the Foundation of Innovation in Medicine, who defined a ‘nutraceutical’ as a ‘food, or parts of a food, that provide medical or health benefits, including the prevention and treatment of disease’.
Nutraceuticals are rarely legally classed as medicines, but instances exist in certain countries for particular entities, for example coenzyme Q10 in Japan and melatonin in the UK. This consequent lack of regulation for most nutraceuticals has resulted in a number of poor quality products being available on the market.
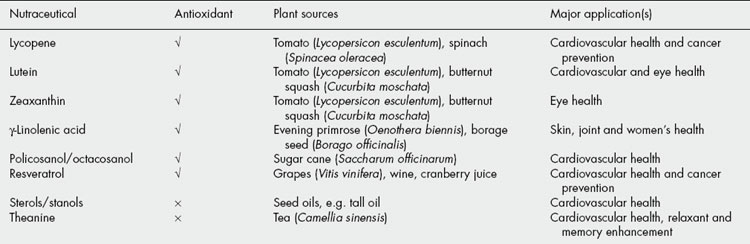
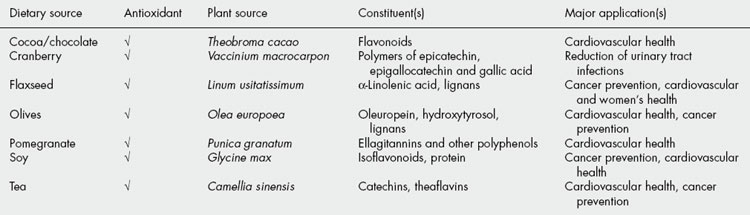
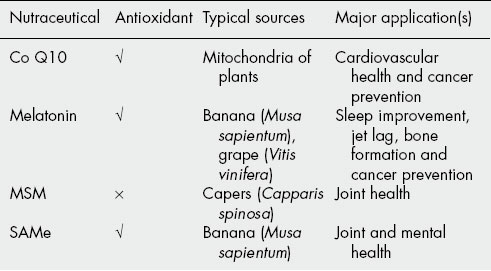
There are a number of sources of nutraceuticals, including basic human and mammalian metabolites, dietary components of plant and animal origin, synthetic constituents and plant secondary metabolites; increasingly, they are also produced by microbial fermentation. Arguably the greatest number are derived from plants and are used either as single purified components, such as resveratrol, purified multi-component products, such as pycnogenol, or whole plant foods, such as flaxseed. The most researched nutraceuticals of plant origin are those derived from soy and tea, but large numbers of scientific and medical publications relate to the constituents of grapes and wine, and also the many plants rich in polyphenolic components. Table 32.1 lists plant sources and therapeutic activities of a number of commercially available single-component nutraceuticals, which often occur in a number of plants. Various purified multi-component nutraceuticals are also obtained from specific plants (Table 32.2). Those from grape, soy and tea could realistically be obtained from the diet. Increasingly, a number of foods are being promoted as sources of nutraceuticals specifically for consumers who prefer eating a healthy diet instead of taking supplements; Table 32.3 depicts a wide variety of such products. The last group of nutraceuticals occurs in the plant kingdom either widely, such as coenzyme Q10 and S-adenosylmethionine (SAMe), or only in a few specific plants but at insubstantial levels, and are therefore not suitable for realistic incorporation in the diet. These latter nutraceuticals are often produced by chemical or biotechnological synthesis (Table 32.4).

The range of therapeutic applications is wide, encompassing many areas in which conventional pharmaceuticals treat only the symptoms of the disease state. A number of these nutraceuticals have been shown to treat the underlying cause of the illness, e.g. α-linolenic acid. As a consequence of this, many nutraceutical manufacturers and pharmaceutical companies are increasingly investigating the possibility of formulating and marketing plant based nutraceuticals.
Many of the nutraceuticals owe their activities to antioxidant activity (activity is highlighted in Tables 32.1-32.4), but this may not be the full story. It has been claimed that many also have other activities, including enhancement or inhibition of Phase I and II metabolizing enzymes, and modulation of DNA repair.
In addition to the increasing number of clinical trials being published to support the use of plant nutraceuticals, evidence is accumulating regarding synergistic interactions, adverse effects, and quality of commercially available single and multicomponent nutraceuticals.
Carotenoids
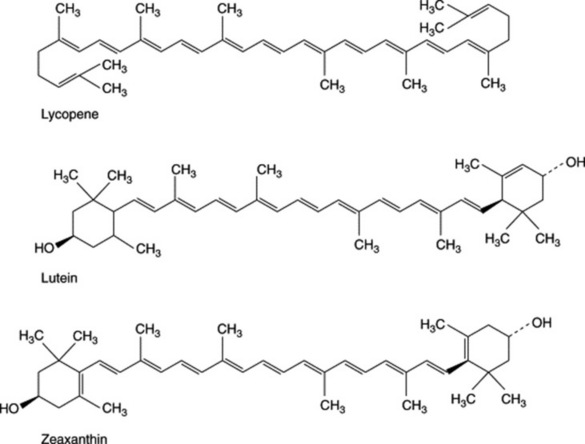
A number of plant-derived carotenoids such as lycopene, lutein and zeaxanthin are currently commercially available as single entities and have wide-ranging activities; their structures are shown in Fig. 32.1. Lycopene is present in red fruits and vegetables, particularly tomatoes, and lutein is present in spinach, peas and watercress. Foods that are yellow—maize, orange juice, honeydew melon and orange pepper—are also good sources of lutein.
The recommended daily intake of lycopene is 35 mg, but a number of Western societies consume from 5–25 mg, with processed products accounting for at least 50% of the total intake, therefore supplementation is often advised. A wide range of lycopene levels has been reported in tomatoes (1–15 mg/100 g), and lutein has been found to occur at 0.08 mg/100 g in tomatoes and 2.38 mg/100 g in butter squash. The mixture of lutein and zeaxanthin stereoisomers have also been reported at levels of 40 mg/100 g in kale and 12 mg/100 g in spinach. Zeaxanthin also co-occurs with lutein at 0.28 mg/100 g in butter squash.
Lycopene
Lycopene has antioxidant and free-radical scavenging activity, and serum levels have been shown to be protective against myocardial infarction (MI). Many researchers believe that these mechanisms are most likely to account for its beneficial effects in cancers. Reactive oxygen species (ROS) are the main source of oxidative damage that can generate structural alterations in DNA and decrease DNA repair by damaging essential proteins, and ultimately cause cancer. A number of trials have shown levels of cancer of the oral cavity, pharynx, oesophagus and colorectum, decreased with increasing levels of lycopene intake. An association with lycopene intake is less likely in ovarian and breast cancers.
Epidemiological literature has shown that diets rich in tomatoes are associated with lower lung cancer rates. The presence of lycopene in the human lung following lycopene supplementation has been demonstrated, and it is believed that an increased intake of lycopene might provide an additional level of protection against oxidative damage. A high intake of tomato products is associated with a 35% lower risk of total prostate cancer, and a 53% lowered risk of advanced prostate cancer. A decline in protective effect of a range of tomato products have been shown to correspond to a decline in plasma lycopene levels.
Overall, preliminary evidence suggests that lycopene intake, and serum lycopene levels are associated with a reduced risk of developing cancer, most notably prostate and lung cancer.
Lutein
Plasma lutein concentration is believed to be inversely related to heart disease, and an inverse relationship has been reported between serum lutein levels and progression of intima-media thickness in carotid arteries.
Lutein and zeaxanthin have been implicated in maintenance of eye health and they selectively accumulate in the retina of mammals, which gives the macula lutea its yellow colour, and makes up a screening pigment known as the macular pigment. This pigment may have both acute and chronic effects on visual performance. Lutein and zeaxanthin are carried in human serum, mainly by high-density lipoproteins (HDL). Lutein and zeaxanthin are both antioxidant and are able to filter blue light. There is evidence that a diet high in carotenoids is associated with a lower risk of age-related macular degeneration (AMD). One case control study found a 43% lower risk of AMD in individuals consuming the highest levels of carotenoids (especially lutein and zeaxanthin) compared with those consuming the least. A strong inverse association was found for consumption of spinach containing high levels.
γ-Linolenic acid
γ-Linolenic acid occurs in Oenothera spp., notably O. biennis, at levels of 7–9 % in the fixed oil. Borage oil yields 25%, but it is not widely found elsewhere in substantial amounts, although it is also present in starflower oil and blackcurrant seed oil. γ-Linolenic acid is not usually purified and the complete oil is used for oral supplementation.
It is an essential intermediate between linoleic acid and dihomogammalinolenic acid (DGLA), and thereafter prostaglandins, thromboxanes and leukotrienes. Disruption of its production by the action of delta-6-desaturase on linoleic acid is thought to be responsible for a number of human disease states. Atopic eczema and premenstrual syndrome are two of the most popular applications. Metabolism of γ-linolenic acid to DGLA in healthy individuals may reduce inflammation via competitive inhibition of leukotrienes and 2-series prostaglandins. Trials using 1.4 or 2.8 g/daily of γ-linolenic acid for up to 12 months have shown progressive improvements in symptoms of rheumatoid arthritis.
Policosanol/octacosanol
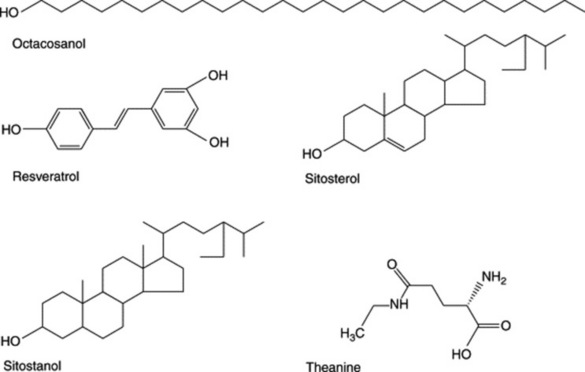
Policosanol is found in sugar cane waste and the leaves of alfalfa and wheat, and is also present in wheat germ. The major component, octacosanol is present at levels of 67% in material obtained from sugar cane waste and wheat germ.
Policosanol was developed in Cuba, and the majority of the reseach (over 60 clinical trials) was carried out there. Most studies confirm effective lipid-lowering effects at doses of 10–20 mg/day. Typical improvements include a lowering of low-density lipoprotein-cholesterol (LDL-C) by 18–26%, total cholesterol by 13–17%, and an increase in HDL-C by 15–28%. Comparison of policosanol (10 mg) with lovastatin (20 mg) showed similar effects on lipid levels, but none of the statin side effects were observed with policosanol. Policosanol is also thought to act by inhibition of cholesterol biosynthesis, but direct inhibition of HMG-CoA reductase as seen with the statins is not the mode of action.
Antiplatelet activity also occurs, at 20% of the dose as with aspirin.
Resveratrol
Resveratrol is found in the leaves, skins and petals of Vitis vinifera, and also wines and grape juice, and levels are elevated when the vine is infected with the fungus, Botrytis cinerea. Red wines contain increased levels due to extended time in contact with the skins. A number of other stilbene derivatives are also found in grape products. Resveratrol is also present in other plant products, such as peanut butter. Wide-ranging levels of resveratrol have been found in wines from different varieties of grapes and different geographical sources; 0.3–4.7 mg/l (French Barolo, French Chateauneuf). Concommitant levels of catechin, 23–136 mg/l (French Barolo, French Burgundy) and epicatechin, 17–64 mg/l (French Barolo, French Beaujolais) are also present.
Research in animals and humans has demonstrated a range of biological activities, including antioxidant activity, inhibition of platelet aggregation and modulation of hepatic apolipoprotein and lipid synthesis. Red wine is the major dietary source of resveratrol, and it is implicated in risk reduction for a number of cancers, including upper digestive tract, lung and colon cancers. Resveratrol inhibits metabolic activation of carcinogens, induces apoptosis and is anti-inflammatory.
Sterols/stanols
These both exist in all plants, and the major sources are the vegetable oils. Cholesterol absorption ranges from 35 to 70%, but sitosterol and camposterol, which are the major plant sterols, are both poorly absorbed in the intestine (0.4–4%), and the stanols even less so (0.02–0.3%). They are thought to act by inhibition of cholesterol absorption. Plant sterols and stanols are being actively used for reduction in blood cholesterol levels, and the majority of these investigations have involved sterol and stanol enrichment of the subjects’ diet, and a positive association has been found for cholesterol reduction. The effects of a plant-sterol-enriched reduced-fat spread have been monitored over 5 weeks, with patients receiving either 1.1 and 2.2 g daily of sterol and a 40% reduced-fat spread. Total cholesterol and LDL-C values were reduced by 5.2% and 6.6%, and 7.6% and 8.1%, respectively, at these two levels of supplementation. A later comparison of trials using a number of sterols and stanols in fortified diets, revealed that effective doses ranged from 1.5 to 3.0 g daily, and total cholesterol reduction was of the order of 10%, while LDL-C reductions were between 8% and 15%. The mode of action was thought to be due to interference with the solubilization of cholesterol in intestinal micelles, consequently reducing cholesterol absorption. However, other mechanisms have also been postulated. Tablets and capsules containing sterols and stanols are commercially available, but there is no evidence that these have the same beneficial effects as sterol- and stanol-enriched spreads.
Theanine
Theanine is a non-protein amino acid present in tea, and other species of the genus Camellia. It is the major amino acid in tea, and constitutes 1–2% of the dry weight of tea. Theanine has been shown to possess three potentially useful properties: namely, relaxant, hypotensive activity and memory enhancement.
Oral supplementation with 50–200 mg theanine once weekly, has been reported to increase production of α-brain waves, which causes a state of relaxed alertness. In addition, theanine shows the ability to modulate moods, which is possibly linked to its effects on serotonin, dopamine and other neurotransmitters.
It has been postulated that the reduction in blood pressure may be responsible for mental calming. A reduction in serotonin, and also dopamine, may have an effect on memory and learning ability. It has been reported that doses of theanine up to 2000 mg/kg produced significant reduction in blood pressure in spontaneously hypertensive rats.
Theanine is increasingly being incorporated into a range of convenience foods, as well as pharmaceutical formulations. Confectionary containing 72 mg has been reported to cause relaxation, as indicated by increased generation of α-waves. Whole tea obviously contains both theanine and the catechins (see later), therefore is responsible for a range of activities, often not assigned to specific components.
Long-term social tea drinking appears to have no side effects apart from the effects of the caffeine content, therefore it may be assumed that realistic levels of theanine consumption comparable to those obtained from tea drinking should be safe. The structures of a number of single component nutraceuticals are shown in Fig. 32.2.
GSPE
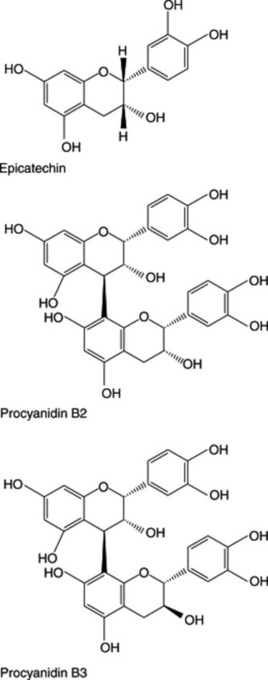
Grapeseed proanthocyanidin extract (GSPE) constituents are based on either catechin or epicatechin, and monomers, dimers, trimers and other oligomers. The procyanidins are polymers of catechin or epicatechin monomers, composed of 2–12 monomers. Dimeric procyanidins named procyanidin B1 (PCB1), B2, B3 and B4, depending on the configuration of catechin and epicatechin subunits, are present. A number of these catechin derivatives are present as their gallates in addition to the free form. The structures of epicatechin and procyanidin B2 are shown in Fig. 32.3.
Levels of proanthocyanidins have been estimated in a number of wines, Greek red seed extracts have been quantified, PCB1 17 mg/100 g, PCB2 16 mg/100 g, catechin 191 mg/100 g, and epicatechin 100 mg/100 g, and white seed extracts found to contain marginally less. Japanese grape extracts have been found to contain much lower levels.
GSPE is a powerful antioxidant, with higher activity than vitamins C and E, and it is believed that this is responsible for its cardioprotective activity against cardiovascular disease and circulation defects. Most research has shown that GSPE causes a 60–90% reduction in oxidation of LDL-C, and consequently a reduction in atherosclerosis. GSPE is widely used for treatment of vascular disorders such as varicose veins, venous insufficiency and microvascular problems in Europe.
Pycnogenol
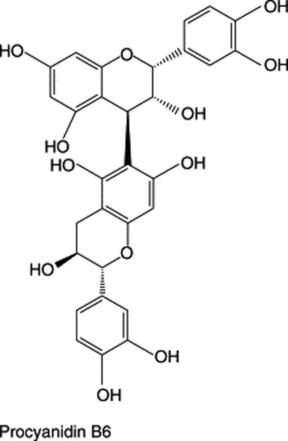
Pycnogenol is the registered name of a standardized extract of the bark of the French maritime pine, Pinus pinaster Aiton, subspecies Atlantica des Villar, containing mainly phenolic acids and procyanidins. A number of phenolic acids that are derivatives of benzoic acid, vanillic acid or gallic acid, or cinnamic acid derivatives, exist both free and in combination with glucose. The major procyanidin dimers include B1, consisting of catechin and epicatechin, and B3, consisting of two catechin monomers and lower concentrations of the equivalent dimers. Monomeric catechin, free taxifolin and its glucoside, as well as vanillin are also present. The structures of procyanidin B3 and B6 are shown in Fig. 32.3.
Historically, pine bark has been used for treating inflammatory diseases, which gives some credence to the use of pycnogenol. A range of cardiovascular effects has also been reported, including vasorelaxant effects, ability to inhibit angiotensin-converting enzyme (ACE) and increase in the microcirculation by increasing capillary resistance.
Pycnogenol, is a highly potent antioxidant with a high affinity for collagen. Larger procyanidins bind to proteins of damaged blood vessels to lower capillary permeability and reduce basement membrane leakage. Pycnogenol increases production of nitric oxide, which may be impaired in certain disease states, such as diabetes, by stimulating endothelial nitric oxide synthetase, and the nitric oxide produced relaxes constricted blood vessels. Pycnogenol reduces leukocyte-mediated degeneration of retinal capillaries, and has also been shown to prevent increased platelet activity without increasing bleeding time.
Adults taking pycnogenol have been reported to have significantly reduced serum leukotrienes. A study conducted in children with mild-to-moderate asthma using the supplement for 3 months showed significantly more improvement in pulmonary functions and asthma symptoms and found that they could reduce their use of prescription medication.
Soy isoflavones
The major soy consumers live in East Asia, and their foods include a wide variety of different forms, some examples being whole soybeans, soy sauce, tofu (soybean curd), tempeh, soymilk, miso (fermented soybean paste) and natto (fermented soybeans).
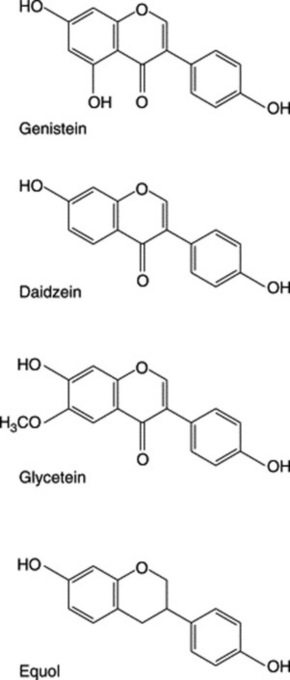
The major isoflavones present in soybeans in order of concentration are genistein, daidzein, and glycitein, and they occur as β-glycosides. The isoflavone content varies between 0.4 and 2.4 mg/g, depending on growing conditions and crop variety. Processed products contain a much lower isoflavone content due to manufacturing methods, such as alcohol washing of soy concentrates. Genistein occurs in the range of 1–150 mg/100 g in the raw soybean, and is converted to its β-glycoside genistin in biological fluids. Daidzein and its β-glycoside daidzin occur in lower concentrations, at levels of 0.5–91 mg/100 g. Glycitin and its aglycone glycitein, are also present and only found in relatively small amounts.
Daidzein is metabolized by human intestinal flora to give equol in 30–50% of the population. Babies are unable to produce equol, and the ability is developed in susceptible individuals. Equol is powerfully oestrogenic, more so than estradiol, and is therefore probably the major active component in hormone-dependent conditions. Fig. 32.4 shows the structures of the major soy isoflavones and equol.
In 1999, the FDA approved manufacturers of soy foods to state the health claim that ‘consumption of at least 25g of soy protein per day may be beneficial to a reduced risk of developing CHD’. It has been claimed that much of the support for this decision was obtained from a meta-analysis published in 1999. The results of this analysis showed that consumption of soy protein instead of animal protein reduced LDL-C levels by 7–24%, depending on initial cholesterol levels. However, it was not clear whether the benefits reported were due to the soy protein or to the constituent isoflavones. A more recent meta-analysis in 2005 reported that soy protein containing isoflavones significantly reduced total cholesterol, LDL-C and triglycerides, while increasing HDL-C. Soy has been reported to improve vascular function and to have beneficial effects in preventing onset and development of atherosclerosis.
Low levels of isoflavones (60–100 mg) taken for up to 12 weeks have been reported to increase memory, pattern recognition and mental flexibility. Improvements in both young males and females, in both short- and long-term memory, and also in mental flexibility, have been reported.
Epidemiological data suggest that consumption of soy isoflavones at typical Chinese or Japanese dietary levels should potentially reduce the risk of developing cancer. Japanese adults are thought to consume around 30–40 mg daily, but the quantity of soy products that need to be consumed to reach these levels of intake varies considerably depending on the dietary form of the soy. The mortality from clinically diagnosed prostate cancer has been shown to be lower in countries with high soy consumption. The death rate of men dying from prostate cancer in Japan is about 25% the level found in the US, and in Japanese men with prostate cancer, many tumours are muchsmaller on average. However, Asian emigrants who move to the US and change their dietary habits show a marked increase in the risk of developing prostate or breast cancer, reaching levels comparable to those found in indigenous inhabitants. This is likely to be a result of higher fat and much lower soy isoflavone content of the diet, suggesting that the protective effect found in inhabitants of Asia is diet related. Also, women who had consumed tofu during adolescence were less likely to develop both premenopausal and postmenopoausal breast cancer as adults.
Recent research has identified a further two bioactive constituents, the Bowman–Birk protease inhibitor, and lunasin, a unique 43-amino-acid peptide. Both of these have anticancer activity and may be partially responsible for the beneficial effects of soy consumption.
Soy isoflavones, up to 100 mg per day, may be a safe and effective alternative therapy for many menopausal symptoms. They are thought to be promising as supplements in preventing and treating postmenopausal osteoporosis, due to their oestrogenic activity, and consequently as potential replacements for estrogen deficiency. Most studies with soy isoflavones in osteoporosis have therefore restricted themselves to female subjects during or after the menopause. Epidemiological studies have shown strong evidence that soy isoflavones have a positive effect on bone mineral density (BMD). Far lower rates of osteoporosis and fractures have been observed in oriental women than in their Western counterparts. Over 4.5 years, the level of consumption of soy protein and isoflavones by Chinese women was found to be possibly associated with a reduction in bone fracture, particularly in the early years following menopause. Data from intervention studies are limited, and have shown contradicting results. Clinical trials in postmenopausal and perimenopausal women that have analysed bone mineral content and BMD have demonstrated that isoflavones can significantly increase BMD at the lumbar spine.
Whole soybean contains many constituents, as well as protein and isoflavonoids, so there is the possibility that unknown synergistic effects may be seen.
Studies with isoflavones in humans, suggest that doses ranging from 1 to 16 mg/kg body weight are reasonably safe, although higher doses are being recommended for prevention of bone loss in postmenopausal women. Genistein at high doses, such as 600 mg per day, has been shown in vitro to inhibit cell growth and induce apoptosis. In addition, some reproductive disturbances, such as uterotropic effects,have been reported in animals fed a diet rich in isoflavones or other phytoestrogens.
Tea catechins
Tea has been discussed previously (see section Alkaloids, Purine alkaloids), and is known to contain caffeine and a number of polyphenols. Black tea accounts for approximately 78% of the total tea consumed world wide, with green tea representing 20% and oolong tea accounting for less than 2%.
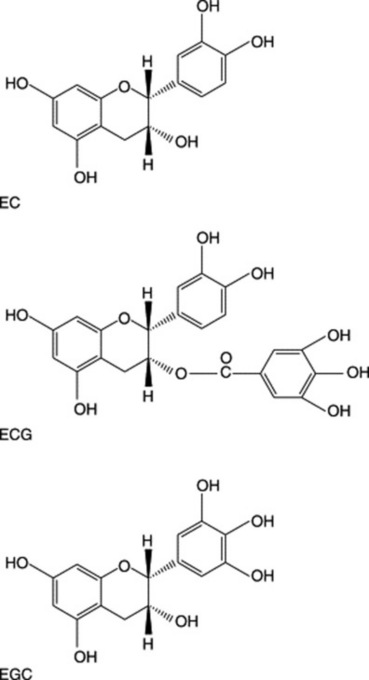
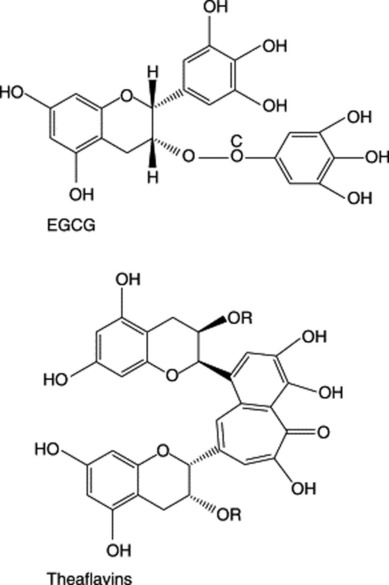
The polyphenols include catechins, quercetin, myricetin and kaempferol; these account for 30–42% of the dry weight of tea. Catechins are the main components and the four principal ones found in tea are (−)-epicatechin (EC), (−)-epicatechin gallate (ECG), (−)-epigallocatechin (EGC) and (−)-epigallocatechin gallate (EGCG). EGCG is the most abundant, accounting for 50–80% of the catechins. A typical brewed cup of green tea, approximately 240 ml, can contain up to 200 mg of EGCG. Fig. 32.5 shows the structures of typical tea constituents.
A number of epidemiological surveys have been carried out on the effects of tea consumption, initially with green tea but later with black and oolong teas. The major findings are decreased serum total-cholesterol and triglyceride, with an increase in HDL-C and reduction in the proportion of lipoprotein cholesterol and very-low-density lipoprotein cholesterol (VLDL-C). In particular, black tea consumption has positive effects on endothelial function, atherosclerosis of coronary arteries and hypertension. Subjects consuming 120 ml tea/day for a year have been shown to have a 46% lower risk than non-tea-drinkers.
Tea polyphenols are also thought to have antiplatelet, antithrombotic and anti-inflammatory activity, and thereby reduce the risk of congestive heart disease. Meta-analysis of 17 studies has shown that an increase in tea consumption of three cups/day is associated with an 11% reduction in incidence of myocardial infarction.
EGCG has been claimed to be the most important active constituent, although it is known to have low bioavailability. Studies in human lung cancer cell lines found ECG to be most active in inhibiting growth, followed by EGCG, then EGC, but EC was inactive. Theaflavin-3–3′-digallate appears to have similar activity to that of EGCG and therefore the inhibitory activity of black tea (containing theaflavin-3–3′-digallate) against the development of cancer may be due to the combination of catechins and theaflavins. Tea polyphenols have been proposed to act via a number of different mechanisms to exert their cancer chemopreventive effects.
Studies have shown that EGCG acts specifically on certain cancer cells by mechanisms such as induction of apoptosis, cell-cycle arrest and inhibition of cell growth, but that it does not cause these effects in normal cells. The inhibition of cell growth is thought to be caused by the involvement of tea polyphenols in the activation of genes, via signalling mechanisms.
Laboratory animals with lung cancer treated with black tea had a 19% incidence of tumours, compared with 47% in the control. Apparently contradictory results in Japanese patients have been published. The age of cancer onset in females was increased from 65.7 years, in those who drank less than three cups of green tea a day, to 74.4 years in those consuming over ten cups a day. The age of cancer onset in males was shown to increase from 63.3 years to 68.3 years. The smaller delay in age seen in males was thought to be attributable to the higher number of male smokers. However, the incidence of cancer increased in individuals consuming over ten cups of tea a day, over the age of 80 years. The increase in incidence was higher than in those who drank fewer cups of green tea.
Lung, oral and oesophageal cancers are particularly caused by cigarette smoking. The incidence of lung cancer in males in the US is twice that in Japan, even though the prevalence of smokers in Japan is nearly twice that of the US. This could be due to a number of other factors, including genetic and environmental factors. Green tea is consumed far more in Japan than in the US, a fact that has suggested the possible chemopreventive effects of tea against smoking-induced cancers.
Consumption of ten cups of green tea a day, providing approximately 3000–4000 mg of EGCG, has been shown to produce a chemopreventive effect, and it is possible that there is a dose–response relationship between consumption of tea and cancer prevention.
Cocoa/chocolate
The fresh seed of the cocoa plant, Theobroma cacao, contains epicatechol, leucoanthocyanins and anthocyanins, which are decomposed during processing (see Cocoa seed, Alkaloids). Chocolate, which is derived from the fermented seeds, contains 0.8 mg/g of catechin monomers and 4.6 mg/g procyanidins, the latter occurring at levels five to ten times greater than in cranberry juice. The content of catechin and epicatechin represents 10 mg/g. The structure of epicatechin is shown in Fig. 32.5. In vitro experiments have shown chocolate to inhibit LDL oxidation. Concentrations used are consistent with plasma epicatechin levels observed following consumption of realistic amounts of dark chocolate. The activity of chocolate in atherosclerosis might be due to its effects on improving endothelial function, which has been demonstrated in both healthy and impaired individuals. This could be causedby its antioxidant activity, but it is also able to modulate platelet activity, inhibiting platelet activation and reducing platelet function, and hence inflammation.
Cranberry
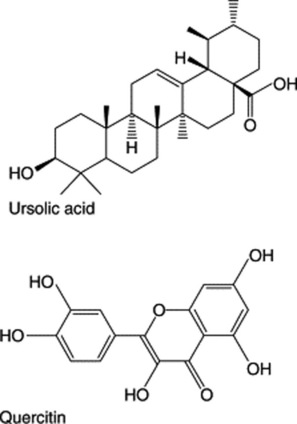
A number of polyphenols have been identified, including ursolic acid, benzoic acid and derivatives, quercitin and hydroxyl flavonol glycosides, such as quercitin glucoside and galactoside. Typical constituents are shown in Fig. 32.6. Cranberry also contains polymeric proanthocyanidins that are thought to be responsible for beneficial health effects, especially those relating to interference with microbial adhesion. Evidence is seen, particularly in the urinary tract, of Esherichia coli, and in the gastrointestinal tract of Helicobacter pylori. A large body of epidemiological and clinical evidence, and evidence of the mechanism of action of cranberry and its components, exists in the area of urinary tract infections (UTIs). Initial research suggested that the anti-adhesive effect on E. coli, with consumption of 300 ml/day of cranberry juice, reduced the risk of UTIs. The action of a large-molecular-weight, non-dialysable polymer of cranberry (NDM) on the pathogenicity of H. pylori has only been examined in vitro, but it may be possible that it could be inhibited from adhering in vivo and prevent the development of stomach ulcers. A number of Gram negative anaerobic bacteria are particularly prone to form dental biofilms. NDM can inhibit the co-aggregation of various oral bacteria in the gingival cavity and produce a 90% inhibitory effect on the enzymes responsible for synthesis of biofilm polysaccharides. Manipulation of the ecology of bacteria in the gingival cavity using cranberry could be an effective approach in controlling periodontal diseases.
Flaxseed
Lignans
Flax contains two major lignans—secoisolariciresinol diglucoside and matairesinol—the major mammalian metabolites of which are enterolactone and enterodiol. Six other lignans have been identified, and these are variably converted to enterolactone and enterodiol, and also to enterofuran. Levels of 370 mg secoisolariciresinol diglucoside per 100 g flax have been reported, but there are other sources, and a low level of 273 μg per 100 g is present in soy. Fig. 32.7 outlines the human metabolism of the major flax lignans.
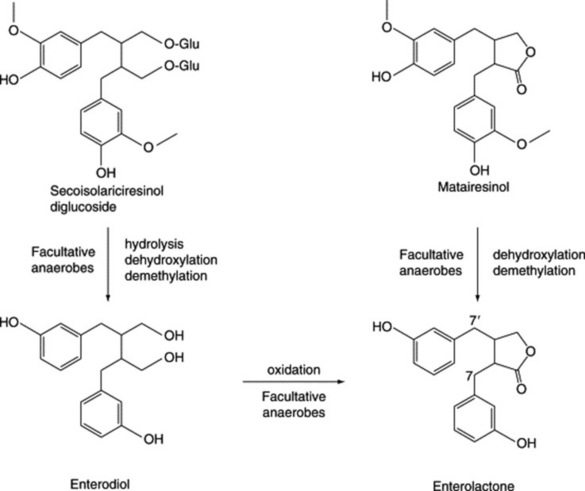
Fig. 32.7 Structures of secoisolariciresinol diglucoside and matairesinol, showing their major human metabolites. Reproduced from Rowland I, Faughnan M, Hoey L, et al. Bioavailability of phyto-oestrogens. Brit J Nutr 2003; 89: S45–S58, with permission granted by the authors and British Journal of Nutrition.
α-Linoleic acid
There are many sources of α-linoleic acid, flaxseed being the richest, but candlenut, hemp seed, pumpkin seed, canola, walnut and soy contain lesser amounts. Flaxseed oil contains more than 50% α-linoleic acid, which is an essential fatty acid. A high consumption of dietary α-linoleic acid has been shown to result in a reduced prevalence of carotid artery plaques and reduced intima-media thickness of the arteries. However, epidemiological studies have shown that a high intake or blood level of α-linoleic acid can increase the incidence of prostate cancer. Flax lignans have been shown to produce a 73% reduction in the development of hypercholesterolaemic atherosclerosis.
Flaxseed has reported anticancer properties, which are thought to be caused by the lignans, but flaxseed oil (containing α-linoleic acid as the major fatty acid) has also been shown to have activity against metastasis. A significant inverse relationship between the metabolite serum enterolactone level and breast cancer incidence has been reported.
The lignan metabolites, enterodiol and enterolactone, are thought to be weakly oestrogenic and/or antioestrogenic, and may be of use against hormone-dependent cancers.
In one study into menopausal symptoms, supplementation of women’s diets with 40 g/day of flaxseed was shown to produce a decrease in the number of hot flushes, and attenuated menopausal symptoms. A number of studies have confirmed the positive benefits of flax on hot flushes and vaginal dryness, and it is likely that consumption of 40 g or more of flaxseed is required to elicit beneficial effects, whereas 25 g is insufficient.
Olives
The oil extracted from the flesh contains at least 30 phenolic constituents, the major ones being oleuropein, hydroxytyrosol and tyrosol, and these are all powerful antioxidant and radical scavengers. Hydroxytyrosol is a hydrolysis product of oleuopein, and increases in concentration during ripening of the fruit. Both of these have antimicrobial activity. In addition, a hydroxycinnamic derivative, verbascocide, and pinoresinol lignans have been identified. Fig. 32.8 shows a number of major olive phenolics.
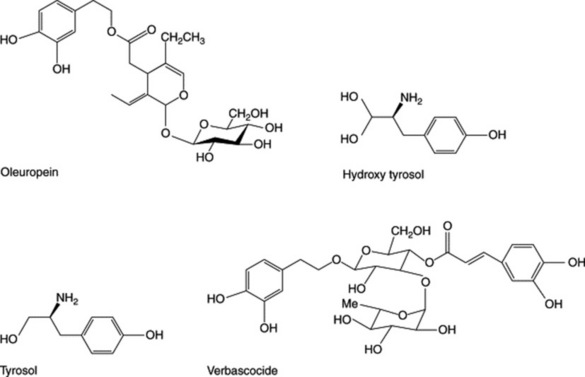
There is a large amount of epidemiological data concerning the ‘Mediterranean diet’, and olive oil in particular. Studies have shown that populations with high olive oil consumption (c. 50 g/day) have a low incidence of associated coronary heart disease, and this is thought to be due to the 25 mg of olive phenolics ingested daily. Animal studies have shown oleuropein to lower blood pressure, relieve arrhythmias and prevent internal muscle spasms. Oleuropein and verbascoside have been found to inhibit platelet aggregation. Bactericidal and bacteriostatic activity of oleuropein and its metabolites have been demonstrated against many organisms, and also inhibit growth and enterotoxin B production by Staphylococcus aureus. Oleuropein and other olive phenolics have been found to inhibit growth of E. coli and other organisms, and verbascoside also has similar activity.
The antioxidant ability of most of these constituents is thought to be responsible for protective activity against a number of cancers, notably breast, prostate and colon cancers, coronary heart disease and the effects of ageing.
Pomegranate
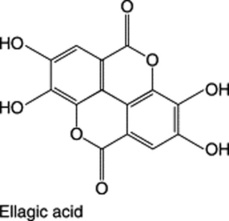
The constituent present in the highest concentration is punicalagin, which is the major fruit ellagitannin. It also contains ellagic acid in free and bound forms, gallotannins and anthocyanins (cyanidin, delphinidin and pelargonidin glycosides), and other flavonoids (quercitin, kaempferol and luteolin glycosides). The structure of ellagic acid is shown in Fig. 32.8. There is great variability in levels of these constituents between the juice and pericarp, and a range of extracts and individual components has been investigated for biological activity. Comparison of activities of these extracts and individual entities with the popular commercially available pomegranate juice can lead to difficulties.
The antibacterial activity of four different extracts from pomegranate fruit rind on a number of organisms have been reported, and the methanolic extract has also been shown to act synergistically with five different antibiotics against isolated strains of methicillin-resistant Staphylococcus aureus (MRSA) and methicillin-sensitive Staphylococcus aureus (MSSA) have been reported. The antiviral activity of pomegranate has been investigated, and it was found that a mixture of ferrous salt and pomegranate rind extract reduced the infectivity of the poliovirus, herpes simplex virus type 1 (HSV-1) and human immunodeficiency virus type 1 (HIV-1) in cell culture assays, indicating a possible use in halting the spread of these diseases. A link between the antioxidant activity of juice polyphenols and antiatherogenic effects has been reported, using both humans and mice. This activity was attributed to the antioxidant capacity of the juice to reduce lipid peroxidation in lipoproteins, macrophages and platelets, with tannins being implicated in some of these effects. Evidence indicates a possible therapeutic use of pomegranate juice in realistic daily doses (50 ml/day, and for 240 ml/day in CHD).
A methanolic extract of pomegranate flower has been investigated for activity in diabetes, and was found to inhibit the increase in plasma glucose in rats loaded with glucose after 6 weeks of treatment.
The effects on a range of cancers have been researched. Pomegranate constituents may interfere with colon cancer cell formation and progression at multiple points. A significant effect of pomegranate fermented juice on breast cancer in vitro, has been reported, however, few in vivo data are available.
Possibly due to its antioxidant effects, pomegranate is an inhibitor of the markers of skin tumour promotion, along with other markers that could signify further anticancer activities. The constituents responsible for these activities are unknown, pomegranate fractions have shown the potential to prevent UV-B mediated events that could lead to the development of skin cancer. Different pomegranate fractions have shown possible synergistic, interactions against the proliferation and invasiveness of prostate cancer cells. Other areas of possible therapeutic activity include chronic obstructive pulmonary disease, neurological protection, and erectile dysfunction.
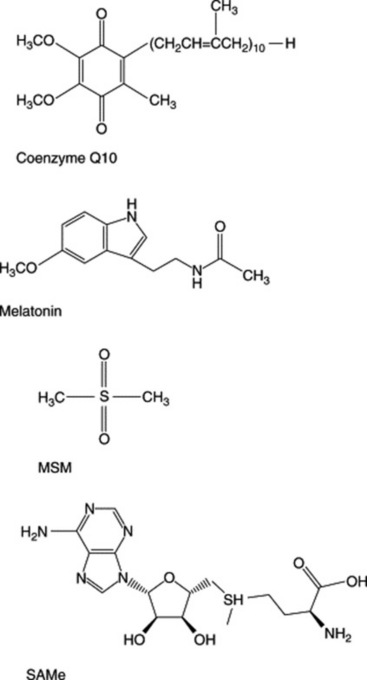
Coenzyme Q10
Coenzyme Q10 occurs widely in vegetables, particularly spinach, and it has been estimated that the average level in human plasma is 1 mg/l in human plasma. It is a powerful antioxidant and free-radical scavenger, and is manufactured and used as a medicine in Japan.
Coenzyme Q10 occurs naturally in the body and is mainly located in the mitochondria of myocardium, liver and kidney cells. It acts as an electron carrier in the mitochondrial synthesis of ATP, has membrane-stabilizing effects and has been used for the treatment of cardiovascular diseases, including heart failure, hypertension, angina and arrhythmias, although the evidence to support its use is contradictory. Significantly reduced levels of myocardium coenzyme Q10, of the order of 50% of normal levels, have been reported in heart failure in animals and humans. Contradictory results have been reported in trials using coenzyme Q10 supplementation in heart failure patients.
Deficiency in coenzyme Q10 has been shown to be significantly higher in cancer patients and asthmatics than in healthy people, and supplementation is thought to have beneficial effects in these disease states.
Melatonin
Endogenous levels of melatonin are a result of production by the pineal gland, normally starting as darkness falls, with maximal production between 2 and 4 a.m. Between 5 and 25 μg/day is secreted by juveniles, but levels decrease with age. In extreme diets, the consumption of plant material containing high levels of melatonin could conceivably alter serum concentrations. Melatonin has been identified in bananas, tomatoes, cucumbers and beetroots, but massive amounts of these foods would have to be eaten to achieve pharmacological doses.
Melatonin has been investigated in many different applications, due to its physiological roles. It controls the circadian rhythms, and has been widely researched as an aid to shift work adaptation, jet lag and for insomnia. The ‘melatonin replacement’ hypothesis states that age-related decline in melatonin production contributes to insomnia, and that replacement with physiological doses improves sleep. Melatonin has also been found to be a powerful free-radical scavenger and its use as an antioxidant in ageing and related problems has been studied.
Trials of melatonin in jet lag have been studied in great detail, and daily doses of melatonin from 0.5 to 5.0 mg are similarly effective when taken close to the target bedtime at the destination, when traversing five or more time zones. However, doses of 5 mg seemed to be no more effective than lower doses. The benefit is also likely to be greater with more time zones crossed, but less for travel in a westerly direction.
It is apparent that light pollution at night increases the risk of breast cancer; and the risk increases with the length of night shifts; night-shift work, including the work of flight attendants, has been shown to increase breast cancer risk by 48%. The reduced risk of breast cancer in blind women, who cannot perceive light and therefore do not have reduced melatonin levels, suggests possible beneficial activity for melatonin in cancer prevention.
The impact of melatonin on various cancers has been studied both alone and with conventional chemotherapy. Melatonin was found to reduce the death risk at 1 year, with similar effects in different cancers.
A rapid decline in melatonin secretion occurs by old age and supplementation has been suggested to be protective against degenerative conditions including osteoporosis. Bone formation/resorption cycles are also thought to follow a circadian pattern, which might in part be modulated by the cyclical secretion of melatonin.
MSM
Methylsulphonyl methane (MSM) has been found in capers and asparagus, amongst a number of food plants, and is one of the compounds responsible for the pungent urinary odour found in individuals after consumption of asparagus. It exists in human plasma at levels of about 4 mg/person, and 4–11 mg are excreted per 24 hours in the urine.
Only two trials of MSM use in patients with osteoarthritis (OA) have been conducted. One trial used 500 mg three times daily and the other 3 g twice daily, both over 2 weeks. Both resulted in statistically significant reduction in the indices for measurement of severity of OA. How MSM acts in joint disease is not known, but its actions might be due to involvement of its sulphur content in the formation of cartilage matrix.
SAMe
S-Adenosylmethionine (SAMe) is found in every living cell, where it acts as a methyl donor in over 100 reactions catalysed by methyltransferases. It acts as a precursor in the aminopropylation pathway leading to the polyamines, e.g. spermidine.
The majority of clinical applications are in the areas of depressive disorders, OA, fibromalgia and liver dysfunction. The benefits of SAMe in reduction of symptoms of OA were accidentally discovered during clinical trials for its use in depression. SAMe (either 400 mg intravenous or 1200 mg/day orally) has been shown to produce similar benefits to non-steroidal anti-inflammatory drugs (NSAIDs) in reduction of pain and functional limitation. SAMe is metaboloically unstable, and enteric formulations and salt derivatives have been used to prolong the activity.
The structures of a number of nutraceuticals obtained from non- plant sources are outlined in Fig. 32.9.
Synergistic effects
Synergistic interactions between a large number of nutraceuticals and conventional medicines have been the subject of numerous patents, although there is often little published research available. Both soy and tea components are widely quoted in these interactions.
The effects of piperine in enhancing bioavailability of a number of nutraceuticals has been reported.
Many combination products are now commercially available, often with no published supporting evidence available.
Adverse effects
The majority of nutraceuticals appear to be remarkably safe when collating data on their LD50s from a range of animal species. Interactions with prescription medicines have been reported for a number of them, including melatonin with methamphetamine, policosanol with aspirin, warfarin with cimetidine, SAMe with clomipramine, and coenzyme Q10 with warfarin. Prescription medicines have also been reported to depress levels of nutraceuticals; coenzyme Q10 levels have been adversely affected by a number of these, particularly the statins. Overall, a small range of adverse effects are documented, for the majority these are minor gastrointestinal problems, but caution has been advised with soy products.
Quality of commercially available products
The quality of a number of formulated plant nutraceuticals has been reviewed, but no data are available for resveratrol or pycnogenol products. Poor quality has been reported for a number of these products, based on comparison with levels stated on the labels, and similar great variability in levels of active constituents has been found in flaxseed products, teas, grape products and wines, and soy foods. Similarvariability will undoubtedly occur in other food sources such as the constituents of cocoa and chocolate, cranberry, olives or pomegranate.
Conclusions
There are a number of clearly defined single component nutraceuticals with both in vitro and clinical evidence to substantiate their usage. However, others have limited available evidence.
The situation regarding complex supplements, e.g. tea and soy, makes it exceedingly difficult to effectively quantify the evidence, simply because of their complex nature. This fact often makes it difficult to establish which constituent(s) are demonstrating the effects; there is also the associated problem that it is at present unknown whether synergistic effects or the effects of the food matrix are responsible for the reported effects. Similar problems in identification of the precise origin of any effects can occur with grape products containg both resveratrol and GSPE. GSPE, pycnogenol, tea and chocolate all contain catechins and procyanidins, which are most likely the cause of their activity; these components also occur widely in a number of edible plants.
The majority of plant nutraceuticals are antioxidant and, although we have been aware of their claimed benefits for many years, it is apparent that the picture is not clear. It has been proposed that although humans are continually exposed to reactive oxygen species (ROS), we derive most from the oxygen we breathe. Plants are also exposed to high levels of oxidative stress as they produce oxygen via photosynthesis. It is postulated that they synthesize a range of antioxidants to compensate. However, these particular food sources of antioxidants also produce high levels of ROS in the form of H2O2. It has been claimed that this situation stimulates a response from human antioxidant systems, but that excessive levels of antioxidant nutraceuticals do not work because they help generate excessive levels of ROS!
Davies E, Greenacre D, Lockwood GB. Adverse effects and toxicity of nutraceuticals. Reviews in Food and Nutrition Toxicity. 2005;3:165-195.
Eschenauer G, Sweet BV. Pharmacology and therapeutic uses of theanine. American Journal of Health-System Pharmacy 63. 2006;26:28-30.
Lockwood GB. Nutraceutical supplements. Encyclopedia of Pharmaceutical Technology. 2005:1-23.
Lockwood GB. Nutraceuticals: a balanced view for healthcare professionals. London: Pharmaceutical Press, 2007.
Melton S. The antioxidant myth. New Scientist, August. 2006;5:40-43.
Payne E, Potts L, Lockwood B. Nutraceuticals for cardiovascular protection. In: Starks TP, editor. Focus on nutrition research. Haupauge, NY, pp 1–32: Nova Science Publishers, 2007.
Rapport L, Lockwood B. Nutraceuticals. London: Pharmaceutical Press, 2002;27-76. 97–136
Soler-Rivas C, Espin JC, Wichers HJ. Oleuropein and related compounds. Journal of the Science of Food and Agriculture. 2000;80:1013-1023.